1. Introduction
Titanium, which has been established as a classic material with optimal biological properties, is used for both implants and superstructures, but its unaesthetic surface may be a prerequisite for unsatisfactory aesthetic results [
1,
2]. Highly aesthetic restorative ceramic materials could compensate for this shortcoming and have relatively predictable behavior in prosthetic restoration, but their application on implant supports still raises some debatable questions [
1,
3,
4,
5]. LDS ceramics have high optical and mechanical properties. Their bending strength of 350–400 MPa and fracture toughness of 3.5–4.5 K render them suitable for making monolithic restorations with high aesthetic characteristics [
1,
3,
6]. LDS is considered more aesthetic than zirconium dioxide, which has lower translucency, and its whiter color often cannot meet the high aesthetic criteria [
7,
8].
The examined fatigue of monolithic single-implant restorations of LDS on a central incisor compared to the same restorations cemented on a tooth shows the highest survival rate in the test group of implants, which confirms that this type of superstructure could successfully withstand the masticatory forces in the oral cavity but should be used carefully, according to the indications and the clinical situation [
2,
4,
9,
10,
11].
The study of some mechanical characteristics, such as fatigue, impact strength, and micro-permeability of the implant superstructures made of different materials in the front and distal areas, as well as their biological characteristics in relation to the soft tissues in the oral cavity, will lead to recommendations for their optimal application. Another weak point of titanium base abutment and its restoration is the adhesive connection between the titanium base abutment and the ceramic superstructure, which is essential for long-term clinical success. For the cement space evaluation, the proper internal cement gap of the conventional fabricated all-ceramic crown, e.g., slip casting or hot pressing technique, is within a range of 25–50 μm. A space of 25–30 μm is provided for the cement and space of 20 μm compensates for distortion of the wax pattern [
9].
Most studies focus on one group of teeth and do not provide a definitive prescription for the use of the material over a commercial titanium base in different teeth groups considering their specific morphological characteristics, especially in the critical transmucosal area. There is a lack of studies concerning a titanium base with preconditioned bonding surface for single tooth restorations as well [
1,
2,
3,
4,
9,
10].
These statements illustrate the need to study the mechanical behavior of the material adhesively cemented to a preconditioned commercial titanium bonding base and the possibilities for its application, as well as the behavior of superstructures by different tooth groups. Therefore, the aim of this study was to register the mechanical behavior and the microleakage of monolithic crown abutments made of LDS adhesively bonded to a preconditioned titanium bonding base after mechanical cycling. The working hypothesis was that the unequal thickness of the ceramic material surrounding the standard rounded titanium abutment would create critical areas at risk of fracture due to specific anatomical features and inter-individual varieties of transmucosal profiles, and that, based on natural teeth in different functional teeth groups, this could be successfully overcome by the special “soft edge” design of the bonding titanium base surface ideally suited to the LDS restoration materials, therefore supporting long-term clinical use.
2. Materials and Methods
In this in vitro study, the mechanical behavior and the microleakage of monolithic crown abutments of lithium disilicate bonded to titanium base after mechanical cycling were evaluated according to the type of teeth on three levels (central incisor, second premolar, and first molar). The sample size was calculated based on a previous study [
4,
5,
12,
13] that evaluated the mechanical performance of implants after mechanical cycling. The sample size was calculated by using a graphing software program (SigmaPlot 14.0; Systat Software, Inc., San Jose, CA, USA).
A Viteo
® titanium bonding base for single-tooth restoration abutments with 6 mm height was scanned with a high-precision laboratory laser scanner (Zirkonzahn S600 ARTI, Norcross, GA, USA). Crown restorations were CAD-designed using customized transmucosal profiles based on the natural teeth shapes (
Figure 1).
They were divided into three functional groups: upper central incisors, upper premolars, and upper first molars consisting of 11 samples each. The design, shape, and volume of the crown abutments were based on the natural tooth morphology. The transmucosal height was considered to be 3 mm.
The crown abutments were milled from IPS e.max multi-wax pattern (Ivoclar Vivadent, Schaan, Liechtenstein) using a Zirkonzahn m4 wet heavy metal-milling unit. The final restorations were pressed by IPS e.max ingots (Ivoclar Vivadent, Schaan, Liechtenstein), with minor hand work and crystallization process performed in IPS Programat press furnace, according to the manufacturer’s guidelines (e.max press ingots IPS (multi investment system)).
All samples were adhesively bonded to the Viteo® base in conformity with the manufacturer’s protocol. Each base was cleaned with a steam cleaner and blow-dried. After that, the base was screwed to the model analog and the monolithic crown was inserted. Then, the relative position was marked with a waterproof pen. Monobond Plus was applied to the base for 60 s and then the excess was distributed with air. The screw cannel was sealed with foam pellet.
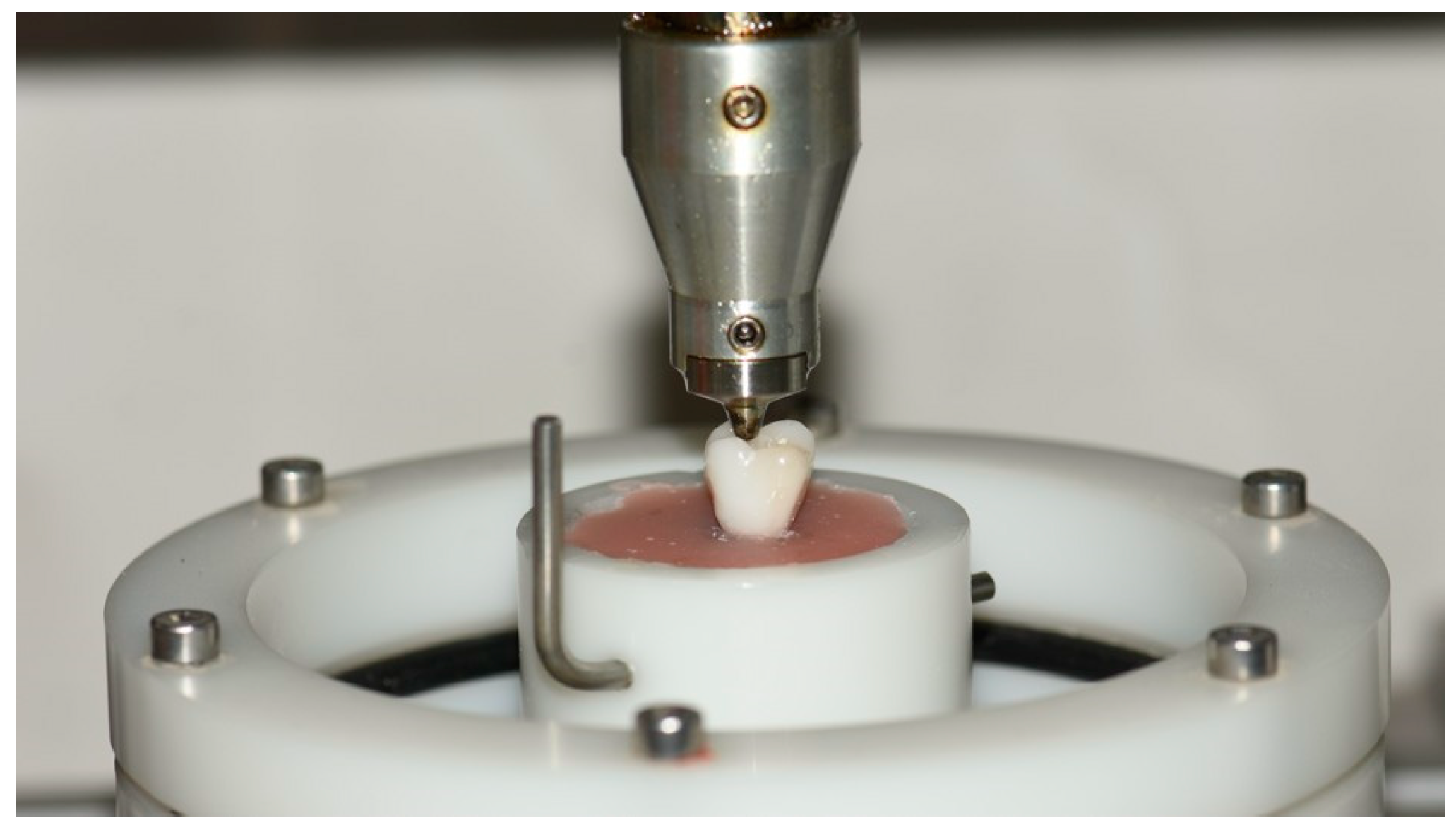
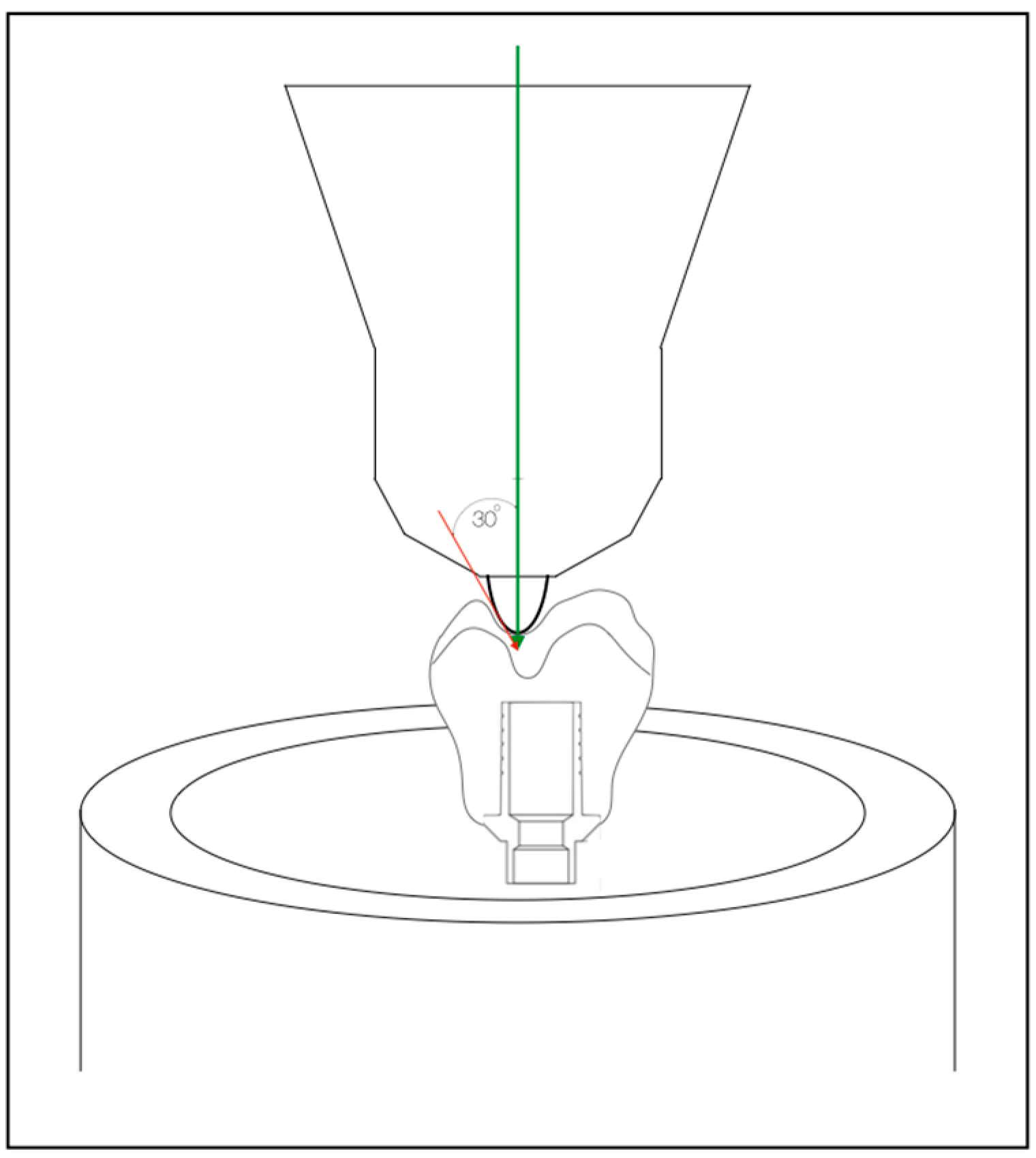
The ceramic structure was cleaned the same way as the base. Afterwards, the bonding surface was etched with 5% hydrofloric acid (IPS Ceramic Etching Gel) for 20 s. The surface was rinsed under running water and dried with air. Monobond Plus was applied and left to react for 60 s. Then the residue was distributed with dry air. A new mixing syringe was attached to the Multilink Hybrid Abutment (Ivoclar Vivadent, Schaan, Leichenstein) for cementation of each sample. A thin layer of the cement was applied to the bonding surface of the base and to the ceramic suprastructure. Afterwards, both components were assembled in alignment, according to the position of the marking waterproof pen. The parts were slightly pressed to each other, their position was checked, and they were then tightly pressed for 5 s. All probes were manually cleaned from the excess immediately after cementation with scalpel blade #15. Glycerine gel was applied on the crown margin to prevent formation of an inhibition layer. After the polymerization of the cement was completed (Bluephase Power Cure, Ivoclar Vivadent, Schaan, Leichtenstein), the glycerine gel was rinsed off with water. All crown abutments were screw-retained, attached to the implants with titanium screws and tightened up to 35 Ncm. The screws were retightened after 10 min to avoid the possibility of screw loosening. The samples were then stored in distilled water at 37 °C for 24 h before testing. All samples were subjected to dynamic loading in a computer-controlled dual-axis chewing simulator (Chewing Simulator CS-4; SD-Mechatronik, Westerham, Germany) for 250,000 loading cycles (1 clinical year of operation) at a frequency of 2 Hz. A loading force of 50 N for the group of incisors and 150 N for premolars and molars was applied by a standard sample pot steel cone 30° antagonist. Samples were embedded in the sample pots with PMMA and steel cone antagonist touching the crown. Vertical strokes were performed according to the manufacturer’s recommendations (
Figure 2 and
Figure 3).
After the loading cycles were completed, specimens were immersed in freshly mixed 5% methylene blue dye solution for 24 h at 37 °C. After the dye exposure, the specimens were thoroughly washed under running tap water for 5 min (
Figure 4).
Microleakage staining was observed with a stereomicroscope (SteREO Discovery V8; Carl Zeiss Microscopy GmbH, Jena, Germany) at ×8 magnification and classified by using a semiquantitative numerical scale—13.17:0 (no staining present), 1 (staining around connections shoulder), 2 (staining around hexagonal area of the connection), and 3 (absorbent paper point-stained).
After microleakage evaluation, seven parameters (abutment screw deformation, abutment deformation, crack or craze line on the ceramic structure, adhesive failure between titanium base and ceramic superstructure, failures in ceramic superstructure or titanium base, remaining cement around titanium base, and ceramic superstructure) were analyzed under stereomicroscope. All evaluations were performed by one experienced examinator (
Table 1).
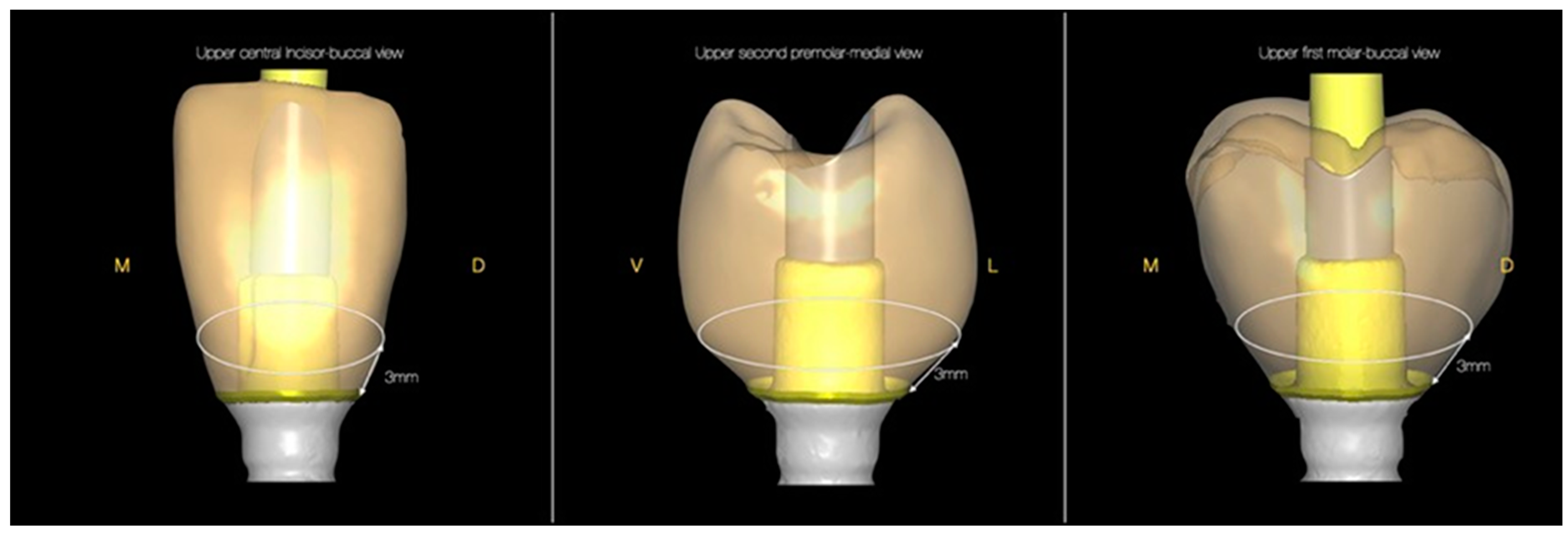
All samples were virtually sectioned horizontally at 3 mm above the implant platform to analyze the volume and thickness of the ceramic material around the compared standard titanium base abutment (
Figure 5 and
Figure 6).
The remaining thickness of the material was measured in the medial, distal, buccal, and palatal areas (
Table 2).
3. Results
Table 1 shows the frequency of registered incidents of the parameters analyzed after the mechanical loading. One fracture was observed in the group of the premolars after loading of 5500 cycles. Fracture lines were drawn over the medial and distal walls. The cement layer of the fractured sample remains on the ceramic surface and the titanium base was clean.
Considering the type of teeth, there are eight defects in relation to the group of central incisors, whereas the group of first molar accounts for seven defects. Second premolar accounts for eleven defects. Despite variations in the number of defects, descriptive statistics measures alone cannot provide definitive conclusions as to whether the observed results are significantly different.
A significant accumulation of dye was registered in all teeth groups, i.e., grade 2 (staining around hexagonal area of the connection), according to the applied scale. It is important to note that the total amount of microleakage tends to vary depending on the type of teeth under consideration (
Table 3). According to the statistical analysis, differences in the microleakage values were not statistically significant (
p = 0.93). Thus, the three groups of teeth show similar microleakage scores when taking into consideration the cumulative outcomes for each group. This conclusion also shows that microleakage takes place regardless of the type of teeth.
ANOVA was also applied in comparing the results from the seven assessed parameters. In this scenario, the combined results from the three groups of teeth were used as a basis for summing up the number of defects per parameter. The purpose of the analysis is to show whether the number of defects remains statistically different depending on the specific parameter under consideration. Initial considerations reveal that such a statistical difference is quite possible given the fact that most defects are concentrated within the “Remaining cement around titanium base and ceramic superstructure” test group. More specifically, this group accounts for 23 out of 26 defects in total. The results from
Table 1 also show that three types of testing parameters do not produce any defects at all. Considering these initial descriptive statistical results, statistical significance of the results is quite likely (
Table 4).
The results from the ANOVA test across techniques confirm the initial expectations. More specifically, the value of F stat is 127—much higher than the significance threshold of 2.85. This also yields a statistically significant p-value of 0.00. Therefore, ANOVA results unambiguously show that defects are unequally distributed across parameters and concentrated in the “Remaining cement around titanium base and ceramic superstructure” test group. These important results demand further analysis.
4. Discussion
According to the working hypothesis of the study, due to the specific anatomical features and inter-individual varieties of transmucosal profiles based on the natural teeth shapes in the different functional teeth groups, the unequal thickness of the ceramic material surrounding the standard rounded titanium abutment would create critical areas at risk of fracture. The measurements coincided with the working hypothesis; therefore, it was accepted.
The subjects of most studies are the groups of molar teeth [
3,
5,
9]. In vitro studies report results on central incisors while only a few of them consider the group of premolar teeth restored with monolithic porcelain restorations on titanium bases [
4,
10].
Existing differences in material and methods make it difficult to perform comparative analysis between the examined dental groups in the different studies. The range of applied masticatory load varies between 200,000 and 1.2 million chewing cycles, which is equivalent to 1 to 5 clinical years of operation. The frequency used is also different and ranges from 0.8 to 2 Hz. Variations also exist in the masticatory pressure force used. Taking into consideration all of these critical points, three test groups were selected and loaded for masticatory simulation equivalent to 1 clinical year of function [
14,
15,
16]. The selected groups included maxillary central incisors, second premolars, and first molars, due to the significant variability in the cervical shape and volume in the different dental groups. This pilot study aimed to determine whether there was a difference in fatigue and an adhesive bond between the different dental groups under the same conditions, and to serve as a starting point for clinical trial design and in vivo comparison between the study groups.
Single restorations of LDS have been well studied in natural teeth, with material fatigue tested on crowns of varying occlusal material thickness. Therefore, specially designed LDS crowns were used in this study in order to recreate the natural tooth morphology and natural emergence profile as much as possible. There are many factors which play an important role in the resistance of the restorations, such as the intra-individual variety of the cervical shape of each tooth group, as well as between the groups in general. Usually, the position of the titanium base was not centered and the peripheral thickness of ceramic material could be critically reduced. The diameter of the deep sub-gingival part and the marginal part of the emergence profile of the restoration differed in the tooth groups, depending on the volume and quality of the surrounding soft tissues. After the evaluation of the initial hypothesis, with a scheme of standardized teeth slices at 3 mm below the CJ line and compared to the standard titanium base abutment, a critical thickness of the ceramic wall of 0.5 mm was chosen. The established critical areas were the medial and distal proximal walls of the molar, the disto-lingual walls of the central incisor, and the proximal walls of the premolar, where the thickness of the ceramic material around the abutment was critically low. These measurements coincided with the results established in the virtually sectioned 3D samples. A fracture of one of the premolar samples was observed over both the medial and distal walls of the restoration, which are the critical areas at risk of fracture. A smooth relationship between the titanium bonding Viteo
® base and the restorative material is the basis for a strong bond that will withstand external influences, which coincided with the working hypothesis; therefore, it was accepted (
Figure 7).
Different studies report high survival rates of samples of titanium bases and monolithic superstructures of LDS, while others report a failure rate of 43.8% when testing the same specimens [
1,
2,
4,
12].
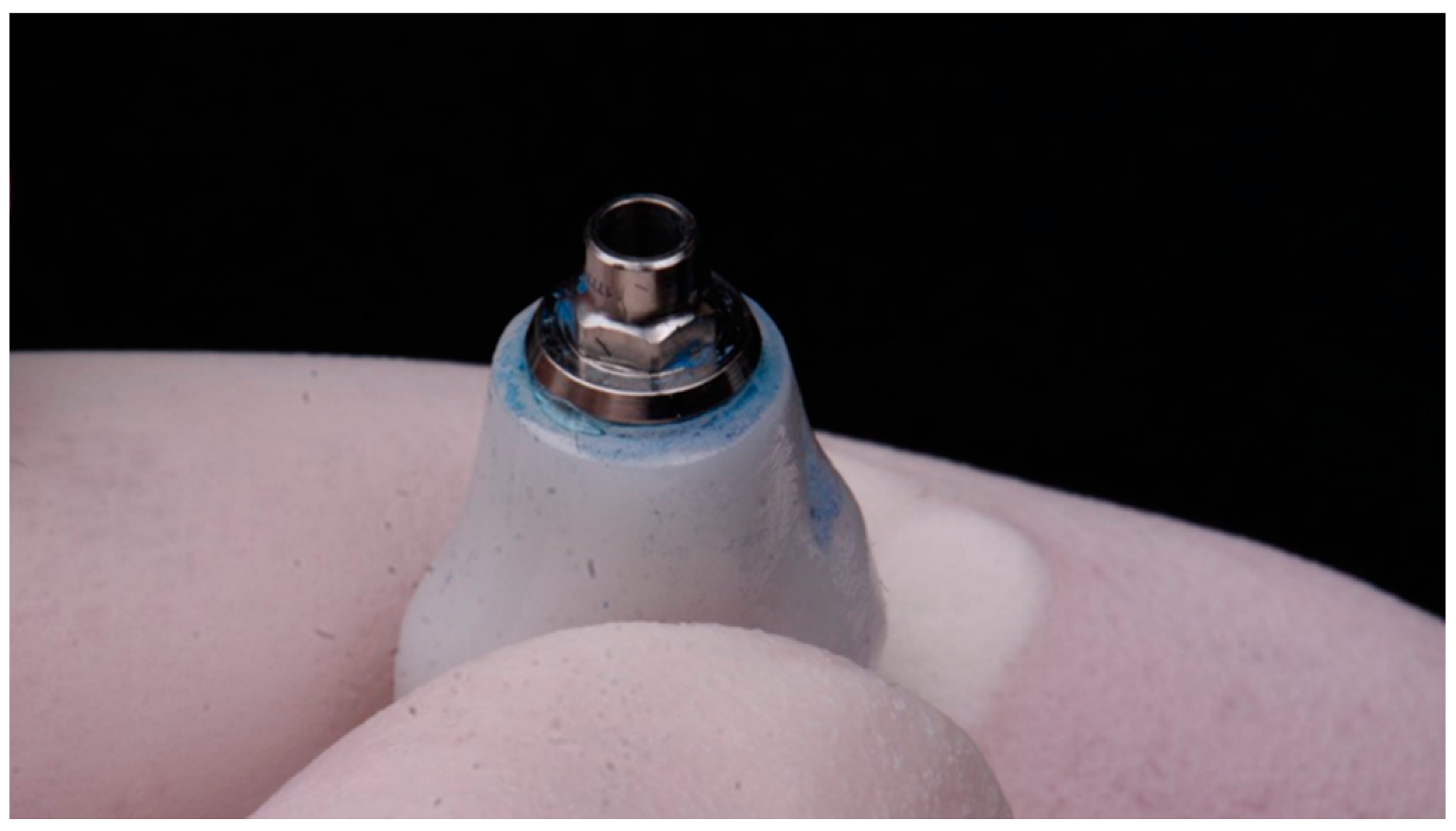
To ensure sufficient fracture resistance of the samples, the LDS part of the abutment was slightly thickened in the connection area with the subsequently placed titanium base platform. This production defect lead to over-contour profile of the restoration, which became a plaque-retentive area, and the excess of the cement could not be properly cleaned. This was visible from the significant accumulation of methylene blue dye in that area (
Figure 8).
All probes were manually cleaned from the excess immediately after cementation with scalpel blade #15. The accumulated methylene blue formed an extremely thin layer on the remaining cement over the cervical area of the hybrid abutments of all study groups. This was classified as type 2 on the used scale [
13,
17]. This confirmed that all excess should be precisely cleaned. The sub-gingival areas should be machine-polished with rubber under magnification to maximum smoothness. The positive crown edge should be finished and “riveted” in order to avoid compromising the adhesive bond in the long run and creating plaque-retentive zones.
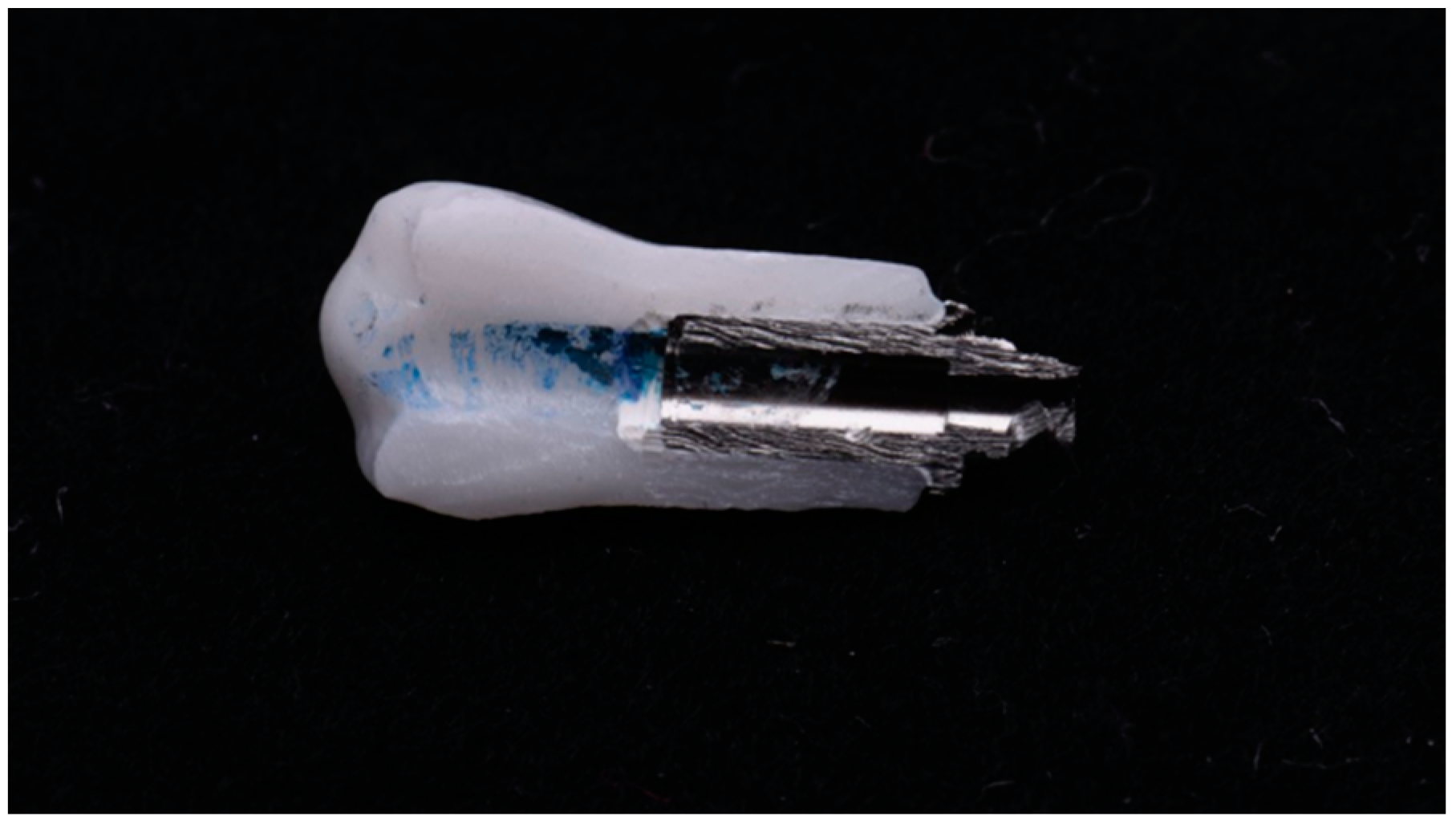
All samples were vertically sectioned through the center of the restorations, from the mesial to the distal surface, with a water-cooled diamond saw with 1 mm thickness. However, no dye penetration was registered (
Figure 9).
According to some authors [
18,
19], microleakage evaluation with methylene blue dye solution is a reliable method for examination. The size of the dye particles is similar to the size of bacteria, which infiltrates the area around the implants and inoculates the micro-gap, causing inflammation.
The long-term stability of LDS abutment crowns is related to the stability of the adhesive bond between the titanium base and the ceramic restoration. There was no difference in the adhesive bond strength in the different tooth groups and the fatigue of the material did not have a significant impact on its strength.
Despite wide consideration of these results, and despite the satisfactory strength of the lithium disilicate, many claim that it should not be the first choice of material for distal implant restorations [
4,
14,
20].
5. Conclusions
The failure of hybrid abutments could be related to the correct seal between the titanium base and the ceramic restorations. The soft-edge design and the bonding surface of titanium base are ideal for CAD/CAM and press LDS materials, thus supporting the clinical success of the restoration.
The type of teeth could also be related to the presence of failures due to inter-individual varieties of transmucosal profiles. The minimum wall thickness has to be maintained at all times. The preconditioned bonding surface ensures quick and reliable bonding and reduces the risk of fractures.
Author Contributions
Conceptualization, G.I. and D.F.; methodology, D.S.; software, B.T.; validation, G.I. and D.F.; formal analysis, G.I.; investigation, D.S.; resources, D.S.; data curation, B.T.; writing—original draft preparation, D.S.; writing—review and editing, G.I.; visualization, D.F.; supervision, D.F.; project administration, D.J. All authors have read and agreed to the published version of the manuscript.
Funding
This research received no external funding.
Data Availability Statement
All data are presented in this study. If further information is required, please contact the corresponding author.
Conflicts of Interest
The authors declare no conflict of interest. The funders had no role in the design of the study; in the collection, analyses, or interpretation of data; in the writing of the manuscript; or in the decision to publish the results.
References
- Elsayed, A.; Wille, S.; Al-Akhali, M.; Kern, M. Comparison of fracture strength and failure mode of different ceramic implant abutments. J. Prosthet. Dent. 2017, 117, 499–506. [Google Scholar] [CrossRef] [PubMed]
- Kaweewongprasert, P.; Phasuk, K.; Levon, J.A.; Eckert, G.J.; Feitosa, S.; Valandro, L.F.; Bottino, M.C.; Morton, D. Fatigue Failure Load of Lithium Disilicate Restorations Cemented on a Chairside Titanium-Base. J. Prosthodont. 2019, 28, 973–981. [Google Scholar] [CrossRef] [PubMed]
- Preis, V.; Hahnel, S.; Behr, M.; Bein, L.; Rosentritt, M. In-vitro fatigue and fracture testing of CAD/CAM-materials in implant-supported molar crowns. Dent. Mater. 2017, 33, 427–433. [Google Scholar] [CrossRef] [PubMed]
- Nouh, I.; Kern, M.; Sabet, A.E.; AboelFadl, A.K.; Hamdy, A.M.; Chaar, M.S. Mechanical behavior of posterior all-ceramic hybrid-abutment-crowns versus hybrid-abutments with separate crowns-A laboratory study. Clin. Oral Implant. Res. 2019, 30, 90–98. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Dogan, D.O.; Gorler, O.; Mutaf, B.; Ozcan, M.; Eyuboglu, G.B.; Ulgey, M. Fracture Resistance of Molar Crowns Fabricated with Monolithic All-Ceramic CAD/CAM Materials Cemented on Titanium Abutments: An In Vitro Study. J. Prosthodont. 2015, 26, 309–314. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Heintze, S.; Reinhardt, M.; Peschke, A. Fatigue resistance of CAD/CAM all-ceramic molar crowns of reduced thickness. Dent. Mater. 2017, 33, e38. [Google Scholar] [CrossRef]
- Aboushelib, M.N.; Kleverlaan, C.J.; Feilzer, A.J. Effect of Zirconia Type on Its Bond Strength with Different Veneer Ceramics. J. Prosthodont. 2008, 17, 401–408. [Google Scholar] [CrossRef] [PubMed]
- Baldissara, P.; Llukacej, A.; Ciocca, L.; Valandro, L.F.; Scotti, R. Translucency of zirconia copings made with different CAD/CAM systems. J. Prosthet. Dent. 2010, 104, 6–12. [Google Scholar] [CrossRef]
- Ebert, A.; Hedderich, J.; Kern, M. Retention of zirconia ceramic copings bonded to titanium abutments. Int. J. Oral Maxillofac. Implant. 2008, 22, 921–927. [Google Scholar]
- Elshiyab, S.H.; Nawafleh, N.; Öchsner, A.; George, R. Fracture resistance of implant-supported monolithic crowns cemented to zirconia hybrid-abutments: Zirconia-based crowns vs. lithium disilicate crowns. J. Adv. Prosthodont. 2018, 10, 65–72. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Camatta, H.P.; Ferreira, R.M.; Ferrairo, B.M.; Strelhow, S.S.; Rubo, J.H.; Mori, A.A.; Ferruzzi, F. Mechanical Behavior and Fracture Loads of Screw-Retained and Cement-Retained Lithium Disilicate Implant-Supported Crowns. J. Prosthodont. 2021, 30, 690–697. [Google Scholar] [CrossRef] [PubMed]
- Alessandretti, R.; Borba, M.; Della Bona, A. Cyclic contact fatigue resistance of ceramics for monolithic and multilayer dental restorations. Dent. Mater. 2020, 36, 535–541. [Google Scholar] [CrossRef]
- Elsayed, A.; Wille, S.; Al-Akhali, M.; Kern, M. Effect of fatigue loading on the fracture strength and failure mode of lithium disilicate and zirconia implant abutments. Clin. Oral Implant. Res. 2018, 29, 20–27. [Google Scholar] [CrossRef]
- Verdugo, C.L.; Núñez, G.J.; Avila, A.A.; Martín, C.L.S. Microleakage of the prosthetic abutment/implant interface with internal and external connection:In vitrostudy. Clin. Oral Implant. Res. 2014, 25, 1078–1083. [Google Scholar] [CrossRef] [PubMed]
- Schultheis, S.; Strub, J.R.; Gerds, T.A.; Guess, P.C. Monolithic and bi-layer CAD/CAM lithium–disilicate versus metal–ceramic fixed dental prostheses: Comparison of fracture loads and failure modes after fatigue. Clin. Oral Investig. 2013, 17, 1407–1413. [Google Scholar] [CrossRef] [PubMed]
- Seydler, B.; Rues, S.; Müller, D.; Schmitter, M. In vitro fracture load of monolithic lithium disilicate ceramic molar crowns with different wall thicknesses. Clin. Oral Investig. 2014, 18, 1165–1171. [Google Scholar] [CrossRef] [PubMed]
- Zhao, K.; Wei, Y.-R.; Pan, Y.; Zhang, X.-P.; Swain, M.; Guess, P.C. Influence of veneer and cyclic loading on failure behavior of lithium disilicate glass-ceramic molar crowns. Dent. Mater. 2014, 30, 164–171. [Google Scholar] [CrossRef] [PubMed]
- Ortega-Martínez, J.; Delgado, L.M.; Ortiz-Hernández, M.; Punset, M.; Cano-Batalla, J.; Cayon, M.R.; Cabratosa-Termes, J. In vitro assessment of PEEK and titanium implant abutments: Screw loosening and microleakage evaluations under dynamic mechanical testing. J. Prosthet. Dent. 2020, 127, 470–476. [Google Scholar] [CrossRef]
- Wachtel, A.; Zimmermann, T.; Spintig, T.; Beuer, F.; Müller, W.-D.; Schwitalla, A.D. A Novel Approach to Prove Bacterial Leakage of Implant-Abutment Connections In Vitro. J. Oral Implant. 2016, 42, 452–457. [Google Scholar] [CrossRef] [PubMed]
- Weyhrauch, M.; Igiel, C.; Scheller, H.; Weibrich, G.; Lehmann, K.M. Fracture Strength of Monolithic All-Ceramic Crowns on Titanium Implant Abutments. Int. J. Oral Maxillofac. Implant. 2016, 31, 304–309. [Google Scholar] [CrossRef] [PubMed]
Figure 1.
The hybrid crown abutments milled from IPS e.max multi-wax pattern (Ivoclar Vivadent, Shaan, Liechtenstein).
Figure 1.
The hybrid crown abutments milled from IPS e.max multi-wax pattern (Ivoclar Vivadent, Shaan, Liechtenstein).
Figure 2.
Dynamic loading of upper molar with masticatory simulator (CS-4, SD Mechatronik, Westerham, Germany) for fatigue testing. Embedded implant with crown in standard sample pot. Steel cone antagonist adjusted to touch the crown at the fissure.
Figure 2.
Dynamic loading of upper molar with masticatory simulator (CS-4, SD Mechatronik, Westerham, Germany) for fatigue testing. Embedded implant with crown in standard sample pot. Steel cone antagonist adjusted to touch the crown at the fissure.
Figure 3.
Dynamic loading with masticatory simulator scheme. Vertical stroke up: 2 mm, vertical stroke down: 2.5 mm, speed up: 60 mm/s, speed down: 20 mm/s, horizontal stroke: 0 mm, speed: 20 mm/s.
Figure 3.
Dynamic loading with masticatory simulator scheme. Vertical stroke up: 2 mm, vertical stroke down: 2.5 mm, speed up: 60 mm/s, speed down: 20 mm/s, horizontal stroke: 0 mm, speed: 20 mm/s.
Figure 4.
Hybrid abutment specimens after the dye exposure, thoroughly washed under running tap water for 5 min.
Figure 4.
Hybrid abutment specimens after the dye exposure, thoroughly washed under running tap water for 5 min.
Figure 5.
Three-dimensional model of standardized abutments virtually sectioned horizontally at 3 mm above the implant platform. Front view.
Figure 5.
Three-dimensional model of standardized abutments virtually sectioned horizontally at 3 mm above the implant platform. Front view.
Figure 6.
Three-dimensional model of standardized abutments virtually sectioned horizontally at 3 mm above the implant platform. Occlusal view of critical areas at risk of fracture.
Figure 6.
Three-dimensional model of standardized abutments virtually sectioned horizontally at 3 mm above the implant platform. Occlusal view of critical areas at risk of fracture.
Figure 7.
Fracture lines over the medial and distal walls. The cement layer of the fractured sample remains on the ceramic surface and the titanium base.
Figure 7.
Fracture lines over the medial and distal walls. The cement layer of the fractured sample remains on the ceramic surface and the titanium base.
Figure 8.
Over-contour profile of the restoration and the excess of the cement are visible from the significant accumulation of blue dye in that area.
Figure 8.
Over-contour profile of the restoration and the excess of the cement are visible from the significant accumulation of blue dye in that area.
Figure 9.
Subsequently, the dye penetration was evaluated under magnification. No microleakage was observed in any of the samples. The cement layer was equally distributed without any signs of penetration of the dye.
Figure 9.
Subsequently, the dye penetration was evaluated under magnification. No microleakage was observed in any of the samples. The cement layer was equally distributed without any signs of penetration of the dye.
Table 1.
Parameters analyzed after the loading and exposure in methylene blue dye solution. Number of registered incidents.
Table 1.
Parameters analyzed after the loading and exposure in methylene blue dye solution. Number of registered incidents.
| Test | Abutment | Abutment | Crack or Craze | Adhesive | Failures in | Failures in | Remaining |
|---|
| Groups | Screw Deformation | Deformation | Line on the Ceramic Structure | Failure between Titanium Base and Ceramic Superstructure | Titanium Base | Ceramic Superstructure | Cement around Titanium Base and Ceramic Superstructure |
|---|
| Central incisor | 0 | 0 | 0 | 0 | 0 | 0 | 8 |
| Second premolar | 0 | 0 | 1 | 1 | 0 | 1 | 8 |
| First molar | 0 | 0 | 0 | 0 | 0 | 0 | 7 |
Table 2.
Measurements of remaining thickness of the ceramic walls around the implant abutment on the scheme and on the 3D model slices. Critical areas possessing a thickness of less than 0.5 mm are considered to pose a high risk of fracture.
Table 2.
Measurements of remaining thickness of the ceramic walls around the implant abutment on the scheme and on the 3D model slices. Critical areas possessing a thickness of less than 0.5 mm are considered to pose a high risk of fracture.
| Test Groups of Maxillary Teeth | Medial | Distal | Buccal | Palatal |
|---|
| Central incisor | scheme | 1.3 mm | 1 mm | 1.3 mm | 1 mm |
| 3D model | 0.5 mm | 1.8 mm | 1.5 mm | 1.5 mm |
| Second premolar | scheme | 0.5 mm | 0.3 mm | 2.1 mm | 2.2mm |
| 3D model | 0.3 mm | 0.1 mm | 2 mm | 2.3 mm |
| First molar | scheme | 0.5 mm | 0.3 mm | 2 mm | 2.2 mm |
| 3D model | 0.5 mm | 1 mm | 3.2 mm | 2.1 mm |
Table 3.
Comparison between groups (single-factor ANOVA).
Table 3.
Comparison between groups (single-factor ANOVA).
| SUMMARY |
|---|
| Groups | Count | Sum | Average | Variance | | |
|---|
| Central incisor | 7 | 8 | 1.14 | 9.14 | | |
| Second premolar | 7 | 11 | 1.57 | 8.29 | | |
| First molar | 7 | 7 | 1 | 7 | | |
| ANOVA | | | | | | |
| Source of variance | SS | dF | MS | F | p-value | F crit |
| Between groups | 1.24 | 2 | 0.62 | 0.076 | 0.93 | 3.55 |
| Within groups | 146.4 | 18 | 8.14 | | | |
| Total | 147.81 | 20 | | | | |
Table 4.
Comparison across seven analysis techniques (single-factor ANOVA).
Table 4.
Comparison across seven analysis techniques (single-factor ANOVA).
| SUMMARY |
|---|
| Groups | Count | Sum | Average | Variance | | |
|---|
| Abutment screw deformation | 3 | 0 | 0 | 0 | | |
| Abutment deformation | 3 | 0 | 0 | 0 | | |
| Crack- or craze-line on the ceramic structure | 3 | 1 | 0.33 | 0.33 | | |
| Adhesive failure between titanium base and ceramic superstructure | 3 | 1 | 0.33 | 0.33 | | |
| Failures in titanium base | 3 | 0 | 0 | 0 | | |
| Failures in ceramic superstructure | 3 | 1 | 0.33 | 0.33 | | |
| Remaining cement around titanium base and ceramic superstructure | 3 | 23 | 7.67 | 0.33 | | |
| ANOVA | | | | | | |
| Source of variance | SS | dF | MS | F | p-value | F crit |
| Between groups | 145.14 | 6 | 24.19 | 127 | 0.00 | 2.85 |
| Within groups | 2.67 | 14 | 0.19 | | | |
| Total | 147.81 | 20 | | | | |
| Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).


 ,
, 





{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}