
Can Pre-Operative Neutrophil-to-Lymphocyte Ratio (NLR) Help Predict Non-Metastatic Renal Carcinoma Recurrence after Nephrectomy? (UroCCR-61 Study)

 , and
, and 
Abstract
Simple Summary
Abstract
1. Introduction
2. Materials and Methods
2.1. Study Design
2.2. Study Objectives and Endpoints
2.3. Statistical Analysis
3. Results
3.1. Baseline Characteristics of the Study Population According to Recurrence or Not
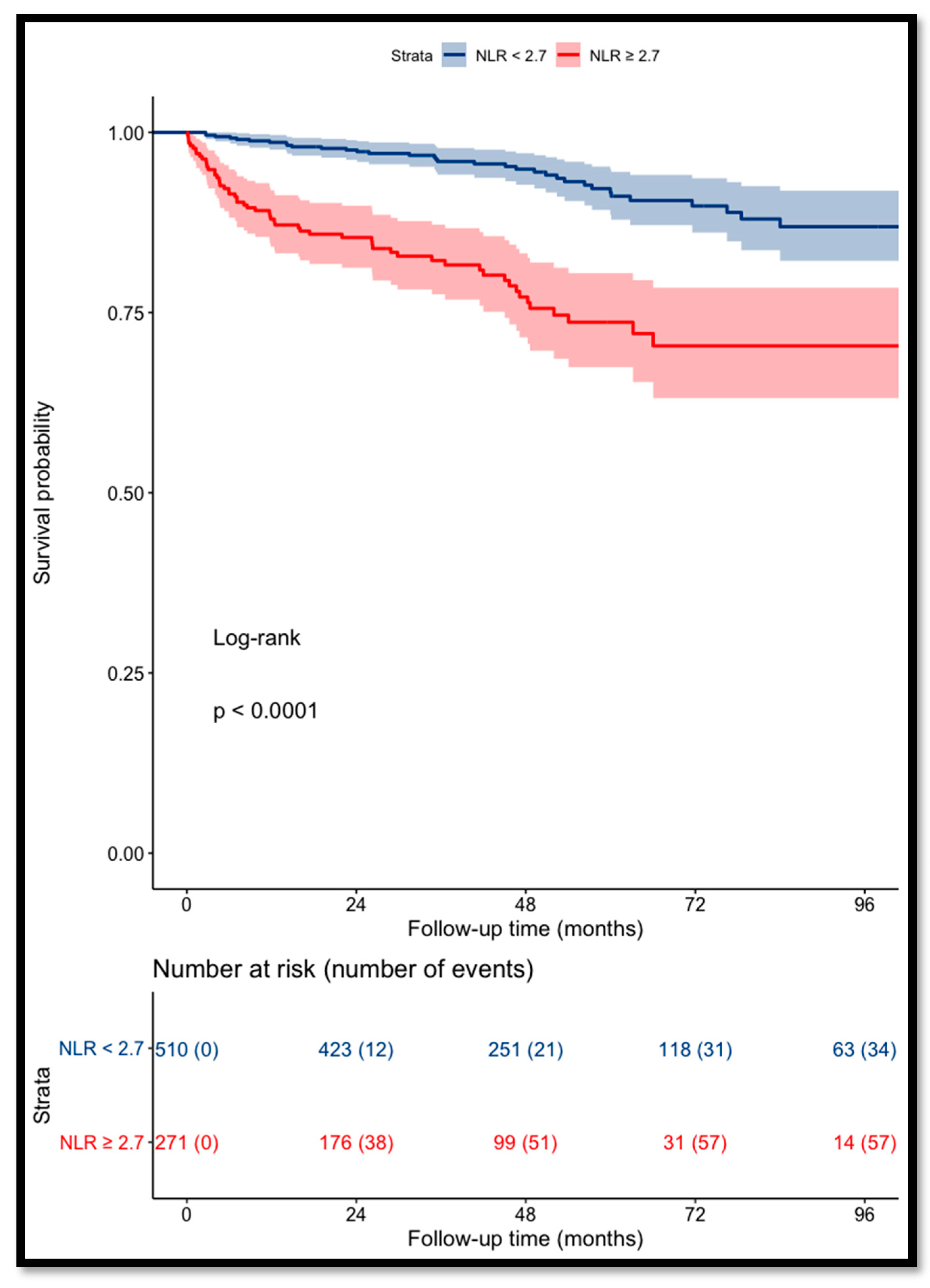
3.2. Prognostic Value of NLR on Recurrence-Free Survival
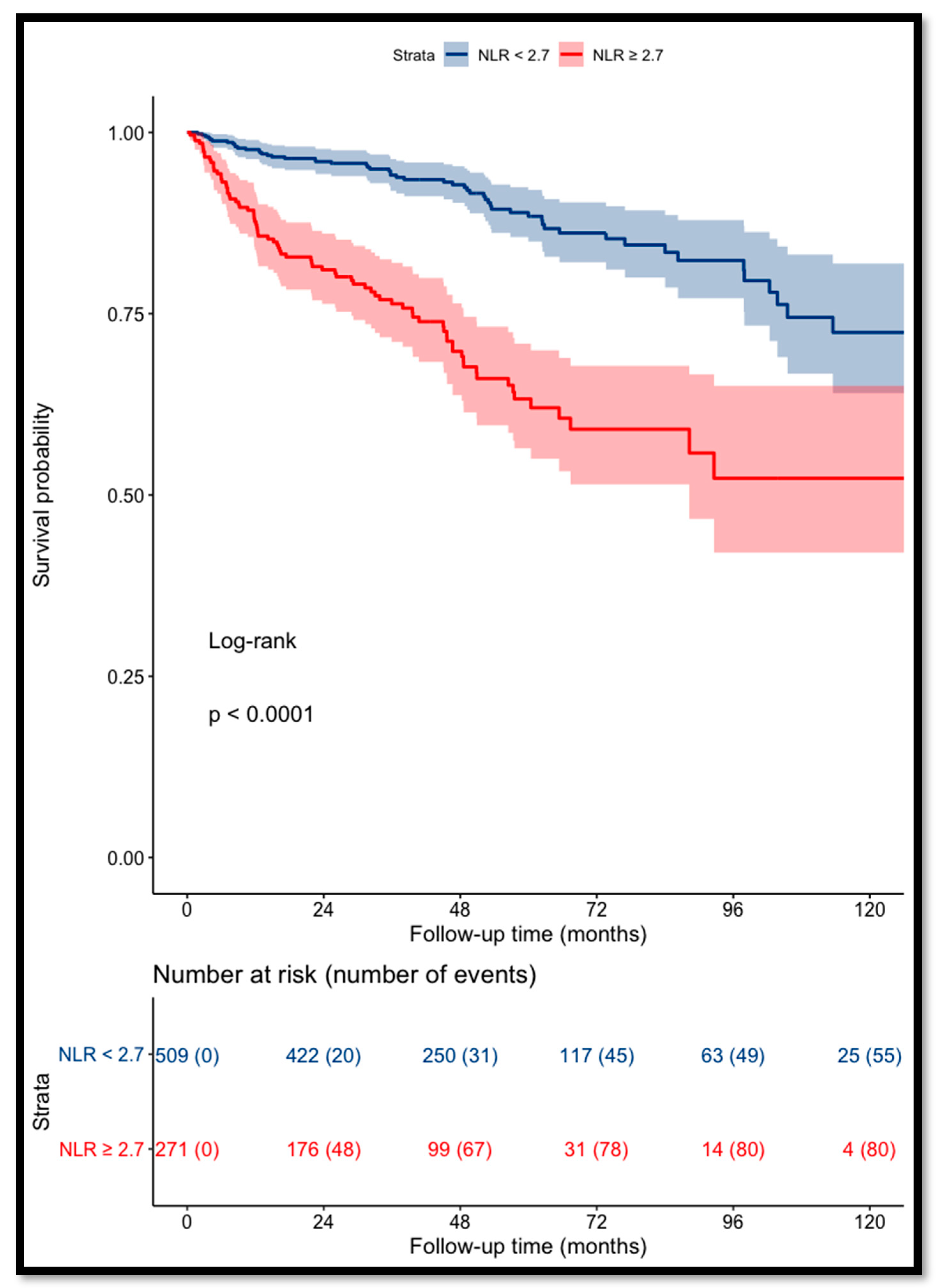
3.3. Prognostic Value of NLR on Overall Survival
3.4. Prognostic Value of Pre-operative NLR Combined with UISS Score on Recurrence-Free Survival: UroCCR-61 Predictive Model
3.5. NLR at the Time of Recurrence
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Antonelli, A.; Cozzoli, A.; Zani, D.; Zanotelli, T.; Nicolai, M.; Cunico, S.C.; Simeone, C. The follow-up management of non-metastatic renal cell carcinoma: Definition of a surveillance protocol. BJU Int. 2007, 99, 296–300. [Google Scholar] [CrossRef]
- Choueiri, T.K.; Tomczak, P.; Park, S.H.; Venugopal, B.; Ferguson, T.; Chang, Y.-H.; Hajek, J.; Symeonides, S.N.; Lee, J.L.; Sarwar, N.; et al. Adjuvant Pembrolizumab after Nephrectomy in Renal-Cell Carcinoma. N. Engl. J. Med. 2021, 385, 683–694. [Google Scholar] [CrossRef]
- Patard, J.-J.; Kim, H.L.; Lam, J.S.; Dorey, F.J.; Pantuck, A.J.; Zisman, A.; Ficarra, V.; Han, K.-R.; Cindolo, L.; De La Taille, A.; et al. Use of the University of California Los Angeles Integrated Staging System to Predict Survival in Renal Cell Carcinoma: An International Multicenter Study. J. Clin. Oncol. 2004, 22, 3316–3322. [Google Scholar] [CrossRef] [PubMed]
- Grivennikov, S.I.; Greten, F.R.; Karin, M. Immunity, Inflammation, and Cancer. Cell 2010, 140, 883–899. [Google Scholar] [CrossRef]
- Zhao, H.; Wu, L.; Yan, G.; Chen, Y.; Zhou, M.; Wu, Y.; Li, Y. Inflammation and tumor progression: Signaling pathways and targeted intervention. Signal Transduct. Target. Ther. 2021, 6, 263. [Google Scholar] [CrossRef]
- Templeton, A.J.; McNamara, M.G.; Šeruga, B.; Vera-Badillo, F.E.; Aneja, P.; Ocaña, A.; Leibowitz-Amit, R.; Sonpavde, G.; Knox, J.J.; Tran, B.; et al. Prognostic Role of Neutrophil-to-Lymphocyte Ratio in Solid Tumors: A Systematic Review and Meta-Analysis. JNCI J. Natl. Cancer Inst. 2014, 106, dju124. [Google Scholar] [CrossRef]
- Nunno, V.D.; Mollica, V.; Gatto, L.; Santoni, M.; Cosmai, L.; Porta, C.; Massari, F. Prognostic impact of neutrophil-to-lymphocyte ratio in renal cell carcinoma: A systematic review and meta-analysis. Immunotherapy 2019, 11, 631–643. [Google Scholar] [CrossRef] [PubMed]
- Hu, H.; Yao, X.; Xie, X.; Wu, X.; Zheng, C.; Xia, W.; Ma, S. Prognostic value of preoperative NLR, dNLR, PLR and CRP in surgical renal cell carcinoma patients. World J. Urol. 2017, 35, 261–270. [Google Scholar] [CrossRef] [PubMed]
- Grimes, N.; Hannan, C.; Tyson, M.; Thwaini, A. The role of neutrophil-lymphocyte ratio as a prognostic indicator in patients undergoing nephrectomy for renal cell carcinoma. Can. Urol. Assoc. J. 2018, 12, E345–E348. [Google Scholar] [CrossRef] [PubMed]
- Viers, B.R.; Houston Thompson, R.; Boorjian, S.A.; Lohse, C.M.; Leibovich, B.C.; Tollefson, M.K. Preoperative neutrophil-lymphocyte ratio predicts death among patients with localized clear cell renal carcinoma undergoing nephrectomy. Urol. Oncol. Semin. Orig. Investig. 2014, 32, 1277–1284. [Google Scholar] [CrossRef] [PubMed]
- Amin, M.B.; Greene, F.L.; Edge, S.B.; Compton, C.C.; Gershenwald, J.E.; Brookland, R.K.; Meyer, L.; Gress, D.M.; Byrd, D.R.; Winchester, D.P. The Eighth Edition AJCC Cancer Staging Manual: Continuing to build a bridge from a population-based to a more “personalized” approach to cancer staging: The Eighth Edition AJCC Cancer Staging Manual. CA. Cancer J. Clin. 2017, 67, 93–99. [Google Scholar] [CrossRef]
- Bensalah, K.; Bigot, P.; Albiges, L.; Bernhard, J.C.; Bodin, T.; Boissier, R.; Correas, J.M.; Gimel, P.; Hetet, J.F.; Long, J.A.; et al. Recommandations françaises du Comité de cancérologie de l’AFU–actualisation 2020–2022: Prise en charge du cancer du rein. Prog. En Urol. 2020, 30, S2–S51. [Google Scholar] [CrossRef]
- Mantovani, A.; Allavena, P.; Sica, A.; Balkwill, F. Cancer-related inflammation. Nature 2008, 454, 436–444. [Google Scholar] [CrossRef] [PubMed]
- Grivas, N.; Kafarakis, V.; Tsimaris, I.; Raptis, P.; Hastazeris, K.; Stavropoulos, N. Clinico-pathological prognostic factors of renal cell carcinoma: A 15-year review from a single center in Greece. Urol. Ann. 2014, 6, 116. [Google Scholar] [CrossRef]
- Ohno, Y.; Nakashima, J.; Ohori, M.; Gondo, T.; Hatano, T.; Tachibana, M. Followup of neutrophil-to-lymphocyte ratio and recurrence of clear cell renal cell carcinoma. J. Urol. 2012, 187, 411–417. [Google Scholar] [CrossRef] [PubMed]
- Pichler, M.; Hutterer, G.C.; Stoeckigt, C.; Chromecki, T.F.; Stojakovic, T.; Golbeck, S.; Eberhard, K.; Gerger, A.; Mannweiler, S.; Pummer, K.; et al. Validation of the pre-treatment neutrophil–lymphocyte ratio as a prognostic factor in a large European cohort of renal cell carcinoma patients. Br. J. Cancer 2013, 108, 901–907. [Google Scholar] [CrossRef]
- Ohno, Y.; Nakashima, J.; Ohori, M.; Hatano, T.; Tachibana, M. Pretreatment Neutrophil-to-Lymphocyte Ratio as an Independent Predictor of Recurrence in Patients With Nonmetastatic Renal Cell Carcinoma. J. Urol. 2010, 184, 873–878. [Google Scholar] [CrossRef]
- Wen, R.-M.; Zhang, Y.-J.; Ma, S.; Xu, Y.-L.; Chen, Y.-S.; Li, H.-L.; Bai, J.; Zheng, J.-N. Preoperative Neutrophil to Lymphocyte Ratio as a Prognostic Factor in Patients with Non-metastatic Renal Cell Carcinoma. Asian Pac. J. Cancer Prev. 2015, 16, 3703–3708. [Google Scholar] [CrossRef] [PubMed]
- de Martino, M.; Pantuck, A.J.; Hofbauer, S.; Waldert, M.; Shariat, S.F.; Belldegrun, A.S.; Klatte, T. Prognostic Impact of Preoperative Neutrophil-to-Lymphocyte Ratio in Localized Nonclear Cell Renal Cell Carcinoma. J. Urol. 2013, 190, 1999–2004. [Google Scholar] [CrossRef] [PubMed]
- Boissier, R.; Campagna, J.; Branger, N.; Karsenty, G.; Lechevallier, E. The prognostic value of the neutrophil-lymphocyte ratio in renal oncology: A review. Urol. Oncol. Semin. Orig. Investig. 2017, 35, 135–141. [Google Scholar] [CrossRef]
- Ljungberg, B.; Albiges, L.; Abu-Ghanem, Y.; Bensalah, K.; Dabestani, S.; Fernández-Pello, S.; Giles, R.H.; Hofmann, F.; Hora, M.; Kuczyk, M.A.; et al. European Association of Urology Guidelines on Renal Cell Carcinoma: The 2019 Update. Eur. Urol. 2019, 75, 799–810. [Google Scholar] [CrossRef] [PubMed]





{kind=link}
{kind=link}
{kind=link}
{kind=link}
| n= | Overall Cohort (n = 786) | Recurrence (n = 135) | No Recurrence (n = 651) | p-Value | |
|---|---|---|---|---|---|
| Age, years ± SD | 786 | 60.9 ± 13.5 | 64 ± 12.4 | 60.2 ± 13.6 | 0.002 |
| Gender, n (%) | 786 | 0.9 | |||
| Male | 548 (69.7%) | 94 (69.6%) | 454 (69.7%) | ||
| Female | 238 (30.3%) | 41 (30.4%) | 197 (30.3%) | ||
| ECOG, n (%) | 783 | 0.01 | |||
| 0 | 558 (71.3%) | 83 (61.5%) | 475 (73.3%) | ||
| 1 | 161 (20.6%) | 41 (30.4%) | 120 (18.5%) | ||
| 2 | 58 (7.4%) | 9 (6.6%) | 49 (7.6%) | ||
| 3 | 6 (0.7%) | 2 (1.5%) | 4 (0.6%) | ||
| Symptoms, n (%) | 782 | <0.001 | |||
| Incidental | 556 (71.1%) | 77 (57.9%) | 479 (73.8%) | ||
| Local | 162 (20.7%) | 35 (26.3%) | 127 (19.6%) | ||
| General | 64 (8.2%) | 21 (15.8%) | 43 (6.6%) | ||
| Pre-operative NLR ± SD | 786 | 2.8 ± 2.4 | 4.2 ± 4 | 2.4 ± 1.7 | <0.001 |
| Type of treatment, n (%) | 786 | <0.001 | |||
| Partial nephrectomy | 517 (65.8%) | 55 (40.7%) | 462 (71%) | ||
| Radical nephrectomy | 269 (34.2%) | 80 (59.3%) | 189 (29%) | ||
| Surgical approach, n (%) | 740 | <0.001 | |||
| Open | 169 (22.8%) | 50 (39.7%) | 119 (19.4%) | ||
| Laparoscopic | 571 (77.2%) | 76 (60.3%) | 495 (80.6%) | ||
| Pathological tumor size, mm ± SD | 784 | 48.3 ± 29.3 | 68.1 ± 38.2 | 44.2 ± 25.3 | <0.001 |
| pT stage, n (%) | 785 | <0.001 | |||
| 1 | 495 (63.1%) | 49 (36.3%) | 446 (68.6%) | ||
| 2 | 52 (6.6%) | 10 (7.4%) | 42 (6.5%) | ||
| 3 | 231 (29.4%) | 71 (52.6%) | 160 (24.6%) | ||
| 4 | 7 (0.9%) | 5 (3.7%) | 2 (0.3%) | ||
| Surgical margins, n (%) | 785 | 0.09 | |||
| Negative | 753 (96%) | 126 (93.4%) | 627 (96.5%) | ||
| Positive | 32 (4%) | 9 (6.6%) | 23 (3.5%) | ||
| Fuhrman grade, n (%) | 775 | <0.001 | |||
| I | 15 (1.9%) | 0 (0%) | 15 (2.4%) | ||
| II | 365 (47.1%) | 32 (24.3%) | 333 (52%) | ||
| III | 296 (38.2%) | 65 (47.8%) | 231 (36.1%) | ||
| IV | 99 (12.8%) | 38 (27.9%) | 61 (9.6%) | ||
| Histology, n (%) | 786 | <0.001 | |||
| Clear cell | 583 (74.2%) | 121 (89.6%) | 462 (70.9%) | ||
| Papillary | 110 (14%) | 10 (7.4%) | 100 (15.4%) | ||
| Chromophobe | 63 (8%) | 2 (1.5%) | 61 (9.4%) | ||
| Other | 30 (3.8%) | 2 (1.5%) | 28 (4.3%) | ||
| Sarcomatoid features, n (%) | 772 | 75 (9.7%) | 25 (19.4%) | 50 (7.8%) | <0.001 |
| Micro vascular invasion, n (%) | 776 | 1113 (14.6%) | 40 (30.5%) | 73 (11.3%) | <0.001 |
| UISS score, n (%) | 774 | <0.001 | |||
| Low | 249 (32.2%) | 13 (9.6%) | 236 (36.9%) | ||
| Intermediate | 430 (55.5%) | 83 (61.5%) | 347 (54.3%) | ||
| High | 95 (12.3%) | 39 (28.9%) | 56 (8.8%) | ||
| NLR at relapse or last follow-up ± SD | 485 | 3.4 ± 4.7 | 4.9 ± 3.7 | 2.9 ± 4.9 | <0.001 |
| n | Recurrence | |
|---|---|---|
| Recurrence localization, n (%) | 135 | |
| Local | 35 (25.9%) | |
| Contralateral kidney | 18 (13.3%) | |
| Retroperitoneal lymph node | 9 (6.7%) | |
| Thoracic | 70 (51.9%) | |
| Bone | 14 (10.4%) | |
| Hepatic | 8 (5.9%) | |
| Cerebral | 7 (5.2%) | |
| Other | 18 (13.3%) |
| Uni-Variate Analysis | Multi-Variate Analysis | |||
|---|---|---|---|---|
| HR (95% CI) | p-Value | HR (95% CI) | p-Value | |
| Gender, male vs. female | 1.03 [0.71–1.48] | 0.8 | 0.80 [0.54–1.18] | 0.3 |
| Age, ≥61 vs. <61 | 1.51 [1.08–2.16] | 0.01 | 1.32 [0.90–1.95] | 0.1 |
| Pre-operative NLR, ≥2.7 vs. <2.7 | 3.61 [2.56–5.13] | <0.001 | 2.89 [1.94–4.31] | <0.001 |
| Type of treatment, radical vs. partial nephrectomy | 2.42 [1.73–3.45] | <0.001 | 1.19 [0.76–1.87] | 0.2 |
| Surgical approach, laparoscopic vs. open | 0.56 [0.40–0.81] | 0.002 | 0.63 [0.43–0.92] | 0.02 |
| pT stage, 3–4 vs. 1–2 | 3.8 [2.69–5.35] | <0.001 | 1.80 [1.15–2.83] | 0.01 |
| Fuhrman grade, 3–4 vs. 1–2 | 3.15 [2.12–4.69] | <0.001 | 1.5 [0.92–2.43] | 0.09 |
| Histology, clear cell vs. other | 3.12 [1.79–5.4] | <0.001 | 2.9 [1.1–7.8] | 0.02 |
| Sarcomatoid features | 3.74 [2.40–5.83] | <0.001 | 1.89 [1.15–3.11] | 0.01 |
| Micro-vascular invasion | 3.07 [2.12–4.47] | <0.001 | 1.10 [0.69–1.75] | 0.6 |
| Surgical margins, positive vs. negative | 2.19 [1.11–4.32] | 0.02 | 1.58 [0.75–3.3] | 0.2 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Allenet, C.; Klein, C.; Rouget, B.; Margue, G.; Capon, G.; Alezra, E.; Blanc, P.; Estrade, V.; Bladou, F.; Robert, G.; et al. Can Pre-Operative Neutrophil-to-Lymphocyte Ratio (NLR) Help Predict Non-Metastatic Renal Carcinoma Recurrence after Nephrectomy? (UroCCR-61 Study). Cancers 2022, 14, 5692. https://doi.org/10.3390/cancers14225692
Allenet C, Klein C, Rouget B, Margue G, Capon G, Alezra E, Blanc P, Estrade V, Bladou F, Robert G, et al. Can Pre-Operative Neutrophil-to-Lymphocyte Ratio (NLR) Help Predict Non-Metastatic Renal Carcinoma Recurrence after Nephrectomy? (UroCCR-61 Study). Cancers. 2022; 14(22):5692. https://doi.org/10.3390/cancers14225692
Chicago/Turabian StyleAllenet, Clément, Clément Klein, Benjamin Rouget, Gaëlle Margue, Grégoire Capon, Eric Alezra, Peggy Blanc, Vincent Estrade, Franck Bladou, Grégoire Robert, and et al. 2022. "Can Pre-Operative Neutrophil-to-Lymphocyte Ratio (NLR) Help Predict Non-Metastatic Renal Carcinoma Recurrence after Nephrectomy? (UroCCR-61 Study)" Cancers 14, no. 22: 5692. https://doi.org/10.3390/cancers14225692
APA StyleAllenet, C., Klein, C., Rouget, B., Margue, G., Capon, G., Alezra, E., Blanc, P., Estrade, V., Bladou, F., Robert, G., & Bernhard, J.-C. (2022). Can Pre-Operative Neutrophil-to-Lymphocyte Ratio (NLR) Help Predict Non-Metastatic Renal Carcinoma Recurrence after Nephrectomy? (UroCCR-61 Study). Cancers, 14(22), 5692. https://doi.org/10.3390/cancers14225692