Assessment of p53 in Endometrial Carcinoma Biopsy and Corresponding Hysterectomy Cases in a Real-World Setting: Which Cases Need Molecular Work-Up?

 ,
,  , and
, and
Simple Summary
Abstract
1. Introduction
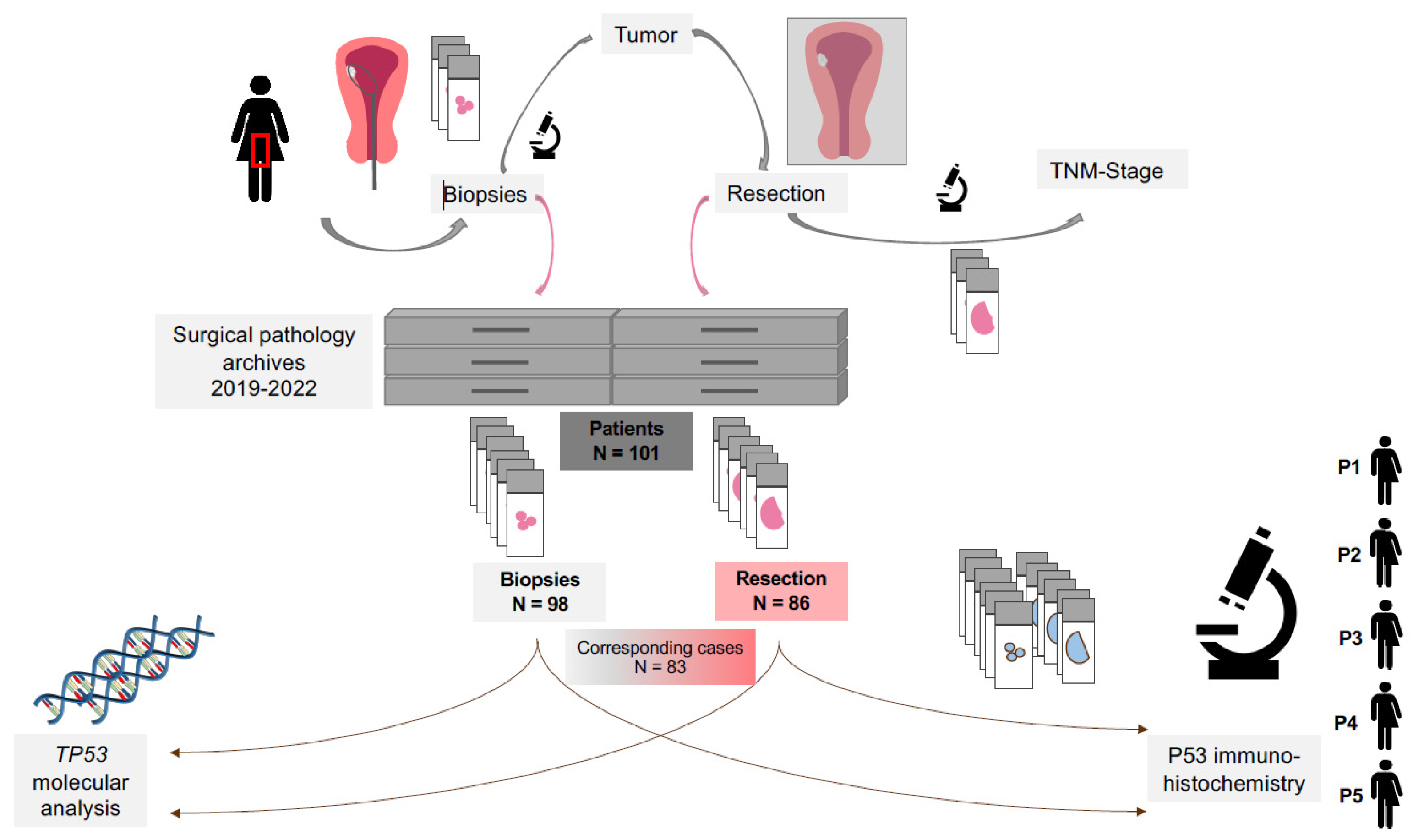
2. Materials and Methods
2.1. Patient Cohort
2.2. Immunohistochemical Assessment
2.3. Parallel Sequencing (Next-Generation Sequencing, NGS)
2.4. Data/Statistical Analysis
3. Results
3.1. Clinicopathological Features
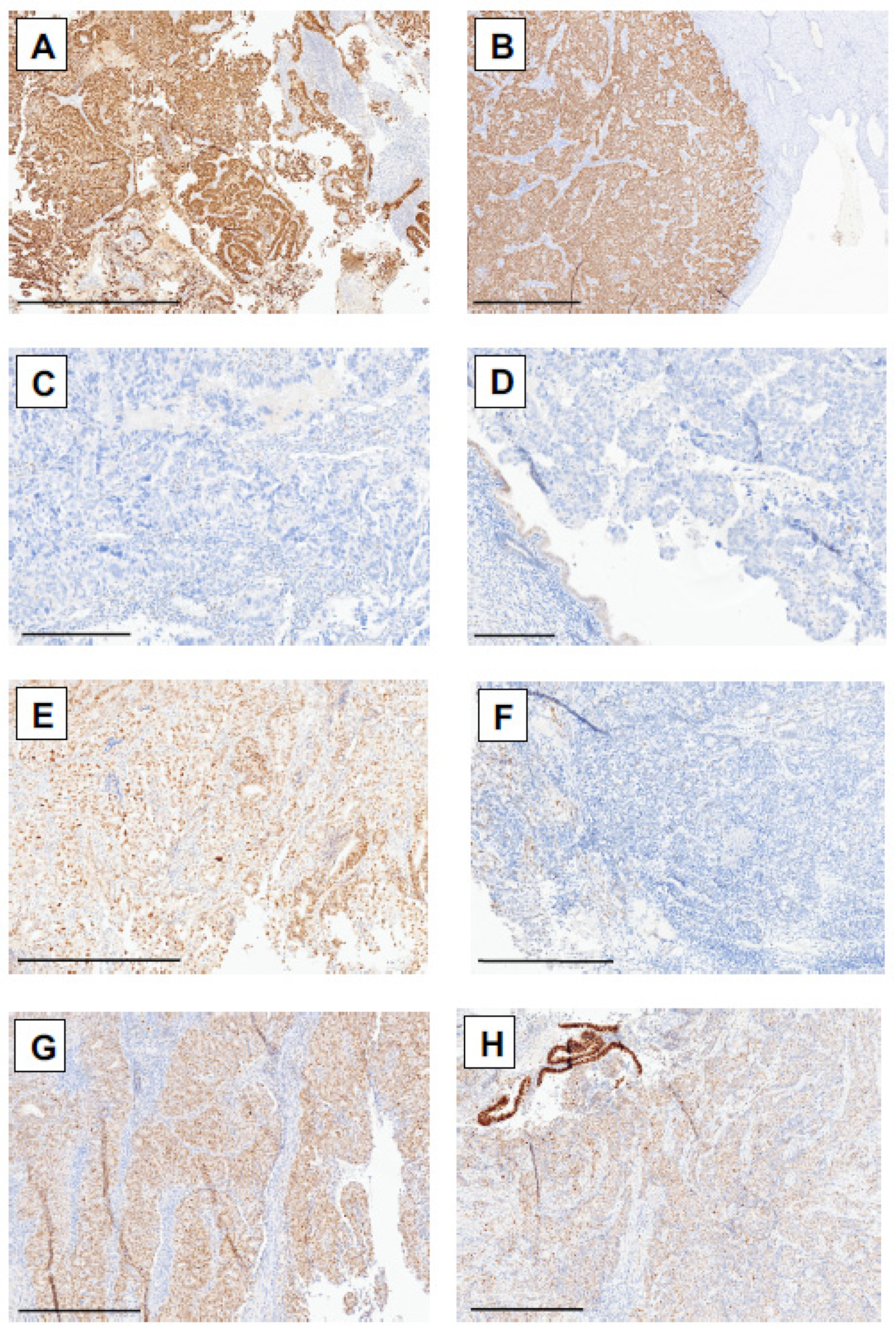
3.2. Immunohistochemical Assessment of p53 Status in Biopsy and Resection Samples in Correlation with Molecular TP53 Status in Patients with Endometrial Carcinoma
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
Abbreviations
| IHC | Immunohistochemistry |
| dMMR | Deficient mismatch repair proteins |
| MSI | Microsatellite instable |
| MSS | Microsatellite stable |
| pMMR | Proficient mismatch repair proteins |
| WHO | World Health Organization |
References
- Bray, F.; Laversanne, M.; Sung, H.; Ferlay, J.; Siegel, R.L.; Soerjomataram, I.; Jemal, A. Global Cancer Statistics 2022: GLOBOCAN Estimates of Incidence and Mortality Worldwide for 36 Cancers in 185 Countries. CA Cancer J. Clin. 2024, 74, 229–263. [Google Scholar] [CrossRef] [PubMed]
- Hosh, M.; Antar, S.; Nazzal, A.; Warda, M.; Gibreel, A.; Refky, B. Uterine Sarcoma: Analysis of 13,089 Cases Based on Surveillance, Epidemiology, and End Results Database. Int. J. Gynecol. Cancer 2016, 26, 1098–1104. [Google Scholar] [CrossRef] [PubMed]
- Matias-Guiu, X.; Lax, S.F.; Bosse, T.; Davidson, B.; Singh, N.; Euscher, E.D.; Raspollini, M.R.; Liu, C.; Lortet-Tieulent, J. Endometrioid carcinoma of the uterine corpus. In Female Genital Tumors, 5th ed.; WHO Classification of Tumors Series; International Agency for Research on Cancer: Lyon, France, 2020; Volume 4. [Google Scholar]
- Vrede, S.W.; Kasius, J.; Bulten, J.; Teerenstra, S.; Huvila, J.; Colas, E.; Gil-Moreno, A.; Boll, D.; Vos, M.C.; van Altena, A.M.; et al. Relevance of Molecular Profiling in Patients with Low-Grade Endometrial Cancer. JAMA Netw. Open 2022, 5, e2247372. [Google Scholar] [CrossRef]
- Espinosa, I.; D’Angelo, E.; Prat, J. Endometrial Carcinoma: 10 Years of TCGA (the Cancer Genome Atlas): A Critical Reappraisal with Comments on FIGO 2023 Staging. Gynecol. Oncol. 2024, 186, 94–103. [Google Scholar] [CrossRef]
- Cancer Genome Atlas Research Network; Kandoth, C.; Schultz, N.; Cherniack, A.D.; Akbani, R.; Liu, Y.; Shen, H.; Robertson, A.G.; Pashtan, I.; Shen, R.; et al. Integrated Genomic Characterization of Endometrial Carcinoma. Nature 2013, 497, 67–73. [Google Scholar] [CrossRef]
- Nero, C.; Pasciuto, T.; Cappuccio, S.; Corrado, G.; Pelligra, S.; Zannoni, G.F.; Santoro, A.; Piermattei, A.; Minucci, A.; Lorusso, D.; et al. Further Refining 2020 ESGO/ESTRO/ESP Molecular Risk Classes in Patients with Early-Stage Endometrial Cancer: A Propensity Score-Matched Analysis. Cancer 2022, 128, 2898–2907. [Google Scholar] [CrossRef]
- Leon-Castillo, A.; Horeweg, N.; Peters, E.E.M.; Rutten, T.; Ter Haar, N.; Smit, V.T.H.B.M.; Kroon, C.D.; Boennelycke, M.; Hogdall, E.; Hogdall, C.; et al. Prognostic Relevance of the Molecular Classification in High-Grade Endometrial Cancer for Patients Staged by Lymphadenectomy and without Adjuvant Treatment. Gynecol. Oncol. 2022, 164, 577–586. [Google Scholar] [CrossRef]
- Jamieson, A.; Vermij, L.; Kramer, C.J.H.; Jobsen, J.J.; Jürgemlienk-Schulz, I.; Lutgens, L.; Mens, J.W.; Haverkort, M.A.D.; Slot, A.; Nout, R.A.; et al. Clinical Behavior and Molecular Landscape of Stage I P53-Abnormal Low-Grade Endometrioid Endometrial Carcinomas. Clin. Cancer Res. 2023, 29, 4949–4957. [Google Scholar] [CrossRef]
- Bosse, T.; Nout, R.A.; McAlpine, J.N.; McConechy, M.K.; Britton, H.; Hussein, Y.R.; Gonzalez, C.; Ganesan, R.; Steele, J.C.; Harrison, B.T.; et al. Molecular Classification of Grade 3 Endometrioid Endometrial Cancers Identifies Distinct Prognostic Subgroups. Am. J. Surg. Pathol. 2018, 42, 561–568. [Google Scholar] [CrossRef]
- Casanova, J.; Babiciu, A.; Duarte, G.S.; da Costa, A.G.; Serra, S.S.; Costa, T.; Catarino, A.; Leitão, M.M.; Lima, J. Abnormal P53 High-Grade Endometrioid Endometrial Cancer: A Systematic Review and Meta-Analysis. Cancers 2025, 17, 38. [Google Scholar] [CrossRef]
- Talhouk, A.; McConechy, M.K.; Leung, S.; Li-Chang, H.H.; Kwon, J.S.; Melnyk, N.; Yang, W.; Senz, J.; Boyd, N.; Karnezis, A.N.; et al. A Clinically Applicable Molecular-Based Classification for Endometrial Cancers. Br. J. Cancer 2015, 113, 299–310. [Google Scholar] [CrossRef] [PubMed]
- Vermij, L.; Léon-Castillo, A.; Singh, N.; Powell, M.E.; Edmondson, R.J.; Genestie, C.; Khaw, P.; Pyman, J.; McLachlin, C.M.; Ghatage, P.; et al. P53 Immunohistochemistry in Endometrial Cancer: Clinical and Molecular Correlates in the PORTEC-3 Trial. Mod. Pathol. 2022, 35, 1475–1483. [Google Scholar] [CrossRef] [PubMed]
- Singh, N.; Piskorz, A.M.; Bosse, T.; Jimenez-Linan, M.; Rous, B.; Brenton, J.D.; Gilks, C.B.; Köbel, M. P53 Immunohistochemistry Is an Accurate Surrogate for TP53 Mutational Analysis in Endometrial Carcinoma Biopsies. J. Pathol. 2020, 250, 336–345. [Google Scholar] [CrossRef] [PubMed]
- Kommoss, S.; McConechy, M.K.; Kommoss, F.; Leung, S.; Bunz, A.; Magrill, J.; Britton, H.; Kommoss, F.; Grevenkamp, F.; Karnezis, A.; et al. Final Validation of the ProMisE Molecular Classifier for Endometrial Carcinoma in a Large Population-Based Case Series. Ann. Oncol. 2018, 29, 1180–1188. [Google Scholar] [CrossRef]
- Raffone, A.; Travaglino, A.; Mascolo, M.; Carotenuto, C.; Guida, M.; Mollo, A.; Insabato, L.; Zullo, F. Histopathological Characterization of ProMisE Molecular Groups of Endometrial Cancer. Gynecol. Oncol. 2020, 157, 252–259. [Google Scholar] [CrossRef]
- Talhouk, A.; McConechy, M.K.; Leung, S.; Yang, W.; Lum, A.; Senz, J.; Boyd, N.; Pike, J.; Anglesio, M.; Kwon, J.S.; et al. Confirmation of ProMisE: A Simple, Genomics-Based Clinical Classifier for Endometrial Cancer. Cancer 2017, 123, 802–813. [Google Scholar] [CrossRef]
- Sakamoto, I.; Kagami, K.; Nozaki, T.; Hirotsu, Y.; Amemiya, K.; Oyama, T.; Omata, M. P53 Immunohistochemical Staining and TP53 Gene Mutations in Endometrial Cancer: Does Null Pattern Correlate with Prognosis? Am. J. Surg. Pathol. 2023, 47, 1144–1150. [Google Scholar] [CrossRef]
- Köbel, M.; Ronnett, B.M.; Singh, N.; Soslow, R.A.; Gilks, C.B.; McCluggage, W.G. Interpretation of P53 Immunohistochemistry in Endometrial Carcinomas: Toward Increased Reproducibility. Int. J. Gynecol. Pathol. Off. J. Int. Soc. Gynecol. Pathol. 2019, 38 (Suppl. 1), S123–S131. [Google Scholar] [CrossRef]
- Rabban, J.T.; Garg, K.; Ladwig, N.R.; Zaloudek, C.J.; Devine, W.P. Cytoplasmic Pattern P53 Immunoexpression in Pelvic and Endometrial Carcinomas with TP53 Mutation Involving Nuclear Localization Domains: An Uncommon But Potential Diagnostic Pitfall with Clinical Implications. Am. J. Surg. Pathol. 2021, 45, 1441–1451. [Google Scholar] [CrossRef]
- Concin, N.; Matias-Guiu, X.; Vergote, I.; Cibula, D.; Mirza, M.R.; Marnitz, S.; Ledermann, J.; Bosse, T.; Chargari, C.; Fagotti, A.; et al. ESGO/ESTRO/ESP Guidelines for the Management of Patients with Endometrial Carcinoma. Int. J. Gynecol. Cancer 2021, 31, 12–39. [Google Scholar] [CrossRef]
- Berek, J.S.; Matias-Guiu, X.; Creutzberg, C.; Fotopoulou, C.; Gaffney, D.; Kehoe, S.; Lindemann, K.; Mutch, D.; Concin, N.; Endometrial Cancer Staging Subcommittee; et al. FIGO Staging of Endometrial Cancer: 2023. Int. J. Gynecol. Obstet. 2023, 162, 383–394. [Google Scholar] [CrossRef] [PubMed]
- Köbel, M.; Piskorz, A.M.; Lee, S.; Lui, S.; LePage, C.; Marass, F.; Rosenfeld, N.; Mes Masson, A.; Brenton, J.D. Optimized P53 Immunohistochemistry Is an Accurate Predictor of TP53 Mutation in Ovarian Carcinoma. J. Pathol. Clin. Res. 2016, 2, 247–258. [Google Scholar] [CrossRef] [PubMed]
- Heydt, C.; Fassunke, J.; Künstlinger, H.; Ihle, M.A.; König, K.; Heukamp, L.C.; Schildhaus, H.-U.; Odenthal, M.; Büttner, R.; Merkelbach-Bruse, S. Comparison of Pre-Analytical FFPE Sample Preparation Methods and Their Impact on Massively Parallel Sequencing in Routine Diagnostics. PLoS ONE 2014, 9, e104566. [Google Scholar] [CrossRef]
- Hoang, L.N.; Kinloch, M.A.; Leo, J.M.; Grondin, K.; Lee, C.-H.; Ewanowich, C.; Köbel, M.; Cheng, A.; Talhouk, A.; McConechy, M.; et al. Interobserver Agreement in Endometrial Carcinoma Histotype Diagnosis Varies Depending on The Cancer Genome Atlas (TCGA)-Based Molecular Subgroup. Am. J. Surg. Pathol. 2017, 41, 245–252. [Google Scholar] [CrossRef]
- Talhouk, A.; Hoang, L.N.; McConechy, M.K.; Nakonechny, Q.; Leo, J.; Cheng, A.; Leung, S.; Yang, W.; Lum, A.; Köbel, M.; et al. Molecular Classification of Endometrial Carcinoma on Diagnostic Specimens Is Highly Concordant with Final Hysterectomy: Earlier Prognostic Information to Guide Treatment. Gynecol. Oncol. 2016, 143, 46–53. [Google Scholar] [CrossRef]
- Stelloo, E.; Nout, R.A.; Naves, L.C.L.M.; ter Haar, N.T.; Creutzberg, C.L.; Smit, V.T.H.B.M.; Bosse, T. High Concordance of Molecular Tumor Alterations between Pre-Operative Curettage and Hysterectomy Specimens in Patients with Endometrial Carcinoma. Gynecol. Oncol. 2014, 133, 197–204. [Google Scholar] [CrossRef]
- Plotkin, A.; Kuzeljevic, B.; De Villa, V.; Thompson, E.F.; Gilks, C.B.; Clarke, B.A.; Köbel, M.; McAlpine, J.N. Interlaboratory Concordance of ProMisE Molecular Classification of Endometrial Carcinoma Based on Endometrial Biopsy Specimens. Int. J. Gynecol. Pathol. 2020, 39, 537–545. [Google Scholar] [CrossRef]
- Guo, Q.; Tang, S.; Ju, X.; Feng, Z.; Zhang, Z.; Peng, D.; Liu, F.; Du, H.; Wang, J.; Zhang, Y.; et al. Identification of Molecular Subtypes for Endometrial Carcinoma Using a 46-Gene next-Generation Sequencing Panel: A Retrospective Study on a Consecutive Cohort. ESMO Open 2024, 9, 103710. [Google Scholar] [CrossRef]
- Rios-Doria, E.; Momeni-Boroujeni, A.; Friedman, C.F.; Selenica, P.; Zhou, Q.; Wu, M.; Marra, A.; Leitao, M.M.; Iasonos, A.; Alektiar, K.M.; et al. Integration of Clinical Sequencing and Immunohistochemistry for the Molecular Classification of Endometrial Carcinoma. Gynecol. Oncol. 2023, 174, 262–272. [Google Scholar] [CrossRef]


{kind=link}
{kind=link}
{kind=link}
| Variables | Values |
|---|---|
| total number of patients | 101 |
| Biopsies Resections | 98 86 |
| Age, years Mean (±SD) Min, max | 63 (13.5 ± SD) Min. 20 years, max. 90 years |
| pT stage, resection (n = 86) (%) pT1a pT1b pT2 pT3a pT3b | 48 (55.8%) 28 (32.6%) 7 (8.1%) 2 (2.3%) 1 (1.2%) |
| pN stage, resection (n = 86) (%) pN0 pN1 NA | 25 (29.1%) 2 (2.3%) 59 (68.6%) |
| Tumor size in cm (n = 86) Mean (±SD) NA (n) | 3.1 (±2.0) 8 cases |
| Subtype biopsy (n = 98) (%) Serous Endometrioid | 4 (4.1%) 94 (95.1%) |
| Subtype resection (n = 86) (%) Serous Endometrioid Mixed serous and endometrioid | 5 (5.8%) 79 (91.9%) 2 (2.3%) |
| Grading biopsy (n = 98) (%) 1 2 3 | 29 (29.6%) 51 (52.0%) 18 (18.4%) |
| Grading resection (n = 86) (%) 1 2 3 | 28 (32.6%) 37 (43.0%) 21 (24.4%) |
| MMR/MSI-status (n = 101) (%) pMMR/MSS dMMR/MSI NA | 70 (69.3%) 29 (28.7%) 2 (2.0%) |
| Molecular results Biopsies Resections | 92 (93.9%) 77 (89.5%) |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2025 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Eich, M.-L.; Siemanowsk-Hrach, J.; Drebber, U.; Friedrichs, N.; Mallmann, P.; Domröse, C.; Ratiu, D.; Merkelbach-Bruse, S.; Büttner, R.; Quaas, A.; et al. Assessment of p53 in Endometrial Carcinoma Biopsy and Corresponding Hysterectomy Cases in a Real-World Setting: Which Cases Need Molecular Work-Up? Cancers 2025, 17, 1506. https://doi.org/10.3390/cancers17091506
Eich M-L, Siemanowsk-Hrach J, Drebber U, Friedrichs N, Mallmann P, Domröse C, Ratiu D, Merkelbach-Bruse S, Büttner R, Quaas A, et al. Assessment of p53 in Endometrial Carcinoma Biopsy and Corresponding Hysterectomy Cases in a Real-World Setting: Which Cases Need Molecular Work-Up? Cancers. 2025; 17(9):1506. https://doi.org/10.3390/cancers17091506
Chicago/Turabian StyleEich, Marie-Lisa, Janna Siemanowsk-Hrach, Uta Drebber, Nicolaus Friedrichs, Peter Mallmann, Christian Domröse, Dominik Ratiu, Sabine Merkelbach-Bruse, Reinhard Büttner, Alexander Quaas, and et al. 2025. "Assessment of p53 in Endometrial Carcinoma Biopsy and Corresponding Hysterectomy Cases in a Real-World Setting: Which Cases Need Molecular Work-Up?" Cancers 17, no. 9: 1506. https://doi.org/10.3390/cancers17091506
APA StyleEich, M.-L., Siemanowsk-Hrach, J., Drebber, U., Friedrichs, N., Mallmann, P., Domröse, C., Ratiu, D., Merkelbach-Bruse, S., Büttner, R., Quaas, A., & Schömig-Markiefka, B. (2025). Assessment of p53 in Endometrial Carcinoma Biopsy and Corresponding Hysterectomy Cases in a Real-World Setting: Which Cases Need Molecular Work-Up? Cancers, 17(9), 1506. https://doi.org/10.3390/cancers17091506