
Afatinib Treatment Alone or with Bevacizumab in a Real-World Cohort of Non-Small Cell Lung Cancer Patients with Epidermal Growth Factor Receptor Mutation

 , , ,
, , ,
Abstract
Simple Summary
Abstract
1. Introduction
2. Methods
2.1. Patients and Treatment
2.2. Statistical Analysis
3. Results
3.1. Baseline Patient Characteristics
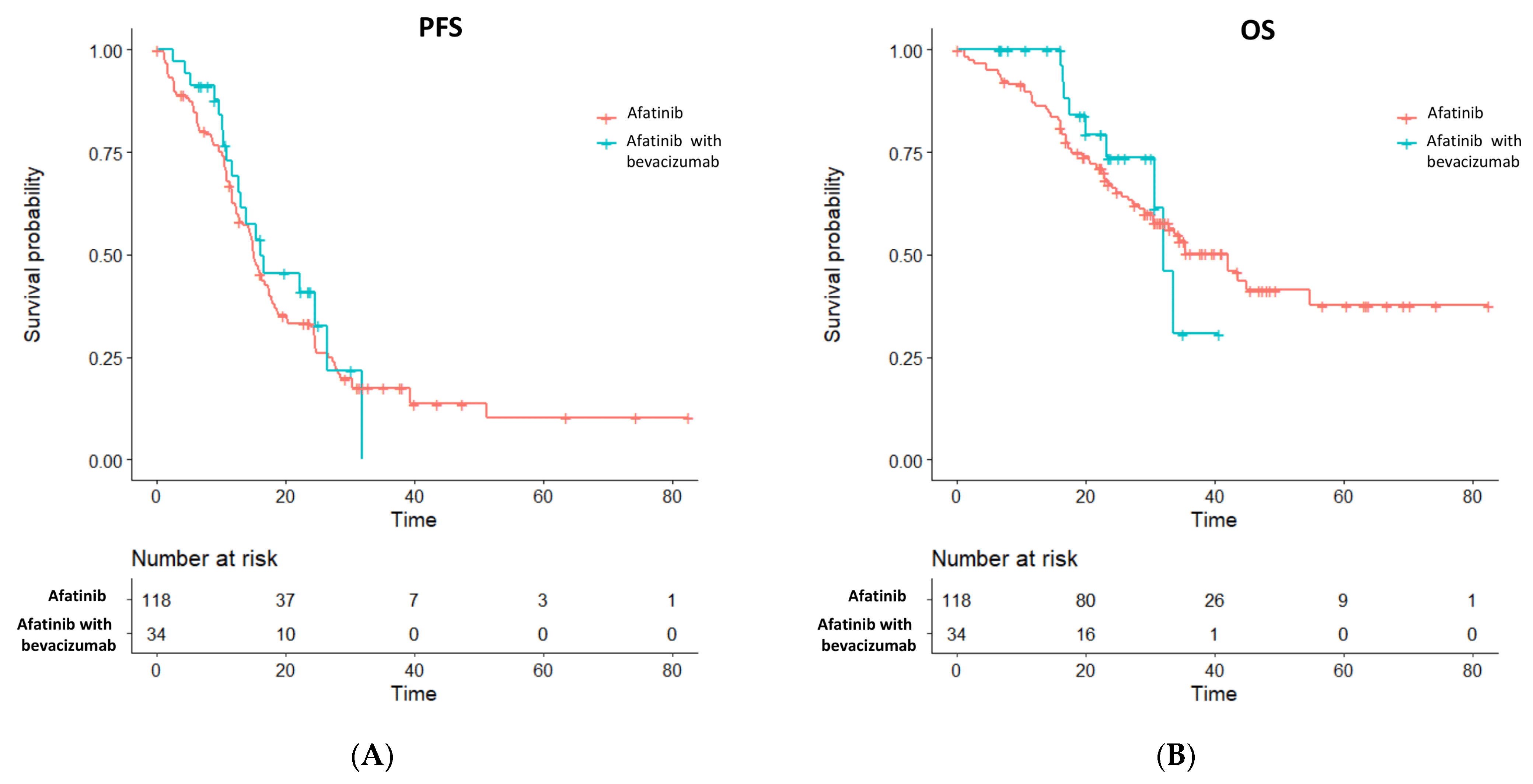
3.2. Efficacies of Bevacizumab in a Propensity Score-Matched Cohort
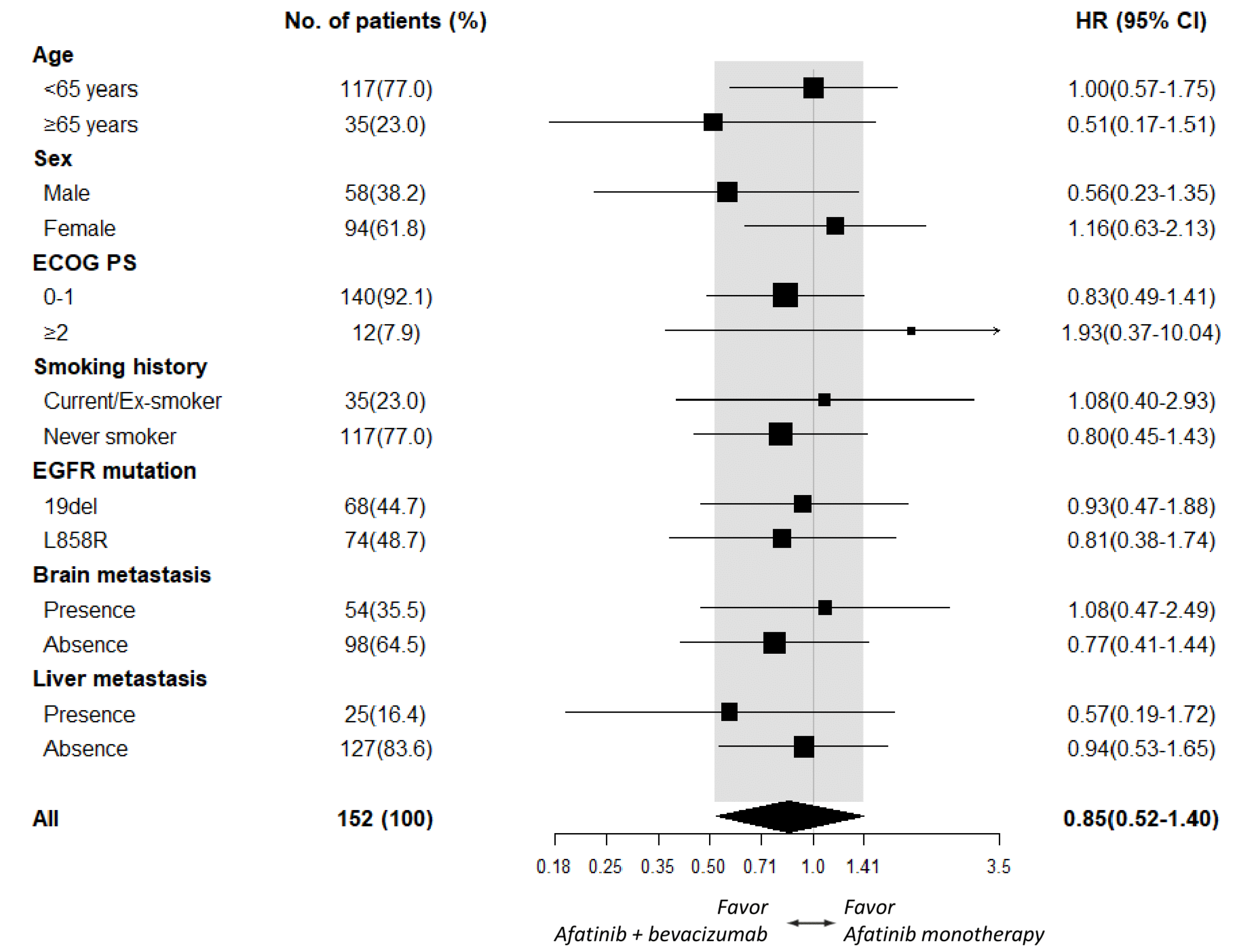
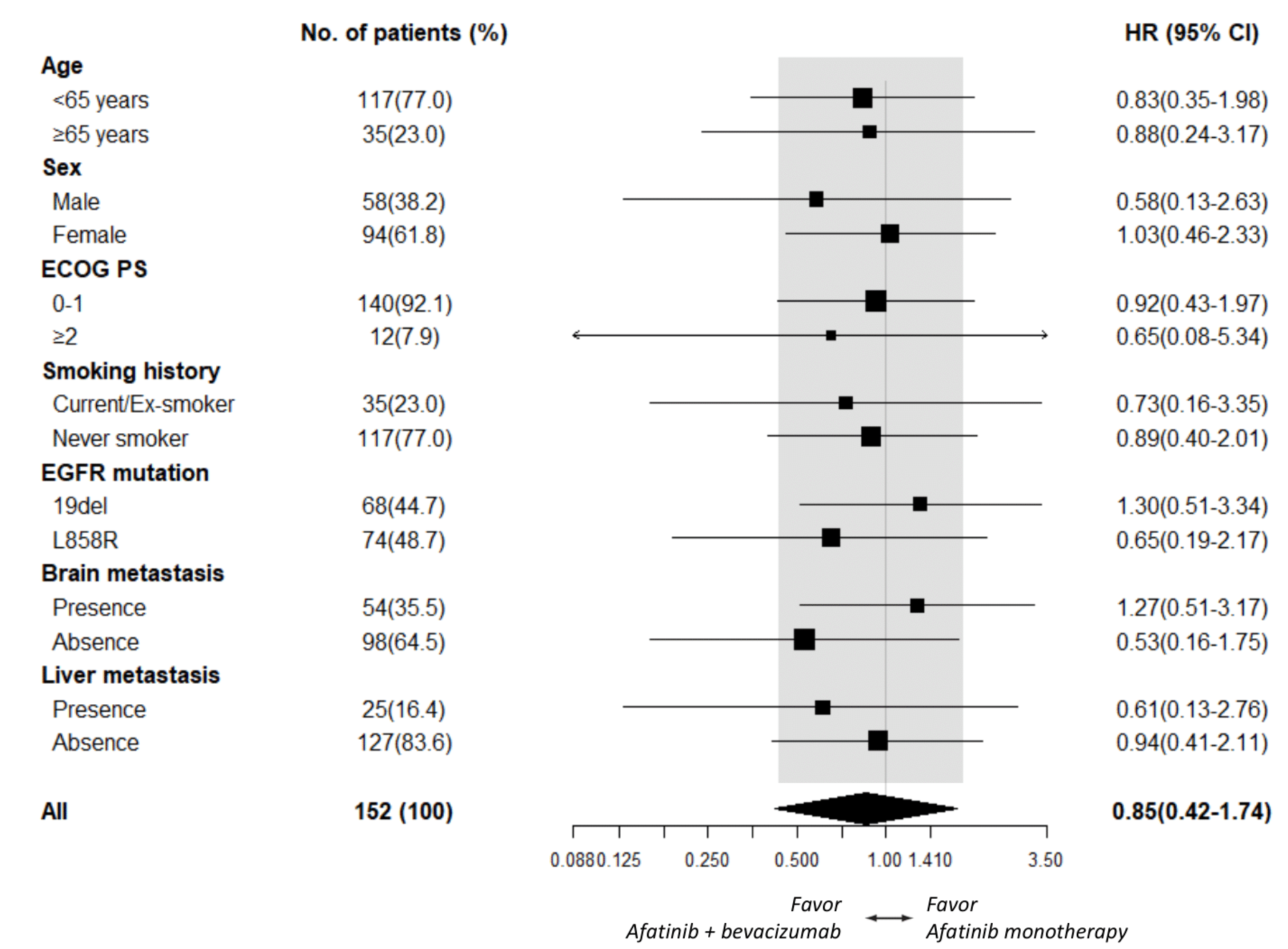
3.3. Subgroup Analysis of the Progression-Free and Overall Survival
3.4. Development of Secondary EGFR T790M Mutation
4. Discussion
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Paz-Ares, L.; Tan, E.-H.; O’Byrne, K.; Zhang, L.; Hirsh, V.; Boyer, M.; Yang, J.C.-H.; Mok, T.; Lee, K.H.; Lu, S.; et al. Afatinib versus gefitinib in patients with EGFR mutation-positive advanced non-small-cell lung cancer: Overall survival data from the phase IIb LUX-Lung 7 trial. Ann. Oncol. 2017, 28, 270–277. [Google Scholar] [CrossRef]
- Wu, Y.-L.; Cheng, Y.; Zhou, X.; Lee, K.H.; Nakagawa, K.; Niho, S.; Tsuji, F.; Linke, R.; Rosell, R.; Corral, J.; et al. Dacomitinib versus gefitinib as first-line treatment for patients with EGFR-mutation-positive non-small-cell lung cancer (ARCHER 1050): A randomised, open-label, phase 3 trial. Lancet Oncol. 2017, 18, 1454–1466. [Google Scholar] [CrossRef]
- Soria, J.-C.; Ohe, Y.; Vansteenkiste, J.; Reungwetwattana, T.; Chewaskulyong, B.; Lee, K.H.; Dechaphunkul, A.; Imamura, F.; Nogami, N.; Kurata, T.; et al. Osimertinib in Untreated EGFR-Mutated Advanced Non–Small-Cell Lung Cancer. N. Engl. J. Med. 2018, 378, 113–125. [Google Scholar] [CrossRef]
- Yang, Z.; Tam, K.Y. Combination Strategies Using EGFR-TKi in NSCLC Therapy: Learning from the Gap between Pre-Clinical Results and Clinical Outcomes. Int. J. Biol. Sci. 2018, 14, 204–216. [Google Scholar] [CrossRef] [PubMed]
- Sharma, S.V.; Bell, D.W.; Settleman, J.; Haber, D.A. Epidermal growth factor receptor mutations in lung cancer. Nat. Rev. Cancer 2007, 7, 169–181. [Google Scholar] [CrossRef] [PubMed]
- Dickson, P.V.; Hamner, J.B.; Sims, T.L.; Fraga, C.H.; Ng, C.Y.; Rajasekeran, S.; Hagedorn, N.L.; McCarville, M.B.; Stewart, C.F.; Davidoff, A.M. Bevacizumab-Induced Transient Remodeling of the Vasculature in Neuroblastoma Xenografts Results in Improved Delivery and Efficacy of Systemically Administered Chemotherapy. Clin. Cancer Res. 2007, 13, 3942–3950. [Google Scholar] [CrossRef] [PubMed]
- Wildiers, H.; Guetens, G.; De Boeck, G.; Verbeken, E.K.; Landuyt, B.; Landuyt, W.; A De Bruijn, E.; Van Oosterom, A.T. Effect of antivascular endothelial growth factor treatment on the intratumoral uptake of CPT-11. Br. J. Cancer 2003, 88, 1979–1986. [Google Scholar] [CrossRef] [PubMed]
- O’Connor, J.P.; Carano, R.A.; Clamp, A.R.; Ross, J.; Ho, C.C.; Jackson, A.; Parker, G.J.; Rose, C.J.; Peale, F.V.; Friesenhahn, M.; et al. Quantifying Antivascular Effects of Monoclonal Antibodies to Vascular Endothelial Growth Factor: Insights from Imaging. Clin. Cancer Res. 2009, 15, 6674–6682. [Google Scholar] [CrossRef] [PubMed]
- Larsen, A.K.; Ouaret, D.; El Ouadrani, K.; Petitprez, A. Targeting EGFR and VEGF(R) pathway cross-talk in tumor survival and angiogenesis. Pharmacol. Ther. 2011, 131, 80–90. [Google Scholar] [CrossRef]
- Saito, H.; Fukuhara, T.; Furuya, N.; Watanabe, K.; Sugawara, S.; Iwasawa, S.; Tsunezuka, Y.; Yamaguchi, O.; Okada, M.; Yoshimori, K.; et al. Erlotinib plus bevacizumab versus erlotinib alone in patients with EGFR-positive advanced non-squamous non-small-cell lung cancer (NEJ026): Interim analysis of an open-label, randomised, multicentre, phase 3 trial. Lancet Oncol. 2019, 20, 625–635. [Google Scholar] [CrossRef]
- Seto, T.; Kato, T.; Nishio, M.; Goto, K.; Atagi, S.; Hosomi, Y.; Yamamoto, N.; Hida, T.; Maemondo, M.; Nakagawa, K.; et al. Erlotinib alone or with bevacizumab as first-line therapy in patients with advanced non-squamous non-small-cell lung cancer harbouring EGFR mutations (JO25567): An open-label, randomised, multicentre, phase 2 study. Lancet Oncol. 2014, 15, 1236–1244. [Google Scholar] [CrossRef]
- Zhou, Q.; Wu, Y.L.; Cheng, Y.; Liu, Y.; Chen, G.; Cui, J.; Yang, N.; Song, Y.; Li, X.L.; Lu, S.; et al. 1480O-CTONG 1509: Phase III study of bevacizumab with or without erlotinib in untreated Chinese patients with advanced EGFR-mutated NSCLC. Ann. Oncol. 2019, 30, v603. [Google Scholar] [CrossRef]
- Stinchcombe, T.E.; Jänne, P.A.; Wang, X.; Bertino, E.M.; Weiss, J.; Bazhenova, L.; Gu, L.; Lau, C.; Paweletz, C.; Jaslowski, A.; et al. Effect of Erlotinib Plus Bevacizumab vs Erlotinib Alone on Progression-Free Survival in Patients With Advanced EGFR-Mutant Non-Small Cell Lung Cancer: A Phase 2 Randomized Clinical Trial. JAMA Oncol. 2019, 5, 1448–1455. [Google Scholar] [CrossRef] [PubMed]
- Ichihara, E.; Hotta, K.; Nogami, N.; Kuyama, S.; Kishino, D.; Fujii, M.; Kozuki, T.; Tabata, M.; Harada, D.; Chikamori, K.; et al. Phase II Trial of Gefitinib in Combination with Bevacizumab as First-Line Therapy for Advanced Non–Small Cell Lung Cancer with Activating EGFR Gene Mutations: The Okayama Lung Cancer Study Group Trial 1001. J. Thorac. Oncol. 2015, 10, 486–491. [Google Scholar] [CrossRef] [PubMed]
- Ito, K.; Murotani, K.; Kubo, A.; Kunii, E.; Taniguchi, H.; Shindoh, J.; Asada, K.; Imaizumi, K.; Takahashi, K.; Karayama, M.; et al. Propensity score analysis of overall survival between first- and second-generation EGFR-TKIs using real-world data. Cancer Sci. 2020, 111, 3705–3713. [Google Scholar] [CrossRef]
- Pluzanski, A.; Krzakowski, M.; Kowalski, D.; Dziadziuszko, R. Real-world clinical outcomes of first-generation and second-generation epidermal growth factor receptor tyrosine kinase inhibitors in a large cohort of European non-small-cell lung cancer patients. ESMO Open 2020, 5, e001011. [Google Scholar] [CrossRef]
- Su, V.Y.-F.; Yang, K.-Y.; Huang, T.-Y.; Hsu, C.-C.; Chen, Y.-M.; Yen, J.-C.; Chou, Y.-C.; Chang, Y.-L.; He, C.-H. The efficacy of first-line tyrosine kinase inhibitors combined with co-medications in Asian patients with EGFR mutation non-small cell lung cancer. Sci. Rep. 2020, 10, 1–14. [Google Scholar] [CrossRef]
- Ko, R.; Shukuya, T.; Imamura, C.K.; Tokito, T.; Shimada, N.; Koyama, R.; Yamada, K.; Ishii, H.; Azuma, K.; Takahashi, K. Phase I study of afatinib plus bevacizumab in patients with advanced non-squamous non-small cell lung cancer harboring EGFR mutations. Transl. Lung Cancer Res. 2021, 10, 183–192. [Google Scholar] [CrossRef]
- Ninomiya, T.; Nogami, N.; Kozuki, T.; Harada, D.; Kubo, T.; Ohashi, K.; Ichihara, E.; Kuyama, S.; Kudo, K.; Bessho, A.; et al. Survival of chemo-naïve patients with EGFR mutation-positive advanced non-small cell lung cancer after treatment with afatinib and bevacizumab: Updates from the Okayama Lung Cancer Study Group Trial 1404. Jpn. J. Clin. Oncol. 2021, 51, 1269–1276. [Google Scholar] [CrossRef]
- Hsu, P.-C.; Huang, C.-Y.; Wang, C.-C.; Kuo, S.C.-H.; Chu, C.-H.; Tung, P.-H.; Huang, A.C.-C.; Wang, C.-L.; Chiu, L.-C.; Fang, Y.-F.; et al. The Combination of Afatinib and Bevacizumab in Untreated EGFR-Mutated Advanced Lung Adenocarcinoma: A Multicenter Observational Study. Pharmaceuticals 2020, 13, 331. [Google Scholar] [CrossRef]
- Naumov, G.N.; Nilsson, M.B.; Cascone, T.; Briggs, A.; Straume, O.; Akslen, L.A.; Lifshits, E.; Byers, L.A.; Xu, L.; Wu, H.-K.; et al. Combined Vascular Endothelial Growth Factor Receptor and Epidermal Growth Factor Receptor (EGFR) Blockade Inhibits Tumor Growth in Xenograft Models of EGFR Inhibitor Resistance. Clin. Cancer Res. 2009, 15, 3484–3494. [Google Scholar] [CrossRef]
- Ichihara, E.; Ohashi, K.; Takigawa, N.; Osawa, M.; Ogino, A.; Tanimoto, M.; Kiura, K. Effects of Vandetanib on Lung Adenocarcinoma Cells Harboring Epidermal Growth Factor Receptor T790M Mutation in vivo. Cancer Res. 2009, 69, 5091–5098. [Google Scholar] [CrossRef] [PubMed][Green Version]
- Rosell, R.; Dafni, U.; Felip, E.; Curioni-Fontecedro, A.; Gautschi, O.; Peters, S.; Massuti, B.; Palmero, R.; Aix, S.P.; Carcereny, E.; et al. Erlotinib and bevacizumab in patients with advanced non-small-cell lung cancer and activating EGFR mutations (BELIEF): An international, multicentre, single-arm, phase 2 trial. Lancet Respir. Med. 2017, 5, 435–444. [Google Scholar] [CrossRef]
- Fukuhara, T.; Saito, H.; Furuya, N.; Watanabe, K.; Sugawara, S.; Iwasawa, S.; Tsunezuka, Y.; Yamaguchi, O.; Okada, M.; Yoshimori, K.; et al. Evaluation of plasma EGFR mutation as an early predictor of response of erlotinib plus bevacizumab treatment in the NEJ026 study. EBioMedicine 2020, 57, 102861. [Google Scholar] [CrossRef] [PubMed]
- Nakagawa, K.; Garon, E.B.; Seto, T.; Nishio, M.; Aix, S.P.; Paz-Ares, L.; Chiu, C.-H.; Park, K.; Novello, S.; Nadal, E.; et al. Ramucirumab plus erlotinib in patients with untreated, EGFR-mutated, advanced non-small-cell lung cancer (RELAY): A randomised, double-blind, placebo-controlled, phase 3 trial. Lancet Oncol. 2019, 20, 1655–1669. [Google Scholar] [CrossRef]
- Tsai, J.S.; Su, P.L.; Yang, S.C.; Chang, C.C.; Lin, C.Y.; Yen, Y.T.; Tseng, Y.L.; Lai, W.W.; Lin, C.C.; Su, W.C. EGFR-TKI plus bevacizumab versus EGFR-TKI monotherapy for patients with EGFR muta-tion-positive advanced non-small cell lung cancer-A propensity score matching analysis. J. Formos. Med. Assoc. 2021, 120, 1729–1739. [Google Scholar] [CrossRef]
- Piccirillo, M.C.; Bonanno, L.; Garassino, M.C.C.; Dazzi, C.; Cavanna, L.; Esposito, G.; Burgio, M.A.; Rosetti, F.; Rizzato, S.; Arenare, L.; et al. Bevacizumab + erlotinib vs erlotinib alone as first-line treatment of pts with EGFR mutated advanced non squamous NSCLC: Final analysis of the multicenter, randomized, phase III BEVERLY trial. Ann. Oncol. 2021, 32 (Suppl. 5), S949–S1039. [Google Scholar]
- Bagheri-Yarmand, R.; Vadlamudi, R.K.; Wang, R.A.; Mendelsohn, J.; Kumar, R. Vascular endothelial growth factor up-regulation via p21-activated kinase-1 signaling regulates heregulin-beta1-mediated angiogenesis. J. Biol. Chem. 2000, 275, 39451–39457. [Google Scholar] [CrossRef] [PubMed]
- Kumar, R.; Paul, A.M.; Amjesh, R.; George, B.; Pillai, M.R. Coordinated dysregulation of cancer progression by the HER family and p21-activated kinases. Cancer Metastasis Rev. 2020, 39, 583–601. [Google Scholar] [CrossRef]
- Mota, J.M.; Collier, K.A.; Costa, R.L.B.; Taxter, T.; Kalyan, A.; Leite, C.A.; Chae, Y.K.; Giles, F.J.; Carneiro, B.A. A comprehensive review of heregulins, HER3, and HER4 as potential therapeutic targets in cancer. Oncotarget 2017, 8, 89284–89306. [Google Scholar] [CrossRef] [PubMed]
- Yen, L.; You, X.-L.; Al Moustafa, A.-E.; Batist, G.; E Hynes, N.; Mader, S.; Meloche, S.; A Alaoui-Jamali, M. Heregulin selectively upregulates vascular endothelial growth factor secretion in cancer cells and stimulates angiogenesis. Oncogene 2000, 19, 3460–3469. [Google Scholar] [CrossRef] [PubMed]
- Russell, K.S.; Stern, D.F.; Polverini, P.J.; Bender, J.R. Neuregulin activation of ErbB receptors in vascular endothelium leads to angiogenesis. Am. J. Physiol. Content 1999, 277, H2205–H2211. [Google Scholar] [CrossRef] [PubMed]
- Iivanainen, E.; Heikkinen, S.M.; Junttila, T.T.; Klint, P.; Claesson-Welsh, L.; Cao, Y.; Elenius, K. Neuregulin-1 stimulates angiogenesis via paracrine up-regulation of VEGF-A expression. Cancer Res. 2005, 65 (Suppl. 9), 911. [Google Scholar]
- Agulnik, M.; Nelson, V.; Ziehr, J.; Johnson, M. Afatinib: Emerging next-generation tyrosine kinase inhibitor for NSCLC. OncoTargets Ther. 2013, 6, 135–143. [Google Scholar] [CrossRef] [PubMed]
- Ninomiya, T.; Takigawa, N.; Ichihara, E.; Ochi, N.; Murakami, T.; Honda, Y.; Kubo, T.; Minami, D.; Kudo, K.; Tanimoto, M.; et al. Afatinib Prolongs Survival Compared with Gefitinib in an Epidermal Growth Factor Receptor-Driven Lung Cancer Model. Mol. Cancer Ther. 2013, 12, 589–597. [Google Scholar] [CrossRef]
- Ramalingam, S.S.; Vansteenkiste, J.; Planchard, D.; Cho, B.C.; Gray, J.E.; Ohe, Y.; Zhou, C.; Reungwetwattana, T.; Cheng, Y.; Chewaskulyong, B.; et al. Overall Survival with Osimertinib in Untreated, EGFR-Mutated Advanced NSCLC. N. Engl. J. Med. 2020, 382, 41–50. [Google Scholar] [CrossRef]
- Helena, A.Y.; Schoenfeld, A.J.; Makhnin, A.; Kim, R.; Rizvi, H.; Tsui, D.; Falcon, C.; Houck-Loomis, B.; Meng, F.; Yang, J.L.; et al. Effect of Osimertinib and Bevacizumab on Progression-Free Survival for Patients With Metastatic EGFR-Mutant Lung Cancers: A Phase 1/2 Single-Group Open-Label Trial. JAMA Oncol. 2020, 6, 1048–1054. [Google Scholar]
- Ito, K.; Morise, M.; Wakuda, K.; Hataji, O.; Shimokawaji, T.; Takahashi, K.; Furuya, N.; Takeyama, Y.; Goto, Y.; Abe, T.; et al. A multicenter cohort study of osimertinib compared with afatinib as first-line treatment for EGFR-mutated non-small-cell lung cancer from practical dataset: CJLSG1903. ESMO Open 2021, 6, 100115. [Google Scholar] [CrossRef]




{kind=link}
{kind=link}
{kind=link}
| Varialbles | Total (%) N = 405 | Afatinib Plus Bevacizumab (%) N = 38 | Afatinib Alone (%) N = 367 | p Value |
|---|---|---|---|---|
| Age (mean ± SD) | 54.6 ± 10.9 | 63.9 ± 11.5 | <0.001 | |
| Age ≥ 65 | 180 (44.4) | 9 (23.7) | 171 (46.6) | 0.009 |
| ECOGPS 0-1 | 370 (91.4) | 36 (94.7) | 334 (91.0) | 0.760 |
| Gender | ||||
| Male | 161 (39.8) | 15 (39.5) | 146 (39.8) | 1.000 |
| Current/ex-smoker | 83 (20.5) | 8 (21.1) | 75 (20.4) | 1.000 |
| Histology | ||||
| Adenocarcinoma | 399 (98.5) | 37 (97.4) | 362 (98.6) | 0.449 |
| Others | 6 (1.5) | 1 (2.6) | 5 (1.4) | |
| EGFR mutation | ||||
| L858R | 185 (45.7) | 19 (50.0) | 166 (45.2) | 0.887 |
| 19deletion | 196 (48.4) | 17 (44.7) | 179 (48.8) | |
| Uncommon | 24 (5.9) | 2 (5.3) | 22 (6.0) | |
| Disease Stage | ||||
| III | 23 (5.7) | 0 | 23 (6.3) | 0.150 |
| IV | 382 (94.3) | 38 (100.0) | 344 (93.7) | |
| Site of Metastasis | ||||
| Brain | 121 (29.9) | 14 (36.8) | 107 (29.2) | 0.354 |
| Liver | 50 (12.3) | 6 (15.8) | 44 (12.0) | 0.445 |
| Varialbles | Total (%) N = 152 | Afatinib and Bevacizumab Combination (%) N = 34 | Afatinib Alone (%) N = 118 | p Value |
|---|---|---|---|---|
| Age (mean ± SD) | 56.0 ± 10.8 | 58.0 ± 9.2 | 0.341 | |
| Age ≥ 65 | 35 (23.0) | 9 (26.5) | 26 (22.0) | 0.645 |
| ECOG PS 0-1 | 140 (92.1) | 32 (94.1) | 108 (91.5) | 1.000 |
| Gender | ||||
| Male | 58 (38.2) | 14 (41.2) | 44 (37.3) | 0.693 |
| Current/ex-smoker | 35 (23.0) | 7 (20.6) | 28 (23.7) | 0.819 |
| Histology | ||||
| Adenocarcinoma | 150 (98.7) | 33 (97.1) | 117 (99.2) | 0.399 |
| Others | 2 (1.3) | 1 (2.9) | 1 (0.8) | |
| EGFR mutation | ||||
| L858R | 74 (48.7) | 16 (47.1) | 58 (49.2) | 0.952 |
| 19deletion | 68 (44.7) | 16 (47.1) | 52 (44.1) | |
| Uncommon | 10 (6.6) | 2 (5.8) | 8 (6.7) | |
| Disease Stage | ||||
| IV | 152 (100.0) | 34 (100.0) | 118 (100.0) | 1.000 |
| Site of Metastasis | ||||
| Brain | 54 (35.5) | 13 (38.2) | 41 (34.7) | 0.839 |
| Liver | 25 (16.4) | 6 (17.6) | 19 (16.1) | 0.798 |
| Afatinib dose reduction | 51 (33.6) | 12 (35.3) | 39 (33.1) | 0.838 |
| Variables, n (%) | Afatinib Plus Bevacizumab N = 34 | Afatinib Alone N = 118 |
|---|---|---|
| Response | ||
| No. of patients | 28 | 80 |
| % (95% CI) | 82.4 (65.4–93.2) | 67.8 (58.6–76.1) |
| Complete response—No. (%) | 0 | 2 (1.7) |
| Partial response—No. (%) | 28 (82.4) | 78 (66.1) |
| Stable disease—No. (%) | 4 (11.8) | 25 (21.2) |
| Progression disease—No. (%) | 2 (5.8) | 13 (11.0) |
| Median duration of response—month (95% CI) | 22.2 (13.0–not reach) | 17.8 (15.7–24.3) |
| Treatments, n (%) | Afatinib Plus Bevacizumab N = 34 | Afatinib Alone N = 118 |
|---|---|---|
| Third-generation EGFR-TKI | 12 (35.3) | 33 (28.0) |
| Chemotherapy | 9 (26.5) | 38 (32.2) |
| Immune checkpoint inhibitor | 2 (5.9) | 6 (5.1) |
| Other TKIs | 3 (8.8) | 16 (13.6) |
| Variables | Univariate Analysis | Mutivariate Analysis | ||
|---|---|---|---|---|
| Odd Ratio (95% C.I.) | p-Value | Odd Ratio (95% C.I.) | p-Value | |
| Age ≥ 65 | 0.95 (0.51–1.77) | 0.874 | -- | -- |
| Male | 0.62 (0.33–1.13) | 0.122 | 0.59 (0.31–1.13) | 0.111 |
| ECOG PS 0-1 | 1.00 (0.27–3.72) | 1.000 | -- | -- |
| Current/ex-smoker | 0.60 (0.29–1.21) | 0.157 | -- | -- |
| EGFR L858R mutation | 0.62 (0.33–1.16) | 0.137 | 0.51 (0.26–0.97) | 0.044 |
| EGFR uncommon mutation | 0.21 (0.03–0.94) | 0.063 | 0.14 (0.02–0.64) | 0.021 |
| Brain metastasis | 1.02 (0.52–1.96) | 0.959 | -- | -- |
| Liver metastasis | 0.90 (0.35–2.25) | 0.816 | -- | -- |
| PFS ≥ 12 months | 2.40 (1.27–4.60) | 0.008 | 2.71 (1.39–5.41) | 0.004 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Kuo, C.-H.S.; Chiu, T.-H.; Tung, P.-H.; Huang, C.-H.; Ju, J.-S.; Huang, A.C.-C.; Wang, C.-C.; Ko, H.-W.; Hsu, P.-C.; Fang, Y.-F.; et al. Afatinib Treatment Alone or with Bevacizumab in a Real-World Cohort of Non-Small Cell Lung Cancer Patients with Epidermal Growth Factor Receptor Mutation. Cancers 2022, 14, 316. https://doi.org/10.3390/cancers14020316
Kuo C-HS, Chiu T-H, Tung P-H, Huang C-H, Ju J-S, Huang AC-C, Wang C-C, Ko H-W, Hsu P-C, Fang Y-F, et al. Afatinib Treatment Alone or with Bevacizumab in a Real-World Cohort of Non-Small Cell Lung Cancer Patients with Epidermal Growth Factor Receptor Mutation. Cancers. 2022; 14(2):316. https://doi.org/10.3390/cancers14020316
Chicago/Turabian StyleKuo, Chih-Hsi Scott, Tzu-Hsuan Chiu, Pi-Hung Tung, Chi-Hsien Huang, Jia-Shiuan Ju, Allen Chung-Cheng Huang, Chin-Chou Wang, Ho-Wen Ko, Ping-Chih Hsu, Yueh-Fu Fang, and et al. 2022. "Afatinib Treatment Alone or with Bevacizumab in a Real-World Cohort of Non-Small Cell Lung Cancer Patients with Epidermal Growth Factor Receptor Mutation" Cancers 14, no. 2: 316. https://doi.org/10.3390/cancers14020316
APA StyleKuo, C.-H. S., Chiu, T.-H., Tung, P.-H., Huang, C.-H., Ju, J.-S., Huang, A. C.-C., Wang, C.-C., Ko, H.-W., Hsu, P.-C., Fang, Y.-F., Guo, Y.-K., & Yang, C.-T. (2022). Afatinib Treatment Alone or with Bevacizumab in a Real-World Cohort of Non-Small Cell Lung Cancer Patients with Epidermal Growth Factor Receptor Mutation. Cancers, 14(2), 316. https://doi.org/10.3390/cancers14020316