

Sentinel Lymph Node Mapping in Presumed Low- and Intermediate-Risk Endometrial Cancer Management (SLIM): A Multicenter, Prospective Cohort Study in The Netherlands

 , ,
, ,  and
and
Abstract
Simple Summary
Abstract
1. Introduction
2. Materials and Methods
2.1. Study Design
2.2. Statistical Analyses
3. Results
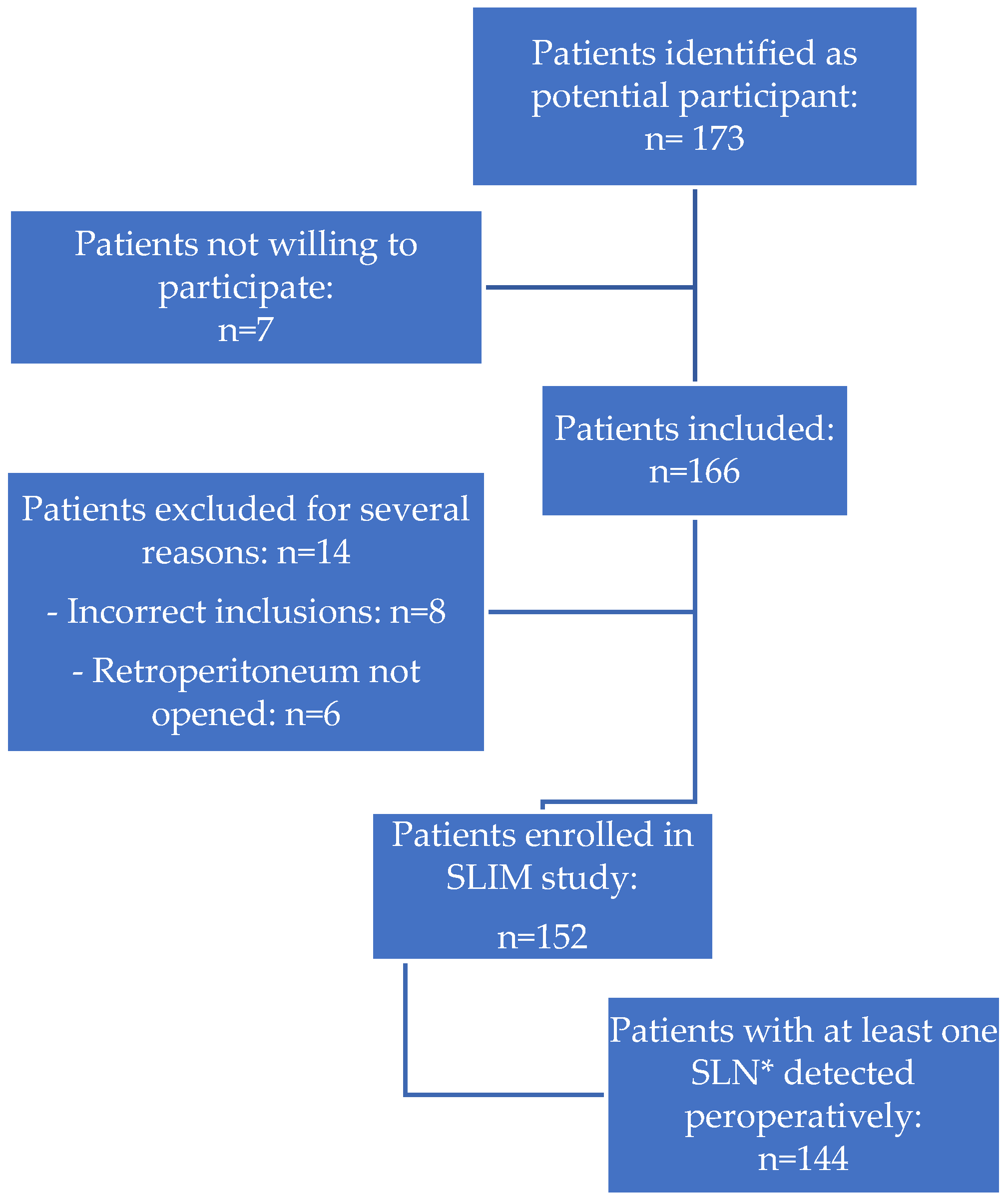
3.1. Detection Rate of SLN Mapping
3.2. Incidence of SLN Metastases
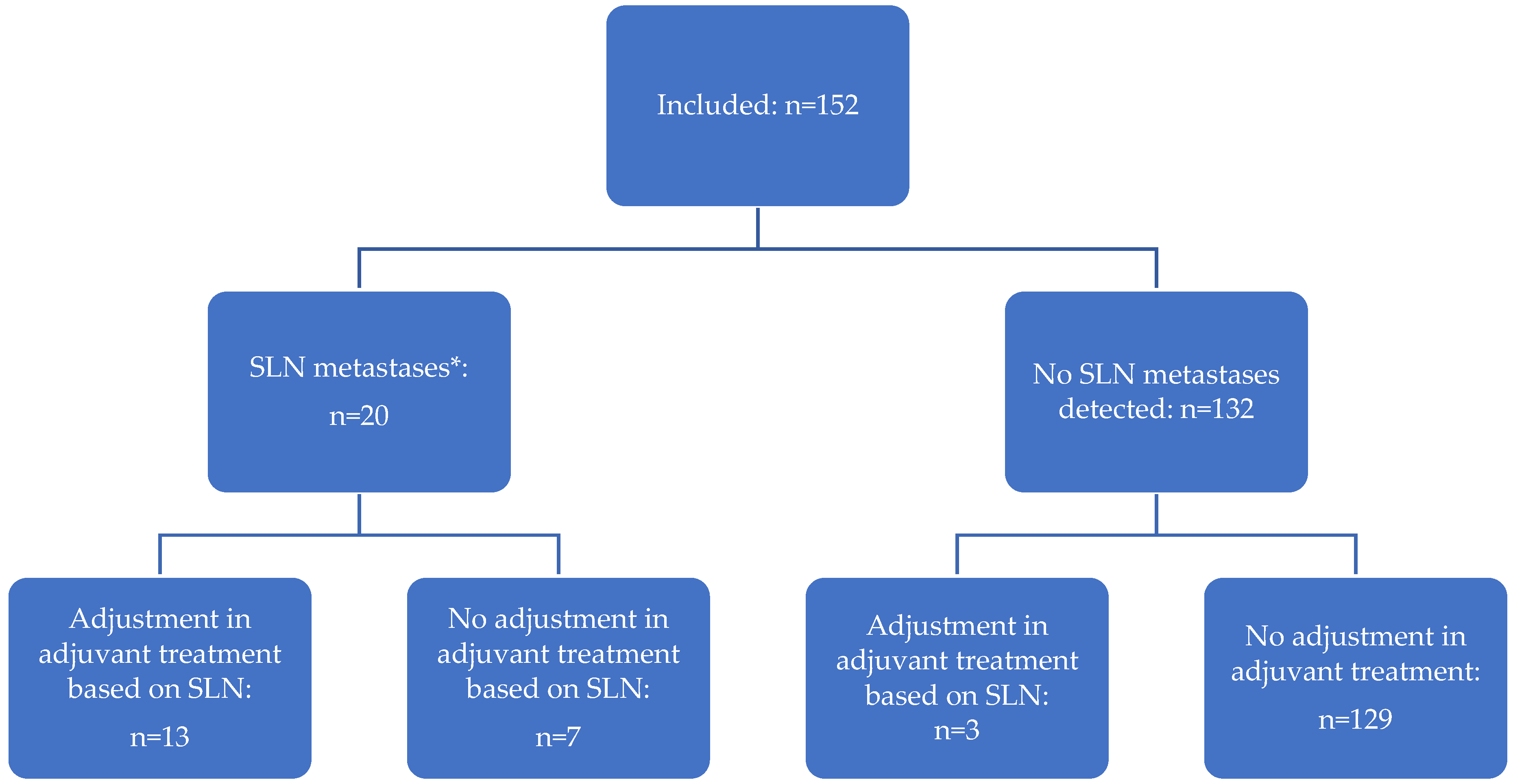
3.3. Adjusting Adjuvant Management Based on Lymph Node Status
3.4. Complications of SLN Mapping
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Federatie Medisch Specialisten, Integraal Kankercentrum Nederland. Richtlijnendatabase: Richtlijn Endometriumcarcinoom. 2011. Available online: https://richtlijnendatabase.nl/richtlijn/endometriumcarcinoom/endometriumcarcinoom_-_startpagina.html (accessed on 1 July 2022).
- Koskas, M.; Rouzier, R.; Amant, F. Staging for endometrial cancer: The controversy around lymphadenectomy-Can this be resolved? Best Pract. Res. Clin. Obstet. Gynaecol. 2015, 29, 845–857. [Google Scholar] [CrossRef]
- Abdullah, N.A.; Huang, K.; Casanova, J.; Artazcoz, S.; Jarruwale, P.; Benavides, D.R.; Lee, C. Sentinel lymph node in endometrial cancer: A systematic review on laparoscopic detection. Gynecol. Minim. Invasive Ther. 2013, 2, 75–78. [Google Scholar] [CrossRef]
- Lewin, S.N.; Herzog, T.J.; Barrena Medel, N.I.; Deutsch, I.; Burke, W.M.; Sun, X.; Wright, J.D. Comparative performance of the 2009 international Federation of gynecology and obstetrics’ staging system for uterine corpus cancer. Obstet. Gynecol. 2010, 116, 1141–1149. [Google Scholar] [CrossRef] [PubMed]
- Tejerizo-García, A.; Jiménez-López, J.S.; Muñoz-González, J.L.; Bartolomé-Sotillos, S.; Marqueta-Marqués, L.; López-González, G.; Gómez, J.F. Overall survival and disease-free survival in endometrial cancer: Prognostic factors in 276 patients. OncoTargets Ther. 2013, 9, 1305–1313. [Google Scholar] [PubMed]
- Lurain, J.R.; Rice, B.L.; Rademaker, A.W.; Poggensee, L.E.; Schink, J.C.; Miller, D.S. Prognostic factors associated with recurrence in clinical stage I adenocarcinoma of the endometrium. Obstet. Gynecol. 1991, 78, 63–69. [Google Scholar]
- Holloway, R.W.; Abu-Rustum, N.R.; Backes, F.J.; Boggess, J.F.; Gotlieb, W.H.; Jeffrey Lowery, W.; Rossi, E.C.; Tanner, E.J.; Wolsky, R.J. Sentinel lymph node mapping and staging in endometrial cancer: A Society of Gynecologic Oncology literature review with consensus recommendations. Gynecol. Oncol. 2017, 146, 405–415. [Google Scholar] [CrossRef]
- Koh, W.J.; Abu-Rustum, N.R.; Bean, S.; Bradley, K.; Campos, S.M.; Cho, K.R.; Chon, H.S.; Chu, C.; Cohn, D.; Crispens, M.A.; et al. Uterine Neoplasms, Version 1.2018, NCCN Clinical Practice Guidelines in Oncology. J. Natl. Compr. Cancer Netw. 2018, 16, 170–199. [Google Scholar] [CrossRef]
- Ballester, M.; Bendifallah, S.; Daraï, E. European guidelines (ESMO-ESGO-ESTRO consensus conference) for the management of endometrial cancer. Bull. Cancer 2017, 104, 1032–1038. [Google Scholar] [CrossRef]
- Clark, L.H.; Soper, J.T. Endometrial Cancer and the Role of Lymphadenectomy. Obstet. Gynecol. Surv. 2016, 71, 353–360. [Google Scholar] [CrossRef]
- Frost, J.A.; Webster, K.E.; Bryant, A.; Morrison, J. Lymphadenectomy for the management of endometrial cancer. Cochrane Database Syst. Rev. 2017, 10, Cd007585. [Google Scholar] [CrossRef]
- Abu-Rustum, N.R.; Alektiar, K.; Iasonos, A.; Lev, G.; Sonoda, Y.; Aghajanian, C.; Chi, D.S.; Barakat, R.R. The incidence of symptomatic lower-extremity lymphedema following treatment of uterine corpus malignancies: A 12-year experience at Memorial Sloan-Kettering Cancer Center. Gynecol. Oncol. 2006, 103, 714–718. [Google Scholar] [CrossRef]
- Cardosi, R.J.; Cox, C.S.; Hoffman, M.S. Postoperative neuropathies after major pelvic surgery. Obstet. Gynecol. 2002, 100, 240–244. [Google Scholar] [CrossRef]
- Kitchener, H.; Swart, A.M.; Qian, Q.; Amos, C.; Parmar, M.K. Efficacy of systematic pelvic lymphadenectomy in endometrial cancer (MRC ASTEC trial): A randomised study. Lancet 2009, 373, 125–136. [Google Scholar]
- Panici, P.B.; Basile, S.; Maneschi, F.; Lissoni, A.A.; Signorelli, M.; Scambia, G.; Angioli, R.; Tateo, S.; Mangili, G.; Katsaros, D.; et al. Systematic pelvic lymphadenectomy vs. no lymphadenectomy in early-stage endometrial carcinoma: Randomized clinical trial. J. Natl. Cancer Inst. 2008, 100, 1707–1716. [Google Scholar] [CrossRef]
- de Boer, S.M.; Powell, M.E.; Mileshkin, L.; Katsaros, D.; Bessette, P.; Haie-Meder, C.; Ottevanger, P.B.; Ledermann, J.A.; Khaw, P.; D’Amico, R.; et al. Adjuvant chemoradiotherapy versus radiotherapy alone in women with high-risk endometrial cancer (PORTEC-3): Patterns of recurrence and post-hoc survival analysis of a randomised phase 3 trial. Lancet Oncol. 2019, 20, 1273–1285. [Google Scholar] [CrossRef]
- Matei, D.; Filiaci, V.; Randall, M.E.; Mutch, D.; Steinhoff, M.M.; DiSilvestro, P.A.; Moxley, K.M.; Kim, Y.M.; Powell, M.A.; O’Malley, D.M.; et al. Adjuvant Chemotherapy plus Radiation for Locally Advanced Endometrial Cancer. N. Engl. J. Med. 2019, 380, 2317–2326. [Google Scholar] [CrossRef]
- Hogberg, T. Adjuvant chemotherapy in endometrial cancer. Int. J. Gynecol. Cancer 2010, 20 (Suppl. 2), S57–S59. [Google Scholar] [CrossRef]
- Bodurtha Smith, A.J.; Fader, A.N.; Tanner, E.J. Sentinel lymph node assessment in endometrial cancer: A systematic review and meta-analysis. Am. J. Obstet. Gynecol. 2017, 216, 459–476.e10. [Google Scholar] [CrossRef]
- How, J.A.; O’Farrell, P.; Amajoud, Z.; Lau, S.; Salvador, S.; How, E.; Gotlieb, W.H. Sentinel lymph node mapping in endometrial cancer: A systematic review and meta-analysis. Minerva Ginecol. 2018, 70, 194–214. [Google Scholar] [CrossRef]
- Obermair, H.M.; O’Hara, M.; Obermair, A.; Janda, M. Paucity of data evaluating patient centred outcomes following sentinel lymph node dissection in endometrial cancer: A systematic review. Gynecol. Oncol. Rep. 2021, 36, 100763. [Google Scholar] [CrossRef]
- Bogani, G.; Murgia, F.; Ditto, A.; Raspagliesi, F. Sentinel node mapping vs. lymphadenectomy in endometrial cancer: A systematic review and meta-analysis. Gynecol. Oncol. 2019, 153, 676–683. [Google Scholar] [CrossRef]
- Plante, M.; Stanleigh, J.; Renaud, M.C.; Sebastianelli, A.; Grondin, K.; Grégoire, J. Isolated tumor cells identified by sentinel lymph node mapping in endometrial cancer: Does adjuvant treatment matter? Gynecol. Oncol. 2017, 146, 240–246. [Google Scholar] [CrossRef] [PubMed]
- Jewell, E.L.; Huang, J.J.; Abu-Rustum, N.R.; Gardner, G.J.; Brown, C.L.; Sonoda, Y.; Barakat, R.R.; Levine, D.A.; Leitao, M.M. Detection of sentinel lymph nodes in minimally invasive surgery using indocyanine green and near-infrared fluorescence imaging for uterine and cervical malignancies. Gynecol. Oncol. 2014, 133, 274–277. [Google Scholar] [CrossRef] [PubMed]
- Concin, N.; Matias-Guiu, X.; Vergote, I.; Cibula, D.; Mirza, M.R.; Marnitz, S.; Ledermann, J.; Bosse, T.; Chargari, C.; Fagotti, A.; et al. ESGO/ESTRO/ESP guidelines for the management of patients with endometrial carcinoma. Int. J. Gynecol. Cancer 2020, 31, 12–39. [Google Scholar] [CrossRef] [PubMed]
- Abu-Rustum, N.R. Update on sentinel node mapping in uterine cancer: 10-year experience at Memorial Sloan-Kettering Cancer Center. J. Obstet. Gynaecol. Res. 2014, 40, 327–334. [Google Scholar] [CrossRef] [PubMed]
- Chi, D.S.; Barakat, R.R.; Palayekar, M.J.; Levine, D.A.; Sonoda, Y.; Alektiar, K.; Brown, C.L.; Abu-Rustum, N.R. The incidence of pelvic lymph node metastasis by FIGO staging for patients with adequately surgically staged endometrial adenocarcinoma of endometrioid histology. Int. J. Gynecol. Cancer 2008, 18, 269–273. [Google Scholar] [CrossRef]
- Canlorbe, G.; Bendifallah, S.; Laas, E.; Raimond, E.; Graesslin, O.; Hudry, D.; Coutant, C.; Touboul, C.; Bleu, G.; Collinet, P.; et al. Tumor Size, an Additional Prognostic Factor to Include in Low-Risk Endometrial Cancer: Results of a French Multicenter Study. Ann. Surg. Oncol. 2016, 23, 171–177. [Google Scholar] [CrossRef]
- Creasman, W.T.; Morrow, C.P.; Bundy, B.N.; Homesley, H.D.; Graham, J.E.; Heller, B. Surgical pathologic spread patterns of endometrial cancer. A Gynecologic Oncology Group Study. Cancer 1987, 60 (Suppl. 8), 2035–2041. [Google Scholar] [CrossRef]
- Masubuchi, S.; Fujimoto, I.; Masubuchi, K. Lymph node metastasis and prognosis of endometrial carcinoma. Gynecol. Oncol. 1979, 7, 36–46. [Google Scholar] [CrossRef]
- Boronow, R.C.; Morrow, C.P.; Creasman, W.T.; Disaia, J.; Silverberg, S.G.; Miller, A.; Blessing, J.A. Surgical staging in endometrial cancer: Clinical-pathologic findings of a prospective study. Obstet. Gynecol. 1984, 63, 825–832. [Google Scholar]
- Milam, M.R.; Java, J.; Walker, J.L.; Metzinger, D.S.; Parker, L.P.; Coleman, R.L. Nodal metastasis risk in endometrioid endometrial cancer. Obstet. Gynecol. 2012, 119 Pt 1, 286–292. [Google Scholar] [CrossRef]
- Visser, N.C.M.; Reijnen, C.; Massuger, L.; Nagtegaal, I.D.; Bulten, J.; Pijnenborg, J.M.A. Accuracy of Endometrial Sampling in Endometrial Carcinoma: A Systematic Review and Meta-analysis. Obstet. Gynecol. 2017, 130, 803–813. [Google Scholar] [CrossRef]
- Moloney, K.; Janda, M.; Frumovitz, M.; Leitao, M.; Abu-Rustum, N.R.; Rossi, E.; Nicklin, J.L.; Plante, M.; Lecuru, F.R.; Buda, A.; et al. Development of a surgical competency assessment tool for sentinel lymph node dissection by minimally invasive surgery for endometrial cancer. Int. J. Gynecol. Cancer 2021, 31, 647–655. [Google Scholar] [CrossRef]
- Nout, R.A.; Smit, V.T.; Putter, H.; Jürgenliemk-Schulz, I.M.; Jobsen, J.J.; Lutgens, L.C.; van der Steen-Banasik, E.M.; Mens, J.W.; Slot, A.; Kroese, M.C.; et al. Vaginal brachytherapy versus pelvic external beam radiotherapy for patients with endometrial cancer of high-intermediate risk (PORTEC-2): An open-label, non-inferiority, randomised trial. Lancet 2010, 375, 816–823. [Google Scholar] [CrossRef]
- van den Heerik, A.; Horeweg, N.; Nout, R.A.; van der Steen-Banasik, E.M.L.L.; Westerveld, G.H.; van den Berg, H.A.; Slot, A.; Koppe FL, A.; Kommoss, S. PORTEC-4a: International randomized trial of molecular profile-based adjuvant treatment for women with high-intermediate risk endometrial cancer. Int. J. Gynecol. Cancer 2020, 30, 2002–2007. [Google Scholar] [CrossRef]
- Burg, L.C.; Vermeulen, R.J.; Bekkers RL, M.; Wijn SR, W.; Rovers, M.M.; Govers, T.M.; Zusterzeel, L.M. A cost-effectiveness analysis of three approaches for lymph node assessment in patients with low- and intermediate-risk endometrial cancer. Gynecol. Oncol. 2021, 161, 251–260. [Google Scholar] [CrossRef]
- Aarts, J.W.M.; Burg, L.C.; Kasius, J.C.; Groenewoud, H.; A Kraayenbrink, A.; Stalmeier, P.; Zusterzeel, P.L.M. Patients’ and gynecologists’ views on sentinel lymph node mapping in low- and intermediate-risk endometrial cancer: A Dutch vignette study. Int. J. Gynecol. Cancer 2020, 30, 813–818. [Google Scholar] [CrossRef]
- Paydar, I.; DeWees, T.; Powell, M.; Mutch, D.G.; Grigsby, W.; Schwarz, J.K. Adjuvant radiotherapy in Stage II endometrial carcinoma: Is brachytherapy alone sufficient for local control? Brachytherapy 2015, 14, 427–432. [Google Scholar] [CrossRef]
- Khoury-Collado, F.; St Clair, C.; Abu-Rustum, N.R. Sentinel Lymph Node Mapping in Endometrial Cancer: An Update. Oncologist 2016, 21, 461–466. [Google Scholar] [CrossRef]
- Sullivan, S.A.; Rossi, E.C. Sentinel Lymph Node Biopsy in Endometrial Cancer: A New Standard of Care? Curr. Treat. Options Oncol. 2017, 18, 62. [Google Scholar] [CrossRef]
- Rossi, E.C.; Kowalski, L.D.; Scalici, J.; Cantrell, L.; Schuler, K.; Hanna, R.K.; Method, M.; Ade, M.; Ivanova, A.; Boggess, J.F. A comparison of sentinel lymph node biopsy to lymphadenectomy for endometrial cancer staging (FIRES trial): A multicentre, prospective, cohort study. Lancet Oncol. 2017, 18, 384–392. [Google Scholar] [CrossRef] [PubMed]
- Geppert, B.; Lönnerfors, C.; Bollino, M.; Persson, J. Sentinel lymph node biopsy in endometrial cancer-Feasibility, safety and lymphatic complications. Gynecol. Oncol. 2018, 148, 491–498. [Google Scholar] [CrossRef] [PubMed]
- Restaino, S.; Buda, A.; Puppo, A.; Capozzi, V.A.; Sozzi, G.; Casarin, J.; Gallitelli, V.; Murgia, F.; Vizzielli, G.; Baroni, A.; et al. Anatomical distribution of sentinel lymph nodes in patients with endometrial cancer: A multicenter study. Int. J. Gynecol. Cancer 2022, 32, 517–524. [Google Scholar] [CrossRef] [PubMed]
- Marchocki, Z.; Cusimano, M.C.; Clarfield, L.; Kim, S.R.; Fazelzad, R.; Espin-Garcia, O.; Bouchard-Fortier, G.; Rossi, E.C.; Stewart, K.I.; Soliman, T.; et al. Sentinel lymph node biopsy in high-grade endometrial cancer: A systematic review and meta-analysis of performance characteristics. Am. J. Obstet. Gynecol. 2021, 225, e1–e367. [Google Scholar] [CrossRef] [PubMed]
- Holloway, R.W.; Gupta, S.; Stavitzski, N.M.; Zhu, X.; Takimoto, E.L.; Gubbi, A.; Bigsby, G.E.; Brudie, L.A.; Kendrick, J.E.; Ahmad, S. Sentinel lymph node mapping with staging lymphadenectomy for patients with endometrial cancer increases the detection of metastasis. Gynecol. Oncol. 2016, 141, 206–210. [Google Scholar] [CrossRef]
- Raimond, E.; Ballester, M.; Hudry, D.; Bendifallah, S.; Daraï, E.; Graesslin, O.; Coutant, C. Impact of sentinel lymph node biopsy on the therapeutic management of early-stage endometrial cancer: Results of a retrospective multicenter study. Gynecol. Oncol. 2014, 133, 506–511. [Google Scholar] [CrossRef]
- Tucker, K.; Staley, S.A.; Gehrig, A.; Soper, J.T.; Boggess, J.F.; Ivanova, A.; Rossi, E. Defining the learning curve for successful staging with sentinel lymph node biopsy for endometrial cancer among surgeons at an academic institution. Int. J. Gynecol. Cancer 2020, 30, 346–351. [Google Scholar] [CrossRef]
- Kim, S.; Ryu, K.J.; Min, K.J.; Lee, S.; Jung, U.S.; Hong, J.H.; Song, J.Y.; Lee, J.K.; Lee, N.W. Learning curve for sentinel lymph node mapping in gynecologic malignancies. J. Surg. Oncol. 2020, 121, 599–604. [Google Scholar] [CrossRef]
- Thomaier, L.; Jager, L.; Stone, R.; Wethington, S.; Fader, A.; Tanner, E.J. Risk of empty lymph node packets in sentinel lymph node mapping for endometrial cancer using indocyanine green. Int. J. Gynecol. Cancer 2019, 29, 513–517. [Google Scholar] [CrossRef]
- Zorzato, P.C.; Bosco, M.; Franchi, M.P.; Mariani, A.; Cianci, S.; Garzon, S.; Uccella, S. Sentinel lymph node for endometrial cancer treatment: Review of the literature. Minerva Med. 2021, 112, 70–80. [Google Scholar] [CrossRef]
- de Boer, M.; van Deurzen, C.H.; van Dijck, J.A.; Borm, G.F.; van Diest, J.; Adang, E.M.; Nortier, J.W.; Rutgers, E.J.; Seynaeve, C.; Menke-Pluymers, M.B.; et al. Micrometastases or isolated tumor cells and the outcome of breast cancer. N. Engl. J. Med. 2009, 361, 653–663. [Google Scholar] [CrossRef]
- Weixler, B.; Warschkow, R.; Güller, U.; Zettl, A.; von Holzen, U.; Schmied, B.M.; Zuber, M. Isolated tumor cells in stage I & II colon cancer patients are associated with significantly worse disease-free and overall survival. BMC Cancer 2016, 16, 106. [Google Scholar]
- Scheri, R.P.; Essner, R.; Turner, R.R.; Ye, X.; Morton, D.L. Isolated tumor cells in the sentinel node affect long-term prognosis of patients with melanoma. Ann. Surg. Oncol. 2007, 14, 2861–2866. [Google Scholar] [CrossRef]
- Bogani, G.; Mariani, A.; Paolini, B.; Ditto, A.; Raspagliesi, F. Low-volume disease in endometrial cancer: The role of micrometastasis and isolated tumor cells. Gynecol. Oncol. 2019, 153, 670–675. [Google Scholar] [CrossRef]
- Todo, Y.; Kato, H.; Okamoto, K.; Minobe, S.; Yamashiro, K.; Sakuragi, N. Isolated tumor cells and micrometastases in regional lymph nodes in stage I to II endometrial cancer. J. Gynecol. Oncol. 2016, 27, e1. [Google Scholar] [CrossRef]
- Casarin, J.; Multinu, F.; Abu-Rustum, N.; Cibula, D.; A Cliby, W.; Ghezzi, F.; Leitao, M.; Konishi, I.; Nam, J.-H.; Querleu, D.; et al. Factors influencing the adoption of the sentinel lymph node technique for endometrial cancer staging: An international survey of gynecologic oncologists. Int. J. Gynecol. Cancer 2019, 29, 60–67. [Google Scholar] [CrossRef]
- Skanjeti, A.; Dhomps, A.; Paschetta, C.; Tordo, J.; Giammarile, F. Sentinel Node Mapping in Gynecologic Cancers: A Comprehensive Review. Semin Nucl. Med. 2019, 49, 521–533. [Google Scholar] [CrossRef]
- How, J.; Gauthier, C.; Abitbol, J.; Lau, S.; Salvador, S.; Gotlieb, R.; Pelmus, M.; Ferenczy, A.; Probst, S.; Brin, S.; et al. Impact of sentinel lymph node mapping on recurrence patterns in endometrial cancer. Gynecol. Oncol. 2017, 144, 503–509. [Google Scholar] [CrossRef]
- Obermair, A.; Nicklin, J.; Gebski, V.; Hayes, S.C.; Graves, N.; Mileshkin, L.; Lin, M.Y.; Beale, P.; Baxter, E.; Robledo, K.; et al. A phase III randomized clinical trial comparing sentinel node biopsy with no retroperitoneal node dissection in apparent early-stage endometrial cancer-ENDO-3: ANZGOG trial 1911/2020. Int. J. Gynecol. Cancer 2021, 31, 1595–1601. [Google Scholar] [CrossRef]
- Grassi, T.; Mariani, A.; Cibula, D.; Soliman, T.; Suman, V.J.; Weaver, A.L.; Pedra Nobre, S.; Weigelt, B.; Glaser, G.E.; Cappuccio, S.; et al. A prospective multicenter international single-arm observational study on the oncological safety of the sentinel lymph node algorithm in stage I intermediate-risk endometrial cancer (SELECT, SEntinel Lymph node Endometrial Cancer Trial). Int. J. Gynecol. Cancer 2020, 30, 1627–1632. [Google Scholar] [CrossRef]
- Nederlandse Kanker Registratie (NKR), Integraal Kankercentrum Nederland (IKNL). 2022. Available online: https://iknl.nl/nkr-cijfers (accessed on 14 January 2022).



{kind=link}
{kind=link}
| Characteristics | Patients (n = 152) |
|---|---|
| Age in years, median (range) | 66 (39–84) |
| Menopausal status | |
| Premenopausal (%) | 19 (12) |
| Postmenopausal (%) | 133 (88) |
| BMI in kg/m2, median (range) | 29.7 (17.6–52.2) |
| <25 kg/m2 (%) | 30 (20) |
| >25 kg/m2 (%) | 122 (80) |
| Preoperative histological grade, n (%) | |
| Grade 1 | 113 (74) |
| Grade 2 | 39 (26) |
| Postoperative histological grade, n (%) | |
| Grade 1 | 107 (70) |
| Grade 2 | 33 (22) |
| Grade 3 | 5 (3) |
| Non-endometrioid | 7 (5) |
| Time in minutes between ICG 1 injection and removal of SLNs, mean (range) | 27 (5–90) |
| Number of removed SLNs 2 per hemipelvis, mean | 1.2 |
| Peroperative (surgical) SLN detection, n (%) | |
| No detection | 8 (5) |
| At least unilateral detection | 144 (95) |
| Bilateral detection | 116 (76) |
| Postoperative (pathological) SLN detection, n (%) | |
| No detection | 13 (9) |
| At least unilateral detection | 139 (91) |
| Bilateral detection | 100 (61) |
| SLN metastasis, n (%) | |
| No SLN detection | 13 (8.6) |
| None | 119 (78) |
| Macro-metastasis | 10 (6.6) |
| Micro-metastasis | 7 (4.6) |
| Isolated tumor cells | 3 (2.0) |
| Postoperative FIGO stage, n (%) | |
| IA | 84 (55) |
| IB | 39 (26) |
| II | 6 (4) |
| IIIA | 6 (4) |
| IIIB | 0 |
| IIIC | 17 (11) |
| IV | 0 |
| Complications | |
| Peroperative | 9 (6.0) 3 |
| Postoperative | 19 (13) 4 |
| Characteristics | Sentinel Lymph Node Positive 1 (n = 20) | Sentinel Lymph Node Negative (n = 119) | p-Value |
|---|---|---|---|
| Age | 0.041 | ||
| <60 years | 3 (15%) | 46 (39%) | |
| ≥60 years | 17 (85%) | 73 (61%) | |
| BMI | 0.619 | ||
| <25 | 5 (25%) | 25 (21%) | |
| ≥25 | 15 (75%) | 94 (79%) | |
| Pre-operative CA-125 | 0.346 | ||
| <35 U/mL | 14 (70%) | 94 (79%) | |
| ≥35 U/mL | 6 (30%) | 19 (16%) | |
| Unknown | 0 | 6 (5%) | |
| Pre-operative histological grade | 0.595 | ||
| Grade 1 | 14 (70%) | 90 (76%) | |
| Grade 2 | 6 (30%) | 29 (24%) | |
| Postoperative histological grade | <0.001 | ||
| Grade 1 | 9 (45%) | 95 (80%) | |
| Grade 2 | 5 (25%) | 23 (19%) | |
| Grade 3 | 4 (20%) | 1 (1%) | |
| Non-endometrioid | 2 (10%) | 0 | |
| Tumor size | 0.566 | ||
| <20 mm | 6 (30%) | 34 (29%) | |
| ≥20 mm | 12 (60%) | 68 (57%) | |
| Unknown | 2 (10%) | 17 (14%) | |
| Myometrial invasion | 0.004 | ||
| None | 1 (5%) | 26 (22%) | |
| <50% | 5 (25%) | 55 (46%) | |
| ≥50% | 14 (70%) | 38 (32%) | |
| Lymphovascular space invasion | <0.001 | ||
| Present | 11 (55%) | 15 (13%) | |
| Absent | 7 (35%) | 102 (86%) | |
| Unknown | 2 (10%) | 2 (1%) | |
| ER/PR status 2 | n/a | ||
| Both positive | 14 (70%) | 50 (42%) | |
| Both negative | 1 (5%) | 0 | |
| ER pos/PR neg | 4 (20%) | 3 (3%) | |
| ER/PR unknown | 1 (5%) | 66 (55%) |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Burg, L.C.; Kruitwagen, R.F.P.M.; de Jong, A.; Bulten, J.; Bonestroo, T.J.J.; Kraayenbrink, A.A.; Boll, D.; Lambrechts, S.; Smedts, H.P.M.; Bouman, A.; et al. Sentinel Lymph Node Mapping in Presumed Low- and Intermediate-Risk Endometrial Cancer Management (SLIM): A Multicenter, Prospective Cohort Study in The Netherlands. Cancers 2023, 15, 271. https://doi.org/10.3390/cancers15010271
Burg LC, Kruitwagen RFPM, de Jong A, Bulten J, Bonestroo TJJ, Kraayenbrink AA, Boll D, Lambrechts S, Smedts HPM, Bouman A, et al. Sentinel Lymph Node Mapping in Presumed Low- and Intermediate-Risk Endometrial Cancer Management (SLIM): A Multicenter, Prospective Cohort Study in The Netherlands. Cancers. 2023; 15(1):271. https://doi.org/10.3390/cancers15010271
Chicago/Turabian StyleBurg, Lara C., Roy F. P. M. Kruitwagen, Annemarie de Jong, Johan Bulten, Tijmen J. J. Bonestroo, Arjan A. Kraayenbrink, Dorry Boll, Sandrina Lambrechts, Huberdina P. M. Smedts, Annechien Bouman, and et al. 2023. "Sentinel Lymph Node Mapping in Presumed Low- and Intermediate-Risk Endometrial Cancer Management (SLIM): A Multicenter, Prospective Cohort Study in The Netherlands" Cancers 15, no. 1: 271. https://doi.org/10.3390/cancers15010271
APA StyleBurg, L. C., Kruitwagen, R. F. P. M., de Jong, A., Bulten, J., Bonestroo, T. J. J., Kraayenbrink, A. A., Boll, D., Lambrechts, S., Smedts, H. P. M., Bouman, A., Engelen, M. J. A., Kasius, J. C., Bekkers, R. L. M., & Zusterzeel, P. L. M. (2023). Sentinel Lymph Node Mapping in Presumed Low- and Intermediate-Risk Endometrial Cancer Management (SLIM): A Multicenter, Prospective Cohort Study in The Netherlands. Cancers, 15(1), 271. https://doi.org/10.3390/cancers15010271