
Hypothyroidism following Radiotherapy for Head and Neck Cancer: A Systematic Review of the Literature and Opportunities to Improve the Therapeutic Ratio
 ,
,  ,
,  ,
, 
Abstract
:Simple Summary
Abstract
1. Introduction
2. Materials and Methods
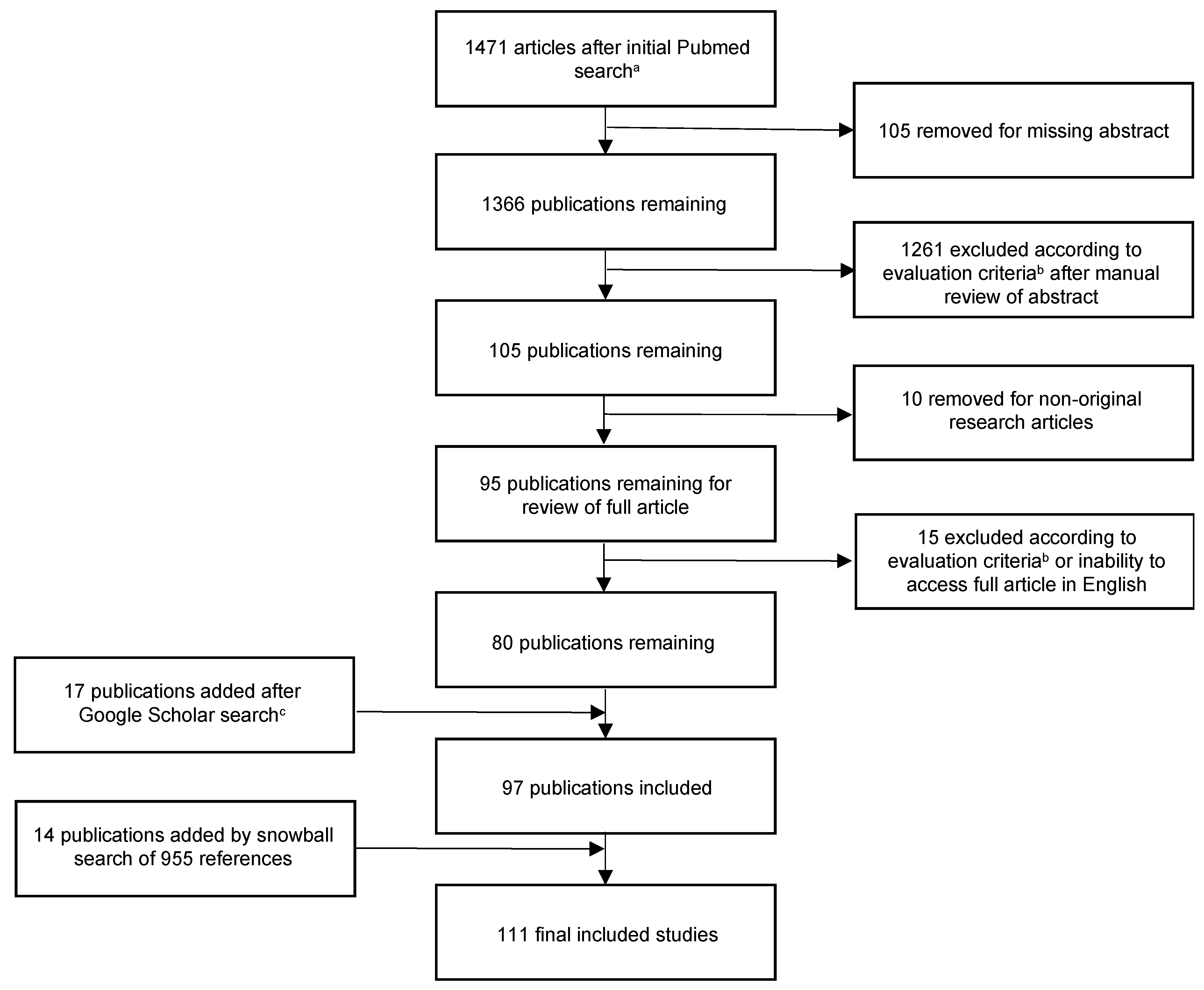
2.1. Search Protocol and Article Identification
2.2. Article Evaluation and Data Collection
3. Results
3.1. Estimated Incidence of RT-Induced Hypothyroidism
3.2. Radiation Modality, Technique, and Dosimetric Predictors of Hypothyroidism
3.3. Interventions Aimed at Preventing RT-Induced Hypothyroidism
3.4. Impact of Patient and Physician Factors on RT-Induced Hypothyroidism
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Bianchi, G.; Zaccheroni, V.; Solaroli, E.; Vescini, F.; Cerutti, R.; Zoli, M.; Marchesini, G. Health-related quality of life in patients with thyroid disorders. Qual. Life Res. 2004, 13, 45–54. [Google Scholar] [CrossRef] [PubMed]
- Watt, T.; Groenvold, M.; Rasmussen, A.K.; Bonnema, S.J.; Hegedüs, L.; Bjorner, J.B.; Feldt-Rasmussen, U. Quality of life in patients with benign thyroid disorders. A review. Eur. J. Endocrinol. 2006, 154, 501–510. [Google Scholar] [CrossRef] [PubMed]
- Thvilum, M.; Brandt, F.; Almind, D.; Christensen, K.; Hegedüs, L.; Brix, T.H. Excess Mortality in Patients Diagnosed with Hypothyroidism: A Nationwide Cohort Study of Singletons and Twins. J. Clin. Endocrinol. Metab. 2013, 98, 1069–1075. [Google Scholar] [CrossRef] [PubMed]
- Bano, A.; Dhana, K.; Chaker, L.; Kavousi, M.; Ikram, M.A.; Mattace-Raso, F.U.S.; Peeters, R.P.; Franco, O.H. Association of Thyroid Function with Life Expectancy with and without Cardiovascular Disease: The Rotterdam Study. JAMA Intern. Med. 2017, 177, 1650–1657. [Google Scholar] [CrossRef] [PubMed]
- Benvenga, S. When thyroid hormone replacement is ineffective? Curr. Opin. Endocrinol. Diabetes 2013, 20, 467–477. [Google Scholar] [CrossRef]
- Chaker, L.; Bianco, A.C.; Jonklaas, J.; Peeters, R.P. Hypothyroidism. Lancet 2017, 390, 1550–1562. [Google Scholar] [CrossRef]
- Peeters, R.P. Subclinical Hypothyroidism. N. Engl. J. Med. 2017, 376, 2556–2565. [Google Scholar] [CrossRef]
- Moher, D.; Liberati, M.; Tetzlaff, J.; Altman, D.G.; PRISMA Group. Preferred reporting items for systematic reviews and meta-analyses: The PRISMA statement. PLoS Med. 2009, 6, e1000097. [Google Scholar] [CrossRef]
- Page, M.J.; McKenzie, J.E.; Bossuyt, P.M.; Boutron, I.; Hoffmann, T.C.; Mulrow, C.D.; Shamseer, L.; Tetzlaff, J.M.; Akl, E.A.; Brennan, S.E.; et al. The PRISMA 2020 Statement: An Updated Guideline for Reporting Systematic Reviews. BMJ 2021, 372, n71. [Google Scholar] [CrossRef]
- Wohlin, C. Guidelines for Snowballing in Systematic Literature Studies and a Replication in Software Engineering. In Proceedings of the 18th International Conference on Evaluation and Assessment in Software Engineering, New York, NY, USA, 13–14 May 2014; ACM: London, UK, 2014; pp. 1–10. [Google Scholar]
- Greenhalgh, T.; Peacock, R. Effectiveness and efficiency of search methods in systematic reviews of complex evidence: Audit of primary sources. BMJ 2005, 331, 1064–1065. [Google Scholar] [CrossRef]
- Peng, G.; Wang, T.; Yang, K.-Y.; Zhang, S.; Zhang, T.; Li, Q.; Han, J.; Wu, G. A prospective, randomized study comparing outcomes and toxicities of intensity-modulated radiotherapy vs. conventional two-dimensional radiotherapy for the treatment of nasopharyngeal carcinoma. Radiother. Oncol. 2012, 104, 286–293. [Google Scholar] [CrossRef] [PubMed]
- Murthy, V.; Narang, K.; Ghosh-Laskar, S.; Gupta, T.; Budrukkar, A.; Agrawal, J.P. Hypothyroidism after 3-dimensional conformal radiotherapy and intensity-modulated radiotherapy for head and neck cancers: Prospective data from 2 randomized controlled trials. Head Neck 2014, 36, 1573–1580. [Google Scholar] [CrossRef] [PubMed]
- Boomsma, M.J.; Bijl, H.P.; Christianen, M.E.; Beetz, I.; Chouvalova, O.; Steenbakkers, R.J.; van der Laan, B.F.; Wolffenbuttel, B.H.; Oosting, S.F.; Schilstra, C.; et al. A Prospective Cohort Study on Radiation-induced Hypothyroidism: Development of an NTCP Model. Int. J. Radiat. Oncol. 2012, 84, e351–e356. [Google Scholar] [CrossRef] [PubMed]
- Rønjom, M.F.; Brink, C.; Bentzen, S.M.; Hegedüs, L.; Overgaard, J.; Johansen, J. Hypothyroidism after primary radiotherapy for head and neck squamous cell carcinoma: Normal tissue complication probability modeling with latent time correction. Radiother. Oncol. 2013, 109, 317–322. [Google Scholar] [CrossRef] [PubMed]
- Bakhshandeh, M.; Hashemi, B.; Mahdavi, S.R.M.; Nikoofar, A.; Vasheghani, M.; Kazemnejad, A. Normal Tissue Complication Probability Modeling of Radiation-Induced Hypothyroidism after Head-and-Neck Radiation Therapy. Int. J. Radiat. Oncol. 2013, 85, 514–521. [Google Scholar] [CrossRef]
- Huang, S.; Wang, X.; Hu, C.; Ying, H. Hypothalamic–pituitary–thyroid dysfunction induced by intensity-modulated radiotherapy (IMRT) for adult patients with nasopharyngeal carcinoma. Med. Oncol. 2013, 30, 710. [Google Scholar] [CrossRef]
- Akgun, Z.; Atasoy, B.M.; Ozen, Z.; Yavuz, D.; Gulluoglu, B.; Sengoz, M.; Abacioglu, U. V30 as a predictor for radiation-induced hypothyroidism: A dosimetric analysis in patients who received radiotherapy to the neck. Radiat. Oncol. 2014, 9, 104. [Google Scholar] [CrossRef]
- Kim, M.Y.; Yu, T.; Wu, H.-G. Dose-volumetric Parameters for Predicting Hypothyroidism after Radiotherapy for Head and Neck Cancer. Jpn. J. Clin. Oncol. 2014, 44, 331–337. [Google Scholar] [CrossRef]
- Chyan, A.; Chen, J.; Shugard, E.; Lambert, L.; Quivey, J.M.; Yom, S.S. Dosimetric predictors of hypothyroidism in oropharyngeal cancer patients treated with intensity-modulated radiation therapy. Radiat. Oncol. 2014, 9, 269. [Google Scholar] [CrossRef]
- Fujiwara, M.; Kamikonya, N.; Odawara, S.; Suzuki, H.; Niwa, Y.; Takada, Y.; Doi, H.; Terada, T.; Uwa, N.; Sagawa, K.; et al. The threshold of hypothyroidism after radiation therapy for head and neck cancer: A retrospective analysis of 116 cases. J. Radiat. Res. 2015, 56, 577–582. [Google Scholar] [CrossRef]
- Rønjom, M.F.; Brink, C.; Lorenzen, E.L.; Hegedüs, L.; Johansen, J. Variation of normal tissue complication probability (NTCP) estimates of radiation-induced hypothyroidism in relation to changes in delineation of the thyroid gland. Acta Oncol. 2015, 54, 1188–1194. [Google Scholar] [CrossRef] [PubMed]
- Pil, J.; Nevens, D.; Van Der Vorst, A.; Gadan, C.; Nuyts, S. The incidence of hypothyroidism after radiotherapy for head and neck cancer. B-ENT 2016, 12, 257–262. [Google Scholar] [PubMed]
- Luo, R.; Li, M.; Yang, Z.; Zhan, Y.; Huang, B.; Lu, J.; Xu, Z.; Lin, Z. Nomogram for radiation-induced hypothyroidism prediction in nasopharyngeal carcinoma after treatment. Br. J. Radiol. 2017, 90, 20160686. [Google Scholar] [CrossRef] [PubMed]
- Lee, V.; Chan, S.-Y.; Choi, C.-W.; Kwong, D.; Lam, K.-O.; Tong, C.-C.; Sze, C.-K.; Ng, S.; Leung, T.-W.; Lee, A. Dosimetric Predictors of Hypothyroidism after Radical Intensity-modulated Radiation Therapy for Non-metastatic Nasopharyngeal Carcinoma. Clin. Oncol. 2016, 28, e52–e60. [Google Scholar] [CrossRef]
- Ling, S.; Bhatt, A.D.; Brown, N.V.; Nguyen, P.; Sipos, J.A.; Chakravarti, A.; Rong, Y. Correlative study of dose to thyroid and incidence of subsequent dysfunction after head and neck radiation. Head Neck 2016, 39, 548–554. [Google Scholar] [CrossRef]
- Sommat, K.; Ong, W.S.; Hussain, A.; Soong, Y.L.; Tan, T.; Wee, J.; Fong, K.W. Thyroid V40 Predicts Primary Hypothyroidism after Intensity Modulated Radiation Therapy for Nasopharyngeal Carcinoma. Int. J. Radiat. Oncol. 2017, 98, 574–580. [Google Scholar] [CrossRef]
- Zhai, R.-P.; Kong, F.-F.; Du, C.-R.; Hu, C.-S.; Ying, H.-M. Radiation-induced hypothyroidism after IMRT for nasopharyngeal carcinoma: Clinical and dosimetric predictors in a prospective cohort study. Oral Oncol. 2017, 68, 44–49. [Google Scholar] [CrossRef]
- Sachdev, S.; Refaat, T.; Bacchus, I.D.; Sathiaseelan, V.; Mittal, B.B. Thyroid V50 Highly Predictive of Hypothyroidism in Head-and-Neck Cancer Patients Treated with Intensity-modulated Radiotherapy (IMRT). Am. J. Clin. Oncol. 2017, 40, 413–417. [Google Scholar] [CrossRef]
- Lin, Z.; Yang, Z.; He, B.; Wang, D.; Gao, X.; Tam, S.-Y.; Wu, V.W.C. Pattern of radiation-induced thyroid gland changes in nasopharyngeal carcinoma patients in 48 months after radiotherapy. PLoS ONE 2018, 13, e0200310. [Google Scholar] [CrossRef]
- Xu, Y.; Shao, Z.; Tang, T.; Liu, G.; Yao, Y.; Wang, J.; Zhang, L. A dosimetric study on radiation-induced hypothyroidism following intensity-modulated radiotherapy in patients with nasopharyngeal carcinoma. Oncol. Lett. 2018, 16, 6126–6132. [Google Scholar] [CrossRef]
- Lertbutsayanukul, C.; Kitpanit, S.; Prayongrat, A.; Kannarunimit, D.; Netsawang, B.; Chakkabat, C. Validation of previously reported predictors for radiation-induced hypothyroidism in nasopharyngeal cancer patients treated with intensity-modulated radiation therapy, a post hoc analysis from a Phase III randomized trial. J. Radiat. Res. 2018, 59, 446–455. [Google Scholar] [CrossRef]
- El-Shebiney, M.; El-Mashad, N.; El-Mashad, W.; El-Ebiary, A.A.; Kotkat, A.E. Radiotherapeutic factors affecting the incidence of developing hypothyroidism after radiotherapy for head and neck squamous cell cancer. J. Egypt. Natl. Cancer Inst. 2018, 30, 33–38. [Google Scholar] [CrossRef] [PubMed]
- McDowell, L.J.; Rock, K.; Xu, W.; Chan, B.; Waldron, J.; Lu, L.; Ezzat, S.; Pothier, D.; Bernstein, L.J.; So, N.; et al. Long-Term Late Toxicity, Quality of Life, and Emotional Distress in Patients with Nasopharyngeal Carcinoma Treated with Intensity Modulated Radiation Therapy. Int. J. Radiat. Oncol. 2018, 102, 340–352. [Google Scholar] [CrossRef]
- Luo, R.; Wu, V.W.C.; He, B.; Gao, X.; Xu, Z.; Wang, D.; Yang, Z.; Li, M.; Lin, Z. Development of a normal tissue complication probability (NTCP) model for radiation-induced hypothyroidism in nasopharyngeal carcinoma patients. BMC Cancer 2018, 18, 575. [Google Scholar] [CrossRef]
- Kamal, M.; Peeler, C.R.; Yepes, P.; Mohamed, A.S.R.; Blanchard, P.; Frank, S.; Chen, L.; Jethanandani, A.; Kuruvilla, R.; Greiner, B.; et al. Radiation-Induced Hypothyroidism after Radical Intensity Modulated Radiation Therapy for Oropharyngeal Carcinoma. Adv. Radiat. Oncol. 2020, 5, 111–119. [Google Scholar] [CrossRef] [PubMed]
- Prpic, M.; Kruljac, I.; Kust, D.; Suton, P.; Purgar, N.; Bilos, L.K.; Gregov, M.; Mrcela, I.; Franceschi, M.; Djakovic, N.; et al. Dose-volume derived nomogram as a reliable predictor of radiotherapy-induced hypothyroidism in head and neck cancer patients. Radiol. Oncol. 2019, 53, 488–496. [Google Scholar] [CrossRef]
- Huang, C.; Tan, H.; Guo, R.; Zhang, Y.; Peng, H.; Peng, L.; Lin, A.; Mao, Y.; Sun, Y.; Ma, J.; et al. Thyroid dose-volume thresholds for the risk of radiation-related hypothyroidism in nasopharyngeal carcinoma treated with intensity-modulated radiotherapy—A single-institution study. Cancer Med. 2019, 8, 6887–6893. [Google Scholar] [CrossRef]
- Lin, A.J.; Zhang, J.; Cho-Lim, J.; Inouye, W.; Lee, S.P. Postradiation hypothyroidism in head and neck cancers: A Department of Veterans Affairs single-institution case-control dosimetry study. Med. Dosim. 2019, 44, 56–60. [Google Scholar] [CrossRef]
- Peng, L.; Mao, Y.-P.; Huang, C.-L.; Guo, R.; Ma, J.; Wen, W.-P.; Tang, L.-L. A New Model for Predicting Hypothyroidism after Intensity-Modulated Radiotherapy for Nasopharyngeal Carcinoma. Front. Oncol. 2020, 10. [Google Scholar] [CrossRef]
- Kinclová, I.; Hajtmanová, E.; Matula, P.; Balentová, S.; Muríň, P.; Ďuroška, M.; Kozlíková, K. Model-based calculation of thyroid gland normal tissue complication probability in head and neck cancer patients after radiation therapy. Strahlenther. Onkol. 2020, 196, 561–568. [Google Scholar] [CrossRef]
- Zhou, L.; Chen, J.; Shen, W.; Chen, Z.-L.; Huang, S.; Tao, C.-J.; Chen, M.; Yu, Z.-H.; Chen, Y.-Y. Thyroid V50 is a risk factor for hypothyroidism in patients with nasopharyngeal carcinoma treated with intensity-modulated radiation therapy: A retrospective study. Radiat. Oncol. 2020, 15, 68. [Google Scholar] [CrossRef] [PubMed]
- Zhu, M.-Y.; Wu, H.-J.; Miao, J.-J.; Di, M.-P.; Chen, B.-Y.; Huang, H.-G.; Mai, H.-Q.; Wang, L.; Zhao, C. Radiation-induced hypothyroidism in patients with nasopharyngeal carcinoma treated with intensity-modulated radiation therapy with or without chemotherapy: Development of a nomogram based on the equivalent dose. Oral Oncol. 2021, 120, 105378. [Google Scholar] [CrossRef] [PubMed]
- Inoue, E.; Okajima, K.; Doi, H.; Fukuda, K.; Oguma, Y.; Ri, A.; Nishikawa, D.; Yane, K.; Matsuura, T.; Nishimura, Y. Factors predictive of the development of hypothyroidism after intensity-modulated radiation therapy for pharyngeal cancer. Acta Oto-Laryngologica 2021, 141, 1022–1026. [Google Scholar] [CrossRef]
- Lu, H.-H.; Chiu, N.-T.; Tsai, M.-H. Early post-treatment 18F-FDG PET/CT for predicting radiation-induced hypothyroidism in head and neck cancer. Cancer Imaging 2022, 22, 59. [Google Scholar] [CrossRef]
- Zhai, R.; Lyu, Y.; Ni, M.; Kong, F.; Du, C.; Hu, C.; Ying, H. Predictors of radiation-induced hypothyroidism in nasopharyngeal carcinoma survivors after intensity-modulated radiotherapy. Radiat. Oncol. 2022, 17, 57. [Google Scholar] [CrossRef] [PubMed]
- Pal, S.K.; Das, S.; Isiah, R.; John, S. Determining the Occurrence of Hypothyroidism following Treatment with Radiation Therapy in Head and Neck Carcinoma Patients and the Associated Role of Risk Factors and Dose-Volume Histograms: A Prospective Study. Cureus 2022, 14, e31590. [Google Scholar] [CrossRef]
- Jia-Mahasap, B.; Assavanopakun, K.; Chitapanarux, I.; Kittidachanan, K.; Sirikul, W. Incidence of radiation-induced hypothyroidism following head and neck irradiation: A single-center analysis. Rep. Pract. Oncol. Radiother. 2022, 27, 479–489. [Google Scholar] [CrossRef]
- Chow, J.C.; Lui, J.C.; Cheung, K.-M.; Tam, A.H.; Lam, M.H.; Yuen, T.Y.; Lee, F.K.; Leung, A.K.; Au, K.-H.; Ng, W.-T.; et al. Post-radiation primary hypothyroidism in patients with head and neck cancer: External validation of thyroid gland dose–volume constraints with long-term endocrine outcomes. Radiother. Oncol. 2022, 177, 105–110. [Google Scholar] [CrossRef]
- Harris, J.; Almarzouki, H.; Barber, B.; Scrimger, R.; Romney, J.; O’Connell, D.; Urken, M.; Seikaly, H. Free Thyroid Transfer: A Novel Procedure to Prevent Radiation-induced Hypothyroidism. Int. J. Radiat. Oncol. 2016, 96, 42–45. [Google Scholar] [CrossRef]
- Harris, J.; Barber, B.; Almarzouki, H.; Scrimger, R.; Romney, J.; O’Connell, D.; Urken, M.; Seikaly, H. Free thyroid transfer: Short-term results of a novel procedure to prevent post-radiation hypothyroidism. Head Neck 2016, 39, 1234–1238. [Google Scholar] [CrossRef]
- Katna, R.; Kalyani, N.; Deshpande, A. Free thyroid transfer to anterolateral thigh for prevention of radiation induced hypothyroidism: An initial experience. Am. J. Otolaryngol. 2018, 40, 160–163. [Google Scholar] [CrossRef]
- Zoberi, I.; Wasserman, T.H.; Chao, K.C. A prospective, nonrandomized study of the impact of amifostine on subsequent hypothyroidism in irradiated patients with head and neck cancers. Semin. Radiat. Oncol. 2002, 12, 14–17. [Google Scholar] [CrossRef] [PubMed]
- Alterio, D.; Jereczek-Fossa, B.A.; Franchi, B.; D’onofrio, A.; Piazzi, V.; Rondi, E.; Ciocca, M.; Gibelli, B.; Grosso, E.; Tradati, N.; et al. Thyroid disorders in patients treated with radiotherapy for head-and-neck cancer: A retrospective analysis of seventy-three patients. Int. J. Radiat. Oncol. 2007, 67, 144–150. [Google Scholar] [CrossRef] [PubMed]
- Ishibashi, N.; Maebayashi, T.; Aizawa, T.; Sakaguchi, M.; Okada, M.; Matsushita, J. Computed Tomography Density Change in the Thyroid Gland before and after Radiation Therapy. Anticancer Res. 2018, 38, 417–421. [Google Scholar] [CrossRef] [PubMed]
- Lin, Z.; Wu, V.W.-C.; Lin, J.; Feng, H.; Chen, L. A Longitudinal Study on the Radiation-Induced Thyroid Gland Changes after External Beam Radiotherapy of Nasopharyngeal Carcinoma. Thyroid 2011, 21, 19–23. [Google Scholar] [CrossRef] [PubMed]
- Ulger, S.; Ulger, Z.; Yildiz, F.; Ozyar, E. Incidence of Hypothyroidism after Radiotherapy for Nasopharyngeal Carcinoma. Med. Oncol. 2007, 24, 91–94. [Google Scholar] [CrossRef]
- Ranta, P.; Kytö, E.; Nissi, L.; Kinnunen, I.; Vahlberg, T.; Minn, H.; Haapio, E.; Nelimarkka, L.; Irjala, H. Dysphagia, hypothyroidism, and osteoradionecrosis after radiation therapy for head and neck cancer. Laryngoscope Investig. Otolaryngol. 2021, 7, 108–116. [Google Scholar] [CrossRef]
- Wu, Y.-H.; Wang, H.-M.; Chen, H.H.-W.; Lin, C.-Y.; Chen, E.Y.-C.; Fan, K.-H.; Huang, S.-F.; Chen, I.-H.; Liao, C.-T.; Cheng, A.-J.; et al. Hypothyroidism after Radiotherapy for Nasopharyngeal Cancer Patients. Int. J. Radiat. Oncol. 2010, 76, 1133–1139. [Google Scholar] [CrossRef]
- Galbo, A.M.L.; De Bree, R.; Lips, P.; Leemans, C.R. Detecting hypothyroidism after treatment for laryngeal or hypopharyngeal carcinomas: A nationwide survey in The Netherlands. Eur. Arch. Oto-Rhino-Laryngology 2008, 266, 713–718. [Google Scholar] [CrossRef]
- Gormley, M.; Creaney, G.; Schache, A.; Ingarfield, K.; Conway, D.I. Reviewing the epidemiology of head and neck cancer: Definitions, trends and risk factors. Br. Dent. J. 2022, 233, 780–786. [Google Scholar] [CrossRef]
- Alfouzan, A.F. Radiation therapy in head and neck cancer. Saudi Med. J. 2021, 42, 247–254. [Google Scholar] [CrossRef] [PubMed]
- Saloura, V.; Langerman, A.; Rudra, S.; Chin, R.; Cohen, E.E. Multidisciplinary Care of the Patient with Head and Neck Cancer. Surg. Oncol. Clin. N. Am. 2013, 22, 179–215. [Google Scholar] [CrossRef] [PubMed]
- Barton, M.B.; Jacob, S.; Shafiq, J.; Wong, K.; Thompson, S.R.; Hanna, T.P.; Delaney, G.P. Estimating the demand for radiotherapy from the evidence: A review of changes from 2003 to 2012. Radiother. Oncol. 2014, 112, 140–144. [Google Scholar] [CrossRef]
- Pinnix, C.C.; Cella, L.; Andraos, T.Y.; Ayoub, Z.; Milgrom, S.A.; Gunther, J.; Thosani, S.; Wogan, C.; Conson, M.; D’Avino, V.; et al. Predictors of Hypothyroidism in Hodgkin Lymphoma Survivors after Intensity Modulated Versus 3-Dimensional Radiation Therapy. Int. J. Radiat. Oncol. 2018, 101, 530–540. [Google Scholar] [CrossRef]
- Supriya, C.; Nilesh, R.; Mayuri, C.; Sadhana, K.; Reena, E.; Tapas, D.; Lavanya, G.; Prachi, M.; Amita, M.; Shylasree, T.; et al. Late toxicity within a Phase III clinical trial of IG-IMRT in cervix cancer (PARCER): Reanalysis with time weighted adverse event reporting (MOSES). Radiother. Oncol. 2022, 177, 16–20. [Google Scholar] [CrossRef]
- Wortman, B.G.; Post, C.C.; Powell, M.E.; Khaw, P.; Fyles, A.; D’Amico, R.; Haie-Meder, C.; Jürgenliemk-Schulz, I.M.; McCormack, M.; Do, V.; et al. Radiation Therapy Techniques and Treatment-Related Toxicity in the PORTEC-3 Trial: Comparison of 3-Dimensional Conformal Radiation Therapy Versus Intensity-Modulated Radiation Therapy. Int. J. Radiat. Oncol. 2021, 112, 390–399. [Google Scholar] [CrossRef] [PubMed]
- Michalski, J.M.; Yan, Y.; Watkins-Bruner, D.; Bosch, W.R.; Winter, K.; Galvin, J.M.; Bahary, J.-P.; Morton, G.C.; Parliament, M.B.; Sandler, H.M. Preliminary toxicity analysis of 3-dimensional conformal radiation therapy versus intensity modulated radiation therapy on the high-dose arm of the radiation therapy oncology group 0126 prostate cancer trial. Int. J. Radiat. Oncol. Biol. Phys. 2013, 87, 932–938. [Google Scholar] [CrossRef]
- Gupta, T.; Agarwal, J.; Jain, S.; Phurailatpam, R.; Kannan, S.; Ghosh-Laskar, S.; Murthy, V.; Budrukkar, A.; Dinshaw, K.; Prabhash, K.; et al. Three-dimensional conformal radiotherapy (3D-CRT) versus intensity modulated radiation therapy (IMRT) in squamous cell carcinoma of the head and neck: A randomized controlled trial. Radiother. Oncol. 2012, 104, 343–348. [Google Scholar] [CrossRef]
- van Leeuwen, C.M.; Oei, A.L.; Crezee, J.; Bel, A.; Franken, N.A.P.; Stalpers, L.J.A.; Kok, H.P. The alfa and beta of tumours: A review of parameters of the linear-quadratic model, derived from clinical radiotherapy studies. Radiat. Oncol. 2018, 13, 96. [Google Scholar] [CrossRef]
- Thomas, H.; Timmermann, B. Paediatric proton therapy. Br. J. Radiol. 2020, 93. [Google Scholar] [CrossRef]
- Lin, S.H.; Hobbs, B.P.; Verma, V.; Tidwell, R.S.; Smith, G.L.; Lei, X.; Corsini, E.M.; Mok, I.; Wei, X.; Yao, L.; et al. Randomized Phase IIB Trial of Proton Beam Therapy Versus Intensity-Modulated Radiation Therapy for Locally Advanced Esophageal Cancer. J. Clin. Oncol. 2020, 38, 1569–1579. [Google Scholar] [CrossRef] [PubMed]
- Yang, J.T.; Wijetunga, N.A.; Pentsova, E.; Wolden, S.; Young, R.J.; Correa, D.; Zhang, Z.; Zheng, J.; Steckler, A.; Bucwinska, W.; et al. Randomized Phase II Trial of Proton Craniospinal Irradiation Versus Photon Involved-Field Radiotherapy for Patients with Solid Tumor Leptomeningeal Metastasis. J. Clin. Oncol. 2022, 40, 3858–3867. [Google Scholar] [CrossRef] [PubMed]
- Frank, S.J.; Blanchard, P.; Lee, J.J.; Sturgis, E.M.; Kies, M.S.; Machtay, M.; Vikram, B.; Garden, A.S.; Rosenthal, D.I.; Gunn, G.B.; et al. Comparing Intensity-Modulated Proton Therapy with Intensity-Modulated Photon Therapy for Oropharyngeal Cancer: The Journey from Clinical Trial Concept to Activation. Semin. Radiat. Oncol. 2018, 28, 108–113. [Google Scholar] [CrossRef] [PubMed]



{kind=link}
{kind=link}
{kind=link}
| Factor | Count (%) N = 111 | Estimated Hypothyroidism Incidence (%), Reported as Median (IQR) |
|---|---|---|
| Publication Year | ||
| 2000 and prior | 19 (17) | 34 (21–43) |
| 2001–2005 | 8 (7) | 44 (40–47) |
| 2006–2010 | 15 (14) | 31.6 (20.8–45.3) |
| 2011–2015 | 22 (20) | 33.3 (22.8–45) |
| 2016–2020 | 32 (29) | 42.3 (25–46.2) |
| 2021–2022 | 15 (14) | 42 (30.4–54.3) |
| Design | ||
| Prospective | 31 (28) | 37 (27.4–47) |
| Retrospective | 80 (72) | 36.1 (24–46) |
| Interventional | ||
| Yes | 4 (4) | - |
| No | 97 (96) | - |
| Mean/Median Follow Up (months) | ||
| Min | 6 | - |
| First Quartile | 21 | - |
| Median | 32 | - |
| Third Quartile | 50.2 | - |
| Max | 120 | - |
| Unspecified/NA | 24 | - |
| Sample size | Median 102 (62–184.75) | - |
| Participant Type | ||
| Patients | 99 (98) | - |
| Physicians | 2 (2) | - |
| Cancer Site | ||
| General Head and Neck | 64 (58) | 36.7 (26–44.7) |
| Nasopharynx | 28 (25) | 35 (23–46.2) |
| Oropharynx | 6 (5) | 57.5 (35.3–62.5) |
| Larynx/Hypopharynx | 10 (9) | 39.5 (28.7–48.7) |
| Oral Cavity | 3 (3) | 17.9 (16.1–19.7) |
| Radiation Therapy Modality | ||
| Photons | 87 (78) | - |
| Photons/Electrons | 2 (2) | - |
| Particle Therapy | 0 | - |
| Unspecified | 22 (20) | - |
| Radiation Therapy Technique | ||
| IMRT | 36 (32) | 42 (27.4–49.1) |
| Non-IMRT (2D or 3DCRT) | 38 (34) | 35 (21.8–41.6) |
| IMRT and 3DCRT | 10 (9) | 46.5 (27.5–50.8) |
| MRI-guided radiotherapy | 0 | - |
| Unspecified/NA | 27 (24) | 35 (23.9–48.2) |
| Multimodality Therapy | ||
| All therapies allowed | 89 (80) | 36.4 (24.8–45.7) |
| Surgery excluded | 13 (12) | 38.8 (30–47) |
| Surgery required | 4 (4) | 38.6 (26.2–50.5) |
| Unspecified/NA | 5 (5) | 36.4 (25.4–48.2) |
| Thyroid Evaluation | ||
| Biochemical | 73 (66) | 38.8 (26.7–46.2) |
| Clinical | 2 (2) | 4.9 |
| Biochemical and Clinical | 32 (29) | 31.1 (23.9–49.5) |
| Biochemical and Radiographic | 2 (2) | 42 |
| Unspecified/NA * | 2 (2) | - |
| Author | Year | Proposed Predictive Dosimetric and OAR Parameters |
|---|---|---|
| Boomsma, M.J. [14] | 2012 | Dmean, thyroid volume |
| Rønjom, M.F. [15] | 2013 | 25% risk of hypothyroidism for D10cc = 26 Gy, D15cc = 38 Gy, D20cc = 48 Gy, D25cc = 61 Gy |
| Bakhshandeh, M. [16] | 2013 | D50 < 44 Gy |
| Huang, S. [17] | 2013 | Dmean, V40 |
| Murthy, V. [13] | 2014 | D100 was significant predictor on MVA |
| Akgun, Z. [18] | 2014 | Dmean, thyroid volume, V30 |
| Kim, M.Y. [19] | 2014 | V45 Gy < 50% |
| Chyan, A. [20] | 2014 | Dmean < 49 Gy, VS 45 Gy > 3cc, VS 50 Gy > 5cc, V50 Gy < 45% |
| Fujiwara, M. [21] | 2015 | Dmean < 30 Gy |
| Rønjom, M.F. [22] | 2015 | Dmean, thyroid volume |
| Pil, J. [23] | 2016 | Dmean, thyroid volume |
| Luo, R. [24] | 2016 | V50 Gy |
| Lee, V. [25] | 2016 | VS 60 Gy > 10cc, VS 45 Gy > 5 cm |
| Ling, S. [26] | 2017 | D50 < 50 Gy, V50 < 50%, Dmean <54.58 Gy |
| Sommat, K. [27] | 2017 | V40 < 85% |
| Zhai, R. [28] | 2017 | V45 < 50%; V50 < 35% |
| Sachdev, S. [29] | 2017 | V50 Gy < 60% |
| Lin, Z. [30] | 2018 | Dmean, D50 |
| Xu, Y. [31] | 2018 | V50 < 54.5%, Dmean < 51.6 Gy |
| Lertbutsayanukul, C. [32] | 2018 | VS 60 Gy > 10cc |
| El-Shebiney, M. [33] | 2018 | V30 < 42.1% |
| McDowell [34] | 2018 | V50 > 90%. V45 > 99% |
| Luo, R. [35] | 2018 | V50 Gy, Dmax pituitary |
| Kamal, M. [36] | 2019 | Dmean, thyroid volume |
| Prpic, M. [37] | 2019 | Dmin, thyroid volume |
| Huang, C. [38] | 2019 | V25 < 60%, V35 < 55%, V45 < 45% |
| Lin, A.J. [39] | 2019 | V50 Gy < 75% |
| Peng, L. [40] | 2020 | V30, V60, thyroid volume |
| Kinclová, I. [41] | 2020 | V40 < 85% |
| Zhou, L. [42] | 2020 | V50 Gy, thyroid volume < 12.82cc |
| Zhu, M.Y. [43] | 2021 | V35 |
| Inoue, E. [44] | 2021 | V45 Gy > 67% |
| Lu, H.H. [45] | 2022 | Dmean, thyroid volume |
| Zhai, R. [46] | 2022 | V40 < 80% |
| Pal, S.K. [47] | 2022 | D50, DmeanV50 Gy |
| Jia-Mahasap, B. [48] | 2022 | VS 50 Gy |
| Chow, J.C.H. [49] | 2022 | VS 60 Gy |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Rooney, M.K.; Andring, L.M.; Corrigan, K.L.; Bernard, V.; Williamson, T.D.; Fuller, C.D.; Garden, A.S.; Gunn, B.; Lee, A.; Moreno, A.C.; et al. Hypothyroidism following Radiotherapy for Head and Neck Cancer: A Systematic Review of the Literature and Opportunities to Improve the Therapeutic Ratio. Cancers 2023, 15, 4321. https://doi.org/10.3390/cancers15174321
Rooney MK, Andring LM, Corrigan KL, Bernard V, Williamson TD, Fuller CD, Garden AS, Gunn B, Lee A, Moreno AC, et al. Hypothyroidism following Radiotherapy for Head and Neck Cancer: A Systematic Review of the Literature and Opportunities to Improve the Therapeutic Ratio. Cancers. 2023; 15(17):4321. https://doi.org/10.3390/cancers15174321
Chicago/Turabian StyleRooney, Michael K., Lauren M. Andring, Kelsey L. Corrigan, Vincent Bernard, Tyler D. Williamson, Clifton D. Fuller, Adam S. Garden, Brandon Gunn, Anna Lee, Amy C. Moreno, and et al. 2023. "Hypothyroidism following Radiotherapy for Head and Neck Cancer: A Systematic Review of the Literature and Opportunities to Improve the Therapeutic Ratio" Cancers 15, no. 17: 4321. https://doi.org/10.3390/cancers15174321
APA StyleRooney, M. K., Andring, L. M., Corrigan, K. L., Bernard, V., Williamson, T. D., Fuller, C. D., Garden, A. S., Gunn, B., Lee, A., Moreno, A. C., Morrison, W. H., Phan, J., Rosenthal, D. I., Spiotto, M., & Frank, S. J. (2023). Hypothyroidism following Radiotherapy for Head and Neck Cancer: A Systematic Review of the Literature and Opportunities to Improve the Therapeutic Ratio. Cancers, 15(17), 4321. https://doi.org/10.3390/cancers15174321