
Levels of Evidence Supporting United States Guidelines in Pancreatic Adenocarcinoma Treatment


Abstract
:Simple Summary
Abstract
1. Introduction
2. Methods
2.1. Data Sources and Search Strategy
2.2. Eligibility Criteria for Current Guidelines
2.3. Search Strategy and Eligibility for Prior Guidelines
2.4. Data Extraction and Presentation
2.5. Classification of Evidence (Level of Evidence and Class of Recommendation)
2.5.1. Definition of High Level of Evidence (LOE)
- − “high” quality of evidence from the GRADE methodology used in the ASCO guidelines (confidence that the true effect lies close to that of the estimate), and
- − “Category 1” from the NCCN guidelines (high-level evidence).
2.5.2. Class of Recommendation
2.6. Outcome Measures
2.6.1. Primary Outcome Measure
2.6.2. Secondary Outcome Measures
3. Results
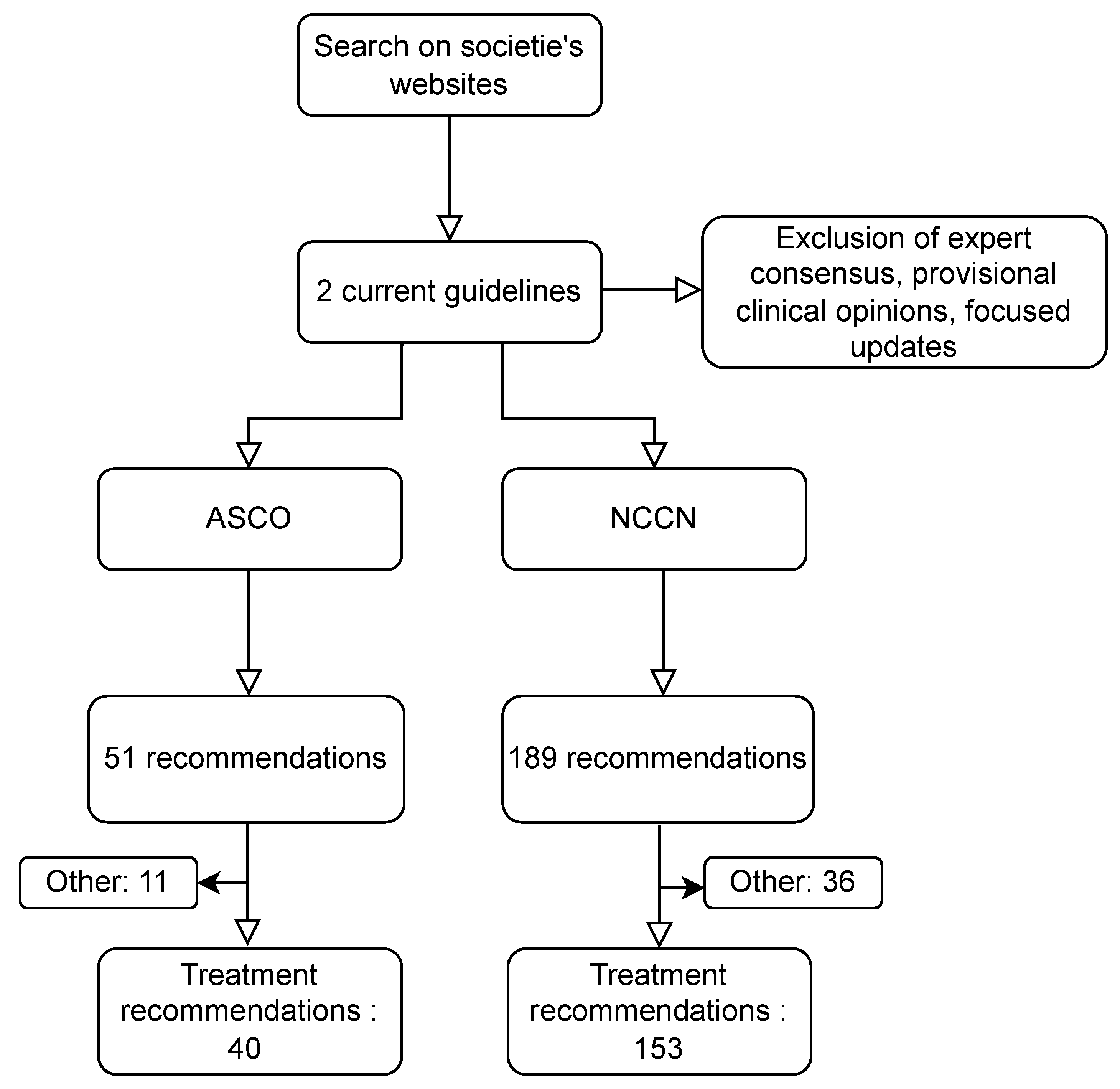
3.1. Characteristics of Current Guidelines
3.2. Outcome Results
3.2.1. Primary Outcome Measure
3.2.2. Secondary Outcome Measures
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
Appendix A. Search Strategy
References
- Bray, F.; Ferlay, J.; Soerjomataram, I.; Siegel, R.L.; Torre, L.A.; Jemal, A. Global Cancer Statistics 2018: GLOBOCAN Estimates of Incidence and Mortality Worldwide for 36 Cancers in 185 Countries. CA Cancer J. Clin. 2018, 68, 394–424. [Google Scholar] [CrossRef] [PubMed]
- Rawla, P.; Sunkara, T.; Gaduputi, V. Epidemiology of Pancreatic Cancer: Global Trends, Etiology and Risk Factors. World J. Oncol. 2019, 10, 10–27. [Google Scholar] [CrossRef] [PubMed]
- Gaddam, S.; Abboud, Y.; Oh, J.; Samaan, J.S.; Nissen, N.N.; Lu, S.C.; Lo, S.K. Incidence of Pancreatic Cancer by Age and Sex in the US, 2000–2018. JAMA 2021, 326, 2075–2077. [Google Scholar] [CrossRef] [PubMed]
- Huang, J.; Lok, V.; Ngai, C.H.; Zhang, L.; Yuan, J.; Lao, X.Q.; Ng, K.; Chong, C.; Zheng, Z.-J.; Wong, M.C.S. Worldwide Burden of, Risk Factors for, and Trends in Pancreatic Cancer. Gastroenterology 2021, 160, 744–754. [Google Scholar] [CrossRef]
- Pluchino, L.A.; D’Amico, T.A. National Comprehensive Cancer Network Guidelines: Who Makes Them? What Are They? Why Are They Important? Ann. Thorac. Surg. 2020, 110, 1789–1795. [Google Scholar] [CrossRef]
- Evidence-Based Medicine Working Group Evidence-Based Medicine. A New Approach to Teaching the Practice of Medicine. JAMA 1992, 268, 2420–2425. [Google Scholar] [CrossRef]
- Balshem, H.; Helfand, M.; Schünemann, H.J.; Oxman, A.D.; Kunz, R.; Brozek, J.; Vist, G.E.; Falck-Ytter, Y.; Meerpohl, J.; Norris, S.; et al. GRADE Guidelines: 3. Rating the Quality of Evidence. J. Clin. Epidemiol. 2011, 64, 401–406. [Google Scholar] [CrossRef]
- Guyatt, G.H.; Oxman, A.D.; Vist, G.; Kunz, R.; Brozek, J.; Alonso-Coello, P.; Montori, V.; Akl, E.A.; Djulbegovic, B.; Falck-Ytter, Y.; et al. GRADE Guidelines: 4. Rating the Quality of Evidence—Study Limitations (Risk of Bias). J. Clin. Epidemiol. 2011, 64, 407–415. [Google Scholar] [CrossRef]
- Guyatt, G.H.; Oxman, A.D.; Montori, V.; Vist, G.; Kunz, R.; Brozek, J.; Alonso-Coello, P.; Djulbegovic, B.; Atkins, D.; Falck-Ytter, Y.; et al. GRADE Guidelines: 5. Rating the Quality of Evidence—Publication Bias. J. Clin. Epidemiol. 2011, 64, 1277–1282. [Google Scholar] [CrossRef]
- Guyatt, G.H.; Oxman, A.D.; Kunz, R.; Brozek, J.; Alonso-Coello, P.; Rind, D.; Devereaux, P.J.; Montori, V.M.; Freyschuss, B.; Vist, G.; et al. GRADE Guidelines 6. Rating the Quality of Evidence—Imprecision. J. Clin. Epidemiol. 2011, 64, 1283–1293. [Google Scholar] [CrossRef]
- Guyatt, G.H.; Oxman, A.D.; Kunz, R.; Woodcock, J.; Brozek, J.; Helfand, M.; Alonso-Coello, P.; Glasziou, P.; Jaeschke, R.; Akl, E.A.; et al. GRADE Guidelines: 7. Rating the Quality of Evidence—Inconsistency. J. Clin. Epidemiol. 2011, 64, 1294–1302. [Google Scholar] [CrossRef]
- Guyatt, G.H.; Oxman, A.D.; Kunz, R.; Woodcock, J.; Brozek, J.; Helfand, M.; Alonso-Coello, P.; Falck-Ytter, Y.; Jaeschke, R.; Vist, G.; et al. GRADE Guidelines: 8. Rating the Quality of Evidence—Indirectness. J. Clin. Epidemiol. 2011, 64, 1303–1310. [Google Scholar] [CrossRef] [PubMed]
- Guyatt, G.H.; Oxman, A.D.; Sultan, S.; Glasziou, P.; Akl, E.A.; Alonso-Coello, P.; Atkins, D.; Kunz, R.; Brozek, J.; Montori, V.; et al. GRADE Guidelines: 9. Rating up the Quality of Evidence. J. Clin. Epidemiol. 2011, 64, 1311–1316. [Google Scholar] [CrossRef] [PubMed]
- Guyatt, G.; Oxman, A.D.; Sultan, S.; Brozek, J.; Glasziou, P.; Alonso-Coello, P.; Atkins, D.; Kunz, R.; Montori, V.; Jaeschke, R.; et al. GRADE Guidelines: 11. Making an Overall Rating of Confidence in Effect Estimates for a Single Outcome and for All Outcomes. J. Clin. Epidemiol. 2013, 66, 151–157. [Google Scholar] [CrossRef]
- Andrews, J.; Guyatt, G.; Oxman, A.D.; Alderson, P.; Dahm, P.; Falck-Ytter, Y.; Nasser, M.; Meerpohl, J.; Post, P.N.; Kunz, R.; et al. GRADE Guidelines: 14. Going from Evidence to Recommendations: The Significance and Presentation of Recommendations. J. Clin. Epidemiol. 2013, 66, 719–725. [Google Scholar] [CrossRef]
- Andrews, J.C.; Schünemann, H.J.; Oxman, A.D.; Pottie, K.; Meerpohl, J.J.; Coello, P.A.; Rind, D.; Montori, V.M.; Brito, J.P.; Norris, S.; et al. GRADE Guidelines: 15. Going from Evidence to Recommendation-Determinants of a Recommendation’s Direction and Strength. J. Clin. Epidemiol. 2013, 66, 726–735. [Google Scholar] [CrossRef] [PubMed]
- Halperin, J.L.; Levine, G.N.; Al-Khatib, S.M.; Birtcher, K.K.; Bozkurt, B.; Brindis, R.G.; Cigarroa, J.E.; Curtis, L.H.; Fleisher, L.A.; Gentile, F.; et al. Further Evolution of the ACC/AHA Clinical Practice Guideline Recommendation Classification System: A Report of the American College of Cardiology/American Heart Association Task Force on Clinical Practice Guidelines. J. Am. Coll. Cardiol. 2016, 67, 1572–1574. [Google Scholar] [CrossRef] [PubMed]
- Takaori, K.; Bassi, C.; Biankin, A.; Brunner, T.B.; Cataldo, I.; Campbell, F.; Cunningham, D.; Falconi, M.; Frampton, A.E.; Furuse, J.; et al. International Association of Pancreatology (IAP)/European Pancreatic Club (EPC) Consensus Review of Guidelines for the Treatment of Pancreatic Cancer. Pancreatology 2016, 16, 14–27. [Google Scholar] [CrossRef]
- Li, C.C.; Wang, Y.Q.; Li, Y.P.; Li, X.L. Critical Appraisal of Clinical Practice Guidelines for Treating Pancreatic Cancer Based on the Global Disease Burden. J. Evid. Based Med. 2015, 8, 11–21. [Google Scholar] [CrossRef]
- Liu, X.-J.; Yang, T.; Shi, X.; Xiao, B.-H.; An, L.-Y.; Zheng, S.-Y.; Qi, Y.-X.; Sun, D.-L. Systematic Appraisal of Guidelines for the Diagnosis of Pancreatic Cancer. Gland. Surg. 2021, 10, 1487–1498. [Google Scholar] [CrossRef]
- Desai, A.P.; Go, R.S.; Poonacha, T.K. Category of Evidence and Consensus Underlying National Comprehensive Cancer Network Guidelines: Is There Evidence of Progress? Int. J. Cancer 2021, 148, 429–436. [Google Scholar] [CrossRef] [PubMed]
- Moses, H.; Dorsey, E.R.; Matheson, D.H.M.; Thier, S.O. Financial Anatomy of Biomedical Research. JAMA 2005, 294, 1333–1342. [Google Scholar] [CrossRef] [PubMed]
- Tunis, S.R.; Stryer, D.B.; Clancy, C.M. Practical Clinical Trials: Increasing the Value of Clinical Research for Decision Making in Clinical and Health Policy. JAMA 2003, 290, 1624–1632. [Google Scholar] [CrossRef] [PubMed]
- Boutron, I.; Créquit, P.; Williams, H.; Meerpohl, J.; Craig, J.C.; Ravaud, P. Future of Evidence Ecosystem Series: 1. Introduction Evidence Synthesis Ecosystem Needs Dramatic Change. J. Clin. Epidemiol. 2020, 123, 135–142. [Google Scholar] [CrossRef]
- Créquit, P.; Boutron, I.; Meerpohl, J.; Williams, H.C.; Craig, J.; Ravaud, P. Future of Evidence Ecosystem Series: 2. Current Opportunities and Need for Better Tools and Methods. J. Clin. Epidemiol. 2020, 123, 143–152. [Google Scholar] [CrossRef]
- Ross, J.S. Randomized Clinical Trials and Observational Studies Are More Often Alike Than Unlike. JAMA Intern. Med. 2014, 174, 1557. [Google Scholar] [CrossRef] [PubMed]
- Faraoni, D.; Schaefer, S.T. Randomized Controlled Trials vs. Observational Studies: Why Not Just Live Together? BMC Anesthesiol. 2016, 16, 102. [Google Scholar] [CrossRef]
- Feinstein, A. The Role of Observational Studies in the Evaluation of Therapy. Stat. Med. 1984, 3, 341–345. [Google Scholar] [CrossRef]
- Lauer, M.S.; D’Agostino, R.B. The Randomized Registry Trial—the next Disruptive Technology in Clinical Research? N. Engl. J. Med. 2013, 369, 1579–1581. [Google Scholar] [CrossRef]
- James, S.; Rao, S.V.; Granger, C.B. Registry-Based Randomized Clinical Trials—a New Clinical Trial Paradigm. Nat. Rev. Cardiol. 2015, 12, 312–316. [Google Scholar] [CrossRef]



{kind=link}
{kind=link}
{kind=link}
| ASCO | NCCN | |||||
|---|---|---|---|---|---|---|
| Level of Evidence | Total | High | Other | Total | High | Other |
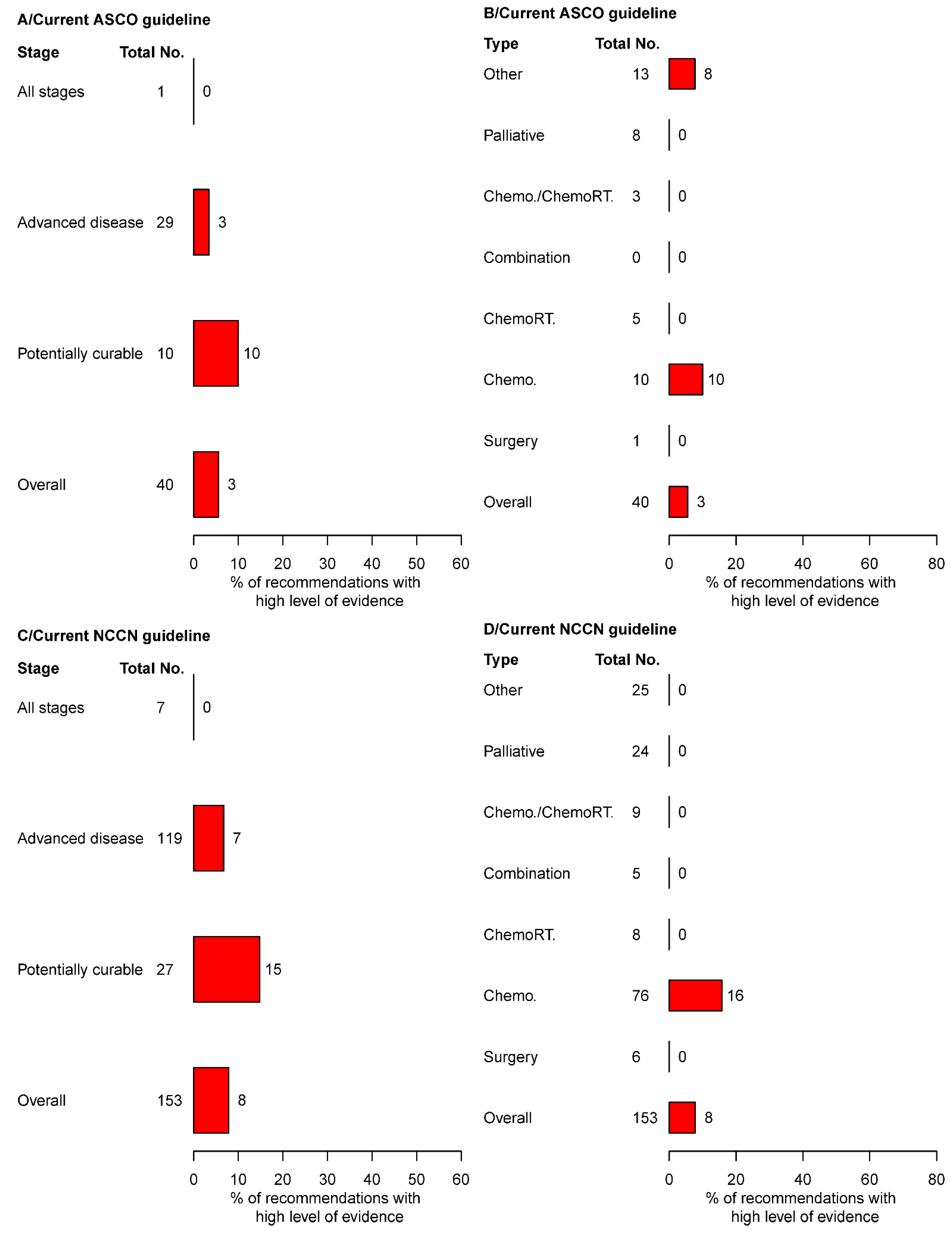
| Therapeutic recommendations | 40 | 2 | 38 | 153 | 12 | 141 |
| Disease stage | ||||||
| Potentially curable | 10 | 1 | 9 | 27 | 4 | 23 |
| Advanced | 29 | 1 | 28 | 119 | 8 | 111 |
| All stages | 1 | 0 | 1 | 7 | 0 | 7 |
| Treatment category | ||||||
| Surgery | 1 | 0 | 1 | 6 | 0 | 6 |
| Chemotherapy | 10 | 1 | 9 | 76 | 12 | 64 |
| Chemoradiotherapy | 5 | 0 | 5 | 8 | 0 | 8 |
| Combination | 0 | 0 | 0 | 5 | 0 | 5 |
| Chemotherapy or chemoradiotherapy | 3 | 0 | 3 | 9 | 0 | 9 |
| Palliative | 8 | 0 | 8 | 24 | 0 | 24 |
| Other | 13 | 1 | 12 | 25 | 0 | 25 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Pellat, A.; Boutron, I.; Coriat, R.; Ravaud, P. Levels of Evidence Supporting United States Guidelines in Pancreatic Adenocarcinoma Treatment. Cancers 2022, 14, 4062. https://doi.org/10.3390/cancers14164062
Pellat A, Boutron I, Coriat R, Ravaud P. Levels of Evidence Supporting United States Guidelines in Pancreatic Adenocarcinoma Treatment. Cancers. 2022; 14(16):4062. https://doi.org/10.3390/cancers14164062
Chicago/Turabian StylePellat, Anna, Isabelle Boutron, Romain Coriat, and Philippe Ravaud. 2022. "Levels of Evidence Supporting United States Guidelines in Pancreatic Adenocarcinoma Treatment" Cancers 14, no. 16: 4062. https://doi.org/10.3390/cancers14164062
APA StylePellat, A., Boutron, I., Coriat, R., & Ravaud, P. (2022). Levels of Evidence Supporting United States Guidelines in Pancreatic Adenocarcinoma Treatment. Cancers, 14(16), 4062. https://doi.org/10.3390/cancers14164062