
Risk Factors and Clinicopathological Features for Developing a Subsequent Primary Cutaneous Squamous and Basal Cell Carcinomas

 ,
, 
Abstract
:Simple Summary
Abstract
1. Introduction
2. Materials and Methods
3. Results
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Gurung, P.; Kanneganti, T.D. Autoinflammatory skin disorders: The inflammasomme in focus. Trends Mol. Med. 2016, 22, 545–564. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Ciążyńska, M.; Olejniczak-Staruch, I.; Sobolewska-Sztychny, D.; Narbutt, J.; Skibińska, M.; Lesiak, A. Ultraviolet radiation and chronic inflammation—Molecules and mechanisms involved in skin carcinogenesis: A narrative review. Life 2021, 11, 326. [Google Scholar] [CrossRef] [PubMed]
- Donaldson, M.R.; Coldiron, B.M. No end in sight: The skin cancer epidemic continues. Semin. Cutan. Med. Surg. 2011, 30, 3–5. [Google Scholar] [CrossRef] [PubMed]
- Scrivener, Y.; Grosshans, E.; Cribier, B. Variations of basal cell carcinomas according to gender, age, location and histopathological subtype. Br. J. Dermatol. 2002, 147, 41–47. [Google Scholar] [CrossRef]
- Smeets, N.W.; Kuijpers, D.I.; Nelemans, P.; Ostertag, J.U.; Verhaegh, M.E.; Krekels, G.A.; Neumann, H.A. Mohs’ micrographic surgery for treatment of basal cell carcinoma of the face--results of a retrospective study and review of the literature. Br. J. Dermatol. 2004, 151, 141–147. [Google Scholar] [CrossRef]
- Cigna, E.; Tarallo, M.; Maruccia, M.; Sorvillo, V.; Pollastrini, A.; Scuderi, N. Basal cell carcinoma: 10 years of experience. J. Ski. Cancer 2011, 2011, 476362. [Google Scholar] [CrossRef] [Green Version]
- Szewczyk, M.P.; Pazdrowski, J.; Dańczak-Pazdrowska, A.; Golusiński, P.; Majchrzak, E.; Luczewski, L.; Marszałek, S.; Silny, W.; Golusiński, W. Analysis of selected recurrence risk factors after treatment of head and neck basal cell carcinoma. Postepy Dermatol. I Alergol. 2014, 31, 146–151. [Google Scholar] [CrossRef] [Green Version]
- Bartoš, V.; Pokorný, D.; Zacharová, O.; Haluska, P.; Doboszová, J.; Kullová, M.; Adamicová, K.; Péč, M.; Péč, J. Recurrent basal cell carcinoma: A clinicopathological study and evaluation of histomorphological findings in primary and recurrent lesions. Acta Dermatovenerologica Alpina Pannonica et Adriatica 2011, 20, 67–75. [Google Scholar]
- Bichakjian, C.; Olencki, T.; Aasi, S.; Alam, M.; Andersen, J.; Blitzblau, R.; Bowen, G.; Contreras, C.; Daniels, G.; Decker, R.; et al. Basal Cell Carcinoma, NCCN Clinical Practice Guidelines in Oncology; NCCN: Fort Washington, PA, USA, 2018; Available online: https://www.nccn.org (accessed on 1 June 2022).
- Neugut, A.I.; Meadows, A.T.; Robinson, E. Multiple Primary Cancers; Lippincott Williams Wilkins: Philadelphia, PA, USA, 1999; pp. 445–469. [Google Scholar]
- Ferrone, C.R.; Ben Porat, L.; Panageas, K.S.; Berwick, M.; Halpern, A.C.; Patel, A.; Coit, D.G. Clinicopathological features of and risk factors for multiple primary melanomas. JAMA 2005, 294, 1647–1654. [Google Scholar] [CrossRef] [Green Version]
- Graells, J. The risk and risk factors of a second non-melanoma skin cancer: A study in a Mediterranean population. J. Eur. Acad. Dermatol. Venereol. JEADV 2004, 18, 142–147. [Google Scholar] [CrossRef]
- Flohil, S.C.; van der Leest, R.J.; Arends, L.R.; de Vries, E.; Nijsten, T. Risk of subsequent cutaneous malignancy in patients with prior keratinocyte carcinoma: A systematic review and meta-analysis. Eur. J. Cancer 2013, 49, 2365–2375. [Google Scholar] [CrossRef] [PubMed]
- van der Leest, R.J.; Flohil, S.C.; Arends, L.R.; de Vries, E.; Nijsten, T. Risk of subsequent cutaneous malignancy in patients with prior melanoma: A systematic review and meta-analysis. J. Eur. Acad. Dermatol. Venereol. JEADV 2015, 29, 1053–1062. [Google Scholar] [CrossRef] [PubMed]
- Rees, J.R.; Zens, M.S.; Gui, J.; Celaya, M.O.; Riddle, B.L.; Karagas, M.R. Non melanoma skin cancer and subsequent cancer risk. PLoS ONE 2014, 9, e99674. [Google Scholar] [CrossRef] [PubMed]
- Fitzpatrick, T.B. The validity and practicality of sun-reactive skin types I through VI. Arch. Dermatol. 1988, 124, 869–871. [Google Scholar] [CrossRef]
- Marcil, I.; Stern, R.S. Risk of developing a subsequent nonmelanoma skin cancer in patients with a history of nonmelanoma skin cancer: A critical review of the literature and meta-analysis. Arch. Dermatol. 2000, 136, 1524–1530. [Google Scholar] [CrossRef] [Green Version]
- Wehner, M.R.; Linos, E.; Parvataneni, R.; Stuart, S.E.; Boscardin, W.J.; Chren, M.M. Timing of subsequent new tumors in patients who present with basal cell carcinoma or cutaneous squamous cell carcinoma. JAMA Dermatol. 2015, 151, 382–388. [Google Scholar] [CrossRef] [Green Version]
- Veien, K.; Veien, N.K. Risk of developing subsequent nonmelanoma skin cancers. Arch. Dermatol. 2001, 137, 1251. [Google Scholar]
- Epstein, E. Value of follow-up after treatment of basal cell carcinoma. Arch. Dermatol. 1973, 108, 798–800. [Google Scholar] [CrossRef]
- Robinson, J.K. Risk of developing another basal cell carcinoma. A 5-year prospective study. Cancer 1987, 60, 118–120. [Google Scholar] [CrossRef]
- Ciążyńska, M.; Kamińska-Winciorek, G.; Lange, D.; Lewandowski, B.; Reich, A.; Sławińska, M.; Pabianek, M.; Szczepaniak, K.; Hankiewicz, A.; Ułańska, M.; et al. The incidence and clinical analysis of non-melanoma skin cancer. Sci. Rep. 2021, 11, 4337. [Google Scholar] [CrossRef]
- Ciążyńska, M.; Sławińska, M.; Kamińska-Winciorek, G.; Lange, D.; Lewandowski, B.; Reich, A.; Pabianek, M.; Szczepaniak, K.; Hankiewicz, A.; Ułańska, M.; et al. Clinical and epidemiological analysis of basosquamous carcinoma: Results of the multicenter study. Sci. Rep. 2020, 10, 18475. [Google Scholar] [CrossRef] [PubMed]
- Greenberg, E.R.; Baron, J.A.; Stukel, T.A.; Stevens, M.M.; Mandel, J.S.; Spencer, S.K.; Elias, P.M.; Lowe, N.; Nierenberg, D.W.; Bayrd, G. A clinical trial of beta carotene to prevent basal-cell and squamous-cell cancers of the skin. The Skin Cancer Prevention Study Group. N. Engl. J. Med. 1990, 323, 789–795. [Google Scholar] [CrossRef] [PubMed]
- Karagas, M.R.; Stukel, T.A.; Greenberg, E.R.; Baron, J.A.; Mott, L.A.; Stern, R.S.; Skin Cancer Prevention Study Group. Risk of subsequent basal cell carcinoma and squamous cell carcinoma of the skin among patients with prior skin cancer. JAMA 1992, 267, 3305–3310. [Google Scholar] [CrossRef] [PubMed]
- Tangrea, J.A.; Edwards, B.K.; Taylor, P.R.; Hartman, A.M.; Peck, G.L.; Salasche, S.J.; Menon, P.A.; Benson, P.M.; Mellette, J.R.; Guill, M.A.; et al. Long-term therapy with low-dose isotretinoin for prevention of basal cell carcinoma: A multicenter clinical trial. J. Natl. Cancer Inst. 1992, 84, 328–332. [Google Scholar] [CrossRef]
- Bergstresser, P.R.; Halprin, K.M. Multiple sequential skin cancers. The risk of skin cancer in patients with previous skin cancer. Arch. Dermatol. 1975, 111, 995–996. [Google Scholar] [CrossRef]
- Frankel, D.H.; Hanusa, B.H.; Zitelli, J.A. New primary nonmelanoma skin cancer in patients with a history of squamous cell carcinoma of the skin. Implications and recommendations for follow-up. J. Am. Acad. Dermatol. 1992, 26, 720–726. [Google Scholar] [CrossRef]
- Czarnecki, D.; Mar, A.; Staples, M.; Giles, G.; Meehan, C. The development of non-melanocytic skin cancers in people with a history of skin cancer. Dermatology 1994, 189, 364–367. [Google Scholar] [CrossRef]
- Chen, J.; Shih, J.; Tran, A.; Mullane, A.; Thomas, C.; Aydin, N.; Misra, S. Gender-based differences and barriers in skin protection behaviors in melanoma survivors. J. Skin Cancer 2016, 2016, 3874572. [Google Scholar] [CrossRef] [Green Version]
- Chlebicka, I.; Stefaniak, A.; Matusiak, Ł.; Szepietowski, J.C. Basal cell carcinoma: What new can be learned about the most common human cancer? A cross-sectional prospective study of 180 cases in a single centre. Postępy Dermatologii I Alergologii 2021, 38, 1086–1091. [Google Scholar] [CrossRef]
- Vitasa, B.C.; Taylor, H.R.; Strickland, P.T.; Rosenthal, F.S.; West, S.; Abbey, H.; Ng, S.K.; Munoz, B.; Emmett, E.A. Association of nonmelanoma skin cancer and actinic keratosis with cumulative solar ultraviolet exposure in Maryland watermen. Cancer 1990, 65, 2811–2817. [Google Scholar] [CrossRef]
- Kricker, A.; Armstrong, B.K.; English, D.R.; Heenan, P.J. Does intermittent sun exposure cause basal cell carcinoma? A case-control study in Western Australia. Int. J. Cancer 1995, 60, 489–494. [Google Scholar] [CrossRef] [PubMed]
- Gudbjartsson, D.F.; Sulem, P.; Stacey, S.N.; Goldstein, A.M.; Rafnar, T.; Sigurgeirsson, B.; Benediktsdottir, K.R.; Thorisdottir, K.; Ragnarsson, R.; Sveinsdottir, S.G.; et al. ASIP and TYR pigmentation variants associate with cutaneous melanoma and basal cell carcinoma. Nat. Genet. 2008, 40, 886–891. [Google Scholar] [CrossRef] [PubMed]
- Stacey, S.N.; Gudbjartsson, D.F.; Sulem, P.; Bergthorsson, J.T.; Kumar, R.; Thorleifsson, G.; Sigurdsson, A.; Jakobsdottir, M.; Sigurgeirsson, B.; Benediktsdottir, K.R.; et al. Common variants on 1p36 and 1q42 are associated with cutaneous basal cell carcinoma but not with melanoma or pigmentation traits. Nat. Genet. 2008, 40, 1313–1318. [Google Scholar] [CrossRef] [PubMed]
- Wallberg, P.; Kaaman, T.; Lindberg, M. Multiple Basal Cell Carcinoma. Med. J. Swed. Acta Derm. Venereol. Stock. 1998, 78, 127–129. [Google Scholar] [CrossRef] [Green Version]
- Hallaji, Z.; Rahimi, H.; Mirshams-Shahshahani, M. Comparison of risk factors of single Basal cell carcinoma with multiple Basal cell carcinomas. Indian J. Dermatol. 2011, 56, 398–402. [Google Scholar] [CrossRef]

{kind=link}
{kind=link}
{kind=link}
| Single KC | Multiple KC | ||||
|---|---|---|---|---|---|
| Total Number of Patients | 7786 | 2300 | p value | ||
| Sex | p < 0.01 | ||||
| Male | 3581 | 45.99% | 1224 | 53.22% | |
| Female | 4205 | 54.01% | 1076 | 46.78% | |
| Age | p = 0.15 | ||||
| Mean | 70.16 | 71.17 | |||
| Min | 20 | 29 | |||
| Max | 102 | 87 | |||
| Location of first primary KC | p = 0.07 | ||||
| Face | 5624 | 77.97% | 1613 | 74.33% | |
| Trunk | 827 | 11.47% | 292 | 13.46% | |
| Upper limb | 210 | 2.91% | 79 | 3.64% | |
| Lower limb | 274 | 3.80% | 82 | 3.78% | |
| Scalp | 111 | 1.54% | 49 | 2.26% | |
| Neck | 167 | 2.32% | 55 | 2.53% | |
| Unknown | 573 | 130 | |||
| Type of first primary KC | p < 0.01 | ||||
| SCC | 1168 | 15.00% | 385 | 16.74% | |
| BCC | 6618 | 85.00% | 1915 | 83.26% | |
| Nodular | 1891 | 51.74% | 554 | 39.12% | |
| Superficial | 1159 | 31.71% | 456 | 32.20% | |
| Infiltrative | 489 | 13.38% | 333 | 23.52% | |
| Basosquamous | 116 | 3.17% | 73 | 5.16% | |
| Unknown BCC subtype | 2963 | 499 | |||
| Univariate and Multivariable Analysis: HR (95% CI); p Value | |
|---|---|
| Male gender a | 1.37 (1.25–1.51); p < 0.0001 |
| Diagnosis of a BCC b | 0.88 (0.77–1.01); p = 0.064 |
| Diagnosis of a high-risk BCC c | 2.01 (1.73–2.34); p < 0.0001 |
| History of KC development d | 1.91 (1.63–2.21); p < 0.0001 |
| Age e | 0.93 (0.87–9.98); p = 0.132 |
| Size of primary lesion e | 1.06 (1.01–1.11); p = 0.173 |
| Site of First Primary KC | Site of Second Primary KC | ||||||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Face | Trunk | Upper Limb | Lower Limb | Scalp | Neck | Unknown | Total | ||||||||
| Face | 1372 | 85.1% | 75 | 4.6% | 23 | 1.4% | 22 | 1.4% | 16 | 1.0% | 32 | 2.0% | 73 | 4.5% | 1613 |
| Trunk | 111 | 38.0% | 115 | 39.4% | 26 | 8.9% | 14 | 4.8% | 6 | 2.1% | 5 | 1.7% | 15 | 5.1% | 292 |
| Upper limb | 23 | 29.1% | 13 | 16.5% | 30 | 38.0% | 4 | 5.1% | 1 | 1.3% | 4 | 5.1% | 4 | 5.1% | 79 |
| Lower limb | 24 | 29.3% | 8 | 9.8% | 7 | 8.5% | 40 | 48.8% | 0 | 0.0% | 0 | 0.0% | 3 | 3.7% | 82 |
| Scalp | 21 | 42.9% | 4 | 8.2% | 1 | 2.0% | 3 | 6.1% | 16 | 32.7% | 3 | 6.1% | 1 | 2.0% | 49 |
| Neck | 22 | 40.0% | 7 | 12.7% | 0 | 0.0% | 2 | 3.6% | 1 | 1.8% | 22 | 40.0% | 1 | 1.8% | 55 |
| Unknown | 67 | 51.5% | 23 | 17.7% | 4 | 3.1% | 5 | 3.8% | 1 | 0.8% | 4 | 3.1% | 26 | 20.0% | 130 |
| Total | 1640 | 245 | 91 | 90 | 41 | 70 | 123 | 2300 | |||||||
| Type of First Primary KC | Type of Second Primary KC | ||||||||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| SCC | BCC | BCC Subtype | Total | ||||||||||||||
| Nodular | Superficial | Infiltrative | Basosquamous | Unknown BCC | Total BCC | ||||||||||||
| SCC | 221 | 62.3% | 134 | 37.7% | 17 | 4.8% | 5 | 1.4% | 3 | 0.8% | 0 | 0.0% | 109 | 30.7% | 355 | ||
| BCC | 243 | 12.5% | 1702 | 87.5% | 567 | 29.2% | 643 | 33.1% | 323 | 16.6% | 66 | 3.4% | 103 | 5.3% | 1945 | ||
| BCC subtype | Nodular | 71 | 12.7% | 488 | 87.3% | 289 | 51.7% | 96 | 17.2% | 12 | 2.1% | 7 | 1.3% | 84 | 15.0% | 559 | |
| Superficial | 69 | 11.4% | 535 | 88.6% | 74 | 12.3% | 427 | 70.7% | 16 | 2.6% | 15 | 2.5% | 3 | 0.5% | 604 | ||
| Infiltrative | 18 | 5.5% | 312 | 94.5% | 86 | 26.1% | 62 | 18.8% | 155 | 47.0% | 5 | 1.5% | 4 | 1.2% | 330 | ||
| Basosquamous | 6 | 8.1% | 68 | 91.9% | 6 | 8.1% | 14 | 18.9% | 17 | 23.0% | 31 | 41.9% | 0 | 0.0% | 74 | ||
| unknown BCC | 79 | 20.9% | 299 | 79.1% | 112 | 29.6% | 44 | 11.6% | 123 | 32.5% | 8 | 2.1% | 12 | 3.2% | 378 | ||
| Total | 464 | 1836 | 2300 | ||||||||||||||
| First | Second | Third | Fourth | Fifth | ||||||
|---|---|---|---|---|---|---|---|---|---|---|
| n = | 2300 | n = | 2300 | n = | 736 | n = | 347 | n = | 182 | |
| Location of primary KC | ||||||||||
| Face | 1613 | 74.3% | 1640 | 75.3% | 531 | 72.1% | 236 | 68.0% | 132 | 72.5% |
| Trunk | 292 | 13.5% | 245 | 11.3% | 93 | 12.6% | 52 | 15.0% | 24 | 13.2% |
| Upper limb | 79 | 3.6% | 91 | 4.2% | 41 | 5.6% | 23 | 6.6% | 11 | 6.0% |
| Lower limb | 82 | 3.8% | 90 | 4.1% | 29 | 3.9% | 13 | 3.7% | 2 | 1.1% |
| Scalp | 49 | 2.3% | 41 | 1.9% | 18 | 2.4% | 10 | 2.9% | 3 | 1.6% |
| Neck | 55 | 2.5% | 70 | 3.2% | 25 | 3.4% | 13 | 3.7% | 10 | 5.5% |
| Unknown | 130 | 123 | 0 | 0 | 0 | |||||
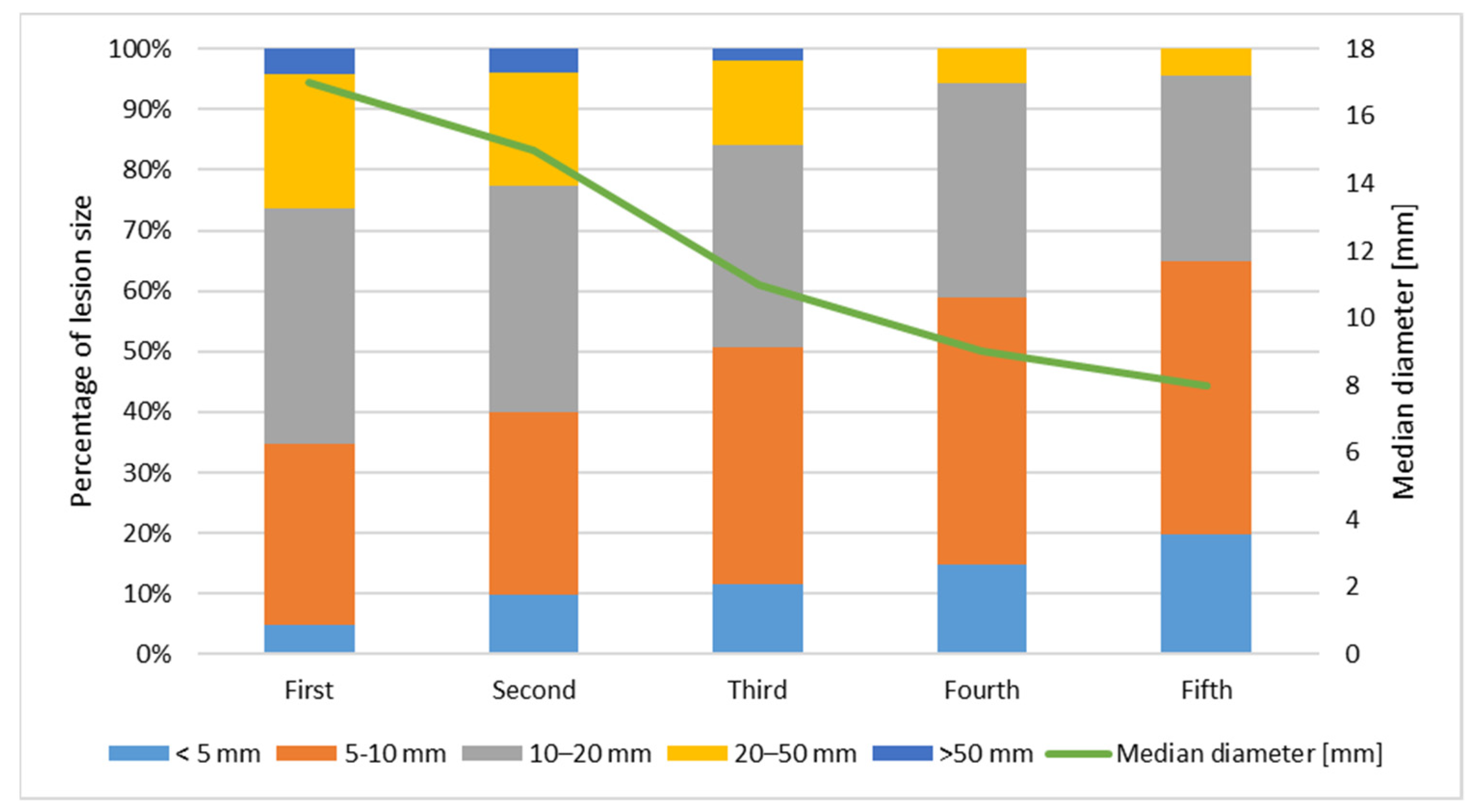
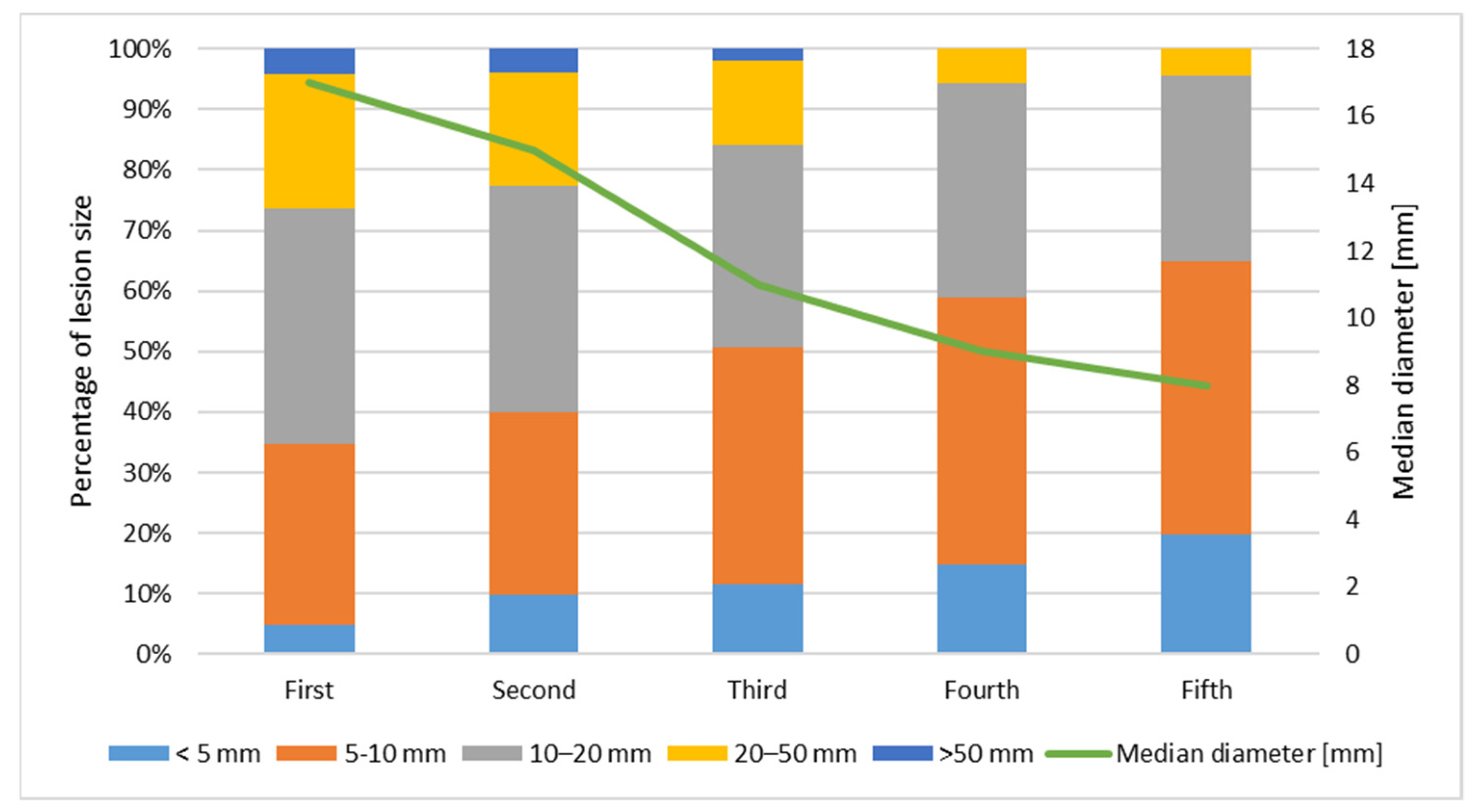
| Size of primary KC [diameter, mm] | ||||||||||
| <5 | 104 | 4.8% | 221 | 9.9% | 85 | 11.5% | 51 | 14.7% | 36 | 19.8% |
| 5–10 | 654 | 30.0% | 667 | 30.0% | 287 | 39.0% | 153 | 44.1% | 82 | 45.1% |
| 10–20 | 846 | 38.8% | 832 | 37.4% | 246 | 33.4% | 122 | 35.2% | 56 | 30.8% |
| 20–50 | 487 | 22.3% | 419 | 18.8% | 101 | 13.7% | 20 | 5.8% | 8 | 4.4% |
| >50 | 89 | 4.1% | 85 | 3.8% | 15 | 2.0% | 0 | 0.0% | 0 | 0.0% |
| unknown | 120 | 76 | 2 | 1 | 0 | |||||
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Ciążyńska, M.; Pabianek, M.; Sławińska, M.; Reich, A.; Lewandowski, B.; Szczepaniak, K.; Ułańska, M.; Nejc, D.; Brodowski, R.; Sobjanek, M.; et al. Risk Factors and Clinicopathological Features for Developing a Subsequent Primary Cutaneous Squamous and Basal Cell Carcinomas. Cancers 2022, 14, 3069. https://doi.org/10.3390/cancers14133069
Ciążyńska M, Pabianek M, Sławińska M, Reich A, Lewandowski B, Szczepaniak K, Ułańska M, Nejc D, Brodowski R, Sobjanek M, et al. Risk Factors and Clinicopathological Features for Developing a Subsequent Primary Cutaneous Squamous and Basal Cell Carcinomas. Cancers. 2022; 14(13):3069. https://doi.org/10.3390/cancers14133069
Chicago/Turabian StyleCiążyńska, Magdalena, Marta Pabianek, Martyna Sławińska, Adam Reich, Bogumił Lewandowski, Katarzyna Szczepaniak, Małgorzata Ułańska, Dariusz Nejc, Robert Brodowski, Michał Sobjanek, and et al. 2022. "Risk Factors and Clinicopathological Features for Developing a Subsequent Primary Cutaneous Squamous and Basal Cell Carcinomas" Cancers 14, no. 13: 3069. https://doi.org/10.3390/cancers14133069
APA StyleCiążyńska, M., Pabianek, M., Sławińska, M., Reich, A., Lewandowski, B., Szczepaniak, K., Ułańska, M., Nejc, D., Brodowski, R., Sobjanek, M., Owczarek, W., Kamińska-Winciorek, G., Lange, D., Słowińska, M., Wróbel, K., Bieniek, A., Woźniacka, A., Pękala, A., Kuncman, Ł., ... Lesiak, A. (2022). Risk Factors and Clinicopathological Features for Developing a Subsequent Primary Cutaneous Squamous and Basal Cell Carcinomas. Cancers, 14(13), 3069. https://doi.org/10.3390/cancers14133069