
Dosimetric and Clinical Prognostic Factors in Single-Isocenter Linac-Based Stereotactic Radiotherapy for Brain Metastases

 , ,
, ,  and
and
Abstract
Simple Summary
Abstract
1. Introduction
2. Materials and Methods
2.1. Patient Population
2.2. Simulation, Planning, and Treatment
2.3. Clinical and Dosimetric Outcomes
2.4. Statistical Analysis
3. Results
3.1. Population Characteristics
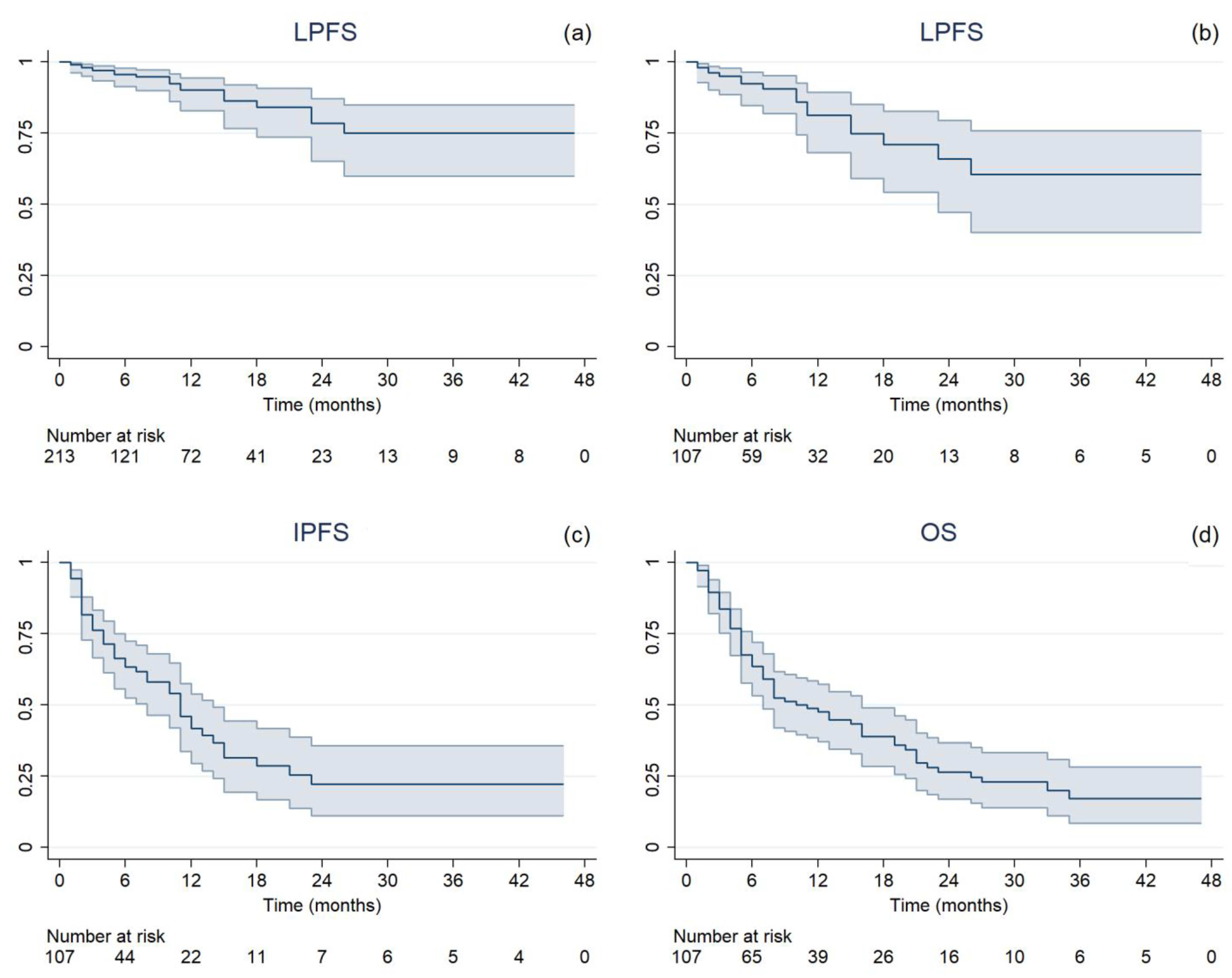
3.2. Treatment Outcomes
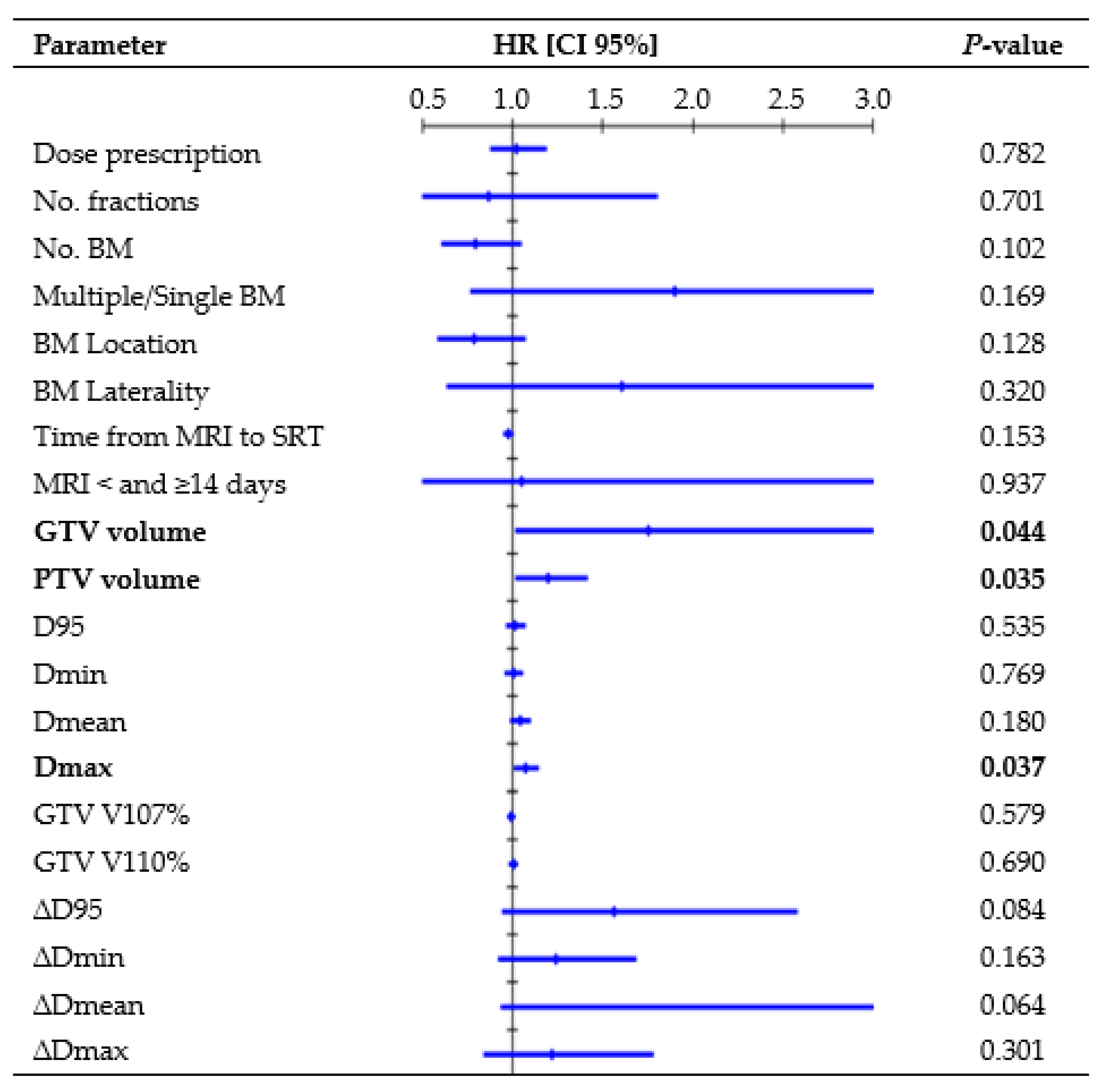
3.3. Prognostic Factors
3.3.1. LPFS Analysis per Single Lesion
3.3.2. LPFS Analysis per Treatment
3.3.3. IPFS Analysis per Treatment
3.3.4. OS Analysis per Treatment
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Muldoon, L.L.; Soussain, C.; Jahnke, K.; Johanson, C.; Siegal, T.; Smith, Q.R.; Hall, W.A.; Hynynen, K.; Senter, P.D.; Peereboom, D.M.; et al. Chemotherapy delivery issues in central nervous system malignancy: A reality check. J. Clin. Oncol. 2007, 25, 2295–2305. [Google Scholar] [CrossRef] [PubMed]
- Amaral, T.; Kiecker, F.; Schaefer, S.; Stege, H.; Kaehler, K.; Terheyden, P.; Gesierich, A.; Gutzmer, R.; Haferkamp, S.; Uttikal, J.; et al. Combined immunotherapy with nivolumab and ipilimumab with and without local therapy in patients with melanoma brain metastasis: A DeCOG* study in 380 patients. J. Immunother. Cancer 2020, 8, e000333. [Google Scholar] [CrossRef]
- Altan, M.; Wang, Y.; Song, J.; Welsh, J.; Tang, C.; Guha-Thakurta, N.; Blumenschein, G.R.; Carter, B.W.; Wefel, J.S.; Ghia, A.J.; et al. Nivolumab and ipilimumab with concurrent stereotactic radiosurgery for intracranial metastases from non-small cell lung cancer: Analysis of the safety cohort for non-randomized, open-label, phase I/II trial. J. Immunother. Cancer 2023, 11, e006871, Erratum in J. Immunother. Cancer 2023, 11, e006871corr1. [Google Scholar] [CrossRef] [PubMed]
- Vaios, E.J.; Shenker, R.F.; Hendrickson, P.G.; Wan, Z.; Niedzwiecki, D.; Winter, S.F.; Shih, H.A.; Dietrich, J.; Wang, C.; Salama, A.K.S.; et al. Long-Term Intracranial Outcomes with Combination Dual Immune-Checkpoint Blockade and Stereotactic Radiosurgery in Patients with Melanoma and Non-Small Cell Lung Cancer Brain Metastases. Int. J. Radiat. Oncol. Biol. Phys. 2024, 118, 1507–1518. [Google Scholar] [CrossRef] [PubMed]
- Corrao, G.; Franchi, M.; Zaffaroni, M.; Vincini, M.G.; de Marinis, F.; Spaggiari, L.; Orecchia, R.; Marvaso, G.; Jereczek-Fossa, B.A. Upfront Advanced Radiotherapy and New Drugs for NSCLC Patients with Synchronous Brain Metastases: Is the Juice Worth the Squeeze? A Real-World Analysis from Lombardy, Italy. Cancers 2023, 15, 1103. [Google Scholar] [CrossRef]
- Koide, Y.; Nagai, N.; Miyauchi, R.; Kitagawa, T.; Aoyama, T.; Shimizu, H.; Tachibana, H.; Kodaira, T. Radiotherapy or systemic therapy versus combined therapy in patients with brain metastases: A propensity-score matched study. J. Neurooncol. 2022, 160, 191–200. [Google Scholar] [CrossRef] [PubMed]
- Gondi, V.; Bauman, G.; Bradfield, L.; Burri, S.H.; Cabrera, A.R.; Cunningham, D.A.; Eaton, B.R.; Hattangadi-Gluth, J.A.; Kim, M.M.; Kotecha, R.; et al. Radiation Therapy for Brain Metastases: An ASTRO Clinical Practice Guideline. Pract. Radiat. Oncol. 2022, 12, 265–282. [Google Scholar] [CrossRef] [PubMed]
- Susko, M.S.; Garcia, M.A.; Ma, L.; Nakamura, J.L.; Raleigh, D.R.; Fogh, S.; Theodosopoulos, P.; McDermott, M.; Sneed, P.K.; Braunstein, S.E. Stereotactic Radiosurgery to More Than 10 Brain Metastases: Evidence to Support the Role of Radiosurgery for Ideal Hippocampal Sparing in the Treatment of Multiple Brain Metastases. World Neurosurg. 2020, 135, e174–e180. [Google Scholar] [CrossRef]
- Vogelbaum, M.A.; Brown, P.D.; Messersmith, H.; Brastianos, P.K.; Burri, S.; Cahill, D.; Dunn, I.F.; Gaspar, L.E.; Gatson, N.T.N.; Gondi, V.; et al. Treatment for Brain Metastases: ASCO-SNO-ASTRO Guideline. J. Clin. Oncol. 2022, 40, 492–516, Erratum in J. Clin. Oncol. 2022, 40, 1392. [Google Scholar] [CrossRef]
- Le Rhun, E.; Guckenberger, M.; Smits, M.; Dummer, R.; Bachelot, T.; Sahm, F.; Galldiks, N.; de Azambuja, E.; Berghoff, A.S.; Metellus, P.; et al. EANO-ESMO Clinical Practice Guidelines for diagnosis, treatment and follow-up of patients with brain metastasis from solid tumours. Ann. Oncol. 2021, 32, 1332–1347. [Google Scholar] [CrossRef]
- Grishchuk, D.; Dimitriadis, A.; Sahgal, A.; De Salles, A.; Fariselli, L.; Kotecha, R.; Levivier, M.; Ma, L.; Pollock, B.E.; Regis, J.; et al. ISRS Technical Guidelines for Stereotactic Radiosurgery: Treatment of Small Brain Metastases (≤1 cm in Diameter). Pract. Radiat. Oncol. 2023, 13, 183–194. [Google Scholar] [CrossRef] [PubMed]
- Redmond, K.J.; Gui, C.; Benedict, S.; Milano, M.T.; Grimm, J.; Vargo, J.A.; Soltys, S.G.; Yorke, E.; Jackson, A.; El Naqa, I.; et al. Tumor Control Probability of Radiosurgery and Fractionated Stereotactic Radiosurgery for Brain Metastases. Int. J. Radiat. Oncol. Biol. Phys. 2021, 110, 53–67. [Google Scholar] [CrossRef] [PubMed]
- Rahimy, E.; Soltys, S.G. Stereotactic Radiosurgery for Brain Metastases: Review of Existing Data and Future Directions. Appl. Radiat. Oncol. 2023, 2, 5–14. [Google Scholar] [CrossRef]
- Minniti, G.; Scaringi, C.; Paolini, S.; Lanzetta, G.; Romano, A.; Cicone, F.; Osti, M.; Enrici, R.M.; Esposito, V. Single-Fraction Versus Multifraction (3 × 9 Gy) Stereotactic Radiosurgery for Large (>2 cm) Brain Metastases: A Comparative Analysis of Local Control and Risk of Radiation-Induced Brain Necrosis. Int. J. Radiat. Oncol. Biol. Phys. 2016, 95, 1142–1148. [Google Scholar] [CrossRef] [PubMed]
- Shaw, E.; Scott, C.; Souhami, L.; Dinapoli, R.; Kline, R.; Loeffler, J.; Farnan, N. Single dose radiosurgical treatment of recurrent previously irradiated primary brain tumors and brain metastases: Final report of RTOG protocol 90-05. Int. J. Radiat. Oncol. Biol. Phys. 2000, 47, 291–298. [Google Scholar] [CrossRef]
- Minniti, G.; Clarke, E.; Lanzetta, G.; Osti, M.F.; Trasimeni, G.; Bozzao, A.; Romano, A.; Enrici, R.M. Stereotactic radiosurgery for brain metastases: Analysis of outcome and risk of brain radionecrosis. Radiat. Oncol. 2011, 6, 48. [Google Scholar] [CrossRef]
- Stelzer, K.J. Epidemiology and prognosis of brain metastases. Surg. Neurol. Int. 2013, 4 (Suppl. 4), S192–S202. [Google Scholar] [CrossRef]
- Venur, V.A.; Ahluwalia, M.S. Prognostic scores for brain metastasis patients: Use in clinical practice and trial design. Chin. Clin. Oncol. 2015, 4, 18. [Google Scholar] [CrossRef]
- Sperduto, P.W.; Berkey, B.; Gaspar, L.E.; Mehta, M.; Curran, W. A new prognostic index and comparison to three other indices for patients with brain metastases: An analysis of 1,960 patients in the RTOG database. Int. J. Radiat. Oncol. Biol. Phys. 2008, 70, 510–514. [Google Scholar] [CrossRef]
- Sperduto, P.W.; Chao, S.T.; Sneed, P.K.; Luo, X.; Suh, J.; Toberge, D.; Bhatt, A.; Jensen, A.W.; Brown, P.D.; Shih, H.; et al. Diagnosis-specific prognostic factors, indexes, and treatment outcomes for patients with newly diagnosed brain metastases: A multi-institutional analysis of 4259 patients. Int. J. Radiat. Oncol. Biol. Phys. 2010, 77, 655–661. [Google Scholar] [CrossRef]
- Faccenda, V.; Panizza, D.; Pisoni, V.; Trivellato, S.; Daniotti, M.C.; Bianchi, S.P.; De Ponti, E.; Arcangeli, S. Single-Isocenter Linac-Based Radiosurgery for Brain Metastases with Coplanar Arcs: A Dosimetric and Clinical Analysis. Cancers 2023, 15, 4496. [Google Scholar] [CrossRef] [PubMed]
- Grimm, J.; Marks, L.B.; Jackson, A.; Kavanagh, B.D.; Xue, J.; Yorke, E. High Dose per Fraction, Hypofractionated Treatment Effects in the Clinic (HyTEC): An Overview. Int. J. Radiat. Oncol. Biol. Phys. 2021, 110, 1–10. [Google Scholar] [CrossRef] [PubMed]
- Chukwueke, U.N.; Wen, P.Y. Use of the Response Assessment in Neuro-Oncology (RANO) criteria in clinical trials and clinical practice. CNS Oncol. 2019, 8, CNS28. [Google Scholar] [CrossRef] [PubMed]
- Nicosia, L.; Navarria, P.; Pinzi, V.; Giraffa, M.; Russo, I.; Tini, P.; Giaj-Levra, N.; Alongi, F.; Minniti, G. Stereotactic radiosurgery for the treatment of brainstem metastases: A multicenter retrospective study. Radiat. Oncol. 2022, 17, 140. [Google Scholar] [CrossRef] [PubMed]
- Leyrat, B.; Khalill, T.; Lemaire, J.J.; Casile, M.; Molnar, I.; Dedieu, V.; Chassin, V.; Dupic, G.; Bellière, A.; Durando, X.; et al. Local control and radionecrosis of brain metastases from non-small-cell lung cancer treated by hypofractionated stereotactic radiotherapy: Evaluation of predictive factors. Clin. Transl. Radiat. Oncol. 2022, 6, 1–8. [Google Scholar] [CrossRef] [PubMed]
- Wiggenraad, R.; Verbeek-de Kanter, A.; Kal, H.B.; Taphoorn, M.; Vissers, T.; Struikmans, H. Dose-effect relation in stereotactic radiotherapy for brain metastases. A systematic review. Radiother. Oncol. 2011, 98, 292–297. [Google Scholar] [CrossRef]
- Loo, M.; Clavier, J.B.; Attal Khalifa, J.; Moyal, E.; Khalifa, J. Dose-Response Effect and Dose-Toxicity in Stereotactic Radiotherapy for Brain Metastases: A Review. Cancers 2021, 13, 6086. [Google Scholar] [CrossRef]
- De Azevedo Santos, T.R.; Tundisi, C.F.; Ramos, H.; Maia, M.A.; Pellizzon, A.C.; Silva, M.L.; Fogaroli, R.C.; Chen, M.J.; Suzuki, S.H.; Dias, J.E., Jr.; et al. Local control after radiosurgery for brain metastases: Predictive factors and implications for clinical decision. Radiat. Oncol. 2015, 10, 63. [Google Scholar] [CrossRef]
- Berthet, C.; Lucia, F.; Bourbonne, V.; Schick, U.; Lecouillard, I.; Le Deroff, C.; Barateau, A.; de Crevoisier, R.; Castelli, J. The dosimetric parameters impact on local recurrence in stereotactic radiotherapy for brain metastases. Br. J. Radiol. 2024, 97, 820–827. [Google Scholar] [CrossRef]
- Alongi, F.; Nicosia, L.; Figlia, V.; Giaj-Levra, N.; Cuccia, F.; Mazzola, R.; Ricchetti, F.; Rigo, M.; Vitale, C.; De Simone, A.; et al. Long-term disease outcome and volume-based decision strategy in a large cohort of multiple brain metastases treated with a mono-isocentric linac-based Stereotactic Radiosurgery technique. Clin. Transl. Oncol. 2021, 23, 1561–1570. [Google Scholar] [CrossRef]
- Reinhardt, P.; Ahmadli, U.; Uysal, E.; Shrestha, B.K.; Schucht, P.; Hakim, A.; Ermiş, E. Single versus multiple fraction stereotactic radiosurgery for medium-sized brain metastases (4–14 cc in volume): Reducing or fractionating the radiosurgery dose? Front. Oncol. 2024, 14, 1333245. [Google Scholar] [CrossRef] [PubMed]
- Bodensohn, R.; Maier, S.H.; Belka, C.; Minniti, G.; Niyazi, M. Stereotactic Radiosurgery of Multiple Brain Metastases: A Review of Treatment Techniques. Cancers 2023, 15, 5404. [Google Scholar] [CrossRef] [PubMed]
- Sahgal, A.; Aoyama, H.; Kocher, M.; Neupane, B.; Collette, S.; Tago, M.; Shaw, P.; Beyene, J.; Chang, E.L. Phase 3 trials of stereotactic radiosurgery with or without whole-brain radiation therapy for 1 to 4 brain metastases: Individual patient data meta-analysis. Int. J. Radiat. Oncol. Biol. Phys. 2015, 91, 710–717. [Google Scholar] [CrossRef] [PubMed]
- Seymour, Z.A.; Fogh, S.E.; Westcott, S.K.; Braunstein, S.; Larson, D.A.; Barani, I.J.; Nakamura, J.; Sneed, P.K. Interval from Imaging to Treatment Delivery in the Radiation Surgery Age: How Long Is Too Long? Int. J. Radiat. Oncol. Biol. Phys. 2015, 93, 126–132. [Google Scholar] [CrossRef] [PubMed]
- Kutuk, T.; Tolakanahalli, R.; Williams, A.; Tom, M.C.; Vadhan, J.D.; Appel, H.; Hall, M.D.; Wieczorek, D.J.J.; Davis, S.; McDermott, M.W.; et al. Impact of MRI timing on tumor volume and anatomic displacement for brain metastases undergoing stereotactic radiosurgery. Neurooncol. Pract. 2021, 8, 674–683. [Google Scholar] [CrossRef]
- Sandström, H.; Jokura, H.; Chung, C.; Toma-Dasu, I. Multi-institutional study of the variability in target delineation for six targets commonly treated with radiosurgery. Acta Oncol. 2018, 57, 1515–1520. [Google Scholar] [CrossRef]
- Growcott, S.; Dembrey, T.; Patel, R.; Eaton, D.; Cameron, A. Inter-Observer Variability in Target Volume Delineations of Benign and Metastatic Brain Tumours for Stereotactic Radiosurgery: Results of a National Quality Assurance Programme. Clin. Oncol. (R. Coll. Radiol.) 2020, 32, 13–25. [Google Scholar] [CrossRef]
- Barillaro, A.; Caroprese, M.; Cella, L.; Viggiano, A.; Buccelli, F.; Daponte, C.; Feoli, C.; Oliviero, C.; Clemente, S.; Farella, A.; et al. Stereotactic Radiation Therapy for Brain Metastases: Factors Affecting Outcomes and Radiation Necrosis. Cancers 2023, 15, 2094. [Google Scholar] [CrossRef]
- Singh, C.; Qian, J.M.; Yu, J.B.; Chiang, V.L. Local tumor response and survival outcomes after combined stereotactic radiosurgery and immunotherapy in non-small cell lung cancer with brain metastases. J. Neurosurg. 2019, 132, 512–517. [Google Scholar] [CrossRef]
- Ali, M.A.; Hirshman, B.R.; Wilson, B.; Carroll, K.T.; Proudfoot, J.A.; Goetsch, S.J.; Alksne, J.F.; Ott, K.; Aiyama, H.; Nagano, O.; et al. Survival Patterns of 5750 Stereotactic Radiosurgery-Treated Patients with Brain Metastasis as a Function of the Number of Lesions. World Neurosurg. 2017, 107, 944–951.e1. [Google Scholar] [CrossRef]
- Minniti, G.; Capone, L.; Alongi, F.; Figlia, V.; Nardiello, B.; El Gawhary, R.; Scaringi, C.; Bianciardi, F.; Tolu, B.; Gentile, P.; et al. Initial Experience with Single-Isocenter Radiosurgery to Target Multiple Brain Metastases Using an Automated Treatment Planning Software: Clinical Outcomes and Optimal Target Volume Margins Strategy. Adv. Radiat. Oncol. 2020, 5, 856–864. [Google Scholar] [CrossRef] [PubMed]
- Palmer, J.D.; Sebastian, N.T.; Chu, J.; DiCostanzo, D.; Bell, E.H.; Grecula, J.; Arnett, A.; Blakaj, D.M.; McGregor, J.; Elder, J.B.; et al. Single-Isocenter Multitarget Stereotactic Radiosurgery Is Safe and Effective in the Treatment of Multiple Brain Metastases. Adv. Radiat. Oncol. 2019, 5, 70–76. [Google Scholar] [CrossRef] [PubMed]


{kind=link}
{kind=link}
{kind=link}
| Parameter | No. | |
|---|---|---|
| Number of patients | 100 | |
| Primary origin tumor | Lung | 53 |
| Melanoma | 18 | |
| Breast | 17 | |
| Other | 12 | |
| Histological type | Adenocarcinoma | 66 |
| Melanoma | 18 | |
| Squamous Cell | 7 | |
| Other | 9 | |
| Mutations * | Wild-Type | 49 |
| PD-L1 | 29 (56.9%) | |
| EGFR | 9 (17.6%) | |
| BRAF | 8 (15.7%) | |
| HER2 | 6 (11.8%) | |
| ALK | 3 (5.9%) | |
| PS ECOG | 0 | 33 |
| 1 | 52 | |
| 2 | 12 | |
| 3 | 1 | |
| Median time from the diagnosis of the primary tumor to BM [range] | 23 months [0–312] | |
| Timing of BM | Synchronous | 69 |
| Metachronous | 31 | |
| Polymetastatic progression | Yes | 40 |
| No | 60 | |
| Pre-RT ST | Yes | 70 |
| No | 30 | |
| Pre-RT ST regimen ** | Chemotherapy | 25 (35.7%) |
| Immunotherapy | 26 (37.1%) | |
| Targeted therapy | 15 (21.4%) | |
| Hormonal therapy | 4 (5.7%) | |
| No. of systemic line ** | First-line | 43 (61.4%) |
| Second-line | 18 (25.7%) | |
| Third-line or higher | 9 (12.9%) |
| Parameter | Planned Dose | Delivered Dose | Difference | Planned BED10 | Delivered BED10 | Difference |
|---|---|---|---|---|---|---|
| GTV D95% | 21.2 Gy | 20.9 Gy | −0.3% | 62.5 Gy | 61.3 Gy | −0.5% |
| [11.1–28.9] | [11.2–28.6] | [−14.8–2.2] | [23.9–73.1] | [23.8–72.7] | [−22.9–3.6] | |
| GTV D99% | 20.9 Gy | 20.6 Gy | −0.4% | 61.0 Gy | 59.5 Gy | −0.6% |
| [9.8–28.8.] | [9.8–28.4] | [−14.9–4.5] | [19.4–73.1] | [19.5–72.7] | [−22.9–1.4] | |
| GTV Dmean | 21.8 Gy | 21.7 Gy | −0.1% | 66.9 Gy | 66.9 Gy | −0.1% |
| [14.8–30] | [14.7–29.4] | [−6.0–0.9] | [36.6–76.4] | [36.4–76] | [−9.9–1.4] | |
| GTV D0.035 cc | 22.5 Gy | 22.3 Gy | 0.0% | 69.8 Gy | 69.6 Gy | −0.1% |
| [15.0–30.9] | [15.0–30.9] | [−6.7–5.2] | [37.7–80.8] | [37.6–81.7] | [−11.0–−0.3] | |
| GTV V107% | 15.4% | 8.7% | – | – | – | – |
| [0.0–100] | [0.0–94.7] | |||||
| GTV V110% | 0.0% | 0.0% | – | – | – | – |
| [0.0–82.9] | [0.0–62.5] |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Faccenda, V.; Colciago, R.R.; Bianchi, S.P.; De Ponti, E.; Panizza, D.; Arcangeli, S. Dosimetric and Clinical Prognostic Factors in Single-Isocenter Linac-Based Stereotactic Radiotherapy for Brain Metastases. Cancers 2024, 16, 3243. https://doi.org/10.3390/cancers16183243
Faccenda V, Colciago RR, Bianchi SP, De Ponti E, Panizza D, Arcangeli S. Dosimetric and Clinical Prognostic Factors in Single-Isocenter Linac-Based Stereotactic Radiotherapy for Brain Metastases. Cancers. 2024; 16(18):3243. https://doi.org/10.3390/cancers16183243
Chicago/Turabian StyleFaccenda, Valeria, Riccardo Ray Colciago, Sofia Paola Bianchi, Elena De Ponti, Denis Panizza, and Stefano Arcangeli. 2024. "Dosimetric and Clinical Prognostic Factors in Single-Isocenter Linac-Based Stereotactic Radiotherapy for Brain Metastases" Cancers 16, no. 18: 3243. https://doi.org/10.3390/cancers16183243
APA StyleFaccenda, V., Colciago, R. R., Bianchi, S. P., De Ponti, E., Panizza, D., & Arcangeli, S. (2024). Dosimetric and Clinical Prognostic Factors in Single-Isocenter Linac-Based Stereotactic Radiotherapy for Brain Metastases. Cancers, 16(18), 3243. https://doi.org/10.3390/cancers16183243