
Potential of Alkalization Therapy for the Management of Metastatic Pancreatic Cancer: A Retrospective Study

 , ,
, , 

Abstract
:Simple Summary
Abstract
1. Introduction
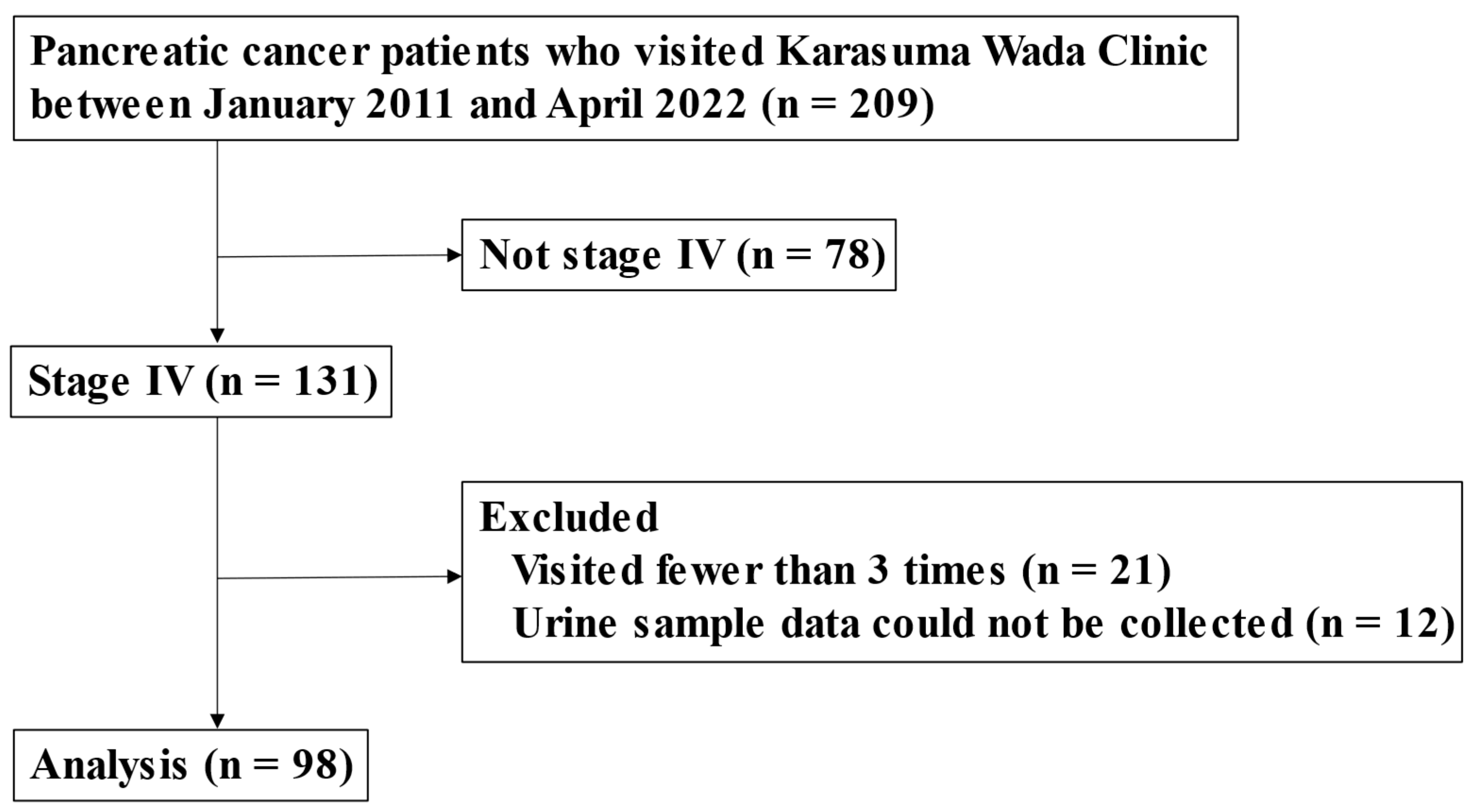
2. Patients and Methods
2.1. Study Design
2.2. Alkalization Therapy
2.3. Assessment Procedures
2.4. Statistical Analyses
3. Results
3.1. Patient Characteristics
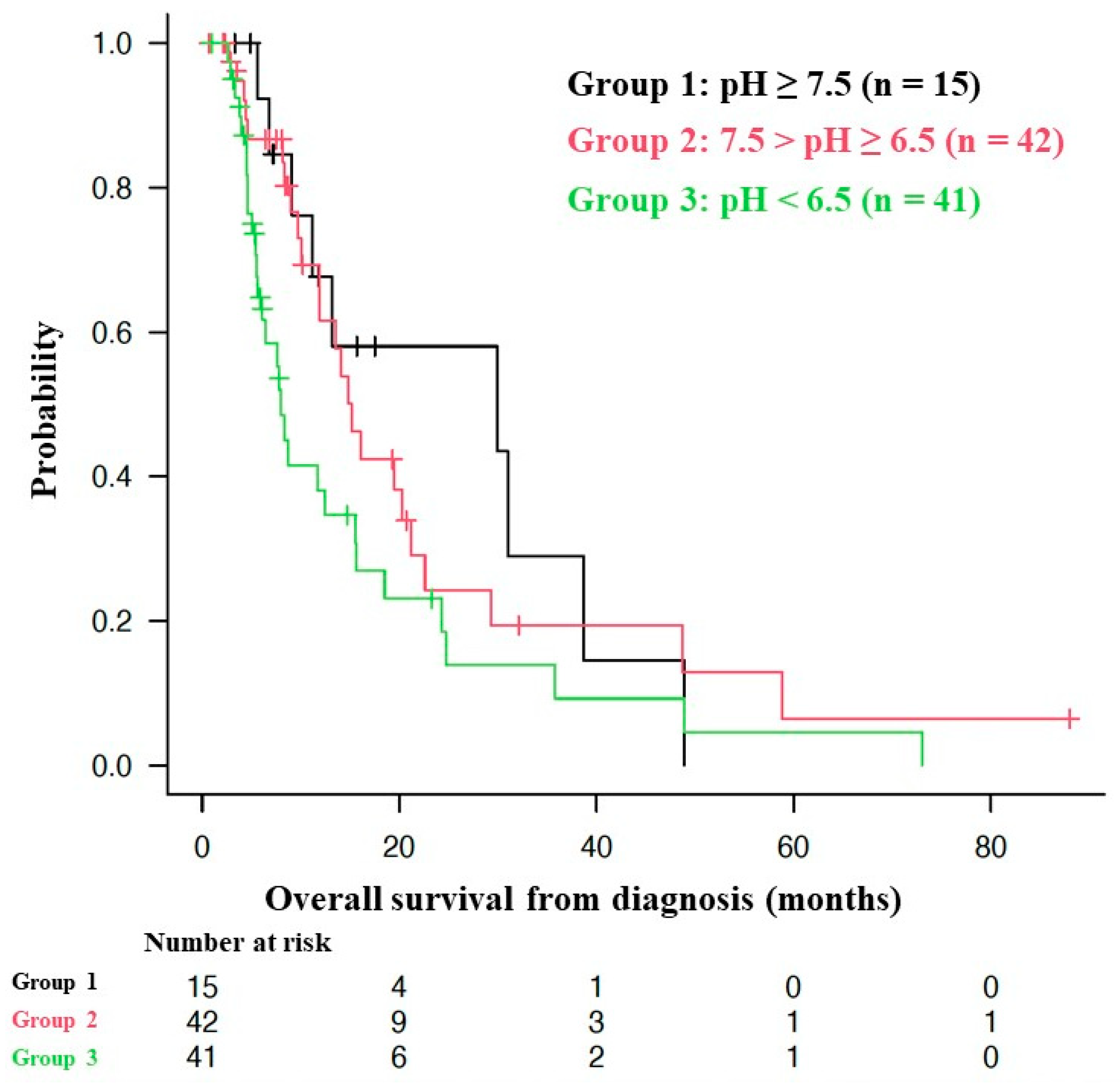
3.2. OS of Patients with Different Urine pHs
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Klein, A.P. Pancreatic cancer epidemiology: Understanding the role of lifestyle and inherited risk factors. Nat. Rev. Gastroenterol. Hepatol. 2021, 18, 493–502. [Google Scholar] [CrossRef] [PubMed]
- Monitoring of Cancer Incidence in Japan—Survival 2009–2011 Report (Center for Cancer Control and Information Services, National Cancer Center, 2020). (In Japanese). Available online: https://ganjoho.jp/reg_stat/statistics/stat/cancer/10_pancreas.html (accessed on 5 October 2023).
- Park, W.; Chawla, A.; O’Reilly, E.M. Pancreatic Cancer. A Review. J. Am. Med. Assoc. 2021, 326, 851–862. [Google Scholar] [CrossRef] [PubMed]
- Schnelldorfer, T.; Ware, A.L.; Sarr, M.G.; Smyrk, T.C.; Zhang, L.; Qin, R.; Gullerud, R.E.; Donohue, J.H.; Nagorney, D.M.; Farnell, M.B. Long-Term Survival After Pancreatoduodenectomy for Pancreatic Adenocarcinoma. Ann. Surg. 2008, 247, 456–462. [Google Scholar] [CrossRef] [PubMed]
- Tanaka, J.; Nakagawa, T.; Harada, K.; Morizane, C.; Tanaka, H.; Shiba, S.; Ohba, A.; Hijioka, S.; Takai, E.; Yachida, S.; et al. Efficient and accurate KRAS genotyping using digital PCR combined with melting curve analysis for ctDNA from pancreatic cancer patients. Sci. Rep. 2023, 13, 3039. [Google Scholar] [CrossRef] [PubMed]
- Okusaka, T.; Furuse, J. Recent advances in chemotherapy for pancreatic cancer: Evidence from Japan and recommendations in guidelines. J. Gastroenterol. 2020, 55, 369–382. [Google Scholar] [CrossRef] [PubMed]
- Okusaka, T.; Nakamura, M.; Yoshida, M.; Kitano, M.; Ito, Y.; Mizuno, N.; Hanada, K.; Ozaka, M.; Morizane, C.; Takeyama, Y.; et al. Clinical Practice Guidelines for Pancreatic Cancer 2022 from the Japan Pancreas Society: A synopsis. Int. J. Clin. Oncol. 2023, 28, 493–511. [Google Scholar] [CrossRef] [PubMed]
- Corbet, C.; Feron, O. Tumour acidosis: From the passenger to the driver’s seat. Nat. Rev. Cancer 2017, 17, 577–593. [Google Scholar] [CrossRef] [PubMed]
- Koppenol, W.H.; Bounds, P.L.; Dang, C.V. Otto Warburg’s contributions to current concepts of cancer metabolism. Nat. Rev. Cancer 2011, 11, 325–337. [Google Scholar] [CrossRef]
- Neri, D.; Supuran, C.T. Interfering with pH regulation in tumours as a therapeutic strategy. Nat. Rev. Drug Discov. 2011, 10, 767–777. [Google Scholar] [CrossRef]
- Hamaguchi, R.; Okamoto, T.; Sato, M.; Hasegawa, M.; Wada, H. Effects of an Alkaline Diet on EGFR-TKI Therapy in EGFR Mutation-positive NSCLC. Anticancer. Res. 2017, 37, 5141–5145. [Google Scholar] [CrossRef]
- Robey, I.F.; Lopez, A.M.; Roe, D.J. Safety and Tolerability of Long-Term Sodium Bicarbonate Consumption in Cancer Care. J. Integr. Oncol. 2014, 4, 128. [Google Scholar] [CrossRef]
- Ando, H.; Eshima, K.; Ishida, T. Neutralization of Acidic Tumor Microenvironment (TME) with Daily Oral Dosing of Sodium Potassium Citrate (K/Na Citrate) Increases Therapeutic Effect of Anti-cancer Agent in Pancreatic Cancer Xenograft Mice Model. Biol. Pharm. Bull. 2021, 44, 266–270. [Google Scholar] [CrossRef] [PubMed]
- Wada, H.; Hamaguchi, R.; Narui, R.; Morikawa, H. Meaning and Significance of “Alkalization Therapy for Cancer”. Front. Oncol. 2022, 12, 920843. [Google Scholar] [CrossRef]
- Hamaguchi, R.; Ito, T.; Narui, R.; Morikawa, H.; Uemoto, S.; Wada, H. Effects of Alkalization Therapy on Chemotherapy Outcomes in Advanced Pancreatic Cancer: A Retrospective Case-Control Study. In Vivo 2020, 34, 2623–2629. [Google Scholar] [CrossRef] [PubMed]
- Isowa, M.; Hamaguchi, R.; Narui, R.; Morikawa, H.; Wada, H. Effects of alkalization therapy on hepatocellular carcinoma: A retrospective study. Front. Oncol. 2023, 13, 1179049. [Google Scholar] [CrossRef] [PubMed]
- Kanda, Y. Investigation of the freely available easy-to-use software ‘EZR’ for medical statistics. Bone Marrow Transplant. 2013, 48, 452–458. [Google Scholar] [CrossRef] [PubMed]
- Kommalapati, A.; Tella, S.H.; Goyal, G.; Ma, W.W.; Mahipal, A. Contemporary Management of Localized Resectable Pancreatic Cancer. Cancers 2018, 10, 24. [Google Scholar] [CrossRef] [PubMed]
- Kleeff, J.; Korc, M.; Apte, M.; La Vecchia, C.; Johnson, C.D.; Biankin, A.V.; Neale, R.E.; Tempero, M.; Tuveson, D.A.; Hruban, R.H.; et al. Pancreatic cancer. Nat. Rev. Dis. Primers 2016, 2, 16022. [Google Scholar] [CrossRef]
- Hanahan, D.; Weinberg, R.A. Hallmarks of cancer: The next generation. Cell 2011, 144, 646–674. [Google Scholar] [CrossRef]
- Gatenby, R.A.; Gillies, R.J. Why do cancers have high aerobic glycolysis? Nat. Rev. Cancer 2004, 4, 891–899. [Google Scholar] [CrossRef]
- Cardone, R.A.; Casavola, V.; Reshkin, S.J. The role of disturbed pH dynamics and the Na+/H+ exchanger in metastasis. Nat. Rev. Cancer 2005, 5, 786–795. [Google Scholar] [CrossRef] [PubMed]
- Cairns, R.A.; Harris, I.S.; Mak, T.W. Regulation of cancer cell metabolism. Nat. Rev. Cancer 2011, 11, 85–95. [Google Scholar] [CrossRef] [PubMed]
- Gillies, R.; Raghunand, N.; Garcia-Martin, M.; Gatenby, R. pH imaging. A review of pH measurement methods and applications in cancers. IEEE Eng. Med. Biol. Mag. 2004, 23, 57–64. [Google Scholar] [CrossRef] [PubMed]
- Gillies, R.J.; Raghunand, N.; Karczmar, G.S.; Bhujwalla, Z.M. MRI of the tumor microenvironment. J. Magn. Reson. Imaging 2002, 16, 430–450. [Google Scholar] [CrossRef] [PubMed]
- Helmlinger, G.; Yuan, F.; Dellian, M.; Jain, R.K. Interstitial pH and pO2 gradients in solid tumors in vivo: High-resolution measurements reveal a lack of correlation. Nat. Med. 1997, 3, 177–182. [Google Scholar] [CrossRef] [PubMed]
- Gallagher, F.A.; Kettunen, M.I.; Day, S.E.; Hu, D.-E.; Ardenkjær-Larsen, J.H.; Zandt, R.I.; Jensen, P.R.; Karlsson, M.; Golman, K.; Lerche, M.H.; et al. Magnetic resonance imaging of pH in vivo using hyperpolarized 13C-labelled bicarbonate. Nature 2008, 453, 940–943. [Google Scholar] [CrossRef] [PubMed]
- Bogdanov, A.; Bogdanov, A.; Chubenko, V.; Volkov, N.; Moiseenko, F.; Moiseyenko, V. Tumor acidity: From hallmark of cancer to target of treatment. Front. Oncol. 2022, 12, 979154. [Google Scholar] [CrossRef]
- Gillies, R.J.; Ibrahim-Hashim, A.; Ordway, B.; Gatenby, R.A. Back to basic: Trials and tribulations of alkalizing agents in cancer. Front. Oncol. 2022, 12, 981718. [Google Scholar] [CrossRef]
- Luciani, F.; Spada, M.; De Milito, A.; Molinari, A.; Rivoltini, L.; Montinaro, A.; Marra, M.; Lugini, L.; Logozzi, M.; Lozupone, F.; et al. Effect of Proton Pump Inhibitor Pretreatment on Resistance of Solid Tumors to Cytotoxic Drugs. JNCI J. Natl. Cancer Inst. 2004, 96, 1702–1713. [Google Scholar] [CrossRef]
- De Milito, A.; Iessi, E.; Logozzi, M.; Lozupone, F.; Spada, M.; Marino, M.L.; Federici, C.; Perdicchio, M.; Matarrese, P.; Lugini, L.; et al. Proton Pump Inhibitors Induce Apoptosis of Human B-Cell Tumors through a Caspase-Independent Mechanism Involving Reactive Oxygen Species. Cancer Res. 2007, 67, 5408–5417. [Google Scholar] [CrossRef]
- De Milito, A.; Canese, R.; Marino, M.L.; Borghi, M.; Iero, M.; Villa, A.; Venturi, G.; Lozupone, F.; Iessi, E.; Logozzi, M.; et al. pH-dependent antitumor activity of proton pump inhibitors against human melanoma is mediated by inhibition of tumor acidity. Int. J. Cancer 2009, 127, 207–219. [Google Scholar] [CrossRef] [PubMed]
- Chen, C.-H.; Lee, C.-Z.; Lin, Y.-C.; Kao, L.-T.; Lin, H.-C. Negative Association of Proton Pump Inhibitors with Subsequent Development of Breast Cancer: A Nationwide Population-Based Study. J. Clin. Pharmacol. 2019, 59, 350–355. [Google Scholar] [CrossRef] [PubMed]
- Ding, D.; Sung, F.; Chen, W.; Wang, J.; Lin, S. Proton pump inhibitors reduce breast cancer risk in gastric ulcer patients: A population-based cohort study. Breast J. 2019, 26, 474–478. [Google Scholar] [CrossRef] [PubMed]
- Wang, B.-Y.; Zhang, J.; Wang, J.-L.; Sun, S.; Wang, Z.-H.; Wang, L.-P.; Zhang, Q.-L.; Lv, F.-F.; Cao, E.-Y.; Shao, Z.-M.; et al. Intermittent high dose proton pump inhibitor enhances the antitumor effects of chemotherapy in metastatic breast cancer. J. Exp. Clin. Cancer Res. 2015, 34, 85. [Google Scholar] [CrossRef] [PubMed]
- Astigiano, S.; Puglisi, A.; Mastracci, L.; Fais, S.; Barbieri, O. Systemic alkalinisation delays prostate cancer cell progression in TRAMP mice. J. Enzym. Inhib. Med. Chem. 2017, 32, 363–368. [Google Scholar] [CrossRef] [PubMed]
- Azzarito, T.; Lugini, L.; Spugnini, E.P.; Canese, R.; Gugliotta, A.; Fidanza, S.; Fais, S. Effect of Modified Alkaline Supplementation on Syngenic Melanoma Growth in CB57/BL Mice. PLoS ONE 2016, 11, e0159763. [Google Scholar] [CrossRef]
- Ozaka, M.; Ishii, H.; Sato, T.; Ueno, M.; Ikeda, M.; Uesugi, K.; Sata, N.; Miyashita, K.; Mizuno, N.; Tsuji, K.; et al. A phase II study of modified FOLFIRINOX for chemotherapy-naïve patients with metastatic pancreatic cancer. Cancer Chemother. Pharmacol. 2018, 81, 1017–1023. [Google Scholar] [CrossRef]
- Ueno, H.; Ikeda, M.; Ueno, M.; Mizuno, N.; Ioka, T.; Omuro, Y.; Nakajima, T.E.; Furuse, J. Phase I/II study of nab-paclitaxel plus gemcitabine for chemotherapy-naive Japanese patients with metastatic pancreatic cancer. Cancer Chemother. Pharmacol. 2016, 77, 595–603. [Google Scholar] [CrossRef]
- Amrhein, V.; Greenland, S.; McShane, B. Scientists rise up against statistical significance. Nature 2019, 567, 305–307. [Google Scholar] [CrossRef]


{kind=link}
{kind=link}
{kind=link}
| Group 1 (n = 15) Urine pH ≥ 7.5 | Group 2 (n = 42) 7.5 ≥ Urine pH > 6.5 | Group 3 (n = 41) 6.5 ≥ Urine pH | |||||||
|---|---|---|---|---|---|---|---|---|---|
| Age (years) | 65.3 (45–85) | 62.6 (33–85) | 66.1 (27–88) | ||||||
| Sex (%) | |||||||||
| Men | 9 (60.0) | 23 (54.8) | 21 (51.2) | ||||||
| Women | 6 (40.0) | 19 (45.2) | 20 (48.8) | ||||||
| Performance status (%) | |||||||||
| 0 | 8 (53.3) | 30 (71.4) | 25 (61.0) | ||||||
| 1 | 7 (46.7) | 12 (28.6) | 16 (39.0) | ||||||
| Comorbidities (%) | |||||||||
| Hypertension | 3 (20.0) | 7 (16.7) | 8 (19.5) | ||||||
| Hyperlipidemia | 3 (20.0) | 8 (19.0) | 4 (9.8) | ||||||
| Diabetes | 2 (13.3) | 10 (23.8) | 5 (12.2) | ||||||
| Hyperuricemia | 1 (6.7) | 2 (4.8) | 3 (7.3) | ||||||
| Arrhythmia | 2 (13.3) | 2 (4.8) | 1 (2.4) | ||||||
| Angina | 0 | 2 (4.8) | 0 | ||||||
| COPD | 0 | 2 (4.8) | 0 | ||||||
| Depression | 2 (13.3) | 0 | 1 (2.4) | ||||||
| Others | 3 * (20.0) | 5 ** (11.9) | 6 *** (14.6) | ||||||
| Malignant disease (past history) | 0 | 5 (11.9) | 5 (12.2) | ||||||
| None | 5 (33.3) | 16 (38.1) | 20 (48.8) | ||||||
| Radiation (%) | |||||||||
| Yes | 0 (0.0) | 2 (4.8) | 5 (12.2) | ||||||
| No | 15 (100.0) | 40 (95.2) | 36 (87.8) | ||||||
| Chemotherapy (%) | 1st line | 2nd line | 3rd line | 1st line | 2nd line | 3rd line | 1st line | 2nd line | 3rd line |
| FOLFIRINOX | 4 (26.7) | 2 (13.3) | 0 | 4 (9.5) | 2 (4.8) | 0 | 4 (9.8) | 1 (2.4) | 0 |
| FOLFIRI | 0 | 2 (13.3) | 0 | 0 | 0 | 0 | 0 | 0 | 0 |
| Gemcitabine plus nab-paclitaxel | 8 (53.3) | 0 | 0 | 14 (33.3) | 5 (11.9) | 1 (2.4) | 12 (29.3) | 2 (4.9) | 0 |
| Gemcitabine plus erlotinib | 0 | 0 | 0 | 3 (7.1) | 1 (2.4) | 0 | 2 (4.9) | 2 (4.9) | 1 (2.4) |
| Gemcitabine plus S-1 | 0 | 0 | 0 | 4 (9.5) | 0 | 0 | 4 (9.8) | 1 (2.4) | 0 |
| Gemcitabine | 2 (13.3) | 1 (6.7) | 0 | 8 (19.0) | 3 (7.1) | 0 | 5 (12.2) | 1 (2.4) | 0 |
| S-1 | 0 | 2 (13.3) | 1 (6.7) | 3 (7.1) | 4 (9.5) | 0 | 2 (4.9) | 6 (14.6) | 0 |
| Erlotinib | 0 | 0 | 0 | 4 (9.5) | 0 | 0 | 3 (7.3) | 0 | 1 (2.4) |
| Unknown | 0 | 0 | 1 (6.7) | 0 | 2 (4.8) | 0 | 2 (4.9) | 0 | 0 |
| None | 1 (6.7) | 8 (53.3) | 13 (86.7) | 2 (4.8) | 25 (59.5) | 41 (97.6) | 7 (17.1) | 28 (68.3) | 39 (95.1) |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Isowa, M.; Hamaguchi, R.; Narui, R.; Morikawa, H.; Okamoto, T.; Wada, H. Potential of Alkalization Therapy for the Management of Metastatic Pancreatic Cancer: A Retrospective Study. Cancers 2024, 16, 61. https://doi.org/10.3390/cancers16010061
Isowa M, Hamaguchi R, Narui R, Morikawa H, Okamoto T, Wada H. Potential of Alkalization Therapy for the Management of Metastatic Pancreatic Cancer: A Retrospective Study. Cancers. 2024; 16(1):61. https://doi.org/10.3390/cancers16010061
Chicago/Turabian StyleIsowa, Masahide, Reo Hamaguchi, Ryoko Narui, Hiromasa Morikawa, Toshihiro Okamoto, and Hiromi Wada. 2024. "Potential of Alkalization Therapy for the Management of Metastatic Pancreatic Cancer: A Retrospective Study" Cancers 16, no. 1: 61. https://doi.org/10.3390/cancers16010061
APA StyleIsowa, M., Hamaguchi, R., Narui, R., Morikawa, H., Okamoto, T., & Wada, H. (2024). Potential of Alkalization Therapy for the Management of Metastatic Pancreatic Cancer: A Retrospective Study. Cancers, 16(1), 61. https://doi.org/10.3390/cancers16010061