
Does the New FIGO 2018 Staging System Allow Better Prognostic Differentiation in Early Stage Cervical Cancer? A Dutch Nationwide Cohort Study


 , , and
, , and
Abstract
:Simple Summary
Abstract
1. Introduction
2. Methods
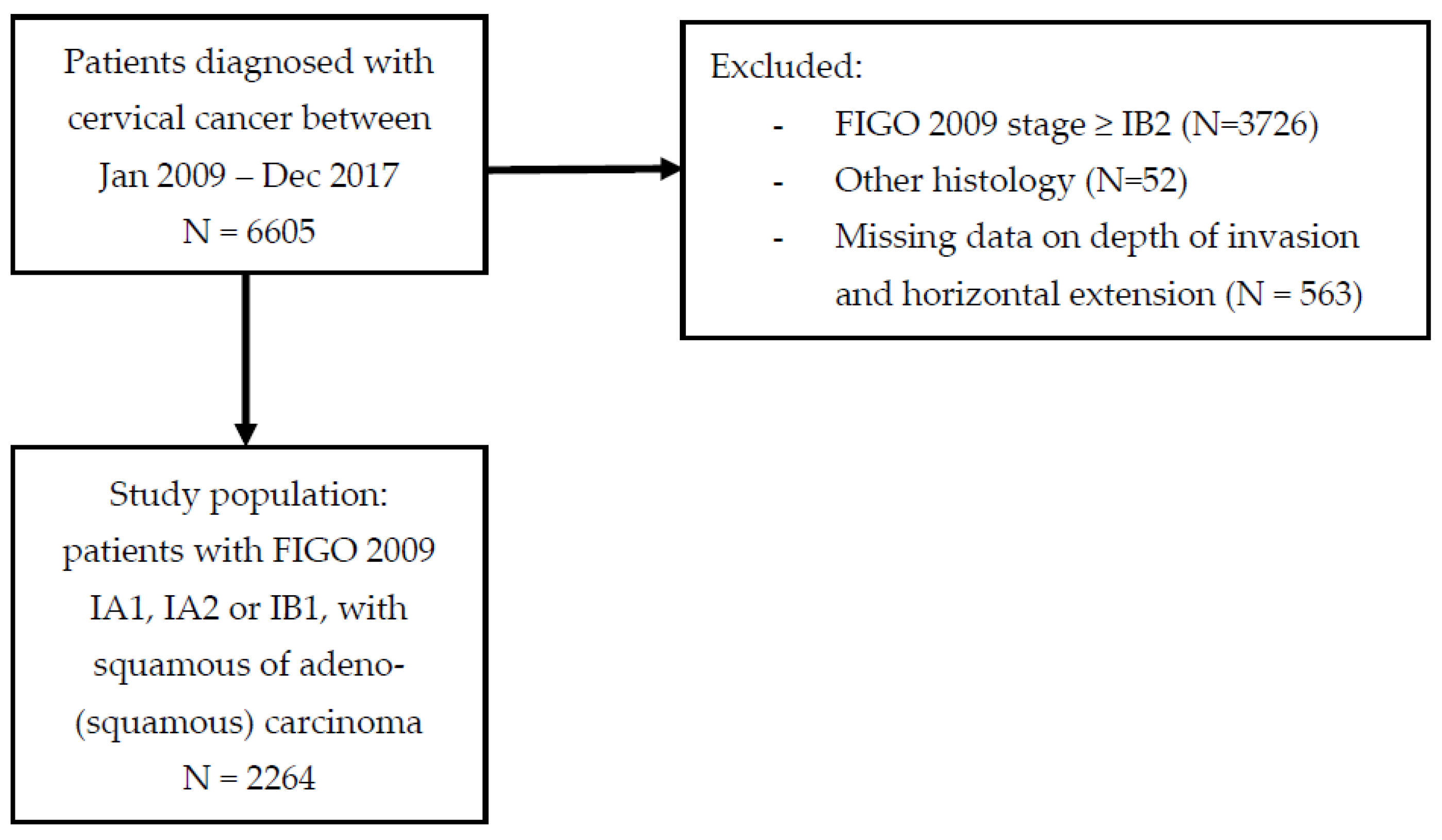
2.1. Study Design and Population
2.2. Data Collection and Outcome Measures
2.3. Statistical Analyses
3. Results
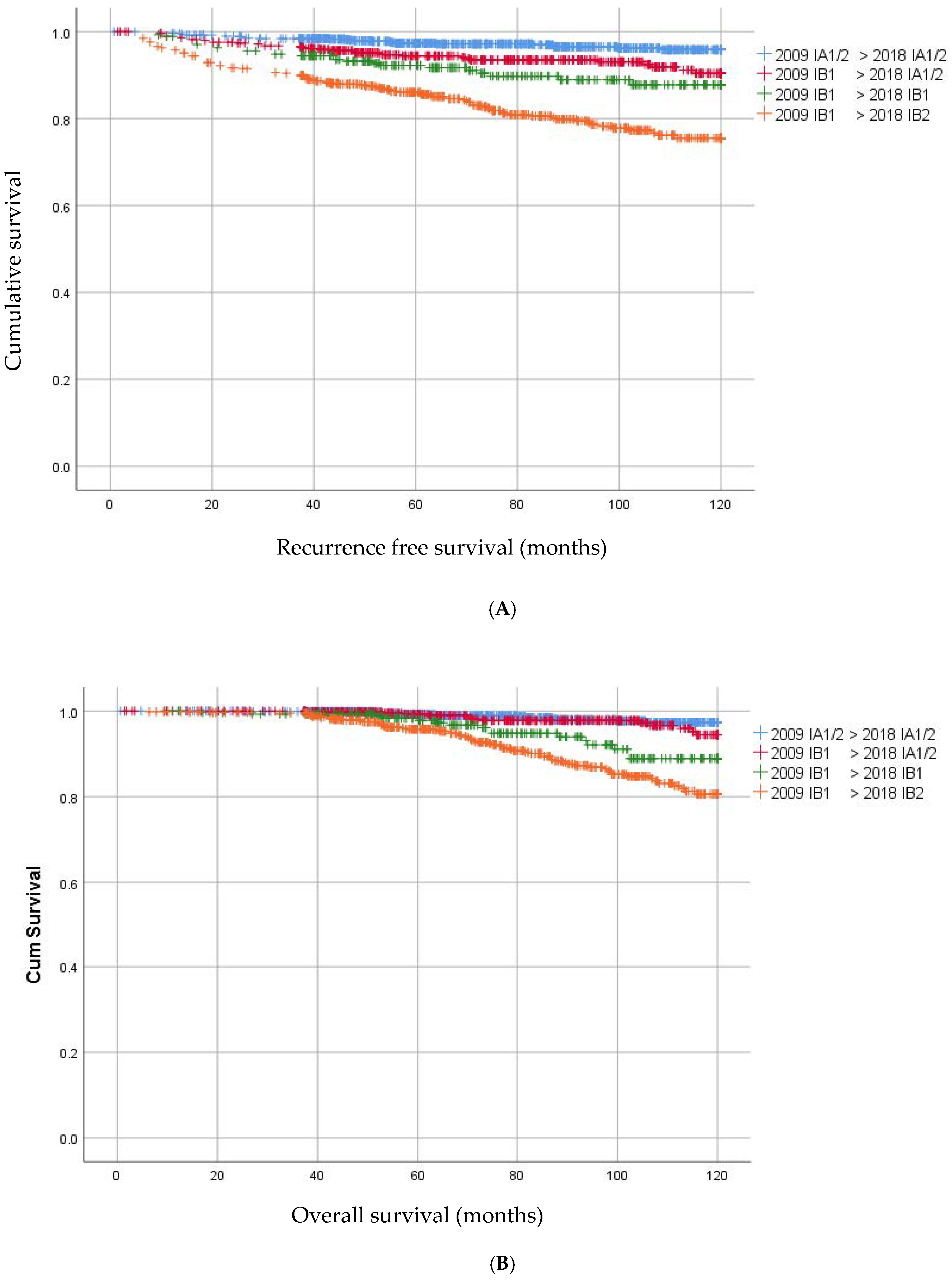
3.1. Survival and Recurrence Analyses
3.2. Parametrial Invasion
3.3. Lymph Node Involvement
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Pecorelli, S. Revised FIGO staging for carcinoma of the vulva, cervix, and endometrium. Int. J. Gynaecol. Obstet. 2009, 105, 103–104. [Google Scholar] [CrossRef] [PubMed]
- Bhatla, N.; Berek, J.S.; Cuello Fredes, M.; Denny, L.A.; Grenman, S.; Karunaratne, K.; Kehoe, S.T.; Konishi, I.; Olawaiye, A.B.; Prat, J.; et al. Revised FIGO staging for carcinoma of the cervix uteri. Int. J. Gynaecol. Obstet. 2019, 145, 129–135. [Google Scholar] [CrossRef] [PubMed]
- Sponholtz, S.E.; Mogensen, O.; Hildebrandt, M.G.; Schledermann, D.; Parner, E.; Markauskas, A.; Froding, L.P.; Fuglsang, K.; Holm, J.; Bjornholt, S.M.; et al. From FIGO-2009 to FIGO-2018 in women with early-stage cervical cancer; Does the revised staging reflect risk groups? Gynecol. Oncol. 2021, 163, 281–288. [Google Scholar] [CrossRef]
- Schmeler, K.M.; Frumovitz, M.; Ramirez, P.T. Conservative management of early stage cervical cancer: Is there a role for less radical surgery? Gynecol. Oncol. 2011, 120, 321–325. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Matsuo, K.; Machida, H.; Mandelbaum, R.S.; Konishi, I.; Mikami, M. Validation of the 2018 FIGO cervical cancer staging system. Gynecol. Oncol. 2019, 152, 87–93. [Google Scholar] [CrossRef]
- Margolis, B.; Cagle-Colon, K.; Chen, L.; Tergas, A.I.; Boyd, L.; Wright, J.D. Prognostic significance of lymphovascular space invasion for stage IA1 and IA2 cervical cancer. Int. J. Gynecol. Cancer 2020, 30, 735–743. [Google Scholar] [CrossRef]
- Wenzel, H.H.B.; Van Kol, K.G.G.; Nijman, H.W.; Lemmens, V.; Van der Aa, M.A.; Ebisch, R.M.F.; Bekkers, R.L.M. Cervical cancer with ≤5 mm depth of invasion and >7 mm horizontal spread—Is lymph node assessment only required in patients with LVSI? Gynecol. Oncol. 2020, 158, 282–286. [Google Scholar] [CrossRef]
- Wright, J.D.; Matsuo, K.; Huang, Y.; Tergas, A.I.; Hou, J.Y.; Khoury-Collado, F.; St Clair, C.M.; Ananth, C.V.; Neugut, A.I.; Hershman, D.L. Prognostic Performance of the 2018 International Federation of Gynecology and Obstetrics Cervical Cancer Staging Guidelines. Obstet. Gynecol. 2019, 134, 49–57. [Google Scholar] [CrossRef]
- Du, R.X.; Li, L.; Ma, S.Q.; Tan, X.J.; Zhong, S.; Wu, M. Lymph nodes metastasis in cervical cancer: Incidences, risk factors, consequences and imaging evaluations. Asia-Pac. J. Clin. Oncol. 2018, 14, e380–e385. [Google Scholar] [CrossRef] [Green Version]
- Nanthamongkolkul, K.; Hanprasertpong, J. Predictive Factors of Pelvic Lymph Node Metastasis in Early-Stage Cervical Cancer. Oncol. Res. Treat. 2018, 41, 194–198. [Google Scholar] [CrossRef]
- Kato, H.; Todo, Y.; Suzuki, Y.; Ohba, Y.; Minobe, S.; Okamoto, K.; Yamashiro, K.; Sakuragi, N. Re-consideration of lymphadenectomy for stage Ib1 cervical cancer. J. Obstet. Gynaecol. Res. 2012, 38, 420–426. [Google Scholar] [CrossRef]
- Milam, M.R.; Frumovitz, M.; dos Reis, R.; Broaddus, R.R.; Bassett, R.L., Jr.; Ramirez, P.T. Preoperative lymph-vascular space invasion is associated with nodal metastases in women with early-stage cervical cancer. Gynecol. Oncol. 2007, 106, 12–15. [Google Scholar] [CrossRef] [PubMed]
- Togami, S.; Kamio, M.; Yanazume, S.; Yoshinaga, M.; Douchi, T. Can pelvic lymphadenectomy be omitted in stage IA2 to IIB uterine cervical cancer? Int. J. Gynecol. Cancer 2014, 24, 1072–1076. [Google Scholar] [CrossRef] [PubMed]
- Wang, Y.; Yao, T.; Yu, J.; Li, J.; Chen, Q.; Lin, Z. Can pelvic lymphadenectomy be omitted in patients with stage IA2, IB1, and IIA1 squamous cell cervical cancer? Springerplus 2016, 5, 1262. [Google Scholar] [CrossRef] [Green Version]
- Buchanan, T.; Pierce, J.Y.; Graybill, W.; Kohler, M.; Creasman, W. Why do we continue to overtreat stage Ia carcinoma of the cervix? Am. J. Obstet. Gynecol. 2017, 217, 413–417. [Google Scholar] [CrossRef] [PubMed]
- van Meurs, H.; Visser, O.; Buist, M.R.; Ten Kate, F.J.; van der Velden, J. Frequency of pelvic lymph node metastases and parametrial involvement in stage IA2 cervical cancer: A population-based study and literature review. Int. J. Gynecol. Cancer 2009, 19, 21–26. [Google Scholar] [CrossRef]
- Widschwendter, P.; Janni, W.; Scholz, C.; De Gregorio, A.; De Gregorio, N.; Friedl, T.W.P. Prognostic factors for and pattern of lymph-node involvement in patients with operable cervical cancer. Arch. Gynecol. Obstet. 2019, 300, 1709–1718. [Google Scholar] [CrossRef]
- Benedetti-Panici, P.; Maneschi, F.; D’Andrea, G.; Cutillo, G.; Rabitti, C.; Congiu, M. Early cervical carcinoma: The natural history of lymph node involvement redefined on the basis of thorough parametrectomy and giant section study. Cancer 2000, 88, 2267–2274. [Google Scholar] [CrossRef]
- Landoni, F.; Bocciolone, L.; Perego, P.; Maneo, A.; Bratina, G.; Mangioni, C. Cancer of the Cervix, Figo Stages Ib and Iia—Patterns of Local Growth and Paracervical Extension. Int. J. Gynecol. Cancer 1995, 5, 329–334. [Google Scholar] [CrossRef]
- Strnad, P.; Robova, H.; Skapa, P.; Pluta, M.; Hrehorcak, M.; Halaska, M.; Rob, L. A prospective study of sentinel lymph node status and parametrial involvement in patients with small tumour volume cervical cancer. Gynecol. Oncol. 2008, 109, 280–284. [Google Scholar] [CrossRef]
- Kinney, W.K.; Hodge, D.O.; Egorshin, E.V.; Ballard, D.J.; Podratz, K.C. Identification of a low-risk subset of patients with stage IB invasive squamous cancer of the cervix possibly suited to less radical surgical treatment. Gynecol. Oncol. 1995, 57, 3–6. [Google Scholar] [CrossRef] [PubMed]
- Landoni, F.; Maneo, A.; Cormio, G.; Perego, P.; Milani, R.; Caruso, O.; Mangioni, C. Class II versus class III radical hysterectomy in stage IB-IIA cervical cancer: A prospective randomized study. Gynecol. Oncol. 2001, 80, 3–12. [Google Scholar] [CrossRef] [PubMed]
- Magrina, J.F.; Goodrich, M.A.; Weaver, A.L.; Podratz, K.C. Modified radical hysterectomy: Morbidity and mortality. Gynecol. Oncol. 1995, 59, 277–282. [Google Scholar] [CrossRef] [PubMed]
- Ramirez, P.T.; Frumovitz, M.; Pareja, R.; Lopez, A.; Vieira, M.; Ribeiro, R.; Buda, A.; Yan, X.; Shuzhong, Y.; Chetty, N.; et al. Minimally Invasive versus Abdominal Radical Hysterectomy for Cervical Cancer. Engl. J. Med. 2018, 379, 1895–1904. [Google Scholar] [CrossRef]
- Wenzel, H.H.B.; Smolders, R.G.V.; Beltman, J.J.; Lambrechts, S.; Trum, H.W.; Yigit, R.; Zusterzeel, P.L.M.; Zweemer, R.P.; Mom, C.H.; Bekkers, R.L.M.; et al. Survival of patients with early-stage cervical cancer after abdominal or laparoscopic radical hysterectomy: A nationwide cohort study and literature review. Eur. J. Cancer 2020, 133, 14–21. [Google Scholar] [CrossRef]
- Falconer, H.; Palsdottir, K.; Stalberg, K.; Dahm-Kähler, P.; Ottander, U.; Lundin, E.S.; Wijk, L.; Kimmig, R.; Jensen, P.T.; Zahl Eriksson, A.G.; et al. Robot-assisted approach to cervical cancer (RACC): An international multi-center, open-label randomized controlled trial. Int. J. Gynecol. Cancer 2019, 29, 1072–1076. [Google Scholar] [CrossRef]



{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Stage | 2009 FIGO Definition | 2018 FIGO Definition |
|---|---|---|
| I | Confined to the cervix | Confined to the cervix |
| IA | ≤5 mm depth and ≤7 mm width | ≤5 mm depth * |
| IA1 | ≤3 mm depth | ≤3 mm depth |
| IA2 | >3 mm and not >5 mm depth | >3 mm and ≤5 mm depth |
| IB | >5 mm depth | >5 mm depth |
| IB1 | ≤4 cm maximum diameter | ≤ 2 cm maximum diameter * |
| IB2 | ≥4 cm maximum diameter | >2 cm and ≤4 cm maximum diameter * |
| IB3 | - | >4 cm maximum diameter * |
| II | Beyond the uterus but not involving the lower one-third of the vagina or pelvic sidewall | Beyond the uterus but not involving the lower one-third of the vagina or pelvic sidewall |
| IIA | Upper two-thirds of the vagina | Upper two-thirds of the vagina |
| IIA1 | Upper two-thirds of the vagina and ≤4 cm | Upper two-thirds of the vagina and ≤4 cm |
| IIA2 | Upper two-thirds of the vagina and >4 cm | Upper two-thirds of the vagina and >4 cm |
| IIB | Parametrial invasion | Parametrial invasion |
| III | Lower vagina, pelvic sidewall and ureters | Lower vagina, pelvic sidewall, ureters and lymph nodes * |
| IIIA | Lower one-third of the vagina | Lower one-third of the vagina |
| IIIB | Pelvic side wall | Pelvic side wall |
| IIIC | - | Pelvic and para-aortic lymph node involvement * |
| Pelvic lymph node involvement | ||
| IIIC1 | - | Para-aortic lymph node involvement |
| IIIC2 | - | |
| IV | Adjacent and distant organs | Adjacent and distant organs |
| IVA | Rectal or bladder involvement | Rectal or bladder involvement |
| IVB | Distant organs outside the pelvis | Distant organs outside the pelvis |
| Characteristics | Total Group N = 2264 | IA1/2 = IA1/2 N = 896 | IB1 -> IA1/2 N = 501 | IB1 = IB1 N = 274 | IB1 -> IB2 N = 593 | p-Value |
|---|---|---|---|---|---|---|
| Baseline and clinical characteristics | ||||||
| Age in years (median IQR) | 40 (34–47) | 39 (33–45) | 40 (34–46) | 43 (37–50) | 43 (35–51) | <0.05 |
| Body mass index (BMI) | 0.43 | |||||
| <18.5 kg/m2 | 39 (1.7%) | 7 (0.8%) | 13 (2.6%) | 11 (4.0%) | 8 (1.3%) | |
| 18.5–24.9 kg/m2 | 896 (39.6%) | 188 (21.0%) | 251 (50.1%) | 150 (54.7%) | 307 (51.8%) | |
| 25–29.9 kg/m2 | 460 (20.3%) | 88 (9.8%) | 140 (27.9% | 66 (24.1%) | 166 (28.0%) | |
| Obese (≥30 kg/m2) | 252 (11.1%) | 55 (6.1%) | 74 (14.8%) | 39 (14.2%) | 84 (14.2%) | |
| Unknown | 617 (27.3%) | 558 (62.3%) | 23 (4.6%) | 8 (2.9%) | 28 (4.7%) | |
| Surgery | <0.05 | |||||
| Exconisation/LLETZ | 439 (19.4) | 418 (46.7) | 19 (3.8%) | 1 (0.4%) | 1 (0.2%) | |
| Simple hysterectomy | 496 (21.9) | 440 (49.1%) | 34 (6.8%) | 13 (4.7) | 9 (1.5%) | |
| Radical trachelectomy | 145 (6.4) | 4 (0.4%) | 83 (16.6%) | 22 (8.0%) | 36 (6.1%) | |
| Radical hysterectomy | 1184 (52.3) | 34 (3.8%) | 365 (72.9%) | 238 (86.9%) | 547 (92.2%) | |
| Histopathological findings | ||||||
| Histology | <0.05 | |||||
| Squamous | 1676 (7.0%) | 760 (84.8%) | 339 (67.7%) | 162 (59.1%) | 415 (70.0%) | |
| Adeno | 520 (2.0%) | 127 (14.2%) | 149 (29.7%) | 98 (35.8%) | 146 (24.6%) | |
| Adeno-squamous | 68 (3.0%) | 9 (1.0%) | 13 (2.6%) | 14 (5.1%) | 32 (5.4%) | |
| Differentiation grade | <0.05 | |||||
| Grade 1 | 232 (10.2%) | 110 (1.3%) | 48 (9.6%) | 26 (9.5%) | 48 (8.1%) | |
| Grade 2 | 605 (26.7%) | 105 (11.7%) | 191 (38.1%) | 102 (37.2%) | 207 (34.9%) | |
| Grade 3 | 380 (1.8%) | 26 (2.9%) | 89 (17.8%) | 72 (2.3%) | 193 (32.5%) | |
| Unknown | 1047 (46.2%) | 655 (73.1%) | 173 (34.5%) | 74 (27.0%) | 145 (24.5%) | |
| LVSI | <0.05 | |||||
| Yes | 580 (25.6%) | 80 (8.9%) | 126 (25.1%) | 108 (3.,4%) | 266 (44.9%) | |
| No | 1038 (45.8%) | 367 (41.0%) | 292 (58.3%) | 123 (44.9%) | 256 (43.2%) | |
| Unknown | 646 (28.5%) | 449 (5.1%) | 83 (16.6%) | 43 (15.7%) | 71 (12.0%) | |
| Depth of invasion | <0.05 | |||||
| <3 mm | 1058 (46.7%) | 807 (90.1%) | 235 (46.9%) | 4 (1.5%) | 12 (2.0%) | |
| 3–5 mm | 400 (17.7%) | 98 (9.9%) | 266 (53.1%) | 2 (0.7%) | 43 (7.3%) | |
| >5 mm | 794 (35.1%) | 0 (0%) | 0 (0%) | 263 (96.0%) | 531 (89.5%) | |
| Unknown | 12 (0.5%) | 0 (0%) | 0 (0%) | 5 (1.8%) | 7 (1.2%) | |
| Positive lymph nodes | <0.05 | |||||
| Yes | 193 (8.5%) | 1 (0.1%) | 24 (4.8%) | 48 (17.5%) | 120 (20.2%) | |
| No | 1255 (55.4%) | 79 (8.8%) | 477 (95.2%) | 226 (82.5%) | 473 (79.8%) | |
| No lymphadenectomy | 816 (36.0%) | 816 (91.1%) | 0 (0%) | 0 (0%) | 0 (0%) | |
| Parametrial invasion | <0.05 | |||||
| Yes | 36 (1.6%) | 0 (0%) | 2 (0.4%) | 11 (4.0%) | 23 (3.9%) | |
| No | 1293 (57.1%) | 38 (4.2%) | 446 (89.0%) | (90.9%) | 560 (94.4%) | |
| No parametrectomy | 935 (41.3%) | 858 (95.8%) | 53 (10.6%) | 14 (5.1%) | 10 (1.7%) | |
| Follow up in months (median, IQR) | 83 (57–111) | 84 (58–112) | 87 (57–115) | 78 (53–106) | 80 (56–108) | 0.17 |
| Recurrence | <0.05 | |||||
| Total | 151 (6.7%) | 22 (2.4%) | 28 (5.6%) | 20 (7.3%) | 81 (13.7%) | |
| Local | 78 (3.4%) | 17 (1.9%) | 19 (3.8%) | 6 (2.2%) | 36 (6.1%) | |
| Locoregional | 22 (1.0%) | 3 (0.3%) | 5 (1.0%) | 2 (0.7%) | 12 (2.0%) | |
| Distant | 51 (2.3%) | 2 (0.2%) | 4 (0.8%) | 12 (4.4%) | 33 (5.6%) | |
| Time to recurrence (months) (median, IQR) | 22 (13–45) | 26 (15–52) | 30 (13–48) | 27 (15–46) | 19 (10–39) | <0.05 |
| Parametrial Invasion N = 36 | No Parametrial Invasion N = 1293 | p-Value Univariate | |
|---|---|---|---|
| Age (median, IQR) | 54 (range 41–61) | 42 (range 35–49) | <0.01 |
| BMI | 0 (0%) | 31 (2.5%) | 0.69 |
| Underweight (<18.5 kg/m2) | 21 (60.0%) | 668 (53.9%) | |
| Normal (18.5–24.9 kg/m2) | 10 (28.6%) | 348 (28.1%) | |
| Overweight (25–29.9 kg/m2) | 4 (11.4%) | 192 (15.4%) | |
| Obese (≥30 kg/m2) | |||
| Histology | 0.01 | ||
| Adeno(squamous)carcinoma | 5 (13.9%) | 434 (33.6%) | |
| Squamous carcinoma | 31 (86.1%) | 859 (66.4%) | |
| Differentiation | <0.01 | ||
| 1 | 1 (3.2%) | 117 (12.7%) | |
| 2 | 9 (29.0%) | 476 (51.8%) | |
| 3 | 21 (67.7%) | 326 (35.5%) | |
| LVSI | <0.01 | ||
| Yes | 23 (76.7%) | 469 (41.4%) | |
| No | 7 (23.3%) | 663 (58.6%) | |
| Invasion depth | <0.01 | ||
| <3 mm | 2 (5.6%) | 228 (17.8%) | |
| 3–5 mm | 0 (0%) | 313 (24.4%) | |
| >5 mm | 34 (94.4%) | 740 (57.8%) | |
| Lateral extent | 0.56 | ||
| <7 mm | 2 (5.6%) | 107 (8.3%) | |
| 7 mm or more | 34 (94.4%) | 1186 (91.7%) |
| Lymph Node Involvement N = 193 | No Lymph Node Involvement N = 1255 | p-Value Univariate | |
|---|---|---|---|
| Age (median, IQR) | 42 (35–50) | 41 (35–49) | 0.42 |
| BMI | 0.19 | ||
| Underweight (<18.5 kg/m2) | 5 (2.7%) | 28 (2.4%) | |
| Normal (18.5–24.9 kg/m2) | 109 (58.9%) | 636 (53.9%) | |
| Overweight (25–29.9 kg/m2) | 53 (28.6%) | 329 (27.9%) | |
| Obese (≥30 kg/m2) | 18 (9.7%) | 187 (15.8%) | |
| Histology | 0.08 | ||
| Adeno(squamous)carcinoma | 51 (26.4%) | 412 (32.8%) | |
| Squamous carcinoma | 142 (73.6%) | 843 (67.2%) | |
| Differentiation | <0.01 | ||
| 1 | 10 (6.6%) | 125 (14.0%) | |
| 2 | 67 (44.1%) | 486 (54.4%) | |
| 3 | 75 (49.3%) | 282 (31.6%) | |
| LVSI | <0.01 | ||
| Yes | 132 (80.0%) | 488 (43.3%) | |
| No | 33 (20.0%) | 638 (56.7%) | |
| Invasion depth | <0.01 | ||
| <3 mm | 12 (6.3%) | 298 (23.9%) | |
| 3–5 mm | 22 (11.6%) | 310 (24.9%) | |
| >5 mm | 155 (82.0%) | 639 (51.2%) | |
| Lateral extent | <0.01 | ||
| <7 mm | 7 (3.6%) | 152 (12.1%) | |
| 7 or more | 186 (96.4%) | 1103 (87.9%) | |
| Parametrial invasion | <0.01 | ||
| Yes | 18 (9.3%) | 18 (1.4%) | |
| No | 175 (90.7%) | 1237 (98.6%) |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Ten Eikelder, M.L.G.; Hinten, F.; Smits, A.; Van der Aa, M.A.; Bekkers, R.L.M.; IntHout, J.; Wenzel, H.H.B.; Zusterzeel, P.L.M. Does the New FIGO 2018 Staging System Allow Better Prognostic Differentiation in Early Stage Cervical Cancer? A Dutch Nationwide Cohort Study. Cancers 2022, 14, 3140. https://doi.org/10.3390/cancers14133140
Ten Eikelder MLG, Hinten F, Smits A, Van der Aa MA, Bekkers RLM, IntHout J, Wenzel HHB, Zusterzeel PLM. Does the New FIGO 2018 Staging System Allow Better Prognostic Differentiation in Early Stage Cervical Cancer? A Dutch Nationwide Cohort Study. Cancers. 2022; 14(13):3140. https://doi.org/10.3390/cancers14133140
Chicago/Turabian StyleTen Eikelder, Mieke L. G., Floor Hinten, Anke Smits, Maaike A. Van der Aa, Ruud L. M. Bekkers, Joanna IntHout, Hans H. B. Wenzel, and Petra L. M. Zusterzeel. 2022. "Does the New FIGO 2018 Staging System Allow Better Prognostic Differentiation in Early Stage Cervical Cancer? A Dutch Nationwide Cohort Study" Cancers 14, no. 13: 3140. https://doi.org/10.3390/cancers14133140
APA StyleTen Eikelder, M. L. G., Hinten, F., Smits, A., Van der Aa, M. A., Bekkers, R. L. M., IntHout, J., Wenzel, H. H. B., & Zusterzeel, P. L. M. (2022). Does the New FIGO 2018 Staging System Allow Better Prognostic Differentiation in Early Stage Cervical Cancer? A Dutch Nationwide Cohort Study. Cancers, 14(13), 3140. https://doi.org/10.3390/cancers14133140