
Manifestations of Ovarian Cancer in Relation to Other Pelvic Diseases by MRI


{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Abstract
Simple Summary
Abstract
1. Introduction
1.1. Data Search
1.2. Epidemiology
Pitfalls and Diagnostic Challenges
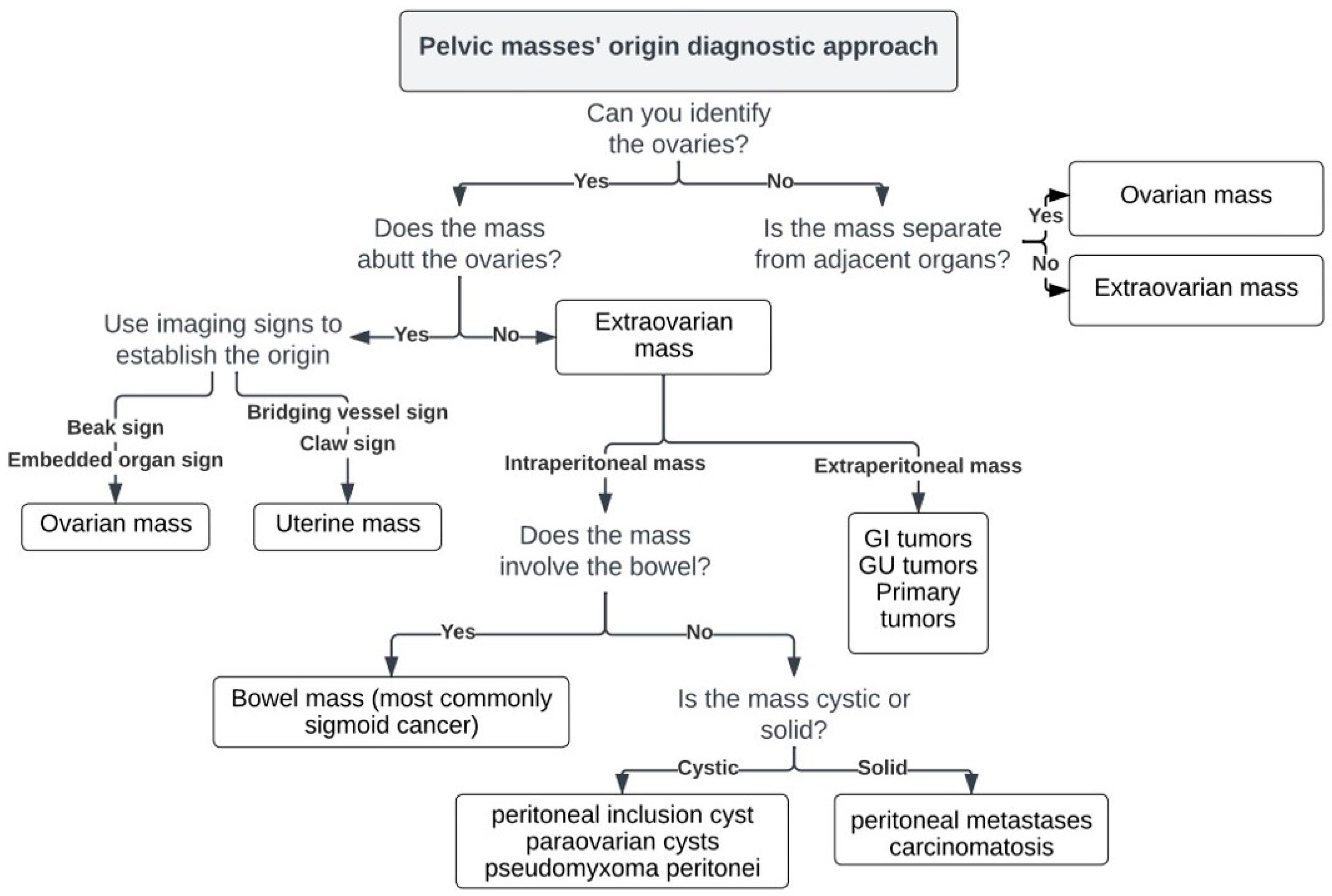
1.3. Origin and Characterization of a Pelvic Mass
- Identify the ovaries.
- Describe relationship to the ovary.
1.4. Importance of Accurate Diagnosis in Treatment Decisions
1.5. Special Subgroups
1.5.1. Adolescence
1.5.2. Pregnancy
2. Typical and Atypical Findings of Ovarian Cancer and Mimickers on MRI
2.1. Borderline and Malignant Neoplasms
2.1.1. High-Grade Serous Cystadenocarcinoma (HGSC)
2.1.2. Serous Borderline Neoplasms and Low-Grade Serous Cystadenocarcinoma
2.1.3. Mucinous Borderline Neoplasms and Mucinous Cystadenocarcinoma
2.1.4. Endometrioid Carcinoma and Clear Cell Carcinoma
2.2. Benign Tumors That Can Mimic EOC
2.2.1. Cystadenofibroma
2.2.2. Fibrothecoma
2.2.3. Pelvic Inflammatory Disease—Tubo-Ovarian Abscess (TOA)
2.3. Rare Ovarian Neoplasms That Can Mimic EOC
2.3.1. Brenner Tumor
2.3.2. Monodermal Teratoma (Struma Ovarii)
2.3.3. Granulosa Cell Tumor
2.3.4. Lymphoma
2.3.5. Metastases
2.4. Adolescence-Germ Cell Tumors
2.4.1. Mature Cystic Teratoma (Dermoid)
2.4.2. Immature Teratoma
2.4.3. Dysgerminoma
2.5. Pregnancy
2.5.1. Corpus Luteum Cysts/Theca Lutein Cysts
2.5.2. Decidualized Endometrioma
2.5.3. Epithelial Ovarian Cancer
2.6. Non-Ovarian Masses
2.6.1. Mucinous Rectosigmoid Cancer
2.6.2. Appendiceal Mucocele—PMP
2.6.3. Liposarcoma/Schwannoma
3. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Kurman, R.; Carcanjiu, M.; Herrington, S.; Young, R. Tumours of the Ovary. In World Health Organization Classification of Tumours of the Female Reproductive Organs; IARC: Lyon, France, 2014; pp. 11–86. [Google Scholar]
- Huang, J.; Chan, W.C.; Ngai, C.H.; Lok, V.; Zhang, L.; Lucero-Prisno, D.E.; Xu, W.; Zheng, Z.-J.; Elcarte, E.; Withers, M.; et al. Worldwide Burden, Risk Factors, and Temporal Trends of Ovarian Cancer: A Global Study. Cancers 2022, 14, 2230. [Google Scholar] [CrossRef] [PubMed]
- Timmerman, D.; Van Calster, B.; Testa, A.C.; Guerriero, S.; Fischerova, D.; Lissoni, A.A.; Van Holsbeke, C.; Fruscio, R.; Czekierdowski, A.; Jurkovic, D.; et al. Ovarian Cancer Prediction in Adnexal Masses Using Ultrasound-Based Logistic Regression Models: A Temporal and External Validation Study by the IOTA Group. Ultrasound Obstet. Gynecol. 2010, 36, 226–234. [Google Scholar] [CrossRef] [PubMed]
- Van Holsbeke, C.; Daemen, A.; Yazbek, J.; Holland, T.K.; Bourne, T.; Mesens, T.; Lannoo, L.; Boes, A.-S.; Joos, A.; Van De Vijver, A.; et al. Ultrasound Experience Substantially Impacts on Diagnostic Performance and Confidence When Adnexal Masses Are Classified Using Pattern Recognition. Gynecol. Obstet. Investig. 2010, 69, 160–168. [Google Scholar] [CrossRef]
- Adusumilli, S.; Hussain, H.K.; Caoili, E.M.; Weadock, W.J.; Murray, J.P.; Johnson, T.D.; Chen, Q.; Desjardins, B. MRI of Sonographically Indeterminate Adnexal Masses. Am. J. Roentgenol. 2006, 187, 732–740. [Google Scholar] [CrossRef]
- Sadowski, E.A.; Paroder, V.; Patel-Lippmann, K.; Robbins, J.B.; Barroilhet, L.; Maddox, E.; McMahon, T.; Sampene, E.; Wasnik, A.P.; Blaty, A.D.; et al. Indeterminate Adnexal Cysts at US: Prevalence and Characteristics of Ovarian Cancer. Radiology 2018, 287, 1041–1049. [Google Scholar] [CrossRef] [PubMed]
- Zhang, X.; Mao, Y.; Zheng, R.; Zheng, Z.; Huang, Z.; Huang, D.; Zhang, J.; Dai, Q.; Zhou, X.; Wen, Y. The Contribution of Qualitative CEUS to the Determination of Malignancy in Adnexal Masses, Indeterminate on Conventional US—A Multicenter Study. PLoS ONE 2014, 9, e93843. [Google Scholar] [CrossRef]
- Karaosmanoglu, D.; Karcaaltincaba, M.; Karcaaltincaba, D.; Akata, D.; Ozmen, M. MDCT of the Ovarian Vein: Normal Anatomy and Pathology. Am. J. Roentgenol. 2009, 192, 295–299. [Google Scholar] [CrossRef]
- Lee, J.H.; Jeong, Y.K.; Park, J.K.; Hwang, J.C. “Ovarian Vascular Pedicle” Sign Revealing Organ of Origin of a Pelvic Mass Lesion on Helical CT. Am. J. Roentgenol. 2003, 181, 131–137. [Google Scholar] [CrossRef]
- Arikawa, S.; Uchida, M.; Shinagawa, M.; Tohnan, T.; Hayabuchi, N. Significance of the “Beak Sign” in the Differential Diagnosis of Uterine Lipoleiomyoma from Ovarian Dermoid Cyst. Kurume Med. J. 2006, 53, 37–40. [Google Scholar] [CrossRef]
- Kim, J.C.; Kim, S.S.; Park, J.Y. “Bridging Vascular Sign” in the MR Diagnosis of Exophytic Uterine Leiomyoma. J. Comput. Assist. Tomogr. 2000, 24, 57–60. [Google Scholar] [CrossRef]
- Sahin, H.; Panico, C.; Ursprung, S.; Simeon, V.; Chiodini, P.; Frary, A.; Carmo, B.; Smith, J.; Freeman, S.; Jimenez-Linan, M.; et al. Non-contrast MRI can accurately characterize adnexal masses: A retrospective study. Eur. Radiol. 2021, 31, 6962–6973. [Google Scholar] [CrossRef] [PubMed]
- Lee, S.I.; Kang, S.K. MRI Improves the Characterization of Incidental Adnexal Masses Detected at Sonography. Radiology 2023, 307, e222866. [Google Scholar] [CrossRef] [PubMed]
- Liu, B.; Liao, J.; Gu, W.; Wang, J.; Li, G.; Wang, L. ADNEX Model-Based Diagnosis of Ovarian Cancer Using MRI Images. Contrast Media Mol. Imaging 2021, 2021, 2146578. [Google Scholar] [CrossRef] [PubMed]
- Forstner, R.; Thomassin-Naggara, I.; Cunha, T.M.; Kinkel, K.; Masselli, G.; Kubik-Huch, R.; Spencer, J.A.; Rockall, A. ESUR Recommendations for MR Imaging of the Sonographically Indeterminate Adnexal Mass: An Update. Eur. Radiol. 2017, 27, 2248–2257. [Google Scholar] [CrossRef]
- Jeong, Y.-Y.; Outwater, E.K.; Kang, H.K. Imaging Evaluation of Ovarian Masses. RadioGraphics 2000, 20, 1445–1470. [Google Scholar] [CrossRef]
- Thomassin-Naggara, I.; Poncelet, E.; Jalaguier-Coudray, A.; Guerra, A.; Fournier, L.S.; Stojanovic, S.; Millet, I.; Bharwani, N.; Juhan, V.; Cunha, T.M.; et al. Ovarian-Adnexal Reporting Data System Magnetic Resonance Imaging (O-RADS MRI) Score for Risk Stratification of Sonographically Indeterminate Adnexal Masses. JAMA Netw. Open 2020, 3, e1919896. [Google Scholar] [CrossRef]
- Kang, S.K.; Reinhold, C.; Atri, M.; Benson, C.B.; Bhosale, P.R.; Jhingran, A.; Lakhman, Y.; Maturen, K.E.; Nicola, R.; Pandharipande, P.V.; et al. ACR Appropriateness Criteria for Staging And Follow-Up of Ovarian Cancer. J. Am. Coll. Radiol. 2018, 15, S198–S207. [Google Scholar] [CrossRef]
- Kobal, B.; Noventa, M.; Cvjeticanin, B.; Barbic, M.; Meglic, L.; Herzog, M.; Bordi, G.; Vitagliano, A.; Saccardi, C.; Skof, E. Primary Debulking Surgery versus Primary Neoadjuvant Chemotherapy for High Grade Advanced Stage Ovarian Cancer: Comparison of Survivals. Radiol. Oncol. 2018, 52, 307–319. [Google Scholar] [CrossRef]
- McEvoy, S.H.; Nougaret, S.; Abu-Rustum, N.R.; Vargas, H.A.; Sadowski, E.A.; Menias, C.O.; Shitano, F.; Fujii, S.; Sosa, R.E.; Escalon, J.G.; et al. Fertility-Sparing for Young Patients with Gynecologic Cancer: How MRI Can Guide Patient Selection Prior to Conservative Management. In Abdominal Radiology; Springer: New York, NY, USA, 2017; pp. 2488–2512. [Google Scholar] [CrossRef]
- Colombo, N.; Ledermann, J.A. Updated Treatment Recommendations for Newly Diagnosed Epithelial Ovarian Carcinoma from the ESMO Clinical Practice Guidelines. Ann. Oncol. 2021, 32, 1300–1303. [Google Scholar] [CrossRef]
- Mutch, D.G.; Prat, J. 2014 FIGO Staging for Ovarian, Fallopian Tube and Peritoneal Cancer. Gynecol. Oncol. 2014, 133, 401–404. [Google Scholar] [CrossRef]
- Timmerman, D.; Testa, A.C.; Bourne, T.; Ameye, L.; Jurkovic, D.; Van Holsbeke, C.; Paladini, D.; Van Calster, B.; Vergote, I.; Van Huffel, S.; et al. Simple Ultrasound-Based Rules for the Diagnosis of Ovarian Cancer. Ultrasound Obstet. Gynecol. 2008, 31, 681–690. [Google Scholar] [CrossRef] [PubMed]
- Viora, E.; Piovano, E.; Baima Poma, C.; Cotrino, I.; Castiglione, A.; Cavallero, C.; Sciarrone, A.; Bastonero, S.; Iskra, L.; Zola, P. The ADNEX Model to Triage Adnexal Masses: An External Validation Study and Comparison with the IOTA Two-Step Strategy and Subjective Assessment by an Experienced Ultrasound Operator. Eur. J. Obstet. Gynecol. Reprod. Biol. 2020, 247, 207–211. [Google Scholar] [CrossRef] [PubMed]
- Amor, F.; Vaccaro, H.; Alcázar, J.L.; León, M.; Craig, J.M.; Martinez, J. Gynecologic Imaging Reporting and Data System. J. Ultrasound Med. 2009, 28, 285–291. [Google Scholar] [CrossRef] [PubMed]
- Andreotti, R.F.; Timmerman, D.; Strachowski, L.M.; Froyman, W.; Benacerraf, B.R.; Bennett, G.L.; Bourne, T.; Brown, D.L.; Coleman, B.G.; Frates, M.C.; et al. O-RADS US Risk Stratification and Management System: A Consensus Guideline from the ACR Ovarian-Adnexal Reporting and Data System Committee. Radiology 2020, 294, 168–185. [Google Scholar] [CrossRef]
- Low, R.N.; Barone, R.M.; Lucero, J. Comparison of MRI and CT for Predicting the Peritoneal Cancer Index (PCI) Preoperatively in Patients Being Considered for Cytoreductive Surgical Procedures. Ann. Surg. Oncol. 2015, 22, 1708–1715. [Google Scholar] [CrossRef]
- Northridge, J.L. Adnexal Masses in Adolescents. Pediatr. Ann. 2020, 49, e183–e187. [Google Scholar] [CrossRef]
- Janssen, C.L.; Littooij, A.S.; Fiocco, M.; Huige, J.C.B.; de Krijger, R.R.; Hulsker, C.C.C.; Goverde, A.J.; Zsiros, J.; Mavinkurve-Groothuis, A.M.C. The Diagnostic Value of Magnetic Resonance Imaging in Differentiating Benign and Malignant Pediatric Ovarian Tumors. Pediatr. Radiol. 2021, 51, 427–434. [Google Scholar] [CrossRef]
- Webb, K.E.; Sakhel, K.; Chauhan, S.P.; Abuhamad, A.Z. Adnexal Mass during Pregnancy: A Review. Am. J. Perinatol. 2015, 32, 1010–1016. [Google Scholar] [CrossRef]
- Telischak, N.A.; Yeh, B.M.; Joe, B.N.; Westphalen, A.C.; Poder, L.; Coakley, F.V. MRI of Adnexal Masses in Pregnancy. Am. J. Roentgenol. 2008, 191, 364–370. [Google Scholar] [CrossRef]
- Botha, M.H.; Rajaram, S.; Karunaratne, K. Cancer in Pregnancy. Int. J. Gynecol. Obstet. 2018, 143, 137–142. [Google Scholar] [CrossRef]
- Yacobozzi, M.; Nguyen, D.; Rakita, D. Adnexal Masses in Pregnancy. Semin. Ultrasound CT MRI 2012, 33, 55–64. [Google Scholar] [CrossRef] [PubMed]
- Bourgioti, C.; Konidari, M.; Gourtsoyianni, S.; Moulopoulos, L.A. Imaging during Pregnancy: What the Radiologist Needs to Know. Diagn. Interv. Imaging 2021, 102, 593–603. [Google Scholar] [CrossRef] [PubMed]
- Yin, M.; Wang, T.; Li, S.; Zhang, X.; Yang, J. Decidualized Ovarian Endometrioma Mimicking Malignancy in Pregnancy: A Case Report and Literature Review. J. Ovarian Res. 2022, 15, 33. [Google Scholar] [CrossRef]
- Murase, E.; Siegelman, E.S.; Outwater, E.K.; Perez-Jaffe, L.A.; Tureck, R.W. Uterine Leiomyomas: Histopathologic Features, MR Imaging Findings, Differential Diagnosis, and Treatment. RadioGraphics 1999, 19, 1179–1197. [Google Scholar] [CrossRef]
- Jung, S.E.; Lee, J.M.; Rha, S.E.; Byun, J.Y.; Jung, J.I.; Hahn, S.T. CT and MR Imaging of Ovarian Tumors with Emphasis on Differential Diagnosis. RadioGraphics 2002, 22, 1305–1325. [Google Scholar] [CrossRef] [PubMed]
- Seidman, J.; Russell, P.; Kurman, R. Surface Epithelial Tumors of the Ovary. In Blaustein’s Pathology of the Female Genital Tract; Springer: New York, NY, USA, 2002; pp. 791–904. [Google Scholar]
- Thomassin-Naggara, I.; Aubert, E.; Rockall, A.; Jalaguier-Coudray, A.; Rouzier, R.; Daraï, E.; Bazot, M. Adnexal Masses: Development and Preliminary Validation of an MR Imaging Scoring System. Radiology 2013, 267, 432–443. [Google Scholar] [CrossRef] [PubMed]
- Boger-Megiddo, I.; Weiss, N.S. Histologic Subtypes and Laterality of Primary Epithelial Ovarian Tumors. Gynecol. Oncol. 2005, 97, 80–83. [Google Scholar] [CrossRef]
- Hart, W.R. Borderline Epithelial Tumors of the Ovary. Mod. Pathol. 2005, 18, S33–S50. [Google Scholar] [CrossRef]
- Folkins, A.K.; Longacre, T.A. Low-Grade Serous Neoplasia of the Female Genital Tract. Surg. Pathol. Clin. 2019, 12, 481–513. [Google Scholar] [CrossRef]
- Bazot, M.; Haouy, D.; Daraï, E.; Cortez, A.; Dechoux-Vodovar, S.; Thomassin-Naggara, I. Is MRI a Useful Tool to Distinguish between Serous and Mucinous Borderline Ovarian Tumours? Clin. Radiol. 2013, 68, e1–e8. [Google Scholar] [CrossRef]
- Outwater, E.K.; Huang, A.B.; Dunton, C.J.; Talerman, A.; Capuzzi, D.M. Papillary Projections in Ovarian Neoplasms: Appearance on MRI. J. Magn. Reson. Imaging 1997, 7, 689–695. [Google Scholar] [CrossRef] [PubMed]
- Marko, J.; Marko, K.I.; Pachigolla, S.L.; Crothers, B.A.; Mattu, R.; Wolfman, D.J. Mucinous Neoplasms of the Ovary: Radiologic-Pathologic Correlation. RadioGraphics 2019, 39, 982–997. [Google Scholar] [CrossRef] [PubMed]
- Peres, L.C.; Cushing-Haugen, K.L.; Köbel, M.; Harris, H.R.; Berchuck, A.; Rossing, M.A.; Schildkraut, J.M.; Doherty, J.A. Invasive Epithelial Ovarian Cancer Survival by Histotype and Disease Stage. JNCI J. Natl. Cancer Inst. 2019, 111, 60–68. [Google Scholar] [CrossRef]
- Okada, S.; Ohaki, Y.; Inoue, K.; Kawamura, T.; Hayashi, T.; Kato, T.; Kumazaki, T. Calcifications in Mucinous and Serous Cystic Ovarian Tumors. J. Nippon. Med. Sch. 2005, 72, 29–33. [Google Scholar] [CrossRef] [PubMed]
- Zhao, S.H.; Qiang, J.W.; Zhang, G.F.; Wang, S.J.; Qiu, H.Y.; Wang, L. MRI in Differentiating Ovarian Borderline from Benign Mucinous Cystadenoma: Pathological Correlation. J. Magn. Reson. Imaging 2014, 39, 162–166. [Google Scholar] [CrossRef]
- Okamoto, Y.; Tanaka, Y.O.; Tsunoda, H.; Yoshikawa, H.; Minami, M. Malignant or Borderline Mucinous Cystic Neoplasms Have a Larger Number of Loculi than Mucinous Cystadenoma: A Retrospective Study with MR. J. Magn. Reson. Imaging 2007, 26, 94–99. [Google Scholar] [CrossRef]
- Ferreira, C.R.; Carvalho, J.P.; Soares, F.A.; Siqueira, S.A.C.; Carvalho, F.M. Mucinous Ovarian Tumors Associated with Pseudomyxoma Peritonei of Adenomucinosis Type: Immunohistochemical Evidence That They Are Secondary Tumors. Int. J. Gynecol. Cancer 2008, 18, 59–65. [Google Scholar] [CrossRef]
- Fadare, O.; Parkash, V. Pathology of Endometrioid and Clear Cell Carcinoma of the Ovary. Surg. Pathol. Clin. 2019, 12, 529–564. [Google Scholar] [CrossRef]
- Watson, P.; Bützow, R.; Lynch, H.T.; Mecklin, J.-P.; Järvinen, H.J.; Vasen, H.F.A.; Madlensky, L.; Fidalgo, P.; Bernstein, I. The Clinical Features of Ovarian Cancer in Hereditary Nonpolyposis Colorectal Cancer. Gynecol. Oncol. 2001, 82, 223–228. [Google Scholar] [CrossRef]
- Matias-Guiu, X.; Stewart, C.J.R. Endometriosis-Associated Ovarian Neoplasia. Pathology 2018, 50, 190–204. [Google Scholar] [CrossRef]
- Tanaka, Y.O.; Yoshizako, T.; Nishida, M.; Yamaguchi, M.; Sugimura, K.; Itai, Y. Ovarian Carcinoma in Patients with Endometriosis. Am. J. Roentgenol. 2000, 175, 1423–1430. [Google Scholar] [CrossRef] [PubMed]
- Tanaka, Y.O.; Okada, S.; Yagi, T.; Satoh, T.; Oki, A.; Tsunoda, H.; Yoshikawa, H. MRI of Endometriotic Cysts in Association With Ovarian Carcinoma. Am. J. Roentgenol. 2010, 194, 355–361. [Google Scholar] [CrossRef] [PubMed]
- van Niekerk, C.C.; Bulten, J.; Vooijs, G.P.; Verbeek, A.L.M. The Association between Primary Endometrioid Carcinoma of the Ovary and Synchronous Malignancy of the Endometrium. Obstet. Gynecol. Int. 2010, 2010, 465162. [Google Scholar] [CrossRef]
- Matsuura, Y.; Robertson, G.; Marsden, D.E.; Kim, S.-N.; Gebski, V.; Hacker, N.F. Thromboembolic Complications in Patients with Clear Cell Carcinoma of the Ovary. Gynecol. Oncol. 2007, 104, 406–410. [Google Scholar] [CrossRef]
- Savvari, P.; Peitsidis, P.; Alevizaki, M.; Dimopoulos, M.-A.; Antsaklis, A.; Papadimitriou, C.A. Paraneoplastic Humorally Mediated Hypercalcemia Induced by Parathyroid Hormone-Related Protein in Gynecologic Malignancies: A Systematic Review. Onkologie 2009, 32, 517–523. [Google Scholar] [CrossRef] [PubMed]
- Avesani, G.; Caliolo, G.; Gui, B.; Petta, F.; Panico, C.; La Manna, V.; Moro, F.; Testa, A.C.; Scambia, G.; Manfredi, R. Pearls and Potential Pitfalls for Correct Diagnosis of Ovarian Cystadenofibroma in MRI: A Pictorial Essay. Korean J. Radiol. 2021, 22, 1809. [Google Scholar] [CrossRef]
- Tang, Y.Z.; Liyanage, S.; Narayanan, P.; Sahdev, A.; Sohaib, A.; Singh, N.; Rockall, A. The MRI Features of Histologically Proven Ovarian Cystadenofibromas—An Assessment of the Morphological and Enhancement Patterns. Eur. Radiol. 2013, 23, 48–56. [Google Scholar] [CrossRef] [PubMed]
- Jung, D.C.; Kim, S.H.; Kim, S.H. MR Imaging Findings of Ovarian Cystadenofibroma and Cystadenocarcinofibroma: Clues for the Differential Diagnosis. Korean J. Radiol. 2006, 7, 199. [Google Scholar] [CrossRef]
- Chen, J.; Wang, J.; Chen, X.; Wang, Y.; Wang, Z.; Li, D. Computed Tomography and Magnetic Resonance Imaging Features of Ovarian Fibrothecoma. Oncol. Lett. 2017, 14, 1172–1178. [Google Scholar] [CrossRef]
- Cho, Y.J.; Lee, H.S.; Kim, J.M.; Joo, K.Y.; Kim, M.-L. Clinical Characteristics and Surgical Management Options for Ovarian Fibroma/Fibrothecoma: A Study of 97 Cases. Gynecol. Obstet. Invest. 2013, 76, 182–187. [Google Scholar] [CrossRef]
- Shinagare, A.B.; Meylaerts, L.J.; Laury, A.R.; Mortele, K.J. MRI Features of Ovarian Fibroma and Fibrothecoma With Histopathologic Correlation. Am. J. Roentgenol. 2012, 198, W296–W303. [Google Scholar] [CrossRef] [PubMed]
- Zhang, H.; Zhang, G.-F.; Wang, T.-P.; Zhang, H. Value of 3.0 T Diffusion-Weighted Imaging in Discriminating Thecoma and Fibrothecoma from Other Adnexal Solid Masses. J. Ovarian Res. 2013, 6, 58. [Google Scholar] [CrossRef] [PubMed]
- Chung, B.M.; bin Park, S.; Lee, J.B.; Park, H.J.; Kim, Y.S.; Oh, Y.J. Magnetic Resonance Imaging Features of Ovarian Fibroma, Fibrothecoma, and Thecoma. Abdom. Imaging 2015, 40, 1263–1272. [Google Scholar] [CrossRef] [PubMed]
- Agostinho, L.; Horta, M.; Salvador, J.C.; Cunha, T.M. Benign Ovarian Lesions with Restricted Diffusion. Radiol. Bras. 2019, 52, 106–111. [Google Scholar] [CrossRef]
- Tanaka, Y.O.; Tsunoda, H.; Kitagawa, Y.; Ueno, T.; Yoshikawa, H.; Saida, Y. Functioning Ovarian Tumors: Direct and Indirect Findings at MR Imaging. RadioGraphics 2004, 24 (Suppl. 1), S147–S166. [Google Scholar] [CrossRef]
- Chen, H.; Liu, Y.; Shen, L.; Jiang, M.; Yang, Z.; Fang, G. Ovarian Thecoma-Fibroma Groups: Clinical and Sonographic Features with Pathological Comparison. J. Ovarian Res. 2016, 9, 81. [Google Scholar] [CrossRef]
- Thomassin-Naggara, I.; Darai, E.; Bazot, M. Gynecological Pelvic Infection: What Is the Role of Imaging? Diagn. Interv. Imaging 2012, 93, 491–499. [Google Scholar] [CrossRef]
- Revzin, M.V.; Mathur, M.; Dave, H.B.; Macer, M.L.; Spektor, M. Pelvic Inflammatory Disease: Multimodality Imaging Approach with Clinical-Pathologic Correlation. RadioGraphics 2016, 36, 1579–1596. [Google Scholar] [CrossRef]
- Tukeva, T.A.; Aronen, H.J.; Karjalainen, P.T.; Molander, P.; Paavonen, T.; Paavonen, J. MR Imaging in Pelvic Inflammatory Disease: Comparison with Laparoscopy and US. Radiology 1999, 210, 209–216. [Google Scholar] [CrossRef]
- Bonde, A.; Andreazza Dal Lago, E.; Foster, B.; Javadi, S.; Palmquist, S.; Bhosale, P. Utility of the Diffusion Weighted Sequence in Gynecological Imaging: Review Article. Cancers 2022, 14, 4468. [Google Scholar] [CrossRef]
- Takeuchi, M.; Matsuzaki, K.; Sano, N.; Furumoto, H.; Nishitani, H. Malignant Brenner Tumor with Transition from Benign to Malignant Components. J. Comput. Assist. Tomogr. 2008, 32, 553–554. [Google Scholar] [CrossRef] [PubMed]
- Moon, W.J.; Koh, B.H.; Kim, S.K.; Kim, Y.S.; Rhim, H.C.; Cho, O.K.; Hahm, C.K.; Byun, J.Y.; Cho, K.S.; Kim, S.H. Brenner Tumor of the Ovary: CT and MR Findings. J. Comput. Assist. Tomogr. 2000, 24, 72–76. [Google Scholar] [CrossRef] [PubMed]
- Euscher, E.D. Germ Cell Tumors of the Female Genital Tract. Surg. Pathol. Clin. 2019, 12, 621–649. [Google Scholar] [CrossRef] [PubMed]
- Makani, S.; Kim, W.; Gaba, A.R. Struma Ovarii with a Focus of Papillary Thyroid Cancer: A Case Report and Review of the Literature. Gynecol. Oncol. 2004, 94, 835–839. [Google Scholar] [CrossRef]
- Taylor, E.C.; Irshaid, L.; Mathur, M. Multimodality Imaging Approach to Ovarian Neoplasms with Pathologic Correlation. RadioGraphics 2020, 41, 289–315. [Google Scholar] [CrossRef]
- Elsherif, S.; Bourne, M.; Soule, E.; Lall, C.; Bhosale, P. Multimodality Imaging and Genomics of Granulosa Cell Tumors. Abdom. Radiol. 2020, 45, 812–827. [Google Scholar] [CrossRef]
- Zhang, H.; Zhang, H.; Gu, S.; Zhang, Y.; Liu, X.; Zhang, G. MR Findings of Primary Ovarian Granulosa Cell Tumor with Focus on the Differentiation with Other Ovarian Sex Cord-Stromal Tumors. J. Ovarian Res. 2018, 11, 46. [Google Scholar] [CrossRef]
- Fotopoulou, C.; Savvatis, K.; Braicu, E.-I.; Brink-Spalink, V.; Darb-Esfahani, S.; Lichtenegger, W.; Sehouli, J. Adult Granulosa Cell Tumors of the Ovary: Tumor Dissemination Pattern at Primary and Recurrent Situation, Surgical Outcome. Gynecol. Oncol. 2010, 119, 285–290. [Google Scholar] [CrossRef]
- Lagoo, A.S.; Robboy, S.J. Lymphoma of the Female Genital Tract: Current Status. Int. J. Gynecol. Pathol. 2006, 25, 1–21. [Google Scholar] [CrossRef]
- Slonimsky, E.; Korach, J.; Perri, T.; Davidson, T.; Apter, S.; Inbar, Y. Gynecological Lymphoma. J. Comput. Assist. Tomogr. 2018, 42, 435–440. [Google Scholar] [CrossRef]
- Crawshaw, J.; Sohaib, S.A.; Wotherspoon, A.; Shepherd, J.H. Primary Non-Hodgkin’s Lymphoma of the Ovaries: Imaging Findings. Br. J. Radiol. 2007, 80, e155–e158. [Google Scholar] [CrossRef] [PubMed]
- Agnes, A.; Biondi, A.; Ricci, R.; Gallotta, V.; D’Ugo, D.; Persiani, R. Krukenberg Tumors: Seed, Route and Soil. Surg. Oncol. 2017, 26, 438–445. [Google Scholar] [CrossRef] [PubMed]
- Lerwill, M.F.; Young, R.H. Metastatic Tumors of the Ovary. In Blaustein’s Pathology of the Female Genital Tract; Springer: New York, NY, USA, 2008; pp. 929–998. [Google Scholar]
- Koyama, T.; Mikami, Y.; Saga, T.; Tamai, K.; Togashi, K. Secondary Ovarian Tumors: Spectrum of CT and MR Features with Pathologic Correlation. Abdom. Imaging 2007, 32, 784–795. [Google Scholar] [CrossRef] [PubMed]
- Khunamornpong, S.; Suprasert, P.; Pojchamarnwiputh, S.; Na Chiangmai, W.; Settakorn, J.; Siriaunkgul, S. Primary and Metastatic Mucinous Adenocarcinomas of the Ovary: Evaluation of the Diagnostic Approach Using Tumor Size and Laterality. Gynecol. Oncol. 2006, 101, 152–157. [Google Scholar] [CrossRef]
- Xu, Y.; Yang, J.; Zhang, Z.; Zhang, G. MRI for Discriminating Metastatic Ovarian Tumors from Primary Epithelial Ovarian Cancers. J. Ovarian Res. 2015, 8, 61. [Google Scholar] [CrossRef]
- Kurokawa, R.; Nakai, Y.; Gonoi, W.; Mori, H.; Tsuruga, T.; Makise, N.; Ushiku, T.; Abe, O. Differentiation between Ovarian Metastasis from Colorectal Carcinoma and Primary Ovarian Carcinoma: Evaluation of Tumour Markers and “Mille-Feuille Sign” on Computed Tomography/Magnetic Resonance Imaging. Eur. J. Radiol. 2020, 124, 108823. [Google Scholar] [CrossRef]
- Talerman, A. Germ Cell Tumors of the Ovary. In Blaustein’s Pathology of the Female Genital Tract; Springer: New York, NY, USA, 2002; pp. 967–1034. [Google Scholar]
- Jezierska, M.; Gawrychowska, A.; Stefanowicz, J. Diagnostic, Prognostic and Predictive Markers in Pediatric Germ Cell Tumors—Past, Present and Future. Diagnostics 2022, 12, 278. [Google Scholar] [CrossRef]
- Heo, S.H.; Kim, J.W.; Shin, S.S.; Jeong, S.I.; Lim, H.S.; Choi, Y.D.; Lee, K.H.; Kang, W.D.; Jeong, Y.Y.; Kang, H.K. Review of Ovarian Tumors in Children and Adolescents: Radiologic-Pathologic Correlation. RadioGraphics 2014, 34, 2039–2055. [Google Scholar] [CrossRef]
- bin Park, S.; Kim, J.K.; Kim, K.-R.; Cho, K.-S. Imaging Findings of Complications and Unusual Manifestations of Ovarian Teratomas. RadioGraphics 2008, 28, 969–983. [Google Scholar] [CrossRef]
- Saleh, M.; Bhosale, P.; Menias, C.O.; Ramalingam, P.; Jensen, C.; Iyer, R.; Ganeshan, D. Ovarian Teratomas: Clinical Features, Imaging Findings and Management. Abdom. Radiol. 2021, 46, 2293–2307. [Google Scholar] [CrossRef]
- Outwater, E.K.; Siegelman, E.S.; Hunt, J.L. Ovarian Teratomas: Tumor Types and Imaging Characteristics. RadioGraphics 2001, 21, 475–490. [Google Scholar] [CrossRef] [PubMed]
- Nakayama, T.; Yoshimitsu, K.; Irie, H.; Aibe, H.; Tajima, T.; Nishie, A.; Asayama, Y.; Matake, K.; Kakihara, D.; Matsuura, S.; et al. Diffusion-Weighted Echo-Planar MR Imaging and ADC Mapping in the Differential Diagnosis of Ovarian Cystic Masses: Usefulness of Detecting Keratinoid Substances in Mature Cystic Teratomas. J. Magn. Reson. Imaging 2005, 22, 271–278. [Google Scholar] [CrossRef] [PubMed]
- Poncelet, E.; Delpierre, C.; Kerdraon, O.; Lucot, J.-P.; Collinet, P.; Bazot, M. Value of Dynamic Contrast-Enhanced MRI for Tissue Characterization of Ovarian Teratomas: Correlation with Histopathology. Clin. Radiol. 2013, 68, 909–916. [Google Scholar] [CrossRef] [PubMed]
- Kido, A.; Togashi, K.; Konishi, I.; Kataoka, M.L.; Koyama, T.; Ueda, H.; Fujii, S.; Konishi, J. Dermoid Cysts of the Ovary with Malignant Transformation: MR Appearance. Am. J. Roentgenol. 1999, 172, 445–449. [Google Scholar] [CrossRef]
- Verguts, J.; Amant, F.; Moerman, P.; Vergote, I. HPV Induced Ovarian Squamous Cell Carcinoma: Case Report and Review of the Literature. Arch. Gynecol. Obstet. 2007, 276, 285–289. [Google Scholar] [CrossRef]
- Yamaoka, T.; Togashi, K.; Koyama, T.; Fujiwara, T.; Higuchi, T.; Iwasa, Y.; Fujii, S.; Konishi, J. Immature Teratoma of the Ovary: Correlation of MR Imaging and Pathologic Findings. Eur. Radiol. 2003, 13, 313–319. [Google Scholar] [CrossRef]
- Laufer, M.; Goldstein, D. Benign and Malignant Ovarian Masses. In Pediatric and Adolescent Gynecology; Lippincott Williams & Wilkins: Philadelphia, PA, USA, 2005; p. 685. [Google Scholar]
- Kitajima, K.; Hayashi, M.; Kuwata, Y.; Imanaka, K.; Sugimura, K. MRI Appearances of Ovarian Dysgerminoma. Eur. J. Radiol. Extra 2007, 61, 23–25. [Google Scholar] [CrossRef]
- Shaaban, A.M.; Rezvani, M.; Elsayes, K.M.; Baskin, H.; Mourad, A.; Foster, B.R.; Jarboe, E.A.; Menias, C.O. Ovarian Malignant Germ Cell Tumors: Cellular Classification and Clinical and Imaging Features. RadioGraphics 2014, 34, 777–801. [Google Scholar] [CrossRef]
- Schwartz, N.; Timor-Tritsch, I.E.; WANG, E. Adnexal Masses in Pregnancy. Clin. Obstet. Gynecol. 2009, 52, 570–585. [Google Scholar] [CrossRef]
- van Holsbeke, C.; Amant, F.; Veldman, J.; de Boodt, A.; Moerman, P.; Timmerman, D. Hyperreactio Luteinalis in a Spontaneously Conceived Singleton Pregnancy. Ultrasound Obstet. Gynecol. 2009, 33, 371–373. [Google Scholar] [CrossRef]
- Cathcart, A.M.; Nezhat, F.R.; Emerson, J.; Pejovic, T.; Nezhat, C.H.; Nezhat, C.R. Adnexal Masses during Pregnancy: Diagnosis, Treatment, and Prognosis. Am. J. Obstet. Gynecol. 2022. [Google Scholar] [CrossRef] [PubMed]
- Barbieri, M.; Somigliana, E.; Oneda, S.; Ossola, M.W.; Acaia, B.; Fedele, L. Decidualized Ovarian Endometriosis in Pregnancy: A Challenging Diagnostic Entity. Hum. Reprod. 2009, 24, 1818–1824. [Google Scholar] [CrossRef] [PubMed]
- Takeuchi, M.; Matsuzaki, K.; Nishitani, H. Magnetic Resonance Manifestations of Decidualized Endometriomas During Pregnancy. J. Comput. Assist. Tomogr. 2008, 32, 353–355. [Google Scholar] [CrossRef] [PubMed]
- Bourgioti, C.; Preza, O.; Panourgias, E.; Chatoupis, K.; Antoniou, A.; Nikolaidou, M.E.; Moulopoulos, L.A. MR Imaging of Endometriosis: Spectrum of Disease. Diagn. Interv. Imaging 2017, 98, 751–767. [Google Scholar] [CrossRef]
- Thomassin-Naggara, I.; Fedida, B.; Sadowski, E.; Chevrier, M.-C.; Chabbert-Buffet, N.; Ballester, M.; Tavolaro, S.; Darai, E. Complex US Adnexal Masses during Pregnancy: Is Pelvic MR Imaging Accurate for Characterization? Eur. J. Radiol. 2017, 93, 200–208. [Google Scholar] [CrossRef]
- Bourgioti, C.; Konidari, M.; Moulopoulos, L.A. Imaging of Gynecologic Malignancy in a Reproductive Age Female. Radiol. Clin. N. Am. 2020, 58, 413–430. [Google Scholar] [CrossRef]
- Nougaret, S.; Nikolovski, I.; Paroder, V.; Vargas, H.A.; Sala, E.; Carrere, S.; Tetreau, R.; Hoeffel, C.; Forstner, R.; Lakhman, Y. MRI of Tumors and Tumor Mimics in the Female Pelvis: Anatomic Pelvic Space–Based Approach. RadioGraphics 2019, 39, 1205–1229. [Google Scholar] [CrossRef]
- Dhage-Ivatury, S.; Sugarbaker, P.H. Update on the Surgical Approach to Mucocele of the Appendix. J. Am. Coll. Surg. 2006, 202, 680–684. [Google Scholar] [CrossRef]
- Van Hooser, A.; Williams, T.R.; Myers, D.T. Mucinous Appendiceal Neoplasms: Pathologic Classification, Clinical Implications, Imaging Spectrum and Mimics. Abdom. Radiol. 2018, 43, 2913–2922. [Google Scholar] [CrossRef]
- Carr, N.J.; Cecil, T.D.; Mohamed, F.; Sobin, L.H.; Sugarbaker, P.H.; González-Moreno, S.; Taflampas, P.; Chapman, S.; Moran, B.J. A Consensus for Classification and Pathologic Reporting of Pseudomyxoma Peritonei and Associated Appendiceal Neoplasia. Am. J. Surg. Pathol. 2016, 40, 14–26. [Google Scholar] [CrossRef]
- Chira, R.I.; Nistor-Ciurba, C.C.; Mociran, A.; Mircea, P.A. Appendicular Mucinous Adenocarcinoma Associated with Pseudomyxoma Peritonei, a Rare and Difficult Imaging Diagnosis. Med. Ultrason. 2016, 18, 257. [Google Scholar] [CrossRef] [PubMed]
- Nishino, M.; Hayakawa, K.; Minami, M.; Yamamoto, A.; Ueda, H.; Takasu, K. Primary Retroperitoneal Neoplasms: CT and MR Imaging Findings with Anatomic and Pathologic Diagnostic Clues. RadioGraphics 2003, 23, 45–57. [Google Scholar] [CrossRef] [PubMed]
- Kransdorf, M.J.; Bancroft, L.W.; Peterson, J.J.; Murphey, M.D.; Foster, W.C.; Temple, H.T. Imaging of Fatty Tumors: Distinction of Lipoma and Well-Differentiated Liposarcoma. Radiology 2002, 224, 99–104. [Google Scholar] [CrossRef] [PubMed]
- Hoarau, N.; Slim, K.; da Ines, D. CT and MR Imaging of Retroperitoneal Schwannoma. Diagn. Interv. Imaging 2013, 94, 1133–1139. [Google Scholar] [CrossRef]
- Isobe, K.; Shimizu, T.; Akahane, T.; Kato, H. Imaging of Ancient Schwannoma. Am. J. Roentgenol. 2004, 183, 331–336. [Google Scholar] [CrossRef] [PubMed]
- Yu, Y.; Wu, J.; Ye, J.; Chen, M. Radiological Findings of Malignant Peripheral Nerve Sheath Tumor: Reports of Six Cases and Review of Literature. World J. Surg. Oncol. 2016, 14, 142. [Google Scholar] [CrossRef] [PubMed]























Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Bourgioti, C.; Konidari, M.; Moulopoulos, L.A. Manifestations of Ovarian Cancer in Relation to Other Pelvic Diseases by MRI. Cancers 2023, 15, 2106. https://doi.org/10.3390/cancers15072106
Bourgioti C, Konidari M, Moulopoulos LA. Manifestations of Ovarian Cancer in Relation to Other Pelvic Diseases by MRI. Cancers. 2023; 15(7):2106. https://doi.org/10.3390/cancers15072106
Chicago/Turabian StyleBourgioti, Charis, Marianna Konidari, and Lia Angela Moulopoulos. 2023. "Manifestations of Ovarian Cancer in Relation to Other Pelvic Diseases by MRI" Cancers 15, no. 7: 2106. https://doi.org/10.3390/cancers15072106
APA StyleBourgioti, C., Konidari, M., & Moulopoulos, L. A. (2023). Manifestations of Ovarian Cancer in Relation to Other Pelvic Diseases by MRI. Cancers, 15(7), 2106. https://doi.org/10.3390/cancers15072106