Simple Summary
Diffusion tensor imaging (DTI) is an image-guided tool, especially in brain tumor resection surgery. Neuroimaging tools are essential for operative planning, particularly for maximizing tumor resection and, at the same time, preserving brain function. In this systematic review, we discuss the utilization of DTI in brain tumor resection, by looking into its ability to assess the perioperative approach, as well as evaluating its benefits for successful surgery. The present study proposes to use DTI as a vital neuroimaging tool for preoperative planning in brain tumor resection surgery.
Abstract
The diffusion tensor imaging technique has been recognized as a neuroimaging tool for in vivo visualization of white matter tracts. However, DTI is not a routine procedure for preoperative planning for brain tumor resection. Our study aimed to systematically evaluate the effectiveness of DTI and the outcomes of surgery. The electronic databases, PubMed/MEDLINE and Scopus, were searched for relevant studies. Studies were systematically reviewed based on the application of DTI in pre-surgical planning, modification of operative planning, re-evaluation of preoperative DTI data intraoperatively, and the outcome of surgery decisions. Seventeen studies were selected based on the inclusion and exclusion criteria. Most studies agreed that preoperative planning using DTI improves postoperative neuro-deficits, giving a greater resection yield and shortening the surgery time. The results also indicate that the re-evaluation of preoperative DTI intraoperatively assists in a better visualization of white matter tract shifts. Seven studies also suggested that DTI modified the surgical decision of the initial surgical approach and the rate of the GTR in tumor resection surgery. The utilization of DTI may give essential information on white matter tract pathways, for a better surgical approach, and eventually reduce the risk of neurologic deficits after surgery.
1. Introduction
Preoperative planning in brain surgery plays a significant role in the successful outcome of the surgery, which eventually improves patients’ quality of life. Furthermore, preoperative planning in neurosurgery maximizes tumor resection, while preserving the brain’s neurological functions [1]. Diffusion tensor imaging (DTI) is one of the non-invasive neuroimaging tools for visualizing white matter tracts and pre-identifying tumor locations. This technique can also measure the interaction between the tumor and the surrounding areas of the brain, especially in the eloquent brain area [2]. However, this technique is not a routine technique for preoperative mapping, due to its artefacts and limitations, including the technique and preprocessing discrepancies that need to be addressed before data post-processing [3].
In previous studies, DTI was utilized in brain tumor patients, mainly to classify the tissue’s characteristics and understand the effects of tumor growth on the microstructural integrity of the surrounding brain tissue [4,5,6]. Besides, DTI was also used for navigating the anatomy of the tumor, giving essential routes for neurosurgery and to decide the surgical approaches [7,8]. Intensive research on DTI in brain tumor surgery has been carried out, mainly on the evaluation of brain tumor resection, and been incorporated with other modalities; for example, when combined with functional magnetic resonance imaging (fMRI). To date, no single technique has become the ultimate technique for understanding radiological assessment for brain tumor resection surgery [6]. Many methods have been developed and used alongside DTI, mainly to ensure efficacy, as DTI has been shown to have many limitations and artefacts [3,9,10]. Some studies even claimed that non-invasive DTI provided minor complementary information for brain mapping, which is critical in neurosurgery [11].
Thus, this systematic review investigates the effectiveness and benefits of utilizing DTI as a single neuro-navigation tool for brain tumor resection. The present review also compared DTI intervention group with non-DTI group. Finally, the present study evaluated the modification of the preoperative planning based on the DTI data findings, the re-evaluation of intraoperative DTI, and the best surgical approach.
2. Materials and Methods
2.1. Search Strategy and Study Selection
Two independent researchers conducted a systematic search using the National Centre for Biotechnology Information (PubMed) and Scopus electronic databases. The preferred reporting items for systematic reviews and meta-analyses guidelines (PRISMA) were used as the reporting guidelines [12] (Supplementary Materials Tables S1 and S2) and followed previous studies [13,14,15,16,17,18]. The search was performed to identify studies reporting diffusion tensor imaging, brain tumors, and preoperative mapping. We sought to evaluate clinical studies on brain tumor patients who had diffusion tensor imaging for brain resection surgery and a preoperative surgical planning review. This will aid in the re-evaluation of the surgical strategy, resulting in surgical decision modification and improved outcomes. We also included articles that made a comparison between the intervention of DTI and a control group.
The article search was conducted between the earliest record and 27 January 2022. Search terms used included ‘brain neoplasm or brain cancer or brain lesion or brain tumour or brain tumor’ and ‘surgery approach or surgery operation or surgery planning or surgery process or surgical procedure’ and ‘DTI or diffusion tensor imaging or diffusion tensor tractography or tractography or fiber tracking or fibre tracking’; and the full advanced search used for each database can be found in Supplementary Material Table S3. We also manually searched the Google Scholar database for related papers in references and citations. There were no restrictions on the status of the publication or the date of publication. All records were collected into a final database after deleting duplicates, which were then screened by title and abstract.
2.2. PICOS and Inclusion and Exclusion Criteria
Consensus for eligibility was reached through discussion and using the PICOS strategy, as summarized in Table 1.

Table 1.
PICOS strategy for selection of the study.
The inclusion and exclusion criteria were also screened. The papers were limited to adult humans aged >17 years old, and the articles were written in English. No limitation was set for sample size and year of publication. Second, we excluded articles that also utilized other imaging modalities, such as computed tomography (CT), positron emission tomography (PET), ultrasound, navigated transcranial magnetic stimulation (nTMS), fMRI, and other diffusion-weighted techniques, i.e., high angular resolution diffusion imaging (HARDI). However, magnatice resoncance imaging (MRI) were included. Review papers, systematic review papers, and technical notes were also excluded.
3. Results
3.1. Data Extraction and Study Design
Seventeen studies fulfilled all the criteria for the systematic review, out of 2270 publications. The detailed flow processes of article selection for this systematic review are presented in Figure 1.
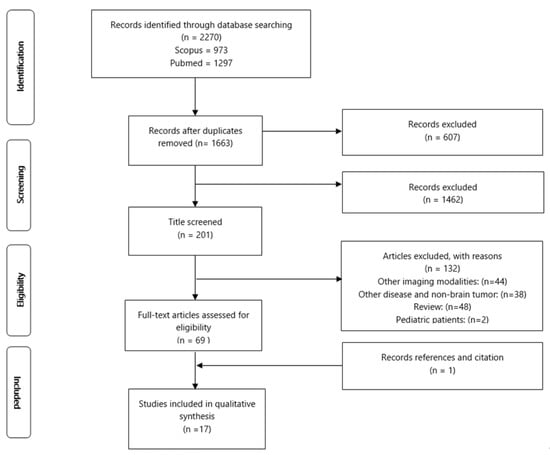
Figure 1.
Flow diagram of the PRISMA study selection process.
Based on the quality assessment tools published by the National Heart, Lung, and Blood Institute, these studies were assessed as reasonable and fair (Supplementary Materials Table S4). This systematic review was registered under the International Prospective Register of Systematic Reviews (PROSPERO)—CRD42022314014. The articles were published from the year 2005 to 2021. The studies included both prospective studies (n = 9) [7,8,19,20,21,22,23,24,25] and retrospective (n = 8) [1,26,27,28,29,30,31,32]. Data collection was performed by extracting information on demographic data, composed of the author, year of publication, type of study, origin country, number of patients and participants, patients’ mean age, tumor type and its histology, tumor location, and the details of the control group, as shown in Table 2. For the main objective, we evaluated, extracted, and tabulated the information in Table 3 and Table 4. The information comprised (1) the evaluation of white matter tract tractography of interest in preoperative planning and intraoperative assessment; (2) type of surgery, any modification of the surgical approach planned based on DTI tractography assessment; (3) surgical outcome of the study; and, finally, a (4) summary of the main findings of the selected articles, as well as an overview of the (5) comparison between the DTI intervention group and the control group, are tabulated.
Table 2.
Demographic data of the patients, control participants, and tumor characteristics.
Table 3.
Comparison between the assessed DTI group and the control group.
Table 4.
Surgical Planning Approach Modification, Preoperative and Intraoperative Assessment Based on DTI and Tractography Data and Its Surgical Outcome.
3.2. Participants
The sample size ranged from 8 to 230 participants, including controlled participants. The total number of patients reviewed was 877, with 234 control patients, with slightly more male patient recruitment (n = 360) compared to female patient recruitment (n = 283). The age range for these studies was 1 to 87 years old, and we included five studies [21,24,26,27,30] that had pediatric patients, but this would not affect our objective, as only a few patients were involved. All types of tumor were studied. Although there were studies with patients with cavernous malformation brain lesions, our study excluded only the irrelevant patients, who were diagnosed with arteriovenous malformations, cavernous angiomas, and cavernous malformations, as the authors listed all of the individuals’ tumor types. Thus, we included these two papers [19,26]. The tumor site was not exclusive; however, three of the publications discussed tumors exclusively in the brainstem [1,26,30]. We decided to include all tumors from all locations. This information is summarized in Table 2. The white matter tracts of interest in the studies were primarily those in close proximity to the tumor and those associated with brain function, such as the corticospinal tract related to motor function [19,20,27,30,31,32], optic radiation responsible for eyesight [1,7,8,21,23,29,31], and inferior longitudinal fasciculus and arcuate fascicles that link to language [7,8,20,22,23,28,29,31]. These tracts were relevant for postoperative deficit assessment. In the following section, we will discuss the use of DTI in brain resection surgery.
3.3. Utilization of DTI in Brain Resection Surgery
All of the studies discussed the utilization of the DTI in brain tumor resection. One of them was primarily concerned with the ability to reconstruct the fiber tract in the presence of a brain tumor [1,7,8,19,20,21,22,23,24,25,26,27,28,29,30,31,32]. In addition, the use of DTI could predetermine the preplanning surgical approach [8]. Evaluation of DTI was performed in comparison with control patients, non-DTI, and DTI patients’ groups [1,21,22,23,25,28]; intraoperatively evaluation [1,7,8,19,20,21,22,23,24,25,26,27,28,29,30,31]; and quantified the sensitivity and specificity of the DTI technique in its tract identification, tumor resection rate, and mobility prediction [20,21,23,24,27,31]. We emphasized all these benefits of DTI for our primary investigation on whether re-evaluation and modifications of the preplanning surgery were made [7,8,26,27,29,30,32]. Finally, the effectiveness of the surgery was measured by positive indications of the outcome, mainly the gross total resection of the tumor [1,7,8,22,23,25,26,27,29,32] and any development of postoperative neurological deficits [1,19,20,21,23,24,26,28,30,31,32].
3.4. Comparison to the Control Group (n = 6)
We compared the DTI group and the non-DTI group for evidence to prove that the DTI is a practical neuro-navigation tool for neurosurgery. Most of the studies conducted [1,21,22,23,25,28] compared the DTI result with the outcome of the surgery. The investigations contrasted the DTI and non-DTI groups, with the DTI group having a higher chance of total gross resection and a lower risk of postoperative impairment [1,22,25]. Zakaria et al. looked into automated whole-brain tractography (AWBT) and compared it to brain mapping in groups with and without it. Although the risk was similar in both groups, those with AWBT with brain mapping were more likely to recover from any postoperative neurological abnormalities [28].
In a preliminary study on the clinical application of DTI on the optic pathway by Hajiabadi et al. (2016), comparisons were made of the assessment of preoperative, intraoperative, and postoperative effects on visual impairment caused by the compression of the optic chiasm. The control group recruited were patients diagnosed with other diseases. They claimed that patients with an abnormal visual impairment score had optic chiasm compression. For the control group, the visual examinations recorded normal visual status in preoperative and postoperative periods, revealing that the fibers crossing the optic chiasm were without any alterations [21]. In addition to greater GTR in high-grade glioma (HGG) patients and better postoperative Karnofsky Performance Status score ratings, DTI navigational surgery gave a 43 percent reduction in the risk of death during neurosurgery compared to non-DTI navigational surgery [25].
3.5. Preoperative and Intraoperative DTI Tractography Evaluation (n = 4)
Nimsky et al. (2005), Hajiabadi et al. (2006), Aibar-Duran et al. (2020), and Maesawa et al. (2010) investigated preoperative tractography and intraoperative tractography [21,23,24,27]. All of these studies reported the use of intraoperative scanned DTI and its evaluation compared to preoperative DTI, except for Aibar-Duran et al. who evaluated the intraoperative navigated DTI. Nimsky et al. (2005) and Maesawa et al. (2010) documented fiber shifting intraoperatively, and the inward and outward shifting were determined to be undetectable preoperatively [24,27]. According to Hajiabadi et al., the postoperative mean distance between the optic tracts in tractography decreased intraoperatively. In the majority of the patients, there were no crossing fibers in the optic chiasm prior to surgery. Intraoperatively, however, the fibers were detected in five more individuals [21]. A study conducted by Aibar-Duran et al. (2020), which compared intraoperative navigated DTI with a control group, concluded that intraoperative navigated DTI tractography would shorten the awake surgery time [23].
3.6. Surgical Approach or Preoperative Plan Modification Concerning DTI Data or Tractography (n = 7)
The assessment of fiber trajectories of the tumor patient preoperatively or intraoperatively can result in the modification of initial surgical planning. Seven studies discussed these changes. Romano et al. (2009) delineated that the preoperative DTI depicted an inaccurate shifting of the central white matter tract, and that revision of surgical planning was needed to determine the resection margin. The study concluded that MR-tractography modified the planned surgical procedure in nearly 82 percent of cases [7]. Similarly to this, the location of the surgical approach was changed in Cao et al. (2010), and this modification only happened in one out of eight patients for the brainstem lesion [26]. Maesawa et al. (2010) outlined conditions to determine the surgical approach regarding the need for intraoperative DTI rescanning, resulting in total resection of the brain tumors of patients [27].
Research conducted by Faust and Vajkoczy (2016) revealed not the modification of surgical planning, but the predetermined surgical approach based on the location of the tractography of optic radiation tracts in relation to the tumor. Temporal tumor growth effects on optic radiation caused fixed pattern displacement, and these patterns provided a potential entry point for surgical tumor resection [8].
In contrast to these real studies, Alexopoulous et al. (2019) performed a stimulation of neurosurgeons’ decision-making in preoperative surgical planning. Two blinded neurosurgeons analyzed preoperative DTI and MRI scan imaging and determined the surgical decision for the brain tumor resection. However, after analyzing DTI tractography data on a few of their patients, they discovered that this technique had no effect on the surgical strategy. Nonetheless, it did corroborate the resection decision to move from total resection to subtotal resection, initially solely based on MRI, resulting in better surgical results [29]. Similarly, Buchmann et al. observed that DTI fiber tracking did not influence surgical planning or intraoperative course. However, post hoc imaging DTI offered the neurosurgeon the opportunity to adjust the surgical approach strategy in one of the instances analyzed [32]. In contrast to Alexopoulous et al. and Buchmann et al., Xiao et al. considered a change in surgical approach in more than a quarter of patients, based on the DTI data results in their study on the visualization of corticospinal tract. Following the DTI data, surgical approach selection was more diversified and particular than prior to the DTI result, with a preference for far lateral approaches [30].
3.7. Evaluation of DTI Tractography Utilization on Postoperative Surgical Outcome
The surgical outcome was assessed to evaluate GTR and the patients’ postoperative neurological function. In the present study, several of the selected papers reported their achievements based on the increasing decision rate in deciding the total gross resection of the patients [1,7,8,22,23,25,26,27,29], and the neurological deficits improved after time postoperatively [1,19,20,21,23,24,26,28,30,31,32], in the case where DTI was integrated as a preoperative planning tool. Many of the studies concluded that with the aid of DTI, the modification to initial preoperative planning could have been made mainly to exchange the outcome, in terms of maximizing the removal of the tumor [1,7,8,19,20,21,22,23,24,25,26,27,28,29,30,31,32]. In addition, the optimum surgical decision for tumor resection was given to the patients, mainly in cooperation with determining the best surgical type and approach [8,25] or changing the initial preoperative planning intraoperatively [7,26]. The utilization of DTI for postoperative outcome improvement mainly resulted in the improvement of neurological deficits. Some studies agreed that this could predict postoperative deficits and functional preservation [31].
4. Discussion
The present study discussed the utilization of DTI in brain tumor preoperative planning, to evaluate the benefits of DTI and its significance for successful neurosurgery. We found a specific selection of articles that used only DTI neuroimaging for preoperative, intraoperative, and postoperative assessment, aside from routine MRI scanning. These selected studies highlighted a few points. First of all, DTI is the only tool for in vivo visualization of white matter tract pathways, and it may aid in understanding the anatomy, architecture, and microstructure of the tracts, as well as localizing tumors involving the fiber tracts [1,7,8,19,20,21,22,23,24,25,26,27,28,29,30,31,32]. The sensitivity and specificity were proven by identifying tracts as 95% and 100%, respectively [33]. Most of the tracts were successfully reconstructed [1,7,24]; however, the technique has improved over time. The DTI technique is one of many tools used for preoperative planning and its impact on neurosurgical outcomes could depend on multiple factors. However, from our review, using DTI preoperatively could predict potential postoperative neurological deficits and increase the possibility of preserving brain functions [1,19,20,21,22,23,24,26,27,28,29,30,31]. Therefore, the introduction of DTI for preoperative planning and intraoperatively would be a significant step for a better surgical outcomes, based on the comparisons made in this study [1,21,22,23,25,28].
We compared the interventions in DTI and control groups, to assess their efficacy. This comparison showed that the most DTI utilizing group had better surgical decision outcomes on total gross resection. Furthermore, the postoperative neurological deficits were mostly improved and required less time for neurosurgery compared to the control group [1,21,22,23,25,28]. This is parallel with the statement by Aibar-Duran et al. 2020, in which the sensitivity and specificity for predicting complete tumor resection were 88% and 62.5 for the non-DTI group and 100% and 80% for the DTI group [23]. Thus, DTI provided the optimum surgical decision-making in deciding GTR and revealed the surgical path that could potentially alleviate the patient’s neurological deficits postoperatively.
Preoperative tractography was utilized for surgical planning, so that a proper plan could be executed. Robust analysis of the white matter tract tractography pattern, colors, and fiber pathways would benefit a neurosurgeon, as additional information is essential. The characterization and criteria of white matter tract microstructure interaction with the different types of the tumor would give an initial suggestion on how the surgical approach should be assigned [1,10]. In addition, by also analyzing the tumor location and its shifting effect on the white matter tract, this minor piece of information could become the permanent method for surgical approaches, as Faust and Vajkoczy (2016) reported. The surgical procedure was predetermined by the optic radiation fiber shift pattern, which could benefit the cases where DTI is unavailable [8].
In this review, we analyzed all types of tumors and grouped them into HGG, low-grade gliomas (LGG), and metastasis. Different types of tumors may have different interactions and effects on the fiber tract, which may necessitate surgical intervention [1,4]. Unlike HGG and metastasis, most LGGs have a higher chance of surgical modification [34]. Witwer et al. (2002) reported four types of characterization of white matter tract microstructure changes: displacement, infiltration, edema, and destruction. The classification of these characteristics depends on the value of fractional anisotropy and the visualization of the normality of the microstructure orientation of the white matter tract [4]. Papers have discussed the classification of fiber tracts in different tumors, such as benign and malignant tumors, and showed that most of the malignant tumors depicted a destruction pattern [35,36,37]. In terms of the rate of tumor resection, infiltrating tumors could only yield a subtotal resection, and HGG usually ended with a total resection [34,36]. We have included supratentorial tumors and a few papers on brainstem tumors. It should be known that the treatment and the prognosis of tumors in the brainstem are different, and, as proposed by Cao et al., preplanning of brainstem tumor surgery should be done with an individualized approach [26,35]. This should be addressed properly, as we wanted to conduct a systematic review of the usefulness of DTI in tumor resection surgery in a broader sense.
Intraoperatively navigated tractography gives a more precise fiber tracking depiction than preoperative tractography, and it has the advantage of shortening the surgery time [23]. In addition, brain shifting of the fiber could happen in the brain, and the location of the fibers visualized in preoperative DTI might be different from the intraoperative DTI [24]. White matter tract shifting occurs for many reasons, including gravity or head positioning, surgical equipment, tissue loss, tissue fluid, and tumor type. In the intraoperative session, the brain shifting would be predictable in the case of the head position during the operation. However, the inward and outward shift are unpredictable and mutually exclusive [24,38].
Intraoperative DTI assessment contributes to successful awake-surgery, plus any preoperative error can be corrected intraoperatively [20,33]. Although the utilization of DTI is sufficient, the establishment of brain-mapping for preoperative planning is needed [28]. Thus, it is crucial to integrate this with other navigation methods, such as DES or direct cortical electrostimulation, which is the gold standard for brain tumor resection methods in awake surgery, as an indication of the functional border of the brain [19,20,38,39,40]; as well as the use of mixed techniques, which include fMRI for a complete understanding of the functional part of the brain [38]. This is needed due to the finding that although the predictive accuracy of the DTI technique to locate the tracts was undeniably high, the specificity prediction of the tract correlated with the function and stimulation was low intraoperatively [31].
As shown by Hajiabadi et al. and Voets et al., DTI fiber tracking could predict the postoperative deficit [21,31]. A study by Sollmann et al. (2016) showed that preoperative DTI fiber tracking derived from navigated transcranial magnetic stimulation detected the hemispeheric connectivity, which could contribute to surgery-related aphasia [41]. Postoperative neurological deficits could be avoided with proper surgical planning, and from our standpoint, DTI tractography could assist in preserving the eloquent functioning of the brain, mainly when used together with intraoperative subcortical stimulation combined with neurophysiological assessment [33].
The act of modification and re-evaluation of surgical plans indicates more information is required, and the utilization of DTI should have been done routinely. Most studies had to re-evaluate the planned surgical process in the intraoperative courses [7,27]. Based on our evaluation, the modification was mainly done on the initial GTR, whether the resection was a subtotal or total removal. Ultimately, as backed by most studies, GTR of gliomas, either HGG or LGG, would increase the median survival rate by more than 120% [42]. While most agreed that this only concerns the GTR changes, some have shown its effect in modifying the location of surgical approaches [8,42].
DTI tractography, as an essential tool in neurosurgery care and treatment, still raises questions, as there is no reliable standard [43]. Some findings argue that preoperative DTI is simply one tool of many, and that it does not give any positive feedback in neurosurgery as it cannot influence surgical strategy or modify surgical planning. In this review, Buchmann et al. and Alexopoulos et al. gave us two sides of the same coin [29,32]. A recent systematic review and meta-analysis study shared their analysis, suggesting either a combination of DTI, fMRI, and intraoperative MRI used in intraoperative neuronavigation, or by themselves, was insufficient to conclude that these advanced imaging techniques have the potential to influence the GTR and neurological preservation [44]. The use of imaging modalities in surgery could increase the GTR rate; however, this would not improve the surgical outcome. In their analysis of iMRI studies, the authors pointed out that the imaging modality could permit better GTR and preserve the eloquent area in incomplete resection, when GTR not feasible. However, it is important to highlight that, in regards to their study on DTI, DTI has not been extensively studied and an exclusive meta-analysis on DTI studies should be done [44].
Limitations
We should point out some limitations of our studies, by recognizing the small sample sizes of the selected studies. The DTI and tractography analysis processes have some limitations. The standardization of the fractional anisotropy and angle threshold could be hard to achieve due to edema and infiltration surrounding the tumor [23]. The cons of DTI are that it is user-dependent and requires a vast amount of anatomical knowledge. Importantly, DTI analysis requires understanding the physical nature of fiber, which includes crossing fibers, brain shifting, and corresponding parameters. These are a few examples of issues identified, from the many more addressed by the studies [10,42,45], and these could be systematically reviewed. Understanding the technical aspects of DTI could give us a better view of our study, as subtopic on the DTI acquisition parameters should be done. A magnetic resonance with a field strength of 1.5 Tesla is sufficient for diagnostic purposes when properly protocoled; nevertheless, 3 Tesla is regarded as the ideal instrument for DTI [46]. Quantitative DTI, fractional anisotropy, and mean diffusivity could provide possible indicators for successful surgery. Unlike other diseases, such as epilepsy or multiple sclerosis, the primary goal of DTI in neurosurgery is to visualize the fiber tracts, without delving deeper into its quantitative impact, which may be beneficial in tumor resection procedures and for postoperative neurological preservation. Combining more modalities would benefit the utilization of DTI in understanding the brain structure in neuronavigation. It is sufficient for the eloquent part of the brain to see the behaviors that cater to the brain’s functional part. The main reason why most preoperative DTI uses awake surgery is to ensure the validation of functional parts of the brain; mainly to preserve them. From the historical timeline of the progression of DTI, the utilization of the technique could be seen as a slow process. There are many other techniques of tractography, and DTI tractography data is the most utilized in the clinical field. Diffusion-weighted MRI provided the sequences for tractography; however, a thorough understanding in the processing algorithm is needed [43]. With the advance of scientific research and development, the newest mathematical models of diffusion MRI techniques, which is HARDI, and diffusion spectrum imaging give alternatives to avoid the shortcomings of DTI tractography [47]. In future studies, the emphasis will be on the use of advanced techniques such as HARDI. There needs to be a quantitative evaluation of its effectiveness. A meta-analysis could be the next review, to see if there are significant quantitative findings.
5. Conclusions
We have reviewed some of the benefits of utilizing DTI in neurosurgery, ensuring that many more will be discovered in the future. There are pros and cons to using DTI, mainly regarding its utilization as a single technique. Past and ongoing studies on DTI have shown the effects of DTI’s usage perioperatively and postoperatively. It can give essential information on the related white matter tract pathways and their relation to the tumors’ features, for a better surgical approach; and to a certain extent, potentially decreases the neurological deficit in patients’ quality of life. We can conclude that preoperative DTI has given us important information on fibers, and eventually, could help in evaluating operative planning, based on the evidence when compared to the non-DTI group. Intraoperative DTI, as well as intraoperative navigated DTI, should be used, and validation of the functional white matter tract would be possible with the aid of intraoperative subcortical stimulation and neurophysiological assessment, as collecting as much information as possible about the surrounding tissue of the tumor could assist in alleviating the postoperative deficit. However, more studies are needed, and applications need to be performed and validated, mainly on the use of DTI quantitative parameters, to help with neurosurgery resection. So that artefacts and complications may be controlled and managed in the future, the DTI technique should be used as a routine neuroimaging procedure, mainly in any neurosurgery and diseases that could potentially damage the white matter tract fibers.
Supplementary Materials
The following supporting information can be downloaded at: https://www.mdpi.com/article/10.3390/cancers14102466/s1, Table S1: PRISMA 2020 checklist, Table S2: PRISMA for abstract checklist, Table S3: Advanced Search Keyword Chain for Electronic Database. Table S4: Quality Assessment Selected Studies by NHLBI, NIH.
Author Contributions
All authors contributed to the study. Material preparation, literature search, and analysis were performed by A.A.M. and checked by H.A.M. and N.Y. The first draft of the manuscript was written by A.A.M. and Z.I. contributed in manuscript revision. All authors commented on the previous versions of the manuscript. All authors have read and agreed to the published version of the manuscript.
Funding
This work was supported by the Geran Galakan Penyelidik Muda (Incentive Grant for Young Researchers) Universiti Kebangsaan Malaysia GGPM-2017-016.
Institutional Review Board Statement
Not applicable since this study uses data from previous published study.
Informed Consent Statement
Not applicable since this study uses data from previous published study.
Data Availability Statement
The data supporting reported results can be found in the main article or Supplementary Materials.
Conflicts of Interest
The authors declare no conflict of interest.
References
- Yu, C.S.; Li, K.C.; Xuan, Y.; Ji, X.M.; Qin, W. Diffusion tensor tractography in patients with cerebral tumors: A helpful technique for neurosurgical planning and postoperative assessment. Eur. J. Radiol. 2005, 56, 197–204. [Google Scholar] [CrossRef] [PubMed]
- Yu, Q.; Lin, K.; Liu, Y.; Li, X. Clinical Uses of Diffusion Tensor Imaging Fiber Tracking Merged Neuronavigation with Lesions Adjacent to Corticospinal Tract: A Retrospective Cohort Study. J. Korean Neurosurg. Soc. 2020, 63, 248–260. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Essayed, W.I.; Zhang, F.; Unadkat, P.; Cosgrove, G.R.; Golby, A.J.; O’Donnell, L.J. White matter tractography for neurosurgical planning: A topography-based review of the current state of the art. NeuroImage Clin. 2017, 15, 659–672. [Google Scholar] [CrossRef]
- Witwer, B.P.; Moftakhar, R.; Hasan, K.M.; Deshmukh, P.; Haughton, V.; Field, A.; Arfanakis, K.; Noyes, J.; Moritz, C.; Meyerand, M.E.; et al. Diffusion-tensor imaging of white matter tracts in patients with cerebral neoplasm. J. Neurosurg. 2002, 97, 568–575. [Google Scholar] [CrossRef] [PubMed]
- Wang, J.L.; Elder, J.B. Techniques for Open Surgical Resection of Brain Metastases. Neurosurg. Clin. North Am. 2020, 31, 527–536. [Google Scholar] [CrossRef] [PubMed]
- Li, Y.; Zhang, W. Quantitative evaluation of diffusion tensor imaging for clinical management of glioma. Neurosurg. Rev. 2020, 43, 881–891. [Google Scholar] [CrossRef]
- Romano, A.; D’Andrea, G.; Minniti, G.; Mastronardi, L.; Ferrante, L.; Fantozzi, L.M.; Bozzao, A. Pre-surgical planning and MR-tractography utility in brain tumour resection. Eur. Radiol. 2009, 19, 2798–2808. [Google Scholar] [CrossRef]
- Faust, K.; Vajkoczy, P. Distinct displacements of the optic radiation based on tumor location revealed using preoperative diffusion tensor imaging. J. Neurosurg. 2016, 124, 1343–1352. [Google Scholar] [CrossRef] [Green Version]
- Assaf, Y.; Pasternak, O. Diffusion Tensor Imaging (DTI)-based White Matter Mapping in Brain Research: A Review. J. Mol. Neurosci. 2008, 34, 51–61. [Google Scholar] [CrossRef]
- Soares, J.M.; Marques, P.; Alves, V.; Sousa, N. A hitchhiker’s guide to diffusion tensor imaging. Front. Neurosci. 2013, 7, 31. [Google Scholar] [CrossRef] [Green Version]
- Van Hecke, W.; Emsell, L.; Sunaert, S. Diffusion Tensor Imaging: A Practical Handbook; Springer: New York, NY, USA, 2016; pp. 1–440. [Google Scholar] [CrossRef]
- Moher, D.; Liberati, A.; Tetzlaff, J.; Altman, D.G. Preferred reporting items for systematic reviews and meta-analyses: The PRISMA statement. BMJ 2009, 339, 332–336. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Manan, H.; Yahya, N. Ageing and Olfactory Dysfunction in Trisomy 21: A Systematic Review. Brain Sci. 2021, 11, 952. [Google Scholar] [CrossRef] [PubMed]
- Yahya, N.; Manan, H.A. Utilisation of Diffusion Tensor Imaging in Intracranial Radiotherapy and Radiosurgery Planning for White Matter Dose Optimization: A Systematic Review. World Neurosurg. 2019, 130, e188–e198. [Google Scholar] [CrossRef] [PubMed]
- Manan, H.A.; Franz, E.A.; Yahya, N. The utilisation of resting-state fMRI as a pre-operative mapping tool in patients with brain tumours in comparison to task-based fMRI and intraoperative mapping: A systematic review. Eur. J. Cancer Care 2021, 30, e13428. [Google Scholar] [CrossRef]
- Yahya, N.; Manan, H.A. Diffusion tensor imaging indices to predict cognitive changes following adult radiotherapy. Eur. J. Cancer Care 2021, 30, e13329. [Google Scholar] [CrossRef]
- Voon, N.S.; Manan, H.A.; Yahya, N. Cognitive Decline following Radiotherapy of Head and Neck Cancer: Systematic Review and Meta-Analysis of MRI Correlates. Cancers 2021, 13, 6191. [Google Scholar] [CrossRef]
- Manan, H.A.; Yahya, N.; Han, P.; Hummel, T. A systematic review of olfactory-related brain structural changes in patients with congenital or acquired anosmia. Brain Struct. Funct. 2022, 227, 177–202. [Google Scholar] [CrossRef]
- Okada, T.; Mikuni, N.; Miki, Y.; Kikuta, K.-I.; Urayama, S.-I.; Hanakawa, T.; Fushimi, Y.; Yamamoto, A.; Kanagaki, M.; Fukuyama, H.; et al. Corticospinal Tract Localization: Integration of Diffusion-Tensor Tractography at 3-T MR Imaging with Intraoperative White Matter Stimulation Mapping—Preliminary Results. Radiology 2006, 240, 849–857. [Google Scholar] [CrossRef]
- Bello, L.; Castellano, A.; Fava, E.; Casaceli, G.; Riva, M.; Scotti, G.; Gaini, S.M.; Falini, A. Intraoperative use of diffusion tensor imaging fiber tractography and subcortical mapping for resection of gliomas: Technical considerations. Neurosurg. Focus 2010, 28, E6. [Google Scholar] [CrossRef] [Green Version]
- Hajiabadi, M.; Samii, M.; Fahlbusch, R. A preliminary study of the clinical application of optic pathway diffusion tensor tractography in suprasellar tumor surgery: Preoperative, intraoperative, and postoperative assessment. J. Neurosurg. 2016, 125, 759–765. [Google Scholar] [CrossRef] [Green Version]
- Zhang, H.; Feng, Y.; Cheng, L.; Liu, J.; Li, H.; Jiang, H. Application of diffusion tensor tractography in the surgical treatment of brain tumors located in functional areas. Oncol. Lett. 2020, 19, 615–622. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Aibar-Durán, J.; De Quintana-Schmidt, C.; Holzpafel, M.J..; Hernández, F.M.; Cortés, C.A.; Martínez, G.V.; Bertrán, G.C. Intraoperative Use and Benefits of Tractography in Awake Surgery Patients. World Neurosurg. 2020, 137, e347–e353. [Google Scholar] [CrossRef] [PubMed]
- Nimsky, C.; Ganslandt, O.; Hastreiter, P.; Wang, R.; Benner, T.; Sorensen, A.G.; Fahlbusch, R. Preoperative and Intraoperative Diffusion Tensor Imaging-based Fiber Tracking in Glioma Surgery. Neurosurgery 2005, 56, 130–138. [Google Scholar] [CrossRef] [PubMed]
- Wu, J.S.; Zhou, L.F.; Tang, W.J.; Mao, Y.; Hu, J.; Song, Y.Y.; Hong, X.N.; Du, G.H. Clinical evaluation and follow-up outcome of diffusion tensor imaging-based functional neuronavigation: A prospective, controlled study in patients with gliomas involving pyramidal tracts. Neurosurgery 2007, 61, 935–948. [Google Scholar] [CrossRef]
- Lv, J.; Wei, X.; Quan, W.; Cao, Z. Appliance of preoperative diffusion tensor imaging and fiber tractography in patients with brainstem lesions. Neurol. India 2010, 58, 886–890. [Google Scholar] [CrossRef]
- Maesawa, S.; Fujii, M.; Nakahara, N.; Watanabe, T.; Wakabayashi, T.; Yoshida, J. Intraoperative Tractography and Motor Evoked Potential (MEP) Monitoring in Surgery for Gliomas Around the Corticospinal Tract. World Neurosurg. 2010, 74, 153–161. [Google Scholar] [CrossRef]
- Zakaria, H.; Haider, S.; Lee, I. Automated Whole Brain Tractography Affects Preoperative Surgical Decision Making. Cureus 2017, 9, e1656. [Google Scholar] [CrossRef] [Green Version]
- Alexopoulos, G.; Cikla, U.; El Tecle, N.; Kulkarni, N.; Pierson, M.; Mercier, P.; Kemp, J.; Coppens, J.; Mahmoud, S.; Sehi, M.; et al. The Value of White Matter Tractography by Diffusion Tensor Imaging in Altering a Neurosurgeon’s Operative Plan. World Neurosurg. 2019, 132, e305–e313. [Google Scholar] [CrossRef]
- Xiao, X.; Kong, L.; Pan, C.; Zhang, P.; Chen, X.; Sun, T.; Wang, M.; Qiao, H.; Wu, Z.; Zhang, J.; et al. The role of diffusion tensor imaging and tractography in the surgical management of brainstem gliomas. Neurosurg. Focus 2021, 50, E10. [Google Scholar] [CrossRef]
- Voets, N.L.; Pretorius, P.; Birch, M.D.; Apostolopoulos, V.; Stacey, R.; Plaha, P. Diffusion tractography for awake craniotomy: Accuracy and factors affecting specificity. J. Neuro-Oncol. 2021, 153, 547–557. [Google Scholar] [CrossRef]
- Buchmann, N.; Gempt, J.; Stoffel, M.; Förschler, A.; Meyer, B.; Ringel, F. Utility of diffusion tensor-imaged (DTI) motor fiber tracking for the resection of intracranial tumors near the corticospinal tract. Acta Neurochir. 2011, 153, 68–74. [Google Scholar] [CrossRef] [PubMed]
- Bello, L.; Gambini, A.; Castellano, A.; Carrabba, G.; Acerbi, F.; Fava, E.; Giussani, C.; Cadioli, M.; Blasi, V.; Casarotti, A.; et al. Motor and language DTI Fiber Tracking combined with intraoperative subcortical mapping for surgical removal of gliomas. NeuroImage 2008, 39, 369–382. [Google Scholar] [CrossRef] [PubMed]
- Alam Khan, K.; Jain, S.K.; Sinha, V.D.; Sinha, J. Preoperative Diffusion Tensor Imaging: A Landmark Modality for Predicting the Outcome and Characterization of Supratentorial Intra-Axial Brain Tumors. World Neurosurg. 2019, 124, e540–e551. [Google Scholar] [CrossRef] [PubMed]
- Ibrahim, A.; Gomaa, M.; Sakr, H.; Elzaher, Y.A. Role of diffusion tensor imaging in characterization and preoperative planning of brain neoplasms. Egypt. J. Radiol. Nucl. Med. 2013, 44, 297–307. [Google Scholar] [CrossRef] [Green Version]
- Shalan, M.E.; Soliman, A.Y.; Nassar, I.A.; Alarabawy, R.A. Surgical planning in patients with brain glioma using diffusion tensor MR imaging and tractography. Egypt. J. Radiol. Nucl. Med. 2021, 52, 110. [Google Scholar] [CrossRef]
- Dubey, A.; Kataria, R.; Sinha, V.D. Role of diffusion tensor imaging in brain tumor surgery. Asian J. Neurosurg. 2018, 13, 302–306. [Google Scholar] [CrossRef]
- Gerard, I.J.; Kersten-Oertel, M.; Petrecca, K.; Sirhan, D.; Hall, J.A.; Collins, D.L. Brain shift in neuronavigation of brain tumors: A review. Med Image Anal. 2017, 35, 403–420. [Google Scholar] [CrossRef]
- Costabile, J.D.; Alaswad, E.; D’Souza, S.; Thompson, J.A.; Ormond, D.R. Current Applications of Diffusion Tensor Imaging and Tractography in Intracranial Tumor Resection. Front. Oncol. 2019, 9, 1–9. [Google Scholar] [CrossRef]
- Mikuni, N.; Okada, T.; Enatsu, R.; Miki, Y.; Urayama, S.-I.; Takahashi, J.A.; Nozaki, K.; Fukuyama, H.; Hashimoto, N. Clinical significance of preoperative fibre-tracking to preserve the affected pyramidal tracts during resection of brain tumours in patients with preoperative motor weakness. J. Neurol. Neurosurg. Psychiatry 2007, 78, 716–721. [Google Scholar] [CrossRef] [Green Version]
- Sollmann, N.; Kubitscheck, A.; Maurer, S.; Ille, S.; Hauck, T.; Kirschke, J.S.; Ringel, F.; Meyer, B.; Krieg, S.M. Preoperative language mapping by repetitive navigated transcranial magnetic stimulation and diffusion tensor imaging fiber tracking and their comparison to intraoperative stimulation. Neuroradiology 2016, 58, 807–818. [Google Scholar] [CrossRef]
- Lara-Velazquez, M.; Al-Kharboosh, R.; Jeanneret, S.; Vazquez-Ramos, C.; Mahato, D.; Tavanaiepour, D.; Rahmathulla, G.; Quinones-Hinojosa, A. Advances in Brain Tumor Surgery for Glioblastoma in Adults. Brain Sci. 2017, 7, 166. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Wende, T.; Hoffmann, K.-T.; Meixensberger, J. Tractography in Neurosurgery: A Systematic Review of Current Applications. J. Neurol. Surg. Part A Cent. Eur. Neurosurg. 2020, 81, 442–455. [Google Scholar] [CrossRef] [PubMed]
- Caras, A.; Mugge, L.; Miller, W.; Mansour, T.R.; Schroeder, J.; Medhkour, A. Usefulness and Impact of Intraoperative Imaging for Glioma Resection on Patient Outcome and Extent of Resection: A Systematic Review and Meta-Analysis. World Neurosurg. 2020, 134, 98–110. [Google Scholar] [CrossRef]
- Leclercq, D.; Delmaire, C.; de Champfleur, N.M.; Chiras, J.; Lehéricy, S. Diffusion Tractography: Methods, Validation and Applications in Patients with Neurosurgical Lesions. Neurosurg. Clin. North Am. 2011, 22, 253–268. [Google Scholar] [CrossRef] [PubMed]
- Sąsiadek, M.J.; Szewczyk, P.; Bladowska, J. Application of diffusion tensor imaging (DTI) in pathological changes of the spinal cord. Med Sci. Monit. 2012, 18, RA73–RA79. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Mukherjee, P.; Chung, S.; Berman, J.; Hess, C.; Henry, R. Diffusion Tensor MR Imaging and Fiber Tractography: Technical Considerations. Am. J. Neuroradiol. 2008, 29, 843–852. [Google Scholar] [CrossRef] [PubMed] [Green Version]
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).