

Plasma Cell-Free DNA as a Novel Biomarker for the Diagnosis and Monitoring of Atherosclerosis

 ,
, 
Abstract
1. Introduction
2. Materials and Methods
2.1. Study Cohort
2.2. Sample Preparation and Extraction of cfDNA
2.3. Estimation of DNA Integrity and Concentration of cfDNA
2.4. Laboratory Analyses
2.5. CIMT Measurements
2.6. Animal Models
2.7. Statistical Analysis
3. Results
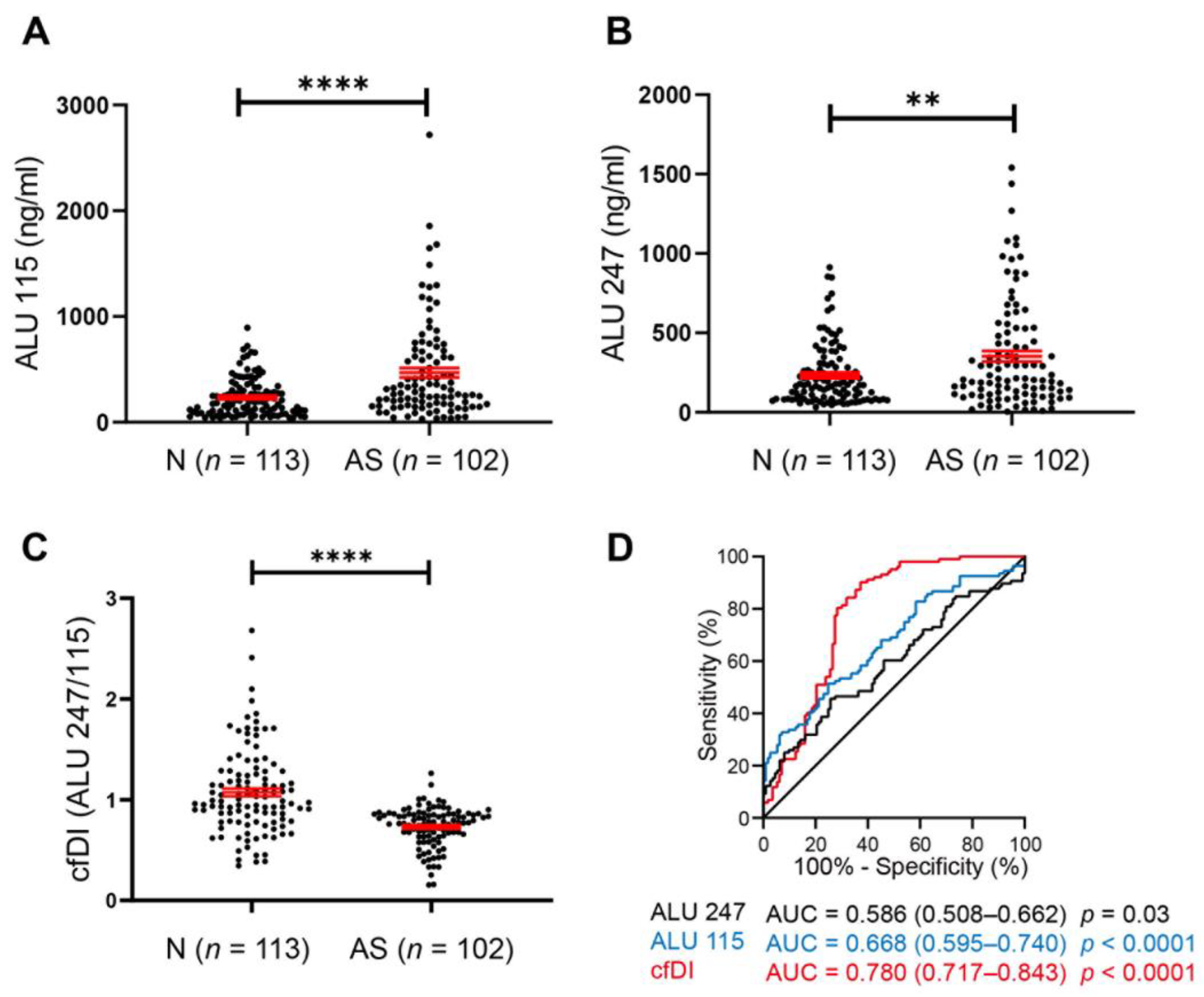
3.1. Diagnostic Role of cfDNA in Human AS Patients
3.2. Decrease in cfDI Is Associated with Plaque Progression
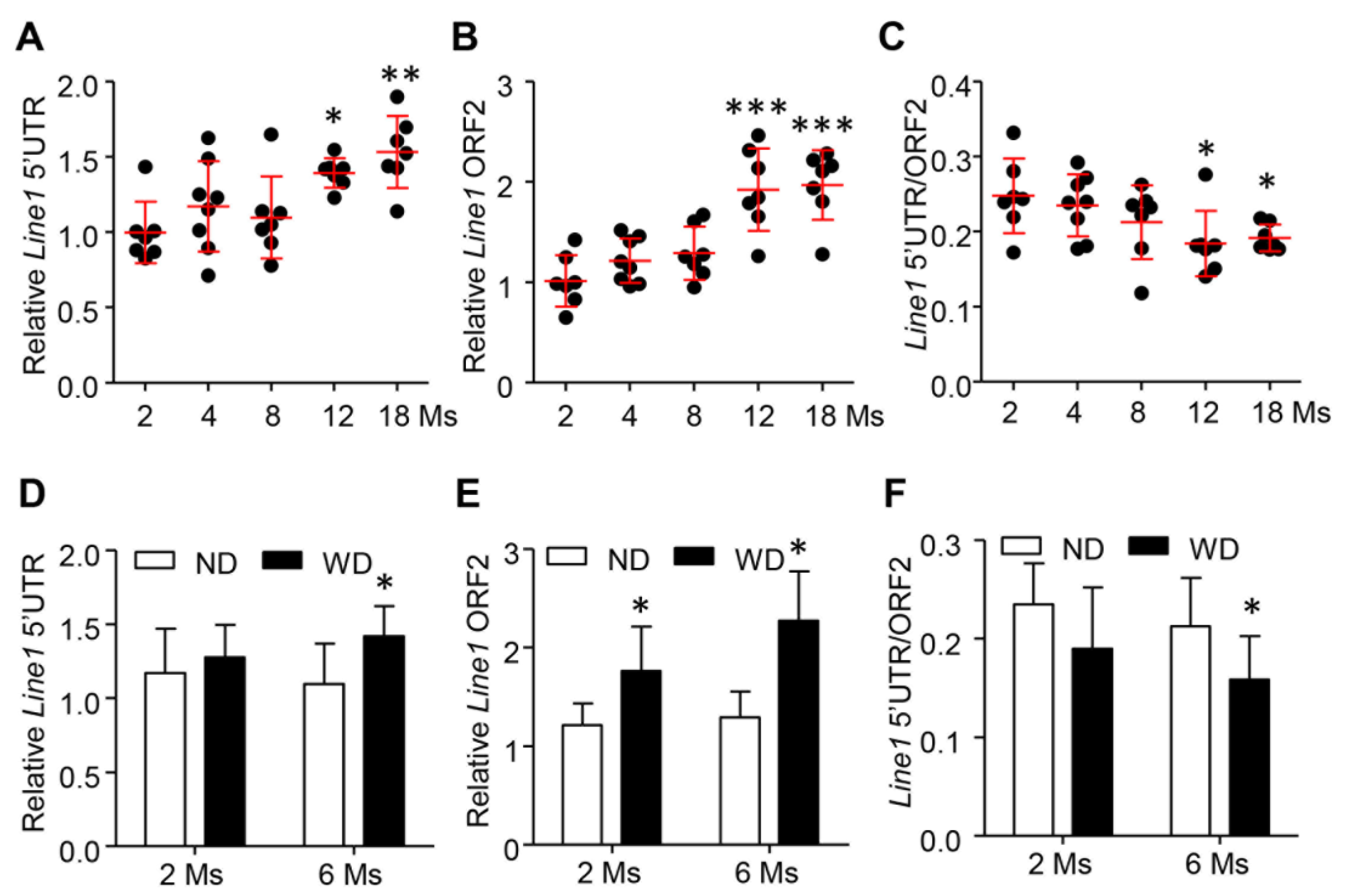
3.3. Release and Cleavage of cfDNA Were Gradually Increased during the Development of AS in ApoE−/− Mice
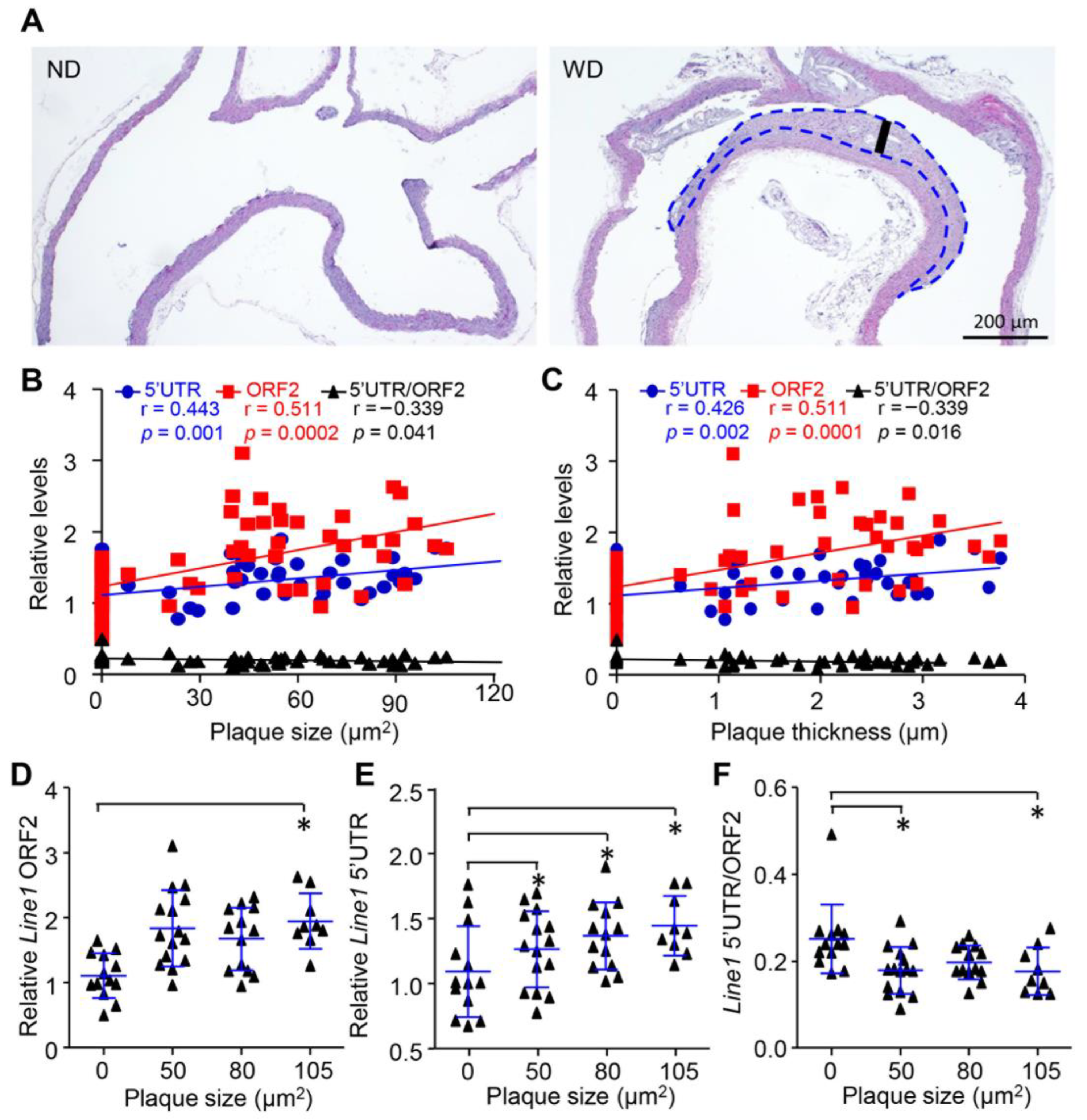
3.4. Release and Cleavage of cfDNA Were Associated with Plaque Progression In Vivo
4. Discussion
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Lo, Y.M.D.; Han, D.S.C.; Jiang, P.; Chiu, R.W.K. Epigenetics, fragmentomics, and topology of cell-free DNA in liquid biopsies. Science 2021, 372, eaaw3616. [Google Scholar] [CrossRef] [PubMed]
- Sidaway, P. cfDNA monitoring is feasible in SCLC. Nat. Rev. Clin. Oncol. 2020, 17, 7. [Google Scholar] [CrossRef] [PubMed]
- Seton-Rogers, S. Closing in on cfDNA-based detection and diagnosis. Nat. Rev. Cancer 2020, 20, 481. [Google Scholar] [CrossRef] [PubMed]
- Campos-Carrillo, A.; Weitzel, J.N.; Sahoo, P.; Rockne, R.; Mokhnatkin, J.V.; Murtaza, M.; Gray, S.W.; Goetz, L.; Goel, A.; Schork, N.; et al. Circulating tumor DNA as an early cancer detection tool. Pharmacol. Ther. 2020, 207, 107458. [Google Scholar] [CrossRef] [PubMed]
- Lo, Y.M.D.; Chan, K.C.A.; Sun, H.; Chen, E.Z.; Jiang, P.; Lun, F.M.F.; Zheng, Y.W.; Leung, T.Y.; Lau, T.K.; Cantor, C.R.; et al. Maternal Plasma DNA Sequencing Reveals the Genome-Wide Genetic and Mutational Profile of the Fetus. Sci. Transl. Med. 2010, 2, 61ra91. [Google Scholar] [CrossRef]
- Ulz, P.; Thallinger, G.G.; Auer, M.; Graf, R.; Kashofer, K.; Jahn, S.W.; Abete, L.; Pristauz, G.; Petru, E.; Geigl, J.B.; et al. Inferring expressed genes by whole-genome sequencing of plasma DNA. Nat. Genet. 2016, 48, 1273–1278. [Google Scholar] [CrossRef]
- Lamminaho, M.; Kujala, J.; Peltonen, H.; Tengström, M.; Kosma, V.-M.; Mannermaa, A. High Cell-Free DNA Integrity Is Associated with Poor Breast Cancer Survival. Cancers 2021, 13, 4679. [Google Scholar] [CrossRef]
- Higazi, A.M.; El Hini, S.H.; El-Sharkawy, E.A.; Gayyed, M.F.; Aziz, N.A.; Matta, R.A. Diagnostic Role of Cell-free DNA Integrity in Thyroid Cancer Particularly for Bethesda IV Cytology. Endocr. Pr. 2021, 27, 673–681. [Google Scholar] [CrossRef]
- Stamenkovic, S.; Cheng, J.; Surowy, H.; Burwinkel, B.; Gündert, M. Circulating cell-free DNA variables as marker of ovarian cancer patients: A pilot study. Cancer Biomark. 2020, 28, 159–167. [Google Scholar] [CrossRef]
- Ranucci, R. Cell-Free DNA: Applications in Different Diseases. Methods Mol. Biol. 2019, 1909, 3–12. [Google Scholar] [CrossRef]
- Hou, Y.-Q.; Liang, D.-Y.; Lou, X.-L.; Zhang, M.; Zhang, Z.-H.; Zhang, L.-R. Branched DNA-based Alu quantitative assay for cell-free plasma DNA levels in patients with sepsis or systemic inflammatory response syndrome. J. Crit. Care 2016, 31, 90–95. [Google Scholar] [CrossRef] [PubMed]
- Mondelo-Macía, P.; Castro-Santos, P.; Castillo-García, A.; Muinelo-Romay, L.; Diaz-Peña, R. Circulating Free DNA and Its Emerging Role in Autoimmune Diseases. J. Pers. Med. 2021, 11, 151. [Google Scholar] [CrossRef] [PubMed]
- Ilatovskaya, D.V.; DeLeon-Pennell, K.Y. An Offer We Cannot Refuse: Cell-Free DNA as a Novel Biomarker of Myocardial Infarction. Am. J. Med. Sci. 2018, 356, 88–89. [Google Scholar] [CrossRef] [PubMed]
- Hao, T.B.; Shi, W.; Shen, X.J.; Qi, J.; Wu, X.H.; Wu, Y.; Tang, Y.Y.; Ju, S.Q. Circulating cell-free DNA in serum as a biomarker for diagnosis and prognostic prediction of colorectal cancer. Br. J. Cancer 2014, 111, 1482–1489. [Google Scholar] [CrossRef]
- Hussein, N.A.; Mohamed, S.N.; Ahmed, M.A. Plasma ALU-247, ALU-115, and cfDNA Integrity as Diagnostic and Prognostic Biomarkers for Breast Cancer. Appl. Biochem. Biotechnol. 2019, 187, 1028–1045. [Google Scholar] [CrossRef]
- Muotri, A.R.; Marchetto, M.C.N.; Coufal, N.G.; Oefner, R.; Yeo, G.; Nakashima, K.; Gage, F.H. L1 retrotransposition in neurons is modulated by MeCP2. Nature 2010, 468, 443–446. [Google Scholar] [CrossRef]
- Kuroki, R.; Murata, Y.; Fuke, S.; Nakachi, Y.; Nakashima, J.; Kujoth, G.C.; Prolla, T.A.; Bundo, M.; Kato, T.; Iwamoto, K. Establishment of Quantitative PCR Assays for Active Long Interspersed Nuclear Element-1 Subfamilies in Mice and Applications to the Analysis of Aging-Associated Retrotransposition. Front. Genet. 2020, 11, 519206. [Google Scholar] [CrossRef] [PubMed]
- Herrington, W.; Lacey, B.; Sherliker, P.; Armitage, J.; Lewington, S. Epidemiology of Atherosclerosis and the Potential to Reduce the Global Burden of Atherothrombotic Disease. Circ. Res. 2016, 118, 535–546. [Google Scholar] [CrossRef]
- Hansson, G.K.; Hermansson, A. The immune system in atherosclerosis. Nat. Immunol. 2011, 12, 204–212. [Google Scholar] [CrossRef]
- Libby, P. The changing landscape of atherosclerosis. Nature 2021, 592, 524–533. [Google Scholar] [CrossRef]
- Wu, L.; Pei, Y.; Zhu, Y.; Jiang, M.; Wang, C.; Cui, W.; Zhang, D. Association of N6-methyladenine DNA with plaque progression in atherosclerosis via myocardial infarction-associated transcripts. Cell Death Dis. 2019, 10, 909. [Google Scholar] [CrossRef] [PubMed]
- Munckhof, I.C.V.D.; Jones, H.; Hopman, M.T.; De Graaf, J.; Nyakayiru, J.; Van Dijk, B.; Eijsvogels, T.; Thijssen, D.H. Relation between age and carotid artery intima-medial thickness: A systematic review. Clin. Cardiol. 2018, 41, 698–704. [Google Scholar] [CrossRef] [PubMed]
- Zhang, D.; Sun, X.; Liu, J.; Xie, X.; Cui, W.; Zhu, Y. Homocysteine Accelerates Senescence of Endothelial Cells via DNA Hypomethylation of Human Telomerase Reverse Transcriptase. Arterioscler. Thromb. Vasc. Biol. 2015, 35, 71–78. [Google Scholar] [CrossRef]
- Zhang, D.; Wen, X.; Wu, W.; Xu, E.; Zhang, Y.; Cui, W. Homocysteine-related hTERT DNA demethylation contributes to shortened leukocyte telomere length in atherosclerosis. Atherosclerosis 2013, 231, 173–179. [Google Scholar] [CrossRef] [PubMed]
- Chin, R.-I.; Chen, K.; Usmani, A.; Chua, C.; Harris, P.K.; Binkley, M.S.; Azad, T.D.; Dudley, J.C.; Chaudhuri, A.A. Detection of Solid Tumor Molecular Residual Disease (MRD) Using Circulating Tumor DNA (ctDNA). Mol. Diagn. Ther. 2019, 23, 311–331. [Google Scholar] [CrossRef] [PubMed]
- Pantel, K.; Alix-Panabières, C. Liquid biopsy and minimal residual disease—Latest advances and implications for cure. Nat. Rev. Clin. Oncol. 2019, 16, 409–424. [Google Scholar] [CrossRef] [PubMed]
- Abbosh, C.; Birkbak, N.; Swanton, C. Early stage NSCLC—Challenges to implementing ctDNA-based screening and MRD detection. Nat. Rev. Clin. Oncol. 2018, 15, 577–586. [Google Scholar] [CrossRef] [PubMed]
- Moss, J.; Magenheim, J.; Neiman, D.; Zemmour, H.; Loyfer, N.; Korach, A.; Samet, Y.; Maoz, M.; Druid, H.; Arner, P.; et al. Comprehensive human cell-type methylation atlas reveals origins of circulating cell-free DNA in health and disease. Nat. Commun. 2018, 9, 5068. [Google Scholar] [CrossRef]
- Grootaert, M.O.J.; Moulis, M.; Roth, L.; Martinet, W.; Vindis, C.; Bennett, M.R.; De Meyer, G.R.Y. Vascular smooth muscle cell death, autophagy and senescence in atherosclerosis. Cardiovasc. Res. 2018, 114, 622–634. [Google Scholar] [CrossRef]
- Paone, S.; Baxter, A.A.; Hulett, M.D.; Poon, I.K.H. Endothelial cell apoptosis and the role of endothelial cell-derived extracellular vesicles in the progression of atherosclerosis. Cell. Mol. Life Sci. 2019, 76, 1093–1106. [Google Scholar] [CrossRef]
- Döring, Y.; Soehnlein, O.; Weber, C. Neutrophil Extracellular Traps in Atherosclerosis and Atherothrombosis. Circ. Res. 2017, 120, 736–743. [Google Scholar] [CrossRef] [PubMed]
- Warnatsch, A.; Ioannou, M.; Wang, Q.; Papayannopoulos, V. Inflammation. Neutrophil extracellular traps license macrophages for cytokine production in atherosclerosis. Science 2015, 349, 316–320. [Google Scholar] [CrossRef] [PubMed]
- Umetani, N.; Giuliano, A.E.; Hiramatsu, S.H.; Amersi, F.; Nakagawa, T.; Martino, S.; Hoon, D.S. Prediction of Breast Tumor Progression by Integrity of Free Circulating DNA in Serum. J. Clin. Oncol. 2006, 24, 4270–4276. [Google Scholar] [CrossRef] [PubMed]
- Mayer, E.L.; Jacobsen, D.W.; Robinson, K. Homocysteine and coronary atherosclerosis. J. Am. Coll. Cardiol. 1996, 27, 517–527. [Google Scholar] [CrossRef]
- Rosenson, R.S.; Brewer, H.B., Jr.; Ansell, B.J.; Barter, P.; Chapman, M.J.; Heinecke, J.W.; Kontush, A.; Tall, A.R.; Webb, N.R. Dysfunctional HDL and atherosclerotic cardiovascular disease. Nat. Rev. Cardiol. 2016, 13, 48–60. [Google Scholar] [CrossRef]
- Tower, J. Programmed cell death in aging. Ageing Res. Rev. 2015, 23, 90–100. [Google Scholar] [CrossRef]
- Zhang, J.-H.; Zhang, Y.; Herman, B. Caspases, apoptosis and aging. Ageing Res. Rev. 2003, 2, 357–366. [Google Scholar] [CrossRef]
- Al Sulaiman, D.; Gatehouse, A.; Ivanov, A.P.; Edel, J.B.; Ladame, S. Length-Dependent, Single-Molecule Analysis of Short Double-Stranded DNA Fragments through Hydrogel-Filled Nanopores: A Potential Tool for Size Profiling Cell-Free DNA. ACS Appl. Mater. Interfaces 2021, 13, 26673–26681. [Google Scholar] [CrossRef]
- Falk, E. Pathogenesis of Atherosclerosis. J. Am. Coll. Cardiol. 2006, 47, C7–C12. [Google Scholar] [CrossRef]
- Xiong, J.; Yu, Z.; Zhang, D.; Huang, Y.; Yang, K.; Zhao, J. A Nomogram for Identifying Subclinical Atherosclerosis in Chronic Kidney Disease. Clin. Interv. Aging 2021, 16, 1303–1313. [Google Scholar] [CrossRef]
- Xu, J.; Chen, Z.; Wang, Y.; Wang, X.; Chen, L.; Yuan, T.; Tang, X.; Lu, Y.; Chen, H.; Chen, M.; et al. Several circulating miRNAs related to hyperlipidemia and atherosclerotic cardiovascular diseases. Lipids Health Dis. 2019, 18, 104. [Google Scholar] [CrossRef] [PubMed]
- Núñez, E.; Fuster, V.; Gómez-Serrano, M.; Valdivielso, J.M.; Fernández-Alvira, J.M.; Martínez-López, D.; Rodríguez, J.M.; Bonzon-Kulichenko, E.; Calvo, E.; Alfayate, A.; et al. Unbiased plasma proteomics discovery of biomarkers for improved detection of subclinical atherosclerosis. eBioMedicine 2022, 76, 103874. [Google Scholar] [CrossRef] [PubMed]
- Tawakol, A.; Abohashem, S.; Zureigat, H. Imaging Apoptosis in Atherosclerosis: From Cell Death, A Ray of Light. J. Am. Coll. Cardiol. 2020, 76, 1875–1877. [Google Scholar] [CrossRef] [PubMed]
- Tabas, I.; Bornfeldt, K.E. Macrophage Phenotype and Function in Different Stages of Atherosclerosis. Circ. Res. 2016, 118, 653–667. [Google Scholar] [CrossRef] [PubMed]
- Xu, R.-H.; Wei, W.; Krawczyk, M.; Wang, W.; Luo, H.; Flagg, K.; Yi, S.; Shi, W.; Quan, Q.; Li, K.; et al. Circulating tumour DNA methylation markers for diagnosis and prognosis of hepatocellular carcinoma. Nat. Mater. 2017, 16, 1155–1161. [Google Scholar] [CrossRef]
- Liu, J.; Zhao, H.; Huang, Y.; Xu, S.; Zhou, Y.; Zhang, W.; Ming, Y.; Wang, X.; Zhao, S.; Li, K.; et al. Genome-wide cell-free DNA methylation analyses improve accuracy of non-invasive diagnostic imaging for early-stage breast cancer. Mol. Cancer 2021, 20, 36. [Google Scholar] [CrossRef] [PubMed]
- Liu, M.C.; Oxnard, G.R.; Klein, E.A.; Swanton, C.; Seiden, M.V.; CCGA Consortium. Sensitive and specific multi-cancer detection and localization using methylation signatures in cell-free DNA. Ann. Oncol. 2020, 31, 745–759. [Google Scholar] [CrossRef] [PubMed]





{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Clinical Factors | AS (n = 102) | N (n = 113) | ||||||||
|---|---|---|---|---|---|---|---|---|---|---|
| β | p Value | 95% CI | β | p Value | 95% CI | |||||
| Plaque size (mm2) | −2.784 | 0.006 | −0.004 | to | −0.001 | |||||
| Plaque thickness (mm) | −3.306 | 0.001 | −0.101 | to | −0.025 | |||||
| CRP (mg/dL) | −0.018 | 0.985 | −0.002 | to | 0.002 | −0.106 | 0.916 | −0.035 | to | 0.031 |
| WBC (×109/L) | −0.757 | 0.451 | −0.030 | to | 0.013 | −0.784 | 0.435 | −0.076 | to | 0.033 |
| MONO (×109/L) | −1.456 | 0.149 | −0.491 | to | 0.076 | 0.210 | 0.834 | −0.755 | to | 0.934 |
| NEUT (×109/L) | −0.466 | 0.643 | −0.032 | to | 0.020 | −1.004 | 0.318 | −0.115 | to | 0.038 |
| LYMPH (×109/L) | −0.402 | 0.688 | −0.064 | to | 0.042 | −0.132 | 0.896 | −0.154 | to | 0.135 |
| TG (mmol/L) | 1.126 | 0.263 | −0.010 | to | 0.036 | 0.753 | 0.453 | −0.043 | to | 0.096 |
| TC (mmol/L) | −0.692 | 0.490 | −0.046 | to | 0.022 | 1.098 | 0.274 | −0.039 | to | 0.136 |
| HDL (mmol/L) | −1.362 | 0.176 | −0.231 | to | 0.043 | 0.935 | 0.352 | −0.144 | to | 0.401 |
| LDL (mmol/L) | −2.640 | 0.010 | −0.100 | to | −0.014 | 0.144 | 0.886 | −0.094 | to | 0.109 |
| Apo A1 (g/L) | −2.072 | 0.041 | −0.344 | to | −0.007 | 0.662 | 0.512 | −0.436 | to | 0.860 |
| Apo B (g/L) | −1.652 | 0.102 | −0.316 | to | 0.029 | 0.888 | 0.380 | −0.411 | to | 1.052 |
| Lpα (ng/L) | −0.237 | 0.813 | 0.000 | to | 0.000 | 0.182 | 0.857 | −0.001 | to | 0.001 |
| HCY (μmol/L) | −2.857 | 0.007 | −0.009 | to | −0.002 | −0.377 | 0.707 | −0.017 | to | 0.011 |
| VB12 (pg/mL) | −0.808 | 0.427 | 0.000 | to | 0.000 | 0.222 | 0.827 | −0.048 | to | 0.060 |
| Folate (nmol/L) | −1.076 | 0.292 | −0.028 | to | 0.009 | 1.167 | 0.255 | −0.001 | to | 0.003 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Qian, B.; Li, K.; Lou, X.; Guo, Y.; Wang, Y.; Wu, L.; Zhang, D. Plasma Cell-Free DNA as a Novel Biomarker for the Diagnosis and Monitoring of Atherosclerosis. Cells 2022, 11, 3248. https://doi.org/10.3390/cells11203248
Qian B, Li K, Lou X, Guo Y, Wang Y, Wu L, Zhang D. Plasma Cell-Free DNA as a Novel Biomarker for the Diagnosis and Monitoring of Atherosclerosis. Cells. 2022; 11(20):3248. https://doi.org/10.3390/cells11203248
Chicago/Turabian StyleQian, Benheng, Kexin Li, Xiaoying Lou, Ye Guo, Yidong Wang, Lianpin Wu, and Donghong Zhang. 2022. "Plasma Cell-Free DNA as a Novel Biomarker for the Diagnosis and Monitoring of Atherosclerosis" Cells 11, no. 20: 3248. https://doi.org/10.3390/cells11203248
APA StyleQian, B., Li, K., Lou, X., Guo, Y., Wang, Y., Wu, L., & Zhang, D. (2022). Plasma Cell-Free DNA as a Novel Biomarker for the Diagnosis and Monitoring of Atherosclerosis. Cells, 11(20), 3248. https://doi.org/10.3390/cells11203248