
Breast Cancer Risk and Breast-Cancer-Specific Mortality following Risk-Reducing Salpingo-Oophorectomy in BRCA Carriers: A Systematic Review and Meta-Analysis

 , , ,
, , ,  ,
, 
Simple Summary
Abstract
1. Introduction
2. Materials and Methods
2.1. Search Strategy and Selection Criteria
2.2. Data Extraction and Quality Assessment
2.3. Data Analysis
3. Results
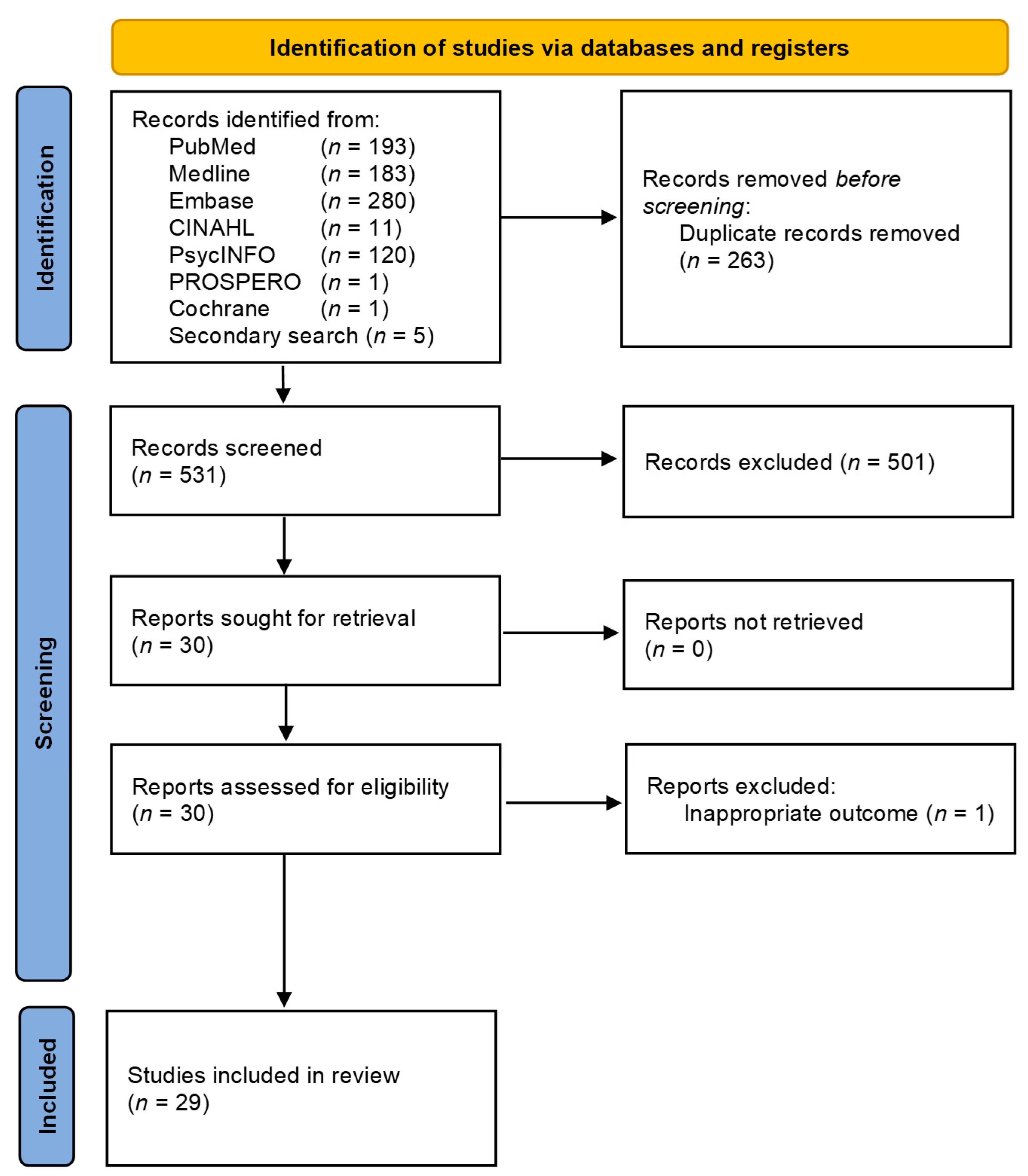
3.1. Study Selection and Characteristics
3.2. Risk of Bias
3.3. Quantitative Synthesis of Results
4. Discussion
4.1. Main Findings
4.2. Comparison with Existing Literature
4.3. Strengths and Limitations
4.4. Implications
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Antoniou, A.; Pharoah, P.D.; Narod, S.; Risch, H.A.; Eyfjord, J.E.; Hopper, J.L.; Loman, N.; Olsson, H.; Johannsson, O.; Borg, A.; et al. Average risks of breast and ovarian cancer associated with BRCA1 or BRCA2 mutations detected in case Series unselected for family history: A combined analysis of 22 studies. Am. J. Hum. Genet. 2003, 72, 1117–1130. [Google Scholar] [CrossRef] [PubMed]
- Chen, S.; Parmigiani, G. Meta-analysis of BRCA1 and BRCA2 penetrance. J. Clin. Oncol. 2007, 25, 1329–1333. [Google Scholar] [CrossRef] [PubMed]
- Kuchenbaecker, K.B.; Hopper, J.L.; Barnes, D.R.; Phillips, K.A.; Mooij, T.M.; Roos-Blom, M.J.; Jervis, S.; van Leeuwen, F.E.; Milne, R.L.; Andrieu, N.; et al. Risks of Breast, Ovarian, and Contralateral Breast Cancer for BRCA1 and BRCA2 Mutation Carriers. JAMA 2017, 317, 2402–2416. [Google Scholar] [CrossRef] [PubMed]
- Evans, D.G.; Shenton, A.; Woodward, E.; Lalloo, F.; Howell, A.; Maher, E.R. Penetrance estimates for BRCA1 and BRCA2 based on genetic testing in a Clinical Cancer Genetics service setting: Risks of breast/ovarian cancer quoted should reflect the cancer burden in the family. BMC Cancer 2008, 8, 155. [Google Scholar] [CrossRef]
- Menon, U.; Harper, J.; Sharma, A.; Fraser, L.; Burnell, M.; ElMasry, K.; Rodeck, C.; Jacobs, I. Views of BRCA gene mutation carriers on preimplantation genetic diagnosis as a reproductive option for hereditary breast and ovarian cancer. Hum. Reprod. 2007, 22, 1573–1577. [Google Scholar] [CrossRef]
- Rebbeck, T.R.; Friebel, T.; Lynch, H.T.; Neuhausen, S.L.; Van’t Veer, L.; Garber, J.E.; Evans, G.R.; Narod, S.A.; Isaacs, C.; Matloff, E.; et al. Bilateral prophylactic mastectomy reduces breast cancer risk in BRCA1 and BRCA2 mutation carriers: The PROSE Study Group. J. Clin. Oncol. 2004, 22, 1055–1062. [Google Scholar] [CrossRef]
- Cuzick, J.; Sestak, I.; Bonanni, B.; Costantino, J.P.; Cummings, S.; DeCensi, A.; Dowsett, M.; Forbes, J.F.; Ford, L.; LaCroix, A.Z.; et al. Selective oestrogen receptor modulators in prevention of breast cancer: An updated meta-analysis of individual participant data. Lancet 2013, 381, 1827–1834. [Google Scholar] [CrossRef]
- Cuzick, J.; Sestak, I.; Forbes, J.F.; Dowsett, M.; Cawthorn, S.; Mansel, R.E.; Loibl, S.; Bonanni, B.; Evans, D.G.; Howell, A.; et al. Use of anastrozole for breast cancer prevention (IBIS-II): Long-term results of a randomised controlled trial. Lancet 2019, 395, 117–122. [Google Scholar] [CrossRef]
- Kauff, N.D.; Satagopan, J.M.; Robson, M.E.; Scheuer, L.; Hensley, M.; Hudis, C.A.; Ellis, N.A.; Boyd, J.; Borgen, P.I.; Barakat, R.R.; et al. Risk-reducing salpingo-oophorectomy in women with a BRCA1 or BRCA2 mutation. N. Engl. J. Med. 2002, 346, 1609–1615. [Google Scholar] [CrossRef]
- Rebbeck, T.R.; Lynch, H.T.; Neuhausen, S.L.; Narod, S.A.; Van’t Veer, L.; Garber, J.E.; Evans, G.; Isaacs, C.; Daly, M.B.; Matloff, E.; et al. Prophylactic oophorectomy in carriers of BRCA1 or BRCA2 mutations. N. Engl. J. Med. 2002, 346, 1616–1622. [Google Scholar] [CrossRef]
- Kauff, N.D.; Domchek, S.M.; Friebel, T.M.; Robson, M.E.; Lee, J.; Garber, J.E.; Isaacs, C.; Evans, D.G.; Lynch, H.; Eeles, R.A.; et al. Risk-reducing salpingo-oophorectomy for the prevention of BRCA1- and BRCA2-associated breast and gynecologic cancer: A multicenter, prospective study. J. Clin. Oncol. 2008, 26, 1331–1337. [Google Scholar] [CrossRef]
- Finch, A.; Beiner, M.; Lubinski, J.; Lynch, H.T.; Moller, P.; Rosen, B.; Murphy, J.; Ghadirian, P.; Friedman, E.; Foulkes, W.D.; et al. Salpingo-oophorectomy and the risk of ovarian, fallopian tube, and peritoneal cancers in women with a BRCA1 or BRCA2 Mutation. JAMA 2006, 296, 185–192. [Google Scholar] [CrossRef]
- Manchanda, R.; Abdelraheim, A.; Johnson, M.; Rosenthal, A.N.; Benjamin, E.; Brunell, C.; Burnell, M.; Side, L.; Gessler, S.; Saridogan, E.; et al. Outcome of risk-reducing salpingo-oophorectomy in BRCA carriers and women of unknown mutation status. Int. J. Obstet. Gynaecol. 2011, 118, 814–824. [Google Scholar] [CrossRef]
- Restaino, S.; Finelli, A.; Pellecchia, G.; Biasioli, A.; Mauro, J.; Ronsini, C.; Martina, M.D.; Arcieri, M.; Della Corte, L.; Sorrentino, F.; et al. Scar-Free Laparoscopy in BRCA-Mutated Women. Medicina 2022, 58, 943. [Google Scholar] [CrossRef]
- Beattie, M.S.; Crawford, B.; Lin, F.; Vittinghoff, E.; Ziegler, J. Uptake, time course, and predictors of risk-reducing surgeries in BRCA carriers. Genet. Test. Mol. Biomark. 2009, 13, 51–56. [Google Scholar] [CrossRef]
- Botkin, J.R.; Smith, K.R.; Croyle, R.T.; Baty, B.J.; Wylie, J.E.; Dutson, D.; Chan, A.; Hamann, H.A.; Lerman, C.; McDonald, J.; et al. Genetic testing for a BRCA1 mutation: Prophylactic surgery and screening behavior in women 2 years post testing. Am. J. Med. Genet. Part A 2003, 118A, 201–209. [Google Scholar] [CrossRef]
- Bradbury, A.R.; Ibe, C.N.; Dignam, J.J.; Cummings, S.A.; Verp, M.; White, M.A.; Artioli, G.; Dudlicek, L.; Olopade, O.I. Uptake and timing of bilateral prophylactic salpingo-oophorectomy among BRCA1 and BRCA2 mutation carriers. Genet. Med. 2008, 10, 161–166. [Google Scholar] [CrossRef]
- Chai, X.; Friebel, T.M.; Singer, C.F.; Evans, D.G.; Lynch, H.T.; Isaacs, C.; Garber, J.E.; Neuhausen, S.L.; Matloff, E.; Eeles, R.; et al. Use of risk-reducing surgeries in a prospective cohort of 1,499 BRCA1 and BRCA2 mutation carriers. Breast Cancer Res. Treat. 2014, 148, 397–406. [Google Scholar] [CrossRef]
- Cragun, D.; Weidner, A.; Lewis, C.; Bonner, D.; Kim, J.; Vadaparampil, S.T.; Pal, T. Racial disparities in BRCA testing and cancer risk management across a population-based sample of young breast cancer survivors. Cancer 2017, 123, 2497–2505. [Google Scholar] [CrossRef]
- D’Alonzo, M.; Pecchio, S.; Liberale, V.; Modaffari, P.; Biglia, N.; Piva, E.; Ponzone, R. Satisfaction and Impact on Quality of Life of Clinical and Instrumental Surveillance and Prophylactic Surgery in BRCA-mutation Carriers. Clin. Breast Cancer 2018, 18, e1361–e1366. [Google Scholar] [CrossRef]
- Evans, D.G.R.; Lalloo, F.; Shenton, A.; Clancy, T.; Hopwood, P.; Ashcroft, L.; Howell, A.; Baildam, A.D.; Brain, A. Uptake of risk-reducing surgery in unaffected women at high risk of breast and ovarian cancer is risk, age, and time dependent. Cancer Epidemiol. Biomark. Prev. 2009, 18, 2318–2324. [Google Scholar] [CrossRef] [PubMed]
- Finkelman, B.S.; Rubinstein, W.S.; Friedman, S.; Friebel, T.M.; Dubitsky, S.; Schonberger, N.S.; Shoretz, R.; Singer, C.F.; Blum, J.L.; Tung, N.; et al. Breast and ovarian cancer risk and risk reduction in Jewish BRCA1/2 mutation carriers. J. Clin. Oncol. 2012, 30, 1321–1328. [Google Scholar] [CrossRef] [PubMed]
- Flippo-Morton, T.; Walsh, K.; Sarantou, T.; White, R.L.; Chambers, K.; Amacker-North, L.; White, B.; Boselli, D.M. Surgical Decision Making in the BRCA-Positive Population: Institutional Experience and Comparison with Recent Literature. Breast J. 2016, 22, 35–44. [Google Scholar] [CrossRef] [PubMed]
- Friebel, T.M.; Domchek, S.M.; Neuhausen, S.L.; Wagner, T.; Evans, D.G.; Isaacs, C.; Garber, J.E.; Daly, M.B.; Eeles, R.; Matloff, E.; et al. Bilateral prophylactic oophorectomy and bilateral prophylactic mastectomy in a prospective cohort of unaffected BRCA1 and BRCA2 mutation carriers. Clin. Breast Cancer 2007, 7, 875–882. [Google Scholar] [CrossRef] [PubMed]
- Garcia, C.; Lyon, L.; Conell, C.; Littell, R.D.; Powell, C.B. Osteoporosis risk and management in BRCA1 and BRCA2 carriers who undergo risk-reducing salpingo-oophorectomy. Gynecol. Oncol. 2015, 138, 723–726. [Google Scholar] [CrossRef]
- Holman, L.L.; Friedman, S.; Daniels, M.S.; Sun, C.C.; Lu, K.H. Acceptability of prophylactic salpingectomy with delayed oophorectomy as risk-reducing surgery among BRCA mutation carriers. Gynecol. Oncol. 2014, 133, 283–286. [Google Scholar] [CrossRef]
- Kim, S.I.; Lim, M.C.; Lee, D.O.; Seo, S.S.; Kang, S.; Park, S.Y.; Kong, S.Y.; Lee, E.S. Uptake of risk-reducing salpingo-oophorectomy among female BRCA mutation carriers: Experience at the National Cancer Center of Korea. J. Cancer Res. Clin. Oncol. 2016, 142, 333–340. [Google Scholar] [CrossRef]
- Kram, V.; Peretz, T.; Sagi, M. Acceptance of Preventive Surgeries by Israeli Women Who had Undergone BRCA Testing. Fam. Cancer 2006, 5, 327–335. [Google Scholar] [CrossRef]
- Kwong, A.; Wong, C.H.; Shea, C.; Suen, D.T.; Choi, C.L. Choice of management of southern Chinese BRCA mutation carriers. World J. Surg. 2010, 34, 1416–1426. [Google Scholar] [CrossRef]
- Lerman, C.; Hughes, C.; Croyle, R.T.; Main, D.; Durham, C.; Snyder, C.; Bonney, A.; Lynch, J.F.; Narod, S.A.; Lynch, H.T. Prophylactic surgery decisions and surveillance practices one year following BRCA1/2 testing. Prev. Med. 2000, 31, 75–80. [Google Scholar] [CrossRef]
- Lodder, L.N.; Frets, P.G.; Trijsburg, R.W.; Meijers-Heijboer, E.J.; Klijn, J.G.M.; Seynaeve, C.; van Geel, A.N.; Tilanus, M.M.A.; Bartels, C.C.M.; Verhoog, L.C.; et al. One Year Follow-Up of Women Opting for Presymptomatic Testing for BRCA1 and BRCA2: Emotional Impact of the Test Outcome and Decisions on Risk Management (Surveillance or Prophylactic Surgery). Breast Cancer Res. Treat. 2002, 73, 97–112. [Google Scholar] [CrossRef]
- Madalinska, J.B.; Hollenstein, J.; Bleiker, E.; van Beurden, M.; Valdimarsdottir, H.B.; Massuger, L.F.; Gaarenstroom, K.N.; Mourits, M.J.E.; Verheijen, R.H.M.; van Dorst, E.B.L.; et al. Quality-of-Life Effects of Prophylactic Salpingo-Oophorectomy Versus Gynecologic Screening Among Women at Increased Risk of Hereditary Ovarian Cancer. J. Clin. Oncol. 2005, 23, 6890–6898. [Google Scholar] [CrossRef]
- Mai, P.L.; Piedmonte, M.; Han, P.K.; Moser, R.P.; Walker, J.L.; Rodriguez, G.; Boggess, J.; Rutherford, T.J.; Zivanovic, O.; Cohn, D.E.; et al. Factors associated with deciding between risk-reducing salpingo-oophorectomy and ovarian cancer screening among high-risk women enrolled in GOG-0199: An NRG Oncology/Gynecologic Oncology Group study. Gynecol. Oncol. 2017, 145, 122–129. [Google Scholar] [CrossRef]
- Manchanda, R.; Burnell, M.; Abdelraheim, A.; Johnson, M.; Sharma, A.; Benjamin, E.; Brunell, C.; Saridogan, E.; Gessler, S.; Oram, D.; et al. Factors influencing uptake and timing of risk reducing salpingo-oophorectomy in women at risk of familial ovarian cancer: A competing risk time to event analysis. Int. J. Obstet. Gynaecol. 2012, 119, 527–536. [Google Scholar] [CrossRef]
- Meijers-Heijboer, E.J.; Verhoog, L.C.; Brekelmans, C.T.; Seynaeve, C.; Tilanus-Linthorst, M.M.; Wagner, A.; Dukel, L.; Devilee, P.; van den Ouweland, A.M.; van Geel, A.N.; et al. Presymptomatic DNA testing and prophylactic surgery in families with a BRCA1 or BRCA2 mutation. Lancet 2000, 355, 2015–2020. [Google Scholar] [CrossRef]
- Metcalfe, K.A.; Ghadirian, P.; Rosen, B.; Foulkes, W.; Kim-Sing, C.; Eisen, A.; Ainsworth, P.; Horsman, D.; Maugard, C.; Provencher, D.; et al. Variation in rates of uptake of preventive options by Canadian women carrying the BRCA1 or BRCA2 genetic mutation. Open Med. A Peer-Rev. Indep. Open-Access J. 2007, 1, e92–e98. [Google Scholar]
- Metcalfe, K.A.; Liede, A.; Hoodfar, E.; Scott, A.; Foulkes, W.D.; Narod, S.A. An evaluation of needs of female BRCA1 and BRCA2 carriers undergoing genetic counselling. J. Med. Genet. 2000, 37, 866–874. [Google Scholar] [CrossRef]
- Nebgen, D.R.; Hurteau, J.; Holman, L.L.; Bradford, A.; Munsell, M.F.; Soletsky, B.R.; Sun, C.C.; Chisholm, G.B.; Lu, K.H. Bilateral salpingectomy with delayed oophorectomy for ovarian cancer risk reduction: A pilot study in women with BRCA1/2 mutations. Gynecol. Oncol. 2018, 150, 79–84. [Google Scholar] [CrossRef]
- Pezaro, C.; James, P.; McKinley, J.; Shanahan, M.; Young, M.A.; Mitchell, G. The consequences of risk reducing salpingo-oophorectomy: The case for a coordinated approach to long-term follow up post surgical menopause. Fam. Cancer 2012, 11, 403–410. [Google Scholar] [CrossRef]
- Ray, J.A.; Loescher, L.J.; Brewer, M. Risk-reduction surgery decisions in high-risk women seen for genetic counseling. J. Genet. Couns. 2005, 14, 473–484. [Google Scholar] [CrossRef]
- Schwartz, M.D.; Isaacs, C.; Graves, K.D.; Poggi, E.; Peshkin, B.N.; Gell, C.; Finch, C.; Kelly, S.; Taylor, K.L.; Perley, L. Long-term outcomes of BRCA1/BRCA2 testing: Risk reduction and surveillance. Cancer 2012, 118, 510–517. [Google Scholar] [CrossRef]
- Skytte, A.B.; Gerdes, A.M.; Andersen, M.K.; Sunde, L.; Brondum-Nielsen, K.; Waldstrom, M.; Kolvraa, S.; Cruger, D. Risk-reducing mastectomy and salpingo-oophorectomy in unaffected BRCA mutation carriers: Uptake and timing. Clin. Genet. 2010, 77, 342–349. [Google Scholar] [CrossRef] [PubMed]
- Tiller, K.; Meiser, B.; Butow, P.; Clifton, M.; Thewes, B.; Friedlander, M.; Tucker, K. Psychological Impact of Prophylactic Oophorectomy in Women at Increased Risk of Developing Ovarian Cancer: A Prospective Study. Gynecol. Oncol. 2002, 86, 212–219. [Google Scholar] [CrossRef] [PubMed]
- Uyei, A.; Peterson, S.K.; Erlichman, J.; Broglio, K.; Yekell, S.; Schmeler, K.; Lu, K.; Meric-Bernstam, F.; Amos, C.; Strong, L.; et al. Association between clinical characteristics and risk-reduction interventions in women who underwent BRCA1 and BRCA2 testing: A single-institution study. Cancer 2006, 107, 2745–2751. [Google Scholar] [CrossRef] [PubMed]
- Westin, S.N.; Sun, C.C.; Lu, K.H.; Schmeler, K.M.; Soliman, P.T.; Lacour, R.A.; Johnson, K.G.; Daniels, M.S.; Bodurka, D.C.; Arun, B.K.; et al. Satisfaction with ovarian carcinoma risk-reduction strategies among women at high risk for breast and ovarian carcinoma. Cancer 2011, 117, 2659–2667. [Google Scholar] [CrossRef]
- Parker, W.H.; Feskanich, D.; Broder, M.S.; Chang, E.; Shoupe, D.; Farquhar, C.M.; Berek, J.S.; Manson, J.E. Long-term mortality associated with oophorectomy compared with ovarian conservation in the nurses’ health study. Obs. Gynecol. 2013, 121, 709–716. [Google Scholar] [CrossRef]
- Fakkert, I.E.; Abma, E.M.; Westrik, I.G.; Lefrandt, J.D.; Wolffenbuttel, B.H.; Oosterwijk, J.C.; Slart, R.H.; van der Veer, E.; de Bock, G.H.; Mourits, M.J. Bone mineral density and fractures after risk-reducing salpingo-oophorectomy in women at increased risk for breast and ovarian cancer. Eur. J. Cancer 2015, 51, 400–408. [Google Scholar] [CrossRef]
- Fakkert, I.E.; van der Veer, E.; Abma, E.M.; Lefrandt, J.D.; Wolffenbuttel, B.H.; Oosterwijk, J.C.; Slart, R.H.; Westrik, I.G.; de Bock, G.H.; Mourits, M.J. Elevated Bone Turnover Markers after Risk-Reducing Salpingo-Oophorectomy in Women at Increased Risk for Breast and Ovarian Cancer. PLoS ONE 2017, 12, e0169673. [Google Scholar] [CrossRef]
- Shuster, L.T.; Gostout, B.S.; Grossardt, B.R.; Rocca, W.A. Prophylactic oophorectomy in premenopausal women and long-term health. Menopause Int. 2008, 14, 111–116. [Google Scholar] [CrossRef]
- Rocca, W.A.; Bower, J.H.; Maraganore, D.M.; Ahlskog, J.E.; Grossardt, B.R.; de Andrade, M.; Melton, L.J. 3rd. Increased risk of cognitive impairment or dementia in women who underwent oophorectomy before menopause. Neurology 2007, 69, 1074–1083. [Google Scholar] [CrossRef]
- Rocca, W.A.; Bower, J.H.; Maraganore, D.M.; Ahlskog, J.E.; Grossardt, B.R.; de Andrade, M.; Melton, L.J. 3rd. Increased risk of parkinsonism in women who underwent oophorectomy before menopause. Neurology 2008, 70, 200–209. [Google Scholar] [CrossRef] [PubMed]
- Rocca, W.A.; Grossardt, B.R.; de Andrade, M.; Malkasian, G.D.; Melton, L.J. 3rd. Survival patterns after oophorectomy in premenopausal women: A population-based cohort study. Lancet Oncol. 2006, 7, 821–828. [Google Scholar] [CrossRef]
- Atsma, F.; Bartelink, M.L.; Grobbee, D.E.; van der Schouw, Y.T. Postmenopausal status and early menopause as independent risk factors for cardiovascular disease: A meta-analysis. Menopause 2006, 13, 265–279. [Google Scholar] [CrossRef]
- Rivera, C.M.; Grossardt, B.R.; Rhodes, D.J.; Brown, R.D., Jr.; Roger, V.L.; Melton, L.J., 3rd; Rocca, W.A. Increased cardiovascular mortality after early bilateral oophorectomy. Menopause 2009, 16, 15–23. [Google Scholar] [CrossRef]
- Gaba, F.; Manchanda, R. Systematic review of acceptability, cardiovascular, neurological, bone health and HRT outcomes following risk reducing surgery in BRCA carriers. Best Pract. Res. Clin. Obs. Gynaecol. 2020, 65, 46–65. [Google Scholar] [CrossRef]
- Manchanda, R.; Gaba, F.; Talaulikar, V.; Pundir, J.; Gessler, S.; Davies, M.; Menon, U.; Royal College of Obstetricians and Gynaecologists. Risk-Reducing Salpingo-Oophorectomy and the Use of Hormone Replacement Therapy Below the Age of Natural Menopause: Scientific Impact Paper No. 66 October 2021: Scientific Impact Paper No. 66. Int. J. Obstet. Gynaecol. 2022, 129, e16–e34. [Google Scholar] [CrossRef]
- Domchek, S.M.; Friebel, T.M.; Neuhausen, S.L.; Wagner, T.; Evans, G.; Isaacs, C.; Garber, J.E.; Daly, M.B.; Eeles, R.; Matloff, E.; et al. Mortality after bilateral salpingo-oophorectomy in BRCA1 and BRCA2 mutation carriers: A prospective cohort study. Lancet Oncol. 2006, 7, 223–229. [Google Scholar] [CrossRef]
- Domchek, S.M.; Friebel, T.M.; Singer, C.F.; Evans, D.G.; Lynch, H.T.; Isaacs, C.; Garber, J.E.; Neuhausen, S.L.; Matloff, E.; Eeles, R.; et al. Association of risk-reducing surgery in BRCA1 or BRCA2 mutation carriers with cancer risk and mortality. J. Am. Med. Assoc. 2010, 304, 967–975. [Google Scholar] [CrossRef]
- Metcalfe, K.; Lynch, H.T.; Foulkes, W.D.; Tung, N.; Kim-Sing, C.; Olopade, O.I.; Eisen, A.; Rosen, B.; Snyder, C.; Gershman, S.; et al. Effect of Oophorectomy on Survival After Breast Cancer in BRCA1 and BRCA2 Mutation Carriers. JAMA Oncol. 2015, 1, 306–313. [Google Scholar] [CrossRef]
- Eisen, A.; Lubinski, J.; Klijn, J.; Moller, P.; Lynch, H.T.; Offit, K.; Weber, B.; Rebbeck, T.; Neuhausen, S.L.; Ghadirian, P.; et al. Breast cancer risk following bilateral oophorectomy in BRCA1 and BRCA2 mutation carriers: An international case-control study. J. Clin. Oncol. 2005, 23, 7491–7496. [Google Scholar] [CrossRef]
- Kotsopoulos, J.; Lubinski, J.; Lynch, H.T.; Kim-Sing, C.; Neuhausen, S.; Demsky, R.; Foulkes, W.D.; Ghadirian, P.; Tung, N.; Ainsworth, P.; et al. Oophorectomy after menopause and the risk of breast cancer in BRCA1 and BRCA2 mutation carriers. Cancer Epidemiol. Biomark. Prev. 2012, 21, 1089–1096. [Google Scholar] [CrossRef] [PubMed]
- Mavaddat, N.; Peock, S.; Frost, D.; Ellis, S.; Platte, R.; Fineberg, E.; Evans, D.G.; Izatt, L.; Eeles, R.A.; Adlard, J.; et al. Cancer Risks for BRCA1 and BRCA2 Mutation Carriers: Results From Prospective Analysis of EMBRACE. J. Natl. Cancer Inst. 2013, 105, 812–822. [Google Scholar] [CrossRef] [PubMed]
- Metcalfe, K.; Gershman, S.; Lynch, H.T.; Ghadirian, P.; Tung, N.; Kim-Sing, C.; Olopade, O.I.; Domchek, S.; McLennan, J.; Eisen, A.; et al. Predictors of contralateral breast cancer in BRCA1 and BRCA2 mutation carriers. Br. J. Cancer 2011, 104, 1384–1392. [Google Scholar] [CrossRef]
- Metcalfe, K.; Lynch, H.T.; Ghadirian, P.; Tung, N.; Olivotto, I.; Warner, E.; Olopade, O.I.; Eisen, A.; Weber, B.; McLennan, J.; et al. Contralateral breast cancer in BRCA1 and BRCA2 mutation carriers. J. Clin. Oncol. 2004, 22, 2328–2335. [Google Scholar] [CrossRef]
- Rebbeck, T.R.; Eisen, A.; Weber, B.L.; Levin, A.M.; Snyder, C.; Watson, P.; Lynch, H.T.; Cannon-Albright, L.; Neuhausen, S.L.; Isaacs, C.; et al. Breast cancer risk after bilateral prophylactic oophorectomy in BRCA1 mutation carriers. J. Natl. Cancer Inst. 1999, 91, 1475–1479. [Google Scholar] [CrossRef]
- Basu, N.N.; Ingham, S.; Howell, A.; Evans, D.G.; Hodson, J.; Lalloo, F.; Bulman, M. Risk of contralateral breast cancer in BRCA1 and BRCA2 mutation carriers: A 30-year semi-prospective analysis. Fam. Cancer 2015, 14, 531–538. [Google Scholar] [CrossRef]
- Heemskerk-Gerritsen, B.A.M.; Seynaeve, C.; van Asperen, C.J.; Ausems, M.G.E.M.; Collée, J.M.; van Doorn, H.C.; Gomez Garcia, E.B.; Kets, C.M.; van Leeuwen, F.E.; Meijers-Heijboer, H.E.J.; et al. Breast Cancer Risk After Salpingo-Oophorectomy in Healthy BRCA1/2 Mutation Carriers: Revisiting the Evidence for Risk Reduction. J. Natl. Cancer Inst. 2015, 107, djv217. [Google Scholar] [CrossRef]
- Kotsopoulos, J.; Huzarski, T.; Gronwald, J.; Singer, C.F.; Moller, P.; Lynch, H.T.; Armel, S.; Karlan, B.; Foulkes, W.D.; Neuhausen, S.L.; et al. Bilateral Oophorectomy and Breast Cancer Risk in BRCA1 and BRCA2 Mutation Carriers. J. Natl. Cancer Inst. 2017, 109, djw177. [Google Scholar] [CrossRef]
- Kotsopoulos, J.; Lubinski, J.; Lynch, H.T.; Tung, N.; Armel, S.; Senter, L.; Singer, C.F.; Fruscio, R.; Couch, F.; Weitzel, J.N.; et al. Oophorectomy and risk of contralateral breast cancer among BRCA1 and BRCA2 mutation carriers. Breast Cancer Res. Treat. 2019, 175, 443–449. [Google Scholar] [CrossRef]
- Klaren, H.M.; van’t Veer, L.J.; van Leeuwen, F.E.; Rookus, M.A. Potential for bias in studies on efficacy of prophylactic surgery for BRCA1 and BRCA2 mutation. J. Natl. Cancer Inst. 2003, 95, 941–947. [Google Scholar] [CrossRef]
- Wacholder, S. Bias in Intervention Studies That Enroll Patients From High-Risk Clinics. J. Natl. Cancer Inst. 2004, 96, 1204–1207. [Google Scholar] [CrossRef] [PubMed]
- Warrens, M.J. Properties of the quantity disagreement and the allocation disagreement. Int. J. Remote Sens. 2015, 36, 1439–1446. [Google Scholar] [CrossRef]
- Wells, G.A.; Shea, B.; O’Connell, D.; Peterson, J.; Welch, V.; Losos, M.; Tugwell, P. The Newcastle-Ottawa Scale (NOS) for Assessing the Quality of Non-randomised Studies in Meta-Analyses. Available online: https://www.ohri.ca/programs/clinical_epidemiology/oxford.asp (accessed on 9 January 2022).
- Viale, L.; Allotey, J.; Cheong-See, F.; Arroyo-Manzano, D.; McCorry, D.; Bagary, M.; Mignini, L.; Khan, K.S.; Zamora, J.; Thangaratinam, S. Epilepsy in pregnancy and reproductive outcomes: A systematic review and meta-analysis. Lancet 2015, 386, 1845–1852. [Google Scholar] [CrossRef]
- Michael, B.; Larry, V.H.; Julian, H.; Hannah, R.W. Introduction to Meta-Analysis; John Wiley and Sons Ltd.: Chichester, UK, 2009. [Google Scholar]
- Guyatt, G.H.; Oxman, A.D.; Kunz, R.; Woodcock, J.; Brozek, J.; Helfand, M.; Alonso-Coello, P.; Glasziou, P.; Jaeschke, R.; Akl, E.A.; et al. GRADE guidelines: 7. Rating the quality of evidence--inconsistency. J. Clin. Epidemiol. 2011, 64, 1294–1302. [Google Scholar] [CrossRef]
- Page, M.J.; McKenzie, J.E.; Bossuyt, P.M.; Boutron, I.; Hoffmann, T.C.; Mulrow, C.D.; Shamseer, L.; Tetzlaff, J.M.; Akl, E.A.; Brennan, S.E.; et al. The PRISMA 2020 statement: An updated guideline for reporting systematic reviews. BMJ 2021, 372, n71. [Google Scholar] [CrossRef]
- Barlin, J.; Pike, M.; Otegbeye, E.; Arnold, A.; Stadler, Z.; Robson, M.; Aghajanian, C.; Offit, K.; Barakat, R.; Kauff, N. Does postmenopausal risk-reducing salpingo-oophorectomy reduce the risk of BRCA-associated breast cancer? Gynecol. Oncol. 2013, 130, e103–e104. [Google Scholar] [CrossRef]
- Chang-Claude, J.; Andrieu, N.; Rookus, M.; Brohet, R.; Antoniou, A.C.; Peock, S.; Davidson, R.; Izatt, L.; Cole, T.; Nogues, C.; et al. Age at menarche and menopause and breast cancer risk in the International BRCA1/2 Carrier Cohort Study. Cancer Epidemiol. Biomark. Prev. 2007, 16, 740–746. [Google Scholar] [CrossRef]
- Kauff, N.D.; Barakat, R.R. Risk-reducing salpingo-oophorectomy in patients with germline mutations in BRCA1 or BRCA2. J. Clin. Oncol. 2007, 25, 2921–2927. [Google Scholar] [CrossRef]
- Kauff, N.D.; Domchek, S.M.; Friebel, T.M.; Lee, J.B.; Roth, R.; Robson, M.E.; Barakat, R.R.; Norton, L.; Offit, K.; Rebbeck, T.R.; et al. Multi-center prospective analysis of risk-reducing salpingo-oophorectomy to prevent BRCA-associated breast and ovarian cancer. J. Clin. Oncol. 2006, 24, 1003. [Google Scholar] [CrossRef]
- Kramer, J.L.; Velazquez, I.A.; Chen, B.E.; Rosenberg, P.S.; Struewing, J.P.; Greene, M.H. Prophylactic oophorectomy reduces breast cancer penetrance during prospective, long-term follow-up of BRCA1 mutation carriers. J. Clin. Oncol. 2005, 23, 8629–8635. [Google Scholar] [CrossRef]
- Menkiszak, J.; Chudecka-Głaz, A.; Gronwald, J.; Cymbaluk-Płoska, A.; Celewicz, A.; Świniarska, M.; Wężowska, M.; Bedner, R.; Zielińska, D.; Tarnowska, P.; et al. Prophylactic salpingo-oophorectomy in BRCA1 mutation carriers and postoperative incidence of peritoneal and breast cancers. J. Ovarian Res. 2016, 9, 11. [Google Scholar] [CrossRef] [PubMed]
- Metcalfe, K.; Sun, P.; Narod, S.A.; Lynch, H.T.; Ghadirian, P.; Tung, N.; Kim-Sing, C.; Olopade, O.I.; Domchek, S.; Eisen, A.; et al. Risk of ipsilateral breast cancer in BRCA1 and BRCA2 mutation carriers. Breast Cancer Res. Treat. 2011, 127, 287–296. [Google Scholar] [CrossRef]
- Metcalfe, K.A.; Lynch, H.T.; Snyder, C.L.; Foulkes, W.; Tung, N.M.; Kim-Sing, C.; Olopade, O.I.; Eisen, A.; Rosen, B.; Sun, P.; et al. The impact of oophorectomy on survival after breast cancer in BRCA1 and BRCA2 mutation carriers. J. Clin. Oncol. 2014, 32, 1507. [Google Scholar] [CrossRef]
- Rebbeck, T.R. Prophylactic oophorectomy in BRCA1 and BRCA2 mutation carriers. J. Clin. Oncol. 2000, 18, 100s. [Google Scholar] [CrossRef]
- Rebbeck, T.R.; Kauff, N.D.; Domchek, S.M.; Rebbeck, T.R.; Kauff, N.D.; Domchek, S.M. Meta-analysis of risk reduction estimates associated with risk-reducing salpingo-oophorectomy in BRCA1 or BRCA2 mutation carriers. J. Natl. Cancer Inst. 2009, 101, 80–87. [Google Scholar] [CrossRef]
- Valachis, A.; Nearchou, A.D.; Lind, P. Surgical management of breast cancer in BRCA-mutation carriers: A systematic review and meta-analysis. Breast Cancer Res. Treat. 2014, 144, 443–455. [Google Scholar] [CrossRef]
- Huzarski, T.; Byrski, T.; Gronwald, J.; Górski, B.; Domagała, P.; Cybulski, C.; Oszurek, O.; Szwiec, M.; Gugała, K.; Stawicka, M.; et al. Ten-Year Survival in Patients With BRCA1-Negative and BRCA1-Positive Breast Cancer. J. Clin. Oncol. 2013, 31, 3191–3196. [Google Scholar] [CrossRef]
- Brekelmans, C.T.; Seynaeve, C.; Menke-Pluymers, M.; Bruggenwirth, H.T.; Tilanus-Linthorst, M.M.; Bartels, C.C.; Kriege, M.; van Geel, A.N.; Crepin, C.M.; Blom, J.C.; et al. Survival and prognostic factors in BRCA1-associated breast cancer. Ann. Oncol. 2006, 17, 391–400. [Google Scholar] [CrossRef]
- Evans, D.G.; Ingham, S.L.; Baildam, A.; Ross, G.L.; Lalloo, F.; Buchan, I.; Howell, A. Contralateral mastectomy improves survival in women with BRCA1/2-associated breast cancer. Breast Cancer Res. Treat. 2013, 140, 135–142. [Google Scholar] [CrossRef]
- Van Sprundel, T.C.; Schmidt, M.K.; Rookus, M.A.; Brohet, R.; van Asperen, C.J.; Rutgers, E.J.; Van’t Veer, L.J.; Tollenaar, R.A. Risk reduction of contralateral breast cancer and survival after contralateral prophylactic mastectomy in BRCA1 or BRCA2 mutation carriers. Br. J. Cancer 2005, 93, 287–292. [Google Scholar] [CrossRef]
- Choi, Y.H.; Terry, M.B.; Daly, M.B.; MacInnis, R.J.; Hopper, J.L.; Colonna, S.; Buys, S.S.; Andrulis, I.L.; John, E.M.; Kurian, A.W.; et al. Association of Risk-Reducing Salpingo-Oophorectomy With Breast Cancer Risk in Women With BRCA1 and BRCA2 Pathogenic Variants. JAMA Oncol. 2021, 7, 585–592. [Google Scholar] [CrossRef] [PubMed]
- Marcinkute, R.; Woodward, E.R.; Gandhi, A.; Howell, S.; Crosbie, E.J.; Wissely, J.; Harvey, J.; Highton, L.; Murphy, J.; Holland, C.; et al. Uptake and efficacy of bilateral risk reducing surgery in unaffected female BRCA1 and BRCA2 carriers. J. Med. Genet. 2022, 59, 133–140. [Google Scholar] [CrossRef] [PubMed]
- Terry, M.B.; Daly, M.B.; Phillips, K.A.; Ma, X.; Zeinomar, N.; Leoce, N.; Dite, G.S.; MacInnis, R.J.; Chung, W.K.; Knight, J.A.; et al. Risk-Reducing Oophorectomy and Breast Cancer Risk Across the Spectrum of Familial Risk. J. Natl. Cancer Inst. 2019, 111, 331–334. [Google Scholar] [CrossRef]
- Heemskerk-Gerritsen, B.A.M.; Hooning, M.J.; Rookus, M.A. Response. J. Natl. Cancer Inst. 2015, 107, 218. [Google Scholar] [CrossRef][Green Version]
- Mavaddat, N.; Antoniou, A.C.; Mooij, T.M.; Hooning, M.J.; Heemskerk-Gerritsen, B.A.; Noguès, C.; Laborde, L.; Breysse, E.; Stoppa-Lyonnet, D.; Gauthier-Villars, M.; et al. Risk-reducing salpingo-oophorectomy, natural menopause, and breast cancer risk: An international prospective cohort of BRCA1 and BRCA2 mutation carriers. Breast Cancer Res. 2020, 22, 8. [Google Scholar] [CrossRef]
- Bui, K.T.; Willson, M.L.; Goel, S.; Beith, J.; Goodwin, A. Ovarian suppression for adjuvant treatment of hormone receptor-positive early breast cancer. Cochrane Database Syst. Rev. 2020, 3, CD013538. [Google Scholar] [CrossRef]
- Eleje, G.U.; Eke, A.C.; Ezebialu, I.U.; Ikechebelu, J.I.; Ugwu, E.O.; Okonkwo, O.O. Risk-reducing bilateral salpingo-oophorectomy in women with BRCA1 or BRCA2 mutations. Cochrane Database Syst. Rev. 2018, 8, CD012464. [Google Scholar] [CrossRef]
- Xiao, Y.L.; Wang, K.; Liu, Q.; Li, J.; Zhang, X.; Li, H.Y. Risk Reduction and Survival Benefit of Risk-Reducing Salpingo-oophorectomy in Hereditary Breast Cancer: Meta-analysis and Systematic Review. Clin. Breast Cancer 2019, 19, e48–e65. [Google Scholar] [CrossRef]
- Gaba, F.; Goyal, S.; Marks, D.; Chandrasekaran, D.; Evans, O.; Robbani, S.; Tyson, C.; Legood, R.; Saridogan, E.; McCluggage, W.G.; et al. Surgical decision making in premenopausal BRCA carriers considering risk-reducing early salpingectomy or salpingo-oophorectomy: A qualitative study. J. Med. Genet. 2021, 59, 122–132. [Google Scholar] [CrossRef]
- Gaba, F.; Robbani, S.; Singh, N.; McCluggage, W.G.; Wilkinson, N.; Ganesan, R.; Bryson, G.; Rowlands, G.; Tyson, C.; Arora, R.; et al. Preventing Ovarian Cancer through early Excision of Tubes and late Ovarian Removal (PROTECTOR): Protocol for a prospective non-randomised multi-center trial. Int. J. Gynecol. Cancer 2020, 31, 286–291. [Google Scholar] [CrossRef]
- Nitschke, A.S.; do Valle, H.A.; Dawson, L.; Kwon, J.S.; Hanley, G.E. Long-Term Non-Cancer Risks in People with BRCA Mutations following Risk-Reducing Bilateral Salpingo-Oophorectomy and the Role of Hormone Replacement Therapy: A Review. Cancers 2023, 15, 711. [Google Scholar] [CrossRef] [PubMed]
- Heemskerk-Gerritsen, B.A.M.; Jager, A.; Koppert, L.B.; Obdeijn, A.I.; Collee, M.; Meijers-Heijboer, H.E.J.; Jenner, D.J.; Oldenburg, H.S.A.; van Engelen, K.; de Vries, J.; et al. Survival after bilateral risk-reducing mastectomy in healthy BRCA1 and BRCA2 mutation carriers. Breast Cancer Res. Treat. 2019, 177, 723–733. [Google Scholar] [CrossRef]
- Nelson, H.D.; Fu, R.; Zakher, B.; Pappas, M.; McDonagh, M. Medication Use for the Risk Reduction of Primary Breast Cancer in Women: Updated Evidence Report and Systematic Review for the US Preventive Services Task Force. JAMA 2019, 322, 868–886. [Google Scholar] [CrossRef]
- Robertson, J.F.R.; Blamey, R.W. The use of gonadotrophin-releasing hormone (GnRH) agonists in early and advanced breast cancer in pre- and perimenopausal women. Eur. J. Cancer 2003, 39, 861–869. [Google Scholar] [CrossRef]




{kind=link}
{kind=link}
{kind=link}
| Studies | Country | Study Design | Population | Intervention | RRM | Outcomes | Reported Outcome Measures (CI 95%) | Follow-Up | Potential Selection Bias |
|---|---|---|---|---|---|---|---|---|---|
| Chang-Claude 2007 [79] | Europe and Canada | Multicentre prospective cohort, retrospective analysis (EMBRACE/HEBON/ GENEPSO/IBCCS datasets) | BC-affected and -unaffected BRCA1/BRCA2 carriers (n = 1601) | RRSO | Censored | PBC risk | * HR 0.57 (0.29–1.09) | Not reported | Immortal person-time Familial event |
| Choi 2021 [93] | US, Australia, Canada | Multicentre prospective cohort (BCFR dataset) | Unaffected BRCA1/BRCA2 carriers (n = 4575) | RRSO | Censored | PBC risk | BRCA1: HR 0.28 (0.10–0.63); BRCA2 HR 0.19 (0.06–0.71) | Not reported | Familial event |
| Eisen 2005 [60] | Europe, USA, Israel | Multicentre matched case-control | BC-affected (cases: 2283) and -unaffected (controls: 2286) BRCA1/BRCA2 carriers (n = 4569; 1439 matched sets) | RRSO | Excluded | PBC risk | ** OR 0.46 (0.32–0.65) * OR 0.46 (0.32–0.65) | Not reported | Cancer-induced testing |
| Finkelman 2012 [22] | Europe and USA | Multicentre prospective cohort (PROSE consortium) | Unaffected BRCA1/BRCA2 carriers (n = 4649) | RRSO | Censored | PBC risk | HR 0.62 (0.47–0.83) | Mean 6.5 years for RRSO group from ascertainment; 4.5 years for non-RRSO group from ascertainment | Immortal person-time Indication |
| Heemskerk-Gerritsen 2015 [96] | Netherlands | Multicentre cohort (both retrospective and prospective—HEBON dataset) | Unaffected BRCA1/BRCA2 carriers (n = 822) | RRSO | Censored | PBC risk | * HR 1.09 (0.67–1.77) | Mean 6.8 years (range 0.5–17.4) for RRSO group; 3.1 years (0.1–15.9) for non-RRSO group from ascertainment | - |
| Kauff 2008 [11] | Europe and USA | Multicentre prospective cohort (PROSE consortium) | Unaffected BRCA1/BRCA2 carriers (n = 597) | RRSO | Censored | PBC risk | HR 0.53 (0.29–0.96) | Mean 3.03 years for RRSO group from date of surgery; 2.77 years for non-RRSO group from ascertainment | Immortal person-time |
| Kotsopoulos 2012 [61] | 12 countries | Multicentre matched case-control | BC-affected (cases-3914) and -unaffected (controls-5063) BRCA1/BRCA2 carriers (n = 8977; 2854 matched sets) | RRSO | Excluded | PBC risk | ** OR 0.52 (0.40–0.66) | Not reported | Familial event Immortal person-time Cancer-induced testing |
| Kotsopoulos 2017 [68] | 12 countries | Multicentre prospective cohort | Unaffected BRCA1/BRCA2 carriers from ascertainment (n = 3722) | RRSO | Excluded | PBC risk | * HR 0.89 (0.69–1.14) | Mean 5.6 years (range 0–21.2) | Indication Immortal person-time |
| Kramer 2005 [82] | USA | Prospective cohort | Unaffected BRCA1 carriers (n = 98) | RRSO | Censored | PBC risk | ** HR 0.38 (0.15–0.97) | Mean 14.1 years from surgery | Indication |
| Marcinkute 2021 [94] | UK | Prospective cohort | Unaffected BRCA1/BRCA2 carriers (n = 887) | RRSO | Censored | PBC risk | HR = 0.77 (0.45–1.34) | Mean 6.26 years from ascertainment | Indication |
| Mavaddat 2020 [97] | Europe, US, Australia, New Zealand | Multicentre prospective cohort (EMBRACE/HEBON/ GENEPSO/ IBCCS/ kConFab/BCFR/MUV/ INHERIT/OUH/GC-HBOC/NIO/CNIO/HCSC/LUND-BRCA/ STOCKHOLM-BRCA/IHCC/ MODSQUAD datasets) | Unaffected BRCA1/BRCA2 carriers (n = 3877) | RRSO | Censored | PBC risk | BRCA1: HR 1.23 (0.94–1.61) BRCA2: HR 0.88 (0.62–1.24) | BRCA1: mean 5.60 (SD 3.67) person-years BRCA2: mean 5.03 (SD 3.44) person-years | - |
| Mavaddat 2013 [62] | UK, Ireland | Multicentre prospective cohort (EMBRACE) | Unaffected BRCA1/BRCA2 carriers (n = 988) | RRSO | Censored | PBC risk; CBC risk | * HR 0.62 (0.35–1.09) * HR 0.59 (0.35–0.99) | Mean 3 years | Indication |
| Rebbeck 1999 [65] | USA | Multicentre retrospective matched case-control | Unaffected BRCA1 carriers (n = 122; cases 43; controls 79) | RRSO | Excluded | PBC risk | ** HR 0.53 (0.33–0.84) | Cases: mean 9.6 years (range <1–36) from surgery; controls: mean 8.1 years (range <1–43) after the time of the matched case’s surgery | Indication |
| Rebbeck 2002 [10] | Europe, USA | Multicentre retrospective matched case-control | Unaffected BRCA1/BRCA2 carriers (n = 241; 99 cases; 142 controls) | RRSO | Excluded | PBC risk | ** HR 0.47 (0.29–0.77) | Cases: mean 10.7 years (range 0.17–42.8) after surgery; controls: 11.9 years (0.34–42.5) after time of matched case’s surgery | Indication |
| Terry, 2018 [95] | US, Australia, Canada | Multicentre prospective cohort (BCFR, kConFab datasets) | Unaffected BRCA1/BRCA2 carriers (n = 1289) | RRSO | Censored | PBC risk | * HR 1.04, (0.87–1.24) | Mean 10.7 years from ascertainment | Familial event |
| Basu 2015 [66] | UK | Cross sectional (both prospective and retrospective) | BC-affected BRCA1/BRCA2 carriers (n = 782 univariable analysis; n = 450 multivariable analysis) | RRSO | Excluded | CBC risk | * HR 0.72 (0.36–1.41) ** HR 0.83 (0.46–1.50) | Median 7.8 years (range 0–37 years) from first BC | Indication |
| Kotsopoulos 2019 [69] | Canada, USA, Europe | Multicentre prospective cohort | BC-affected BRCA1/BRCA2 carriers (n = 2303) | RRSO | Excluded | CBC risk | * HR 0.92 (0.68–1.25) | Mean 9.8 years | Indication |
| Metcalfe 2004 [64] | Canada, USA | Multicentre retrospective cohort | BC-affected BRCA1/BRCA2 carriers or mutation status unknown but from a family with known BRCA1/BRCA2 mutation (n = 336) | RRSO | Excluded | CBC risk | * HR 0.41 (0.18–0.90) | Mean 9.2 years from first BC | Indication Familial event |
| Metcalfe 2011 [84] | Canada, USA | Multicentre retrospective cohort | BC-affected BRCA1/BRCA2 carriers or mutation status unknown but from a family with known BRCA1/BRCA2 mutation (n = 810) | RRSO | Excluded | CBC risk | * RR 0.48 (0.27–0.82) ** RR 0.49 (0.32–0.77) | Mean 11.1 years (range 0.1–32.9) from first BC | - |
| Kauff 2008 [11] | Europe, USA | Multicentre prospective cohort (PROSE consortium) | BC-affected and -unaffected BRCA1/BRCA2 carriers (n = 597) | RRSO | Censored | ~BC risk | ** HR 0.32 (0.08–1.20) | Mean 2.9 years | Immortal person-time |
| Kauff 2002 [9] | USA | Single-centre prospective cohort | BC-affected and -unaffected BRCA1/BRCA2 carriers (n = 170) | RRSO | Censored | ~BC risk | ** HR 0.32 (0.08–1.20) | 127 women-years in RRSO group from surgery, and 120 women-years in non-RRSO group from ascertainment | Immortal person-time |
| Menkiszak 2016 [83] | Poland | Single-centre cohort | BC-affected and -unaffected BRCA1 carriers (n = 195) | RRSO | Not reported | ~BC risk | 4.63% incidence of BC post RRSO | Mean 6.7 years | Indication Familial event Immortal person-time Cancer-induced testing |
| Brekelmans 2005 [90] | Netherlands | Single-centre retrospective case-control | BC-affected BRCA1 carriers (cases = 223); sporadic BC cases in women at population-level risk (controls=446) | RRSO | Not reported | BC-specific mortality | HR 0.38 (0.10–2.07) | Median 5.1 years | Cancer-induced testing Immortal person-time Familial event |
| Evans 2013 [91] | UK | Single-centre retrospective cohort | BC-affected BRCA1/BRCA2 carriers (n = 718) | RRSO | Excluded | BC-specific mortality | # HR 0.46 (0.27–0.78) | Not reported | - |
| Metcalfe 2015 [59] | Canada, USA | Multicentre retrospective cohort | BC-affected BRCA1/BRCA2 carriers or mutation status unknown but from a family with known BRCA1/BRCA2 mutation (n = 676) | RRSO | Included | BC-specific mortality | * HR 0.46 (0.27–0.79) ** HR 0.47 (0.29–0.76) | Mean 12.5 years (0.7–20.0) from first BC | Indication Cancer-induced testing |
| Domchek 2006 [57] | Europe, USA | Multicentre prospective cohort (PROSE consortium) | Unaffected BRCA1/BRCA2 carriers (n = 426 primary analysis) | RRSO | Excluded | BC-specific mortality | * HR 0.10 (0.02–0.71) | Mean 3.6 years (SD 3.7) for RRSO group and mean 1.6 years (SD 1.2) for no RRSO group from BC to death | Cancer-induced testing |
| Domchek 2010 [58] | Europe, USA | Multicentre prospective cohort (PROSE consortium) | BC-affected and -unaffected BRCA1/BRCA2 carriers (n = 2482) | RRSO | Censored | PBC risk; CBC risk; BC-specific mortality | PBC: * HR 0.54 (0.37–0.79); CBC * HR 1.00 (0.56–1.77); mortality: * HR 0.40 (0.26–0.61) | Median 3.65 years (range 0.52–27.4) for RRSO group from surgery; 4.29 years (range 0.5–27.9) for non-RRSO group from ascertainment | Cancer-induced testing Immortal person-time |
| Huzarski, 2013 [89] | Poland | Multicentre prospective cohort (Polish Hereditary Breast Cancer Consortium) | BC-affected BRCA1 Polish founder mutation carriers and non-carriers (n = 3345) | RRSO | Not reported | BC-specific mortality | * HR 0.30 (0.12–0.75) ** HR 0.31 (0.13–0.77) | Not reported | Indication |
| van Sprundel 2005 [92] | Netherlands | Multicentre retrospective cohort | BC-affected BRCA1/BRCA2 carriers (n = 148) | RRSO | Not reported | BC-specific mortality | * HR 0.28 (0.07–1.11) ** HR 0.15 (0.04–0.51) | Not reported | Familial event bias |
| Studies | Selection | Comparability | Outcome/Exposure |
|---|---|---|---|
| Primary Breast Cancer risk | |||
| Chang-Claude 2007 [79] | Medium (***) | Medium (*) | High (*) |
| Choi 2021 [93] | Low (****) | Low (**) | Medium (**) |
| Domchek 2010 [58] | Medium | Medium (*) | Medium (**) |
| Eisen 2005 [60] | High (*) | High (-) | High (*) |
| Finkelman 2012 [22] | Medium (***) | Medium (*) | Low (***) |
| Heemskerk-Gerritsen 2015 [96] | Low (****) | Low (**) | Low (***) |
| Kauff 2008 [11] | High (*) | High (-) | High (*) |
| Kotsopoulos 2012 [61] | High (*) | High (-) | High (*) |
| Kotsopoulos 2017 [68] | Medium (***) | Medium (*) | Medium (**) |
| Kramer 2005 [82] | Medium (***) | Medium (*) | Medium (**) |
| Marcinkute, 2021 [94] | Low (****) | Low (**) | Medium (**) |
| Mavaddat 2020 [97] | Low (****) | Low (**) | Low (***) |
| Mavaddat 2013 [62] | Low (****) | Medium (*) | Medium (**) |
| Rebbeck 1999 [65] | Medium (***) | High (-) | Medium (**) |
| Rebbeck 2002 [10] | Medium (***) | High (-) | Medium (**) |
| Terry 2018 [95] | Medium (***) | Medium (*) | Medium (**) |
| Contralateral Breast Cancer risk | |||
| Basu 2015 [66] | Low (****) | Medium (*) | Low (***) |
| Domchek 2010 [58] | Medium | Medium (*) | Medium (**) |
| Kotsopoulos 2019 [69] | Low (****) | Medium (*) | Low (***) |
| Mavaddat 2013 [62] | Low (****) | Medium (*) | Medium (**) |
| Metcalfe 2004 [64] | Medium (***) | High (-) | Medium (**) |
| Breast Cancer Risk+ | |||
| Kauff 2008 [11] | High (*) | Medium (*) | Medium (**) |
| Kauff 2002 [9] | High (*) | Medium (*) | Medium (**) |
| Menkiszak 2016 [83] | High (*) | High (-) | High (*) |
| Breast-Cancer-Specific Mortality | |||
| Brekelmans 2005 [90] | Medium | High (-) | High (*) |
| Evans 2013 [91] | Low (****) | Low (**) | Medium (**) |
| Metcalfe 2015 [59] | Low (****) | Medium (*) | Medium (**) |
| Domchek 2006 [57] | Medium | Medium (*) | Medium (**) |
| Domchek 2010 [58] | Medium | Medium (*) | Medium (**) |
| Huzarski, 2013 [89] | Medium | Medium (*) | Medium (**) |
| van Sprundel 2005 [92] | Medium | Medium (*) | Medium (**) |
| Outcome | Number of Studies | Certainty of Evidence (GRADE) |
|---|---|---|
| Primary breast cancer | 16 | Low * |
| Contralateral breast cancer | 6 | Low * |
| Breast-cancer-specific mortality | 7 | Moderate ** |
| Breast Cancer Risk/Mortality after Risk-Reducing Salpingo-Oophorectomy | Relative Risk (95%CI) | Min NNT (95%CI) | Mean NNT (95%CI) | Max NNT (95%CI) |
|---|---|---|---|---|
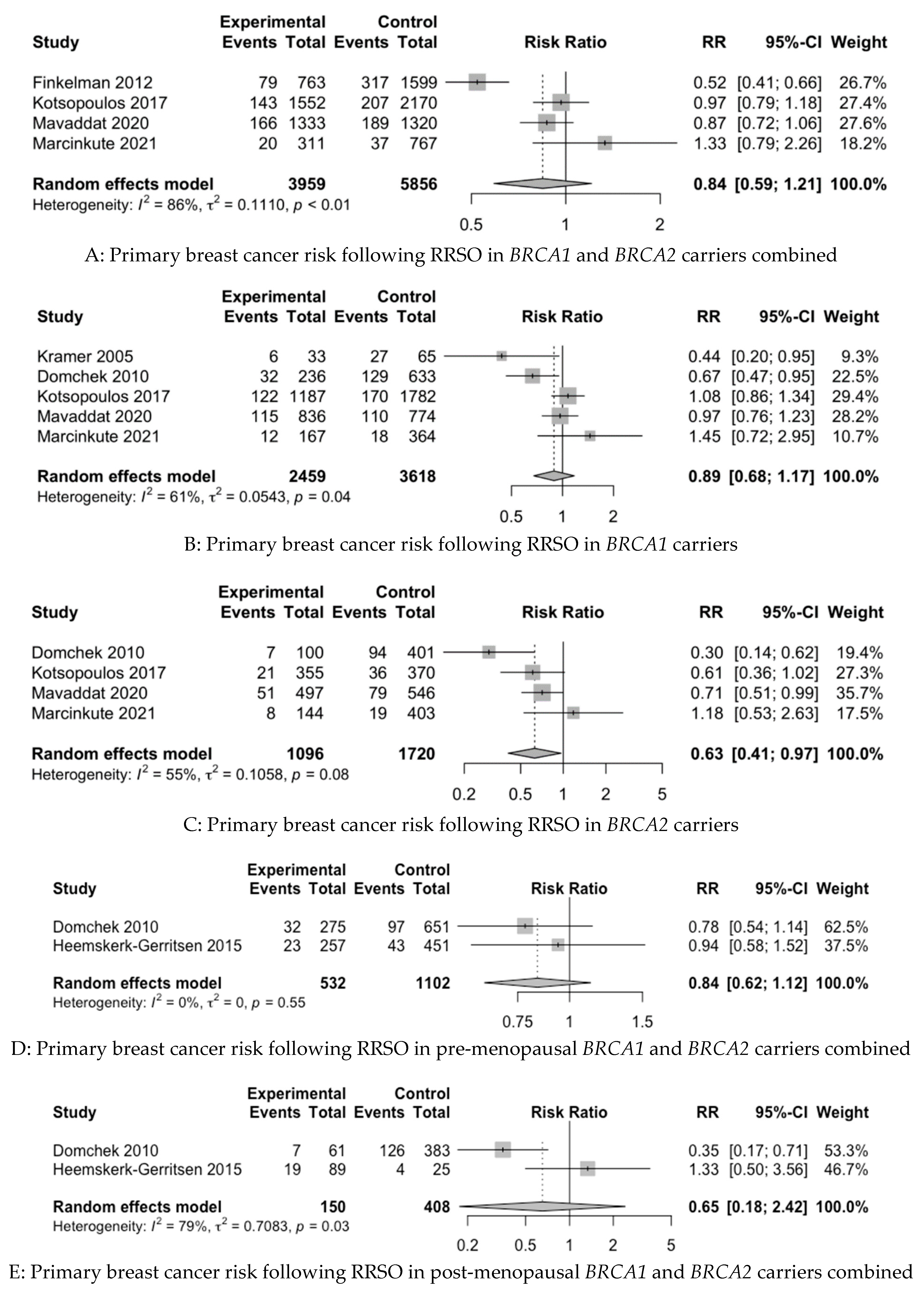
| PBC risk in BRCA1 and BRCA2 carriers combined | 0.84 (0.59–1.21) | - | - | - |
| PBC risk in BRCA1 carriers | 0.89 (0.68–1.17) | - | - | - |
| PBC risk in BRCA2 carriers | 0.63 (0.41–0.97) | 57.05 (35.88–607.28) | 20.55 (12.93–218.75) | 11.47 (7.22–122.1) |
| PBC risk in pre-menopausal BRCA1 and BRCA2 carriers combined | 0.84 (0.62–1.12) | - | - | - |
| PBC risk in post-menopausal BRCA1 and BRCA2 carriers combined | 0.65 (0.18–2.42) | - | - | - |
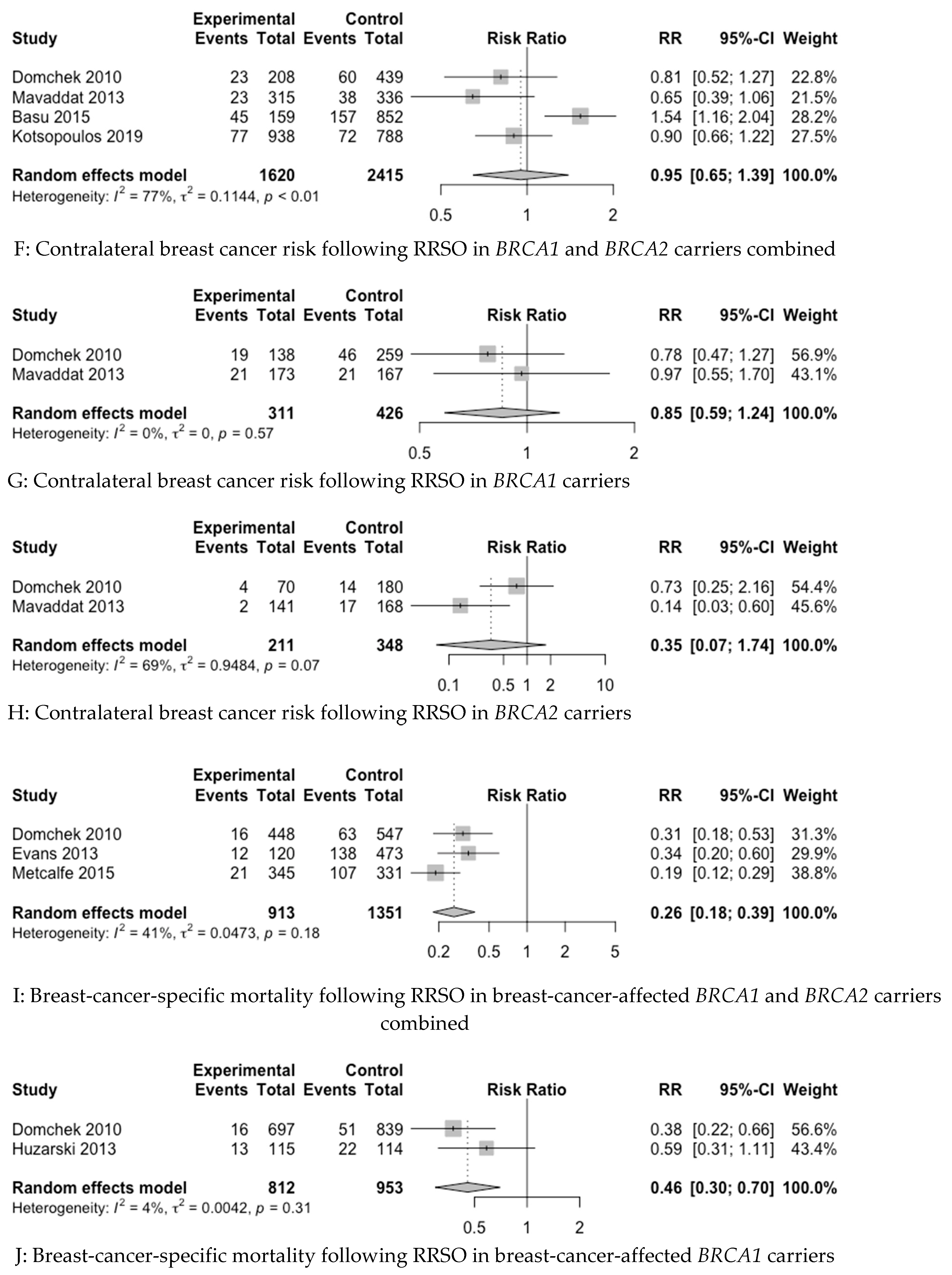
| CBC risk in BRCA1 and BRCA2 carriers combined | 0.95 (0.65–1.39) | - | - | - |
| CBC risk in BRCA1 carriers | 0.85 (0.59–1.24) | - | - | - |
| CBC risk in BRCA2 carriers | 0.35 (0.07–1.74) | - | - | - |
| Mortality in BC-affected BRCA1 and BRCA2 carriers combined | 0.26 (0.18–0.39) | 11.79 (10.58–14.18) | 5.58 (5–6.71) | 4.2 (3.77–5.05) |
| Mortality in BC affected BRCA1 carriers | 0.46 (0.30–0.70) | 30.29 (23.44–54.81) | 14.51 (11.23–26.26) | 9.54 (7.38–17.27) |
| PBC risk in BRCA1 and BRCA2 carriers combined | 0.84 (0.59–1.21) | - | - | - |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Gaba, F.; Blyuss, O.; Tan, A.; Munblit, D.; Oxley, S.; Khan, K.; Legood, R.; Manchanda, R. Breast Cancer Risk and Breast-Cancer-Specific Mortality following Risk-Reducing Salpingo-Oophorectomy in BRCA Carriers: A Systematic Review and Meta-Analysis. Cancers 2023, 15, 1625. https://doi.org/10.3390/cancers15051625
Gaba F, Blyuss O, Tan A, Munblit D, Oxley S, Khan K, Legood R, Manchanda R. Breast Cancer Risk and Breast-Cancer-Specific Mortality following Risk-Reducing Salpingo-Oophorectomy in BRCA Carriers: A Systematic Review and Meta-Analysis. Cancers. 2023; 15(5):1625. https://doi.org/10.3390/cancers15051625
Chicago/Turabian StyleGaba, Faiza, Oleg Blyuss, Alex Tan, Daniel Munblit, Samuel Oxley, Khalid Khan, Rosa Legood, and Ranjit Manchanda. 2023. "Breast Cancer Risk and Breast-Cancer-Specific Mortality following Risk-Reducing Salpingo-Oophorectomy in BRCA Carriers: A Systematic Review and Meta-Analysis" Cancers 15, no. 5: 1625. https://doi.org/10.3390/cancers15051625
APA StyleGaba, F., Blyuss, O., Tan, A., Munblit, D., Oxley, S., Khan, K., Legood, R., & Manchanda, R. (2023). Breast Cancer Risk and Breast-Cancer-Specific Mortality following Risk-Reducing Salpingo-Oophorectomy in BRCA Carriers: A Systematic Review and Meta-Analysis. Cancers, 15(5), 1625. https://doi.org/10.3390/cancers15051625