Simple Summary
As technology progresses, the scope and practice of medicine adapts, resulting in treatment applications that improve the precise and potentially current standard of care. The advent and continued use of proton beam therapy for use in patients with prostate cancer is a slowly evolving topic due to the lack of level 1 evidence demonstrating improved efficacy with its use. Despite this, not all patients are provided with equal access to this treatment modality. While there have been several publications utilizing either single-institutional analyses or national medical databases, to date, a comprehensive review summarizing the disparities and inequities in proton beam therapy use in prostate cancer does not exist. Our research sought to elucidate trends in this topic and create a compendium that can be used to inform future study and equitable advances in the field.
Abstract
Our study sought to review and summarize the reported health disparities and inequities in the utilization of proton beam therapy (PBT) for prostate cancer. We queried the PubMed search engine through 12/2023 for original publications examining disparate utilization of PBT for prostate cancer. The query terms included the following: prostate cancer AND proton AND (disparities OR IMRT OR race OR insurance OR socioeconomic OR inequities)”. Studies were included if they involved United States patients, examined PBT in prostate cancer, and addressed health inequities. From this query, 22 studies met the inclusion criteria, comprising 13 population-based analyses, 5 single-institutional analyses, 3 cost/modeling investigations, and 1 survey-based study. The analyses revealed that in addition to age-related and insurance-related disparities, race and socioeconomic status played significant roles in the receipt of PBT. The likelihood of receiving PBT was lower for non-White patients in population-based and single-institution analyses. Socioeconomic metrics, such as higher median income and higher education level, portended an increased likelihood of receiving PBT. Conclusively, substantial age-based, racial, socioeconomic/insurance-related, and facility-associated disparities and inequities existed for PBT utilization in prostate cancer. The identification of these disparities provides a framework to better address these as the utility of PBT continues to expand across the US and globally.
1. Introduction
Prostate cancer, the most common cancer in males across the United States, is characterized by well-documented disparities in incidence, management, and outcomes [1,2,3,4]. While management options for prostate cancer continue to expand, radiotherapy (RT) remains an essential curative therapeutic option. Although historical forms of RT have been photon (X-ray) based, proton beam therapy (PBT) is a newer modality touted to be dosimetrically favorable to photon-based therapy [5]. However, the degree to which dosimetric benefits may translate to toxicity reduction remains unclear, which is important considering that PBT delivery costs are greater than photon-based RT [6,7]. While preliminary findings of the PARTIQoL trial showed similar results for the reported bowel summary scores of Expanded Prostate Cancer Index Composite (EPIC) patients between the two modalities at 24 months, grade toxicities and other secondary endpoints have not been reported yet. The COMPPARRE trial is also evaluating these differences, and together, the findings will be deterministic in how we approach prostate cancer [8,9]. Because the implementation of PBT has more recently progressed quickly, there remain several areas requiring elucidation through comprehensive summarization.
Well-documented health disparities and inequities exist in prostate cancer incidence, healthcare resource utilization, and mortality. Providing care that is equitable and that does not vary in quality because of personal characteristics such as gender, ethnicity, geographic location, and socioeconomic status is considered one of the six domains of health care quality according to the National Academy of Medicine [10]. Inequities in the utilization of proton beam therapy (PBT) specifically in prostate cancer have not yet been comprehensively summarized.
Studies have demonstrated that PBT is one of the least commonly used modalities of radiation therapy in men with prostate cancer and that its utilization may vary given challenges in access to care [11,12]. To address this knowledge gap, we performed a review of the published articles on disparities in the delivery of PBT for prostate cancer (Table 1). Our purpose was to review and summarize the reported health disparities and inequities in the use of proton beam therapy for prostate cancer in the United States.

Table 1.
List of studies meeting the inclusion criteria regarding health disparities and inequities in the utilization of proton therapy for prostate cancer.
2. Materials and Methods
We queried the PubMed search engine for original studies published in English that studied health disparities in the delivery of PBT for prostate cancer. Query terms were as follows: prostate AND proton AND (disparities OR IMRT OR race OR insurance OR socioeconomic OR inequities). Articles known to the authors and those based on the references of the obtained articles were also utilized. Studies were excluded if they did not specifically evaluate PBT, were not based in the United States, or did not directly examine health inequities. Unpublished abstracts were not included owing to the inability to completely assess their validity and methodologies. There were no date restrictions, and the search included articles published through December 2023. It was infeasible to perform a meta-analysis on the available literature because of the inherent heterogeneity of the study topic.
3. Results
A total of 162 studies were captured in the initial query. Of these, 22 met the inclusion criteria. These 22 studies, published from 2012 to 2023, comprised 13 population-based analyses, 5 single-institutional analyses, 3 cost/modeling investigations, and 1 survey-based study (Figure 1).
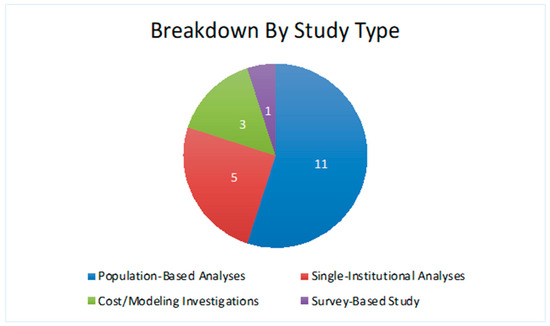
Figure 1.
Breakdown of study characteristics.
The datasets analyzed in these studies include the National Cancer Database (NCDB), the Surveillance, Epidemiology, and End Results (SEER), and several single-institutional studies. Of the 22 articles, 19 had a primary outcome of PBT utilization, with the other 3 evaluating treatment toxicity, clinical benefit, and participation in clinical trials. The most common health inequities pertained to factors such as age, race/ethnicity, socioeconomic status, insurance type, and geography of the patient and treatment center. Of these, a majority of the studies identified racial disparities impacting the use of PBT for prostate cancer management (Figure 2).
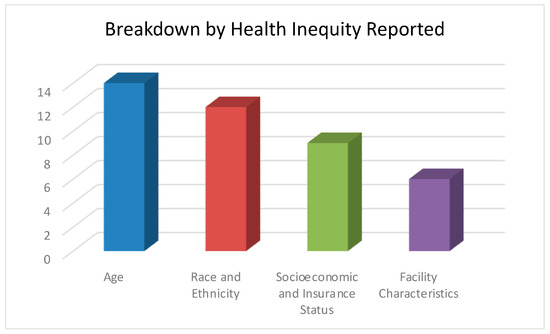
Figure 2.
Breakdown of health inequities reported.
3.1. Age
Age was evaluated in 15 of the 22 (68%) studies, and overall showed a decreased likelihood of receiving PBT with advancing age. For example, a study of 143,702 patients in the National Cancer Database (NCDB) sought to examine trends in and characterization of PBT for prostate cancer [13]. The authors found a steady increase in PBT utilization (2.7% of all external-beam RT in 2004 to 5.6% in 2013), which was most pronounced in low-risk cases. The odds ratio (OR) for PBT in patients ≥ 65 years old was 0.74, when accounting for other factors such as the comorbidity index or insurance status in multivariable analysis (p < 0.001). These findings are very comparable to the findings of a similar NCDB study of 187,730 patients that also sought to evaluate trends and practice patterns for PBT. That study determined through multivariable analysis that each successive year of age at diagnosis was associated with a 5% lower chance of receiving PBT [14]. From a dataset of Medicare beneficiaries (n = 27,647) assessing the same question as the aforementioned NCDB publications, Yu and colleagues found that the percentage of PCa (prostate cancer) patients receiving PBT was 3.3% between the ages of 66 and 69, 2.1% for those 70–74, 1.4% for those 75–79, and 1.0% for those 80–84 [15]. These corresponded to the adjusted ORs, with reference to ages 66–69, of 0.66, 0.45, and 0.33, respectively (p < 0.001).
3.2. Race and Ethnicity
Regarding race and ethnicity, 13 of the 22 (59%) of the investigations reported that non-White populations were less likely to receive PBT. The aforementioned NCDB studies demonstrated ORs for Black and other non-Black minorities (with reference to White patients) to be 0.66 and 0.65, respectively [13], and 0.20 and 0.57, respectively [14] (p < 0.001). These ORs in a single-institution retrospective study (n = 633) aimed at evaluating sociodemographic inequalities in PBT receipt, were 0.29 (p < 0.001) and 0.42 (p < 0.025), respectively [16]. Parikh-Patel et al. underscored these results when their research showed that those who received PBT therapy were disproportionately White (70.7%). This same cohort consisted of only 5.6% non-Hispanic Blacks (p < 0.001) [17]. Unfortunately, these disparities have not waned, as a more recent study utilizing the NCDB found the racial disparity in PBT utilization widening for both ASTRO model policy proton therapy-designated group 1 (PBT use indicated) and group 2 (PBT use still under investigation) cancers, the latter of which includes prostate cancer. The study showed that overall, between 2004 and 2018, Black males were less likely to receive PBT when compared to their White counterparts (OR, 0.67; 95% CI, 0.64–0.71). For group 1 cancers, Black patients were less likely to receive PBT when indicated vs. their White counterparts (0.4% vs. 0.8%; OR, 0.49; 95% CI, 0.44–0.55). For group 2 cancers, racial disparities persisted, as the Black race was a negative predictor of PBT use in comparison to its White counterpart (0.3% vs. 0.4%; OR, 0.75; 95% CI, 0.70–0.80) [18]. To date, there is no evidence to attribute differential rates in adverse events following RT to racial inequities in PBT utilization [19]. A single-institution, matched-pair analysis of health-related quality of life after PBT demonstrated no statistically significant differences in sexual function, urinary incontinence, urinary obstruction, or bowel summary scores between Black and White patients [20]. With respect to clinical trial enrollment, a prospective assessment of patients’ willingness to participate in a hypothetical randomized controlled trial of IMRT versus PBT found that 69% of Black patients endorsed a willingness to enroll, which was numerically higher than White patients (55%) [21]. Of note, the primary motivation for the vast majority (77%) of Black patients for enrollment in such a trial was altruism for other patients, which was numerically different from White patients (45%).
3.3. Socioeconomic and Insurance Status
Of the 22 studies, 10 (45%) individually evaluated socioeconomic and insurance status, with most demonstrating that PBT delivery correlates with numerous markers of socioeconomic status. Yabroff et al. showed that PBT use has increased across all insurance types (private vs. uninsured vs. Medicaid vs. Medicare), in group 1 (annual percent changes (APCs) of 20.89 for private insurance, 22.78 for uninsured, 21.01 for Medicaid, and 28.80 for Medicare; p < 0.001 for all, 2010–2018) and group 2 (APCs of 32.04 for private insurance, 28.24 for Medicare, 53.01 for Medicaid, and 51.31 for the uninsured; p < 0.001 for all, 2014–2018) [22]. The other aforementioned NCDB publications demonstrated that independent predictors of PBT administration included a higher median income, a higher percentage of adults with a high school diploma in the zip code, and a longer travel distance to a PBT center [13,14,16]. While potential confounding factors might stem from the insurance type, as demonstrated in Mendenhall et al.’s study that highlighted the influence of payor type on approval rates (with Medicare notably approving more patients than commercial payors for proton beam therapy for prostate cancer), multivariable analyses were employed to account for insurance-related variables [23,24,25]. These findings were also supported by two single-institutional cost investigations at the MD Anderson Cancer Center and of the Surveillance, Epidemiology, and End Results (SEER) database linked with Medicare [26,33]. Although neither utilized dedicated multivariable analyses, most patients in the PBT cohorts comprised patients with higher median household incomes and/or high school diplomas.
3.4. Facility Characteristics
Of the 22 publications, 6 (30%) evaluated this parameter. Although it is intuitive that academic centers are more likely to deliver PBT [14,27], owing to the availability of newer technologies at these facilities, a cost analysis evaluated the novel characteristics of patient volume and reimbursement scenarios. The up-front cost expenditure to build proton centers, compounded by interest rates, creates a large debt for institutions. Reimbursement models, such as the Affordable Care Act, may make it difficult for facilities to receive an adequate return on investment without sacrificing the quality of care (due to the higher volume needed to fund the operational cost of PBT) Based on this study, the authors concluded that fee-for-service centers and those with higher patient volumes would be more associated with financial stability, whereas accountable care reimbursement would necessitate a substantial increase in patient volume in order to remain financially viable. These factors are important to consider, as facility-related disparities impact patients with a wide variety of socioeconomic, racial, and age-based backgrounds [28].
4. Discussion
Proton therapy for localized prostate cancer is part of a growing body of technological advances aimed at maximizing tumor control while minimizing side effects on surrounding organs-at-risk, providing an advancing modality for increasingly precise and targeted radiation delivery [34,35,36]. With the increasing utility of PBT throughout the nation and worldwide, it is imperative to better summarize the available evidence of disparities and inequities in receipt thereof. While data from a recent single-center, case-matched, retrospective analysis demonstrated similar outcomes in long-term disease control between PBT and IMRT for prostate cancer, it also indirectly underscored the disparities that exist in PBT utilization, demonstrating that significantly fewer Black or African American patients received PBT for PCa relative to their White counterparts, further necessitating a dire need to elucidate mechanisms of disparities and inequities in our healthcare system [29].
This review of 22 publications demonstrates that substantial age-based, racial, socioeconomic/insurance-related, and facility-associated disparities exist for PBT in prostate cancer. The identification of these disparities provides a framework to better address these, as the utility of PBT across several disease sites continues to expand. Indeed, such disparities have also been noted in the utilization of PBT for other malignancies, including pediatric, where the factors associated with PBT utilization are a younger age, having private/managed care rather than Medicaid or no insurance, a higher median household income and parental educational attainment, or traveling more than 200 miles to the center [30,37].
The findings with regard to age are noteworthy. It is well recognized that age is an independent prognostic factor for most tumors, and the chance of experiencing potential decreases in long-term toxicities (albeit not proven for prostate cancer) inversely correlate with age. Additionally, the lower integral dose afforded by PBT may reduce the secondary malignancy rate, which is of less concern in advancing age but may still be relevant, as demonstrated in a recent NCDB study, which found a lower rate of secondary malignancies in patients with prostate cancer undergoing PBT compared to IMRT [38]. Moreover, it is also well recognized that older patients remain under-represented in cancer clinical trials, although it is uncertain which patients in the studies evaluated herein were treated on protocol [39,40]. Nevertheless, it should be noted that the age differences persisted when adjusting for the fact that older patients receive Medicare (which supports PBT to a greater degree than other insurances). A single-institution retrospective study queried their billing center at a large academic center for patients who were considered for PBT from January 2013 to December 2016 using insurance decision (approval vs. denial) as an endpoint. Using multivariate analysis, Medicare insurance was the strongest predictor of insurance approval with an OR of 14.2 (p < 0.001), while secondary insurance approval for treatment had an OR of 2.6 (p < 0.001). While this particular study was limited to head and neck cancers, these findings indicate the pervasiveness of this disparity as it extends to other disease sites [31].
The racial findings herein are likely not unifocal but part of a constellation of several factors that reflect the difficulty of obtaining the proper financial clearances (e.g., prior authorization) to receive oncologic therapy (especially for PBT) in the United States. This is best evidenced by evaluating the ORs prior to, and following, multivariable adjustment in several of the analyses herein. These ORs are often quite different, implying that racial disparities are intertwined and mediated by other variables, such as insurance, income, education, and other factors. Mahal et al. study showed that Black, Hispanic, or other minority patients were significantly less likely to receive proton therapy compared to White patients (adjusted odds ratio (AOR), 0.20 (95% confidence interval (95% CI), 0.18–0.22; p < 0.0001), AOR, 0.57 (95% CI, 0.48- 0.66; p < 0.0001), and AOR, 0.59 (95% CI, 0.50–0.69; p < 0.0001), respectively) [14]. Moreover, a recently published cross-sectional study highlighted that age (>65 years old) and socioeconomic status were negative determinants for access to PBT, further underscoring the multifactorial nature of these findings [41]. Notably, not all of these issues can be adequately addressed by multivariable analyses in retrospective studies, and therefore, it still appears that race has a strong independent impact on PBT utilization, potentially related to intrinsic biases and concerns. Further work to address these notions is needed.
Socioeconomic factors are also important to evaluate but suffer from a lack of adequate granularity in most of the available data. For instance, Medicaid reimbursement varies by state/region [42], and not all private insurers are equally willing to reimburse for a given RT technique [43]. To this extent, the analysis by Elnahal et al. is important, in that they modeled reimbursement scenarios representative of the current economic landscape (i.e., fee-for-service versus accountable care) [27]. As shown in their study, the affordability of PBT for not only proton centers/institutions but also patients of all backgrounds could be significantly impacted by ongoing policy changes and disparately impact certain demographic groups over others. Furthermore, this disparity may be exacerbated by denials and the requirement for prior authorization by insurance companies, which, as Gupta et al. showed, lead to significant delays in patient care (average of ~3 weeks). The study underscored the necessity for a streamlined process and agreement between payors and providers in which coverage policies conform to progressing national guidelines [32].
The limitations of this analysis include mainly the search term methodology, which may have excluded older studies due to the evolution of language and terminology in medicine. The scholarly works referenced in this manuscript have their own inherent specific limitations that include the sample size, length of study, and specific parameters utilized by the researchers.
5. Conclusions
Although PBT utilization is rapidly expanding, not all patients may experience this to an equal degree. This review demonstrates that substantial age-based, racial, socioeconomic/insurance-related, and facility-associated disparities exist for PBT in prostate cancer. The identification of these disparities provides a framework to better address these inequities as the utility of PBT across several disease sites continues to expand. As the utilization of proton therapy increases across various and new disease sites and expands across the country and globally, it is important to assess disparities and inequities in its utilization in order to address and improve equitable access so that all patients may benefit from the study and delivery of protons.
Author Contributions
Conceptualization, C.D.; methodology, C.D.; validation, C.D. and C.G.W.; formal analysis, C.G.W.; investigation, C.G.W.; resources, C.D. and C.G.W.; data curation, C.D. and C.G.W.; writing—original draft preparation, C.G.W.; writing—review and editing, C.D.; visualization, C.G.W.; supervision, C.D.; project administration, C.D.; funding acquisition, C.D. All authors have read and agreed to the published version of the manuscript.
Funding
This research received no external funding.
Data Availability Statement
Our data can be found on PubMed by querying prostate AND proton AND (disparities OR IMRT OR race OR insurance OR socioeconomic OR inequities).
Conflicts of Interest
The authors declare no conflicts of interest.
References
- Imperato, P.J.; Nenner, R.P.; Will, T.O. Radical prostatectomy: Lower rates among African-American men. J. Natl. Med. Assoc. 1996, 88, 589–594. [Google Scholar] [PubMed]
- Hoffman, R.M.; Gilliland, F.D.; Eley, J.W.; Harlan, L.C.; Stephenson, R.A.; Stanford, J.L.; Albertson, P.C.; Hamilton, A.S.; Hunt, W.C.; Potosky, A.L. Racial and ethnic differences in advanced-stage prostate cancer: The Prostate Cancer Outcomes Study. J. Natl. Cancer Inst. 2001, 93, 388–395. [Google Scholar] [CrossRef] [PubMed]
- Albano, J.D.; Ward, E.; Jemal, A.; Anderson, R.; Cokkinides, V.E.; Murray, T.; Henley, J.; Liff, J.; Thun, M.J. Cancer mortality in the United States by education level and race. J. Natl. Cancer Inst. 2007, 99, 1384–1394. [Google Scholar] [CrossRef] [PubMed]
- Chornokur, G.; Dalton, K.; Borysova, M.; Kumar, N. Disparities at Presentation, Diagnosis, Treatment and Survival in African American Men, Affected by Prostate Cancer. Prostate 2011, 71, 985–997. [Google Scholar] [CrossRef]
- Vargas, C.E.; Fryer, A.; Mahajan, C.; Indelicate, D.; Horne, D.; Chellini, A.; McKenzie, C.; Lawlor, P.; Henderson, R.; Li, Z.; et al. Dose–Volume Comparison of Proton Therapy and Intensity-Modulated Radiotherapy for Prostate Cancer. Int. J. Radiat. Oncol. Biol. Phys. 2008, 70, 744–751. [Google Scholar] [CrossRef]
- Verma, V.; Mishra, M.V.; Mehta, M.P. A systematic review of the cost and cost-effectiveness studies of proton radiotherapy. Cancer 2016, 122, 1483–1501. [Google Scholar] [CrossRef]
- Verma, V.; Shah, C.; Rwigema, J.M.; Solberg, T.; Zhu, X.; Simone, C.B., II. Cost-comparativeness of proton versus photon therapy. Chin. Clin. Oncol. 2016, 5, 56. [Google Scholar] [CrossRef]
- Efstathiou, J.A.; Yeap, B.Y.; Michalski, J.M.; Horick, N.; Zietman, A.L.; Christodouleas, J.P.; Kamran, S.C.; Parkih, R.R.; Vapiwala, N.; Mihalcik, S.A.; et al. Prostate Advanced Radiation Technologies Investigating Quality of Life (PARTIQoL): Phase III Randomized Clinical Trial of Proton Therapy vs. IMRT for Localized Prostate Cancer. Int. J. Radiat. Oncol. Biol. Phys. 2024, 120, S1. [Google Scholar] [CrossRef]
- A Prospective Comparative Study of Outcomes with Proton and Photon Radiation in Prostate Cancer (COMPPARE). Available online: https://clinicaltrials.gov/study/NCT03561220 (accessed on 12 December 2020).
- Institute of Medicine (IOM). Crossing the Quality Chasm: A New Health System for the 21st Century; National Academy Press: Washington, DC, USA, 2001. [Google Scholar]
- Agrawal, R.; Dey, A.; Datta, S.; Nassar, A.; Grubb, W.; Traughber, B.; Biswas, T.; Ove, R.; Podder, T. Pattern of Radiotherapy Treatment in Low-Risk, Intermediate-Risk, and High-Risk Prostate Cancer Patients: Analysis of National Cancer Database. Cancers 2022, 14, 5503. [Google Scholar] [CrossRef]
- Mukherjee, K.; Small, W., Jr.; Duszak, R., Jr. Trends and variations in utilization and costs of radiotherapy for prostate cancer: A SEER medicare analysis from 2007 through 2016. Brachytherapy 2022, 21, 12–21. [Google Scholar] [CrossRef]
- Amini, A.; Raben, D.; Crawford, E.D.; Flaig, T.W.; Kessler, E.R.; Lam, E.T.; Maroni, P.; Pugh, T.J. Patient characterization and usage trends of proton beam therapy for localized prostate cancer in the United States: A study of the National Cancer Database. Urol. Oncol. 2017, 35, 438–446. [Google Scholar] [CrossRef] [PubMed]
- Mahal, B.A.; Chen, Y.; Efstathiou, J.A.; Muralidhar, V.; Hoffman, K.E.; Yu, J.B.; Feng, F.Y.; Beard, C.J.; Martin, N.E.; Orio, P.F.; et al. National Trends and Determinants of Proton Therapy Use for Prostate Cancer: A National Cancer Data Base Study. Cancer 2016, 122, 1505–1522. [Google Scholar] [CrossRef] [PubMed]
- Yu, J.B.; Soulos, P.R.; Herrin, J.; Cramer, L.D.; Potosky, A.L.; Roberts, K.B.; Gross, C.P. Proton Versus Intensity-Modulated Radiotherapy for Prostate Cancer: Patterns of Care and Early Toxicity. J. Natl. Cancer Inst. 2013, 105, 25–32. [Google Scholar] [CrossRef]
- Woodhouse, K.D.; Hwang, W.; Vapiwala, N.; Jain, A.; Wang, X.; Both, S.; Shah, M.; Frazier, M.; Gabriel, P.; Christodouleas, J.P.; et al. Sociodemographic disparities in the utilization of proton therapy for prostate cancer at an urban academic center. Adv. Radiat. Oncol. 2017, 2, 132–139. [Google Scholar] [CrossRef][Green Version]
- Parikh-Patel, A.; Morris, C.; Maguire, F.; Daly, M.; Kizer, K. A population-based assessment of proton beam therapy utilization in California. Am. J. Manag. Care 2020, 26, e28–e35. [Google Scholar]
- Nogueira, L.M.; Sineshaw, H.M.; Jemal, A.; Pollack, C.E.; Efstathiou, J.A.; Yabroff, K.R. Association of Race With Receipt of Proton Beam Therapy for Patients With Newly Diagnosed Cancer in the US, 2004–2018. JAMA Netw. Open 2022, 5, e228970. [Google Scholar] [CrossRef] [PubMed] [PubMed Central]
- Sheets, N.C.; Goldin, G.H.; Meyer, A.M.; Wu, Y.; Chang, Y.; Stürmer, T.; Holmes, J.A.; Reeve, B.B.; Godley, P.A.; Carpenter, W.R.; et al. Intensity-modulated radiation therapy, proton therapy, or conformal radiation therapy and morbidity and disease control in localized prostate cancer. JAMA 2012, 307, 1611–1620. [Google Scholar]
- Bryant, C.; Mendenhall, N.P.; Henderson, R.H.; Nichols, R.C.; Mendenhall, W.M.; Morris, C.G.; Williams, C.; Su, Z.; Li, Z.; Hoppe, B.S. Does Race Influence Health-related Quality of Life and Toxicity Following Proton Therapy for Prostate Cancer? Am. J. Clin. Oncol. 2016, 39, 261–265. [Google Scholar] [CrossRef]
- Shah, A.; Efstathiou, J.A.; Paly, J.J.; Halpern, S.D.; Bruner, D.W.; Christodouleas, J.P.; Coen, J.J.; Deville, C.; Vapiwala, N.; Shipley, W.U.; et al. Prospective Preference Assessment of Patients’ Willingness to Participate in a Randomized Controlled Trial of Intensity-Modulated Radiotherapy Versus Proton Therapy for Localized Prostate Cancer. Int. J. Radiat. Oncol. Biol. Phys. 2012, 83, e13–e19. [Google Scholar] [CrossRef]
- Nogueira, L.M.; Jemal, A.; Yabroff, K.R.; Efstathiou, J.A. Assessment of Proton Beam Therapy Use Among Patients With Newly Diagnosed Cancer in the US, 2004–2018. JAMA Netw. Open 2022, 5, e229025. [Google Scholar] [CrossRef]
- Mendenhall, W.M.; Brooks, E.D.; Smith, S.; Morris, C.G.; Bryant, C.B.; Henderson, R.H.; Nichols RCJr McIntyre, K.; Klein, S.L.; Mendenhall, N.P. Insurance Approval for Definitive Proton Therapy for Prostate Cancer. Int. J. Part. Ther. 2021, 8, 36–42. [Google Scholar] [CrossRef] [PubMed]
- Pan, H.Y.; Jiang, J.; Shih, Y.T.; Smith, B.D. Adoption of Radiation Technology Among Privately Insured Nonelderly Patients With Cancer in the United States, 2008 to 2014: A Claims-Based Analysis. J. Am. Coll. Radiol. 2017, 14, 1027–1033. [Google Scholar] [CrossRef] [PubMed]
- Sharma, A.M.; Khairnar, R.; Kowalski, E.S.; Remick, J.; Nichols, E.M.; Mohindra, P.; Yock, T.; Regine, W.; Mishra, M.V. Patient Prioritization for Proton Beam Therapy in a Cost-neutral Payer Environment: Use of the Clinical Benefit Score for Resource Allocation. Cureus 2019, 11, e5703. [Google Scholar] [PubMed]
- Halpern, J.A.; Sedrakyan, A.; Hsu, W.; Mao, J.; Daskivich, T.J.; Nguyen, P.L.; Golden, E.B.; Kang, J.; Hu, J.C. Use, Complications, and Costs of Stereotactic Body Radiotherapy for Localized Prostate Cancer. Cancer 2016, 122, 2496–2504. [Google Scholar] [CrossRef]
- Tang, C.; Lei, X.; Smith, G.L.; Pan, H.Y.; Hoffman, K.E.; Kumar, R.; Chapin, B.F.; Shih, Y.T.; Frank, S.J.; Smith, B.D. Influence of Geography on Prostate Cancer Treatment. Int. J. Radiat. Oncol. Biol. Phys. 2021, 109, 1286–1295. [Google Scholar] [CrossRef]
- Elnahal, S.M.; Kerstiens, J.; Helsper, R.S.; Zietman, A.L.; Johnstone, P.A. Proton Beam Therapy and Accountable Care: The Challenges Ahead. Int. J. Radiat. Oncol. Biol. Phys. 2013, 85, e165–e172. [Google Scholar] [CrossRef]
- Bao, A.; Barsky, A.R.; Both, S.; Christodouleas, J.P.; Deville, C., Jr.; Tochner, Z.A.; Vapiwala, N.; Maxwell, R. Case-Matched Outcomes of Proton Beam and Intensity-Modulated Radiation Therapy for Localized Prostate Cancer. Int. J. Part. Ther. 2023, 10, 1–12. [Google Scholar] [CrossRef]
- Waddle, M.R.; Sio, T.T.; Van Houten, H.K.; Foote, R.L.; Keole, S.R.; Schild, S.E.; Laack, N.; Daniels, T.B.; Crown, W.; Shah, N.D.; et al. Photon and Proton Radiation Therapy Utilization in a Population of More Than 100 Million Commercially Insured Patients. Int. J. Radiat. Oncol. Biol. Phys. 2017, 99, 1078–1082. [Google Scholar] [CrossRef]
- Ning, M.; Gomez, D.; Shah, A.; Kim, C.; Palmer, M.; Thaker, N.; Grosshans, D.; Liao, Z.; Chapman, B.; Brooks, E.; et al. The Insurance Approval Process for Proton Radiation Therapy: A Significant Barrier to Patient Care. Int. J. Radiat. Oncol. Biol. Phys. 2019, 104, 724–733. [Google Scholar] [CrossRef]
- Gupta, A.; Khan, A.J.; Goyal, S.; Millevoi, R.; Elsebai, N.; Jabbour, S.K.; Yue, N.J.; Haffty, B.G.; Parikh, R.R. Insurance Approval for Proton Beam Therapy and its Impact on Delays in Treatment. Int. J. Radiat. Oncol. Biol. Phys. 2019, 104, 714–723. [Google Scholar] [CrossRef]
- Pan, H.Y.; Jiang, J.; Hoffman, K.E.; Tang, C.; Choi, S.L.; Nguyen, Q.-N.; Frank, S.J.; Anscher, M.S.; Shih, Y.-C.T.; Smith, B.D. Comparative toxicities and cost of intensity-modulated radiotherapy, proton radiation, and stereotactic body radiotherapy among younger men with prostate cancer. J. Clin. Oncol. 2018, 36, 1823–1830. [Google Scholar] [CrossRef] [PubMed]
- Ferini, G.; Tripoli, A.; Molino, L.; Cacciola, A.; Lillo, S.; Parisi, S.; Umina, V.; Illari, S.I.; Marchese, V.A.; Cravagno, I.R.; et al. How Much Daily Image-guided Volumetric Modulated Arc Therapy Is Useful for Proctitis Prevention With Respect to Static Intensity Modulated Radiotherapy Supported by Topical Medications Among Localized Prostate Cancer Patients? Anticancer Res. 2021, 41, 2101–2110. [Google Scholar] [CrossRef] [PubMed]
- Alongi, F.; Rigo, M.; Figlia, V.; Cuccia, F.; Giaj-Levra, N.; Nicosia, L.; Ricchetti, F.; Sicignano, G.; De Simone, A.; Naccarato, S.; et al. 1.5 T MR-guided and daily adapted SBRT for prostate cancer: Feasibility, preliminary clinical tolerability, quality of life and patient-reported outcomes during treatment. Radiat. Oncol. 2020, 15, 69. [Google Scholar] [CrossRef] [PubMed] [PubMed Central]
- Podder, T.K.; Fredman, E.T.; Ellis, R.J. Advances in Radiotherapy for Prostate Cancer Treatment. Adv. Exp. Med. Biol. 2018, 1096, 31–47. [Google Scholar] [CrossRef] [PubMed]
- Shen, C.J.; Hu, C.; Ladra, M.M.; Narang, A.K.; Pollack, C.E.; Terezakis, S.A. Socioeconomic factors affect the selection of proton radiation therapy for children. Cancer 2017, 123, 4048–4056. [Google Scholar] [CrossRef]
- Xiang, M.; Chang, D.T.; Pollom, E.L. Second cancer risk after primary cancer treatment with three-dimensional conformal, intensity-modulated, or proton beam radiation therapy. Cancer 2020, 126, 3560–3568. [Google Scholar] [CrossRef]
- Hutchins, L.F.; Unger, J.M.; Crowley, J.J.; Coltman, C.A.J.; Albain, K.S. Underrepresentation of patients 65 years of age or older in cancer-treatment trials. N. Engl. J. Med. 1999, 341, 2061–2067. [Google Scholar] [CrossRef]
- Scher, K.S.; Hurria, A. Under-representation of older adults in cancer registration trials: Known problem, little progress. J. Clin. Oncol. 2012, 30, 2036–2038. [Google Scholar] [CrossRef]
- Burus, T.; VanHelene, A.D.; Rooney, M.K.; Kuhs, K.A.L.; Christian, W.J.; McNair, C.; Mishra, S.; Paulino, A.C.; Smith, G.L.; Frank, S.J.; et al. Travel-Time Disparities in Access to Proton Beam Therapy for Cancer Treatment. JAMA Netw. Open 2024, 7, e2410670. [Google Scholar] [CrossRef]
- Agarwal, A.; Peterson, J.; Hoyle, L.M.; Marks, L.B. Variations in Medicaid Payment Rates for Radiation Oncology. Int. J. Radiat. Oncol. Biol. Phys. 2019, 104, 488–493. [Google Scholar] [CrossRef]
- Roach, M.C.; Thomas, T.O.; Paravati, A.J.; Mahajan, A. Differences in United States insurance payer policies and American Society for Radiation Oncology’s (ASTRO) model policy on stereotactic body radiation therapy (SBRT). Int. J. Radiat. Oncol. Biol. Phys. 2019, 104, 740–744. [Google Scholar] [CrossRef]
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).