
A Systematic Review on Artificial Intelligence Evaluating Metastatic Prostatic Cancer and Lymph Nodes on PSMA PET Scans


Abstract
Simple Summary
Abstract
1. Introduction
2. Materials and Methods
2.1. Literature Search Strategy
2.2. Eligibility Criteria
2.3. Screening and Study Selection
2.4. Quality and Risk of Bias Assessment
3. Results
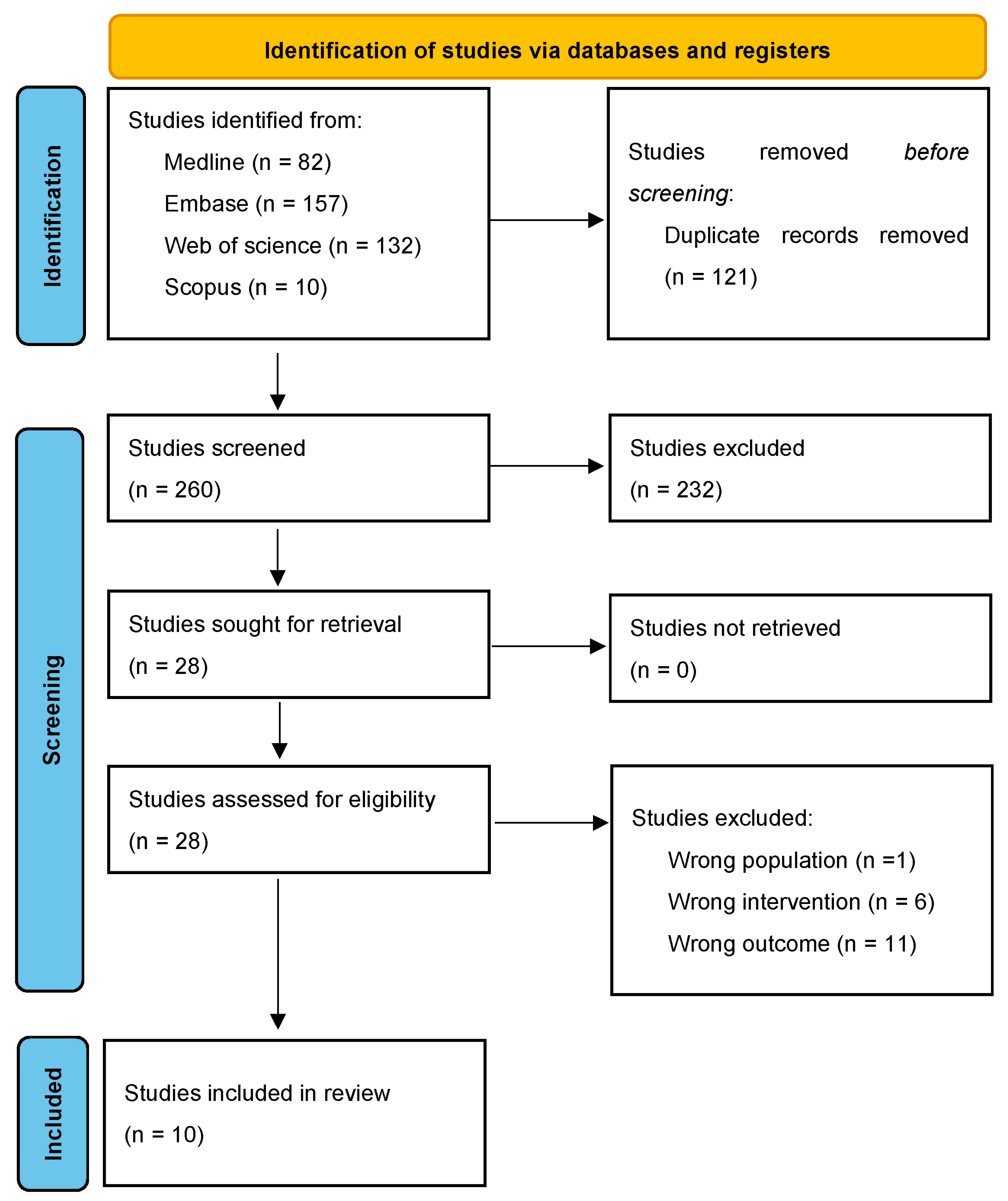
3.1. Screening Process
3.2. Characteristics of Included Studies
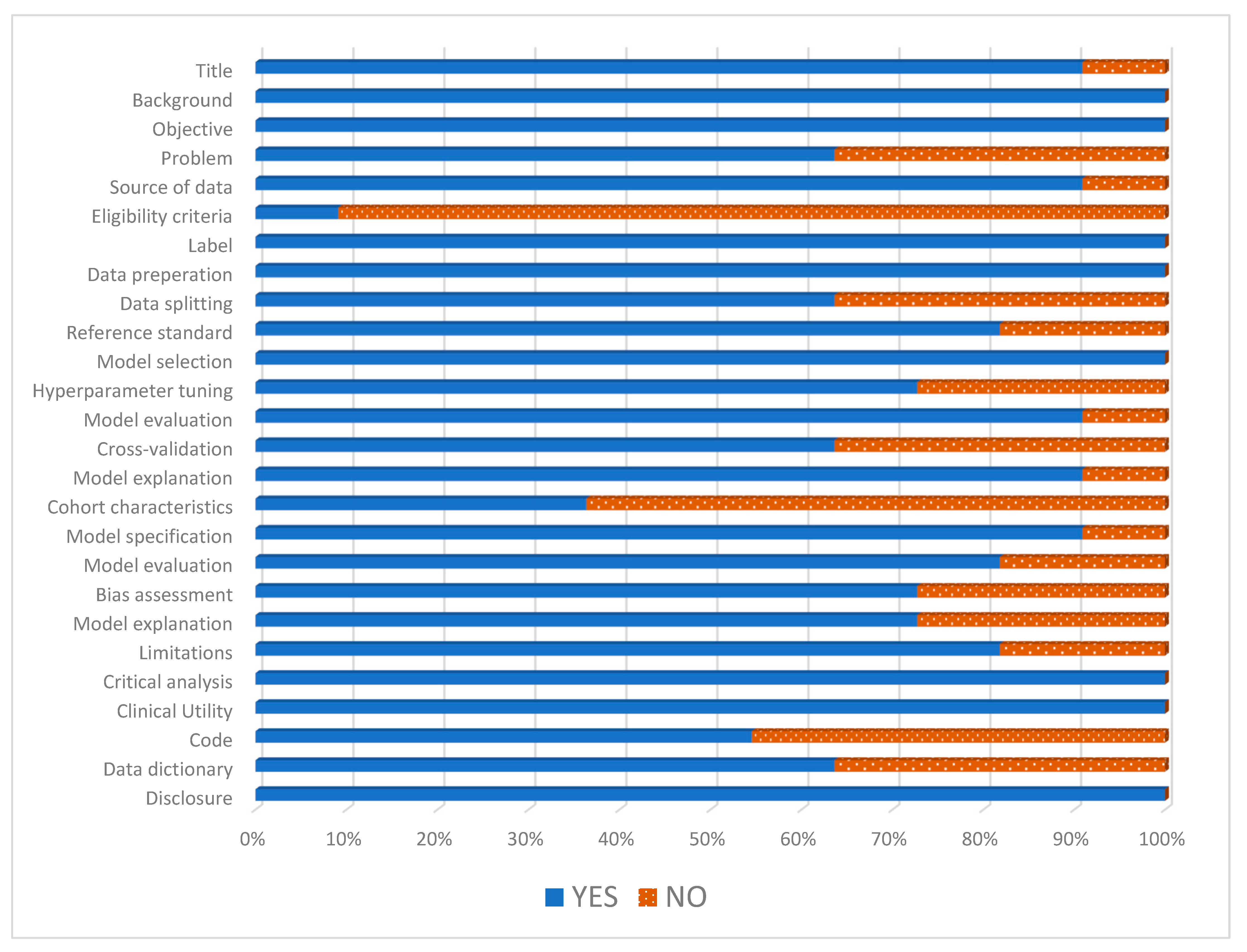
3.3. Quality and Risk of Bias Assessment of Included Studies
3.4. AI’s Ability to Standardise Staging of PCa on PSMA PET Scans
3.5. AI’s Role in Diagnosing Metastasis Disease on PSMA Pet Scans
3.6. AI’s Role in Diagnosing Lymph Node Involvement on PSMA PET Scans
3.7. Estimating Tumour Burden and Prognosis
3.8. Assessing Treatment Response based on PSMA PET Scans
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Conflicts of Interest
References
- National Cancer Institute. Surveillance, Epidemoiology, and End Results Program (SEER). Cancer Stat Facts: Prostate Cancer. Available online: https://seer.cancer.gov/statfacts/html/prost.html (accessed on 20 December 2023).
- Cancer Australia: Prostate Cancer in Australia Statistics. Available online: https://www.canceraustralia.gov.au/cancer-types/prostate-cancer/statistics (accessed on 20 December 2023).
- Sung, H.; Ferlay, J.; Siegel, R.L.; Laversanne, M.; Soerjomataram, I.; Jemal, A.; Bray, F. Global cancer statistics 2020: Globocan estimates of incidence and mortality worldwide for 36 cancers in 185 countries. CA Cancer J. Clin. 2021, 71, 209–249. [Google Scholar] [CrossRef] [PubMed]
- Nafissi, N.N.; Kosiorek, H.E.; Butterfield, R.J.; Moore, C.; Ho, T.; Singh, P.; Bryce, A.H. Evolving natural history of metastatic prostate cancer. Cureus 2020, 12, e11484. [Google Scholar] [CrossRef] [PubMed]
- Kunath, F.; Jensen, K.; Pinart, M.; Kahlmeyer, A.; Schmidt, S.; Price, C.L.; Lieb, V.; Dahm, P. Early versus deferred standard androgen suppression therapy for advanced hormone-sensitive prostate cancer. Cochrane Database Syst. Rev. 2019, 6, Cd003506. [Google Scholar] [CrossRef] [PubMed]
- Ross, J.S.; Sheehan, C.E.; Fisher, H.A.; Kaufman, R.P., Jr.; Kaur, P.; Gray, K.; Webb, I.; Gray, G.S.; Mosher, R.; Kallakury, B.V. Correlation of primary tumor prostate-specific membrane antigen expression with disease recurrence in prostate cancer. Clin. Cancer Res. 2003, 9, 6357–6362. [Google Scholar] [PubMed]
- U.S. Food and Drug Administration. FDA Approves First PSMA-Targeted Pet Imaging Drug for Men with Prostate Cancer. Available online: https://www.fda.gov/news-events/press-announcements/fda-approves-first-psma-targeted-pet-imaging-drug-men-prostate-cancer (accessed on 12 December 2023).
- U.S. Food and Drug Administration. FDA Approves Second PSMA-Targeted Pet Imaging Drug for Men with Prostate Cancer. Available online: https://www.fda.gov/drugs/news-events-human-drugs/fda-approves-second-psma-targeted-pet-imaging-drug-men-prostate-cancer (accessed on 12 December 2023).
- Hofman, M.S.; Lawrentschuk, N.; Francis, R.J.; Tang, C.; Vela, I.; Thomas, P.; Rutherford, N.; Martin, J.M.; Frydenberg, M.; Shakher, R.; et al. Prostate-specific membrane antigen pet-ct in patients with high-risk prostate cancer before curative-intent surgery or radiotherapy (propsma): A prospective, randomised, multicentre study. Lancet 2020, 395, 1208–1216. [Google Scholar] [CrossRef] [PubMed]
- Zhou, J.; Wu, R.; Wang, W.; Zhao, Y.; Liu, X. (68)ga-psma pet/ct for the evaluation of metastasis in patients with prostate cancer: A systematic review and meta-analysis. Hell. J. Nucl. Med. 2022, 25, 297–311. [Google Scholar] [PubMed]
- Fanti, S.; Minozzi, S.; Morigi, J.J.; Giesel, F.; Ceci, F.; Uprimny, C.; Hofman, M.S.; Eiber, M.; Schwarzenbock, S.; Castellucci, P.; et al. Development of standardized image interpretation for 68ga-psma pet/ct to detect prostate cancer recurrent lesions. Eur. J. Nucl. Med. Mol. Imaging 2017, 44, 1622–1635. [Google Scholar] [CrossRef]
- Toriihara, A.; Nobashi, T.; Baratto, L.; Duan, H.; Moradi, F.; Park, S.; Hatami, N.; Aparici, C.M.; Davidzon, G.; Iagaru, A. Comparison of 3 interpretation criteria for (68)ga-psma11 pet based on inter- and intrareader agreement. J. Nucl. Med. 2020, 61, 533–539. [Google Scholar] [CrossRef]
- Zheng, X.; He, B.; Hu, Y.; Ren, M.; Chen, Z.; Zhang, Z.; Ma, J.; Ouyang, L.; Chu, H.; Gao, H.; et al. Diagnostic accuracy of deep learning and radiomics in lung cancer staging: A systematic review and meta-analysis. Front. Public Health 2022, 10, 938113. [Google Scholar] [CrossRef]
- Bedrikovetski, S.; Dudi-Venkata, N.N.; Kroon, H.M.; Seow, W.; Vather, R.; Carneiro, G.; Moore, J.W.; Sammour, T. Artificial intelligence for pre-operative lymph node staging in colorectal cancer: A systematic review and meta-analysis. BMC Cancer 2021, 21, 1058. [Google Scholar] [CrossRef]
- Eiber, M.; Herrmann, K.; Calais, J.; Hadaschik, B.; Giesel, F.L.; Hartenbach, M.; Hope, T.; Reiter, R.; Maurer, T.; Weber, W.A.; et al. Prostate cancer molecular imaging standardized evaluation (promise): Proposed mitnm classification for the interpretation of psma-ligand pet/ct. J. Nucl. Med. 2018, 59, 469–478. [Google Scholar] [CrossRef]
- U.S. Food and Drug Administration. Artificial Intelligence and Machine Learning (Ai/Ml)-Enabled Medical Devices. Available online: https://www.fda.gov/medical-devices/software-medical-device-samd/artificial-intelligence-and-machine-learning-aiml-enabled-medical-devices (accessed on 12 December 2023).
- Lindgren Belal, S.; Frantz, S.; Minarik, D.; Enqvist, O.; Wikström, E.; Edenbrandt, L.; Trägårdh, E. Applications of artificial intelligence in psma pet/ct for prostate cancer imaging. Semin. Nucl. Med. 2024, 54, 141–149. [Google Scholar] [CrossRef] [PubMed]
- Baştanlar, Y.; Ozuysal, M. Introduction to machine learning. Methods Mol. Biol. 2014, 1107, 105–128. [Google Scholar] [PubMed]
- LeCun, Y.; Bengio, Y.; Hinton, G. Deep learning. Nature 2015, 521, 436–444. [Google Scholar] [CrossRef] [PubMed]
- Manimegalai, P.; Suresh Kumar, R.; Valsalan, P.; Dhanagopal, R.; Vasanth Raj, P.T.; Christhudass, J. 3d convolutional neural network framework with deep learning for nuclear medicine. Scanning 2022, 2022, 9640177. [Google Scholar] [CrossRef] [PubMed]
- Brierley, J.D.; Gospodarowicz, M.K.; Wittekind, C. Tnm Classification of Malignant Tumours, 8th ed.; John Wiley & Sons, Incorporated: Chicester, UK, 2017. [Google Scholar]
- Kwong, J.C.C.; McLoughlin, L.C.; Haider, M.; Goldenberg, M.G.; Erdman, L.; Rickard, M.; Lorenzo, A.J.; Hung, A.J.; Farcas, M.; Goldenberg, L.; et al. Standardized reporting of machine learning applications in urology: The stream-uro framework. Eur. Urol. Focus 2021, 7, 672–682. [Google Scholar] [CrossRef] [PubMed]
- Wolff, R.F.; Moons, K.G.M.; Riley, R.D.; Whiting, P.F.; Westwood, M.; Collins, G.S.; Reitsma, J.B.; Kleijnen, J.; Mallett, S. Probast: A tool to assess the risk of bias and applicability of prediction model studies. Ann. Intern. Med. 2019, 170, 51–58. [Google Scholar] [CrossRef] [PubMed]
- Nickols, N.; Anand, A.; Johnsson, K.; Brynolfsson, J.; Borreli, P.; Parikh, N.; Juarez, J.; Jafari, L.; Eiber, M.; Rettig, M. Apromise: A novel automated promise platform to standardize evaluation of tumor burden in (18)f-dcfpyl images of veterans with prostate cancer. J. Nucl. Med. 2022, 63, 233–239. [Google Scholar] [CrossRef]
- Kendrick, J.; Francis, R.J.; Hassan, G.M.; Rowshanfarzad, P.; Ong, J.S.L.; Ebert, M.A. Fully automatic prognostic biomarker extraction from metastatic prostate lesion segmentations in whole-body [(68)ga]ga-psma-11 pet/ct images. Eur. J. Nucl. Med. Mol. Imaging 2022, 50, 67–79. [Google Scholar] [CrossRef]
- Moazemi, S.; Erle, A.; Khurshid, Z.; Lütje, S.; Muders, M.; Essler, M.; Schultz, T.; Bundschuh, R.A. Decision-support for treatment with (177)lu-psma: Machine learning predicts response with high accuracy based on psma-pet/ct and clinical parameters. Ann. Transl. Med. 2021, 9, 818. [Google Scholar] [CrossRef]
- Johnsson, K.; Brynolfsson, J.; Sahlstedt, H.; Nickols, N.G.; Rettig, M.; Probst, S.; Morris, M.J.; Bjartell, A.; Eiber, M.; Anand, A. Analytical performance of apromise: Automated anatomic contextualization, detection, and quantification of [(18)f]dcfpyl (psma) imaging for standardized reporting. Eur. J. Nucl. Med. Mol. Imaging 2022, 49, 1041–1051. [Google Scholar] [CrossRef] [PubMed]
- Leung, K.H.; Rowe, S.P.; Leal, J.P.; Ashrafinia, S.; Sadaghiani, M.S.; Chung, H.W.; Dalaie, P.; Tulbah, R.; Yin, Y.; VanDenBerg, R.; et al. Deep learning and radiomics framework for psma-rads classification of prostate cancer on psma pet. EJNMMI Res. 2022, 12, 76. [Google Scholar] [CrossRef] [PubMed]
- Trägårdh, E.; Enqvist, O.; Ulén, J.; Jögi, J.; Bitzén, U.; Hedeer, F.; Valind, K.; Garpered, S.; Hvittfeldt, E.; Borrelli, P.; et al. Freely available, fully automated ai-based analysis of primary tumour and metastases of prostate cancer in whole-body [(18)f]-psma-1007 pet-ct. Diagnostics 2022, 12, 2101. [Google Scholar] [CrossRef] [PubMed]
- Capobianco, N.; Sibille, L.; Chantadisai, M.; Gafita, A.; Langbein, T.; Platsch, G.; Solari, E.L.; Shah, V.; Spottiswoode, B.; Eiber, M.; et al. Whole-body uptake classification and prostate cancer staging in (68)ga-psma-11 pet/ct using dual-tracer learning. Eur. J. Nucl. Med. Mol. Imaging 2022, 49, 517–526. [Google Scholar] [CrossRef] [PubMed]
- Erle, A.; Moazemi, S.; Lütje, S.; Essler, M.; Schultz, T.; Bundschuh, R.A. Evaluating a machine learning tool for the classification of pathological uptake in whole-body psma-pet-ct scans. Tomography 2021, 7, 301–312. [Google Scholar] [CrossRef] [PubMed]
- Moazemi, S.; Khurshid, Z.; Erle, A.; Lütje, S.; Essler, M.; Schultz, T.; Bundschuh, R.A. Machine learning facilitates hotspot classification in psma-pet/ct with nuclear medicine specialist accuracy. Diagnostics 2020, 10, 622. [Google Scholar] [CrossRef] [PubMed]
- Acar, E.; Leblebici, A.; Ellidokuz, B.E.; Başbınar, Y.; Kaya, G. Machine learning for differentiating metastatic and completely responded sclerotic bone lesion in prostate cancer: A retrospective radiomics study. Br. J. Radiol. 2019, 92, 20190286. [Google Scholar] [CrossRef]
- Duriseti, S.; Berenji, G.; Tsai, S.; Rettig, M.; Nickols, N.G. Quantitative assessment of psma pet response to therapy in castration-sensitive prostate cancer using an automated imaging platform for disease identification and measurement. Eur. J. Hybrid Imaging 2023, 7, 7. [Google Scholar] [CrossRef]
- Rowe, S.P.; Pienta, K.J.; Pomper, M.G.; Gorin, M.A. Psma-rads version 1.0: A step towards standardizing the interpretation and reporting of psma-targeted pet imaging studies. Eur. Urol. 2018, 73, 485–487. [Google Scholar] [CrossRef]
- Nobel, J.M.; Kok, E.M.; Robben, S.G.F. Redefining the structure of structured reporting in radiology. Insights Imaging 2020, 11, 10. [Google Scholar] [CrossRef]
- Miller, D.D.; Brown, E.W. Artificial intelligence in medical practice: The question to the answer? Am. J. Med. 2018, 131, 129–133. [Google Scholar] [CrossRef] [PubMed]
- Poon, A.I.F.; Sung, J.J.Y. Opening the black box of ai-medicine. J. Gastroenterol. Hepatol. 2021, 36, 581–584. [Google Scholar] [CrossRef] [PubMed]
- von Eyben, F.E.; Picchio, M.; von Eyben, R.; Rhee, H.; Bauman, G. 68ga-labeled prostate-specific membrane antigen ligand positron emission tomography/computed tomography for prostate cancer: A systematic review and meta-analysis. Eur. Urol. Focus 2018, 4, 686–693. [Google Scholar] [CrossRef] [PubMed]
- Nensa, F.; Demircioglu, A.; Rischpler, C. Artificial intelligence in nuclear medicine. J. Nucl. Med. 2019, 60, 29s–37s. [Google Scholar] [CrossRef] [PubMed]
- Hvittfeldt, E.; Bitzén, U.; Minarik, D.; Oddstig, J.; Olsson, B.; Trägårdh, E. Pet/ct imaging 2 h after injection of [18f]psma-1007 can lead to higher staging of prostate cancer than imaging after 1 h. Eur. J. Hybrid Imaging 2023, 7, 9. [Google Scholar] [CrossRef] [PubMed]
- Huang, S.; Ong, S.; McKenzie, D.; Mirabelli, A.; Chen, D.C.; Chengodu, T.; Murphy, D.G.; Hofman, M.S.; Lawrentschuk, N.; Perera, M. Comparison of 18f-based psma radiotracers with [68ga]ga-psma-11 in pet/ct imaging of prostate cancer—A systematic review and meta-analysis. Prostate Cancer Prostatic Dis. 2023, 1–11. [Google Scholar] [CrossRef]
- Sweeney, C.J.; Chen, Y.-H.; Carducci, M.; Liu, G.; Jarrard, D.F.; Eisenberger, M.; Wong, Y.-N.; Hahn, N.; Kohli, M.; Cooney, M.M.; et al. Chemohormonal therapy in metastatic hormone-sensitive prostate cancer. N. Engl. J. Med. 2015, 373, 737–746. [Google Scholar] [CrossRef]
- Juan, G.R.; Laura, F.H.; Javier, P.V.; Natalia, V.C.; Mᵃ Isabel, G.R.; Enrique, R.G.; José Luis, S.P.; Pablo, A.L.; Noelia, S.S.; Roser, V.D.; et al. Where do we stand in the management of oligometastatic prostate cancer? A comprehensive review. Cancers 2022, 14, 2017. [Google Scholar] [CrossRef]
- Beegle, C.; Hasani, N.; Maass-Moreno, R.; Saboury, B.; Siegel, E. Artificial intelligence and positron emission tomography imaging workflow:: Technologists’ perspective. PET Clin. 2022, 17, 31–39. [Google Scholar] [CrossRef]
- Xue, S.; Gafita, A.; Afshar-Oromieh, A.; Eiber, M.; Rominger, A.; Shi, K. Voxel-wise prediction of post-therapy dosimetry for 177Lu-PSMA I&T therapy using deep learning. J. Nucl. Med. 2020, 61, 1424. [Google Scholar]
- Xue, S.; Gafita, A.; Afshar-Oromieh, A.; Eiber, M.; Rominger, A.; Shi, K. Organ-regularized Deep Learning for Voxel-wise Prediction of Post-therapy Dosimetry for 177Lu PSMA Therapy. J. Nucl. Med. 2023, 64, 836. [Google Scholar]
- Page, M.J.; McKenzie, J.E.; Bossuyt, P.M.; Boutron, I.; Hoffmann, T.C.; Mulrow, C.D.; Shamseer, L.; Tetzlaff, J.M.; Akl, E.A.; Brennan, S.E.; et al. The PRISMA 2020 statement: An updated guideline for reporting systematic reviews. BMJ 2021, 372, n71. [Google Scholar] [CrossRef]



{kind=link}
{kind=link}
| Author and Year | Study Objective | AI Model and Study Design | PSMA Tracer Used | Inclusion Criteria | Sample Size of (Training/Validation/Test) | Data Input | Comparator | Algorithm Performance | Strength | Limitations |
|---|---|---|---|---|---|---|---|---|---|---|
| Nickols et al., 2021 [24] | Evaluate aPROMISE’s ability to reduce inter-reader variability of PSMA PET-CT | DL Multi-centre Retrospective | 18F- PSMA PET-CT | veterans with intermediate- or high-risk PCa who underwent PSMA scan | NR/NU/109 No cross-validation | NR | Between two nuclear medicine physicians | Cohen pairwise k-agreement for PCa staging between two readers was high (0.82 for miN0M0, 0.90 for miN1M0, 0.77 for miN0M1b.) | Moderate sample size Using external data to evaluate an existing DL software | Retrospective Selective study population (only veterans) |
| Johnsson et al., 2022 [27] | Based on aPROMISE, evaluate the sensitivity of automated detection of potential lesions | DL Multi-centre Retrospective | 18F-PSMA PET-CT | 1. high-risk PCa planned for RP with PLND) 2. radiologic evidence of recurrent or metastatic PCa and considered feasible for biopsy | NR/235/295 No cross-validation | PSMA PET-CT scans annotated by experienced nuclear medicine readers for location, SUVmax, SUVpeak, SUVmean, and uptake volume. | NR | Sensitivity of detecting lesion with metastasis: 91.5% for regional lymph node 90.6% for all lymph node 86.7% for bone | Large sample size Using external data to evaluate an existing DL software | Retrospective Demographic and clinicopathological characteristics of included patients were not reported. No cross-validation |
| Leung et al., 2022 [28] | Develop an ML to perform classification of PSMA uptake and correlate to PSMA-RADS | DL Multi-centre Retrospective | 18F-PSMA PET-CT | Patients who underwent 18F-PSMA PET-CT | 267 patients had 3794 lesions divided into: 2302/760/732 | Scans were segmented by four nuclear medicine physicians then CNN extracted radiomic features and tissue-type information | Probability score compared against PSMA-RADS categories on a t-SNE scatter plot | PSMA-RADS classification at lesion level AUROC 0.87 and accuracy of 0.52. Patient level AUROC 0.9 and accuracy of 0.77. Probability score of PSMA-RADS-1 and 2 was 0.19, PSMA-RADS-3 was 0.5, PSMA-RADS-4 and 5 was 0.86 | Large sample size Has both training and validation set | Retrospective Demographic and clinicopathological characteristics of included patients were not reported. Demographic and clinicopathological characteristics of included patients were not reported. |
| Trägårdh et al., 2023 [29] | Develop and validate a CNN for detecting and quantifying tumour burden (TLV and TLU) of lymph node metastases and bone metastases | CNN Single-centre Retrospective | 18F-PSMA PET-CT | initial staging of high-risk prostate cancer or for the detection of sites of suspected recurrent disease. | 420/120/120 No cross-validation | One independent nuclear medicine physician segmented and annotated the scan. Three main inputs include CT image, PET image, and multi-channel organ mask | Sensitivity of nuclear medicine physicians for detecting lymph nodes (78%) and bone metastasis (59%) | Sensitivity of CNN for detecting lymph nodes (79%) and bone metastasis (62%) correlations of TLV and TLU between CNN and nuclear medicine physicians were all statistically significant and ranged from R = 0.53 to R = 0.83. | Large sample size Data set for testing separate from training data Compared to several nuclear medicine physicians | Single center The same data set is for training and validation. Demographic and clinicopathological characteristics of included patients were not reported. |
| Capobianco et al., 2021 [30] | Develop and evaluate CNN to classify PSMA uptake into anatomical location and determine if it is suspicious for cancer | CNN Single-centre Retrospective | 68Ga-PSMA PET-CT | 1. Primary staging of PCa or for assessment of BCR 2. PSMA-ligand PET-CT for all other indications of PCa. | 121/NU/52 4-fold cross-validation | Nuclear medicine physician labelled PSMA uptake into anatomical location and suspicion for PCa. Data from 18F-FDG PET-CT scans was added to determine if improved CNN | Compared to nuclear medicine physician assessment | CNN had an average precision of 80.4% [CI: 71.1–87.8] for suspicious uptake identification, 77% (CI: 70.0–83.4) accuracy for anatomical classification of suspicious findings, agreement for identification of regional lymph node involvement (81%) and metastatic stage (77%) | Demonstrated combining training information from 18F-FDG PET/CT and 68Ga-PSMA-11 PET/CT led to improved accuracy | Single center Small data set for testing and no separate data set for validation Demographic and clinicopathological characteristics of included patients were not reported. |
| Erle et al., 2021 [31] | Comparing and validating ML algorithms in classifying pathological uptake in PCa | ML Single-centre Retrospective | 68Ga-PSMA PET-CT | PCa patients who underwent PSMA PET-CT for either staging or treatment control | 72/NU/15 3-fold cross-validation | 77 radiomics features calculated using InterView FUSION software from 2452 manually delineated hotspots on PSMA PET-CT | Testing with a hold-out set of 15 patients | AUC = 98% Sensitivity = 97% Specificity = 82% | A detailed explanation of radiomics features used in the development | Small sample size No histopathological confirmation of metastasis |
| Moazemi et al., 2020 [32] | Develop and evaluate ML algorithm in differentiating non-specific from malignant PSMA uptake | ML Single-centre Retrospective | 68Ga-PSMA PET-CT | Follow-up staging or consideration of radionuclide therapy for PCa patients who previously underwent treatment (active or systemic treatment) | 48/24/NU 5-fold cross-validation | 40 textural features calculated using InterView FUSION software from 2419 hotspots determined by nuclear medicine physicians on PSMA PET-CT | Compared to nuclear medicine physician assessment | AUC = 98% Sensitivity = 94% Specificity = 89% | A detailed explanation of radiomics features used in the development Developed and compared five different ML algorithms | Small sample size Patients underwent various treatments (hormonal versus chemotherapy versus radiotherapy) |
| Kendrick et al., 2022 [25] | Develop and evaluate a CNN to extract prognostic biomarkers (TLV and TLU) from PSMA PET-CT | CNN Single-centre Prospective | 68Ga-PSMA PET-CT | BCR PCa following active treatment who received PSMA PET-CT before further surgery, radiotherapy, or systemic treatment. follow up scans 6 months later | 262 */NU/75 * 53 negative scans used as control 5-fold cross-validation | Lesions for each patient scan were manually delineated by an expert Nuclear Medicine Physician | Testing with a hold-out set of 75 patients. | Accuracy = 94.5% Sensitivity = 93.3% Specificity = 96.2% TLV and TLU from CNN were associated with overall survival (both p < 0.005) | Large sample size Prospective Used negative scans as a control | Single center |
| Acar et al., 2019 [33] | Develop ML to differentiate PCa bony metastatic versus sclerotic (responded to treatment) on PSMA PET-CT | ML Single-centre Retrospective | 68Ga-PSMA PET-CT | PCa with known bone metastasis and who were previously treated | 75/NU/NU 10-fold cross-validation | Lesion marked by nuclear medicine physician on LifeX software analysis which extracted HU, 5 histogram data, 3 shape-based data, and 32 s-order textural analysis data | Results from cross-validation | AUC = 76% Accuracy = 73.5% Sensitivity = 73.5% Specificity = 73.7% Weighted KNN ML algorithm could differentiate metastasis bony from completely responded lesions | Used completely responded sclerotic lesions as control | Retrospective Small sample size |
| Duriseti et al., 2023 [34] | Quantifying treatment response by correlating changes in aPROMISE PSMA score to PSA changes | CNN Site NR Retrospective | 18F-PSMA PET-CT | csPCa who underwent PSMA PET-CT before and 3 months or more after surgery, radiotherapy, and/or ADT | NR/NU/30 No cross-validation | aPROMISE was used to identify, quantify, and calculate changes in PSMA tracer avid disease | Compared to post-treatment PSMA PET-CT | Baseline prostate bed PSMA scores were correlated with baseline PSA (p < 0.001). Nodal (p = 0.53) and bony (p = 0.65) baseline PSMA scores did not correlate with baseline PSA. Changes in PSMA scores were significantly correlated with corresponding decreases in PSA for composite and nodal disease, but not for prostate bed or bony disease | Clinicopathological characteristics of included patients reported. | Small sample size No separate data set for development and testing |
| Moazemi et al., 2021 [26] | Develop ML to predict response to 177Lu-PSMA treatment using Baseline PSMA-PET-CT scans and clinical parameters | ML Single-centre Retrospective | 68Ga-PSMA PET-CT | Advanced PCa scheduled for treatment with 177Lu-PSMA | 56/27/NU 3-fold cross-validation | 14 clinical parameters And 73 radiomics features were calculated using InterView FUSION software from a 2070 hotspot determined by a nuclear medicine physician on PSMA PET-CT | a permutation test (null hypothesis = permuted distribution of ground truth labels could have resulted in similar prediction scores) | AUC = 80% Sensitivity = 75% Specificity = 75% Radiomics features (PET_Min, PET_Correlation, CT_Min, CT_Busyness and CT_Coarseness) and clinical parameters such as Alp1 and Gleason score showed best correlations with change in PSA | Included clinical parameters in the development of the AI model A detailed explanation of radiomics features used in the development | Small sample size Single center |
| Study | ROB | Applicability Concerns | Overall | ||||||
|---|---|---|---|---|---|---|---|---|---|
| Participants | Predictors | Outcome | Analysis | Participants | Predictors | Outcome | ROB | Applicability | |
| Nickols et al., 2021 [24] | Low | Low | Low | Low | Low | Unclear | Unclear | Low | Unclear |
| Johnsson et al., 2022 [27] | Low | Low | Low | Low | Low | Low | Low | Low | Low |
| Leung et al., 2022 [28] | Unclear | Low | Low | Low | Unclear | Low | Low | Low | Low |
| Trägårdh et al., 2023 [29] | Low | Low | Low | Low | Low | Low | Low | Low | Low |
| Capobianco et al., 2021 [30] | Low | Low | Low | Low | High | Unclear | Unclear | Low | High |
| Erle et al., 2021 [31] | Low | Low | Low | Low | Low | Low | Low | Low | Low |
| Moazemi et al., 2020 [32] | Low | Low | Low | Low | Low | Low | Low | Low | Low |
| Kendrick et al., 2022 [25] | Low | Low | Low | Low | Low | Low | Low | Low | Low |
| Acar et al., 2019 [33] | Low | Low | Unclear | High | Low | High | Low | High | High |
| Duriseti et al., 2023 [34] | Unclear | Low | Low | Low | Unclear | Unclear | Unclear | Low | Unclear |
| Moazemi et al., 2021 [26] | Low | Low | Low | Low | Low | Low | Low | Low | Low |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Liu, J.; Cundy, T.P.; Woon, D.T.S.; Lawrentschuk, N. A Systematic Review on Artificial Intelligence Evaluating Metastatic Prostatic Cancer and Lymph Nodes on PSMA PET Scans. Cancers 2024, 16, 486. https://doi.org/10.3390/cancers16030486
Liu J, Cundy TP, Woon DTS, Lawrentschuk N. A Systematic Review on Artificial Intelligence Evaluating Metastatic Prostatic Cancer and Lymph Nodes on PSMA PET Scans. Cancers. 2024; 16(3):486. https://doi.org/10.3390/cancers16030486
Chicago/Turabian StyleLiu, Jianliang, Thomas P. Cundy, Dixon T. S. Woon, and Nathan Lawrentschuk. 2024. "A Systematic Review on Artificial Intelligence Evaluating Metastatic Prostatic Cancer and Lymph Nodes on PSMA PET Scans" Cancers 16, no. 3: 486. https://doi.org/10.3390/cancers16030486
APA StyleLiu, J., Cundy, T. P., Woon, D. T. S., & Lawrentschuk, N. (2024). A Systematic Review on Artificial Intelligence Evaluating Metastatic Prostatic Cancer and Lymph Nodes on PSMA PET Scans. Cancers, 16(3), 486. https://doi.org/10.3390/cancers16030486