
Atrial Fibrillation Risk in Relation to the Clinical Staging of Gastric Cancer: A Nationwide Population-Based Cohort Study
 ,
,
Simple Summary
Abstract

1. Introduction
2. Materials and Methods
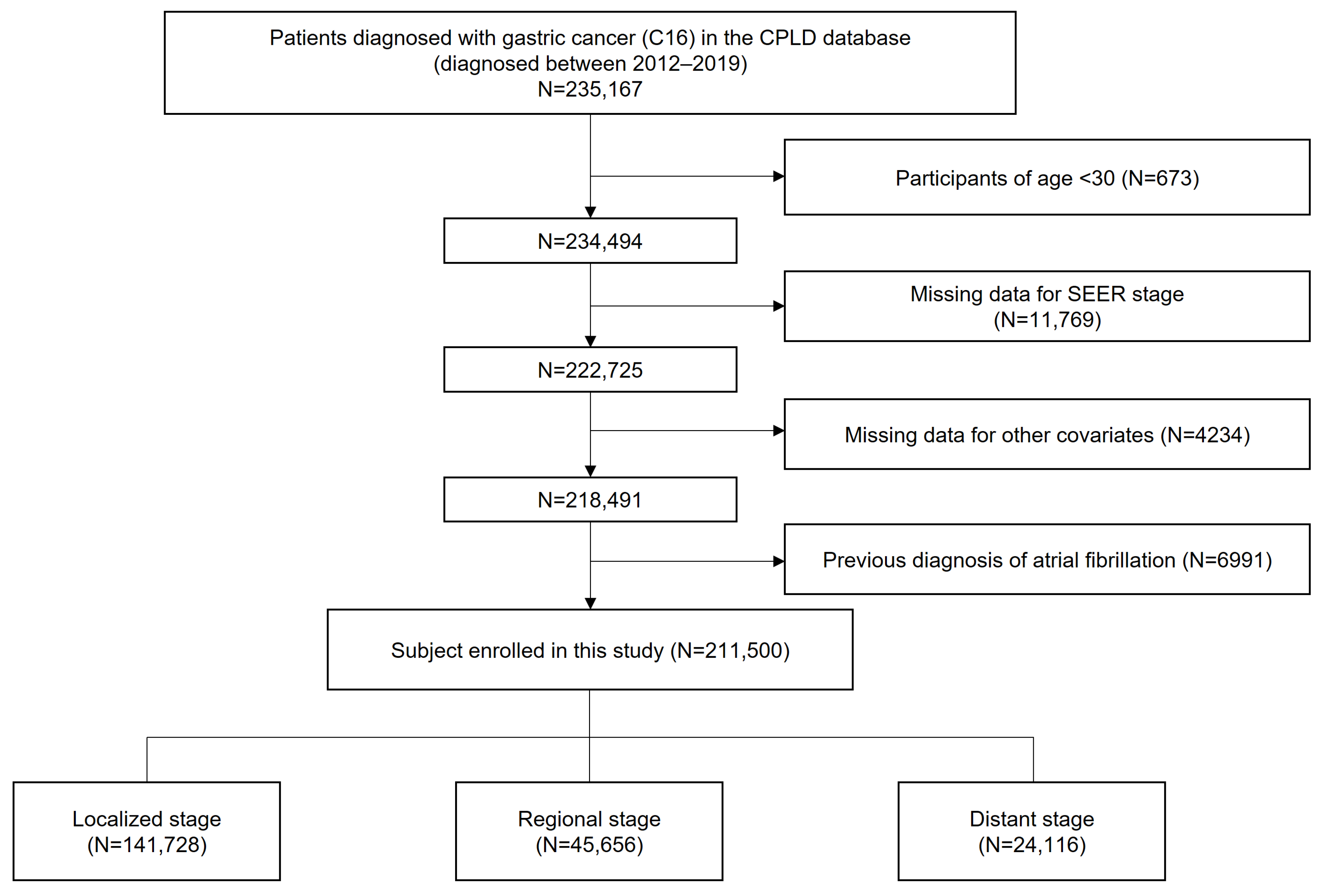
2.1. Data Source and Study Population
2.2. Definitions
2.3. Statistical Analysis
3. Results
3.1. Baseline Characteristics
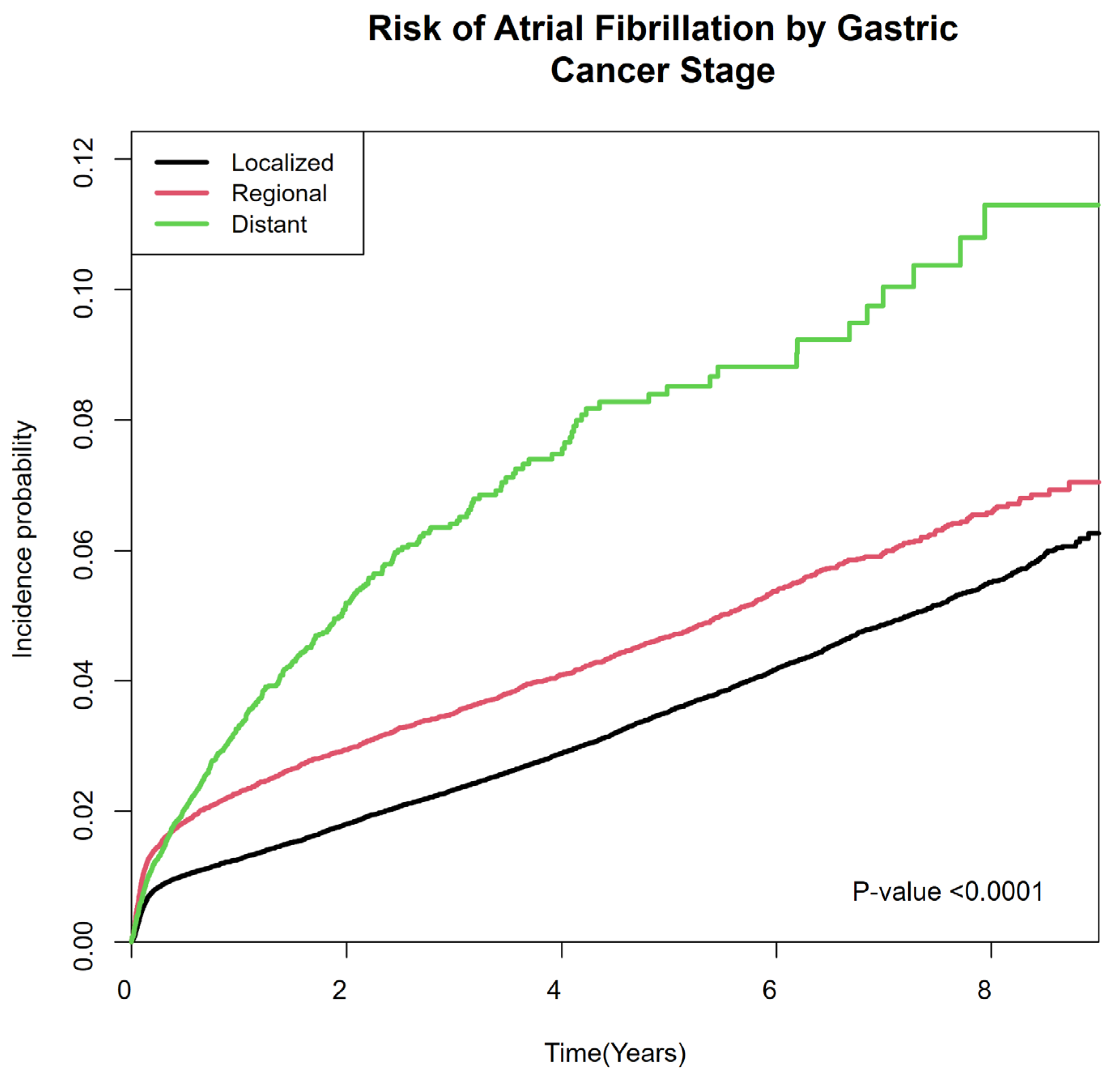
3.2. Risk of Atrial Fibrillation According to the SEER Stage at Diagnosis of Gastric Cancer
3.3. Subgroup Analysis
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Bray, F.; Laversanne, M.; Sung, H.; Ferlay, J.; Siegel, R.L.; Soerjomataram, I.; Jemal, A. Global cancer statistics 2022: GLOBOCAN estimates of incidence and mortality worldwide for 36 cancers in 185 countries. CA Cancer J. Clin. 2024, 74, 229–263. [Google Scholar] [CrossRef]
- Park, E.H.; Jung, K.-W.; Park, N.J.; Kang, M.J.; Yun, E.H.; Kim, H.-J.; Kim, J.-E.; Kong, H.-J.; Im, J.-S.; Seo, H.G. Cancer statistics in Korea: Incidence, mortality, survival, and prevalence in 2021. Cancer Res. Treat. Off. J. Korean Cancer Assoc. 2024, 56, 357–371. [Google Scholar] [CrossRef] [PubMed]
- Choi, H.L.; Kang, D.; Kim, H.; Cho, J.; Jeon, K.H.; Jung, W.; Shin, D.W.; Jeong, S.-M. Increased cardiovascular disease risk among adolescents and young adults with gastric cancer. Gastric Cancer 2024, 27, 1169–1179. [Google Scholar] [CrossRef] [PubMed]
- Wong, M.C.S.; Huang, J.; Chan, P.S.F.; Choi, P.; Lao, X.Q.; Chan, S.M.; Teoh, A.; Liang, P. Global Incidence and Mortality of Gastric Cancer, 1980-2018. JAMA Netw. Open 2021, 4, e2118457. [Google Scholar] [CrossRef] [PubMed]
- Wang, J.; Wang, Q.; Du, X.; Zhu, X.; Nie, C.; Han, X.; Tian, W.; Li, H.; Zhou, H. Risk factors associated with cardiovascular mortality among gastric cancer patients: A population-based analysis. Jpn. J. Clin. Oncol. 2022, 52, 1365–1374. [Google Scholar] [CrossRef]
- Yun, J.P.; Choi, E.-K.; Han, K.-D.; Park, S.H.; Jung, J.-H.; Park, S.H.; Ahn, H.-J.; Lim, J.-H.; Lee, S.-R.; Oh, S. Risk of atrial fibrillation according to cancer type: A nationwide population-based study. Cardio Oncol. 2021, 3, 221–232. [Google Scholar] [CrossRef]
- Jakobsen, C.B.; Lamberts, M.; Carlson, N.; Lock-Hansen, M.; Torp-Pedersen, C.; Gislason, G.H.; Schou, M. Incidence of atrial fibrillation in different major cancer subtypes: A Nationwide population-based 12 year follow up study. BMC Cancer 2019, 19, 1105. [Google Scholar] [CrossRef]
- O’Neal, W.T.; Lakoski, S.G.; Qureshi, W.; Judd, S.E.; Howard, G.; Howard, V.J.; Cushman, M.; Soliman, E.Z. Relation Between Cancer and Atrial Fibrillation (from the REasons for Geographic And Racial Differences in Stroke Study). Am. J. Cardiol. 2015, 115, 1090–1094. [Google Scholar] [CrossRef]
- Zhang, M.; Li, L.-l.; Zhao, Q.-Q.; Peng, X.-d.; Wu, K.; Li, X.; Ruan, Y.-F.; Bai, R.; Liu, N.; Ma, C.S. The Association of New-Onset Atrial Fibrillation and Risk of Cancer: A Systematic Review and Meta-Analysis. Cardiol. Res. Pract. 2020, 2020, 2372067. [Google Scholar] [CrossRef]
- Farmakis, D.; Parissis, J.; Filippatos, G. Insights Into Onco-Cardiology. JACC 2014, 63, 945–953. [Google Scholar] [CrossRef]
- Rahman, F.; Ko, D.; Benjamin, E.J. Association of Atrial Fibrillation and Cancer. JAMA Cardiol. 2016, 1, 384–386. [Google Scholar] [CrossRef]
- Choi, D.W.; Guk, M.Y.; Kim, H.R.; Ryu, K.S.; Kong, H.J.; Cha, H.S.; Kim, H.J.; Chae, H.; Jeon, Y.S.; Kim, H.; et al. Data Resource Profile: The Cancer Public Library Database in South Korea. Cancer Res. Treat. 2024, 56, 1014–1026. [Google Scholar] [CrossRef] [PubMed]
- Mauro, E.; Lucà, F.; Tetta, C.; Parise, O.; Parrini, I.; Parise, G.; Rao, C.M.; Matteucci, F.; Micali, L.R.; Gulizia, M.M.; et al. Breast Cancer and Atrial Fibrillation. J. Clin. Med. 2022, 11, 1417. [Google Scholar] [CrossRef]
- Guha, A.; Fradley, M.G.; Dent, S.F.; Weintraub, N.L.; Lustberg, M.B.; Alonso, A.; Addison, D. Incidence, risk factors, and mortality of atrial fibrillation in breast cancer: A SEER-Medicare analysis. Eur. Heart J. 2021, 43, 300–312. [Google Scholar] [CrossRef] [PubMed]
- Kim, H.W.; Kim, J.-H.; Lim, B.J.; Kim, H.; Kim, H.; Park, J.J.; Youn, Y.H.; Park, H.; Noh, S.H.; Kim, J.W. Sex disparity in gastric cancer: Female sex is a poor prognostic factor for advanced gastric cancer. Ann. Surg. Oncol. 2016, 23, 4344–4351. [Google Scholar] [CrossRef] [PubMed]
- Luan, X.; Niu, P.; Wang, W.; Zhao, L.; Zhang, X.; Zhao, D.; Chen, Y. Sex Disparity in Patients with Gastric Cancer: A Systematic Review and Meta-Analysis. J. Oncol. 2022, 2022, 1269435. [Google Scholar] [CrossRef]
- Buza, V.; Rajagopalan, B.; Curtis, A.B. Cancer Treatment–Induced Arrhythmias. Circ. Arrhythmia Electrophysiol. 2017, 10, e005443. [Google Scholar] [CrossRef]
- Polk, A.; Vaage-Nilsen, M.; Vistisen, K.; Nielsen, D.L. Cardiotoxicity in cancer patients treated with 5-fluorouracil or capecitabine: A systematic review of incidence, manifestations and predisposing factors. Cancer Treat. Rev. 2013, 39, 974–984. [Google Scholar] [CrossRef]
- Sara, J.D.; Kaur, J.; Khodadadi, R.; Rehman, M.; Lobo, R.; Chakrabarti, S.; Herrmann, J.; Lerman, A.; Grothey, A. 5-fluorouracil and cardiotoxicity: A review. Ther. Adv. Med. Oncol. 2018, 10, 1758835918780140. [Google Scholar] [CrossRef]
- Jin, X.; Bai, Y.; Gao, L.; Wu, S. Incidence of and risk factors for cardiotoxicity after fluorouracil-based chemotherapy in locally advanced or metastatic gastric cancer patients. Cancer Chemother. Pharmacol. 2019, 84, 599–607. [Google Scholar] [CrossRef]
- Bao, Y.; Lee, J.; Thakur, U.; Ramkumar, S.; Marwick, T.H. Atrial fibrillation in cancer survivors—A systematic review and meta-analysis. Cardio-Oncol. 2023, 9, 29. [Google Scholar] [CrossRef] [PubMed]
- Van Gelder, I.C.; Rienstra, M.; Bunting, K.V.; Casado-Arroyo, R.; Caso, V.; Crijns, H.J.G.M.; De Potter, T.J.R.; Dwight, J.; Guasti, L.; Hanke, T.; et al. 2024 ESC Guidelines for the management of atrial fibrillation developed in collaboration with the European Association for Cardio-Thoracic Surgery (EACTS): Developed by the task force for the management of atrial fibrillation of the European Society of Cardiology (ESC), with the special contribution of the European Heart Rhythm Association (EHRA) of the ESC. Endorsed by the European Stroke Organisation (ESO). Eur. Heart J. 2024, 45, 3314–3414. [Google Scholar] [CrossRef] [PubMed]
- Joglar José, A.; Chung Mina, K.; Armbruster Anastasia, L.; Benjamin Emelia, J.; Chyou Janice, Y.; Cronin Edmond, M.; Deswal, A.; Eckhardt Lee, L.; Goldberger Zachary, D.; Gopinathannair, R.; et al. 2023 ACC/AHA/ACCP/HRS Guideline for the Diagnosis and Management of Atrial Fibrillation. JACC 2024, 83, 109–279. [Google Scholar] [CrossRef] [PubMed]
- Alonso, A.; Krijthe, B.P.; Aspelund, T.; Stepas, K.A.; Pencina, M.J.; Moser, C.B.; Sinner, M.F.; Sotoodehnia, N.; Fontes, J.D.; Janssens, A.C.; et al. Simple risk model predicts incidence of atrial fibrillation in a racially and geographically diverse population: The CHARGE-AF consortium. J. Am. Heart Assoc. 2013, 2, e000102. [Google Scholar] [CrossRef]
- Hu, W.S.; Lin, C.L. Prediction of new-onset atrial fibrillation for general population in Asia: A comparison of C2HEST and HATCH scores. Int. J. Cardiol. 2020, 313, 60–63. [Google Scholar] [CrossRef]
- Himmelreich, J.C.; Veelers, L.; Lucassen, W.A.; Schnabel, R.B.; Rienstra, M.; van Weert, H.C.; Harskamp, R.E. Prediction models for atrial fibrillation applicable in the community: A systematic review and meta-analysis. EP Eur. 2020, 22, 684–694. [Google Scholar] [CrossRef]
- Hu, P.; Bai, J.a.; Liu, M.; Xue, J.; Chen, T.; Li, R.; Kuai, X.; Zhao, H.; Li, X.; Tian, Y.; et al. Trends of incidence and prognosis of gastric neuroendocrine neoplasms: A study based on SEER and our multicenter research. Gastric Cancer 2020, 23, 591–599. [Google Scholar] [CrossRef]
- Dong, E.; Duan, L.; Wu, B.U. Racial and Ethnic Minorities at Increased Risk for Gastric Cancer in a Regional US Population Study. Clin. Gastroenterol. Hepatol. 2017, 15, 511–517. [Google Scholar] [CrossRef]
- Gill, S.; Shah, A.; Le, N.; Cook, E.F.; Yoshida, E.M. Asian ethnicity–related differences in gastric cancer presentation and outcome among patients treated at a Canadian Cancer Center. J. Clin. Oncol. 2003, 21, 2070–2076. [Google Scholar] [CrossRef]
- Lui, F.H.; Tuan, B.; Swenson, S.L.; Wong, R.J. Ethnic Disparities in Gastric Cancer Incidence and Survival in the USA: An Updated Analysis of 1992–2009 SEER Data. Dig. Dis. Sci. 2014, 59, 3027–3034. [Google Scholar] [CrossRef]

{kind=link}
{kind=link}
{kind=link}
| No. (%) | |||||
|---|---|---|---|---|---|
| Total Population (N = 211,500) | SEER Summary Stage | p-Value | |||
| Localized (N = 141,728) | Regional (N = 45,656) | Distant (N = 24,116) | |||
| Age at diagnosis (years) | <0.0001 | ||||
| 30–39 | 5682 (2.69) | 3171 (2.24) | 1437 (3.15) | 1074 (4.45) | |
| 40–64 | 103,642 (49) | 71,489 (50.44) | 20,968 (45.93) | 11,185 (46.38) | |
| ≥65 | 102,176 (48.31) | 67,068 (47.32) | 23,251 (50.93) | 11,857 (49.17) | |
| Sex | 0.0002 | ||||
| Male | 143,244 (67.73) | 96,397 (68.02) | 30,606 (67.04) | 16,241 (67.35) | |
| Female | 68,256 (32.27) | 45,331 (31.98) | 15,050 (32.96) | 7875 (32.65) | |
| Initial treatment | |||||
| Surgery | 174,298 (82.41) | 129,859 (91.63) | 38,753 (84.88) | 5686 (23.58) | <0.0001 |
| Chemotherapy | 42,532 (20.11) | 6972 (4.92) | 20,401 (44.68) | 15,159 (62.86) | <0.0001 |
| Radiotherapy | 1628 (0.77) | 180 (0.13) | 606 (1.33) | 842 (3.49) | <0.0001 |
| Immunotherapy or hormone therapy | 214 (0.1) | 69 (0.05) | 43 (0.09) | 102 (0.42) | <0.0001 |
| Year of diagnosis (year) | |||||
| 2012–2013 | 53,749 (25.41) | 34,888 (24.62) | 12,598 (27.59) | 6263 (25.97) | |
| 2014–2015 | 52,526 (24.83) | 34,878 (24.61) | 11,576 (25.35) | 6072 (25.18) | |
| 2016–2017 | 53,845 (25.46) | 36,683 (25.88) | 11,115 (24.35) | 6047 (25.07) | |
| 2018–2019 | 51,380 (24.29) | 35,279 (24.89) | 10,367 (22.71) | 5734 (23.78) | |
| Comorbidities | |||||
| Diabetes mellitus | 43,637 (20.63) | 28,880 (20.38) | 9707 (21.26) | 5050 (20.94) | <0.0001 |
| Hypertension | 94,894 (44.87) | 63,970 (45.14) | 20,540 (44.99) | 10,384 (43.06) | <0.0001 |
| Dyslipidemia | 57,169 (27.03) | 41,558 (29.32) | 10,787 (23.63) | 4824 (20) | <0.0001 |
| Income level | <0.0001 | ||||
| Medical aid + 1st and 2nd decile | 41,181 (19.47) | 26,206 (18.49) | 9671 (21.18) | 5304 (21.99) | |
| 3rd to 8th decile | 105,975 (50.11) | 70,187 (49.52) | 23,400 (51.25) | 12,388 (51.37) | |
| 9th and 10th decile | 64,344 (30.42) | 45,335 (31.99) | 12,585 (27.56) | 6424 (26.64) | |
| Residential area, urban | 91,103 (43.07) | 61,443 (43.35) | 19,330 (42.34) | 10,330 (42.83) | 0.0005 |
| Follow-up duration (years) | 3.89 ± 2.58 | 4.49 ± 2.41 | 3.47 ± 2.55 | 1.12 ± 1.37 | <0.0001 |
| SEER Stage | N | Event | IR a | HR (95% CI) | ||||
|---|---|---|---|---|---|---|---|---|
| Model 1 | Model 2 | Model 3 | Model 4 | Model 5 | ||||
| Localized | 141,728 | 4765 | 7.49 | 1 (Ref.) | 1 (Ref.) | 1 (Ref.) | 1 (Ref.) | 1 (Ref.) |
| Regional | 45,656 | 1754 | 11.06 | 1.39 (1.32–1.47) | 1.38 (1.30–1.45) | 1.38 (1.30–1.45) | 1.39 (1.32–1.47) | 1.32 (1.25–1.41) |
| Distant | 24,116 | 747 | 27.73 | 2.29 (2.11–2.48) | 2.33 (2.15–2.52) | 2.33 (2.15–2.52) | 2.39 (2.20–2.59) | 2.00 (1.81–2.22) |
| p-value | ||||||||
| SEER Stage | N | Event | IR a | Adjusted HR b (95% CI) | p for Interaction | ||
|---|---|---|---|---|---|---|---|
| Age | 30–64 | Localized | 74,660 | 1281 | 3.59 | 1 (Ref.) | <0.0001 |
| Regional | 22,405 | 484 | 5.35 | 1.46 (1.30–1.63) | |||
| Distant | 12,259 | 302 | 18.29 | 3.20 (2.77–3.70) | |||
| ≥65 | Localized | 67,068 | 3484 | 12.48 | 1 (Ref.) | ||
| Regional | 23,251 | 1270 | 18.63 | 1.30 (1.21–1.39) | |||
| Distant | 11,857 | 445 | 42.71 | 1.63 (1.45–1.83) | |||
| Sex | Male | Localized | 96,397 | 3540 | 8.21 | 1 (Ref.) | 0.0016 |
| Regional | 30,606 | 1244 | 11.76 | 1.28 (1.10–1.38) | |||
| Distant | 16,241 | 513 | 28.14 | 1.84 (1.64–2.06) | |||
| Female | Localized | 45,331 | 1225 | 5.96 | 1 (Ref.) | ||
| Regional | 15,050 | 510 | 9.65 | 1.43 (1.28–1.59) | |||
| Distant | 7875 | 234 | 26.88 | 2.47 (2.12–2.87) | |||
| Year of diagnosis | 2012–2013 | Localized | 34,888 | 1757 | 7.17 | 1 (Ref.) | <0.0001 |
| Regional | 12,598 | 617 | 9.79 | 1.27 (1.15–1.39) | |||
| Distant | 6263 | 185 | 22.47 | 1.78 (1.51–2.10) | |||
| 2014–2015 | Localized | 34,878 | 1388 | 7.37 | 1 (Ref.) | ||
| Regional | 11,576 | 453 | 9.84 | 1.21 (1.08–1.35) | |||
| Distant | 6072 | 163 | 23.16 | 1.68 (1.41–2.00) | |||
| 2016–2017 | Localized | 36,683 | 1010 | 7.41 | 1 (Ref.) | ||
| Regional | 11,115 | 369 | 11.33 | 1.34 (1.18–1.51) | |||
| Distant | 6047 | 187 | 27.89 | 2.10 (1.77–2.49) | |||
| 2018–2019 | Localized | 35,279 | 610 | 9.14 | 1 (Ref.) | ||
| Regional | 10,367 | 315 | 18.52 | 1.72 (1.50–1.98) | |||
| Distant | 5734 | 212 | 42.76 | 2.79 (2.36–3.31) | |||
| History of diabetes mellitus | No | Localized | 112,848 | 3512 | 6.80 | 1 (Ref.) | 0.4644 |
| Regional | 35,949 | 1261 | 9.79 | 1.30 (1.22–1.40) | |||
| Distant | 19,066 | 552 | 25.20 | 2.04 (1.82–2.28) | |||
| Yes | Localized | 28,880 | 1253 | 10.43 | 1 (Ref.) | ||
| Regional | 9707 | 493 | 16.52 | 1.38 (1.24–1.53) | |||
| Distant | 5050 | 195 | 38.77 | 1.92 (1.63–2.26) | |||
| History of hypertension | No | Localized | 77,758 | 1592 | 4.40 | 1 (Ref.) | 0.0021 |
| Regional | 25,116 | 633 | 6.77 | 1.40 (1.27–1.54) | |||
| Distant | 13,732 | 313 | 18.99 | 2.38 (2.08–2.74) | |||
| Yes | Localized | 63,970 | 3173 | 11.57 | 1 (Ref.) | ||
| Regional | 20,540 | 1121 | 17.21 | 1.29 (1.2–1.39) | |||
| Distant | 10,384 | 434 | 41.52 | 1.81 (1.61–2.04) | |||
| History of dysplipidemia | No | Localized | 100,170 | 3022 | 6.50 | 1 (Ref.) | 0.3318 |
| Regional | 34,869 | 1196 | 9.59 | 1.31 (1.22–1.41) | |||
| Distant | 19,292 | 548 | 25.21 | 2.07 (1.85–2.31) | |||
| Yes | Localized | 41,558 | 1743 | 10.16 | 1 (Ref.) | ||
| Regional | 10,787 | 558 | 16.49 | 1.35 (1.23–1.49) | |||
| Distant | 4824 | 199 | 38.32 | 1.85 (1.57–2.17) |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2025 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Oh, M.J.; Choi, Y.J.; Jung, J.-H.; Lee, S.; Han, K.; Cho, S.-J. Atrial Fibrillation Risk in Relation to the Clinical Staging of Gastric Cancer: A Nationwide Population-Based Cohort Study. Cancers 2025, 17, 2054. https://doi.org/10.3390/cancers17122054
Oh MJ, Choi YJ, Jung J-H, Lee S, Han K, Cho S-J. Atrial Fibrillation Risk in Relation to the Clinical Staging of Gastric Cancer: A Nationwide Population-Based Cohort Study. Cancers. 2025; 17(12):2054. https://doi.org/10.3390/cancers17122054
Chicago/Turabian StyleOh, Mi Jin, Yoon Jin Choi, Jin-Hyung Jung, Seunghan Lee, Kyungdo Han, and Soo-Jeong Cho. 2025. "Atrial Fibrillation Risk in Relation to the Clinical Staging of Gastric Cancer: A Nationwide Population-Based Cohort Study" Cancers 17, no. 12: 2054. https://doi.org/10.3390/cancers17122054
APA StyleOh, M. J., Choi, Y. J., Jung, J.-H., Lee, S., Han, K., & Cho, S.-J. (2025). Atrial Fibrillation Risk in Relation to the Clinical Staging of Gastric Cancer: A Nationwide Population-Based Cohort Study. Cancers, 17(12), 2054. https://doi.org/10.3390/cancers17122054