
Textbook Outcome of Laparoscopic Microwave Ablation for Hepatocellular Carcinoma

 , ,
, ,  , , , , , ,
, , , , , ,  and
and 
Abstract
Simple Summary
Abstract
1. Introduction
2. Materials and Methods
Statistical Analysis
3. Results
3.1. TO Achievement, Determinants, and Risk Groups
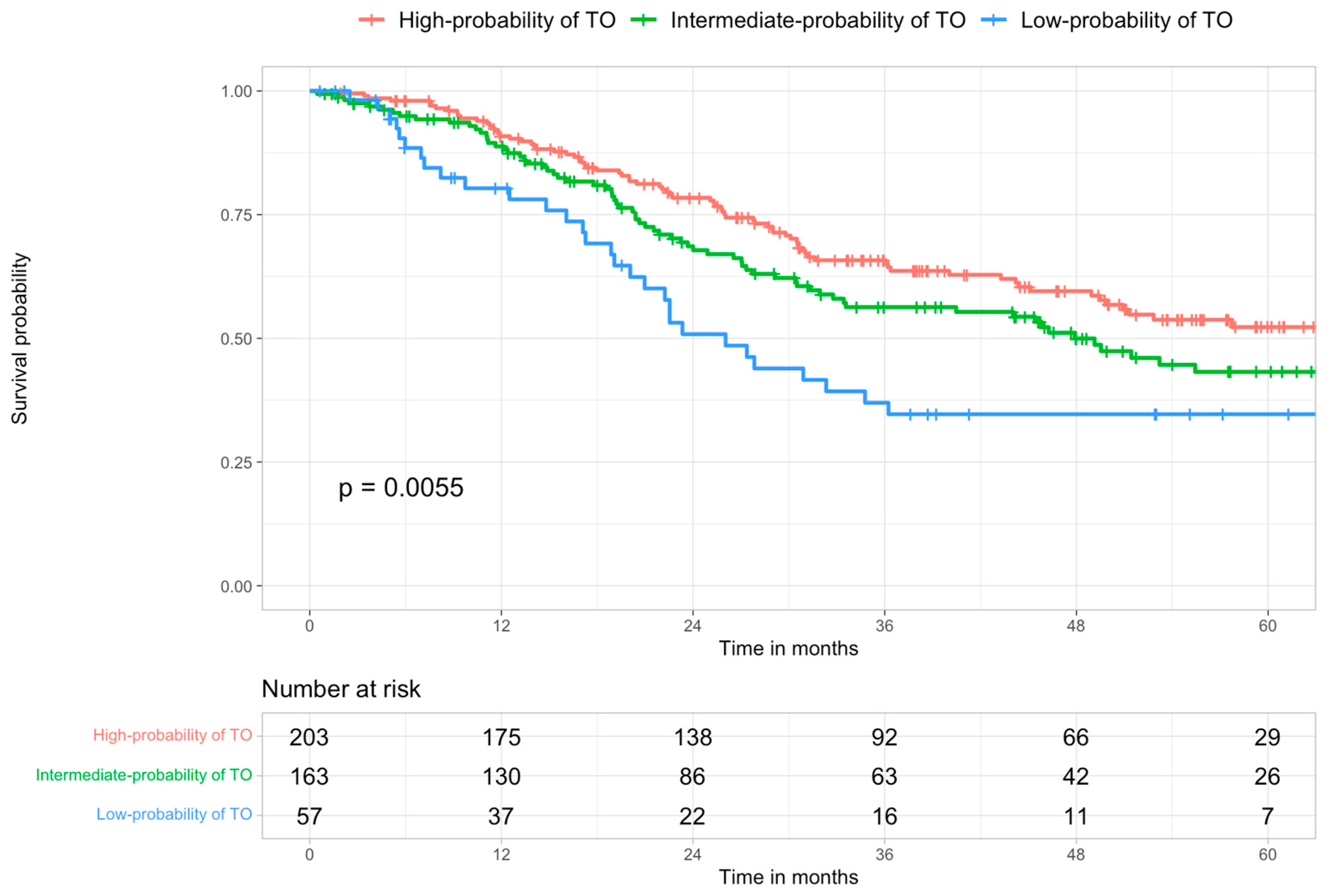
3.2. Survival Analysis
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- van Roessel, S.; Mackay, T.M.; van Dieren, S.; van der Schelling, G.P.; Nieuwenhuijs, V.B.; Bosscha, K.; van der Harst, E.; van Dam, R.M.; Liem, M.S.L.; Festen, S.; et al. Textbook Outcome: Nationwide Analysis of a Novel Quality Measure in Pancreatic Surgery. Ann. Surg. 2020, 271, 155–162. [Google Scholar] [CrossRef]
- van Der Heide, M.F.; de Jel, D.V.; Hoeijmakers, F.; Hoebers, F.J.; de Boer, J.P.; Hamming-Vrieze, O.; Wouters, M.W.; Smeele, L.E. Defining High-Quality Integrated Head and Neck Cancer Care Through a Composite Outcome Measure: Textbook Outcome. Laryngoscope 2022, 132, 78–87. [Google Scholar] [CrossRef] [PubMed]
- Wiseman, J.T.; Abdel-Misih, S.; Beal, E.W.; Zaidi, M.Y.; Staley, C.A.; Grotz, T.; Leiting, J.; Fournier, K.; Lee, A.J.; Dineen, S.; et al. A multi-institutional analysis of Textbook Outcomes among patients undergoing cytoreductive surgery for peritoneal surface malignancies. Surg. Oncol. 2021, 37, 101492. [Google Scholar] [CrossRef]
- Kulshrestha, S.; Vigneswaran, W.T.; Pawlik, T.M.; Baker, M.S.; Luchette, F.A.; Raad, W.; Abdelsattar, Z.M.; Freeman, R.K.; Grenda, T.; Lubawski, J. Assessment of Textbook Outcome After Surgery for Stage I/II Non-small Cell Lung Cancer. In Seminars in Thoracic and Cardiovascular Surgery; WB Saunders: Philadelphia, PA, USA, 2021; Volume 34, pp. 1351–1359. [Google Scholar] [CrossRef]
- Berge, M.G.T.; Beck, N.; Steup, W.H.; Verhagen, A.F.; Van Brakel, T.J.; Schreurs, W.H.; Wouters, M.W.; the Dutch Lung Cancer Audit for Surgery Group. Textbook outcome as a composite outcome measure in non-small-cell lung cancer surgery. Eur. J. Cardio-Thorac. Surg. Off. J. Eur. Assoc. Cardio-Thorac. Surg. 2021, 59, 92–99. [Google Scholar] [CrossRef]
- Halpern, S.E.; Moris, D.; Gloria, J.N.; Shaw, B.I.; Haney, J.C.; Klapper, J.A.; Barbas, A.S.; Hartwig, M.G. Textbook Outcome: Definition and Analysis of a Novel Quality Measure in Lung Transplantation. Ann. Surg. 2021; Publish Ahead of Print. [Google Scholar] [CrossRef]
- Halpern, S.E.; Moris, D.; Shaw, B.I.; Kesseli, S.J.; Samoylova, M.L.; Manook, M.; Schmitz, R.; Collins, B.H.; Sanoff, S.L.; Ravindra, K.V.; et al. Definition and Analysis of Textbook Outcome: A Novel Quality Measure in Kidney Transplantation. World J. Surg. 2021, 45, 1504–1513. [Google Scholar] [CrossRef] [PubMed]
- Lim, C.; Llado, L.; Salloum, C.; Ramos, E.; Lopez-Dominguez, J.; Cachero, A.; Fabregat, J.; Azoulay, D. Textbook Outcome Following Liver Transplantation. World J. Surg. 2021, 45, 3414–3423. [Google Scholar] [CrossRef]
- Moris, D.; Shaw, B.I.; Gloria, J.; Kesseli, S.J.; Samoylova, M.L.; Schmitz, R.; Manook, M.; McElroy, L.M.; Patel, Y.; Berg, C.L.; et al. Textbook Outcomes in Liver Transplantation. World J. Surg. 2020, 44, 3470–3477. [Google Scholar] [CrossRef]
- Görgec, B.; Cacciaguerra, A.B.; Pawlik, T.M.; Aldrighetti, L.A.; Alseidi, A.A.; Cillo, U.; Kokudo, N.; Geller, D.A.; Wakabayashi, G.; Asbun, H.J.; et al. An International Expert Delphi Consensus on Defining Textbook Outcome in Liver Surgery (TOLS). Ann. Surg. 2022; Publish Ahead of Print. [Google Scholar] [CrossRef]
- Görgec, B.; Cacciaguerra, A.B.; Lanari, J.; Russolillo, N.; Cipriani, F.; Aghayan, D.; Zimmitti, G.; Efanov, M.; Alseidi, A.; Mocchegiani, F.; et al. Assessment of Textbook Outcome in Laparoscopic and Open Liver Surgery. JAMA Surg. 2021, 156, e212064. [Google Scholar] [CrossRef]
- Serra, C.; Cossiga, V.; Serenari, M.; Felicani, C.; Mazzotta, E.; Pinato, D.J.; Cescon, M.; Ercolani, G.; Cucchetti, A. Safety and efficacy of percutaneous radiofrequency ablation for hepatocellular carcinoma: A textbook outcome analysis. HPB 2022, 24, 664–671. [Google Scholar] [CrossRef] [PubMed]
- Cillo, U.; Bertacco, A.; Fasolo, E.; Carandina, R.; Vitale, A.; Zanus, G.; Gringeri, E.; D’Amico, F.; Bassi, D.; Neri, D.; et al. Videolaparoscopic microwave ablation in patients with HCC at a European high-volume center: Results of 815 procedures. J. Surg. Oncol. 2019, 120, 956–965. [Google Scholar] [CrossRef] [PubMed]
- Cillo, U.; Noaro, G.; Vitale, A.; Neri, D.; D’Amico, F.; Gringeri, E.; Farinati, F.; Vincenzi, V.; Vigo, M.; Zanus, G.; et al. Laparoscopic microwave ablation in patients with hepatocellular carcinoma: A prospective cohort study. HPB 2014, 16, 979–986. [Google Scholar] [CrossRef] [PubMed]
- Monteiro, A.R.; Garcia, A.R.; Pereira, T.C.; Macedo, F.; Soares, R.F.; Pereira, K.; Serra, T.; Khouri, L.; Ribeiro, J.; Teixeira, M.M. ACE-27 as a prognostic tool of severe acute toxicities in patients with head and neck cancer treated with chemoradiotherapy: A real-world, prospective, observational study. Support Care Cancer Off J. Multinatl. Assoc. Support Care Cancer 2021, 29, 1863–1871. [Google Scholar] [CrossRef] [PubMed]
- Balzan, S.; Belghiti, J.; Farges, O.; Ogata, S.; Sauvanet, A.; Delefosse, D.; Durand, F. The “50-50 criteria” on postoperative day 5: An accurate predictor of liver failure and death after hepatectomy. Ann Surg. 2005, 242, 824–828, discussion 828–829. [Google Scholar] [CrossRef]
- Dindo, D.; Demartines, N.; Clavien, P.A. Classification of Surgical Complications: A New Proposal with Evaluation in a Cohort of 6336 Patients and Results of a Survey. Ann Surg. 2004, 240, 205–213. [Google Scholar] [CrossRef]
- AISF; AIOM; IT-IHPBA; SIC; SIRM; SITO. Raccomandazioni Multisocietarie Italiane (Aisf, Aiom, It-Ihpba, Sic, Sirm, Sito) Per La Gestione Clinica Integrata Del Paziente Con Epatocarcinoma. J. Hepatol. 2018, 69, 182–236. [Google Scholar]
- Galle, P.R.; Forner, A.; Llovet, J.M.; Mazzaferro, V.; Piscaglia, F.; Raoul, J.L.; Schirmacher, P.; Vilgrain, V. EASL Clinical Practice Guidelines: Management of hepatocellular carcinoma. J. Hepatol. 2018, 69, 182–236. [Google Scholar] [CrossRef]
- Pretzsch, E.; Koliogiannis, D.; D’Haese, J.G.; Ilmer, M.; Guba, M.O.; Angele, M.K.; Werner, J.; Niess, H. Textbook outcome in hepato-pancreato-biliary surgery: Systematic review. BJS Open 2022, 6, zrac149. [Google Scholar] [CrossRef] [PubMed]
- Merath, K.; Chen, Q.; Bagante, F.; Beal, E.; Akgul, O.; Dillhoff, M.; Cloyd, J.M.; Pawlik, T.M. Textbook Outcomes Among Medicare Patients Undergoing Hepatopancreatic Surgery. Ann. Surg. 2020, 271, 1116–1123. [Google Scholar] [CrossRef]
- Kazaryan, A.M.; Røsok, B.I.; Edwin, B. Morbidity assessment in surgery: Refinement proposal based on a concept of perioperative adverse events. ISRN Surg. 2013, 2013, 625093. [Google Scholar] [CrossRef]
- Koch, M.; Garden, O.J.; Padbury, R.; Rahbari, N.N.; Adam, R.; Capussotti, L.; Fan, S.T.; Yokoyama, Y.; Crawford, M.; Makuuchi, M.; et al. Bile leakage after hepatobiliary and pancreatic surgery: A definition and grading of severity by the International Study Group of Liver Surgery. Surgery 2011, 149, 680–688. [Google Scholar] [CrossRef]
- Rahbari, N.N.; Garden, O.J.; Padbury, R.; Brooke-Smith, M.; Crawford, M.; Adam, R.; Koch, M.; Makuuchi, M.; Dematteo, R.P.; Christophi, C.; et al. Posthepatectomy liver failure: A definition and grading by the International Study Group of Liver Surgery (ISGLS). Surgery 2011, 149, 713–724. [Google Scholar] [CrossRef]
- Clavien, P.A.; Barkun, J.; de Oliveira, M.L.; Vauthey, J.N.; Dindo, D.; Schulick, R.D.; de Santibañes, E.; Pekolj, J.; Slankamenac, K.; Bassi, C.; et al. The Clavien-Dindo classification of surgical complications: Five-year experience. Ann. Surg. 2009, 250, 187–196. [Google Scholar] [CrossRef]
- Mayo, S.C.; Shore, A.D.; Nathan, H.; Edil, B.H.; Hirose, K.; Anders, R.A.; Wolfgang, C.L.; Schulick, R.D.; Choti, M.A.; Pawlik, T.M. Refining the definition of perioperative mortality following hepatectomy using death within 90 days as the standard criterion. HPB 2011, 13, 473–482. [Google Scholar] [CrossRef]
- Mise, Y.; Vauthey, J.-N.; Zimmitti, G.; Parker, N.H.; Conrad, C.; Aloia, T.A.; Lee, J.E.; Fleming, J.B.; Katz, M.H.G. Ninety-day Postoperative Mortality Is a Legitimate Measure of Hepatopancreatobiliary Surgical Quality. Ann. Surg. 2015, 262, 1071–1078. [Google Scholar] [CrossRef]
- Boutros, C.; Somasundar, P.; Garrean, S.; Saied, A.; Espat, N.J. Microwave coagulation therapy for hepatic tumors: Review of the literature and critical analysis. Surg. Oncol. 2010, 19, e22–e32. [Google Scholar] [CrossRef]
- Salati, U.; Barry, A.; Chou, F.Y.; Ma, R.; Liu, D.M. State of the ablation nation: A review of ablative therapies for cure in the treatment of hepatocellular carcinoma. Future Oncol. Lond. Engl. 2017, 13, 1437–1448. [Google Scholar] [CrossRef]
- Vitale, A.; Trevisani, F.; Farinati, F.; Cillo, U. Treatment of Hepatocellular Carcinoma in the Precision Medicine Era: From Treatment Stage Migration to Therapeutic Hierarchy. Hepatology 2020, 72, 2206–2218. [Google Scholar] [CrossRef] [PubMed]
- Vitale, A.; Farinati, F.; Pawlik, T.M.; Frigo, A.C.; Giannini, E.G.; Napoli, L.; Ciccarese, F.; Rapaccini, G.L.; Di Marco, M.; Caturelli, E.; et al. The concept of therapeutic hierarchy for patients with hepatocellular carcinoma: A multicenter cohort study. Liver Int. 2019, 39, 1478–1489. [Google Scholar] [CrossRef]
- Santambrogio, R.; Barabino, M.; D’Alessandro, V.; Galfrascoli, E.; Zappa, M.A.; Piccolo, G.; Zuin, M.; Opocher, E. Laparoscopic thermoablation for hepatocellular carcinoma in patients with liver cirrhosis: An effective procedure for tricky tumors. Med. Oncol. Northwood Lond. Engl. 2020, 37, 32. [Google Scholar] [CrossRef] [PubMed]
- Santambrogio, R.; Barabino, M.; Bruno, S.; Costa, M.; Ceretti, A.P.; Angiolini, M.R.; Zuin, M.; Meloni, M.F.; Opocher, E. Long-term outcome of laparoscopic ablation therapies for unresectable hepatocellular carcinoma: A single European center experience of 426 patients. Surg. Endosc. 2016, 30, 2103–2113. [Google Scholar] [CrossRef] [PubMed]
- de la Serna, S.; Vilana, R.; Sánchez-Cabús, S.; Calatayud, D.; Ferrer, J.; Molina, V.; Fondevila, C.; Bruix, J.; Fuster, J.; García-Valdecasas, J.-C. Results of laparoscopic radiofrequency ablation for HCC. Could the location of the tumor influence a complete response to treatment? A single European center experience. HPB 2015, 17, 387–393. [Google Scholar] [CrossRef] [PubMed]
- Farinati, F.; Vanin, V.; Giacomin, A.; Pozzan, C.; Cillo, U.; Vitale, A.; Di Nolfo, A.M.; Del Poggio, P.; Benvegnu’, L.; Rapaccini, G.; et al. BCLC stage B hepatocellular carcinoma and transcatheter arterial chemoembolization: A 20-year survey by the Italian Liver Cancer group. Liver Int. 2015, 35, 223–231. [Google Scholar] [CrossRef] [PubMed]
- Cillo, U.; Vitale, A.; Volk, M.L.; Frigo, A.C.; Grigoletto, F.; Brolese, A.; Zanus, G.; D’Amico, F.; Farinati, F.; Burra, P.; et al. The survival benefit of liver transplantation in hepatocellular carcinoma patients. Dig. Liver Dis. 2010, 42, 642–649. [Google Scholar] [CrossRef] [PubMed]






{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Characteristic | Not Achieved TO 1 n = 184 | Achieved TO 1 n = 337 | p2 |
|---|---|---|---|
| Sex (male) | 149/184 (81%) | 290/337 (86%) | 0.13 |
| Age (y) | 64.5 (57.9–69.15) | 62.9 (56.6–67.8) | 0.092 |
| Comorbidities | |||
| - None | 72/183 (39%) | 144/335 (43%) | 0.038 |
| - Mild | 98/183 (54%) | 176/335 (53%) | |
| - Moderate | 13/183 (7.1%) | 15/335 (4.5%) | |
| ECOG PS = 1 | 24/184 (13%) | 36/337 (11%) | 0.42 |
| Liver disease etiology | |||
| - HCV | 93/184 (51%) | 153/337 (45%) | 0.26 |
| - HBV | 36/184 (20%) | 74/337 (22%) | 0.52 |
| - Alcohol | 56/184 (30%) | 104/337 (31%) | 0.92 |
| Platelet count (×103/mL) | 85 (64.5–130) | 95 (67.8–141.5) | 0.031 |
| Portal hypertension | 113/184 (61%) | 171/337 (51%) | 0.019 |
| MELD ≥ 15 | 21/180 (12%) | 10/318 (3.1%) | <0.001 |
| Child–Pugh Classes | |||
| - Child A | 92/159 (58%) | 229/274 (84%) | <0.001 |
| - Child B | 67/159 (42%) | 45/274 (16%) | |
| Previous HCC treatments | 91/184 (49%) | 166/337 (49%) | 0.97 |
| Number of nodules | |||
| - 1 | 93/184 (51%) | 172/337 (51%) | 0.015 |
| - 2 | 42/184 (23%) | 107/337 (32%) | |
| - 3 | 49/184 (27%) | 58/337 (17%) | |
| Diameter of the largest nodule (cm) | |||
| - <2 | 75/184 (41%) | 185/337 (55%) | 0.003 |
| - 2–3 | 54/184 (29%) | 90/337 (27%) | |
| - 3–5 | 55/184 (30%) | 62/337 (18%) | |
| pRBC | 10/183 (5.5%) | 1/331 (0.3%) | <0.001 |
| pFFP | 24/183 (13%) | 5/331 (1.5%) | <0.001 |
| Characteristic | N (%) |
|---|---|
| Fever | 30 (5.8%) |
| Nausea and vomiting | 1 (0.2%) |
| Pleural effusion | 4 (0.8%) |
| Pneumothorax | 3 (0.6%) |
| Ascites | 61 (11.7%) |
| Hemoperitoneum | 1 (0.2%) |
| Liver disfunction (50-50 criteria) | 31 (6.0%) |
| 30 days mortality | 2 (0.4%) |
| Readmission | 12 (2.3%) |
| LOS > 3 days | 96 (18.4%) |
| No CR | 30 (5.8%) |
| Univariable Analysis | Multivariable Analysis | |||||
|---|---|---|---|---|---|---|
| Variables | OR 1 | 95% CI 2 | p | OR1 | 95% CI 2 | p |
| Sex (male) | 1.45 | 0.89, 2.34 | 0.13 | |||
| Age ≥ 70 | 0.74 | 0.46, 1.22 | 0.2 | 0.49 | 0.27, 0.88 | 0.017 |
| Comorbidities | ||||||
| - Mild | 0.90 | 0.62, 1.31 | 0.6 | |||
| - Moderate | 0.58 | 0.26, 1.29 | 0.2 | |||
| ECOG PS = 1 | 0.80 | 0.46, 1.40 | 0.4 | |||
| HCV | 0.81 | 0.57, 1.17 | 0.3 | |||
| HBV | 1.16 | 0.74, 1.82 | 0.5 | |||
| Alcohol | 1.02 | 0.69, 1.51 | >0.9 | |||
| INR | 0.12 | 0.04, 0.35 | <0.001 | |||
| Bilirubin level (mg/dL) | 0.64 | 0.49, 0.80 | <0.001 | |||
| Portal hypertension | 0.65 | 0.45, 0.93 | 0.020 | |||
| MELD ≥ 15 | 0.25 | 0.11, 0.52 | <0.001 | 0.44 | 0.17, 1.09 | 0.086 |
| Child–Pugh class B | 0.27 | 0.17, 0.42 | <0.001 | 0.28 | 0.17, 0.46 | <0.001 |
| Number of nodules | ||||||
| - 2 | 1.38 | 0.89, 2.15 | 0.2 | 1.41 | 0.85, 2.35 | 0.2 |
| - 3 | 0.64 | 0.41, 1.01 | 0.055 | 0.54 | 0.32, 0.93 | 0.025 |
| Portal hypertension | 0.65 | 0.45, 0.93 | 0.020 | |||
| Diameter largest nodule (cm) | ||||||
| - 2–3 | 0.66 | 0.43, 1.02 | 0.061 | |||
| - 3–5 | 0.46 | 0.29, 0.72 | <0.001 | |||
| pRBC | 0.05 | 0.00, 0.28 | 0.005 | |||
| pFFP | 0.10 | 0.03, 0.25 | <0.001 | |||
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Lanari, J.; Caregari, S.; Billato, I.; Gringeri, E.; D’Amico, F.; Gemo, G.; Bassi, D.; D’Amico, F.E.; Boetto, R.; Bertacco, A.; et al. Textbook Outcome of Laparoscopic Microwave Ablation for Hepatocellular Carcinoma. Cancers 2023, 15, 436. https://doi.org/10.3390/cancers15020436
Lanari J, Caregari S, Billato I, Gringeri E, D’Amico F, Gemo G, Bassi D, D’Amico FE, Boetto R, Bertacco A, et al. Textbook Outcome of Laparoscopic Microwave Ablation for Hepatocellular Carcinoma. Cancers. 2023; 15(2):436. https://doi.org/10.3390/cancers15020436
Chicago/Turabian StyleLanari, Jacopo, Silvia Caregari, Ilaria Billato, Enrico Gringeri, Francesco D’Amico, Giancarlo Gemo, Domenico Bassi, Francesco Enrico D’Amico, Riccardo Boetto, Alessandra Bertacco, and et al. 2023. "Textbook Outcome of Laparoscopic Microwave Ablation for Hepatocellular Carcinoma" Cancers 15, no. 2: 436. https://doi.org/10.3390/cancers15020436
APA StyleLanari, J., Caregari, S., Billato, I., Gringeri, E., D’Amico, F., Gemo, G., Bassi, D., D’Amico, F. E., Boetto, R., Bertacco, A., Marchini, A., Lazzari, S., Brolese, M., Ballo, M., Vitale, A., & Cillo, U. (2023). Textbook Outcome of Laparoscopic Microwave Ablation for Hepatocellular Carcinoma. Cancers, 15(2), 436. https://doi.org/10.3390/cancers15020436