
Whole-Body MRI Surveillance—Baseline Findings in the Swedish Multicentre Hereditary TP53-Related Cancer Syndrome Study (SWEP53)

 , , , , ,
, , , , ,
Abstract
:Simple Summary
Abstract

1. Introduction
2. Materials and Methods
2.1. Recruitment of Study Participants
2.2. Surveillance Program
2.3. Imaging Protocols
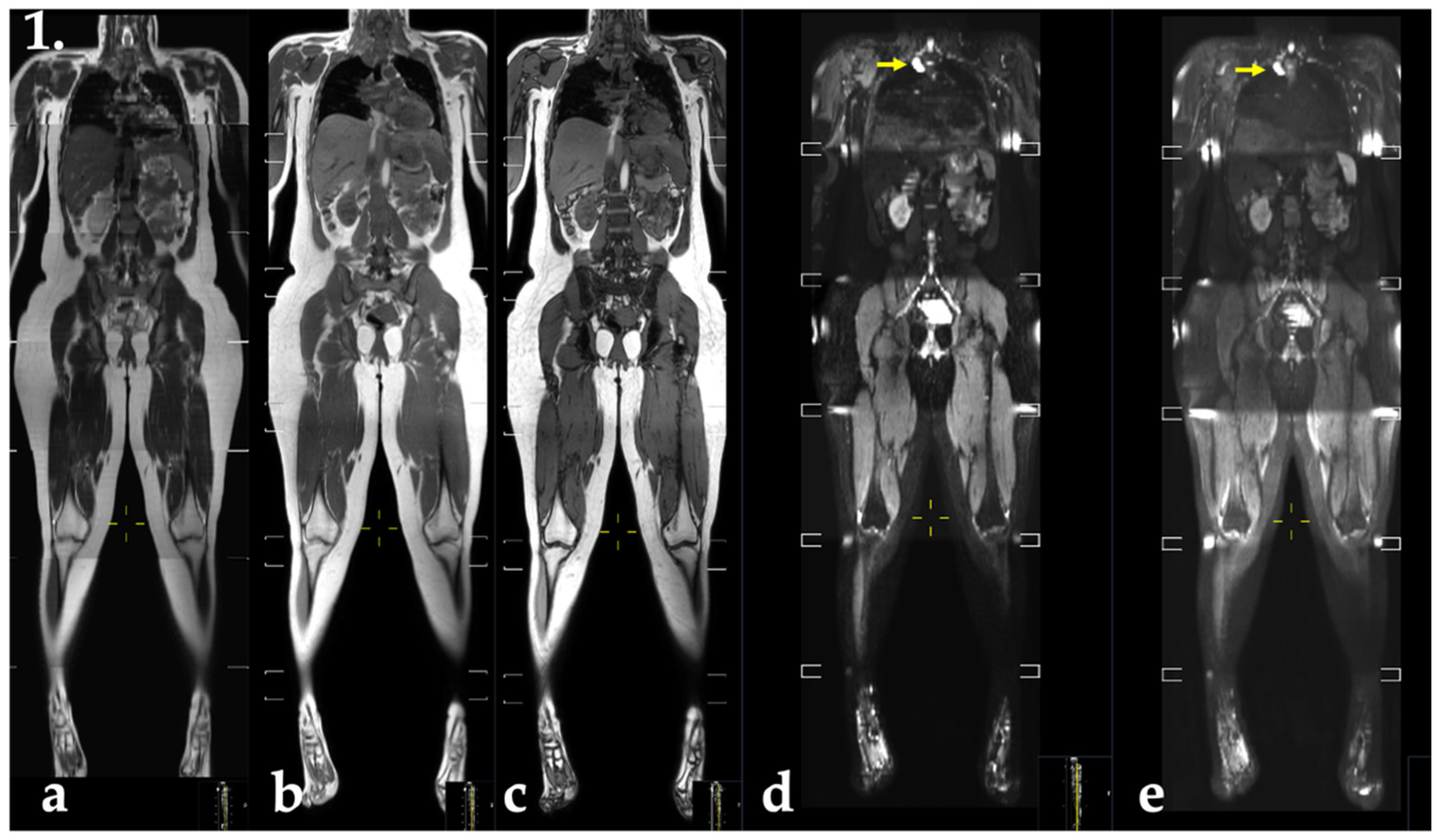
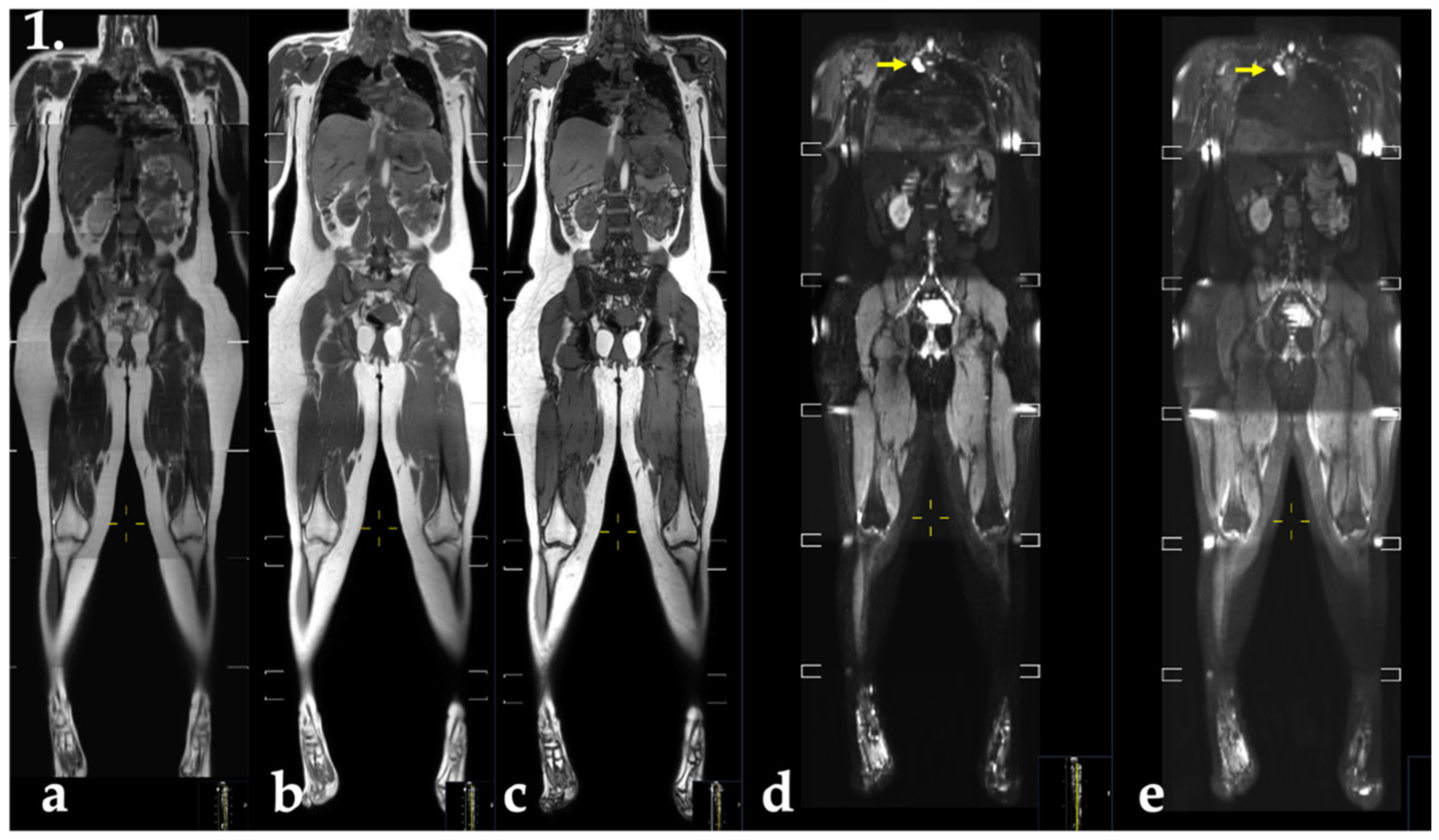
2.4. MRI
2.5. Evaluation
2.6. Data Collection
2.7. Statistical Analyses
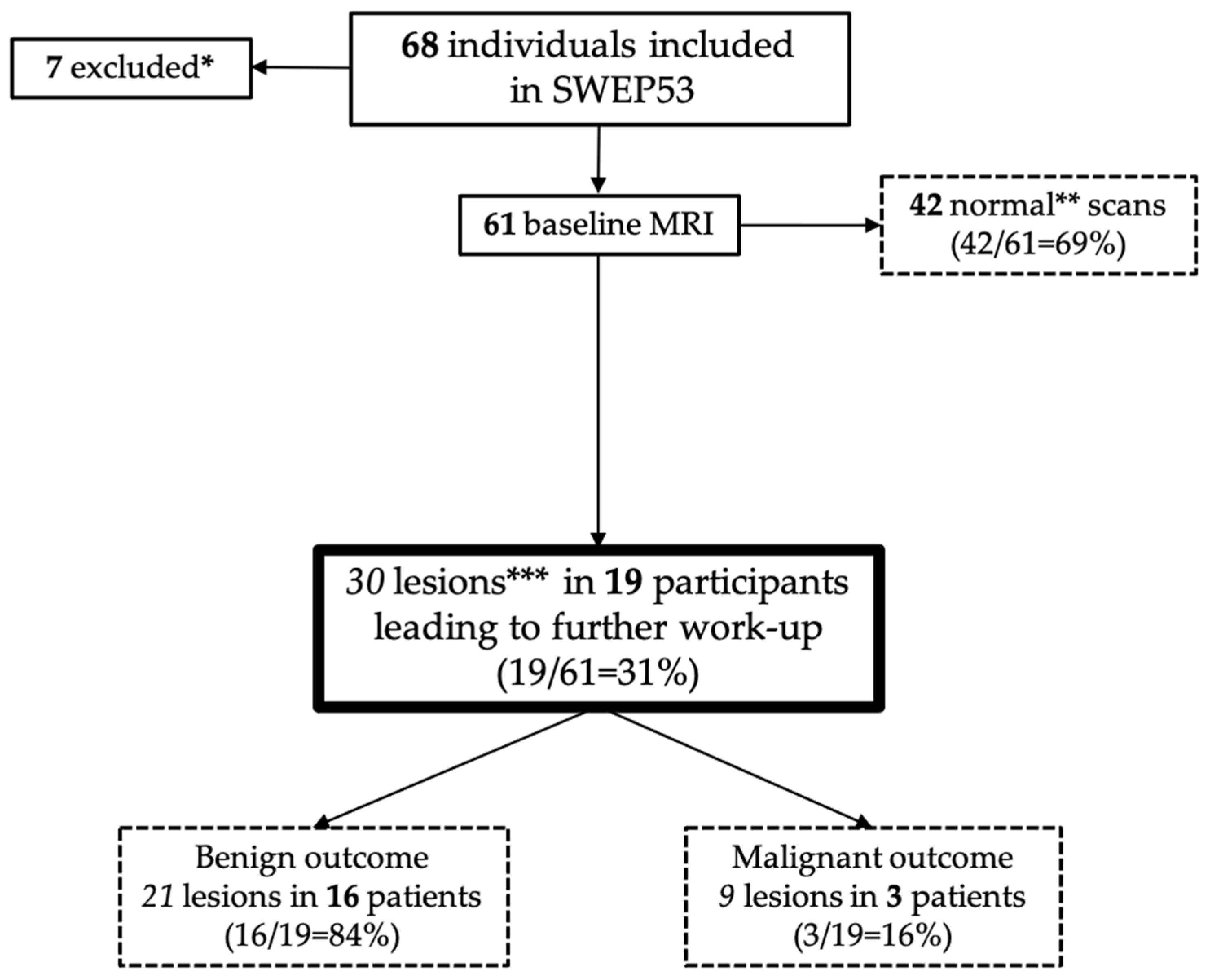
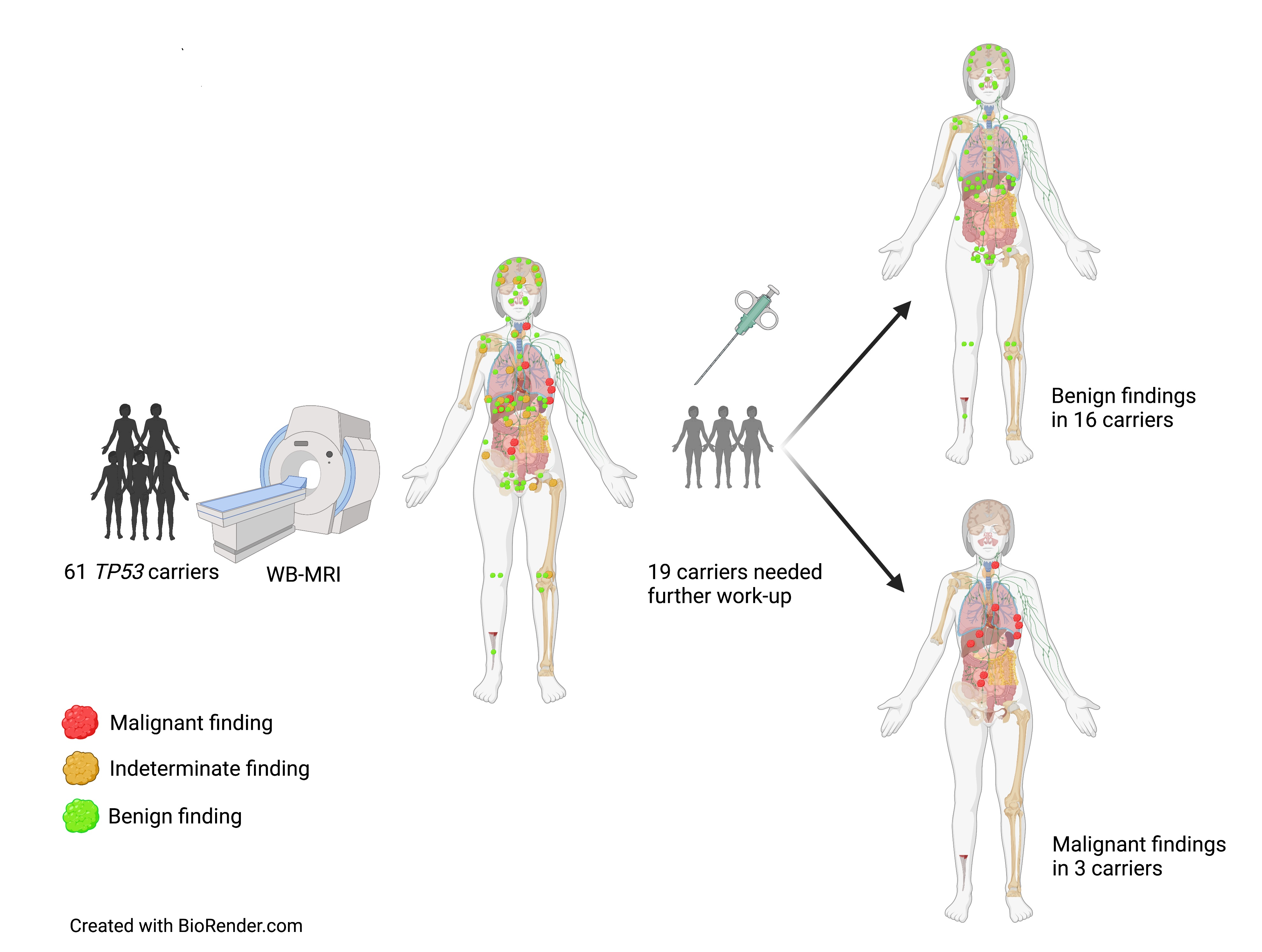
3. Results
3.1. Previous Tumour Spectrum Prior to Inclusion
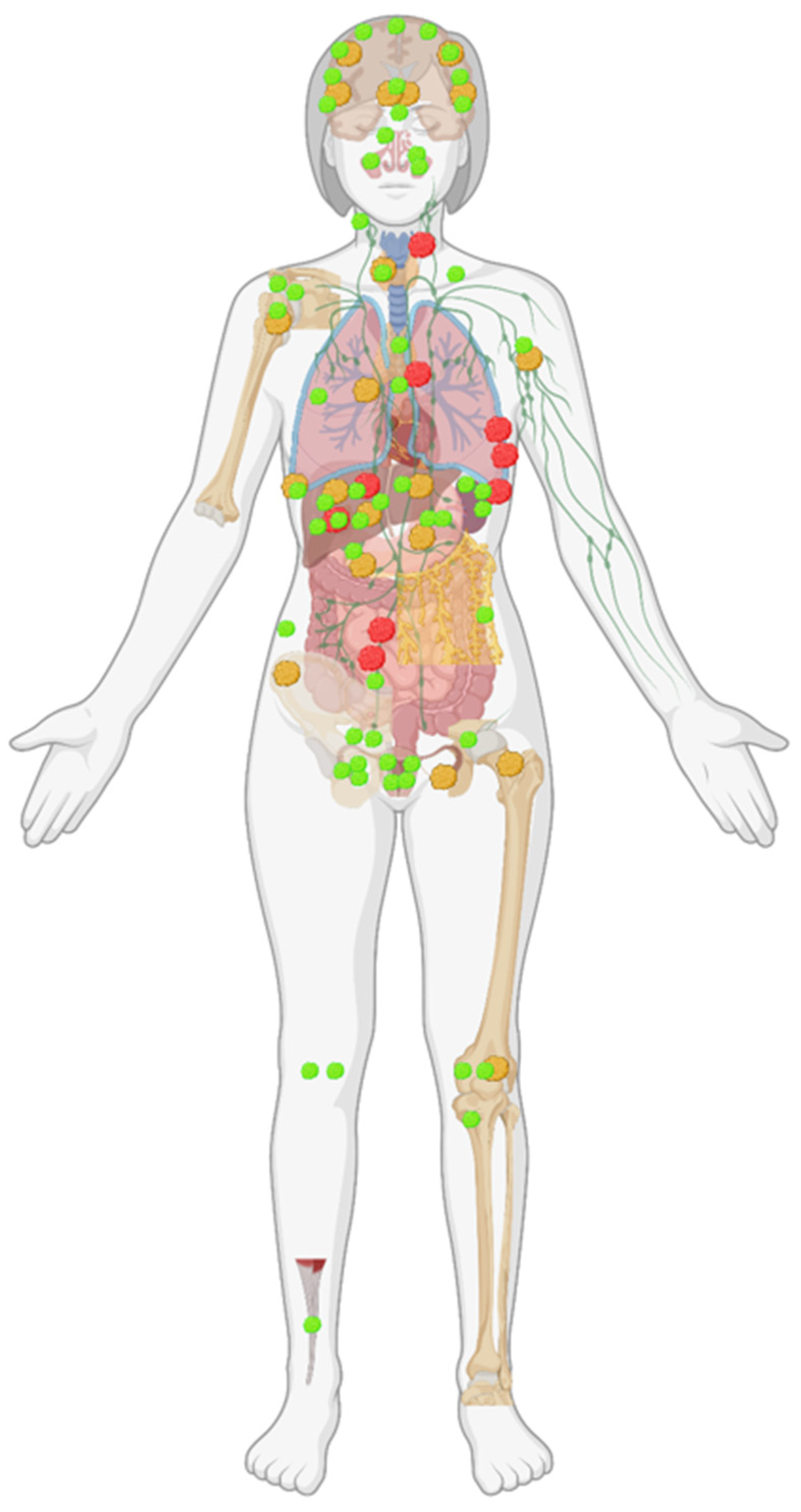
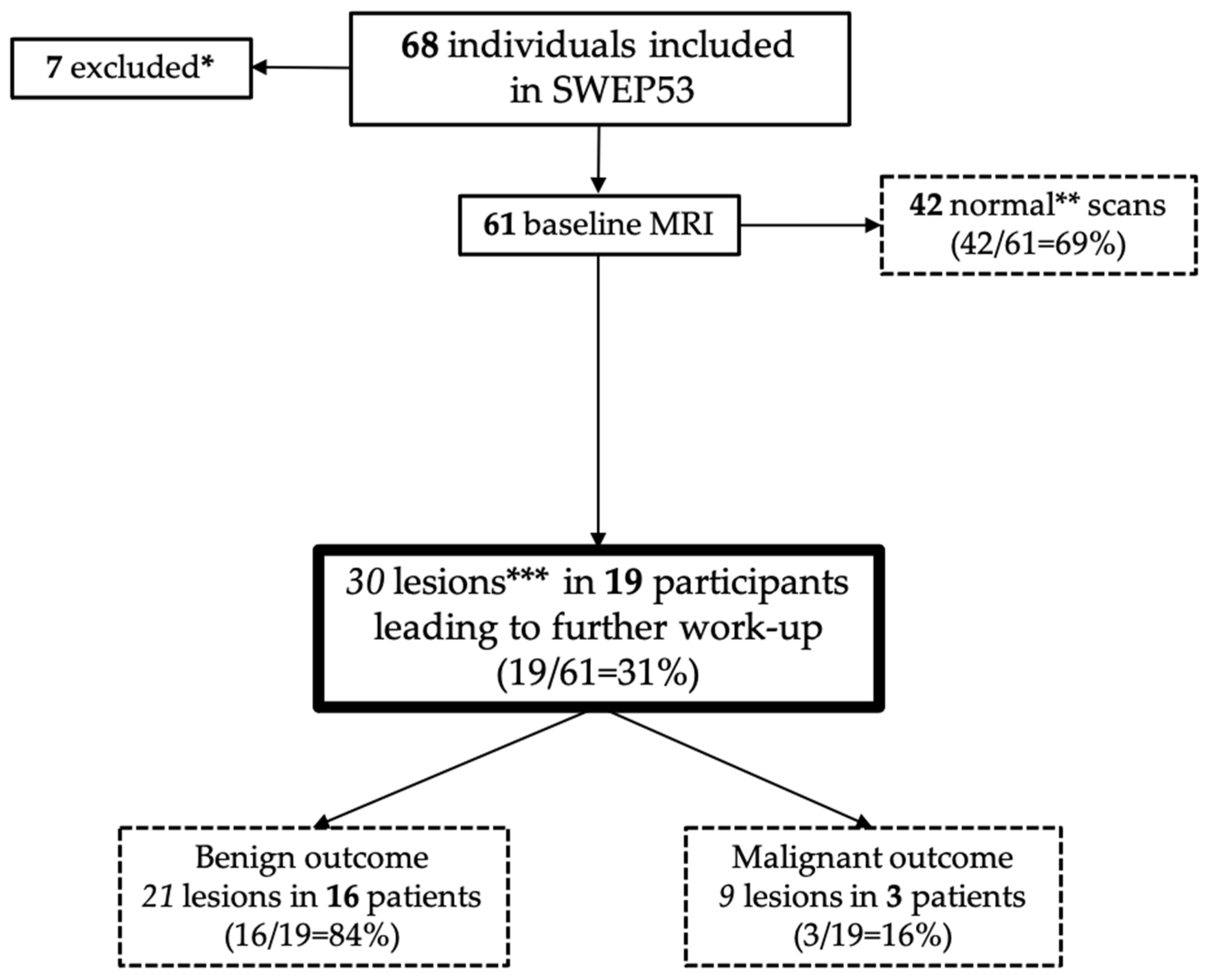
3.2. Baseline Findings
3.2.1. Malignant Findings
3.2.2. Indeterminate Findings
3.2.3. Benign Findings
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Varley, J.M.; Evans, D.G.; Birch, J.M. Li-Fraumeni syndrome—A molecular and clinical review. Br. J. Cancer 1997, 76, 1–14. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Li, F.P.; Fraumeni, J.F. Soft-tissue sarcomas, breast cancer, and other neoplasms. A familial syndrome? Ann. Intern. Med. 1969, 71, 747–752. [Google Scholar] [CrossRef] [Green Version]
- Frebourg, T.; Bajalica Lagercrantz, S.; Oliveira, C.; Magenheim, R.; Evans, D.G. Guidelines for the Li-Fraumeni and heritable TP53-related cancer syndromes. Eur. J. Hum. Genet. EJHG 2020, 28, 1379–1386. [Google Scholar] [CrossRef] [PubMed]
- Bougeard, G.; Renaux-Petel, M.; Flaman, J.M.; Charbonnier, C.; Fermey, P.; Belotti, M.; Gauthier-Villars, M.; Stoppa-Lyonnet, D.; Consolino, E.; Brugières, L.; et al. Revisiting Li-Fraumeni Syndrome From TP53 Mutation Carriers. J. Clin. Oncol. 2015, 33, 2345–2352. [Google Scholar] [CrossRef]
- Gonzalez, K.D.; Noltner, K.A.; Buzin, C.H.; Gu, D.; Wen-Fong, C.Y.; Nguyen, V.Q.; Han, J.H.; Lowstuter, K.; Longmate, J.; Sommer, S.S.; et al. Beyond Li Fraumeni Syndrome: Clinical characteristics of families with p53 germline mutations. J. Clin. Oncol. 2009, 27, 1250–1256. [Google Scholar] [CrossRef] [PubMed]
- Olivier, M.; Goldgar, D.E.; Sodha, N.; Ohgaki, H.; Kleihues, P.; Hainaut, P.; Eeles, R.A. Li-Fraumeni and related syndromes: Correlation between tumor type, family structure, and TP53 genotype. Cancer Res. Chic. Ill 2003, 63, 6643–6650. [Google Scholar]
- Hisada, M.; Garber, J.E.; Li, F.P.; Fung, C.Y.; Fraumeni, J.F. Multiple Primary Cancers in Families With Li-Fraumeni Syndrome. J. Natl. Cancer Inst. 1998, 90, 606–611. [Google Scholar] [CrossRef]
- Heymann, S.; Delaloge, S.; Rahal, A.; Caron, O.; Frebourg, T.; Barreau, L.; Pachet, C.; Mathieu, M.-C.; Marsiglia, H.; Bourgier, C. Radio-induced malignancies after breast cancer postoperative radiotherapy in patients with Li-Fraumeni syndrome. Radiat. Oncol. Lond. Engl. 2010, 5, 104. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Petry, V.; Bonadio, R.C.; Cagnacci, A.Q.C.; Senna, L.A.L.; Campos, R.d.N.G.; Cotti, G.C.; Hoff, P.M.; Fragoso, M.C.B.V.; Estevez-Diz, M.D.P. Radiotherapy-induced malignancies in breast cancer patients with TP53 pathogenic germline variants (Li-Fraumeni syndrome). Fam. Cancer 2020, 19, 47–53. [Google Scholar] [CrossRef] [PubMed]
- Varley, J.M.; McGown, G.; Thorncroft, M.; James, L.A.; Margison, G.P.; Forster, G.; Evans, D.G.R.; Harris, M.; Kelsey, A.M.; Birch, J.M. Are There Low-Penetrance TP53 Alleles? Evidence from Childhood Adrenocortical Tumors. Am. J. Hum. Genet. 1999, 65, 995–1006. [Google Scholar] [CrossRef] [Green Version]
- Villani, A.M.D.; Shore, A.B.; Wasserman, J.D.M.D.; Stephens, D.M.; Kim, R.H.M.D.; Druker, H.M.; Gallinger, B.M.; Naumer, A.M.S.; Kohlmann, W.M.S.; Novokmet, A.B.A.; et al. Biochemical and imaging surveillance in germline TP53 mutation carriers with Li-Fraumeni syndrome: 11 year follow-up of a prospective observational study. Lancet Oncol. 2016, 17, 1295–1305. [Google Scholar] [CrossRef]
- Ballinger, M.L.; Best, A.; Mai, P.L.; Khincha, P.P.; Loud, J.T.; Peters, J.A.; Achatz, M.I.; Chojniak, R.; Balieiro da Costa, A.; Santiago, K.M.; et al. Baseline Surveillance in Li-Fraumeni Syndrome Using Whole-Body Magnetic Resonance Imaging: A Meta-analysis. JAMA Oncol. 2017, 3, 1634–1639. [Google Scholar] [CrossRef] [PubMed]
- Petralia, G.; Padhani, A.R.; Pricolo, P.; Zugni, F.; Martinetti, M.; Summers, P.E.; Grazioli, L.; Colagrande, S.; Giovagnoni, A.; Bellomi, M. Whole-body magnetic resonance imaging (WB-MRI) in oncology: Recommendations and key uses. La Radiol. Med. 2019, 124, 218–233. [Google Scholar] [CrossRef] [PubMed]
- McBride, K.A.; Ballinger, M.L.; Schlub, T.E.; Young, M.-A.; Tattersall, M.H.N.; Kirk, J.; Eeles, R.; Killick, E.; Walker, L.G.; Shanley, S.; et al. Psychosocial morbidity in TP53 mutation carriers: Is whole-body cancer screening beneficial? Fam. Cancer 2017, 16, 423–432. [Google Scholar] [CrossRef]
- Saya, S.; Killick, E.; Thomas, S.; Taylor, N.; Bancroft, E.K.; Rothwell, J.; Benafif, S.; Dias, A.; Mikropoulos, C.; Pope, J.; et al. Baseline results from the UK SIGNIFY study: A whole-body MRI screening study in TP53 mutation carriers and matched controls. Fam. Cancer 2017, 16, 433–440. [Google Scholar] [CrossRef] [Green Version]
- Ruijs, M.W.G.; Loo, C.E.; van Buchem, C.A.J.M.; Bleiker, E.M.A.; Sonke, G.S. Surveillance of Dutch Patients With Li-Fraumeni Syndrome: The LiFe-Guard Study. JAMA Oncol. 2017, 3, 1733–1734. [Google Scholar] [CrossRef]
- Caron, O.; Frébourg, T.; Bourbouloux, E.; Bonadona, V.; Mari, V.; Maugard, C.; Eisinger, F.; Barouk-Simonet, E.; Gauthier-Villars, M.; Tinat, J.; et al. Evaluation of whole body MRI for early detection of cancers in subjects with germ-line TP53 mutation (Li-Fraumeni syndrome). J. Clin. Oncol. 2013, 31, TPS1607. [Google Scholar] [CrossRef]
- Mai, P.L.; Khincha, P.P.; Loud, J.T.; DeCastro, R.M.; Bremer, R.C.; Peters, J.A.; Liu, C.-Y.; Bluemke, D.A.; Malayeri, A.A.; Savage, S.A. Prevalence of Cancer at Baseline Screening in the National Cancer Institute Li-Fraumeni Syndrome Cohort. JAMA Oncol. 2017, 3, 1640–1645. [Google Scholar] [CrossRef]
- Bojadzieva, J.; Amini, B.; Day, S.F.; Jackson, T.L.; Thomas, P.S.; Willis, B.J.; Throckmorton, W.R.; Daw, N.C.; Bevers, T.B.; Strong, L.C. Whole body magnetic resonance imaging (WB-MRI) and brain MRI baseline surveillance in TP53 germline mutation carriers: Experience from the Li-Fraumeni Syndrome Education and Early Detection (LEAD) clinic. Fam. Cancer 2018, 17, 287–294. [Google Scholar] [CrossRef]
- Omran, M.; Blomqvist, L.; Brandberg, Y.; Pal, N.; Kogner, P.; Ståhlbom, A.K.; Tham, E.; Bajalica-Lagercrantz, S. Whole-body MRI within a surveillance program for carriers with clinically actionable germline TP53 variants—the Swedish constitutional TP53 study SWEP53. Hered. Cancer Clin. Pract. 2020, 18, 1–9. [Google Scholar] [CrossRef]
- Weckbach, S.E. Incidental R Adiological Findings; Springer International Publishing: Cham, Switzerland, 2017; p. 209. [Google Scholar]
- Lawrence, W.J.; Donegan, W.L.; Natarajan, N.; Mettlin, C.; Beart, R.; Winchester, D. Adult soft tissue sarcomas: A pattern of care survey of the American college of surgeons. Ann. Surg. 1987, 205, 349–359. [Google Scholar] [CrossRef] [PubMed]
- Meyers, P.A.; Gorlick, R. Osteosarcoma. Pediatr. Clin. N. Am. 1997, 44, 973–989. [Google Scholar] [CrossRef]

{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Participant Characteristics at Inclusion | Women | Men |
|---|---|---|
| No. of patients | 43 | 18 |
| Age mean (range) | 39 (20–74) | 41 (18–55) |
| Geographic region | ||
| Umeå | 3 | 0 |
| Uppsala | 6 | 7 |
| Stockholm | 19 | 10 |
| Linköping | 3 | 0 |
| Gothenburg | 5 | 0 |
| Lund | 7 | 1 |
| Previous cancers | ||
| No tumours | 15 | 14 |
| Breast cancers | 27 (23 patients) | 0 |
| Sarcomas | 8 (6 patients) | 1 |
| Brain tumours | 2 (2 patients) | 1 |
| Adrenocortical carcinomas | 0 | 0 |
| Other tumours * | 7 (6 patients) | 2 (2 patients) |
| Multiple tumours ** | ||
| 1 tumour | 16 | 3 |
| 2 different tumours | 6 | 1 |
| 3 different tumours | 6 | 0 |
| 4 different tumours | 0 | 0 |
| Risk-reducing mastectomy | 21 | 0 |
| WB-MRI Outcomes | Findings (n = Total Number of Findings) | Additional Workup (n = Individuals) | Result | |||
|---|---|---|---|---|---|---|
| Organ | Benign (Green) | Indeterminate (Yellow) | Malignant (Red) | Radiological | Other | |
| Head, neck, arms | ||||||
| Brain | 9 | 4 | 0 | Brain-MRI * (4) | Referral to neurologist (1) | Benign |
| Pituitary | 1 | 2 | 0 | Brain-MRI * (2) | Referral to endocrinologist (2) | Benign |
| Face (subcutaneous) | 1 | 0 | 0 | Benign | ||
| Sinonasal cavity | 3 | 0 | 0 | Benign | ||
| Neck | 0 | 0 | 0 | |||
| Lymph nodes, cervical | 1 | 0 | 1 | Part of workup for A | Benign Malignant (A) | |
| Lymph nodes, axillary | 1 | 1 | 0 | Ultrasound | FNAC (1) | Benign |
| Arms | 3 | 1 | 0 | X-ray | Benign | |
| Thyroid | 1 | 1 | 0 | Ultrasound (1) | FNAC (1) | Benign |
| Supraclavicular fossa | 1 | 0 | 0 | Benign | ||
| Thorax | ||||||
| Lung | 1 | 0 | 0 | Benign | ||
| Lymph nodes, mediastinal | 0 | 1 | 1 | CT thorax-abdomen (1) CT thorax (1) | FNAC (2) | Malignant (B) Benign |
| Pleura | 1 | 1 | 3 | CT thorax (2) US thyroid (1) | FNAC thyroid (1) | Malignant (B) Malignant (A) Benign |
| Subcutaneous | 0 | 0 | 0 | |||
| Vertebral column | 2 | 0 | 0 | Benign | ||
| Abdomen | ||||||
| Peritoneum | 1 | 0 | 0 | Benign | ||
| Stomach | 0 | 1 | 0 | Gastroscopy (outside of study) | Benign | |
| Lymph nodes, retroperitoneal | 1 | 0 | 0 | |||
| Liver | 7 | 3 | 2 | Ultrasound (3) Liver-MRI * (2) | FNAC (2) | Benign (3) and Malignant (B, C) |
| Gall bladder | 1 | 0 | 0 | Benign | ||
| Pancreas | 0 | 1 | 0 | Pancreas-MRI* | Benign | |
| Adrenal | 0 | 0 | 0 | |||
| Kidneys | 3 | 0 | 0 | Benign | ||
| Spleen | 3 | 0 | 0 | Benign | ||
| Lymph nodes, intraabdominal | 0 | 0 | 2 | CT thorax-abdomen (2) Liver-MRI * (1) | Malignant (B, C) | |
| Small bowel, colon, rectum and anus | 0 | 0 | 0 | |||
| Subcutaneous | 1 | 0 | 0 | Benign | ||
| Pelvis | ||||||
| Pelvic bone | 0 | 1 | 0 | FNAC | Benign | |
| Lymph nodes, pelvic | 0 | 0 | 0 | |||
| Uterus | 4 | 1 | 0 | Referral to gynaecologist (1) | Benign | |
| Ovaries | 3 | 1 | 0 | Referral to gynaecologist (1) | Benign | |
| Pelvic free fluid | 2 | 0 | 0 | |||
| Lower body | ||||||
| Legs | 7 | 2 | 0 | New imaging (1) | Operation and biopsy (1) | Benign Benign |
| Total lesions: 88 | 58 | 21 | 9 | 24 | 15 | |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Omran, M.; Tham, E.; Brandberg, Y.; Ahlström, H.; Lundgren, C.; Paulsson-Karlsson, Y.; Kuchinskaya, E.; Silander, G.; Rosén, A.; Persson, F.; et al. Whole-Body MRI Surveillance—Baseline Findings in the Swedish Multicentre Hereditary TP53-Related Cancer Syndrome Study (SWEP53). Cancers 2022, 14, 380. https://doi.org/10.3390/cancers14020380
Omran M, Tham E, Brandberg Y, Ahlström H, Lundgren C, Paulsson-Karlsson Y, Kuchinskaya E, Silander G, Rosén A, Persson F, et al. Whole-Body MRI Surveillance—Baseline Findings in the Swedish Multicentre Hereditary TP53-Related Cancer Syndrome Study (SWEP53). Cancers. 2022; 14(2):380. https://doi.org/10.3390/cancers14020380
Chicago/Turabian StyleOmran, Meis, Emma Tham, Yvonne Brandberg, Håkan Ahlström, Claudia Lundgren, Ylva Paulsson-Karlsson, Ekaterina Kuchinskaya, Gustav Silander, Anna Rosén, Fredrik Persson, and et al. 2022. "Whole-Body MRI Surveillance—Baseline Findings in the Swedish Multicentre Hereditary TP53-Related Cancer Syndrome Study (SWEP53)" Cancers 14, no. 2: 380. https://doi.org/10.3390/cancers14020380
APA StyleOmran, M., Tham, E., Brandberg, Y., Ahlström, H., Lundgren, C., Paulsson-Karlsson, Y., Kuchinskaya, E., Silander, G., Rosén, A., Persson, F., Leonhardt, H., Stenmark-Askmalm, M., Berg, J., van Westen, D., Bajalica-Lagercrantz, S., Blomqvist, L., & on behalf of the Swedish Clinical TP53 Study Group (SweClinTP53). (2022). Whole-Body MRI Surveillance—Baseline Findings in the Swedish Multicentre Hereditary TP53-Related Cancer Syndrome Study (SWEP53). Cancers, 14(2), 380. https://doi.org/10.3390/cancers14020380