
Antibody-Drug Conjugates: The New Treatment Approaches for Ovarian Cancer

 , , , and
, , , and
Abstract
Simple Summary
Abstract
1. Introduction
2. Mechanisms of ADCs
3. Evidence of ADC efficacy
3.1. The Effectiveness of ADCs against Gynecologic Cancers
3.2. The Effectiveness of ADCs Efficacy against OC
4. ADCs as a Promising Treatment for Patients with OC
5. Treatment-Related Adverse Events with ADCs
6. The New Development of ADCs for OC
6.1. Potential of Combining ADCs with Other Agents to Treat OC
6.2. Challenges for Resistance to ADCs
7. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Huang, J.; Chan, W.C.; Ngai, C.H.; Lok, V.; Zhang, L.; Lucero-Prisno, D.E., 3rd; Xu, W.; Zheng, Z.J.; Elcarte, E.; Withers, M.; et al. Worldwide Burden, Risk Factors, and Temporal Trends of Ovarian Cancer: A Global Study. Cancers 2022, 14, 2230. [Google Scholar] [CrossRef] [PubMed]
- Siegel, R.L.; Giaquinto, A.N.; Jemal, A. Cancer statistics, 2024. CA A Cancer J. Clin. 2024, 74, 12–49. [Google Scholar] [CrossRef] [PubMed]
- Karst, A.M.; Drapkin, R. Ovarian cancer pathogenesis: A model in evolution. J. Oncol. 2010, 2010, 932371. [Google Scholar] [CrossRef] [PubMed]
- Burger, R.A.; Brady, M.F.; Bookman, M.A.; Fleming, G.F.; Monk, B.J.; Huang, H.; Mannel, R.S.; Homesley, H.D.; Fowler, J.; Greer, B.E.; et al. Incorporation of bevacizumab in the primary treatment of ovarian cancer. N. Engl. J. Med. 2011, 365, 2473–2483. [Google Scholar] [CrossRef] [PubMed]
- Oza, A.M.; Cook, A.D.; Pfisterer, J.; Embleton, A.; Ledermann, J.A.; Pujade-Lauraine, E.; Kristensen, G.; Carey, M.S.; Beale, P.; Cervantes, A.; et al. Standard chemotherapy with or without bevacizumab for women with newly diagnosed ovarian cancer (ICON7): Overall survival results of a phase 3 randomised trial. Lancet Oncol. 2015, 16, 928–936. [Google Scholar] [CrossRef] [PubMed]
- Moore, K.; Colombo, N.; Scambia, G.; Kim, B.-G.; Oaknin, A.; Friedlander, M.; Lisyanskaya, A.; Floquet, A.; Leary, A.; Sonke, G.S.; et al. Maintenance Olaparib in Patients with Newly Diagnosed Advanced Ovarian Cancer. N. Engl. J. Med. 2018, 379, 2495–2505. [Google Scholar] [CrossRef] [PubMed]
- González-Martín, A.; Pothuri, B.; Vergote, I.; DePont Christensen, R.; Graybill, W.; Mirza, M.R.; McCormick, C.; Lorusso, D.; Hoskins, P.; Freyer, G.; et al. Niraparib in Patients with Newly Diagnosed Advanced Ovarian Cancer. N. Engl. J. Med. 2019, 381, 2391–2402. [Google Scholar] [CrossRef] [PubMed]
- Ray-Coquard, I.; Pautier, P.; Pignata, S.; Pérol, D.; González-Martín, A.; Berger, R.; Fujiwara, K.; Vergote, I.; Colombo, N.; Mäenpää, J.; et al. Olaparib plus Bevacizumab as First-Line Maintenance in Ovarian Cancer. N. Engl. J. Med. 2019, 381, 2416–2428. [Google Scholar] [CrossRef] [PubMed]
- Parmar, M.K.; Ledermann, J.A.; Colombo, N.; du Bois, A.; Delaloye, J.F.; Kristensen, G.B.; Wheeler, S.; Swart, A.M.; Qian, W.; Torri, V.; et al. Paclitaxel plus platinum-based chemotherapy versus conventional platinum-based chemotherapy in women with relapsed ovarian cancer: The ICON4/AGO-OVAR-2.2 trial. Lancet 2003, 361, 2099–2106. [Google Scholar] [CrossRef]
- Pfisterer, J.; Plante, M.; Vergote, I.; Bois, A.d.; Hirte, H.; Lacave, A.J.; Wagner, U.; Stähle, A.; Stuart, G.; Kimmig, R.; et al. Gemcitabine Plus Carboplatin Compared with Carboplatin in Patients with Platinum-Sensitive Recurrent Ovarian Cancer: An Intergroup Trial of the AGO-OVAR, the NCIC CTG, and the EORTC GCG. J. Clin. Oncol. 2006, 24, 4699–4707. [Google Scholar] [CrossRef]
- Pujade-Lauraine, E.; Wagner, U.; Aavall-Lundqvist, E.; Gebski, V.; Heywood, M.; Vasey, P.A.; Volgger, B.; Vergote, I.; Pignata, S.; Ferrero, A.; et al. Pegylated Liposomal Doxorubicin and Carboplatin Compared with Paclitaxel and Carboplatin for Patients with Platinum-Sensitive Ovarian Cancer in Late Relapse. J. Clin. Oncol. 2010, 28, 3323–3329. [Google Scholar] [CrossRef] [PubMed]
- Aghajanian, C.; Blank, S.V.; Goff, B.A.; Judson, P.L.; Teneriello, M.G.; Husain, A.; Sovak, M.A.; Yi, J.; Nycum, L.R. OCEANS: A Randomized, Double-Blind, Placebo-Controlled Phase III Trial of Chemotherapy with or Without Bevacizumab in Patients with Platinum-Sensitive Recurrent Epithelial Ovarian, Primary Peritoneal, or Fallopian Tube Cancer. J. Clin. Oncol. 2012, 30, 2039–2045. [Google Scholar] [CrossRef]
- Coleman, R.L.; Brady, M.F.; Herzog, T.J.; Sabbatini, P.; Armstrong, D.K.; Walker, J.L.; Kim, B.G.; Fujiwara, K.; Tewari, K.S.; O’Malley, D.M.; et al. Bevacizumab and paclitaxel-carboplatin chemotherapy and secondary cytoreduction in recurrent, platinum-sensitive ovarian cancer (NRG Oncology/Gynecologic Oncology Group study GOG-0213): A multicentre, open-label, randomised, phase 3 trial. Lancet Oncol. 2017, 18, 779–791. [Google Scholar] [CrossRef] [PubMed]
- Pfisterer, J.; Shannon, C.M.; Baumann, K.; Rau, J.; Harter, P.; Joly, F.; Sehouli, J.; Canzler, U.; Schmalfeldt, B.; Dean, A.P.; et al. Bevacizumab and platinum-based combinations for recurrent ovarian cancer: A randomised, open-label, phase 3 trial. Lancet Oncol. 2020, 21, 699–709. [Google Scholar] [CrossRef] [PubMed]
- Mirza, M.R.; Monk, B.J.; Herrstedt, J.; Oza, A.M.; Mahner, S.; Redondo, A.; Fabbro, M.; Ledermann, J.A.; Lorusso, D.; Vergote, I.; et al. Niraparib Maintenance Therapy in Platinum-Sensitive, Recurrent Ovarian Cancer. N. Engl. J. Med. 2016, 375, 2154–2164. [Google Scholar] [CrossRef] [PubMed]
- Pujade-Lauraine, E.; Ledermann, J.A.; Selle, F.; Gebski, V.; Penson, R.T.; Oza, A.M.; Korach, J.; Huzarski, T.; Poveda, A.; Pignata, S.; et al. Olaparib tablets as maintenance therapy in patients with platinum-sensitive, relapsed ovarian cancer and a BRCA1/2 mutation (SOLO2/ENGOT-Ov21): A double-blind, randomised, placebo-controlled, phase 3 trial. Lancet Oncol. 2017, 18, 1274–1284. [Google Scholar] [CrossRef] [PubMed]
- Sehouli, J.; Stengel, D.; Oskay-Oezcelik, G.; Zeimet, A.G.; Sommer, H.; Klare, P.; Stauch, M.; Paulenz, A.; Camara, O.; Keil, E.; et al. Nonplatinum Topotecan Combinations Versus Topotecan Alone for Recurrent Ovarian Cancer: Results of a Phase III Study of the North-Eastern German Society of Gynecological Oncology Ovarian Cancer Study Group. J. Clin. Oncol. 2008, 26, 3176–3182. [Google Scholar] [CrossRef]
- Buda, A.; Floriani, I.; Rossi, R.; Colombo, N.; Torri, V.; Conte, P.F.; Fossati, R.; Ravaioli, A.; Mangioni, C. Randomised controlled trial comparing single agent paclitaxel vs epidoxorubicin plus paclitaxel in patients with advanced ovarian cancer in early progression after platinum-based chemotherapy: An Italian Collaborative Study from the ‘Mario Negri’ Institute, Milan, G.O.N.O. (Gruppo Oncologico Nord Ovest) group and I.O.R. (Istituto Oncologico Romagnolo) group. Br. J. Cancer 2004, 90, 2112–2117. [Google Scholar] [CrossRef]
- Gordon, A.N.; Tonda, M.; Sun, S.; Rackoff, W. Long-term survival advantage for women treated with pegylated liposomal doxorubicin compared with topotecan in a phase 3 randomized study of recurrent and refractory epithelial ovarian cancer. Gynecol. Oncol. 2004, 95, 1–8. [Google Scholar] [CrossRef]
- Mutch, D.G.; Orlando, M.; Goss, T.; Teneriello, M.G.; Gordon, A.N.; McMeekin, S.D.; Wang, Y.; Scribner, D.R., Jr.; Marciniack, M.; Naumann, R.W.; et al. Randomized phase III trial of gemcitabine compared with pegylated liposomal doxorubicin in patients with platinum-resistant ovarian cancer. J. Clin. Oncol. 2007, 25, 2811–2818. [Google Scholar] [CrossRef]
- Ferrandina, G.; Ludovisi, M.; Lorusso, D.; Pignata, S.; Breda, E.; Savarese, A.; Medico, P.D.; Scaltriti, L.; Katsaros, D.; Priolo, D.; et al. Phase III Trial of Gemcitabine Compared with Pegylated Liposomal Doxorubicin in Progressive or Recurrent Ovarian Cancer. J. Clin. Oncol. 2008, 26, 890–896. [Google Scholar] [CrossRef]
- Matsumoto, K.; Katsumata, N.; Yamanaka, Y.; Yonemori, K.; Kohno, T.; Shimizu, C.; Andoh, M.; Fujiwara, Y. The safety and efficacy of the weekly dosing of irinotecan for platinum- and taxanes-resistant epithelial ovarian cancer. Gynecol. Oncol. 2006, 100, 412–416. [Google Scholar] [CrossRef]
- Rose, P.G.; Blessing, J.A.; Mayer, A.R.; Homesley, H.D. Prolonged oral etoposide as second-line therapy for platinum-resistant and platinum-sensitive ovarian carcinoma: A Gynecologic Oncology Group study. J. Clin. Oncol. 1998, 16, 405–410. [Google Scholar] [CrossRef] [PubMed]
- ten Bokkel Huinink, W.; Lane, S.R.; Ross, G.A. Long-term survival in a phase III, randomised study of topotecan versus paclitaxel in advanced epithelial ovarian carcinoma. Ann. Oncol. 2004, 15, 100–103. [Google Scholar] [CrossRef] [PubMed]
- Gordon, A.N.; Fleagle, J.T.; Guthrie, D.; Parkin, D.E.; Gore, M.E.; Lacave, A.J. Recurrent epithelial ovarian carcinoma: A randomized phase III study of pegylated liposomal doxorubicin versus topotecan. J. Clin. Oncol. 2001, 19, 3312–3322. [Google Scholar] [CrossRef]
- Katsumata, N.; Tsunematsu, R.; Tanaka, K.; Terashima, Y.; Ogita, S.; Hoshiai, H.; Kohno, I.; Hirabayashi, K.; Yakushiji, M.; Noda, K.; et al. A phase II trial of docetaxel in platinum pre-treated patients with advanced epithelial ovarian cancer: A Japanese Cooperative Study. Ann. Oncol. 2000, 11, 1531–1536. [Google Scholar] [CrossRef]
- Pujade-Lauraine, E.; Hilpert, F.; Weber, B.; Reuss, A.; Poveda, A.; Kristensen, G.; Sorio, R.; Vergote, I.; Witteveen, P.; Bamias, A.; et al. Bevacizumab Combined with Chemotherapy for Platinum-Resistant Recurrent Ovarian Cancer: The AURELIA Open-Label Randomized Phase III Trial. J. Clin. Oncol. 2014, 32, 1302–1308. [Google Scholar] [CrossRef]
- Pujade-Lauraine, E.; Fujiwara, K.; Ledermann, J.A.; Oza, A.M.; Kristeleit, R.; Ray-Coquard, I.-L.; Richardson, G.E.; Sessa, C.; Yonemori, K.; Banerjee, S.; et al. Avelumab alone or in combination with chemotherapy versus chemotherapy alone in platinum-resistant or platinum-refractory ovarian cancer (JAVELIN Ovarian 200): An open-label, three-arm, randomised, phase 3 study. Lancet Oncol. 2021, 22, 1034–1046. [Google Scholar] [CrossRef] [PubMed]
- Hamanishi, J.; Takeshima, N.; Katsumata, N.; Ushijima, K.; Kimura, T.; Takeuchi, S.; Matsumoto, K.; Ito, K.; Mandai, M.; Nakai, H.; et al. Nivolumab Versus Gemcitabine or Pegylated Liposomal Doxorubicin for Patients with Platinum-Resistant Ovarian Cancer: Open-Label, Randomized Trial in Japan (NINJA). J. Clin. Oncol. 2021, 39, 3671–3681. [Google Scholar] [CrossRef]
- Ritchie, M.; Tchistiakova, L.; Scott, N. Implications of receptor-mediated endocytosis and intracellular trafficking dynamics in the development of antibody drug conjugates. MAbs 2013, 5, 13–21. [Google Scholar] [CrossRef]
- Wang, A.-J.; Gao, Y.; Shi, Y.-Y.; Dai, M.-Y.; Cai, H.-B. A review of recent advances on single use of antibody-drug conjugates or combination with tumor immunology therapy for gynecologic cancer. Front. Pharmacol. 2022, 13, 1093666. [Google Scholar] [CrossRef] [PubMed]
- Jain, N.; Smith, S.W.; Ghone, S.; Tomczuk, B. Current ADC Linker Chemistry. Pharm. Res. 2015, 32, 3526–3540. [Google Scholar] [CrossRef] [PubMed]
- Drago, J.Z.; Modi, S.; Chandarlapaty, S. Unlocking the potential of antibody-drug conjugates for cancer therapy. Nat. Rev. Clin. Oncol. 2021, 18, 327–344. [Google Scholar] [CrossRef] [PubMed]
- Pahl, A.; Lutz, C.; Hechler, T. Amanitins and their development as a payload for antibody-drug conjugates. Drug Discov. Today: Technol. 2018, 30, 85–89. [Google Scholar] [CrossRef]
- Chen, H.; Lin, Z.; Arnst, K.E.; Miller, D.D.; Li, W. Tubulin Inhibitor-Based Antibody-Drug Conjugates for Cancer Therapy. Molecules 2017, 22, 1281. [Google Scholar] [CrossRef]
- de Almeida, L.C.; Calil, F.A.; Machado-Neto, J.A.; Costa-Lotufo, L.V. DNA damaging agents and DNA repair: From carcinogenesis to cancer therapy. Cancer Genet. 2021, 252, 6–24. [Google Scholar] [CrossRef] [PubMed]
- Schrama, D.; Reisfeld, R.A.; Becker, J.C. Antibody targeted drugs as cancer therapeutics. Nat. Rev. Drug Discov. 2006, 5, 147–159. [Google Scholar] [CrossRef] [PubMed]
- Birrer, M.J.; Moore, K.N.; Betella, I.; Bates, R.C. Antibody-Drug Conjugate-Based Therapeutics: State of the Science. J. Natl. Cancer Inst. 2019, 111, 538–549. [Google Scholar] [CrossRef] [PubMed]
- Coleman, R.L.; Lorusso, D.; Gennigens, C.; González-Martín, A.; Randall, L.; Cibula, D.; Lund, B.; Woelber, L.; Pignata, S.; Forget, F.; et al. Efficacy and safety of tisotumab vedotin in previously treated recurrent or metastatic cervical cancer (innovaTV 204/GOG-3023/ENGOT-cx6): A multicentre, open-label, single-arm, phase 2 study. Lancet Oncol. 2021, 22, 609–619. [Google Scholar] [CrossRef]
- Vergote, I.B.; Gonzalez Martin, A.; Fujiwara, K.; Kalbacher, E.; Bagameri, A.; Ghamande, S.; Lee, J.Y.; Banerjee, S.; Maluf, F.C.; Lorusso, D.; et al. LBA9 innovaTV 301/ENGOT-cx12/GOG-3057: A global, randomized, open-label, phase III study of tisotumab vedotin vs investigator’s choice of chemotherapy in 2L or 3L recurrent or metastatic cervical cancer. Ann. Oncol. 2023, 34, S1276–S1277. [Google Scholar] [CrossRef]
- Meric-Bernstam, F.; Makker, V.; Oaknin, A.; Oh, D.-Y.; Banerjee, S.; González-Martín, A.; Jung, K.H.; Ługowska, I.; Manso, L.; Manzano, A.; et al. Efficacy and Safety of Trastuzumab Deruxtecan in Patients with HER2-Expressing Solid Tumors: Primary Results from the DESTINY-PanTumor02 Phase II Trial. J. Clin. Oncol. 2024, 42, 47–58. [Google Scholar] [CrossRef] [PubMed]
- Moore, K.N.; Oza, A.M.; Colombo, N.; Oaknin, A.; Scambia, G.; Lorusso, D.; Konecny, G.E.; Banerjee, S.; Murphy, C.G.; Tanyi, J.L.; et al. Phase III, randomized trial of mirvetuximab soravtansine versus chemotherapy in patients with platinum-resistant ovarian cancer: Primary analysis of FORWARD I. Ann. Oncol. 2021, 32, 757–765. [Google Scholar] [CrossRef] [PubMed]
- Moore, K.N.; Angelergues, A.; Konecny, G.E.; García, Y.; Banerjee, S.; Lorusso, D.; Lee, J.Y.; Moroney, J.W.; Colombo, N.; Roszak, A.; et al. Mirvetuximab Soravtansine in FRα-Positive, Platinum-Resistant Ovarian Cancer. N. Engl. J. Med. 2023, 389, 2162–2174. [Google Scholar] [CrossRef] [PubMed]
- Moore, K.; O’Malley, D.; Vergote, I.; Martin, L.; Gonzalez-Martin, A.; Wang, J.; Method, M.; Birrer, M. 18/#499 Mirvetuximab soravtansine and carboplatin for treatment of patients with recurrent folate receptor alpha-positive platinum-sensitive ovarian cancer: A final analysis. Int. J. Gynecol. Cancer 2022, 32, A33–A34. [Google Scholar] [CrossRef]
- Matulonis, U.A.; Lorusso, D.; Oaknin, A.; Pignata, S.; Dean, A.; Denys, H.; Colombo, N.; Gorp, T.V.; Konner, J.A.; Marin, M.R.; et al. Efficacy and Safety of Mirvetuximab Soravtansine in Patients with Platinum-Resistant Ovarian Cancer with High Folate Receptor Alpha Expression: Results from the SORAYA Study. J. Clin. Oncol. 2023, 41, 2436–2445. [Google Scholar] [CrossRef]
- Banerjee, S.; Oza, A.M.; Birrer, M.J.; Hamilton, E.P.; Hasan, J.; Leary, A.; Moore, K.N.; Mackowiak-Matejczyk, B.; Pikiel, J.; Ray-Coquard, I.; et al. Anti-NaPi2b antibody-drug conjugate lifastuzumab vedotin (DNIB0600A) compared with pegylated liposomal doxorubicin in patients with platinum-resistant ovarian cancer in a randomized, open-label, phase II study. Ann. Oncol. 2018, 29, 917–923. [Google Scholar] [CrossRef] [PubMed]
- Lheureux, S.; Alqaisi, H.; Cohn, D.E.; Chern, J.-Y.; Duska, L.R.; Jewell, A.; Corr, B.; Winer, I.S.; Girda, E.; Crispens, M.A.; et al. A randomized phase II study of bevacizumab and weekly anetumab ravtansine or weekly paclitaxel in platinum-resistant or refractory ovarian cancer NCI trial#10150. J Clin Oncol. 2022, 40, 5514. [Google Scholar] [CrossRef]
- Nishikawa, T.; Hasegawa, K.; Matsumoto, K.; Mori, M.; Hirashima, Y.; Takehara, K.; Ariyoshi, K.; Kato, T.; Yagishita, S.; Hamada, A.; et al. Trastuzumab Deruxtecan for Human Epidermal Growth Factor Receptor 2–Expressing Advanced or Recurrent Uterine Carcinosarcoma (NCCH1615): The STATICE Trial. J. Clin. Oncol. 2023, 41, 2789–2799. [Google Scholar] [CrossRef] [PubMed]
- Santin, A.; McNamara, B.; Siegel, E.R.; Harold, J.; Mutlu, L.; Altwerger, G.; Huang, G.S.; Andikyan, V.; Clark, M.B.; Ratner, E.; et al. Preliminary results of a phase II trial with sacituzumab govitecan-hziy in patients with recurrent endometrial carcinoma overexpressing Trop-2. J. Clin. Oncol. 2023, 41, 5599. [Google Scholar] [CrossRef]
- Yagishita, S.; Nishikawa, T.; Yoshida, H.; Shintani, D.; Sato, S.; Miwa, M.; Suzuki, M.; Yasuda, M.; Ogitani, Y.; Jikoh, T.; et al. Co-Clinical Study of [fam-] Trastuzumab Deruxtecan (DS8201a) in Patient-Derived Xenograft Models of Uterine Carcinosarcoma and Its Association with Clinical Efficacy. Clin. Cancer Res. 2023, 29, 2239–2249. [Google Scholar] [CrossRef]
- Markert, S.; Lassmann, S.; Gabriel, B.; Klar, M.; Werner, M.; Gitsch, G.; Kratz, F.; Hasenburg, A. Alpha-folate Receptor Expression in Epithelial Ovarian Carcinoma and Non-neoplastic Ovarian Tissue. Anticancer. Res. 2008, 28, 3567–3572. [Google Scholar] [PubMed]
- Bax, H.J.; Chauhan, J.; Stavraka, C.; Santaolalla, A.; Osborn, G.; Khiabany, A.; Grandits, M.; López-Abente, J.; Palhares, L.C.G.F.; Chan Wah Hak, C.; et al. Folate receptor alpha in ovarian cancer tissue and patient serum is associated with disease burden and treatment outcomes. Br. J. Cancer 2023, 128, 342–353. [Google Scholar] [CrossRef] [PubMed]
- Dilawari, A.; Shah, M.; Ison, G.; Gittleman, H.; Fiero, M.H.; Shah, A.; Hamed, S.S.; Qiu, J.; Yu, J.; Manheng, W.; et al. FDA Approval Summary: Mirvetuximab Soravtansine-Gynx for FRα-Positive, Platinum-Resistant Ovarian Cancer. Clin. Cancer Res. 2023, 29, 3835–3840. [Google Scholar] [CrossRef] [PubMed]
- Perrone, E.; Lopez, S.; Zeybek, B.; Bellone, S.; Bonazzoli, E.; Pelligra, S.; Zammataro, L.; Manzano, A.; Manara, P.; Bianchi, A.; et al. Preclinical Activity of Sacituzumab Govitecan, an Antibody-Drug Conjugate Targeting Trophoblast Cell-Surface Antigen 2 (Trop-2) Linked to the Active Metabolite of Irinotecan (SN-38), in Ovarian Cancer. Front. Oncol. 2020, 10. [Google Scholar] [CrossRef] [PubMed]
- Xu, N.; Zhang, Z.; Zhu, J.; Xu, L.; Li, Y.; Duan, L.; Mao, Y.; Li, H. Overexpression of trophoblast cell surface antigen 2 as an independent marker for a poor prognosis and as a potential therapeutic target in epithelial ovarian carcinoma. Int. J. Exp. Pathol. 2016, 97, 150–158. [Google Scholar] [CrossRef] [PubMed]
- Tuefferd, M.; Couturier, J.; Penault-Llorca, F.; Vincent-Salomon, A.; Broët, P.; Guastalla, J.-P.; Allouache, D.; Combe, M.; Weber, B.; Pujade-Lauraine, E.; et al. HER2 Status in Ovarian Carcinomas: A Multicenter GINECO Study of 320 Patients. PLoS ONE 2007, 2, e1138. [Google Scholar] [CrossRef] [PubMed]
- Kim, Y.N.; Chung, Y.S.; Park, E.; Lee, S.T.; Lee, J.Y. Human epidermal growth factor receptor-2 expression and subsequent dynamic changes in patients with ovarian cancer. Sci. Rep. 2024, 14, 7992. [Google Scholar] [CrossRef] [PubMed]
- Shimizu, T.; Fujiwara, Y.; Yonemori, K.; Koyama, T.; Sato, J.; Tamura, K.; Shimomura, A.; Ikezawa, H.; Nomoto, M.; Furuuchi, K.; et al. First-in-Human Phase 1 Study of MORAb-202, an Antibody-Drug Conjugate Comprising Farletuzumab Linked to Eribulin Mesylate, in Patients with Folate Receptor-α-Positive Advanced Solid Tumors. Clin. Cancer Res. 2021, 27, 3905–3915. [Google Scholar] [CrossRef]
- Nishio, S.; Yunokawa, M.; Matsumoto, K.; Takehara, K.; Hasegawa, K.; Hirashima, Y.; Kato, H.; Ikezawa, H.; Nomoto, M.; Hayato, S.; et al. Safety and efficacy of MORAb-202 in patients (pts) with platinum-resistant ovarian cancer (PROC): Results from the expansion part of a phase 1 trial. J. Clin. Oncol. 2022, 40, 5513. [Google Scholar] [CrossRef]
- Li, X.; Zhou, S.; Abrahams, C.L.; Krimm, S.; Smith, J.; Bajjuri, K.; Stephenson, H.T.; Henningsen, R.; Hanson, J.; Heibeck, T.H.; et al. Discovery of STRO-002, a Novel Homogeneous ADC Targeting Folate Receptor Alpha, for the Treatment of Ovarian and Endometrial Cancers. Mol. Cancer Ther. 2023, 22, 155–167. [Google Scholar] [CrossRef]
- Oaknin, A.; Fariñas-Madrid, L.; García-Duran, C.; Martin, L.P.; O’Malley, D.M.; Schilder, R.J.; Uyar, D.; Moroney, J.W.; Diaz, J.P.; Spira, A.I.; et al. Luveltamab tazevibulin (STRO-002), an anti-folate receptor alpha (FolRα) antibody drug conjugate (ADC), safety and efficacy in a broad distribution of FolRα expression in patients with recurrent epithelial ovarian cancer (OC): Update of STRO-002-GM1 phase 1 dose expansion cohort. J. Clin. Oncol. 2023, 41, 5508. [Google Scholar] [CrossRef]
- Bignotti, E.; Todeschini, P.; Calza, S.; Falchetti, M.; Ravanini, M.; Tassi, R.A.; Ravaggi, A.; Bandiera, E.; Romani, C.; Zanotti, L.; et al. Trop-2 overexpression as an independent marker for poor overall survival in ovarian carcinoma patients. Eur. J. Cancer 2010, 46, 944–953. [Google Scholar] [CrossRef] [PubMed]
- Okajima, D.; Yasuda, S.; Maejima, T.; Karibe, T.; Sakurai, K.; Aida, T.; Toki, T.; Yamaguchi, J.; Kitamura, M.; Kamei, R.; et al. Datopotamab Deruxtecan, a Novel TROP2-directed Antibody-drug Conjugate, Demonstrates Potent Antitumor Activity by Efficient Drug Delivery to Tumor Cells. Mol. Cancer Ther. 2021, 20, 2329–2340. [Google Scholar] [CrossRef] [PubMed]
- Shimizu, T.; Sands, J.; Yoh, K.; Spira, A.; Garon, E.B.; Kitazono, S.; Johnson, M.L.; Meric-Bernstam, F.; Tolcher, A.W.; Yamamoto, N.; et al. First-in-Human, Phase I Dose-Escalation and Dose-Expansion Study of Trophoblast Cell-Surface Antigen 2–Directed Antibody-Drug Conjugate Datopotamab Deruxtecan in Non–Small-Cell Lung Cancer: TROPION-PanTumor01. J. Clin. Oncol. 2023, 41, 4678–4687. [Google Scholar] [CrossRef]
- Bardia, A.; Krop, I.E.; Kogawa, T.; Juric, D.; Tolcher, A.W.; Hamilton, E.P.; Mukohara, T.; Lisberg, A.; Shimizu, T.; Spira, A.I.; et al. Datopotamab Deruxtecan in Advanced or Metastatic HR+/HER2− and Triple-Negative Breast Cancer: Results from the Phase I TROPION-PanTumor01 Study. J. Clin. Oncol. 2024, 42, 2281–2294. [Google Scholar] [CrossRef]
- Vranic, S.; Gatalica, Z. Trop-2 protein as a therapeutic target: A focused review on Trop-2-based antibody-drug conjugates and their predictive biomarkers. Bosn. J. Basic. Med. Sci. 2022, 22, 14–21. [Google Scholar] [CrossRef] [PubMed]
- Syed, Y.Y. Sacituzumab Govitecan: First Approval. Drugs 2020, 80, 1019–1025. [Google Scholar] [CrossRef] [PubMed]
- Zhu, Y.; Zhu, X.; Wei, X.; Tang, C.; Zhang, W. HER2-targeted therapies in gastric cancer. Biochim. Et. Biophys. Acta (BBA) Rev. Cancer 2021, 1876, 188549. [Google Scholar] [CrossRef] [PubMed]
- Xu, Y.; Wang, Y.; Gong, J.; Zhang, X.; Peng, Z.; Sheng, X.; Mao, C.; Fan, Q.; Bai, Y.; Ba, Y.; et al. Phase I study of the recombinant humanized anti-HER2 monoclonal antibody–MMAE conjugate RC48-ADC in patients with HER2-positive advanced solid tumors. Gastric Cancer 2021, 24, 913–925. [Google Scholar] [CrossRef]
- Peng, Z.; Liu, T.; Wei, J.; Wang, A.; He, Y.; Yang, L.; Zhang, X.; Fan, N.; Luo, S.; Li, Z.; et al. Efficacy and safety of a novel anti-HER2 therapeutic antibody RC48 in patients with HER2-overexpressing, locally advanced or metastatic gastric or gastroesophageal junction cancer: A single-arm phase II study. Cancer Commun. 2021, 41, 1173–1182. [Google Scholar] [CrossRef]
- Wang, J.; Liu, Y.; Zhang, Q.; Feng, J.; Fang, J.; Chen, X.; Han, Y.; Li, Q.; Zhang, P.; Yuan, P.; et al. RC48-ADC, a HER2-targeting antibody-drug conjugate, in patients with HER2-positive and HER2-low expressing advanced or metastatic breast cancer: A pooled analysis of two studies. J. Clin. Oncol. 2021, 39, 1022. [Google Scholar] [CrossRef]
- Li, J.; Luo, S.; Liu, T.; Dong, L.; Yuan, X.; Feng, J.; Wang, Y.; Deng, Y.; Chen, J.; Zhang, M.; et al. 684P Phase I trial of SHR-A1811 in HER2-expressing advanced gastric cancer (GC) or gastroesophageal junction adenocarcinoma (GEJ) and colorectal cancer (CRC). Ann. Oncol. 2023, 34, S478. [Google Scholar] [CrossRef]
- Yao, H.; Ryu, M.H.; Park, J.; Voskoboynik, M.; Kim, J.H.; Liu, K.; Barve, M.; Acuna-Villaorduna, A.; Im, S.A.; Roy, A.C.; et al. 656MO The HER2-targeting ADC SHR-A1811 in HER2-expressing/mutated advanced non-breast solid tumors (STs): Results from the global phase I study. Ann. Oncol. 2023, 34, S461–S462. [Google Scholar] [CrossRef]
- Keam, S.J. Trastuzumab Deruxtecan: First Approval. Drugs 2020, 80, 501–508. [Google Scholar] [CrossRef] [PubMed]
- Deeks, E.D. Disitamab Vedotin: First Approval. Drugs 2021, 81, 1929–1935. [Google Scholar] [CrossRef] [PubMed]
- Banerjee, S.; Drapkin, R.; Richardson, D.L.; Birrer, M. Targeting NaPi2b in ovarian cancer. Cancer Treat. Rev. 2023, 112, 102489. [Google Scholar] [CrossRef] [PubMed]
- Levan, K.; Mehryar, M.; Mateoiu, C.; Albertsson, P.; Bäck, T.; Sundfeldt, K. Immunohistochemical evaluation of epithelial ovarian carcinomas identifies three different expression patterns of the MX35 antigen, NaPi2b. BMC Cancer 2017, 17, 303. [Google Scholar] [CrossRef] [PubMed]
- Richardson, D.; Hamilton, E.; Barve, M.; Anderson, C.; Taylor, S.; Lakhani, N.; Buscema, J.; Tolcher, A.; Zarwan, C.; Werner, T.; et al. Updated Results from the Phase 1 Expansion Study of Upifitamab Rilsodotin (UpRi; XMT-1536), a NaPi2b-directed Dolaflexin Antibody Drug Conjugate (ADC) in Ovarian Cancer (076). Gynecol. Oncol. 2022, 166, S48. [Google Scholar] [CrossRef]
- Richardson, D.L.; Harter, P.; O’Malley, D.M.; Martin, A.G.; Herzog, T.J.; Rogalski, C.; Lemming, R.; Keeton, E.; Burger, R.A.; Mirza, M.R. UP-NEXT (GOG-3049/ENGOT-Ov71-NSGO-CTU): A study of upitifamab rilsodotin (UpRi), a NaPi2b-directed antibody drug conjugate (ADC), in platinum-sensitive recurrent ovarian cancer. J. Clin. Oncol. 2023, 41, TPS5614. [Google Scholar] [CrossRef]
- Shintani, D.; Hanaoka, M.; Sato, S.; Yano, M.; Ogasawara, A.; Kato, T.; Yabuno, A.; Yasuda, M.; Kaneda, Y.; Nagata, M.; et al. Clinical significance of cadherin-6 expression in primary and recurrent epithelial ovarian cancer and its association with outcomes: A potential therapeutic target for epithelial ovarian cancer (206). Gynecol. Oncol. 2022, 166, S116. [Google Scholar] [CrossRef]
- Shintani, D.; Hanaoka, M.; Kaneda, Y.; Ogasawara, A.; Yano, M.; Katoh, T.; Yasuda, M.; Nagata, M.; Hasegawa, K. 777P Targeting cadherin-6 in epithelial ovarian cancer: Clinical significance of its expression and efficacy of raludotatug deruxtecan (R-DXd) in patient-derived cell models. Ann. Oncol. 2023, 34, S525–S526. [Google Scholar] [CrossRef]
- Moore, K.N.; Philipovskiy, A.; Harano, K.; Rini, B.I.; Sudo, K.; Kitano, S.; Spigel, D.R.; Lin, J.; Kundu, M.; Bensmaine, A.; et al. 745MO Raludotatug deruxtecan (R-DXd; DS-6000) monotherapy in patients with previously treated ovarian cancer (OVC): Subgroup analysis of a first-in-human phase I study. Ann. Oncol. 2023, 34, S510. [Google Scholar] [CrossRef]
- Liu, K.; Li, M.; Li, Y.; Li, Y.; Chen, Z.; Tang, Y.; Yang, M.; Deng, G.; Liu, H. A review of the clinical efficacy of FDA-approved antibody–drug conjugates in human cancers. Mol. Cancer 2024, 23, 62. [Google Scholar] [CrossRef] [PubMed]
- Kurosaki, A.; Hasegawa, K.; Kato, T.; Abe, K.; Hanaoka, T.; Miyara, A.; O’Shannessy, D.J.; Somers, E.B.; Yasuda, M.; Sekino, T.; et al. Serum folate receptor alpha as a biomarker for ovarian cancer: Implications for diagnosis, prognosis and predicting its local tumor expression. Int. J. Cancer 2016, 138, 1994–2002. [Google Scholar] [CrossRef] [PubMed]
- Anastasio, M.K.; Shuey, S.; Davidson, B.A. Antibody-Drug Conjugates in Gynecologic Cancers. Curr. Treat. Options Oncol. 2024, 25, 1–19. [Google Scholar] [CrossRef] [PubMed]
- Eaton, J.S.; Miller, P.E.; Mannis, M.J.; Murphy, C.J. Ocular Adverse Events Associated with Antibody-Drug Conjugates in Human Clinical Trials. J. Ocul. Pharmacol. Ther. 2015, 31, 589–604. [Google Scholar] [CrossRef] [PubMed]
- Kim, S.K.; Ursell, P.; Coleman, R.L.; Monk, B.J.; Vergote, I. Mitigation and management strategies for ocular events associated with tisotumab vedotin. Gynecol. Oncol. 2022, 165, 385–392. [Google Scholar] [CrossRef] [PubMed]
- Zhu, Y.; Liu, K.; Wang, K.; Zhu, H. Treatment-related adverse events of antibody-drug conjugates in clinical trials: A systematic review and meta-analysis. Cancer 2023, 129, 283–295. [Google Scholar] [CrossRef] [PubMed]
- Kumagai, K.; Aida, T.; Tsuchiya, Y.; Kishino, Y.; Kai, K.; Mori, K. Interstitial pneumonitis related to trastuzumab deruxtecan, a human epidermal growth factor receptor 2-targeting Ab–drug conjugate, in monkeys. Cancer Sci. 2020, 111, 4636–4645. [Google Scholar] [CrossRef]
- Swain, S.M.; Nishino, M.; Lancaster, L.H.; Li, B.T.; Nicholson, A.G.; Bartholmai, B.J.; Naidoo, J.; Schumacher-Wulf, E.; Shitara, K.; Tsurutani, J.; et al. Multidisciplinary clinical guidance on trastuzumab deruxtecan (T-DXd)-related interstitial lung disease/pneumonitis-Focus on proactive monitoring, diagnosis, and management. Cancer Treat. Rev. 2022, 106, 102378. [Google Scholar] [CrossRef]
- Wei, Q.; Li, P.; Yang, T.; Zhu, J.; Sun, L.; Zhang, Z.; Wang, L.; Tian, X.; Chen, J.; Hu, C.; et al. The promise and challenges of combination therapies with antibody-drug conjugates in solid tumors. J. Hematol. Oncol. 2024, 17, 1. [Google Scholar] [CrossRef] [PubMed]
- Cristea, M.C.; Stewart, D.; Synold, T.; Ruel, N.; Mortimer, J.; Wang, E.; Jung, A.; Wilczynski, S.; Konecny, G.E.; Eng, M.; et al. A phase I study of Mirvetuximab Soravtansine and gemcitabine in patients with FRα-positive recurrent ovarian, primary peritoneal, fallopian tube, or endometrial cancer, or triple negative breast cancer. Gynecol. Oncol. 2024, 182, 124–131. [Google Scholar] [CrossRef]
- Gilbert, L.; Oaknin, A.; Matulonis, U.A.; Mantia-Smaldone, G.M.; Lim, P.C.; Castro, C.M.; Provencher, D.; Memarzadeh, S.; Method, M.; Wang, J.; et al. Safety and efficacy of mirvetuximab soravtansine, a folate receptor alpha (FRα)-targeting antibody-drug conjugate (ADC), in combination with bevacizumab in patients with platinum-resistant ovarian cancer. Gynecol. Oncol. 2023, 170, 241–247. [Google Scholar] [CrossRef] [PubMed]
- Kako, T.; Dholakia, J.; Leath, C.; Arend, R. Single-arm phase II trial of carboplatin and mirvetuximab soravtansine as neoadjuvant chemotherapy (NACT) for advanced- stage ovarian, fallopian tube or primary peritoneal cancer (EOC) who are folate receptor α positive (NCT04606914) (578). Gynecol. Oncol. 2022, 166, S281. [Google Scholar] [CrossRef]
- O’Malley, D.M.; Myers, T.K.N.; Zamagni, C.; Diver, E.; Lorusso, D. GLORIOSA: A randomized, open-label, phase 3 study of mirvetuximab soravtansine with bevacizumab vs. bevacizumab as maintenance in platinum-sensitive ovarian, fallopian tube, or primary peritoneal cancer. J. Clin. Oncol. 2023, 41, TPS5622. [Google Scholar] [CrossRef]
- Chiba, Y.; Kojima, Y.; Yazaki, S.; Yoshida, H.; Takamizawa, S.; Kitadai, R.; Saito, A.; Okuma, H.S.; Nishikawa, T.; Shimoi, T.; et al. Trop-2 expression and the tumor immune microenvironment in cervical cancer. Gynecol. Oncol. 2024, 187, 51–57. [Google Scholar] [CrossRef]
- Janjigian, Y.Y.; Oaknin, A.; Lang, J.M.; Ciombor, K.K.; Ray-Coquard, I.L.; Oza, A.M.; Yonemori, K.; Xu, R.-H.; Zhao, J.; Gajavelli, S.; et al. TROPION-PanTumor03: Phase 2, multicenter study of datopotamab deruxtecan (Dato-DXd) as monotherapy and in combination with anticancer agents in patients (pts) with advanced/metastatic solid tumors. J. Clin. Oncol. 2023, 41, TPS3153. [Google Scholar] [CrossRef]
- Nicolò, E.; Giugliano, F.; Ascione, L.; Tarantino, P.; Corti, C.; Tolaney, S.M.; Cristofanilli, M.; Curigliano, G. Combining antibody-drug conjugates with immunotherapy in solid tumors: Current landscape and future perspectives. Cancer Treat. Rev. 2022, 106, 102395. [Google Scholar] [CrossRef] [PubMed]
- Peng, Z.; Li, M.; Li, H.; Gao, Q. PD-1/PD-L1 immune checkpoint blockade in ovarian cancer: Dilemmas and opportunities. Drug Discov. Today 2023, 28, 103666. [Google Scholar] [CrossRef]
- Pawłowska, A.; Rekowska, A.; Kuryło, W.; Pańczyszyn, A.; Kotarski, J.; Wertel, I. Current Understanding on Why Ovarian Cancer Is Resistant to Immune Checkpoint Inhibitors. Int. J. Mol. Sci. 2023, 24, 10859. [Google Scholar] [CrossRef]
- Khoury, R.; Saleh, K.; Khalife, N.; Saleh, M.; Chahine, C.; Ibrahim, R.; Lecesne, A. Mechanisms of Resistance to Antibody-Drug Conjugates. Int. J. Mol. Sci. 2023, 24, 9674. [Google Scholar] [CrossRef] [PubMed]
- Chang, H.L.; Schwettmann, B.; McArthur, H.L.; Chan, I.S. Antibody-drug conjugates in breast cancer: Overcoming resistance and boosting immune response. J. Clin. Investig. 2023, 133, e172156. [Google Scholar] [CrossRef] [PubMed]
- Loganzo, F.; Tan, X.; Sung, M.; Jin, G.; Myers, J.S.; Melamud, E.; Wang, F.; Diesl, V.; Follettie, M.T.; Musto, S.; et al. Tumor Cells Chronically Treated with a Trastuzumab–Maytansinoid Antibody–Drug Conjugate Develop Varied Resistance Mechanisms but Respond to Alternate Treatments. Mol. Cancer Ther. 2015, 14, 952–963. [Google Scholar] [CrossRef] [PubMed]
- Filho, O.M.; Viale, G.; Stein, S.; Trippa, L.; Yardley, D.A.; Mayer, I.A.; Abramson, V.G.; Arteaga, C.L.; Spring, L.M.; Waks, A.G.; et al. Impact of HER2 Heterogeneity on Treatment Response of Early-Stage HER2-Positive Breast Cancer: Phase II Neoadjuvant Clinical Trial of T-DM1 Combined with Pertuzumab. Cancer Discov. 2021, 11, 2474–2487. [Google Scholar] [CrossRef] [PubMed]
- Ogitani, Y.; Aida, T.; Hagihara, K.; Yamaguchi, J.; Ishii, C.; Harada, N.; Soma, M.; Okamoto, H.; Oitate, M.; Arakawa, S.; et al. DS-8201a, A Novel HER2-Targeting ADC with a Novel DNA Topoisomerase I Inhibitor, Demonstrates a Promising Antitumor Efficacy with Differentiation from T-DM1. Clin. Cancer Res. 2016, 22, 5097–5108. [Google Scholar] [CrossRef] [PubMed]
- Saito, A.; Nishikawa, T.; Yoshida, H.; Mizoguchi, C.; Kitadai, R.; Yamamoto, K.; Yazaki, S.; Kojima, Y.; Ishikawa, M.; Kato, T.; et al. Folate receptor alpha is widely expressed and a potential therapeutic target in uterine and ovarian carcinosarcoma. Gynecol. Oncol. 2023, 176, 115–121. [Google Scholar] [CrossRef]
- Matsuda, Y.; Seki, T.; Yamada, K.; Ooba, Y.; Takahashi, K.; Fujii, T.; Kawaguchi, S.; Narita, T.; Nakayama, A.; Kitahara, Y.; et al. Chemical Site-Specific Conjugation Platform to Improve the Pharmacokinetics and Therapeutic Index of Antibody–Drug Conjugates. Mol. Pharm. 2021, 18, 4058–4066. [Google Scholar] [CrossRef]
- Yamazaki, S.; Matsuda, Y. Tag-Free Enzymatic Modification for Antibody−Drug Conjugate Production. ChemistrySelect 2022, 7, e202203753. [Google Scholar] [CrossRef]
- Fujii, T.; Matsuda, Y. Novel formats of antibody conjugates: Recent advances in payload diversity, conjugation, and linker chemistry. Expert. Opin. Biol. Ther. 2023, 23, 1053–1065. [Google Scholar] [CrossRef]
- Figueroa-Vazquez, V.; Ko, J.; Breunig, C.; Baumann, A.; Giesen, N.; Pálfi, A.; Müller, C.; Lutz, C.; Hechler, T.; Kulke, M.; et al. HDP-101, an Anti-BCMA Antibody-Drug Conjugate, Safely Delivers Amanitin to Induce Cell Death in Proliferating and Resting Multiple Myeloma Cells. Mol. Cancer Ther. 2021, 20, 367–378. [Google Scholar] [CrossRef]
 : showing released payload from linker. (4) The payload in a bioactive form that is released into the cytoplasm. Payloads that disrupt microtubule bind to tubulin. DNA-targeting payloads diffuse from the cytoplasm into the nucleus. Intracellular accumulation of the active payload results in cell death.
: showing released payload from linker. (4) The payload in a bioactive form that is released into the cytoplasm. Payloads that disrupt microtubule bind to tubulin. DNA-targeting payloads diffuse from the cytoplasm into the nucleus. Intracellular accumulation of the active payload results in cell death.
: showing released payload from linker. (4) The payload in a bioactive form that is released into the cytoplasm. Payloads that disrupt microtubule bind to tubulin. DNA-targeting payloads diffuse from the cytoplasm into the nucleus. Intracellular accumulation of the active payload results in cell death.
: showing released payload from linker. (4) The payload in a bioactive form that is released into the cytoplasm. Payloads that disrupt microtubule bind to tubulin. DNA-targeting payloads diffuse from the cytoplasm into the nucleus. Intracellular accumulation of the active payload results in cell death.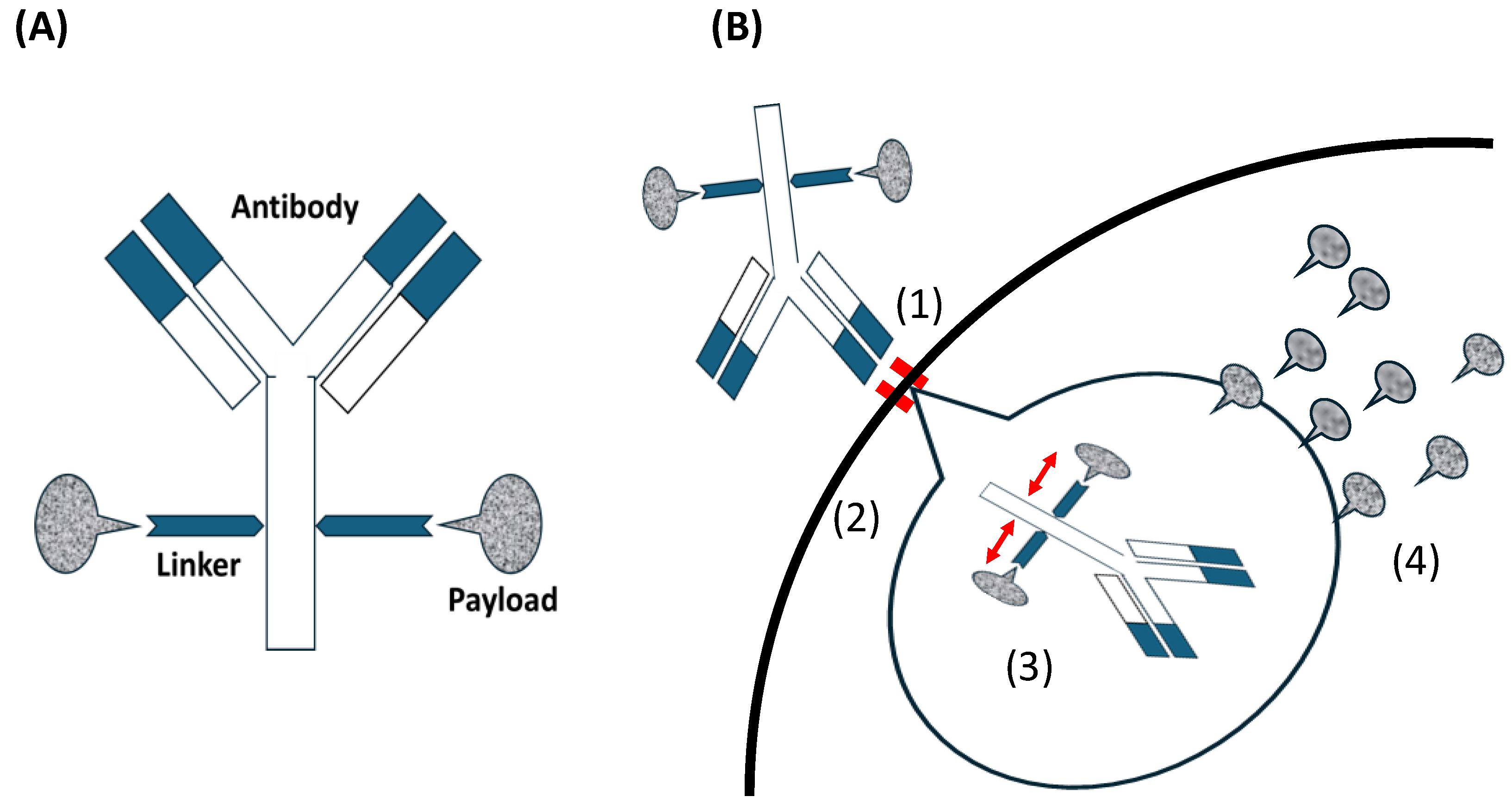

{kind=link}
| Author (Year) | Disease/ Including Status | Agent/ Target/ Paylord | Phase/ PE | Treatment Arm | PFS | OS | ORR | TRAEs |
|---|---|---|---|---|---|---|---|---|
| Moore et al. [42] (2021) | OC PRR and FRα- expression | MIRV/ FRα/ DM4 | III PFS | ICC a vs MIRV | 4.4 vs. 4.1, p = 0.897 (3.3 vs. 4.8, p = 0.049 b) | p = 0.276 c (12.0 vs. 17.3, p = 0.063 d) | 10% vs. 24%, p = 0.014 | MIRV showed a differentiated and more manageable safety profile than chemotherapy. |
| Moore et al. [43] (2023) | OC PRR, HGS and high FRα- expression | MIRV FRα/ DM4 | III PFS | ICC a vs MIRV | 3.98 vs. 5.62, p < 0.001 | 12.75 vs. 16.46, p = 0.005 | 15.9% vs. 42.3% p < 0.001 | 93.7% (over grade3: 54.1%) vs. 96.7% (over grade3: 41.7%) In MIRV group, grade 3 ocular adverse events of blurred vision occurred in 7.8%, keratopathy in 9.2%, and dry eye in 3.2%. |
| Moore et al. [44] (2022) # | OC PSR and FRα- expression | MIRV/ FRα/ DM4 | II ORR | CP + MIRV | 16.4 (95% CI, 10.4–30.2) | none data | 71% (95% CI, 44–90) | The most common TRAEs (all grade, over grade 3): nausea (72%, no), diarrhea (67%, 6%), blurred vision (67%, 0%), thrombocytopenia (61%, 17%), fatigue (61%, 11%), and neutropenia (56%, 28%). |
| Matulonis et al. [45] (2023) | OC PRR, HGS and high FRα- expression | MIRV/ FRα/ DM4 | II ORR | MIRV | 4.3 (95% CI, 3.7–5.2) | 13.8 (95% CI, 12.0–NR) | 32.4% (95% CI, 23.6–42.2) | The most common TRAEs (all grade, over grade 3): blurred vision (41%, 6%), keratopathy (29%, 9%) and nausea (29%, no). |
| Banerjee et al. [46] (2018) | OC PRR | LIFA/ NaPi2b/MMAE | II PFS | PLD vs. LIFA | 3.1 vs. 5.3 HR:0.78 (95% CI, 0.46–1.31 ) | - | 15% vs. 34% p = 0.03 | Neuropathy, abdominal pain, diarrhea and neutropenia were significantly increased in LIFA. |
| Meric-Bernstam et al. [41] (2024) | OC+ PRR *** | T-Dxd/ HER2/ Deruxtecan | II ORR | T-Dxd | 5.9 (95% CI, 4.0–8.3) | 13.2 (95%CI, 8.0–17.7) | 45.0% (95% CI, 29.3–61.5) | + |
| Lheureux et al. [47] (2022) # | OCC PRR and HGS or HGEM | AR/ Mesthelin/ Tubulinpo- lymerization inhibitor | II PFS | PB vs. ARB | 9.6 vs. 5.3 HR:1.7 (95% CI, 0.9–3.4) | - | 55% vs. 18% | The most common TRAEs in the ARB arm were mostly grade 1/2 increase AST (71%) and ALT (64%), thrombocytopenia (61%), fatigue (57%), and peripheral neuropathy (46%). |
| Vergote et al. [40] (2023) # | CC Recurrent or metastatic disease * | TV TF/ MMAE | III OS | ICC e vs TV | HR: 0.67 c (95% CI, 0.54–0.82) | 9.5 vs. 11.5, HR:0.70 (95% CI:0.54–0.89) | 5.2% vs. 17.8% p < 0.0001 | 85.4% (over grade 3: 45.2%) vs. 87.6% (over grade 3: 29.2%). AEs were consistent with the known TV safety profile, including for ocular, peripheral neuropathy, and bleeding AEs. |
| Coleman et al. [39] (2021) | CC Recurrent or metastatic disease * | TV TF/ MMAE | II ORR | TV | 4.2 (95% CI, 3.0–4.4) | 12.1 (95% CI, 9.6–13.9) | 24% (95% CI, 16–33) | The most common TRAEs: conjunctivitis (26%), dry eye (23%), and keratitis (11%). None of serious TRAEs. |
| Meric-Bernstam et al. [41] (2024) | CC+ Recurrent or metastatic disease *** | T-Dxd/ HER2/ Deruxtecan | II ORR | T-Dxd | l 7.0 (95% CI, 4.2–11.1) | 13.6 (95% CI, 11.1–NR) | 50.0% (95% CI, 33.8–66.2) | + |
| Nishikawa and Hasegawa et al. [48] (2023) | UCS Recurrent with HER2 expression (≥1+) ** | T-Dxd/ HER2/ Deruxtecan | II ORR | T-Dxd | 6.7 (95% CI, 5.4–8.8) | 15.8 (95% CI, 10.5–NR) | 54.5% (95% CI, 32.2–75.6) f 70.0% (95% CI, 34.8–93.3) g | Over grade 3 of TRAEs occurred in 61% of all, with the most common being decreased neutrophil count (27%), anemia (24%), and decreased lymphocyte count (21%). |
| Santin et al. [49] (2023) # | EC PRR, HGS and high FRα expression | IMMU-132 (SG)/ TROP2/Govitecan | II ORR | IMMU-132 h | 5.7 | 22.5 | 35% | The treatment was well-tolerated with no new or unexpected safety signals reported. |
| Meric-Bernstam et al. [41] (2024) | EC+ Locally advanced, metastatic disease or recurrence *** | T-Dxd/ HER2/ Deruxtecan | II ORR | T-Dxd | 11.1 (95% CI, 7.1–NR) | 26.0 (95% CI, 12.8–NR) | 57.5% (95% CI, 40.9–73.0) | +Over grade 3 occurred in 40.8% of all, with the most common being neutropenia (10.9%) and anemia (10.9%). Serious event occurred in 13.5% patients. TRAEs resulting in death occurred in 1.5%. |
| Primary or Recurrent | Including Status | Agent | Target | Paylord | ClinicalTrials.gov Identifier (Trial Name) | Phase | RCT | Description |
|---|---|---|---|---|---|---|---|---|
| Recurrent | PRR and High grade carcinoma | DS-6000 | CDH6 | Deruxtecan | NCT06161025 | II/III | Yes | ICC a vs. DS-6000 |
| Recurrent | PSR, HGSC and NaPi2b-positive | UpRi | NaPi2b | AF-HPA | NCT05329545 | III | Yes | After PR or CR of platinum-based therapy, UpRi vs. Placebo |
| Recurrent | PRR | IMGN853 (MIRV) | FRα | DM4 | NCT05622890 | III | No | IMGN853 (MIRV) |
| Recurrent | PRR and HGSC | MORAb-202 | FRα | Ecteribulin | NCT05613088 | II | Yes | ICC b vs. MORAb-202 |
| Recurrent | PRR | IMGN853 (MIRV) | FRα | DM4 | NCT05622890 | II | No | IMGN853 |
| Recurrent | PSR | MIRV | FRα | DM4 | NCT05887609 | II | Yes | After chemotherapy including platinum drug as maintenance Olaparib vs. MIRV |
| Recurrent | PRR | STRO-002 (luvelta) | FRα | SC209 | NCT06238687 | II | No | STRO-002 |
| Recurrent | PRR | Dato-DXd | TROP2 | Deruxtecan | NCT05489211 | II | No | Dato-DXD |
| Recurrent | PRR | ESG401 | TROP2 | SN-38 | NCT04892342 | II | No | ESG401 |
| Recurrent | PRR | IMMU-132 (Sacituzumab Govitecan) | TROP2 | Govitecan | NCT06028932 | II | No | IMMU-132 |
| Recurrent | PRR | SHR-A1811 (Trastuzumab rezetecan) | HER2 | SHR9265 (topoisomerase I inhibitor) | NCT05896020 | II | No | SHR- A1811 |
| Recurrent | PRR | RC48 (Disitamab vedotin) | HER2 | MMAE | NCT06003231 | II | No | RC48 |
| Recurrent | PRR | BL-B01D1 | EGFR xHER3 | Ed-04 | NCT05803018 | II | No | BL-B01D1 |
| Recurrent | PRR | HS-20089 | B7-H4 | Undisclosed Payload | NCT06014190 | II | No | HS-20089 |
| Recurrent | PRR | BA3021 | Ror2 | Vedotin | NCT04918186 | II | No | BA3021 |
| Primary or Recurrent | Including Status | Agent | Target | Paylord | ClinicalTrials.gov Identifier (Trial Name) | Phase | RCT | Description |
|---|---|---|---|---|---|---|---|---|
| Recurrent | PSR and high FRα expression | MIRV | FRα | DM4 | NCT05445778 (GLORIOSA) | III | Yes | Platinum-based therapy + Bev and Bev maintenance, vs. Platinum-based therapy + Bev and Bev + MIRV maintenance |
| Primary | Newly diagnosed, advanced-stage HGSC | MIRV | FRα | DM4 | NCT04606914 | II | No | CP + MIRV |
| Recurrent | PSR | MIRV | FRα | DM4 | NCT05887609 | II | Yes | After chemotherapy including platinum drug as maintenance Olaparib vs. MIRV |
| Recurrent | PSR | AZD5335 | FRα | AZ14170132 (Topo I inhibitor) | NCT05797168 (FONTANA) | II | No | Saruparib + AZD5335 |
| Recurrent | PSR or PRR | Dato-DXd | TROP2 | Deruxtecan | NCT05489211 (TROPION-PanTumor03) | II | No | CP + Dato-DXD → Saruparib + Dato-DXD (PSR) Dato-DXD monotherapy (PRR) |
| Target Antigen (Expression% in OC) | Agent Name | Anti- Body Type | Linker Name (Type) | Paylord Name (Target) | Common TRAEs | Development Status for OC | Development of Combination Therapy |
|---|---|---|---|---|---|---|---|
| FRα (50–80%) | MIRV | IgG1-kappa | N-Succinimidyl 4-(2 pyridyldithio)-2-sulfobutanoate linker (Cleavable) | DM4 (tubulin) | ocular events, diarrhea, fatigue, nausea, vomiting, peripheral, neuropathy, netropenia | FDA approved | O |
| MORAb-202 | IgG1-kappa | A reduced interchain disulfide bonds to maleimido-PEG2-valine-citrulline-p-aminobenzylcarbamyl linker (Cleavable) | Eribulin (tubulin) | ILD/pneumonitis, nausea, pyrexia, malaise, headache | ongoing Phase II | ||
| STRO-002 (luvelta) | IgG1 | valine citrulline p-aminobenzyl carbamate linker (Cleavable) | SC209 (tubulin) | neutropenia, arthralgia, anemia, neutropenia | ongoing Phase II | ||
| TROP2 (50–60%) | Dato-DXd | IgG1 | A tetrapeptide-based linker (Cleavable) | Deruxtecan (topoisomerase I) | nausea, anemia, decreased WBC, ILD/pneumonitis, | ongoing Phase II | O |
| ESG401 | IgG1 | unrevealed linker | SN38 (topoisomerase I) | leukopenia, neutropenia, anemia, fatigue, nausea, vomiting, thrombocytop-enia, diarrhea, skin rash, oral mucositis | ongoing Phase II | ||
| IMMU-132 (SG) | IgG1-kappa | hRS7 via a hydrolysable CL2A linker (cleavable) | Govitecan (topoisomerase I) | neutropenia, decreased WBC, anaemia, diarrhoea, fatigue, febrile, neutropenia, hypophosphatemia, diarrhoea | ongoing Phase II | ||
| HER2 (12–30%) | T-DXd | IgG1-kappa | Gly-Phe-Leu-Gly (tetrapeptide) | Deruxtecan (topoisomerase I) | nausea, anemia, diarrhea, vomiting, fatigue, neutropenia, ILD/pneumonitis | possibility FDA approved * | |
| SHR-A1811 (Trastumab rezetecan) | IgG1-kappa | unrevealed (cleavable) | SHR9265 (topoisomerase I) | neutropenia, anemia, decreased WBC, ILD/pneumonitis | ongoing Phase II | ||
| RC48 (Disitamab vedotin) | IgG1-kappa | mc-val-cit-PABC (cleavable) | MMAE (tubulin) | peripheral sensory neuropathy, leukopenia, neutropenia, AST/ALT increased, alopecia, asthenia, decreased appetite | ongoing Phase II | ||
| NaPi2b (66%) | UpRi | IgG1-kappa | Fleximer polymer scaffold (cleavable) | AF-HPA (tubulin) | AST increased, fatigue, anemia, thrombocytop-enia, neutropenia, peripheral neuropathy, ocular toxicity, ILD/pneumonitis | ongoing Phase III | |
| CDH6 (85%) | DS-6000 (R-Dxd) | IgG1 | Tetrapeptide based linker (cleavable) | Deruxtecan (topoisomerase I) | nausea, fatigue, vomiting, diarrhoea ** | ongoing Phase II/III |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Sato, S.; Shoji, T.; Jo, A.; Otsuka, H.; Abe, M.; Tatsuki, S.; Chiba, Y.; Takatori, E.; Kaido, Y.; Nagasawa, T.; et al. Antibody-Drug Conjugates: The New Treatment Approaches for Ovarian Cancer. Cancers 2024, 16, 2545. https://doi.org/10.3390/cancers16142545
Sato S, Shoji T, Jo A, Otsuka H, Abe M, Tatsuki S, Chiba Y, Takatori E, Kaido Y, Nagasawa T, et al. Antibody-Drug Conjugates: The New Treatment Approaches for Ovarian Cancer. Cancers. 2024; 16(14):2545. https://doi.org/10.3390/cancers16142545
Chicago/Turabian StyleSato, Sho, Tadahiro Shoji, Ami Jo, Haruka Otsuka, Marina Abe, Shunsuke Tatsuki, Yohei Chiba, Eriko Takatori, Yoshitaka Kaido, Takayuki Nagasawa, and et al. 2024. "Antibody-Drug Conjugates: The New Treatment Approaches for Ovarian Cancer" Cancers 16, no. 14: 2545. https://doi.org/10.3390/cancers16142545
APA StyleSato, S., Shoji, T., Jo, A., Otsuka, H., Abe, M., Tatsuki, S., Chiba, Y., Takatori, E., Kaido, Y., Nagasawa, T., Kagabu, M., & Baba, T. (2024). Antibody-Drug Conjugates: The New Treatment Approaches for Ovarian Cancer. Cancers, 16(14), 2545. https://doi.org/10.3390/cancers16142545