


Spectrum of High-Risk Mutations among Breast Cancer Patients Referred for Multigene Panel Testing in a Romanian Population

 , , , , , , , , , and
, , , , , , , , , and 
Abstract
Simple Summary
Abstract
1. Introduction
2. Materials and Methods
- High-penetrance breast cancer susceptibility genes: BRCA1, BRCA2, TP53, PALB2, CDH1, STK11, PTEN
- Moderate risk genes: ATM, CHEK2, BARD1, RAD51C, RAD51D, NF1
- Low risk genes: MSH2, MSH6, MLH1, PMS2, EPCAM
- Insufficient evidence: RAD50, RAD51B, BRIP1, NBN, BLM, FAM175A, MEN1, MRE11A, MUTYH, XRCC2, APC, RET, FANCA
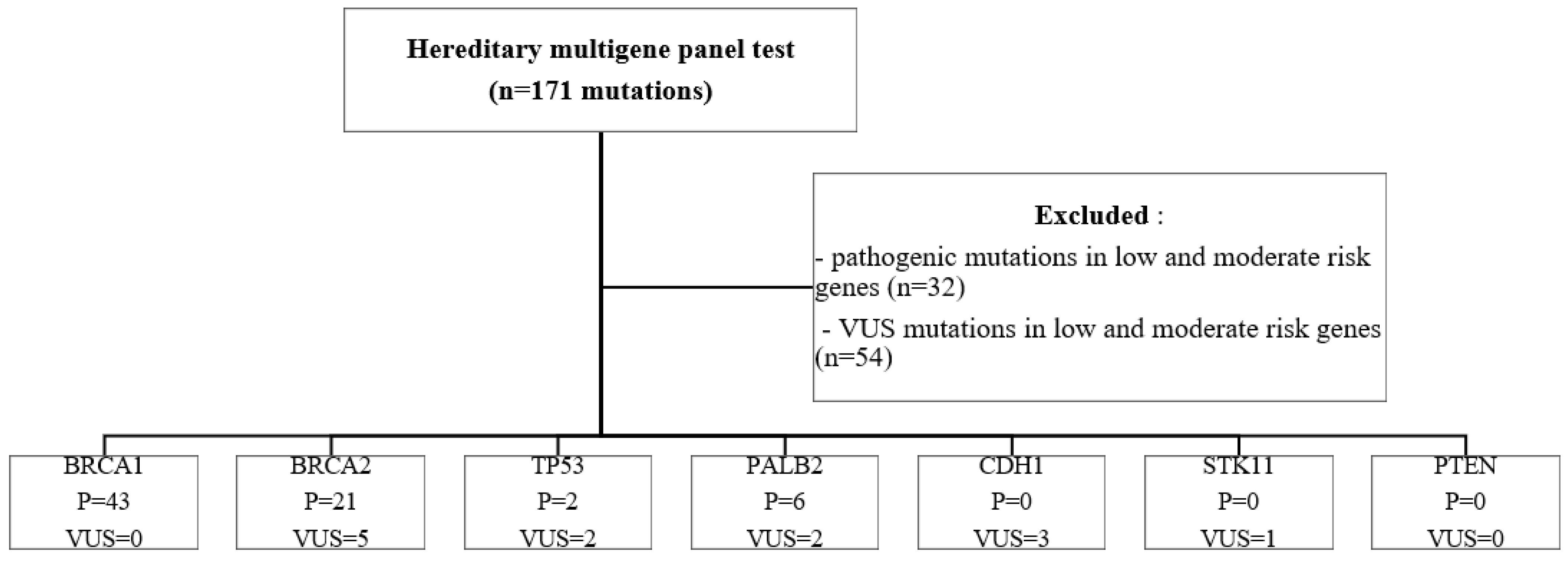
3. Results
4. Discussion
4.1. BRCA 1
4.2. BRCA 2
4.3. TP53
4.4. PALB2
4.5. CDH1
4.6. STK11
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Patruno, M.; De Summa, S.; Resta, N.; Caputo, M.; Costanzo, S.; Digennaro, M.; Pilato, B.; Bagnulo, R.; Pantaleo, A.; Simone, C.; et al. Spectrum of Germline Pathogenic Variants in BRCA1/2 Genes in the Apulian Southern Italy Population: Geographic Distribution and Evidence for Targeted Genetic Testing. Cancers 2021, 13, 4714. [Google Scholar] [CrossRef] [PubMed]
- Kuchenbaecker, K.B.; Hopper, J.L.; Barnes, D.R.; Phillips, K.A.; Mooij, T.M.; Roos-Blom, M.J.; Jervis, S.; Van Leeuwen, F.E.; Milne, R.L.; Andrieu, N.; et al. Risks of Breast, Ovarian, and Contralateral Breast Cancer for BRCA1 and BRCA2 Mutation Carriers. JAMA 2017, 317, 2402–2416. [Google Scholar] [CrossRef] [PubMed]
- Van Marcke, C.; De Leener, A.; Berlière, M.; Vikkula, M.; Duhoux, F.P. Routine use of gene panel testing in hereditary breast cancer should be performed with caution. Crit. Rev. Oncol. Hematol. 2016, 108, 33–39. [Google Scholar] [CrossRef] [PubMed]
- Tung, N.; Domchek, S.M.; Stadler, Z.; Nathanson, K.L.; Couch, F.; Garber, J.E.; Offit, K.; Robson, M.E. Counselling framework for moderate-penetrance cancer-susceptibility mutations. Nat. Rev. Clin. Oncol. 2016, 13, 581–588. [Google Scholar] [CrossRef] [PubMed]
- Daly, M.B.; Pal, T.; Berry, M.P.; Buys, S.S.; Dickson, P.; Domchek, S.M.; Elkhanany, A.; Friedman, S.; Goggins, M.; Hutton, M.L.; et al. Genetic/Familial High-Risk Assessment: Breast, Ovarian, and Pancreatic, Version 2.2021, NCCN Clinical Practice Guidelines in Oncology. J. Natl. Compr. Cancer Netw. 2021, 19, 77–102. [Google Scholar] [CrossRef]
- Pintican, R.M.; Chiorean, A.; Duma, M.; Feier, D.; Szep, M.; Eniu, D.; Goidescu, I.; Dudea, S. Are Mutation Carrier Patients Different from Non-Carrier Patients? Genetic, Pathology, and US Features of Patients with Breast Cancer. Cancers 2022, 14, 2759. Available online: https://www.mdpi.com/2072-6694/14/11/2759 (accessed on 12 January 2022). [CrossRef]
- Vidra, R.; Ciuleanu, T.E.; Nemeș, A.; Pascu, O.; Heroiu, A.M.; Antone, N.; Vidrean, A.I.; Oprean, C.M.; Pop, L.A.; Berindan-Neagoe, I.; et al. Spectrum of BRCA1/2 Mutations in Romanian Breast and Ovarian Cancer Patients. Int. J. Environ. Res. Public Health 2022, 19, 4314. [Google Scholar] [CrossRef]
- Goidescu, I.G.; Eniu, D.T.; Caracostea, G.V.; Cruciat, G.; Stamatian, F. Associations of pathogenic mutations responsible for breast cancer risk with histology and immunohistochemistry in Romanian population. Rev. Romana Med. Lab. 2018, 26, 165–175. [Google Scholar] [CrossRef]
- Mehta, A.; Vasudevan, S.; Sharma, S.K.; Kumar, D.; Panigrahi, M.; Suryavanshi, M.; Gupta, G. Germline BRCA1 and BRCA2 deleterious mutations and variants of unknown clinical significance associated with breast/ovarian cancer: A report from North India. Cancer Manag. Res. 2018, 10, 6505–6516. [Google Scholar] [CrossRef]
- Laitman, Y.; Friebel, T.M.; Yannoukakos, D.; Fostira, F.; Konstantopoulou, I.; Figlioli, G.; Bonanni, B.; Manoukian, S.; Zuradelli, M.; Tondini, C.; et al. The spectrum of BRCA1 and BRCA2 pathogenic sequence variants in Middle Eastern, North African, and South European countries. Hum. Mutat. 2019, 40, e1–e23. [Google Scholar] [CrossRef]
- Gomes, R.; Soares, B.L.; Felicio, P.S.; Michelli, R.; Netto, C.B.; Alemar, B.; Ashton-Prolla, P.; Palmero, E.I.; Moreira, M.Â.M. Haplotypic characterization of BRCA1 c.5266dupC, the prevailing mutation in Brazilian hereditary breast/ovarian cancer. Genet. Mol. Biol. 2020, 43, e20190072. [Google Scholar] [CrossRef]
- Gorski, B.; Byrski, T.; Huzarski, T.; Jakubowska, A.; Menkiszak, J.; Gronwald, J.; Płużańska, A.; Bębenek, M.; Grzybowska, E.; Narod, S.A.; et al. Founder mutations in the BRCA1 gene in Polish families with breast-ovarian cancer. Am. J. Hum. Genet. 2000, 66, 1963–1968. [Google Scholar] [CrossRef] [PubMed]
- Machackova, E.; Foretova, L.; Lukesova, M.; Vasickova, P.; Navratilova, M.; Coene, I.; Pavlu, H.; Kosinova, V.; Kuklova, J.; Claes, K. Spectrum and characterisation of BRCA1 and BRCA2 deleterious mutations in high-risk Czech patients with breast and/or ovarian cancer. BMC Cancer 2008, 8, 140. [Google Scholar] [CrossRef]
- Janavičius, R.; Rudaitis, V.; Mickys, U.; Elsakov, P.; Griškevičius, L. Comprehensive BRCA1 and BRCA2 mutational profile in Lithuania. Cancer Genet. 2014, 207, 195–205. [Google Scholar] [CrossRef]
- Uglanitsa, N.; Oszurek, O.; Uglanitsa, K.; Savonievich, E.; Lubiński, J.; Cybulski, C.; Debniak, T.; Narod, S.A.; Gronwald, J. The contribution of founder mutations in BRCA1 to breast cancer in Belarus. Clin. Genet. 2010, 78, 377–380. [Google Scholar] [CrossRef] [PubMed]
- Sokolenko, A.P.; Rozanov, M.E.; Mitiushkina, N.V.; Sherina, N.Y.; Iyevleva, A.G.; Chekmariova, E.V.; Buslov, K.G.; Shilov, E.S.; Togo, A.V.; Bit-Sava, E.M.; et al. Founder mutations in early-onset, familial and bilateral breast cancer patients from Russia. Fam. Cancer 2007, 6, 281–286. [Google Scholar] [CrossRef]
- Hamel, N.; Feng, B.J.; Foretova, L.; Stoppa-Lyonnet, D.; Narod, S.A.; Imyanitov, E.; Sinilnikova, O.; Tihomirova, L.; Lubinski, J.; Gronwald, J.; et al. On the origin and diffusion of BRCA1 c.5266dupC (5382insC) in European populations. Eur. J. Hum. Genet. 2011, 19, 300–306. [Google Scholar] [CrossRef] [PubMed]
- Gorodetska, I.; Serga, S.; Levkovich, N.; Lahuta, T.; Ostapchenko, L.; Demydov, S.; Anikusko, N.; Cheshuk, V.; Smolanka, I.; Sklyar, S.; et al. The frequency of BRCA1 founder mutation c.5266dupC (5382insC) in breast cancer patients from Ukraine. Hered. Cancer Clin. Pract. 2015, 13, 19. [Google Scholar] [CrossRef]
- Zoure, A.A.; Slaoui, M.; Bambara, H.A.; Sawadogo, A.Y.; Compaoré, T.R.; Ouédraogo, N.L.M.; El Mzibri, M.; Attaleb, M.; Traoré, S.S.; Simpore, J.; et al. BRCA1 c.68_69delAG (exon2), c.181T>G (exon5), c.798_799delTT and 943ins10 (exon11) mutations in Burkina Faso. J. Public Health Afr. 2018, 9, 663. [Google Scholar] [CrossRef]
- Wojcik, P.; Jasiówka, M.; Strycharz, E.; Sobol, M.; Hodorowicz-Zaniewska, D.; Skotnicki, P.; Byrski, T.; Blecharz, P.; Marczyk, E.; Cedrych, I.; et al. Recurrent mutations of BRCA1, BRCA2 and PALB2 in the population of breast and ovarian cancer patients in Southern Poland. Hered. Cancer Clin. Pract. 2016, 14, 5. [Google Scholar] [CrossRef]
- Janavičius, R. Founder BRCA1/2 mutations in the Europe: Implications for hereditary breast-ovarian cancer prevention and control. EPMA J. 2010, 1, 397–412. [Google Scholar] [CrossRef] [PubMed]
- Negura, L.; Uhrhammer, N.; Negura, A.; Artenie, V.; Carasevici, E.; Bignon, Y.-J. Complete BRCA mutation screening in breast and ovarian cancer predisposition families from a North-Eastern Romanian population. Fam. Cancer 2010, 9, 519–523. [Google Scholar] [CrossRef] [PubMed]
- Goidescu, I.G.; Caracostea, G.; Eniu, D.T.; Stamatian, F.V. Prevalence of deleterious mutations among patients with breast cancer referred for multigene panel testing in a Romanian population. Clujul Med. 2018, 91, 157–165. [Google Scholar] [CrossRef] [PubMed]
- Schroeder, C.; Faust, U.; Sturm, M.; Hackmann, K.; Grundmann, K.; Harmuth, F.; Bosse, K.; Kehrer, M.; Benkert, T.; Klink, B.; et al. HBOC multi-gene panel testing: Comparison of two sequencing centers. Breast Cancer Res Treat. 2015, 152, 129–136. [Google Scholar] [CrossRef]
- Surowy, H.M.; Sutter, C.; Mittnacht, M.; Klaes, R.; Schaefer, D.; Evers, C.; Burgemeister, A.L.; Goehringer, C.; Dikow, N.; Heil, J.; et al. Clinical and molecular characterization of the BRCA2 p.Asn3124Ile variant reveals substantial evidence for pathogenic significance. Breast Cancer Res. Treat. 2014, 145, 451–460. [Google Scholar] [CrossRef]
- Stegel, V.; Krajc, M.; Žgajnar, J.; Teugels, E.; De Grève, J.; Hočevar, M.; Novaković, S. The occurrence of germline BRCA1 and BRCA2 sequence alterations in Slovenian population. BMC Med. Genet. 2011, 12, 9. [Google Scholar] [CrossRef]
- Tea, M.K.M.; Kroiss, R.; Muhr, D.; Fuerhauser-Rappaport, C.; Oefner, P.; Wagner, T.M.; Singer, C.F. Central European BRCA2 mutation carriers: Birth cohort status correlates with onset of breast cancer. Maturitas 2014, 77, 68–72. [Google Scholar] [CrossRef]
- Bressac, B.; Kew, M.; Wands, J.; Ozturk, M. Selective G to T mutations of p53 gene in hepatocellular carcinoma from southern Africa. Nature 1991, 350, 429–431. [Google Scholar] [CrossRef]
- Kitayner, M.; Rozenberg, H.; Rohs, R.; Suad, O.; Rabinovich, D.; Honig, B.; Shakked, Z. Diversity in DNA recognition by p53 revealed by crystal structures with Hoogsteen base pairs. Nat. Struct. Mol. Biol. 2010, 17, 423–429. [Google Scholar] [CrossRef]
- Lo Nigro, C.; Vivenza, D.; Monteverde, M.; Lattanzio, L.; Gojis, O.; Garrone, O.; Comino, A.; Merlano, M.; Quinlan, P.R.; Syed, N.; et al. High frequency of complex TP53 mutations in CNS metastases from breast cancer. Br. J. Cancer 2012, 106, 397–404. [Google Scholar] [CrossRef]
- Pritzlaff, M.; Summerour, P.; McFarland, R.; Li, S.; Reineke, P.; Dolinsky, J.S.; Goldgar, D.E.; Shimelis, H.; Couch, F.J.; Chao, E.C.; et al. Male breast cancer in a multi-gene panel testing cohort: Insights and unexpected results. Breast Cancer Res. Treat. 2017, 161, 575–586. [Google Scholar] [CrossRef] [PubMed]
- Noskowicz, M.; Bogdanova, N.; Bermisheva, M.; Takhirova, Z.; Antonenkova, N.; Khusnutdinova, E.; Bremer, M.; Christiansen, H.; Park-Simon, T.W.; Hillemanns, P.; et al. Prevalence of PALB2 mutation c.509_510delGA in unselected breast cancer patients from Central and Eastern Europe. Fam. Cancer 2014, 13, 137–142. [Google Scholar] [CrossRef]
- Dansonka-Mieszkowska, A.; Kluska, A.; Moes, J.; Dabrowska, M.; Nowakowska, D.; Niwinska, A.; Derlatka, P.; Cendrowski, K.; Kupryjanczyk, J. A novel germline PALB2 deletion in Polish breast and ovarian cancer patients. BMC Med. Genet. 2010, 11, 1–9. [Google Scholar] [CrossRef]
- Bogdanova, N.; Sokolenko, A.P.; Iyevleva, A.G.; Abysheva, S.N.; Blaut, M.; Bremer, M.; Christiansen, H.; Rave-Fränk, M.; Dörk, T.; Imyanitov, E.N. PALB2 mutations in German and Russian patients with bilateral breast cancer. Breast Cancer Res. Treat. 2011, 126, 545–550. [Google Scholar] [CrossRef]
- Dudley, B.; Karloski, E.; Monzon, F.A.; Singhi, A.D.; Lincoln, S.E.; Bahary, N.; Brand, R.E. Germline mutation prevalence in individuals with pancreatic cancer and a history of previous malignancy. Cancer 2018, 124, 1691–1700. [Google Scholar] [CrossRef] [PubMed]
- Foley, S.B.; Rios, J.J.; Mgbemena, V.E.; Robinson, L.S.; Hampel, H.L.; Toland, A.E.; Durham, L.; Ross, T. S Use of Whole Genome Sequencing for Diagnosis and Discovery in the Cancer Genetics Clinic. EBioMedicine 2015, 2, 74–81. [Google Scholar] [CrossRef] [PubMed]
- Slade, D. PARP and PARG inhibitors in cancer treatment. Genes Dev. 2020, 34, 360–394. [Google Scholar] [CrossRef] [PubMed]
- Shadbad, M.A.; Safaei, S.; Brunetti, O.; Derakhshani, A.; Lotfinejad, P.; Mokhtarzadeh, A.; Hemmat, N.; Racanelli, V.; Solimando, A.G.; Argentiero, A.; et al. A Systematic Review on the Therapeutic Potentiality of PD-L1-Inhibiting MicroRNAs for Triple-Negative Breast Cancer: Toward Single-Cell Sequencing-Guided Biomimetic Delivery. Genes 2021, 12, 1206. [Google Scholar] [CrossRef]
- Wei, Y.; Jasbi, P.; Shi, X.; Turner, C.; Hrovat, J.; Liu, L.; Rabena, Y.; Porter, P.; Gu, H. Early Breast Cancer Detection Using Untargeted and Targeted Metabolomics. J. Proteome Res. 2021, 20, 3124–3133. [Google Scholar] [CrossRef]
- Liu, Y.; Helgadottir, H.T.; Kharaziha, P.; Choi, J.; López-Giráldez, F.; Mane, S.M.; Höiom, V.; Juhlin, C.C.; Larsson, C.; Bajalica-Lagercrantz, S. Whole-Exome Sequencing of Germline Variants in Non-BRCA Families with Hereditary Breast Cancer. Biomedicines 2022, 10, 1004. [Google Scholar] [CrossRef]



{kind=link}
{kind=link}
| >60% | 41–60% | 15–40% | <15% |
|---|---|---|---|
| BRCA1 | CDH 1 | ATM | MLH1 |
| BRCA2 | PALB2 | BARD1 | MSH2 |
| TP53 | PTEN | CHEK2 | MSH6 |
| STK11 | NF1 | PMS2 | |
| RAD51C | EPCAM | ||
| RAD51D |
| HGVS Mutation | Cases | Percentage | Variant | Type |
|---|---|---|---|---|
| c.3607C>T | 14 | 32.55 | Pathogenic | Nonsense |
| c.5266dupC | 11 | 25.58 | Pathogenic | Frameshift duplication |
| c.181T>G | 3 | 6.97 | Pathogenic | Missense |
| c.3700_3704delGTAAA | 3 | 6.97 | Pathogenic | Frameshift deletion |
| c.2241dupC | 2 | 4.65 | Pathogenic | Frameshift duplication |
| c.843_846delCTCA | 2 | 4.65 | Pathogenic | Frameshift deletion |
| c.135-2A>G | 1 | 2.33 | Pathogenic | Frameshift–splice acceptor |
| c.4035delA | 1 | 2.33 | Pathogenic | Frameshift deletion |
| c.1789G>A | 1 | 2.33 | Pathogenic | Nonsense |
| c.737delT | 1 | 2.33 | Pathogenic | Frameshift deletion |
| c.3187C>T | 1 | 2.33 | Pathogenic | Single nucleotide variant |
| c.4986 + 6T>C | 1 | 2.33 | Pathogenic | Single nucleotide variant |
| c.212 + 1G>T | 1 | 2.33 | Pathogenic | Single nucleotide variant |
| c.5030_5033delCTAA | 1 | 2.33 | Pathogenic | Frameshift deletion |
| HGVS Mutation | Cases | Percentage | Variant | Type |
|---|---|---|---|---|
| c.9371A>T | 9 | 42.85 | Pathogenic | Missense |
| c.8755-1G>A | 3 | 14.28 | Pathogenic | Frameshift–splice acceptor |
| c.1528G>T | 1 | 4.76 | Pathogenic | Nonsense |
| c.9253delA | 1 | 4.76 | Pathogenic | Frameshift deletion |
| c.7007G>C | 1 | 4.76 | Pathogenic | Missense |
| c.8695C>T | 1 | 4.76 | Pathogenic | Nonsense |
| c.7209_7212delCAAAinsGG | 1 | 4.76 | Pathogenic | Frameshift deletion |
| c.6557C>A | 1 | 4.76 | Pathogenic | Single nucleotide variant |
| c.793 + 1G>A | 1 | 4.76 | Pathogenic | Single nucleotide variant |
| c.3462delC | 1 | 4.76 | Pathogenic | Frameshift deletion |
| c.8655dupA pat | 1 | 4.76 | Pathogenic | Frameshift duplication |
| HGVS Mutation | Cases | Percentage | Variant | Type |
|---|---|---|---|---|
| c.93dupA | 3 | 50% | Pathogenic | Frameshift duplication |
| c.509_510delGA | 1 | 16.6% | Pathogenic | Frameshift deletion |
| c.3549C>G | 1 | 16.6% | Pathogenic | Nonsense |
| c.79G>T | 1 | 16.6% | Pathogenic | Nonsense |
| No | Pathogenic Variant | Pathogenic Variant | VUS | VUS |
|---|---|---|---|---|
| 1 | BRCA 1 c.843_846delCTCA | CHEK2 c.470T>C | - | - |
| 2 | RAD51C c.905-2A>G | MUTYH c.536A>G | - | - |
| 3 | ATM c.5318delA | MUTYH c.721C>T | - | - |
| 4 | ATM c.7630-2A>C | CHEK2 c.444\ + 1G>A | - | - |
| 5 | BRCA1 c.3700_3704delGTAAA | BRCA 2 c.9371A>T | - | - |
| 6 | CHEK 2 1283C>T | BLM c.1642C>T | - | - |
| 7 | BRCA1 c.135-2A>G | - | MUTYH c.158-3C>T | |
| 8 | BRCA1 c.2241dupC | - | MEN1 c.777G>A | - |
| 9 | BRCA 1 c.3700_3704delGTAAA | - | CDH1 c.1297G>A | - |
| 10 | BRCA 1 c.3700_3704delGTAAA | - | ATM c.2735G>A | - |
| 11 | BRCA 1 c.5266dupC | - | FANCM c.1576C>G | - |
| 12 | BRCA 2 c.9371A>T | - | ATM c.2735G>A | - |
| 13 | CHEK2 c.1232G>A | - | RAD50 c900G>A | - |
| 14 | NBN c.657_661delACAAA | - | MRE11A c.1091G>A | - |
| 15 | BRCA2 c.9371A>T | - | RAD51B c.976C>G | - |
| 16 | - | - | ATM c.9077T>G | BRCA2 c.3547G>C |
| 17 | - | - | BARD 1 c.1915T>C | RAD51C c.790G>A |
| 18 | - | - | NBN c.511A>G | TP53 c.847C>T |
| 19 | - | - | MSH6 c.2189A>G | RAD51C c.1063G>A |
| 20 | - | - | RAD50 c.1663A>G | RAD51C c.790G>A |
| 21 | - | - | ATM c.1444A>C | FANCA c.2715A>G |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Goidescu, I.G.; Nemeti, G.; Surcel, M.; Caracostea, G.; Florian, A.R.; Cruciat, G.; Staicu, A.; Muresan, D.; Goidescu, C.; Pintican, R.; et al. Spectrum of High-Risk Mutations among Breast Cancer Patients Referred for Multigene Panel Testing in a Romanian Population. Cancers 2023, 15, 1895. https://doi.org/10.3390/cancers15061895
Goidescu IG, Nemeti G, Surcel M, Caracostea G, Florian AR, Cruciat G, Staicu A, Muresan D, Goidescu C, Pintican R, et al. Spectrum of High-Risk Mutations among Breast Cancer Patients Referred for Multigene Panel Testing in a Romanian Population. Cancers. 2023; 15(6):1895. https://doi.org/10.3390/cancers15061895
Chicago/Turabian StyleGoidescu, Iulian Gabriel, Georgiana Nemeti, Mihai Surcel, Gabriela Caracostea, Andreea Roxana Florian, Gheorghe Cruciat, Adelina Staicu, Daniel Muresan, Cerasela Goidescu, Roxana Pintican, and et al. 2023. "Spectrum of High-Risk Mutations among Breast Cancer Patients Referred for Multigene Panel Testing in a Romanian Population" Cancers 15, no. 6: 1895. https://doi.org/10.3390/cancers15061895
APA StyleGoidescu, I. G., Nemeti, G., Surcel, M., Caracostea, G., Florian, A. R., Cruciat, G., Staicu, A., Muresan, D., Goidescu, C., Pintican, R., & Eniu, D. T. (2023). Spectrum of High-Risk Mutations among Breast Cancer Patients Referred for Multigene Panel Testing in a Romanian Population. Cancers, 15(6), 1895. https://doi.org/10.3390/cancers15061895