Simple Summary
Early detection and treatment are known to enhance the prognosis for pancreatic cancer, but there is little known about the characteristics of early pancreatic cancer. We thus aimed to identify the characteristics, clues for early detection, and prognostic factors for early pancreatic cancer by analyzing a large number of patients with stage 1 pancreatic cancers. Our study included 257 stage 1 pancreatic cancer patients and revealed that new-onset diabetes and intraductal papillary mucinous neoplasm (IPMN) were associated with early pancreatic cancers smaller than 2 cm (T1, stage 1A). In particular, pancreatic cancers smaller than 1 cm were closely associated with IPMN. These results indicate that appropriate follow-up and treatment of IPMN are important for the early detection and curing of pancreatic cancer. Since perineural invasion is a significant risk factor for both poor overall and disease-free survival in patients with stage 1 pancreatic cancer, active adjuvant therapy is required in stage 1 pancreatic cancers that feature the presence of perineural invasion.
Abstract
Background: Little is known about the characteristics of early pancreatic cancer. We aimed to identify the characteristics, clues for early detection, and prognostic factors for early pancreatic cancer by analyzing a large number of patients with stage 1 pancreatic cancer. Methods: A clinical data warehouse that includes databases of all the medical records of eight academic institutions was used to select and analyze patients with pancreatic cancer that had been diagnosed from January 2010 to May 2023. Results: In total, 257 stage 1 pancreatic cancer patients were included. There were 134 men (52%), and the average age was 67.2 ± 9.9 years. Compared to patients with stage 1B pancreatic cancer (2–4 cm), patients with stage 1A pancreatic cancer (≤2 cm) had more tumors in the body and tail than in the head (p = 0.028), more new-onset diabetes and less old diabetes (p = 0.010), less jaundice (p = 0.020), more follow-up of IPMN (intraductal papillary mucinous neoplasm, p = 0.029), and more histories of acute pancreatitis (p = 0.013). The pathological findings showed that stage 1A pancreatic cancer involved more IPMNs (p < 0.001) and lower pancreatic intraepithelial neoplasia (p = 0.004). IPMN was present in all 13 pancreatic tumors that were smaller than 1 cm. In multivariate analysis, positive resection margin (odds ratio [OR] 1.536, p = 0.040), venous invasion (OR 1.710, p = 0.010), and perineural invasion (OR 1.968, p = 0.002) were found to be risk factors affecting disease-free survival, while old diabetes (odds ratio [OS] 1.981, p = 0.003) and perineural invasion (OR 2.270, p = 0.003) were found to be risk factors affecting overall survival. Conclusions: IPMN is closely associated with early pancreatic cancer and may provide an opportunity for early detection. The presence of perineural invasion was a crucial prognostic factor for both overall and disease-free survival in patients with stage 1 pancreatic cancer.
1. Introduction
Pancreatic cancer has the poorest prognosis among major cancers. The recently reported five-year relative survival rate of pancreatic cancer was 13% by the American Cancer Society (https://www.cancer.org/cancer/types/pancreatic-cancer/detection-diagnosis-staging/survival-rates.html, accessed on 1 February 2024) and 15.9% by the Korean Cancer Control Institute (https://cancer.go.kr/lay1/S1T648C650/contents.do, accessed on 1 February 2024). Survival rates for pancreatic cancer remain low despite ongoing advances in treatment. The early detection and treatment of low-stage pancreatic cancer is considered to be a good way to improve prognosis [1], yet the characteristics of early pancreatic cancer are still poorly understood. Pancreatic cancer is an uncommon cancer, as it affects 19.2 people in the US and 16.4 people in South Korea per 100,000 people. Stage 1 pancreatic cancer is even rarer, as it represents only 2.1% to 10.4% of all pancreatic cancers [2,3]. More specifically, stage 1A pancreatic cancers make up only 1.9% of all pancreatic cancers in the US [4]. As a result, it is difficult to study large numbers of individuals with early-stage pancreatic cancer, and there has been little research analyzing these uncommon early pancreatic cancers [2].
Pancreatic cancer stage can be determined according to the eighth edition TNM staging system of the American Joint Committee on Cancer (AJCC) Staging Manual [5]: T1 ≤ 2 cm, T2 > 2 cm but ≤ 4 cm, T3 > 4 cm, and T4 tumor involves the celiac axis, the superior mesenteric artery, and/or common hepatic artery; N0 no regional lymph node, N1 metastasis in 1–3 regional lymph nodes, and N2 metastasis in ≥ 4 regional lymph nodes; M0 no distant metastasis and M1 distant metastasis. The stages are 1A (T1N0M0), 1B (T2N0M0), 2 (T3 or N1), 3 (T4 or N2), and 4 (M1). Recent published survival data according to AJCC 8th edition showed that median overall survival was 19.6 months for stage 1, 14.7 months for stage 2, 14.3 months for stage 3, and 6.1 months for stage 4 [6]. In stage 1, median overall survival was 35.8 months for stage 1A and 16.8 months for stage 1B. The risk factors associated with development of pancreatic cancer include obesity [7], type 2 diabetes [8], cigarette smoking [9], family history of pancreatic cancer [10,11], and chronic pancreatitis [12]. Some pancreatic ductal adenocarcinomas arise from macroscopic cystic precursors, intraductal papillary mucinous neoplasms (IPMNs) and mucinous cystic neoplasms.
A clinical data warehouse is a platform that allows information from multiple institutions to be shared anonymously, which makes it possible to identify a large number of patients with pancreatic cancer, including those with stage 1 pancreatic cancers. Thus, we aimed to identify the characteristics of early pancreatic cancer, to provide clues for early detection and identify prognostic factors for early pancreatic cancer by analyzing a large number of patients with stage 1 pancreatic cancer using a clinical data warehouse.
2. Materials and Methods
2.1. Study Population and Data Collection
A clinical data warehouse that contains all of the medical records from eight academic institutions was used to select and study the patients. This study included patients who were diagnosed with pancreatic cancer between January 2010 and May 2023. Of the 9428 patients with pancreatic cancer who met the eligibility criteria, 257 patients (2.7%) were found to have stage 1 pancreatic cancer, as histopathologically determined by surgery according to the AJCC 8th edition. Stage 1 pancreatic cancer includes a maximum tumor diameter of 2 cm or less (T1) and a maximum tumor diameter of 2–4 cm (T2) with no regional lymph node metastasis, and no distant metastasis.
The following clinical information was analyzed: height, weight, age, gender, serum CA 19-9 level, smoking history, drinking history, family history of cancers, history of acute and chronic pancreatitis, follow-up period, death, cause of death, survival period, recurrence time, recurrence site, neoadjuvant therapy, and adjuvant therapy. Surgical findings and pathological examination comprised the name of the surgery, tumor location, tissue diagnosis, degree of differentiation, tumor size, IPMN accompanied by cancer, lymph node metastasis, lymphatic, venous, perineural invasion, and marginal status. Lastly, imaging tests, including CT and MRI, comprised tumor size, main pancreatic duct dilatation, pancreas atrophy, and CBD (common bile duct) invasion.
2.2. Definitions
Age, BMI (body mass index), CA 19-9 level, and jaundice were recorded as of the time of diagnosis. Smoking and drinking were divided according to the presence or absence thereof. In classifying pancreatic tumor locations, the head included the uncinate process, and the body included the neck. (Figure 1). Diabetes diagnosed just before pancreatic cancer was defined as new-onset diabetes. Overlapping symptoms were analyzed separately. IPMN accompanied by cancer was diagnosed by histologic findings in the surgical specimen.
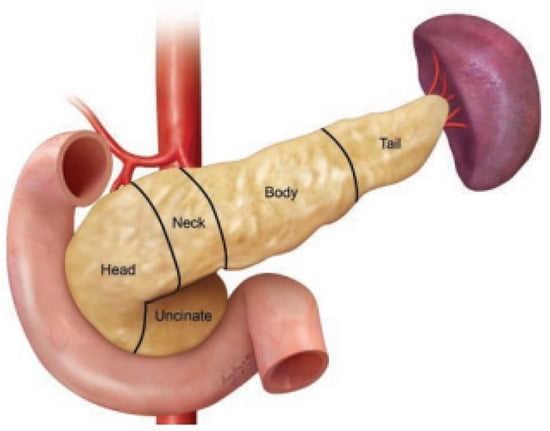
Figure 1.
Normal pancreatic anatomy. Reprinted with permission from ref. [13]. Copyright 2020 Georg Thieme Verlag KG.
2.3. Statistical Analysis
The results are reported in the form of frequency (percent) or mean ± standard deviation unless otherwise specified. The categorical and continuous data of the clinical characteristics in the two groups were compared by Pearson’s chi–square test/Fisher’s exact test and Student’s t test. The life table method was used to determine the median survival time and five-year-survival rate. The cumulative survival of pancreatic cancer was plotted using the Kaplan–Meier method and compared by Log rank test. In both univariate and multivariate analyses, Cox regression analyses were used to identify risk factors associated with pancreatic cancer patients’ survival. Multivariate analysis was performed on the factors that were found to be significant in univariate analysis. The odds ratios (ORs) and their 95% confidence intervals (CIs) are presented together. A p value < 0.05 was considered to indicate statistical significance. SPSS (SPSS for Windows, version 20; Chicago, IL, USA) was used for all statistical analyses.
3. Results
3.1. Characteristics of Patients with Stage 1 Pancreatic Cancer
In total, 257 stage 1 pancreatic cancer patients were included (Table 1). There were 134 men (52%) and 123 women (48%). The average age was 67.2 ± 9.9 years, and 203 (79%) were over 60 years old. The follow-up time for stage 1B (2–4 cm) patients was 25.1 ± 22.5 months, which was shorter than the follow-up time of 33.8 ± 24.7 months for stage 1A (≤2 cm) patients (p = 0.011). Patients with stage 1A pancreatic cancer had more tumors in the body and tail than in the head (p = 0.028), more new-onset diabetes and less old diabetes (p = 0.010), and lower serum CA 19-9 level (p < 0.001) compared to patients with stage 1B pancreatic cancer. However, there were no differences in smoking, alcohol use, BMI, or family history of pancreatic cancer between patients with stage 1A and 1B.

Table 1.
Baseline characteristics of patients with stage 1 pancreatic cancer.
3.2. Reasons for Initial Examination and Image Findings of Stage 1 Pancreatic Cancers
Prior to the diagnosis of pancreatic cancer, the patients visited the hospital for a variety of reasons (Table 2). Compared to stage 1B patients, stage 1A pancreatic cancer patients were more likely to have a follow-up for IPMN and have new-onset diabetes or acute pancreatitis (p = 0.029, 0.001, and 0.013, respectively). On the other hand, stage 1B patients experienced jaundice more frequently (p = 0.020). Meanwhile, abdominal pain, back pain, nausea, vomiting, diarrhea, and constipation did not differ between stage 1A and stage 1B.
Table 2.
Reasons for initial examination in patients with stage 1 pancreatic cancer.
As can be seen from the CT and MRI findings, main pancreatic duct dilatation was similarly observed in 45 (74%) stage 1A and 145 (75%) stage 1B cases. CBD invasion was more predominant in stage 1B than stage 1A (p = 0.028). However, smaller pancreatic tumors (stage 1A) were significantly associated with mural nodules and cystic size increases (p < 0.001 and p = 0.012, respectively). Some pancreatic cancers could not be observed on CT or MRI; there were 14 tumors (5%) that could not be observed on either CT and MRI, 17 tumors (10%) that could be identified on MRI but not on CT, and 11 tumors (6%) that could be identified on CT but not on MRI. However, there was no difference in invisible tumors between stage 1A and stage 1B. When the pancreatic cancer sizes in the pathology were compared to the sizes shown in CT or MRI, both CT and MRI tended to measure the tumor as smaller than the actual pancreatic cancer size, although it was not statistically significant. The average size differences between pathology and CT and between pathology and MRI were 4.24 ± 7.24 mm and 3.24 ± 6.96 mm, respectively. The CT findings showed that four tumors (1.6%) were measured from 20 to 25 mm smaller than the actual tumors, and 30 tumors (11.7%) were measured from 10 to 19 mm smaller than the actual tumors. MRI revealed that 32 tumors (12.5%) were measured more than 10 mm smaller than the actual tumors. Conversely, pancreatic tumors were measured to be 10 mm or larger than the actual tumor in only six cases (2.3%) on CT and only four cases (1.6%) on MRI.
3.3. Surgical Outcomes of Stage 1 Pancreatic Cancers and Clinical Characteristics of Patients with Pancreatic Cancers Smaller Than 1 cm
Examination of the postoperative pathologic findings yielded that stage 1B pancreatic cancers showed a more positive resection margin (p = 0.002), lymphatic invasion (p = 0.008), venous invasion (p = 0.001), and perineural invasion (p < 0.001) than stage 1A cancers (Table 3). IPMNs accompanied by cancers were more often in stage 1A (p < 0.001), while PanIN (pancreatic intraepithelial neoplasia) was more often in stage 1B (p = 0.004). Thirteen patients (5.1%) had pancreatic cancer measuring smaller than 1 cm; all of them had IPMN and an invasive carcinoma component in IPMN (Table 4). Out of these 13 patients, only one (7.7%) had abnormally high CA 19-9 levels (49.1 U/mL); the other patients’ levels were within the normal limit (<37 U/mL). Seven (53.8%) had mural nodules. Consequently, stage 1A featured less lymphatic/venous/perineural invasion and more negative resection margins than stage 1B, and IPMNs were frequently accompanied by pancreatic cancer. In particular, IPMN was present in all cases of very small pancreatic tumors measuring smaller than 1 cm.
Table 3.
Surgical outcomes of stage 1 pancreatic cancers.
Table 4.
Characteristics of pancreatic cancer less than 1 cm in stage 1 pancreatic cancer.
3.4. Survival and Factors Related to Overall Survival and Disease-Free Survival
Patients with stage 1 pancreatic cancer showed a five-year overall survival rate of 41% and a median overall survival time of 3.47 years. The five-year overall survival rates in patients with tumors < 1 cm, 1–2 cm, and 2–4 cm in size were 100%, 59%, and 34%, respectively. Patients with tumors 1–2 cm in size had a higher five-year overall survival rate than patients with tumors 2–4 cm in size (p = 0.002) (Figure 2A). The five-year disease-free survival rate was 28%, and the median disease-free survival period was 1.55 years in patients with stage 1 pancreatic cancers. The five-year disease-free survival rate in patients with tumors < 1 cm, 1–2 cm, and 2–4 cm in size were 100%, 35%, and 23%, respectively. Patients with tumors < 1 cm in size had a higher five-year disease-free survival rate than patients with tumors 1–2 cm in size (p = 0.017), and patients with tumors 1–2 cm in size had a higher five-year disease-free survival rate than patients with tumors 2–4 cm in size (p = 0.001) (Figure 2B). The results of univariate analysis showed that old diabetes, jaundice, CA 19-9 level, IPMN, and perineural invasion were all associated with overall survival (p < 0.05), while alcohol intake, BMI ≥ 25, jaundice, CA 19-9 level, IPMN, resection margin, lymphatic invasion, venous invasion, and perineural invasion were all associated with disease-free survival (p < 0.05) (Table 5). Multivariate analysis revealed that the factors related to overall survival were old diabetes (OR 1.981, 95% CI 1.268–3.093, p = 0.003) and perineural invasion (OR 2.270, 95% CI 1.317–3.914, p = 0.003), and that the factors related to disease-free survival were positive resection margin (OR 1.536, 95% CI 1.021–2.312, p = 0.040), venous invasion (OR 1.710, 95% CI 1.137–2.574, p = 0.010), and perineural invasion (OR 1.968, 95% CI 1.277–3.033, p = 0.002). Perineural invasion was found to be a risk factor that was associated with both overall and disease-free survival.
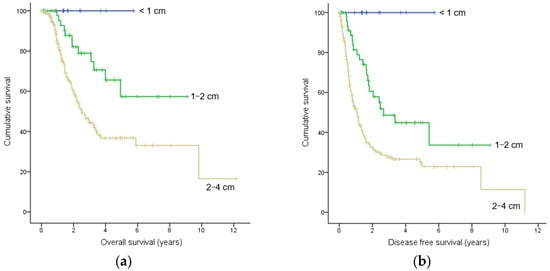
Figure 2.
Kaplan–Meier estimates of the (a) overall survival and (b) disease-free survival according to tumor sizes. Censored subjects are indicated on the Kaplan–Meier curve as tick marks.
Table 5.
Univariate and multivariate analysis of factors for overall survival and disease-free survival in stage 1 pancreatic cancer.
4. Discussion
Pancreatic cancer presents a poor prognosis for several reasons. First, pancreatic cancer typically grows and spreads quickly. This makes it difficult to effectively treat, particularly if metastases have already occurred. Further, there are not many options for treating pancreatic cancer; surgery is frequently the best course of action. However, if the cancer has spread or abutted major vessels, surgery may not be an option. Even though radiation and chemotherapy are frequently used to treat cancer, their efficacy may be compromised in more advanced stages. Further, compared to other forms of cancer, pancreatic cancer cells might be more resistant to radiation and chemotherapy [14]. This resistance may make it more difficult to find a cure or long-term remission. The prognosis for individuals with pancreatic cancer may be improved by ongoing research into novel and more potent medicines, such as immunotherapies and targeted regimens [15]. However, these efforts have not yet met our expectations. Since the prognosis for advanced pancreatic cancer is very poor, early pancreatic cancer detection is crucial for improving the prognosis [16,17]. On the other hand, early-stage pancreatic cancer may not cause noticeable symptoms, and by the time symptoms appear, the disease is often advanced. Moreover, there are no generally accepted screening techniques for pancreatic cancer, unlike several other malignancies. Despite these challenges, efforts must be made to detect and treat early pancreatic cancer.
Several studies have reported the incidence and survival rates of stage 1 pancreatic cancer. The median overall survival rates for 8960 patients following surgical resection for non-metastatic pancreatic adenocarcinoma have been reported to be 38 months for stage 1A and 24 months for stage 1B, according to the Surveillance, Epidemiology and End Results database (2004–2013) [18]. Using institutional databases from four referral centers across Europe and one referral center in the US, the five-year-survival rates have been reported to 39.2% for 118 stage 1A patients and 27.6% for 144 stage 1B patients [19]. According to the Japan Pancreatic Cancer Registry, out of all pancreatic cancers, the proportions of cases in stages 0, 1A, and 1B were 1.7%, 4.1%, and 6.3%, respectively [3]. Patients with stage 0 (in situ), stage 1A, and stage 1B had five-year-survival rates of 85.8%, 68.7%, and 59.7%, respectively, while the five-year-survival rate of cases with pancreatic cancer smaller than 10 mm (TS1a) reached 80.4%, although such cancers only account for 0.8% of all pancreatic cancers. A study analyzed 200 cases of stage 0 and stage 1 pancreatic cancer 14 Japanese institutions [2]. The proportions of cases in stages 0 and I were 0.7% and 2.3%, respectively. The estimated 10 years overall survival rates for stage 0, stage 1 (TS1a), and stage 1 (TS1b, tumor size 11–20 mm) were 94.7%, 93.8%, and 78.9%, respectively. Therefore, stage 1 pancreatic cancer is uncommon, but it has a favorable prognosis. In the present study, there were only 61 (0.6%) and 196 (2.1%) patients with stage 1A and stage 1B pancreatic cancer, respectively among all pancreatic cancers, but their five-year-survival rates were high at 64% and 34%, respectively. In particular, early tumors measuring 10 mm or smaller have an extremely good survival rate.
The goal of early detection pancreatic cancer is to enhance prognosis. Since currently available data demonstrated a difference of more than 10% in survival rates between stages 1A and 1B, it is important to detect stage 1A pancreatic cancer. Therefore, it is essential to understand and characterize stage 1A pancreatic cancer. There have been very few studies examining the clinical manifestations of early pancreatic cancer, and little is known about their characteristics. The present study discovered some clinical distinctions between pancreatic cancer measuring 2–4 cm (stage 1B) and those measuring smaller than 2 cm (stage 1A). New-onset diabetes was more frequent in stage 1A pancreatic cancer, and old diabetes was more frequent in stage 1B, suggesting that new-onset diabetes may provide a clue for detecting pancreatic cancer at earlier stages. There was also more jaundice in stage 1B. Although jaundice is generally considered to be helpful in detecting early pancreatic cancer, our study showed that jaundice is more common in larger tumors in stage 1. Therefore, jaundice was not considered to be a suitable symptom for detecting early curable cancer (stage 1A). History of acute pancreatitis and follow-up of IPMN were more common in patients with stage 1A pancreatic cancer, indicating that these conditions play a significant role in detecting early pancreatic cancer. Further, the number of cases accompanied by IPMN in the surgical specimen was significantly larger in stage 1A than in stage 1B (34% vs. 10%). Therefore, cases of stage 1 pancreatic cancer associated with IPMN could be smaller and earlier cancers.
Pancreatic cancer evaluation currently relies heavily on CT, and MRI combined with MRCP allows for a more thorough examination of the morphological alterations of the pancreatic duct and parenchyma, which helps detect cancers earlier and more effectively [20]. However, in the present study, 5% of cases of pancreatic cancer were not apparent on both CT and MRI, while 16% of cases were only detectable on either CT or MRI. This demonstrates how challenging it is to detect small tumors. All tumors that were smaller than 1 cm discovered in the present study were accompanied by IPMNs, and their invasive cancer components were not discriminated by imaging studies. The actual size of the tumor tended to be larger than that measured on CT or MRI, and the tumor size on CT tended to be smaller than that measured on MRI. Therefore, it is important to keep in mind that the pancreatic cancer might actually be larger than what appears on an MRI or CT scan.
Although stage 1A pancreatic cancer has a better prognosis than stage 1B pancreatic cancer, it is not uncommon for stage 1A pancreatic cancers to recur. The five-year-survival rate of stage 1A pancreatic cancer has been reported to be 39–68% [10]. On the other hand, the prognosis for pancreatic cancers smaller than 1 cm is excellent, and all patient who had tumors smaller than 1 cm in the present study were followed up without recurrence. Thus, to achieve complete cure without recurrence, it is necessary to detect pancreatic cancer smaller than 1 cm and then perform surgery. In the present study, all 13 patients with pancreatic cancer smaller than 1 cm were associated with IPMN. Accordingly, appropriate follow-up and surgery of IPMN is one of the ways to detect early pancreatic cancer and cure it completely.
Perineural invasion was found to be a common factor in both overall survival and disease-free survival in our study. Perineural invasion, which is the neoplastic invasion of tumor cells into or surrounding the nerves, is a common histological feature of many other cancers. Perineural invasion is particularly common in pancreatic cancer, and it is a sign of aggressive tumor behavior and a bad prognosis [21,22]. Further, a tumor’s recurrence may be associated with the intrapancreatic perineural invasion status [23]. Perineural invasion is believed to reflect the initial stages of metastasis, and it can happen without lymphatic or vascular invasion [24,25]. Patients with perineural invasion have been reported to have an overall survival of more than two years less than those without perineural invasion [26]. Moreover, early in the development of pancreatic cancer, neuroplastic alterations such as enhanced neuronal hypertrophy and sprouting have been associated with the dissemination of cancer along with perineural invasion [27,28,29]. Perineural invasion is not uncommon in cases of early pancreatic cancer, whereas lymphatic or venous invasion is uncommon. According to our study, in stage 1A patients, lymphatic invasion occurred in 15% of cases, venous invasion occurred in 11% of cases, and perineural invasion occurred in 42% of cases, suggesting that perineural invasion may occur in early pancreatic cancer. Perineural invasion was significantly related to both overall survival and disease-free survival, which showed that it is important for prognosis. Therefore, in cases of perineural invasion, more aggressive adjuvant therapy is warranted.
There are a few limitations in this study: First, it is a retrospective study. In some cases, it is not possible to obtain all necessary data in detail due to the retrospective design. However, the clinical data warehouse that we used in this study includes all the patient’s medical records, images, laboratory, and pathology results, so it enabled us to identify patients in more detail, unlike other big data sources. Second, aside from CT and MRI, endoscopic ultrasound (EUS) is important for pancreatic cancer screening, but this was not covered in this study. Unfortunately, EUS was not performed in many cases, and EUS findings were not verified, so EUS could not be included in this study. Lastly, there were a few positive radial margins in stage 1B, including seven cases with a positive radial margin of less than 1 mm. Most American pathologists set the standard for R1 as direct invasion, while in Europe, R1 is considered to be present when the distance between the tumor and the resection margin is less than 1 mm [30]. In this study, in cases of less than 1 mm, the resection margin was often almost in contact with the tumor, so the resection margin was classified as positive according to European standards.
5. Conclusions
Although tremendous efforts have been made, up to this point, the prognosis for pancreatic cancer has still not changed significantly. However, early detection and treatment are considered to enhance the prognosis for pancreatic cancer, although this is challenging. Our study revealed that new-onset diabetes and IPMN were associated with early pancreatic cancers that were smaller than 2 cm. In particular, pancreatic cancers smaller than 1 cm were closely associated with IPMN. Therefore, it is important for early detection to closely follow up IPMN and perform surgery at an appropriate time. In the case of newly diagnosed diabetes and acute pancreatitis, it would be helpful to check whether pancreatic cancer is present. Active adjuvant therapy can be considered to be required in early pancreatic cancer when perineural invasion is present, since perineural invasion is related to poor overall and disease-free survival in patients with stage 1 pancreatic cancer.
Author Contributions
Conceptualization, J.H.C.; methodology, J.H.C. and Y.H.C.; validation, C.N.P. and I.S.L.; formal analysis, H.S.K., Y.H.C. and J.H.C.; investigation, H.S.K., Y.H.C., Y.S.L. and J.H.C.; resources, Y.H.C., J.S.L., I.H.J., S.W.K., K.H.P., H.H.C., H.H.L. and J.H.C.; data curation, H.S.K., Y.H.C. and J.H.C.; writing—original draft preparation, J.H.C.; writing—review and editing, J.H.C.; visualization, H.S.K. and Y.H.C.; supervision, C.N.P. and I.S.L. All authors have read and agreed to the published version of the manuscript. H.S.K. and Y.H.C. contributed equally to this work as the first authors.
Funding
This research received no external funding.
Institutional Review Board Statement
This study was conducted in accordance with the Declaration of Helsinki and approved by the Ethics Committee of Institutional Review Board of Bucheon St. Mary’s Hospital (protocol number: HC23WISI0060 and date of approval: 18 July 2023).
Informed Consent Statement
Patient consent was waived due to the nature of this study, which was retrospective and non-interventional.
Data Availability Statement
The datasets generated or analyzed during the current study are not publicly available due to privacy policies but are available from the corresponding author on reasonable request.
Acknowledgments
The authors would like to thank Sang Hi Park for the support in the statistical and comprehensive analysis.
Conflicts of Interest
The authors declare no competing interests.
Abbreviations
IPMN (intraductal papillary mucinous neoplasm), OR (odds ratio), CT (computed tomography), MRI (magnetic resonance imaging), CBD (common bile duct), BMI (body mass index), confidence interval (CI), PanIN (pancreatic intraepithelial neoplasia), PPPD (pancreas-preserving pancreaticoduodenectomy), DP (distal pancreatectomy), TP (total pancreatectomy), SD (standard deviation), EUS (endoscopic ultrasound).
References
- Poruk, K.E.; Firpo, M.A.; Adler, D.G.; Mulvihill, S.J. Screening for pancreatic cancer: Why, how, and who? Ann. Surg. 2013, 257, 17–26. [Google Scholar] [CrossRef]
- Kanno, A.; Masamune, A.; Hanada, K.; Maguchi, H.; Shimizu, Y.; Ueki, T.; Hasebe, O.; Ohtsuka, T.; Nakamura, M.; Takenaka, M.; et al. Multicenter study of early pancreatic cancer in Japan. Pancreatology 2018, 18, 61–67. [Google Scholar] [CrossRef]
- Egawa, S.; Toma, H.; Ohigashi, H.; Okusaka, T.; Nakao, A.; Hatori, T.; Maguchi, H.; Yanagisawa, A.; Tanaka, M. Japan Pancreatic Cancer Registry; 30th year anniversary: Japan Pancreas Society. Pancreas 2012, 41, 985–992. [Google Scholar] [CrossRef] [PubMed]
- Blackford, A.L.; Canto, M.I.; Klein, A.P.; Hruban, R.H.; Goggins, M. Recent Trends in the Incidence and Survival of Stage 1A Pancreatic Cancer: A Surveillance, Epidemiology, and End Results Analysis. J. Natl. Cancer Inst. 2020, 112, 1162–1169. [Google Scholar] [CrossRef]
- Amin, M.B.; Edge, S.; Greene, F.; Byrd, D.R.; Brookland, R.K.; Washington, M.K.; Gershenwald, J.E.; Compton, C.C.; Hess, K.R.; Sullivan, D.C.; et al. AJCC Cancer Staging Manual, 8th ed.; Springer: New York, NY, USA, 2017. [Google Scholar]
- Kang, H.; Kim, S.S.; Sung, M.J.; Jo, J.H.; Lee, H.S.; Chung, M.J.; Park, J.Y.; Park, S.W.; Song, S.Y.; Park, M.S.; et al. Evaluation of the 8th Edition AJCC Staging System for the Clinical Staging of Pancreatic Cancer. Cancers 2022, 14, 4672. [Google Scholar] [CrossRef] [PubMed]
- Arslan, A.A.; Helzlsouer, K.J.; Kooperberg, C.; Shu, X.O.; Steplowski, E.; Bueno-de-Mesquita, H.B.; Fuchs, C.S.; Gross, M.D.; Jacobs, E.J.; Lacroix, A.Z.; et al. Anthropometric measures, body mass index, and pancreatic cancer: A pooled analysis from the Pancreatic Cancer Cohort Consortium (PanScan). Arch. Intern. Med. 2010, 170, 791–802. [Google Scholar] [CrossRef] [PubMed]
- Bosetti, C.; Rosato, V.; Li, D.; Silverman, D.; Petersen, G.M.; Bracci, P.M.; Neale, R.E.; Muscat, J.; Anderson, K.; Gallinger, S.; et al. Diabetes, antidiabetic medications, and pancreatic cancer risk: An analysis from the International Pancreatic Cancer Case-Control Consortium. Ann. Oncol. 2014, 25, 2065–2072. [Google Scholar] [CrossRef]
- Iodice, S.; Gandini, S.; Maisonneuve, P.; Lowenfels, A.B. Tobacco and the risk of pancreatic cancer: A review and meta-analysis. Langenbecks Arch. Surg. 2008, 393, 535–545. [Google Scholar] [CrossRef]
- Hruban, R.H.; Canto, M.I.; Goggins, M.; Schulick, R.; Klein, A.P. Update on familial pancreatic cancer. Adv. Surg. 2010, 44, 293–311. [Google Scholar] [CrossRef]
- Klein, A.P.; Brune, K.A.; Petersen, G.M.; Goggins, M.; Tersmette, A.C.; Offerhaus, G.J.; Griffin, C.; Cameron, J.L.; Yeo, C.J.; Kern, S.; et al. Prospective risk of pancreatic cancer in familial pancreatic cancer kindreds. Cancer Res. 2004, 64, 2634–2638. [Google Scholar] [CrossRef]
- Raimondi, S.; Lowenfels, A.B.; Morselli-Labate, A.M.; Maisonneuve, P.; Pezzilli, R. Pancreatic cancer in chronic pancreatitis; aetiology, incidence, and early detection. Best Pract. Res. Clin. Gastroenterol. 2010, 24, 349–358. [Google Scholar] [CrossRef] [PubMed]
- Taher, A.; Mujtaba, B.; Ramani, N.S.; Patel, A.; Morani, A.C. The Postoperative Pancreas Imaging. J. Gastrointest. Abdom. Radiol. 2020, 3, 87–98. [Google Scholar] [CrossRef]
- Zeng, S.; Pöttler, M.; Lan, B.; Grützmann, R.; Pilarsky, C.; Yang, H. Chemoresistance in Pancreatic Cancer. Int. J. Mol. Sci. 2019, 20, 4504. [Google Scholar] [CrossRef]
- Bear, A.S.; Vonderheide, R.H.; O’Hara, M.H. Challenges and Opportunities for Pancreatic Cancer Immunotherapy. Cancer Cell 2020, 38, 788–802. [Google Scholar] [CrossRef]
- Singhi, A.D.; Koay, E.J.; Chari, S.T.; Maitra, A. Early Detection of Pancreatic Cancer: Opportunities and Challenges. Gastroenterology 2019, 156, 2024–2040. [Google Scholar] [CrossRef] [PubMed]
- Gheorghe, G.; Bungau, S.; Ilie, M.; Behl, T.; Vesa, C.M.; Brisc, C.; Bacalbasa, N.; Turi, V.; Costache, R.S.; Diaconu, C.C. Early Diagnosis of Pancreatic Cancer: The Key for Survival. Diagnostics 2020, 10, 869. [Google Scholar] [CrossRef]
- Kamarajah, S.K.; Burns, W.R.; Frankel, T.L.; Cho, C.S.; Nathan, H. Validation of the American Joint Commission on Cancer (AJCC) 8th Edition Staging System for Patients with Pancreatic Adenocarcinoma: A Surveillance, Epidemiology and End Results (SEER) Analysis. Ann. Surg. Oncol. 2017, 24, 2023–2030. [Google Scholar] [CrossRef] [PubMed]
- van Roessel, S.; Kasumova, G.G.; Verheij, J.; Najarian, R.M.; Maggino, L.; de Pastena, M.; Malleo, G.; Marchegiani, G.; Salvia, R.; Ng, S.C.; et al. International Validation of the Eighth Edition of the American Joint Committee on Cancer (AJCC) TNM Staging System in Patients With Resected Pancreatic Cancer. JAMA Surg. 2018, 153, e183617. [Google Scholar] [CrossRef] [PubMed]
- Lee, E.S.; Lee, J.M. Imaging diagnosis of pancreatic cancer: A state-of-the-art review. World J. Gastroenterol. 2014, 20, 7864–7877. [Google Scholar] [CrossRef]
- Felsenstein, M.; Lindhammer, F.; Feist, M.; Hillebrandt, K.H.; Timmermann, L.; Benzing, C.; Globke, B.; Zocholl, D.; Hu, M.; Fehrenbach, U.; et al. Perineural Invasion in Pancreatic Ductal Adenocarcinoma (PDAC): A Saboteur of Curative Intended Therapies? J. Clin. Med. 2022, 11, 2367. [Google Scholar] [CrossRef]
- Hirai, I.; Kimura, W.; Ozawa, K.; Kudo, S.; Suto, K.; Kuzu, H.; Fuse, A. Perineural invasion in pancreatic cancer. Pancreas 2002, 24, 15–25. [Google Scholar] [CrossRef] [PubMed]
- Zhang, J.F.; Hua, R.; Sun, Y.W.; Liu, W.; Huo, Y.M.; Liu, D.J.; Li, J. Influence of perineural invasion on survival and recurrence in patients with resected pancreatic cancer. Asian Pac. J. Cancer Prev. 2013, 14, 5133–5139. [Google Scholar] [CrossRef] [PubMed]
- Liebig, C.; Ayala, G.; Wilks, J.A.; Berger, D.H.; Albo, D. Perineural invasion in cancer: A review of the literature. Cancer 2009, 115, 3379–3391. [Google Scholar] [CrossRef]
- Chang, A.; Kim-Fuchs, C.; Le, C.P.; Hollande, F.; Sloan, E.K. Neural Regulation of Pancreatic Cancer: A Novel Target for Intervention. Cancers 2015, 7, 1292–1312. [Google Scholar] [CrossRef]
- Chatterjee, D.; Katz, M.H.; Rashid, A.; Wang, H.; Iuga, A.C.; Varadhachary, G.R.; Wolff, R.A.; Lee, J.E.; Pisters, P.W.; Crane, C.H.; et al. Perineural and intraneural invasion in posttherapy pancreaticoduodenectomy specimens predicts poor prognosis in patients with pancreatic ductal adenocarcinoma. Am. J. Surg. Pathol. 2012, 36, 409–417. [Google Scholar] [CrossRef] [PubMed]
- Jobling, P.; Pundavela, J.; Oliveira, S.M.; Roselli, S.; Walker, M.M.; Hondermarck, H. Nerve-Cancer Cell Cross-talk: A Novel Promoter of Tumor Progression. Cancer Res. 2015, 75, 1777–1781. [Google Scholar] [CrossRef]
- Amit, M.; Na’ara, S.; Gil, Z. Mechanisms of cancer dissemination along nerves. Nat. Rev. Cancer 2016, 16, 399–408. [Google Scholar] [CrossRef]
- Jurcak, N.R.; Rucki, A.A.; Muth, S.; Thompson, E.; Sharma, R.; Ding, D.; Zhu, Q.; Eshleman, J.R.; Anders, R.A.; Jaffee, E.M.; et al. Axon Guidance Molecules Promote Perineural Invasion and Metastasis of Orthotopic Pancreatic Tumors in Mice. Gastroenterology 2019, 157, 838–850.e6. [Google Scholar] [CrossRef]
- Gómez-Mateo Mdel, C.; Sabater-Ortí, L.; Ferrández-Izquierdo, A. Pathology handling of pancreatoduodenectomy specimens: Approaches and controversies. World J. Gastrointest. Oncol. 2014, 6, 351–359. [Google Scholar] [CrossRef]
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).