

Self-Completion Questionnaire on Sleep Evaluation in Patients Undergoing Oxaliplatin Therapy: An Observational Study

 ,
,  ,
, 
Abstract
Simple Summary
Abstract
1. Introduction
2. Materials and Methods
2.1. Patients and Inclusion Criteria
2.2. Self-Completion Questionnaire
2.3. Statistical Analysis
3. Results
3.1. Study Population
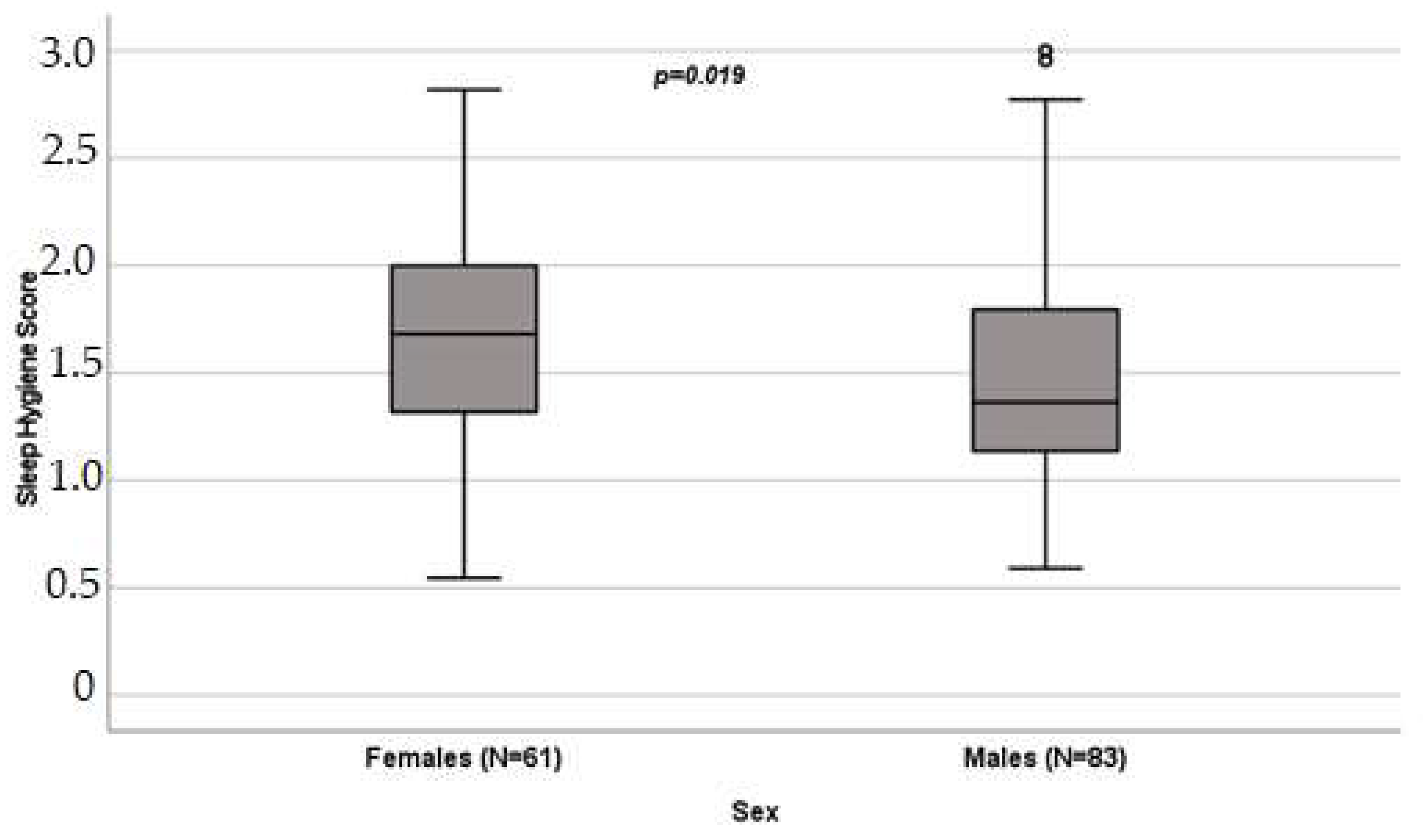
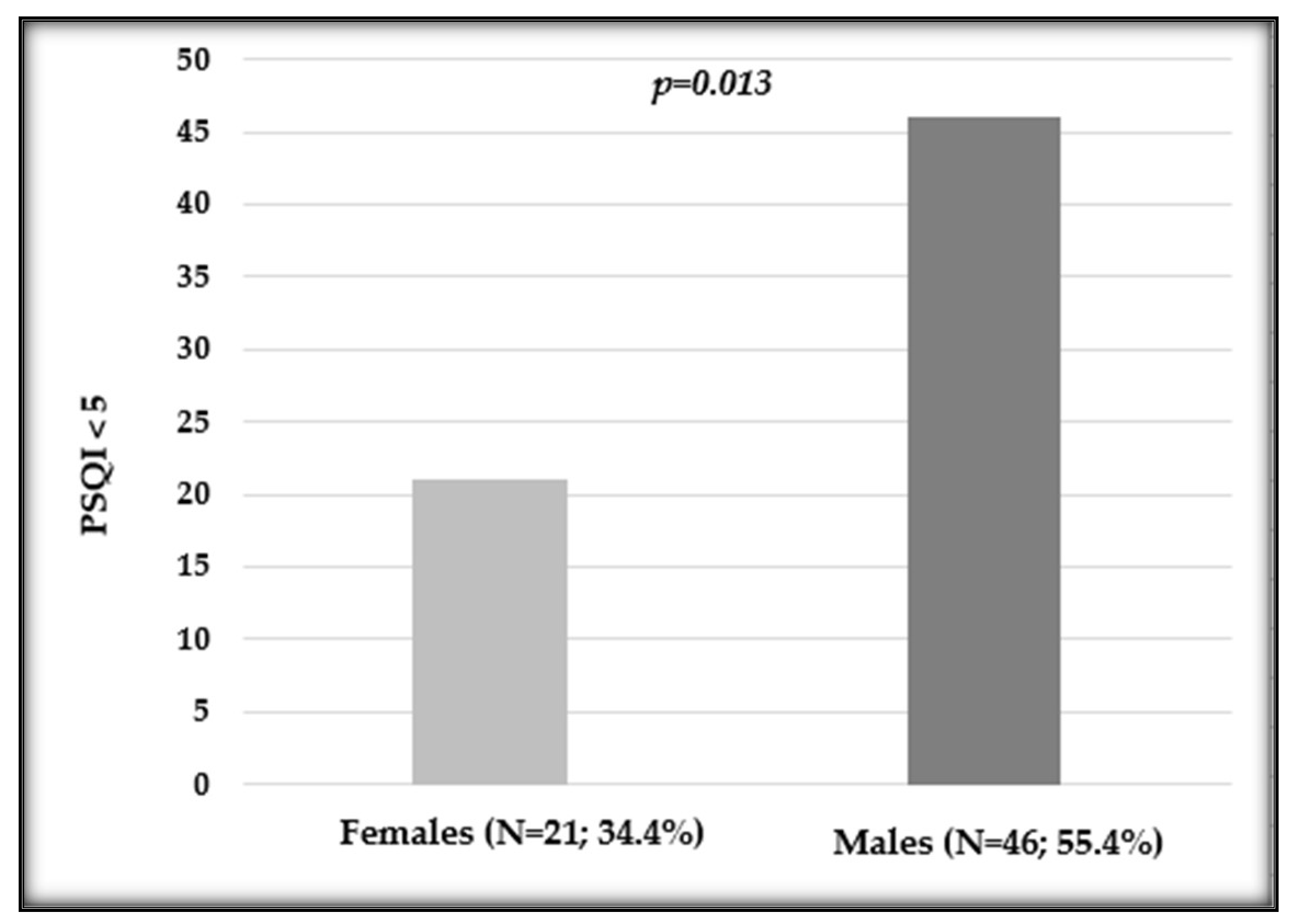
3.2. Influence of Sex on Sleep Quality
3.3. Regression Analyses
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Stewart, N.H.; Arora, V.M. Sleep in Hospitalized Older Adults. Sleep Med. Clin. 2022, 17, 223–232. [Google Scholar] [CrossRef]
- Stewart, N.H.; Arora, V.M. Sleep in Hospitalized Older Adults. Sleep Med. Clin. 2018, 13, 127–135. [Google Scholar] [CrossRef]
- Medic, G.; Wille, M.; Hemels, M.E. Short- and long-term health consequences of sleep disruption. Nat. Sci. Sleep 2017, 9, 151–161. [Google Scholar] [CrossRef] [PubMed]
- Howell, D.; Oliver, T.K.; Keller-Olaman, S.; Davidson, J.R.; Garland, S.; Samuels, C.; Savard, J.; Harris, C.; Aubin, M.; Olson, K.; et al. Sleep disturbance in adults with cancer: A systematic review of evidence for best practices in assessment and management for clinical practice. Ann. Oncol. 2014, 25, 791–800. [Google Scholar] [CrossRef] [PubMed]
- Savard, J.; Savard, M.-H. Insomnia and Cancer: Prevalence, Nature, and Nonpharmacologic Treatment. Sleep Med. Clin. 2013, 8, 373–387. [Google Scholar] [CrossRef]
- Otte, J.L.; Carpenter, J.S.; Manchanda, S.; Rand, K.L.; Skaar, T.C.; Weaver, M.; Chernyak, Y.; Zhong, X.; Igega, C.; Landis, C. Systematic review of sleep disorders in cancer patients: Can the prevalence of sleep disorders be ascertained? Cancer Med. 2015, 4, 183–200. [Google Scholar] [CrossRef] [PubMed]
- Ratcliff, C.G.; Zepeda, S.G.; Hall, M.H.; Tullos, E.A.; Fowler, S.; Chaoul, A.; Spelman, A.; Arun, B.; Cohen, L. Patient characteristics associated with sleep disturbance in breast cancer survivors. Support Care Cancer 2021, 29, 2601–2611. [Google Scholar] [CrossRef] [PubMed]
- Samuelsson, L.B.; Bovbjerg, D.H.; Roecklein, K.A.; Hall, M.H. Sleep and circadian disruption and incident breast cancer risk: An evidence-based and theoretical review. Neurosci. Biobehav. Rev. 2018, 84, 35–48. [Google Scholar] [CrossRef] [PubMed]
- Gonella, S. Sleep-wake cycle in chemotherapy patients: A retrospective study. Minerva Med. 2010, 101, 135–147. [Google Scholar]
- Innominato, P.F.; Spiegel, D.; Ulusakarya, A.; Giacchetti, S.; Bjarnason, G.A.; Lévi, F.; Palesh, O. Subjective sleep and overall survival in chemotherapy-naïve patients with metastatic colorectal cancer. Sleep Med. 2015, 16, 391–398. [Google Scholar] [CrossRef]
- Bernatchez, M.S.; Savard, J.; Ivers, H. Disruptions in sleep-wake cycles in community-dwelling cancer patients receiving palliative care and their correlates. Chronobiol. Int. 2018, 35, 49–62. [Google Scholar] [CrossRef]
- Berger, A.M.; Farr, L.A.; Kuhn, B.R.; Fischer, P.; Agrawal, S. Values of sleep/wake, activity/rest, circadian rhythms, and fatigue prior to adjuvant breast cancer chemotherapy. J. Pain Symptom Manag. 2007, 33, 398–409. [Google Scholar] [CrossRef]
- Yoshikawa, K.; Higashijima, J.; Okitsu, H.; Miyake, H.; Yagi, T.; Miura, M.; Bando, Y.; Ando, T.; Hotchi, M.; Ishikawa, M.; et al. Effects of chemotherapy on quality of life and night-time sleep of colon cancer patients. J. Med. Investig. 2020, 67, 338–342. [Google Scholar] [CrossRef]
- Herrmann, J. Adverse cardiac effects of cancer therapies: Cardiotoxicity and arrhythmia. Nat. Rev. Cardiol. 2020, 17, 474–502. [Google Scholar] [CrossRef] [PubMed]
- Zheng, P.P.; Li, J.; Kros, J.M. Breakthroughs in modern cancer therapy and elusive cardiotoxicity: Critical research-practice gaps, challenges, and insights. Med. Res. Rev. 2018, 38, 325–376. [Google Scholar] [CrossRef] [PubMed]
- Zielinski, M.R.; Gerashchenko, D.; Karpova, S.A.; Konanki, V.; McCarley, R.W.; Sutterwala, F.S.; Strecker, R.E.; Basheer, R. The NLRP3 inflammasome modulates sleep and NREM sleep delta power induced by spontaneous wakefulness, sleep deprivation and lipopolysaccharide. Brain Behav. Immun. 2017, 62, 137–150. [Google Scholar] [CrossRef] [PubMed]
- Grebe, A.; Hoss, F.; Latz, E. NLRP3 Inflammasome and the IL-1 Pathway in Atherosclerosis. Circ. Res. 2018, 122, 1722–1740. [Google Scholar] [CrossRef] [PubMed]
- Quagliariello, V.; Paccone, A.; Iovine, M.; Cavalcanti, E.; Berretta, M.; Maurea, C.; Canale, M.L.; Maurea, N. Interleukin-1 blocking agents as promising strategy for prevention of anticancer drug-induced cardiotoxicities: Possible implications in cancer patients with COVID-19. Eur. Rev. Med. Pharmacol. Sci. 2021, 25, 6797–6812. [Google Scholar] [CrossRef] [PubMed]
- Pengo, M.F.; Won, C.H.; Bourjeily, G. Sleep in Women Across the Life Span. Chest 2018, 154, 196–206. [Google Scholar] [CrossRef] [PubMed]
- Scher, N.; Guetta, L.; Draghi, C.; Yahiaoui, S.; Terzioglu, M.; Butaye, E.; Henriques, K.; Alavoine, M.; Elharar, A.; Guetta, A.; et al. Sleep Disorders and Quality of Life in Patients With Cancer: Prospective Observational Study of the Rafael Institute. JMIR Form. Res. 2022, 6, e37371. [Google Scholar] [CrossRef] [PubMed]
- Adan, A.; Fabbri, M.; Natale, V.; Prat, G. Sleep Beliefs Scale (SBS) and circadian typology. J. Sleep Res. 2006, 15, 125–132. [Google Scholar] [CrossRef]
- Curcio, G.; Tempesta, D.; Scarlata, S.; Marzano, C.; Moroni, F.; Rossini, P.M.; Ferrara, M.; De Gennaro, L. Validity of the Italian version of the Pittsburgh Sleep Quality Index (PSQI). Neurol. Sci. 2013, 34, 511–519. [Google Scholar] [CrossRef]
- Divani, A.; Heidari, M.E.; Ghavampour, N.; Parouhan, A.; Ahmadi, S.; Narimani Charan, O.; Shahsavari, H. Effect of cancer treatment on sleep quality in cancer patients: A systematic review and meta-analysis of Pittsburgh Sleep Quality Index. Support Care Cancer 2022, 30, 4687–4697. [Google Scholar] [CrossRef]
- Chen, M.L.; Yu, C.T.; Yang, C.H. Sleep disturbances and quality of life in lung cancer patients undergoing chemotherapy. Lung Cancer 2008, 62, 391–400. [Google Scholar] [CrossRef]
- Souza, R.C.D.S.; Dos Santos, M.R.; das Chagas Valota, I.A.; Sousa, C.S.; Costa Calache, A.L.S. Factors associated with sleep quality during chemotherapy: An integrative review. Nurs. Open 2020, 7, 1274–1284. [Google Scholar] [CrossRef]
- Romito, F.; Cormio, C.; De Padova, S.; Lorusso, V.; Berio, M.A.; Fimiani, F.; Piattelli, A.; Palazzo, S.; Abram, G.; Dudine, L.; et al. Patients attitudes towards sleep disturbances during chemotherapy. Eur. J. Cancer Care 2014, 23, 385–393. [Google Scholar] [CrossRef]
- Nzwalo, I.; Aboim, M.A.; Joaquim, N.; Marreiros, A.; Nzwalo, H. Systematic Review of the Prevalence, Predictors, and Treatment of Insomnia in Palliative Care. Am. J. Hosp. Palliat. Care 2020, 37, 957–969. [Google Scholar] [CrossRef] [PubMed]
- Strollo, S.E.; Fallon, E.A.; Gapstur, S.M.; Smith, T.G. Cancer-related problems, sleep quality, and sleep disturbance among long-term cancer survivors at 9-years post diagnosis. Sleep Med. 2020, 65, 177–185. [Google Scholar] [CrossRef] [PubMed]
- Innominato, P.F.; Giacchetti, S.; Bjarnason, G.A.; Focan, C.; Garufi, C.; Coudert, B.; Iacobelli, S.; Tampellini, M.; Durando, X.; Mormont, M.C.; et al. Prediction of overall survival through circadian rest-activity monitoring during chemotherapy for metastatic colorectal cancer. Int. J. Cancer 2012, 131, 2684–2692. [Google Scholar] [CrossRef] [PubMed]
- Pai, A.; Sivanandh, B.; Udupa, K. Quality of Sleep in Patients with Cancer: A Cross-sectional Observational Study. Indian J. Palliat. Care 2020, 26, 9–12. [Google Scholar] [CrossRef] [PubMed]
- Al Maqbali, M.; Al Sinani, M.; Alsayed, A.; Gleason, A.M. Prevalence of Sleep Disturbance in Patients With Cancer: A Systematic Review and Meta-Analysis. Clin. Nurs. Res. 2022, 31, 1107–1123. [Google Scholar] [CrossRef] [PubMed]
- Smagula, S.F.; Stone, K.L.; Fabio, A.; Cauley, J.A. Risk factors for sleep disturbances in older adults: Evidence from prospective studies. Sleep Med. Rev. 2016, 25, 21–30. [Google Scholar] [CrossRef] [PubMed]
- Lin, Y.; Bailey, D.E.; Docherty, S.L.; Porter, L.S.; Cooper, B.A.; Paul, S.M.; Hammer, M.J.; Conley, Y.P.; Levine, J.D.; Miaskowski, C. Distinct Sleep Disturbance Profiles in Patients With Gastrointestinal Cancers Receiving Chemotherapy. Cancer Nurs. 2022, 45, E417–E427. [Google Scholar] [CrossRef] [PubMed]
- Induru, R.R.; Walsh, D. Cancer-related insomnia. Am. J. Hosp. Palliat. Care 2014, 31, 777–785. [Google Scholar] [CrossRef]
- Endeshaw, D.; Biresaw, H.; Asefa, T.; Yesuf, N.N.; Yohannes, S. Sleep Quality and Associated Factors Among Adult Cancer Patients Under Treatment at Oncology Units in Amhara Region, Ethiopia. Nat. Sci. Sleep 2022, 14, 1049–1062. [Google Scholar] [CrossRef] [PubMed]
- Siefert, M.L.; Hong, F.; Valcarce, B.; Berry, D.L. Patient and clinician communication of self-reported insomnia during ambulatory cancer care clinic visits. Cancer Nurs. 2014, 37, E51–E59. [Google Scholar] [CrossRef] [PubMed]
- Strik, H.; Cassel, W.; Teepker, M.; Schulte, T.; Riera-Knorrenschild, J.; Koehler, U.; Seifart, U. Why Do Our Cancer Patients Sleep So Badly? Sleep Disorders in Cancer Patients: A Frequent Symptom with Multiple Causes. Oncol. Res. Treat. 2021, 44, 469–475. [Google Scholar] [CrossRef]
- Fakih, R.; Rahal, M.; Hilal, L.; Hamieh, L.; Dany, M.; Karam, S.; Shehab, L.; El Saghir, N.S.; Tfayli, A.; Salem, Z.; et al. Prevalence and Severity of Sleep Disturbances among Patients with Early Breast Cancer. Indian J. Palliat. Care 2018, 24, 35–38. [Google Scholar]
- Palesh, O.; Peppone, L.; Innominato, P.F.; Janelsins, M.; Jeong, M.; Sprod, L.; Savard, J.; Rotatori, M.; Kesler, S.; Telli, M.; et al. Prevalence, putative mechanisms, and current management of sleep problems during chemotherapy for cancer. Nat. Sci. Sleep 2012, 4, 151–162. [Google Scholar] [CrossRef]
- Bischel, L.E.; Ritchie, C.; Kober, K.M.; Paul, S.M.; Cooper, B.A.; Chen, L.M.; Levine, J.D.; Hammer, M.; Wright, F.; Miaskowski, C. Age differences in fatigue, decrements in energy, and sleep disturbance in oncology patients receiving chemotherapy. Eur. J. Oncol. Nurs. 2016, 23, 115–123. [Google Scholar] [CrossRef]
- Chen, D.; Yin, Z.; Fang, B. Measurements and status of sleep quality in patients with cancers. Support Care Cancer 2018, 26, 405–414. [Google Scholar] [CrossRef]
- Kiss, I.; Kuhn, M.; Hrusak, K.; Buchler, B.; Boublikova, L.; Buchler, T. Insomnia in patients treated with checkpoint inhibitors for cancer: A meta-analysis. Front. Oncol. 2022, 12, 946307. [Google Scholar] [CrossRef]
- Akman, T.; Yavuzsen, T.; Sevgen, Z.; Ellidokuz, H.; Yilmaz, A.U. Evaluation of sleep disorders in cancer patients based on Pittsburgh Sleep Quality Index. Eur. J. Cancer Care 2015, 24, 553–559. [Google Scholar] [CrossRef]
- Chung, K.F.; Lee, C.T.; Yeung, W.F.; Chan, M.S.; Chung, E.W.; Lin, W.L. Sleep hygiene education as a treatment of insomnia: A systematic review and meta-analysis. Fam. Pract. 2018, 35, 365–375. [Google Scholar] [CrossRef]
- Palesh, O.G.; Roscoe, J.A.; Mustian, K.M.; Roth, T.; Savard, J.; Ancoli-Israel, S.; Heckler, C.; Purnell, J.Q.; Janelsins, M.C.; Morrow, G.R. Prevalence, demographics, and psychological associations of sleep disruption in patients with cancer: University of Rochester Cancer Center-Community Clinical Oncology Program. J. Clin. Oncol. 2010, 28, 292–298. [Google Scholar] [CrossRef]
- Inhestern, L.; Beierlein, V.; Bultmann, J.C.; Möller, B.; Romer, G.; Koch, U.; Bergelt, C. Anxiety and depression in working-age cancer survivors: A register-based study. BMC Cancer 2017, 17, 347. [Google Scholar] [CrossRef]
- Walker, W.H.; Borniger, J.C. Molecular Mechanisms of Cancer-Induced Sleep Disruption. Int. J. Mol. Sci. 2019, 20, 2780. [Google Scholar] [CrossRef] [PubMed]
- Carney, C.E.; Edinger, J.D.; Kuchibhatla, M.; Lachowski, A.M.; Bogouslavsky, O.; Krystal, A.D.; Shapiro, C.M. Cognitive Behavioral Insomnia Therapy for Those With Insomnia and Depression: A Randomized Controlled Clinical Trial. Sleep 2017, 40, zsx019. [Google Scholar] [CrossRef] [PubMed]
- Kalmbach, D.A.; Cheng, P.; Arnedt, J.T.; Anderson, J.R.; Roth, T.; Fellman-Couture, C.; Williams, R.A.; Drake, C.L. Treating insomnia improves depression, maladaptive thinking, and hyperarousal in postmenopausal women: Comparing cognitive-behavioral therapy for insomnia (CBTI), sleep restriction therapy, and sleep hygiene education. Sleep Med. 2019, 55, 124–134. [Google Scholar] [CrossRef] [PubMed]
- Mansano-Schlosser, T.C.; Ceolim, M.F. Factors associated with sleep quality in the elderly receiving chemotherapy. Rev. Lat. Am. Enfermagem. 2012, 20, 1100–1108. [Google Scholar] [CrossRef] [PubMed]
- Dahiya, S.; Ahluwalia, M.S.; Walia, H.K. Sleep disturbances in cancer patients: Underrecognized and undertreated. Cleve Clin. J. Med. 2013, 80, 722–732. [Google Scholar] [CrossRef]
- Mercadante, S.; Adile, C.; Ferrera, P.; Masedu, F.; Valenti, M.; Aielli, F. Sleep disturbances in advanced cancer patients admitted to a supportive/palliative care unit. Support Care Cancer 2017, 25, 1301–1306. [Google Scholar] [CrossRef]
- Wu, I.H.C.; Balachandran, D.D.; Faiz, S.A.; Bashoura, L.; Escalante, C.P.; Manzullo, E.F. Characteristics of Cancer-Related Fatigue and Concomitant Sleep Disturbance in Cancer Patients. J. Pain Symptom Manag. 2022, 63, e1–e8. [Google Scholar] [CrossRef]
- Panossian, A. Challenges in phytotherapy research. Front. Pharmacol. 2023, 14, 1199516. [Google Scholar] [CrossRef] [PubMed]
- Barnes, J. Quality, efficacy and safety of complementary medicines: Fashions, facts and the future. Part I. Regulation and quality. Br. J. Clin. Pharmacol. 2003, 55, 226–233. [Google Scholar] [CrossRef]
- Seyed Hashemi, M.; Namiranian, N.; Tavahen, H.; Dehghanpour, A.; Rad, M.H.; Jam-Ashkezari, S.; Emtiazy, M.; Hashempur, M.H. Efficacy of Pomegranate Seed Powder on Glucose and Lipid Metabolism in Patients with Type 2 Diabetes: A Prospective Randomized Double-Blind Placebo-Controlled Clinical Trial. Complement. Med. Res. 2021, 28, 226–233. [Google Scholar] [CrossRef] [PubMed]
- Nayebi, N.; Esteghamati, A.; Meysamie, A.; Khalili, N.; Kamalinejad, M.; Emtiazy, M.; Hashempur, M.H. The effects of a Melissa officinalis L. based product on metabolic parameters in patients with type 2 diabetes mellitus: A randomized double-blinded controlled clinical trial. J. Complement. Integr. Med. 2019, 16, 20180088. [Google Scholar] [CrossRef]
- Guadagna, S.; Barattini, D.F.; Rosu, S.; Ferini-Strambi, L. Plant Extracts for Sleep Disturbances: A Systematic Review. Evid. Based Complement. Alternat. Med. 2020, 2020, 3792390. [Google Scholar] [CrossRef]
- Alem, L.; Ansari, H.; Hajigholami, A. Evaluation of Sleep Training Effectiveness on the Quality of Sleep in Cancer Patients during Chemotherapy. Adv. Biomed. Res. 2021, 10, 11. [Google Scholar] [CrossRef] [PubMed]
- Vena, C.; Parker, K.; Cunningham, M.; Clark, J.; McMillan, S. Sleep-wake disturbances in people with cancer part I: An overview of sleep, sleep regulation, and effects of disease and treatment. Oncol. Nurs. Forum. 2004, 31, 735–746. [Google Scholar] [CrossRef]
- Matthews, E.E.; Wang, S.Y. Cancer-Related Sleep Wake Disturbances. Semin Oncol. Nurs. 2022, 38, 151253. [Google Scholar] [CrossRef] [PubMed]
- Moy, S.; Kober, K.M.; Viele, C.; Paul, S.M.; Hammer, M.; Melisko, M.; Wright, F.; Conley, Y.P.; Levine, J.D.; Miaskowski, C. Level of Exercise Influences the Severity of Fatigue, Energy Levels, and Sleep Disturbance in Oncology Outpatients Receiving Chemotherapy. Cancer Nurs. 2022, 45, 3–11. [Google Scholar] [CrossRef] [PubMed]
- Fang, Y.Y.; Hung, C.T.; Chan, J.C.; Huang, S.M.; Lee, Y.H. Meta-analysis: Exercise intervention for sleep problems in cancer patients. Eur. J. Cancer Care 2019, 28, e13131. [Google Scholar] [CrossRef] [PubMed]






{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Variable | All (n = 144) | Males (n = 83) | Females (n = 61) |
|---|---|---|---|
| Age (years) | |||
| Median (IQR) | 62 (54–68) | 62 (56–68) | 59 (52–67.5) |
| Sleep Hygiene score | |||
| Median (IQR) | 1.5 (1.18–1.90) | 1.36 (1.13–1.81) | 1.68 (1.31–2) |
| Pittsburgh Sleep Quality Index (PSQI) | |||
| Median (IQR) | 6 (4–9) | 5 (4–8) | 6 (4–10) |
| PSQI ≤ 5 (percentage, frequency) | 67, 46.5% | 46, 55.4% | 21, 34.4% |
| PSQI > 5 (percentage, frequency) | 77, 53.5% | 37, 44.6% | 40, 65.6% |
| Variable | All (n = 144) | Males (n = 83) | Females (n = 61) |
|---|---|---|---|
| Highest level of education (Frequency, Percentage) | |||
| Primary School Diploma | 4, 2.8% | 3, 3.6% | 1, 1.6% |
| Middle School Diploma | 49, 34% | 29, 34.9% | 20, 32.8% |
| High School Diploma | 62, 43.1% | 36, 43.3% | 26, 42.6% |
| Degree | 28, 19.4% | 14, 16.9% | 14, 23% |
| Marital Status (Frequency, Percentage) | |||
| Married—Cohabiting | 106, 73.6% | 64, 77.1% | 42, 68.9% |
| Separated—Divorced | 17, 11.8% | 10, 12% | 7, 11.5% |
| Unmarried Maiden | 12, 8.3% | 7, 8.4% | 5, 8.3% |
| Widow | 8, 5.6% | 1, 1.2% | 7, 11.5% |
| Tumor Localization (Frequency, Percentage) | |||
| Lungs | 6, 4.2% | 4, 4.8% | 2, 3.3% |
| Intestine | 92, 63.9% | 51, 61.4% | 41, 67.2% |
| Stomach, Esophagus | 27, 18.8% | 19, 22.9% | 8, 13.1% |
| Liver And Biliary Tract | 5, 3.5% | 2, 2.4% | 3, 4.9% |
| Pancreas | 13, 9% | 8, 9.6% | 5, 8.2% |
| Genitourinary Tract | 1, 0.7% | 0 | 1, 1.6% |
| Chemotherapy Administration (Frequency, Percentage) | |||
| Intravenous | 144, 100% | 83, 100% | 61, 100% |
| Oral | 23, 16% | 15, 18.1% | 8, 13.1% |
| Central Venous Catheter (Frequency, Percentage) | |||
| Present | 143, 99.1% | 82, 98.8% | 61, 100% |
| Stoma (Frequency, Percentage) | |||
| Present | 16, 11.1% | 11, 13.3% | 5, 8.2% |
| Nutrition (Frequency, Percentage) | |||
| Oral | 141, 97.9% | 80, 96.4% | 59, 96.7% |
| Parenteral | 3, 2.1% | 2, 2.4% | 1, 1.6% |
| Pain Sensation (Frequency, Percentage) | |||
| Present | 32, 22.2% | 15, 18.1% | 17, 27.9% |
| Pain Relievers (Frequency, Percentage) | |||
| Paracetamol | 20, 13.9% | 10, 12% | 10, 6.4% |
| Non-Steroidal Anti-Inflammatories | 4, 2.8% | 2, 2.4% | 2, 3.3% |
| Opioids | 11, 7.6% | 6, 7.2% | 5, 8.2% |
| Concomitant Pathologies (Frequency, Percentage) | |||
| Cardiovascular Diseases | 48, 33.3% | 27, 32.5% | 21, 34.4% |
| Diabetes | 15, 10.4% | 12, 14.5% | 3, 4.9% |
| Endocrine Disorders | 9, 6.3% | 2, 2.4% | 7, 11.5% |
| Psychiatric Disorders | 6, 4.2% | 2, 2.4% | 4, 6.6% |
| Arthritis, Arthrosis, Osteoporosis, Rheumatic Disorders | 4, 2.8% | 1, 1.2% | 3, 4.9% |
| Gastric Disorders | 3, 2.1% | 1, 1.2% | 2, 3.3% |
| Intestinal Disorders | 1, 0.7% | 1, 1.1% | 0 |
| Genitourinary Disorders | 2, 1.4% | 2, 2.4% | 0 |
| Neurological Disorders | 3, 2.1% | 3, 3.6% | 0 |
| Respiratory Disorders | 0 | 0 | 0 |
| Concomitant Therapies (Frequency, Percentage) | |||
| Corticosteroids | 68, 47.2% | 32, 38.6% | 36, 59% |
| Antiemetics | 67, 46.5% | 35, 42.2% | 32, 52.5% |
| Drugs for Cardiovascular Diseases | 56, 38.9% | 36, 43.4% | 20, 32.8% |
| Antidepressants | 7, 4.9% | 2, 2.4% | 5, 8.2% |
| Benzodiazepines | 7, 4.9% | 4, 4.8% | 3, 4.9% |
| Drugs for Thyroid Diseases | 9, 6.3% | 2, 2.4% | 7, 11.5% |
| Insulin And Oral Hypoglycemics | 13, 9% | 10, 12% | 3, 4.9% |
| Antihistamines | 8, 5.6% | 6, 7.2% | 2, 3.3% |
| Antipsychotics/Mood Stabilizers | 0 | 0 | 0 |
| Antiepileptics/Anticonvulsants | 1, 0.7% | 1, 1.2% | 0 |
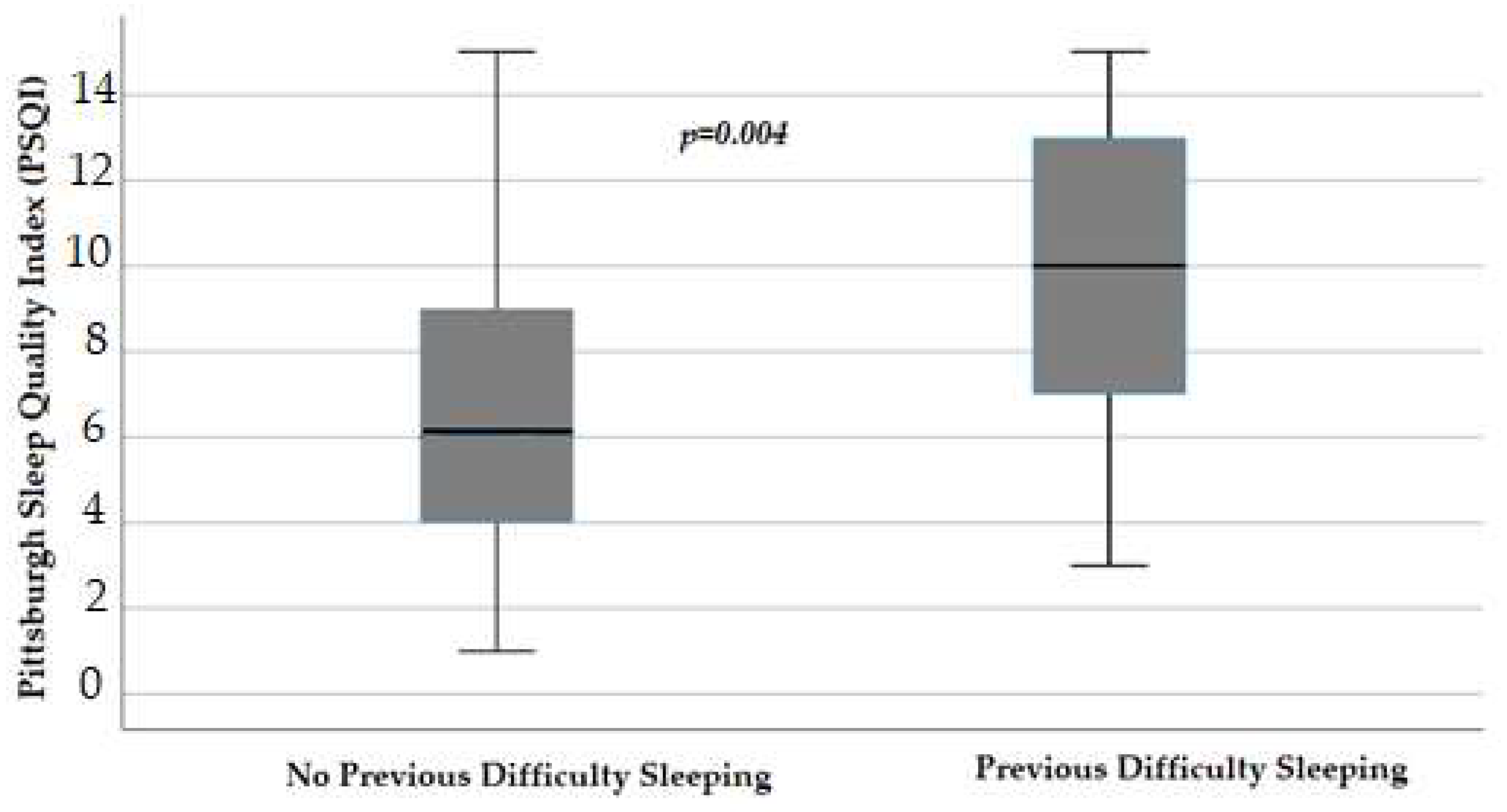
| Previous Difficulty Sleeping (Frequency, Percentage) | |||
| Yes | 23, 16% | 8, 9.6% | 15, 24.6% |
| Treatment for Difficulty Sleeping (Frequency, Percentage) | |||
| Phytotherapeutics | 2, 1.4% | 1, 1.2% | 1, 1.6% |
| Melatonin | 1, 0.7% | 0 | 1, 1.6% |
| Chamomile and Herbal Teas | 4, 2.8% | 3, 3.6% | 1, 1.6% |
| Drugs | 10, 6.9% | 3, 3.6% | 7, 11.5% |
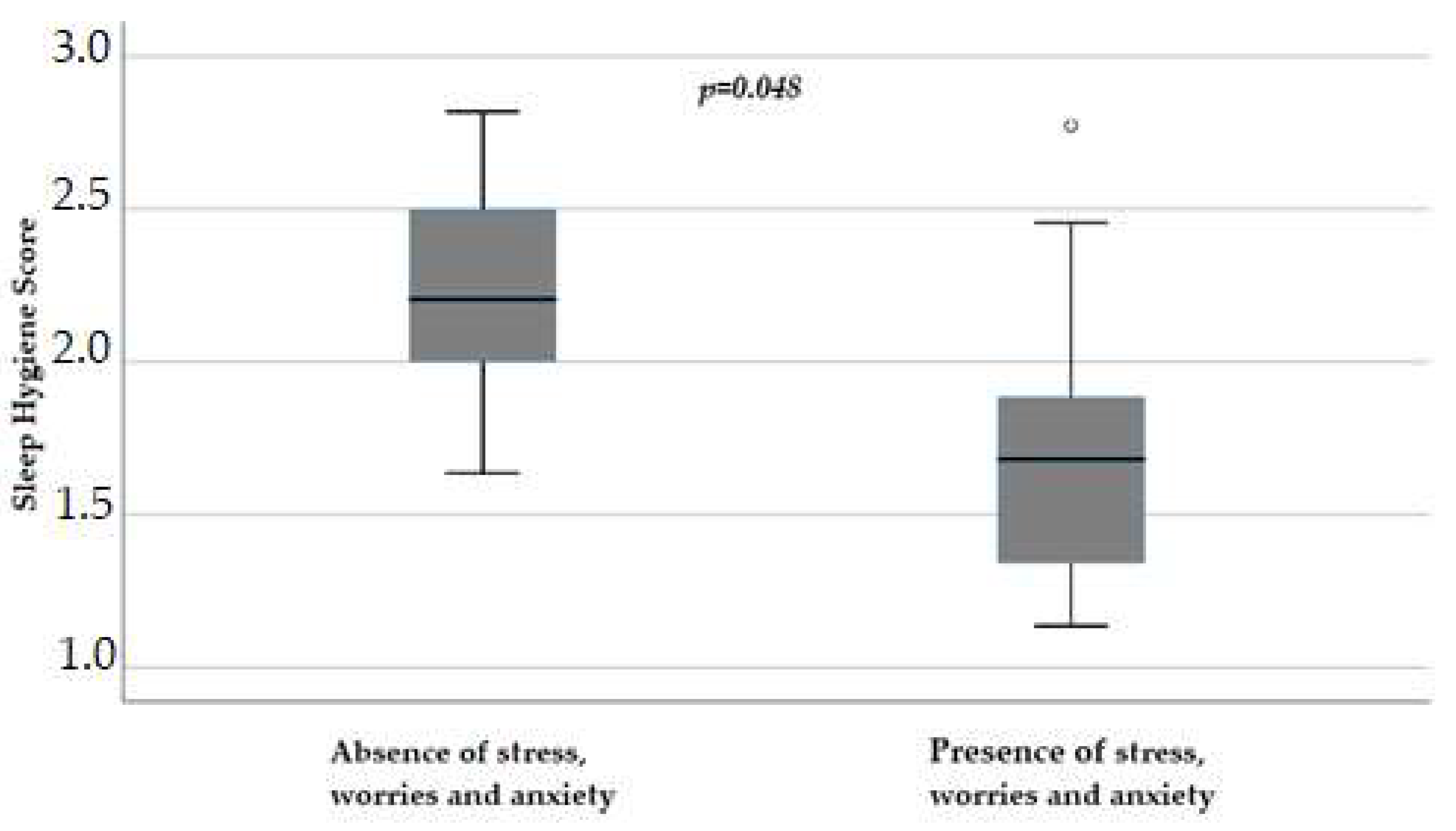
| Stress/Worries/Anxiety (Frequency, Percentage) | |||
| Yes | 18, 12.5% | 11, 13.25% | 7, 11.48% |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Mussa, M.V.; Allegra, S.; Armando, T.; Storto, S.; Ghezzo, B.; Soave, G.; Abbadessa, G.; Chiara, F.; Di Maio, M.; Dagnoni, F.M.; et al. Self-Completion Questionnaire on Sleep Evaluation in Patients Undergoing Oxaliplatin Therapy: An Observational Study. Cancers 2024, 16, 946. https://doi.org/10.3390/cancers16050946
Mussa MV, Allegra S, Armando T, Storto S, Ghezzo B, Soave G, Abbadessa G, Chiara F, Di Maio M, Dagnoni FM, et al. Self-Completion Questionnaire on Sleep Evaluation in Patients Undergoing Oxaliplatin Therapy: An Observational Study. Cancers. 2024; 16(5):946. https://doi.org/10.3390/cancers16050946
Chicago/Turabian StyleMussa, Maria Valentina, Sarah Allegra, Tiziana Armando, Silvana Storto, Beatrice Ghezzo, Giulia Soave, Giuliana Abbadessa, Francesco Chiara, Massimo Di Maio, Fiammetta Maria Dagnoni, and et al. 2024. "Self-Completion Questionnaire on Sleep Evaluation in Patients Undergoing Oxaliplatin Therapy: An Observational Study" Cancers 16, no. 5: 946. https://doi.org/10.3390/cancers16050946
APA StyleMussa, M. V., Allegra, S., Armando, T., Storto, S., Ghezzo, B., Soave, G., Abbadessa, G., Chiara, F., Di Maio, M., Dagnoni, F. M., & De Francia, S. (2024). Self-Completion Questionnaire on Sleep Evaluation in Patients Undergoing Oxaliplatin Therapy: An Observational Study. Cancers, 16(5), 946. https://doi.org/10.3390/cancers16050946