Simple Summary
Our study aimed to investigate the suggested association between body mass index and aggressive histopathological subtypes of thyroid cancer. Thus, we studied 3868 patients who underwent thyroidectomy from 2020 to 2022 at four European centres. We found that overweight and obese patients with papillary thyroid carcinoma had higher rates of aggressive histopathological subtypes, bilateral, multifocal tumours, and larger nodal metastases. These findings suggest that people with higher body mass index may be at an increased risk of developing more aggressive features of thyroid cancer.
Abstract
Obesity’s role in thyroid cancer development is still debated, as well as its association with aggressive histopathological subtypes (AHSs). To clarify the link between Body Mass Index (BMI) and AHS of differentiated thyroid carcinoma (DTC), we evaluated patients who underwent thyroidectomy for DTC from 2020 to 2022 at four European referral centres for endocrine surgery. Based on BMI, patients were classified as normal-underweight, overweight, or obese. AHSs were defined according to 2022 WHO guidelines. Among 3868 patients included, 34.5% were overweight and 19.6% obese. Histological diagnoses were: 93.6% papillary (PTC), 4.8% follicular (FTC), and 1.6% Hürthle cell (HCC) thyroid carcinoma. Obese and overweight patients with PTC had a higher rate of AHSs (p = 0.03), bilateral, multifocal tumours (p = 0.014, 0.049), and larger nodal metastases (p = 0.017). In a multivariate analysis, BMI was an independent predictor of AHS of PTC, irrespective of gender (p = 0.028). In younger patients (<55 years old) with PTC > 1 cm, BMI predicted a higher ATA risk class (p = 0.036). Overweight and obese patients with FTC had larger tumours (p = 0.036). No difference was found in terms of AHS of FTC and HCC based on BMI category. Overweight and obese patients with PTC appear to be at an increased risk for AHS and aggressive clinico-pathological characteristics.
1. Introduction
Thyroid cancer (TC) is an increasingly prevalent disease, particularly in high-income countries, and is projected to become the fourth most common cancer in the United States by 2030 [1,2]. Environmental and socio-demographic factors, including higher body mass index (BMI) and obesity, have been hypothesised to be linked to this surge in TC incidence [3,4,5,6]. Indeed, obesity, a global epidemic affecting 59% of Europeans, has been causally associated with 13 types of cancers, contributing to approximately 200,000 new cases annually [7,8,9,10]. The biological plausibility of obesity’s role in thyroid carcinogenesis has been speculated to involve low-grade chronic inflammation, altered cytokine levels, and increased oxidative stress found in this condition. Insulin resistance and hormonal changes, part of the pathological landscape of obesity, may also play a pivotal role [11,12,13]. However, obesity’s impact on aggressive clinico-pathological characteristics of differentiated thyroid cancer (DTC) remains unclear. Indeed, while some studies have suggested an association between higher BMI and aggressive tumour features of DTC, others have failed to demonstrate such a correlation [14,15,16,17,18]. Conversely, studies exploring the possible link between BMI and aggressive histopathological subtypes of DTC are currently lacking. Identifying TCs with aggressive histology or clinico-pathological characteristics that increase the risk of progression or relapse is crucial for directing therapeutic efforts more effectively and ensuring proper resource management.
This study aimed to assess BMI as a potential risk factor for aggressive DTC subtypes or clinico-pathological characteristics.
2. Materials and Methods
2.1. Study Design and Patient Selection
We conducted a multicentre retrospective cohort study including patients with a histopathologically confirmed diagnosis of DTC who underwent surgery between January 2020 and December 2022 at 4 european tertiary referral centres for endocrine surgery: Endocrine Surgery Unit—Verona University Hospital (Verona, Italy), Endocrine Surgery Unit—Pisa University Hospital (Pisa, Italy), General Surgery Unit—Cagliari University Hospital (Cagliari, Italy), and 1st Propaedeutic Department of Surgery—AHEPA University Hospital (Thessaloniki, Greece).
The patients included in the present study underwent either hemithyroidectomy, total thyroidectomy, or completion thyroidectomy with or without lymphadenectomy. Patients younger than 18, with incomplete data or with a histopathological diagnosis of anaplastic or poorly differentiated TC, medullary TC, thyroid lymphoma or metastasis were excluded from the study. Patients who underwent lobectomy and subsequent completion thyroidectomy were considered as a single case for the purposes of this analysis.
A written informed consent to anonymised data collection was signed by each patient included in the study.
The present study is in accordance with the ethical standards of the 1964 Helsinki Declaration and its later amendments or comparable ethical standards.
2.2. Data Collection
Patients’ clinical data were collected from computerised medical charts and entered into an anonymized database. Data collected included: patient’s age at surgery, gender, BMI, preoperative diagnosis, presence of hyperthyroidism or thyroiditis, type of surgery, number of excised and pathological lymph nodes, histopathological diagnosis, neoplasm diameter, histological variant, multifocality and bilaterality, surgical margin status, vascular infiltration, extrathyroid extension, and American Thyroid Association (ATA) risk score for disease recurrence [19].
Based on BMI, patients were classified as normal-underweight (<25 kg/m2), overweight (25–29.9 kg/m2), or obese (>29.9 kg/m2) according to WHO guidelines [20].
Histopathological subtypes and features of DTC were classified as aggressive (aggressive histopathological subtype, AHS) based on the latest WHO guidelines for TC classification [21], i.e., according to the following criteria: tall cell PTC (proportion of subtype features ≥30% of total); hobnail PTC (proportion of subtype features ≥30% of total); solid PTC (proportion of subtype features ≥50% of total); columnar cell PTC; diffuse sclerosing PTC; extensively invasive FTC; or angioinvasive FTC with >4 invasion foci.
2.3. Statistical Analysis
Continuous variables were expressed as median values and interquartile ranges [IQR], while categorical variables were presented as frequencies and percentages.
Collected sociodemographic and histopathological characteristics were compared between BMI categories using Mann–Whitney, Kruskal–Wallis, and Chi Square tests as appropriate.
Differences in histopathological features between different BMI categories were tested separately for patients with papillary thyroid cancer (PTC), follicular thyroid cancer (FTC), and oncocytic thyroid cancer (HCC).
A multivariate binary logistic regression analysis was performed to test whether BMI represented an independent predictor of AHS using preoperative data as confounders.
For all tests, a p-value < 0.05 was considered statistically significant. Statistical analysis was performed using SPSS (Statistical Package for the Social Sciences, IBM SPSS Statistics for Windows, Version 25.0. IBM Corp.: Armonk, NY, USA).
3. Results
Out of 3925 patients meeting the inclusion criteria, 57 were excluded from the analysis due to missing data. Consequently, the final analysis included 3868 patients.
Sociodemographic and clinicopathological characteristics of the study population are summarised in Table 1 and Table 2 and Figure 1.

Table 1.
Sociodemographic and surgical characteristics of the whole population.
Table 2.
Pathological characteristics of the whole population.
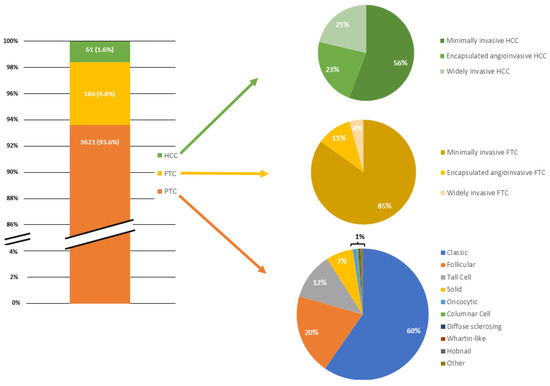
Figure 1.
Bar chart and pie charts depicting the relative proportion of differentiated thyroid cancers included in the study and each histopathologic subtype within each neoplasm.
Among the 3868 patients included, 2765 (71.5%) were female. The median BMI was 25 kg/m2 (IQR 22–28) with 1333 patients (34.5%) classified as overweight and 757 (19.6%) as obese. Histological diagnoses revealed 93.6% PTC, 4.8% FTC, and 1.6% HCC. Nearly 47% of patients underwent surgery with a preoperative diagnosis of malignancy. Total thyroidectomy was performed in 84.5% of cases while 12.7% underwent lobectomy. Central compartment lymphadenectomy and lateral compartment dissection were performed in 20% and 8.2% of patients, respectively.
Differences between histopathological features among BMI categories are summarised in Table 3, Table 4 and Table 5 for PTC, FTC, and HCC, respectively.
Table 3.
Differences in sociodemographic and pathological characteristics of PTC patients between BMI categories.
Table 4.
Differences in sociodemographic and pathological characteristics of FTC patients between BMI categories.
Table 5.
Differences in sociodemographic and pathological characteristics of HCC patients between BMI categories.
Obese and overweight patients with PTC were older (52 and 53 vs. 46 years old; p < 0.0005) and more frequently male (37.3% and 31.6% vs. 20.1%; p < 0.0005) than normal/underweight patients. Obese patients had a higher rate of AHS (22.3% vs. 18.6%; p = 0.03), bilateral (30.9% vs. 25.6%; p = 0.014), multifocal tumours (32.4% vs. 28.2%, p = 0.049), and larger nodal metastases (8 mm vs. 6 mm; p = 0.017) than normal/underweight patients. In the multivariate analysis, BMI was found to be an independent predictor of AHS of PTC, irrespective of gender (B = 0.018, p = 0.028) (Table 6). In younger patients (<55 years old) with PTC > 1 cm, a higher BMI predicted a higher ATA risk class (B = 0.02, p = 0.036). Overweight and obese patients with FTC had larger tumours (p = 0.036). No difference was found in terms of aggressive histopathological features of FTC and HCC based on BMI categories.
Table 6.
Univariate and multivariate logistic regression to identify predictors of AHS.
4. Discussion
Recent evidence has suggested that obesity may increase the risk of various cancers, including TC. However, the specific role of individual obesity-related factors in carcinogenesis remains uncertain [12,22,23]. The association between BMI and TC is believed to be linked to shared hormonal and metabolic factors related to central adiposity, as well as potential interactions with genetic variants of the fat mass and obesity-associated (FTO) gene. Certain FTO gene variants, particularly in combination with higher BMI, have been associated with an elevated risk of TC [24]. Moreover, obesity itself may contribute to chronic low-grade inflammation and altered insulin signalling, promoting tumorigenesis [8]. However, the current understanding lacks data on the correlation between BMI and aggressive histopathological subtypes of thyroid cancer.
Our study identified significant associations between BMI and the AHS of PTC. Overweight and obese patients exhibited a higher proportion of AHSs of PTC compared to their normal/underweight counterparts. This association was consistent across genders.
In other cancer types, BMI has been identified as a risk factor for the emergence of more aggressive subtypes. For instance, in premenopausal women, obesity is associated with an elevated risk of the triple-negative breast cancer subtype and non-luminal subtypes [25,26]. Similarly, a high BMI is linked to an increased risk of borderline serous, invasive endometrioid, and invasive mucinous ovarian cancer subtypes [27]. The authors postulated a potential correlation between different cancer subtypes and the inflammatory adipose microenvironment rich in IL-6 and TNF-alpha, along with heightened levels of IGF-1 observed in obese patients. We speculate that similar molecular pathways may play a role in the development of distinct and more aggressive subtypes of PTC in obese individuals. Such molecular pathways may either act independently or interact with other known drivers of PTC tumorigenesis exacerbating tumor aggressiveness in obese individuals. Further in vivo and in vitro studies are needed to investigate the potential effects of adipose-tissue-derived factors on PTC tumorigenesis in obese patients.
Our data indicate that BMI could serve as a predictor of AHS, irrespective of gender. While the strength of the association is modest, we believe that clinicians should not overlook this finding and should consider incorporating BMI monitoring as part of the routine risk assessment for PTC.
In our study, overweight/obese patients with PTC had a higher proportion of bilateral, multifocal tumours, and larger nodal metastases than normal/underweight patients. Additionally, in younger patients (<55 years old) with PTC > 1 cm, the BMI predicted a higher ATA risk class. These associations were not observed in patients with FTC and HCC.
Studies investigating the relationship between BMI and aggressive histopathological features of TC have yielded conflicting results. While some studies have found no positive association between BMI and aggressive tumour features or recurrence [14,28], others have reported a significant association between higher BMI and extrathyroidal extension, multifocality, and lymph node metastasis in PTC [15,16,29]. Recent evidence suggests that obese patients with TC may activate different pathways compared to normal-weight patients. In a study by Basolo et al. [30], genes involved in metabolic pathways and immune-cell-related mechanisms were expressed differently in the thyroid tissue of obese patients compared to normal-weight patients. Furthermore, in a study on murine animal models by Kim et al., obesity exacerbated TC progression, resulting in increased tumour growth and a more aggressive type of TC [31].
We hypothesise that obesity may be a potential risk factor for the development of aggressive clinicopathological features in PTC, especially in younger patients. Although the exact mechanisms are not fully understood, it is conceivable that specific molecular pathways and gene expression profiles within adipose tissue, along with low-grade chronic inflammation, could play a role in the emergence of these aggressive features in PTC.
The lack of similar associations in patients with FTC and HCC may be attributed to various factors. We can speculate that the molecular mechanisms leading to the expression of aggressive features in TC among obese individuals could be specific to PTC. Additionally, the relatively small sample size of FTC and HCC patients should be considered, potentially impacting the ability to identify comparable associations in these subgroups. Furthermore, the retrospective nature of our study introduces inherent selection bias, potentially limiting the generalizability of these findings to a broader population. Lastly, in the present study, BMI was used as the primary metric for assessing obesity and overweight status, according to WHO definitions. However, although BMI is a widely accepted and practical measure, future research exploring obesity-related associations with cancer subtypes may also benefit from considering additional measures to provide a more comprehensive evaluation.
A significant strength of this study lies in the inclusion of a multicentric, large, diverse and representative sample, enhancing the external validity of our findings. Furthermore, the robustness of our study is underscored by a meticulous data collection process that systematically included a wide range of histopathological features in the analysis. This comprehensive approach contributed to a more nuanced understanding of the subject and improved our possibilities of identifying meaningful associations within the data.
Although our study supports the correlation between BMI and aggressive histopathological variants, further multicentric prospective studies with homogeneous samples are needed to confirm our results.
5. Conclusions
Our study contributes insights into the relationship between obesity and DTC, specifically focusing on the potential role of BMI in predicting AHS and aggressive clinico-pathological features of PTC. Caution should be used in generalizing these results to other TC subtypes, as the molecular dynamics may vary. Prospective studies are needed to confirm our findings.
Author Contributions
Conceptualization, G.D.F., G.L. and G.L.C.; methodology, G.D.F., G.L. and G.L.C.; data collection: G.D.F., G.L., D.S., E.M., P.B., L.R., B.G., M.C., G.K., I.P., E.P. and F.C., formal analysis, G.D.F., G.L. and G.L.C.; investigation, G.D.F., G.L., G.L.C. and P.F.N.; writing—original draft preparation, G.D.F.; writing—review and editing, all authors; supervision, F.M., G.M., P.G.C., T.P. and P.F.N.; project administration, G.D.F. and F.M.; funding acquisition, F.M. All authors have read and agreed to the published version of the manuscript.
Funding
The research leading to these results has received funding from the European Union—NextGenerationEU through the Italian Ministry of University and Research under PNRR–M4C2-I1.3 Project PE_00000019 “HEAL ITALIA” to Fabio Medas CUPF53C22000750006 University of Cagliari. The views and opinions expressed are those of the authors only and do not necessarily reflect those of the European Union or the European Commission. Neither the European Union nor the European Commission can be held responsible for them.
Institutional Review Board Statement
This research study was conducted retrospectively from data obtained for clinical purposes. Ethical approval was waived in view of the retrospective nature of the study and all the procedures being performed were part of the routine care. The present study is in accordance with the ethical standards of the 1964 Helsinki Declaration and its later amendments or comparable ethical standards.
Informed Consent Statement
A written informed consent to anonymised data collection was signed by each patient included in the study.
Data Availability Statement
Data are contained within the article.
Conflicts of Interest
The authors declare no conflicts of interest.
References
- Rahib, L.; Smith, B.D.; Aizenberg, R.; Rosenzweig, A.B.; Fleshman, J.M.; Matrisian, L.M. Projecting Cancer Incidence and Deaths to 2030: The Unexpected Burden of Thyroid, Liver, and Pancreas Cancers in the United States. Cancer Res. 2014, 74, 2913–2921. [Google Scholar] [CrossRef] [PubMed]
- Li, Y.; Huang, Y.; He, X.; Han, C.; Wu, W.; Shen, H.; Xu, Y.; Liu, Y.; Zhu, Z. The Global Burden of Thyroid Cancer in High-Income Asia-Pacific: A Systematic Analysis of the Global Burden of Disease Study. Ther. Adv. Endocrinol. Metab. 2022, 13, 20420188221090012. [Google Scholar] [CrossRef] [PubMed]
- Sanabria, A.; Kowalski, L.P.; Shah, J.P.; Nixon, I.J.; Angelos, P.; Williams, M.D.; Rinaldo, A.; Ferlito, A. Growing Incidence of Thyroid Carcinoma in Recent Years: Factors Underlying Overdiagnosis. Head Neck 2018, 40, 855–866. [Google Scholar] [CrossRef] [PubMed]
- Pizzato, M.; Li, M.; Vignat, J.; Laversanne, M.; Singh, D.; Vecchia, C.L.; Vaccarella, S. The Epidemiological Landscape of Thyroid Cancer Worldwide: GLOBOCAN Estimates for Incidence and Mortality Rates in 2020. Lancet Diabetes Endocrinol. 2022, 10, 264–272. [Google Scholar] [CrossRef] [PubMed]
- Malandrino, P.; Russo, M.; Gianì, F.; Pellegriti, G.; Vigneri, P.; Belfiore, A.; Rizzarelli, E.; Vigneri, R. Increased Thyroid Cancer Incidence in Volcanic Areas: A Role of Increased Heavy Metals in the Environment? Int. J. Mol. Sci. 2020, 21, 3425. [Google Scholar] [CrossRef] [PubMed]
- Mazonakis, M.; Tzedakis, A.; Damilakis, J.; Gourtsoyiannis, N. Thyroid Dose from Common Head and Neck CT Examinations in Children: Is There an Excess Risk for Thyroid Cancer Induction? Eur. Radiol. 2007, 17, 1352–1357. [Google Scholar] [CrossRef]
- Boutari, C.; Mantzoros, C.S. A 2022 Update on the Epidemiology of Obesity and a Call to Action: As Its Twin COVID-19 Pandemic Appears to Be Receding, the Obesity and Dysmetabolism Pandemic Continues to Rage On. Metabolism 2022, 133, 155217. [Google Scholar] [CrossRef] [PubMed]
- Pati, S.; Irfan, W.; Jameel, A.; Ahmed, S.; Shahid, R.K. Obesity and Cancer: A Current Overview of Epidemiology, Pathogenesis, Outcomes, and Management. Cancers 2023, 15, 485. [Google Scholar] [CrossRef] [PubMed]
- Mitchelson, K.A.J.; O’Connell, F.; O’Sullivan, J.; Roche, H.M. Obesity, Dietary Fats, and Gastrointestinal Cancer Risk-Potential Mechanisms Relating to Lipid Metabolism and Inflammation. Metabolites 2024, 14, 42. [Google Scholar] [CrossRef]
- Patel, A.V.; Patel, K.S.; Teras, L.R. Excess Body Fatness and Cancer Risk: A Summary of the Epidemiologic Evidence. Surg. Obes. Relat. Dis. 2023, 19, 742–745. [Google Scholar] [CrossRef]
- Kitahara, C.M.; Platz, E.A.; Park, Y.; Hollenbeck, A.R.; Schatzkin, A.; Berrington de González, A. Body Fat Distribution, Weight Change during Adulthood, and Thyroid Cancer Risk in the NIH-AARP Diet and Health Study. Int. J. Cancer 2012, 130, 1411–1419. [Google Scholar] [CrossRef] [PubMed]
- Harikrishna, A.; Ishak, A.; Ellinides, A.; Saad, R.; Christodoulou, H.; Spartalis, E.; Paschou, S.A. The Impact of Obesity and Insulin Resistance on Thyroid Cancer: A Systematic Review. Maturitas 2019, 125, 45–49. [Google Scholar] [CrossRef] [PubMed]
- Li, L.-R.; Song, J.-L.; Liu, H.-Q.; Chen, C. Metabolic Syndrome and Thyroid Cancer: Risk, Prognosis, and Mechanism. Discov. Oncol. 2023, 14, 23. [Google Scholar] [CrossRef] [PubMed]
- Paes, J.E.; Hua, K.; Nagy, R.; Kloos, R.T.; Jarjoura, D.; Ringel, M.D. The Relationship between Body Mass Index and Thyroid Cancer Pathology Features and Outcomes: A Clinicopathological Cohort Study. J. Clin. Endocrinol. Metab. 2010, 95, 4244–4250. [Google Scholar] [CrossRef] [PubMed]
- Economides, A.; Giannakou, K.; Mamais, I.; Economides, P.A.; Papageorgis, P. Association Between Aggressive Clinicopathologic Features of Papillary Thyroid Carcinoma and Body Mass Index: A Systematic Review and Meta-Analysis. Front. Endocrinol. 2021, 12, 692879. [Google Scholar] [CrossRef] [PubMed]
- Kaliszewski, K.; Diakowska, D.; Rzeszutko, M.; Rudnicki, J. Obesity and Overweight Are Associated with Minimal Extrathyroidal Extension, Multifocality and Bilaterality of Papillary Thyroid Cancer. J. Clin. Med. 2021, 10, 970. [Google Scholar] [CrossRef]
- Shin, A.; Cho, S.; Jang, D.; Abe, S.K.; Saito, E.; Rahman, M.S.; Islam, M.R.; Sawada, N.; Shu, X.-O.; Koh, W.-P.; et al. Body Mass Index and Thyroid Cancer Risk: A Pooled Analysis of Half a Million Men and Women in the Asia Cohort Consortium. Thyroid 2022, 32, 306–314. [Google Scholar] [CrossRef] [PubMed]
- Kwon, H.; Chang, Y.; Cho, A.; Ahn, J.; Park, S.E.; Park, C.-Y.; Lee, W.-Y.; Oh, K.-W.; Park, S.-W.; Shin, H.; et al. Metabolic Obesity Phenotypes and Thyroid Cancer Risk: A Cohort Study. Thyroid 2019, 29, 349–358. [Google Scholar] [CrossRef] [PubMed]
- Haugen, B.R.; Alexander, E.K.; Bible, K.C.; Doherty, G.M.; Mandel, S.J.; Nikiforov, Y.E.; Pacini, F.; Randolph, G.W.; Sawka, A.M.; Schlumberger, M.; et al. 2015 American Thyroid Association Management Guidelines for Adult Patients with Thyroid Nodules and Differentiated Thyroid Cancer: The American Thyroid Association Guidelines Task Force on Thyroid Nodules and Differentiated Thyroid Cancer. Thyroid 2016, 26, 1–133. [Google Scholar] [CrossRef]
- Obesity: Preventing and Managing the Global Epidemic. Report of a WHO Consultation; WHO Technical Report Series 894; World Health Organization: Geneva, Switzerland, 2000; pp. 1–253.
- Baloch, Z.W.; Asa, S.L.; Barletta, J.A.; Ghossein, R.A.; Juhlin, C.C.; Jung, C.K.; LiVolsi, V.A.; Papotti, M.G.; Sobrinho-Simões, M.; Tallini, G.; et al. Overview of the 2022 WHO Classification of Thyroid Neoplasms. Endocr. Pathol. 2022, 33, 27–63. [Google Scholar] [CrossRef]
- Kwon, H.; Han, K.-D.; Park, C.-Y. Weight Change Is Significantly Associated with Risk of Thyroid Cancer: A Nationwide Population-Based Cohort Study. Sci. Rep. 2019, 9, 1546. [Google Scholar] [CrossRef] [PubMed]
- Pellegriti, G.; Frasca, F.; Regalbuto, C.; Squatrito, S.; Vigneri, R. Worldwide Increasing Incidence of Thyroid Cancer: Update on Epidemiology and Risk Factors. J. Cancer Epidemiol. 2013, 2013, 965212. [Google Scholar] [CrossRef] [PubMed]
- Hoang, T.; Song, D.; Lee, J.; Lee, E.K.; Hwangbo, Y.; Kim, J. Association among Body Mass Index, Genetic Variants of FTO, and Thyroid Cancer Risk: A Hospital-Based Case-Control Study of the Cancer Screenee Cohort in Korea. Cancer Res. Treat. 2021, 53, 857–873. [Google Scholar] [CrossRef] [PubMed]
- Kwan, M.L.; Kroenke, C.H.; Sweeney, C.; Bernard, P.S.; Weltzien, E.K.; Castillo, A.; Factor, R.E.; Maxfield, K.S.; Stijleman, I.J.; Kushi, L.H.; et al. Association of High Obesity with PAM50 Breast Cancer Intrinsic Subtypes and Gene Expression. BMC Cancer 2015, 15, 278. [Google Scholar] [CrossRef] [PubMed]
- Torres-de la Roche, L.A.; Steljes, I.; Janni, W.; Friedl, T.W.P.; De Wilde, R.L. The Association between Obesity and Premenopausal Breast Cancer According to Intrinsic Subtypes—A Systematic Review. Geburtshilfe Frauenheilkd. 2020, 80, 601–610. [Google Scholar] [CrossRef] [PubMed]
- Olsen, C.M.; Nagle, C.M.; Whiteman, D.C.; Ness, R.; Pearce, C.L.; Pike, M.C.; Rossing, M.A.; Terry, K.L.; Wu, A.H.; Risch, H.A.; et al. Obesity and Risk of Ovarian Cancer Subtypes: Evidence from the Ovarian Cancer Association Consortium. Endocr. Relat. Cancer 2013, 20, 251–262. [Google Scholar] [CrossRef] [PubMed]
- Grani, G.; Lamartina, L.; Montesano, T.; Ronga, G.; Maggisano, V.; Falcone, R.; Ramundo, V.; Giacomelli, L.; Durante, C.; Russo, D.; et al. Lack of Association between Obesity and Aggressiveness of Differentiated Thyroid Cancer. J. Endocrinol. Investig. 2019, 42, 85–90. [Google Scholar] [CrossRef]
- Kim, M.; Kang, Y.E.; Park, Y.J.; Koo, B.S.; Ku, E.J.; Choi, J.Y.; Lee, E.K.; Kim, B.H. Potential Impact of Obesity on the Aggressiveness of Low- to Intermediate-Risk Papillary Thyroid Carcinoma: Results from a MASTER Cohort Study. Endocrine 2023, 82, 134–142. [Google Scholar] [CrossRef]
- Basolo, A.; Poma, A.M.; Giannini, R.; Ceccarini, G.; Pelosini, C.; Fierabracci, P.; Castany, M.U.; Bechi Genzano, S.; Ambrosini, C.E.; Materazzi, G.; et al. Histological Pattern and Gene Expression Profiling of Thyroid Tissue in Subjects with Obesity. J. Endocrinol. Investig. 2022, 45, 413–423. [Google Scholar] [CrossRef]
- Kim, W.G.; Park, J.W.; Willingham, M.C.; Cheng, S. Diet-Induced Obesity Increases Tumor Growth and Promotes Anaplastic Change in Thyroid Cancer in a Mouse Model. Endocrinology 2013, 154, 2936–2947. [Google Scholar] [CrossRef]
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).