
Real-World Outcomes of Nivolumab, Pembrolizumab, and Atezolizumab Treatment Efficacy in Korean Veterans with Stage IV Non-Small-Cell Lung Cancer


Abstract
:Simple Summary
Abstract
1. Introduction
2. Methods
2.1. Patients and Ethics Statement
2.2. Study Endpoint and Measures
2.3. Statistical Analysis
3. Results
3.1. Patient Characteristics
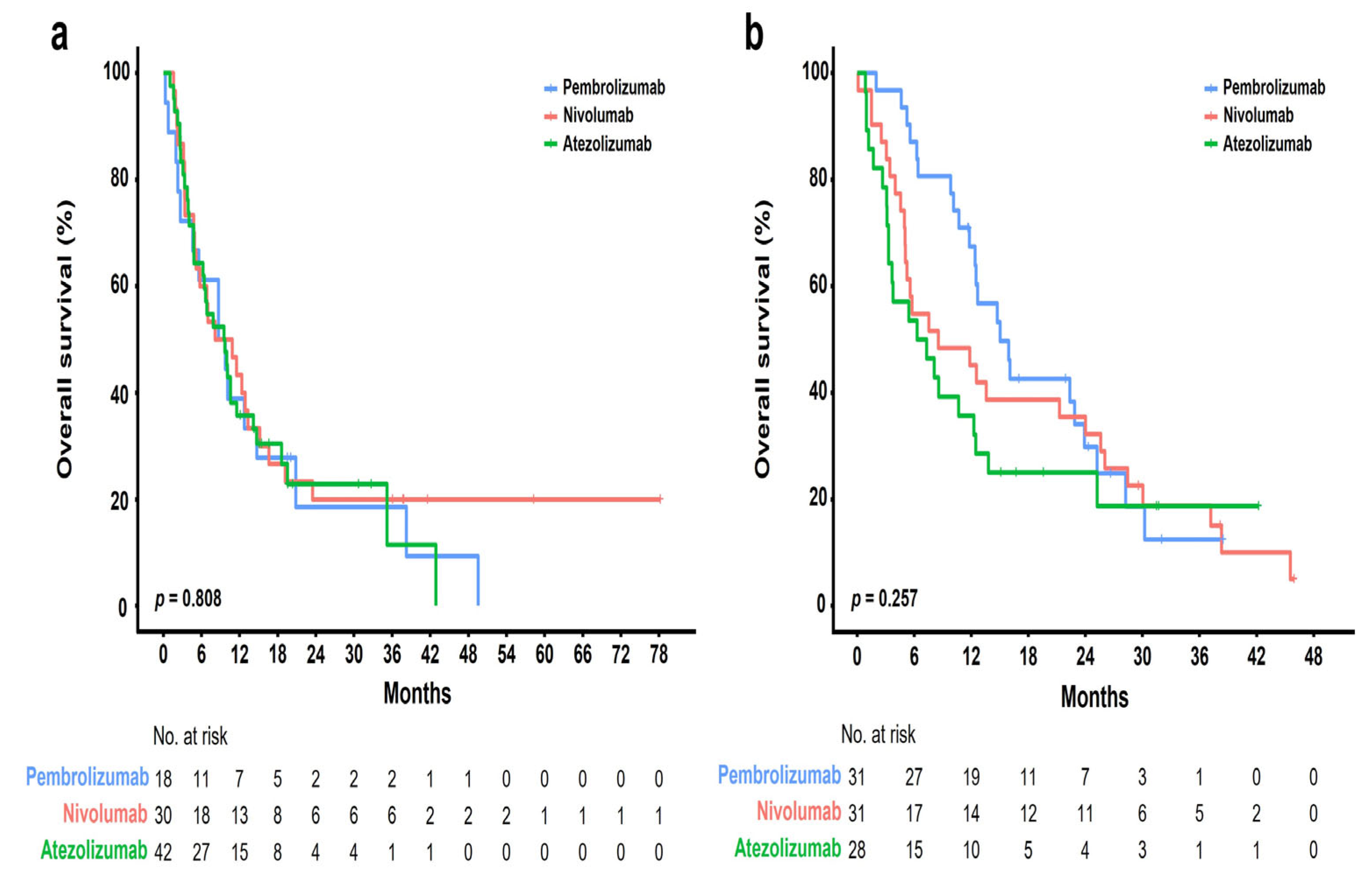
3.2. Treatment Outcomes
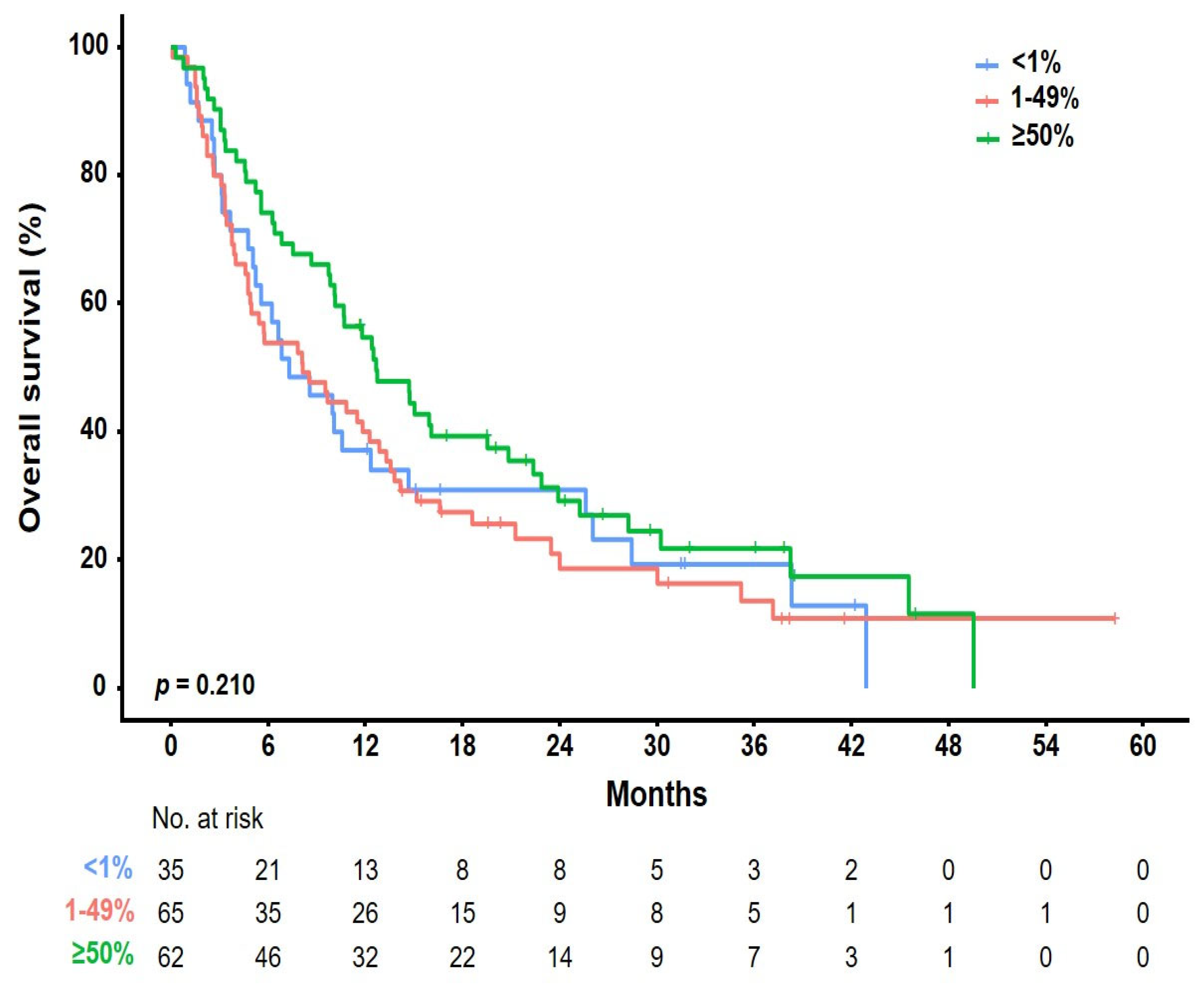
3.3. Prognostic Factors Affecting Overall Survival
3.4. Safety Outcomes
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Cancer Stat Facts Lung and Bronchus Cancer. Available online: https://seer.cancer.gov/statfacts/html/lungb.html (accessed on 1 January 2023).
- Osmani, L.; Askin, F.; Gabrielson, E.; Li, Q.K. Current who guidelines and the critical role of immunohistochemical markers in the subclassification of non-small cell lung carcinoma (nsclc): Moving from targeted therapy to immunotherapy. Semin. Cancer Biol. 2018, 52, 103–109. [Google Scholar] [CrossRef] [PubMed]
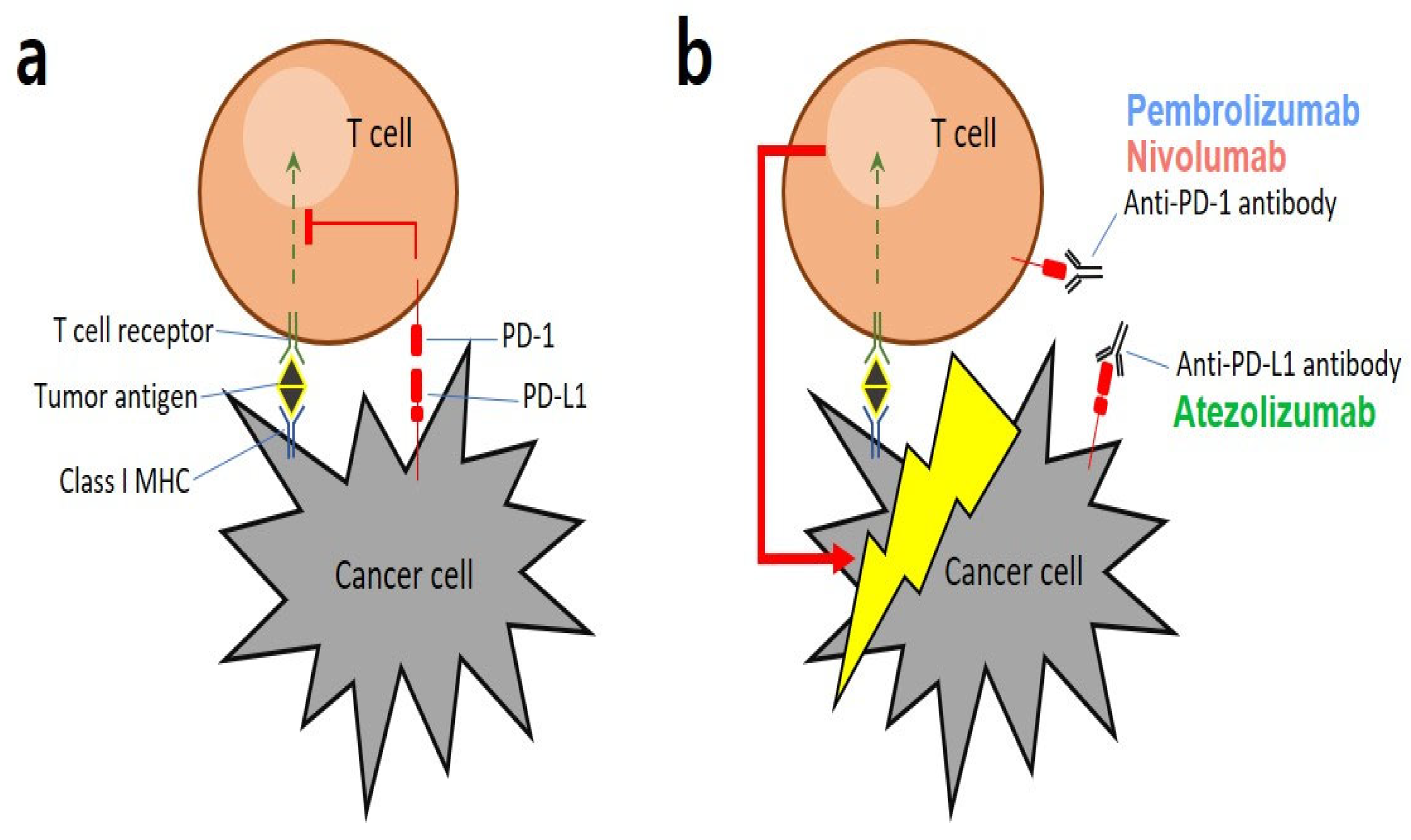
- Ai, L.; Xu, A.; Xu, J. Roles of pd-1/pd-l1 pathway: Signaling, cancer, and beyond. Adv. Exp. Med. Biol. 2020, 1248, 33–59. [Google Scholar] [CrossRef] [PubMed]
- Doroshow, D.B.; Sanmamed, M.F.; Hastings, K.; Politi, K.; Rimm, D.L.; Chen, L.; Melero, I.; Schalper, K.A.; Herbst, R.S. Immunotherapy in non-small cell lung cancer: Facts and hopes. Clin. Cancer Res. 2019, 25, 4592–4602. [Google Scholar] [CrossRef] [PubMed]
- Herbst, R.S.; Baas, P.; Kim, D.W.; Felip, E.; Pérez-Gracia, J.L.; Han, J.Y.; Molina, J.; Kim, J.H.; Arvis, C.D.; Ahn, M.J.; et al. Pembrolizumab versus docetaxel for previously treated, pd-l1-positive, advanced non-small-cell lung cancer (keynote-010): A randomised controlled trial. Lancet 2016, 387, 1540–1550. [Google Scholar] [CrossRef] [PubMed]
- Borghaei, H.; Gettinger, S.; Vokes, E.E.; Chow, L.Q.M.; Burgio, M.A.; de Castro Carpeno, J.; Pluzanski, A.; Arrieta, O.; Frontera, O.A.; Chiari, R.; et al. Five-year outcomes from the randomized, phase iii trials checkmate 017 and 057: Nivolumab versus docetaxel in previously treated non-small-cell lung cancer. J. Clin. Oncol. 2021, 39, 723–733. [Google Scholar] [CrossRef]
- Rittmeyer, A.; Barlesi, F.; Waterkamp, D.; Park, K.; Ciardiello, F.; von Pawel, J.; Gadgeel, S.M.; Hida, T.; Kowalski, D.M.; Dols, M.C.; et al. Atezolizumab versus docetaxel in patients with previously treated non-small-cell lung cancer (oak): A phase 3, open-label, multicentre randomised controlled trial. Lancet 2017, 389, 255–265. [Google Scholar] [CrossRef] [PubMed]
- Reck, M.; Rodríguez-Abreu, D.; Robinson, A.G.; Hui, R.; Csőszi, T.; Fülöp, A.; Gottfried, M.; Peled, N.; Tafreshi, A.; Cuffe, S.; et al. Pembrolizumab versus chemotherapy for pd-l1-positive non-small-cell lung cancer. N. Engl. J. Med. 2016, 375, 1823–1833. [Google Scholar] [CrossRef]
- Ettinger, D.S.; Wood, D.E.; Aisner, D.L.; Akerley, W.; Bauman, J.R.; Bharat, A.; Bruno, D.S.; Chang, J.Y.; Chirieac, L.R.; D’Amico, T.A.; et al. Nccn Guidelines Insights: Non-small Cell Lung Cancer, version 2.2021. J. Natl. Compr. Canc. Netw. 2021, 19, 254–266. [Google Scholar] [CrossRef]
- Marur, S.; Singh, H.; Mishra-Kalyani, P.; Larkins, E.; Keegan, P.; Sridhara, R.; Blumenthal, G.M.; Pazdur, R. Fda analyses of survival in older adults with metastatic non-small cell lung cancer in controlled trials of pd-1/pd-l1 blocking antibodies. Semin. Oncol. 2018, 45, 220–225. [Google Scholar] [CrossRef]
- Zhang, S.; Pease, D.F.; Kulkarni, A.A.; Kumar, M.; Shanley, R.M.; Xu, B.; Joshi, S.P.; Patel, M.R. Real-world outcomes and clinical predictors of immune checkpoint inhibitor monotherapy in advanced lung cancer. Clin. Med. Insights Oncol. 2021, 15, 11795549211004489. [Google Scholar] [CrossRef]
- Botticelli, A.; Salati, M.; Di Pietro, F.R.; Strigari, L.; Cerbelli, B.; Zizzari, I.G.; Giusti, R.; Mazzotta, M.; Mazzuca, F.; Roberto, M.; et al. A nomogram to predict survival in non-small cell lung cancer patients treated with nivolumab. J. Transl. Med. 2019, 17, 99. [Google Scholar] [CrossRef] [PubMed]
- Tamiya, M.; Tamiya, A.; Inoue, T.; Kimura, M.; Kunimasa, K.; Nakahama, K.; Taniguchi, Y.; Shiroyama, T.; Isa, S.I.; Nishino, K.; et al. Metastatic site as a predictor of nivolumab efficacy in patients with advanced non-small cell lung cancer: A retrospective multicenter trial. PLoS ONE 2018, 13, e0192227. [Google Scholar] [CrossRef]
- Schmid, S.; Diem, S.; Li, Q.; Krapf, M.; Flatz, L.; Leschka, S.; Desbiolles, L.; Klingbiel, D.; Jochum, W.; Früh, M. Organ-specific response to nivolumab in patients with non-small cell lung cancer (nsclc). Cancer Immunol. Immunother. 2018, 67, 1825–1832. [Google Scholar] [CrossRef] [PubMed]
- Passiglia, F.; Galvano, A.; Rizzo, S.; Incorvaia, L.; Listì, A.; Bazan, V.; Russo, A. Looking for the best immune-checkpoint inhibitor in pre-treated nsclc patients: An indirect comparison between nivolumab, pembrolizumab and atezolizumab. Int. J. Cancer 2018, 142, 1277–1284. [Google Scholar] [CrossRef] [PubMed]
- Eisenhauer, E.A.; Therasse, P.; Bogaerts, J.; Schwartz, L.H.; Sargent, D.; Ford, R.; Dancey, J.; Arbuck, S.; Gwyther, S.; Mooney, M.; et al. New response evaluation criteria in solid tumours: Revised RECIST guideline (version 1.1). Eur. J. Cancer 2009, 45, 228–247. [Google Scholar] [CrossRef] [PubMed]
- Casaluce, F.; Sgambato, A.; Maione, P.; Spagnuolo, A.; Gridelli, C. Lung cancer, elderly and immune checkpoint inhibitors. J. Thorac. Dis. 2018, 10 (Suppl. S13), S1474–S1481. [Google Scholar] [CrossRef] [PubMed]
- Tagliamento, M.; Frelaut, M.; Baldini, C.; Naigeon, M.; Nencioni, A.; Chaput, N.; Besse, B. The use of immunotherapy in older patients with advanced non-small cell lung cancer. Cancer Treat. Rev. 2022, 106, 102394. [Google Scholar] [CrossRef]
- Zeber, J.E.; Copeland, L.A.; Hosek, B.J.; Karnad, A.B.; Lawrence, V.A.; Sanchez-Reilly, S.E. Cancer rates, medical comorbidities, and treatment modalities in the oldest patients. Crit. Rev. Oncol. Hematol. 2008, 67, 237–242. [Google Scholar] [CrossRef]
- Burdett, N.; Vincent, A.D.; O’Callaghan, M.; Kichenadasse, G. Competing risks in older patients with cancer: A systematic review of geriatric oncology trials. J. Natl. Cancer Inst. 2018, 110, 825–830. [Google Scholar] [CrossRef]
- Mok, T.S.K.; Wu, Y.L.; Kudaba, I.; Kowalski, D.M.; Cho, B.C.; Turna, H.Z.; Castro, G., Jr.; Srimuninnimit, V.; Laktionov, K.K.; Bondarenko, I.; et al. Pembrolizumab versus chemotherapy for previously untreated, pd-l1-expressing, locally advanced or metastatic non-small-cell lung cancer (keynote-042): A randomised, open-label, controlled, phase 3 trial. Lancet 2019, 393, 1819–1830. [Google Scholar] [CrossRef]
- Jassem, J.; Herbst, R.S.; de Marinis, F.d.; Cadranel, J.; Csőszi, T.; Isla, D.; Chen, G.; Syrigos, K.N.; Cortinovis, D.; Hida, T.; et al. Impower110: Clinical safety in a phase III study of atezolizumab (atezo) monotherapy (mono) vs platinum-based chemotherapy (chemo) in first-line non-small cell lung cancer (NSCLC) [Mono. ]. J. Clin. Oncol. 2020, 38, e21623. [Google Scholar] [CrossRef]
- Stenehjem, D.D.; Lubinga, S.J.; Gupte-Singh, K.; Zhang, Y.; Le, T.K.; Penrod, J.R.; Smith, C.B. Real-world effectiveness of nivolumab monotherapy after prior systemic therapy in advanced non-small-cell lung cancer in the united states. Clin. Lung Cancer 2021, 22, e35–e47. [Google Scholar] [CrossRef] [PubMed]
- Morita, R.; Okishio, K.; Shimizu, J.; Saito, H.; Sakai, H.; Kim, Y.H.; Hataji, O.; Yomota, M.; Nishio, M.; Aoe, K.; et al. Real-world effectiveness and safety of nivolumab in patients with non-small cell lung cancer: A multicenter retrospective observational study in japan. Lung Cancer 2020, 140, 8–18. [Google Scholar] [CrossRef] [PubMed]
- Waterhouse, D.; Lam, J.; Betts, K.A.; Yin, L.; Gao, S.; Yuan, Y.; Hartman, J.; Rao, S.; Lubinga, S.; Stenehjem, D. Real-world outcomes of immunotherapy-based regimens in first-line advanced non-small cell lung cancer. Lung Cancer 2021, 156, 41–49. [Google Scholar] [CrossRef] [PubMed]
- Magee, D.E.; Hird, A.E.; Klaassen, Z.; Sridhar, S.S.; Nam, R.K.; Wallis, C.J.D.; Kulkarni, G.S. Adverse event profile for immunotherapy agents compared with chemotherapy in solid organ tumors: A systematic review and meta-analysis of randomized clinical trials. Ann. Oncol. 2020, 31, 50–60. [Google Scholar] [CrossRef]
- Botticelli, A.; Cirillo, A.; Scagnoli, S.; Cerbelli, B.; Strigari, L.; Cortellini, A.; Pizzuti, L.; Vici, P.; De Galitiis, F.; Di Pietro, F.R.; et al. The agnostic role of site of metastasis in predicting outcomes in cancer patients treated with immunotherapy. Vaccines 2020, 8, 203. [Google Scholar] [CrossRef]
- Zhao, E.; Xu, H.; Wang, L.; Kryczek, I.; Wu, K.; Hu, Y.; Wang, G.; Zou, W. Bone marrow and the control of immunity. Cell Mol. Immunol. 2012, 9, 11–19. [Google Scholar] [CrossRef] [PubMed]
- Landi, L.; D’Incà, F.; Gelibter, A.; Chiari, R.; Grossi, F.; Delmonte, A.; Passaro, A.; Signorelli, D.; Gelsomino, F.; Galetta, D.; et al. Bone metastases and immunotherapy in patients with advanced non-small-cell lung cancer. J. Immunother. Cancer 2019, 7, 316. [Google Scholar] [CrossRef]
- Yoneda, T.; Sone, T.; Koba, H.; Shibata, K.; Suzuki, J.; Tani, M.; Nishitsuji, M.; Nishi, K.; Kobayashi, T.; Shirasaki, H.; et al. Long-term survival of patients with non-small cell lung cancer treated with immune checkpoint inhibitor monotherapy in real-world settings. Clin. Lung Cancer 2022, 23, 467–476. [Google Scholar] [CrossRef]
- Velcheti, V.; Patwardhan, P.D.; Liu, F.X.; Chen, X.; Cao, X.; Burke, T. Real-world pd-l1 testing and distribution of pd-l1 tumor expression by immunohistochemistry assay type among patients with metastatic non-small cell lung cancer in the united states. PLoS ONE 2018, 13, e0206370. [Google Scholar] [CrossRef]
- Yuan, P.; Guo, C.Y.; Li, Y.; Jiang, L.L.; Liu, Y.P.; Liu, X.Y.; Ying, J.M. Consistency of pd-l1 immunohistochemical detection platforms in biopsy samples with advanced lung adenocarcinoma: A multicenter study. Zhonghua Bing Li Xue Za Zhi 2018, 47, 840–844. [Google Scholar] [CrossRef]
- Meserve, J.; Facciorusso, A.; Holmer, A.K.; Annese, V.; Sandborn, W.J.; Singh, S. Systematic review with meta-analysis: Safety and tolerability of immune checkpoint inhibitors in patients with pre-existing inflammatory bowel diseases. Aliment. Pharmacol. Ther. 2021, 53, 374–382. [Google Scholar]


{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Pembrolizumab (n = 49) | Nivolumab (n = 61) | Atezolizumab (n = 70) | Total (n = 180) | p-Value | ||
|---|---|---|---|---|---|---|
| Age | Median (IQR) | 75 (74–78) | 76 (74–78) | 76 (74–78) | 76 (74–78) | 0.635 † |
| Sex | Male | 48 (98.0%) | 60 (98.4%) | 69 (98.6%) | 177 (98.3%) | 0.967 * |
| Female | 1 (2.0%) | 1 (1.6%) | 1 (1.4%) | 3 (1.7%) | ||
| ECOG-PS | 0 or 1 | 46 (93.9%) | 60 (98.4%) | 67 (95.7%) | 173 (96.1%) | 0.437 * |
| 2 or 3 | 3 (6.1%) | 1 (1.6%) | 3 (4.3%) | 7 (3.9%) | ||
| Smoking | Current/Ex-smoker | 49 (100%) | 61 (100%) | 70 (100%) | 180 (100%) | |
| Histology | Squamous | 18 (36.7%) | 30 (49.2%) | 42 (60.0%) | 90 (50.0%) | 0.046 |
| Non-squamous | 31 (63.3%) | 31 (50.8%) | 28 (40.0%) | 90 (50.0%) | ||
| Line of therapy | 1st line | 8 (16.3%) | 0 (0%) | 0 (0%) | 8 (4.4%) | <0.001 * |
| 2nd line | 21 (42.9%) | 26 (42.6%) | 39 (55.7%) | 86 (47.8%) | ||
| ≥3rd line | 20 (40.8%) | 35 (57.4%) | 31 (44.3%) | 86 (47.8%) | ||
| PD-L1 expression § | <1% | 0 (0%) | 10 (16.4%) | 25 (35.7%) | 35 (19.4%) | <0.001 |
| 1–49% | 2 (4.1%) | 34 (55.7%) | 29 (41.4%) | 65 (36.1%) | ||
| ≥50% | 46 (93.9%) | 11 (18.0%) | 5 (7.1%) | 62 (34.4%) | ||
| Unknown ‡ | 1 (2.0%) | 6 (9.8%) | 11 (15.7%) | 18 (10.0%) | ||
| Metastatic sites | Liver metastasis | 6 (6.1%) | 2 (3.3%) | 3 (4.3%) | 8 (4.4%) | 0.816 * |
| Brain metastasis | 8 (16.3%) | 10 (16.4%) | 3 (4.3%) | 21 (11.7%) | 0.048 * | |
| Bone metastasis | 4 (8.2%) | 4 (6.6%) | 5 (7.1%) | 13 (7.2%) | 1.000 * | |
| Survival status | Ongoing | 10 (20.4%) | 9 (14.8%) | 15 (21.4%) | 34 (18.9%) | 0.592 |
| Death | 39 (79.6%) | 52 (85.2%) | 55 (78.6%) | 146 (81.1%) |
| Response n (%) [95% CI] | Pembrolizumab (n = 49) | Nivolumab (n = 61) | Atezolizumab (n = 70) | Total (n = 180) |
|---|---|---|---|---|
| CR | 0 | 0 | 0 | 0 |
| PR | 11 (22.4) [11.77–36.62] | 5 (8.2) [2.72–18.10] | 3 (4.3) [0.89–12.02] | 19 (10.6) [6.48–15.99] |
| SD | 18 (36.7) [23.42–51.71] | 29 (47.5) [34.60–60.73] | 18 (25.7) [16.01–37.56] | 65 (36.1) [29.10–43.59] |
| PD | 20 (40.8) [27.00–55.79] | 22 (36.1) [24.16–49.37] | 48 (68.6) [56.37–79.15] | 90 (50.0) [42.47–57.53] |
| NA § | 0 | 5 (8.2) [2.72–18.10] | 1 (1.4) [0.04–7.70] | 6 (3.3) [1.23–7.11] |
| ORR | 11 (22.4) [11.77–36.62] | 5 (8.2) [2.72–18.10] | 3 (4.3) [0.89–12.02] | 19 (10.6) [6.48–15.99] |
| DCR | 29 (59.2) [44.21–73.00] | 34 (55.7) [42.45–68.45] | 21 (30.0) [19.62–42.13] | 84 (46.7) [39.21–52.24] |
| Event/Total ‡ (146/180) | Univariate HR (95% CI) | Univariate p-Value | Multivariate HR § (95% CI) | Multivariate p-Value | ||
|---|---|---|---|---|---|---|
| Age | 146/180 | 1.01 (0.98–1.04) | 0.369 | |||
| Gender | Male | 143/177 | 1 | |||
| Female | 3/3 | 1.70 (0.54–5.36) | 0.365 | |||
| ECOG-PS | 0 or 1 | 140/173 | 1 | |||
| 2 or 3 | 6/7 | 0.92 (0.40–2.08) | 0.834 | |||
| Histology | Squamous | 73/90 | 1 | |||
| Non-squamous | 73/90 | 0.90 (0.65–1.24) | 0.528 | |||
| PD-L1 | <1% | 29/35 | 1 | |||
| 1–49% | 54/65 | 1.04 (0.66–1.64) | 0.859 | 1.12 (0.71–1.77) | 0.635 | |
| ≥50% | 48/62 | 0.76 (0.48–1.20) | 0.241 | 0.73 (0.46–1.16) | 0.179 | |
| Missing † | 15/18 | |||||
| Treatment | Atezolizumab | 55/70 | 1 | |||
| Pembrolizumab | 39/49 | 0.75 (0.50–1.14) | 0.179 | |||
| Nivolumab | 52/61 | 0.84 (0.57–1.23) | 0.361 | |||
| Liver meta | No | 141/172 | 1 | |||
| Yes | 5/8 | 0.90 (0.37–2.21) | 0.826 | |||
| Brain meta | No | 130/159 | 1 | |||
| Yes | 16/21 | 0.97 (0.58–1.64) | 0.915 | 0.61 (0.32–1.17) | 0.136 | |
| Bone meta | No | 135/167 | 1 | |||
| Yes | 11/13 | 1.83 (0.99–3.39) | 0.056 | 2.75 (1.31–5.76) | 0.007 |
| n of Events (%) | Pembrolizumab (n = 49) | Nivolumab (n = 61) | Atezolizumab (n = 70) | |||
|---|---|---|---|---|---|---|
| Any Grade | Grade ≥ 3 | Any Grade | Grade ≥ 3 | Any Grade | Grade ≥ 3 | |
| Fatigue | 4 (8.2) | 0 | 2 (3.3) | 0 | 5 (7.1) | 0 |
| Anorexia | 3 (6.1) | 0 | 6 (8.2) | 0 | 3 (4.2) | 0 |
| Oral mucositis | 0 | 0 | 1 (1.6) | 0 | 0 | 0 |
| Diarrhea * | 0 | 0 | 0 | 0 | 1 (1.4) | 0 |
| Skin rash * | 5 (10.2) | 0 | 3 (4.9) | 0 | 2 (2.8) | 0 |
| Pneumonitis * | 1 (2.0) | 1 (2.0) | 1 (1.6) | 0 | 4 (5.7) | 2 (2.8) |
| Hepatotoxicity * | 1 (2.0) | 0 | 0 | 0 | 0 | 0 |
| Thyroid dysfunction * | 2 (4.1) | 0 | 2 (3.3) | 0 | 2 (2.9) | 0 |
| Study | Agents | Line | Histology % | Patients n | Age, Median (Range) | ECOG ≥ 2 n (%) | PD-L1 Score (%) | PFS (Months) | OS (Months) | ORR (%) |
|---|---|---|---|---|---|---|---|---|---|---|
| KN-010 | Pembro | ≥2 | Sq: 22 Non-sq: 70 Other: 3 | 344 | 63 (56–69) | 3 (1) | ≥50 | 3.9 | 14.9 | 21.2 |
| KN-024 | Pembro | 1 | Sq: 18.8 Non-sq: 81.2 | 154 | 65 (33–90) | 0 | ≥50 | 10.3 | 30 | 20.7 |
| KN-042 [21] | Pembro | 1 | Sq: 38 Non-sq: 62 | 637 | 63 (57–69) | 0 | ≥1 | 7.1 | 20 | 27.3 |
| CM 017 | Nivo | ≥2 | Squamous | 135 | 62 (39–85) | 2 (1.5) | ≥10 | 3.5 | 9.2 | 20 |
| CM 057 | Nivo | ≥2 | Non-sq | 292 | 61 (37–84) | 0 | ≥10 | 2.3 | 12.2 | 19 |
| OAK | Atezo | ≥2 | Sq: 26 Non-sq: 74 | 425 | 63 (33–82) | 0 | All-comer | 2.8 | 13.8 | 14 |
| IMpower 110 [22] | Atezo | 1 | Sq: 25 Non-sq: 75 | 107 | 64 (33–79) | 0 | ≥50 or (IC ≥ 10) | 8.1 | 20 | 40.2 |
| Current study | Overall | ≥1 | Sq: 50 Non-Sq: 50 | 180 | 76 (74–78) | 7 (3.9) | All-comer | nr | 10 | 10.6 |
| Pembro Nivo Atezo | 49 61 70 | 75 (74–78) 76 (74–78) 76 (74–78) | 3 (6.1) 1 (1.6) 3 (4.3) | 12.6 8.4 7.7 | 22.4 8.2 4.3 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Ham, A.; Lee, Y.; Kim, H.S.; Lim, T. Real-World Outcomes of Nivolumab, Pembrolizumab, and Atezolizumab Treatment Efficacy in Korean Veterans with Stage IV Non-Small-Cell Lung Cancer. Cancers 2023, 15, 4198. https://doi.org/10.3390/cancers15164198
Ham A, Lee Y, Kim HS, Lim T. Real-World Outcomes of Nivolumab, Pembrolizumab, and Atezolizumab Treatment Efficacy in Korean Veterans with Stage IV Non-Small-Cell Lung Cancer. Cancers. 2023; 15(16):4198. https://doi.org/10.3390/cancers15164198
Chicago/Turabian StyleHam, Ahrong, Young Lee, Hae Su Kim, and Taekyu Lim. 2023. "Real-World Outcomes of Nivolumab, Pembrolizumab, and Atezolizumab Treatment Efficacy in Korean Veterans with Stage IV Non-Small-Cell Lung Cancer" Cancers 15, no. 16: 4198. https://doi.org/10.3390/cancers15164198
APA StyleHam, A., Lee, Y., Kim, H. S., & Lim, T. (2023). Real-World Outcomes of Nivolumab, Pembrolizumab, and Atezolizumab Treatment Efficacy in Korean Veterans with Stage IV Non-Small-Cell Lung Cancer. Cancers, 15(16), 4198. https://doi.org/10.3390/cancers15164198