
Surviving Elderly Patients with Head-and-Neck Squamous Cell Carcinoma—What Is the Long-Term Quality of Life after Curative Radiotherapy?

 , ,
, , 

Abstract
Simple Summary
Abstract
1. Introduction
2. Results
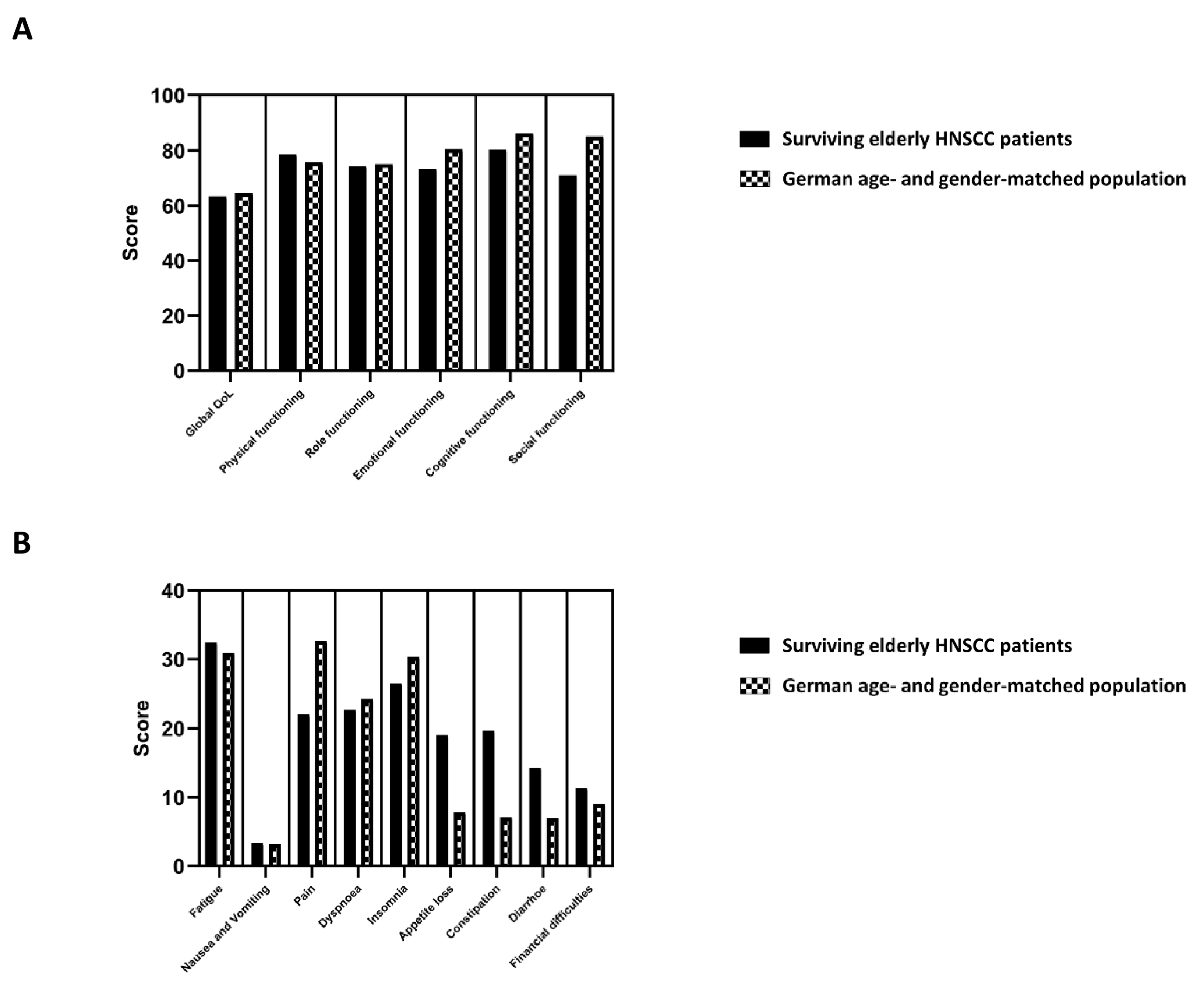
2.1. Long-Term QoL Is Comparable between Surviving Elderly HNSCC Patients and the General Population
2.2. HPV Positivity and Performance Status Correspond with Long-Term QoL in Surviving Elderly HNSCC Patients
2.3. Prior Tumor Resection and Concomitant Chemotherapy Do Not Influence Long-Term QoL in Surviving Elderly HNSCC Patients
2.4. Long-Term QoL in Surviving Elderly HNSCC Patients Does Not Correlate with Physician-Assessed CTCAE-Based Chronic Toxicities
3. Discussion
4. Materials and Methods
4.1. Patients and Treatment
4.2. Toxicity Analyses
4.3. Patient and Tumor Characteristics
4.4. QoL and Patient Satisfaction Questionnaires
4.5. Statistical Analysis
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Bray, F.; Ferlay, J.; Soerjomataram, I.; Siegel, R.L.; Torre, L.A.; Jemal, A. Global cancer statistics 2018: GLOBOCAN estimates of incidence and mortality worldwide for 36 cancers in 185 countries. CA Cancer J. Clin. 2018, 68, 394–424. [Google Scholar] [CrossRef] [PubMed]
- Grenman, R.; Chevalier, D.; Gregoire, V.; Myers, E.; Rogers, S. Treatment of head and neck cancer in the elderly: European Consensus (panel 6) at the EUFOS Congress in Vienna 2007. Eur. Arch. Otorhinolaryngol. 2010, 267, 1619–1621. [Google Scholar] [CrossRef] [PubMed]
- Vigneswaran, N.; Williams, M.D. Epidemiologic trends in head and neck cancer and aids in diagnosis. Oral Maxillofac. Surg. Clin. N. Am. 2014, 26, 123–141. [Google Scholar] [CrossRef] [PubMed]
- Smith, B.D.; Smith, G.L.; Hurria, A.; Hortobagyi, G.N.; Buchholz, T.A. Future of cancer incidence in the United States: Burdens upon an aging, changing nation. J. Clin. Oncol. 2009, 27, 2758–2765. [Google Scholar] [CrossRef] [PubMed]
- Gugić, J.; Strojan, P. Squamous cell carcinoma of the head and neck in the elderly. Rep. Pract. Oncol Radiother. 2012, 18, 16–25. [Google Scholar] [CrossRef]
- Lacas, B.; Carmel, A.; Landais, C.; Wong, S.J.; Licitra, L.; Tobias, J.S.; Burtness, B.; Grazia Ghi, M.; Cohen, E.E.W.; Grau, C.; et al. Meta-analysis of chemotherapy in head and neck cancer (MACH-NC): An update on 107 randomized trials and 19805 patients, on behalf of MACH-NC group. Radiother Oncol. 2021. [Google Scholar] [CrossRef] [PubMed]
- Bonner, J.A.; Harari, P.M.; Giralt, J.; Cohen, R.B.; Jones, C.U.; Sur, R.K.; Raben, D.; Baselga, J.; Spencer, S.A.; Zhu, J.; et al. Radiotherapy plus cetuximab for locoregionally advanced head and neck cancer: 5-year survival data from a phase 3 randomised trial, and relation between cetuximab-induced rash and survival. Lancet Oncol. 2010, 11, 21–28. [Google Scholar] [CrossRef]
- Yellen, S.B.; Cella, D.F.; Leslie, W.T. Age and clinical decision making in oncology patients. J. Natl. Cancer Inst. 1994, 86, 1766–1770. [Google Scholar] [CrossRef]
- Rühle, A.; Haehl, E.; David, H.; Kalckreuth, T.; Sprave, T.; Stoian, R.; Zamboglou, C.; Gkika, E.; Knopf, A.; Grosu, A.L.; et al. The Value of Laboratory Parameters for Anemia, Renal Function, Systemic Inflammation and Nutritional Status as Predictors for Outcome in Elderly Patients with Head-and-Neck Cancers. Cancers 2020, 12, 1698. [Google Scholar] [CrossRef]
- Rühle, A.; Stromberger, C.; Haehl, E.; Senger, C.; David, H.; Stoian, R.; Zamboglou, C.; Knopf, A.; Budach, V.; Grosu, A.L.; et al. Development and validation of a novel prognostic score for elderly head-and-neck cancer patients undergoing radiotherapy or chemoradiation. Radiother. Oncol. 2020, 154, 276–282. [Google Scholar] [CrossRef] [PubMed]
- Sprave, T.; Zamboglou, C.; Verma, V.; Nicolay, N.H.; Grosu, A.L.; Lindenmeier, J.; Tscheulin, D.K. Characterization of health-related quality of life based on the EQ-5D-5L questionnaire in head-and-neck cancer patients undergoing modern radiotherapy. Expert Rev. Pharmacoecon. Outcomes Res. 2020, 20, 673–682. [Google Scholar] [CrossRef]
- Derks, W.; Leeuw, J.R.; Hordijk, G.J.; Winnubst, J.A. Differences in coping style and locus of control between older and younger patients with head and neck cancer. Clin. Otolaryngol. 2005, 30, 186–192. [Google Scholar] [CrossRef] [PubMed]
- Kahn, S.B.; Houts, P.S.; Harding, S.P. Quality of life and patients with cancer: A comparative study of patient versus physician perceptions and its implications for cancer education. J. Cancer Educ. 1992, 7, 241–249. [Google Scholar] [CrossRef] [PubMed]
- Lipscomb, J.; Gotay, C.C.; Snyder, C.F. Patient-reported outcomes in cancer: A review of recent research and policy initiatives. CA Cancer J. Clin. 2007, 57, 278–300. [Google Scholar] [CrossRef] [PubMed]
- Khafif, A.; Posen, J.; Yagil, Y.; Beiser, M.; Gil, Z.; Ben-Yosef, R.; Landsberg, R.; Fliss, D.M. Quality of life in patients older than 75 years following major head and neck surgery. Head Neck 2007, 29, 932–939. [Google Scholar] [CrossRef]
- Silveira, A.P.; Gonçalves, J.; Sequeira, T.; Ribeiro, C.; Lopes, C.; Monteiro, E.; Pimentel, F.L. Geriatric oncology: Comparing health related quality of life in head and neck cancer patients. Head Neck Oncol. 2011, 3, 3. [Google Scholar] [CrossRef]
- Derks, W.; de Leeuw, R.J.; Hordijk, G.J.; Winnubst, J.A. Quality of life in elderly patients with head and neck cancer one year after diagnosis. Head Neck 2004, 26, 1045–1052. [Google Scholar] [CrossRef]
- Derks, W.; de Leeuw, J.R.; Hordijk, G.J.; Winnubst, J.A. Elderly patients with head and neck cancer: Short-term effects of surgical treatment on quality of life. Clin. Otolaryngol. Allied Sci. 2003, 28, 399–405. [Google Scholar] [CrossRef]
- Laraway, D.C.; Lakshmiah, R.; Lowe, D.; Roe, B.; Rogers, S.N. Quality of life in older people with oral cancer. Br. J. Oral Maxillofac. Surg. 2012, 50, 715–720. [Google Scholar] [CrossRef]
- Huang, T.-L.; Tsai, W.-L.; Chien, C.-Y.; Lee, T.-F.; Fang, F.-M. Quality of life for head and neck cancer patients treated by combined modality therapy: The therapeutic benefit of technological advances in radiotherapy. Qual. Life Res. 2010, 19, 1243–1254. [Google Scholar] [CrossRef]
- Wan, L.S.; Lee, T.-F.; Chien, C.-Y.; Chao, P.-J.; Tsai, W.-L.; Fang, F.-M. Health-related Quality of life in 640 head and neck cancer survivors after radiotherapy using EORTC QLQ-C30 and QLQ-H&N35 questionnaires. BMC Cancer 2011, 11, 128. [Google Scholar]
- So, W.K.W.; Chan, R.J.; Chan, D.N.S.; Hughes, B.G.M.; Chair, S.Y.; Choi, K.C.; Chan, C.W.H. Quality-of-life among head and neck cancer survivors at one year after treatment—A systematic review. Eur. J. Cancer 2012, 48, 2391–2408. [Google Scholar] [CrossRef]
- Nolte, S.; Waldmann, A.; Liegl, G.; Petersen, M.A.; Groenvold, M.; Rose, M. Updated EORTC QLQ-C30 general population norm data for Germany. Eur. J. Cancer 2020, 137, 161–170. [Google Scholar] [CrossRef]
- Herce Lopez, J.; Rollon Mayordomo, A.; Lozano Rosado, R.; Salazar Fernandez, C.I.; Gallana, S. Quality of life in long-term oral cancer survivors: A comparison with Spanish general population norms. J. Oral Maxillofac. Surg. 2009, 67, 1607–1614. [Google Scholar] [CrossRef]
- Hammerlid, E.; Taft, C. Health-related quality of life in long-term head and neck cancer survivors: A comparison with general population norms. Br. J. Cancer 2001, 84, 149–156. [Google Scholar] [CrossRef] [PubMed]
- Bower, J.E.; Ganz, P.A.; Desmond, K.A.; Bernaards, C.; Rowland, J.H.; Meyerowitz, B.E.; Belin, T.R. Fatigue in long-term breast carcinoma survivors: A longitudinal investigation. Cancer 2006, 106, 751–758. [Google Scholar] [CrossRef] [PubMed]
- Schmidt, M.E.; Hermann, S.; Arndt, V.; Steindorf, K. Prevalence and severity of long-term physical, emotional, and cognitive fatigue across 15 different cancer entities. Cancer Med. 2020, 9, 8053–8061. [Google Scholar] [CrossRef] [PubMed]
- Vilaseca, I.; Chen, A.Y.; Backscheider, A.G. Long-term quality of life after total laryngectomy. Head Neck 2006, 28, 313–320. [Google Scholar] [CrossRef] [PubMed]
- Dahlstrom, K.R.; Bell, D.; Hanby, D.; Li, G.; Wang, L.-E.; Wei, Q.; Williams, M.D.; Sturgis, E.M. Socioeconomic characteristics of patients with oropharyngeal carcinoma according to tumor HPV status, patient smoking status, and sexual behavior. Oral Oncol. 2015, 51, 832–838. [Google Scholar] [CrossRef]
- Ringash, J.; Fisher, R.; Peters, L.; Trotti, A.; O’Sullivan, B.; Corry, J.; Kenny, L.; Van Den Bogaert, W.; Wratten, C.; Rischin, D. Effect of p16 status on the quality-of-life experience during chemoradiation for locally advanced oropharyngeal cancer: A substudy of randomized trial Trans-Tasman Radiation Oncology Group (TROG) 02.02 (HeadSTART). Int. J. Radiat. Oncol. Biol. Phys. 2017, 97, 678–686. [Google Scholar] [CrossRef]
- Broglie, M.A.; Soltermann, A.; Haile, S.R.; Röösli, C.; Huber, G.F.; Schmid, S.; Stoeckli, S.J. Quality of life of oropharyngeal cancer patients with respect to treatment strategy and p16-positivity. Laryngoscope 2013, 123, 164–170. [Google Scholar] [CrossRef]
- Maxwell, J.H.; Mehta, V.; Wang, H.; Cunningham, D.; Duvvuri, U.; Kim, S.; Johnson, J.T.; Ferris, R.L. Quality of life in head and neck cancer patients: Impact of HPV and primary treatment modality. Laryngoscope 2014, 124, 1592–1597. [Google Scholar] [CrossRef] [PubMed]
- Bernier, J.; Domenge, C.; Ozsahin, M.; Matuszewska, K.; Lefèbvre, J.-L.; Greiner, R.H.; Giralt, J.; Maingon, P.; Rolland, F.; Bolla, M.; et al. Postoperative Irradiation with or without Concomitant Chemotherapy for Locally Advanced Head and Neck Cancer. N. Engl. J. Med. 2004, 350, 1945–1952. [Google Scholar] [CrossRef]
- Cooper, J.S.; Pajak, T.F.; Forastiere, A.A.; Jacobs, J.; Campbell, B.H.; Saxman, S.B.; Kish, J.A.; Kim, H.E.; Cmelak, A.J.; Rotman, M.; et al. Postoperative concurrent radiotherapy and chemotherapy for high-risk squamous-cell carcinoma of the head and neck. N. Engl. J. Med. 2004, 350, 1937–1944. [Google Scholar] [CrossRef]
- Yoshida, E.J.; Luu, M.; David, J.M.; Kim, S.; Mita, A.; Scher, K.; Shiao, S.L.; Tighiouart, M.; Ho, A.S.; Zumsteg, Z.S. Postoperative chemoradiotherapy in patients with head and neck cancer aged 70 or older with positive margins or extranodal extension and the influence of nodal classification. Head Neck 2018, 40, 1228–1236. [Google Scholar] [CrossRef]
- Giacalone, N.J.; Qureshi, M.M.; Mak, K.S.; Kirke, D.; Patel, S.A.; Shah, B.A.; Salama, A.R.; Jalisi, S.; Truong, M.T. Adjuvant chemoradiation does not improve survival in elderly patients with high-risk resected head and neck cancer. Laryngoscope 2018, 128, 831–840. [Google Scholar] [CrossRef]
- VanderWalde, N.A.; Meyer, A.M.; Deal, A.M.; Layton, J.B.; Liu, H.; Carpenter, W.R.; Weissler, M.C.; Hayes, D.N.; Fleming, M.E.; Chera, B.S. Effectiveness of chemoradiation for head and neck cancer in an older patient population. Int. J. Radiat. Oncol. Biol. Phys. 2014, 89, 30–37. [Google Scholar] [CrossRef] [PubMed]
- Logemann, J.A.; Pauloski, B.R.; Rademaker, A.W.; Lazarus, C.L.; Gaziano, J.; Stachowiak, L.; Newman, L.; MacCracken, E.; Santa, D.; Mittal, B. Swallowing disorders in the first year after radiation and chemoradiation. Head Neck 2008, 30, 148–158. [Google Scholar] [CrossRef] [PubMed]
- De Graeff, A.; De Leeuw, J.R.J.; Ros, W.J.G.; Hordijk, G.-J.; Blijham, G.H.; Winnubst, J.A.M. Long-Term Quality of Life of Patients with Head and Neck Cancer. Laryngoscope 2000, 110, 98–106. [Google Scholar] [CrossRef] [PubMed]
- Scrimger, R.; Kanji, A.; Parliament, M.; Warkentin, H.; Field, C.; Jha, N.; Hanson, J. Correlation between saliva production and quality of life measurements in head and neck cancer patients treated with intensity-modulated radiotherapy. Am. J. Clin. Oncol. 2007, 30, 271–277. [Google Scholar] [CrossRef]
- Jensen, K.; Bonde Jensen, A.; Grau, C. The relationship between observer-based toxicity scoring and patient assessed symptom severity after treatment for head and neck cancer. A correlative cross sectional study of the DAHANCA toxicity scoring system and the EORTC quality of life questionnaires. Radiother. Oncol. 2006, 78, 298–305. [Google Scholar] [CrossRef] [PubMed]
- Schuurhuizen, C.; Marino, P.; Braamse, A.M.J.; Buffart, L.M.; Joly, F.; Fizazi, K.; Habibian, M.; Boher, J.M.; Soulie, M.; Oudard, S.; et al. Impact of Patient- and Clinician-Reported Cumulative Toxicity on Quality of Life in Patients with Metastatic Castration-Naïve Prostate Cancer. J. Natl. Compr. Canc. Netw. 2018, 16, 1481–1488. [Google Scholar] [CrossRef] [PubMed]
- Sprave, T.; Zöller, D.; Stoian, R.; Rühle, A.; Kalckreuth, T.; Haehl, E.; Fahrner, H.; Binder, H.; Grosu, A.L.; Heinemann, F.; et al. App-Controlled Treatment Monitoring and Support for Head and Neck Cancer Patients (APCOT): Protocol for a Prospective Randomized Controlled Trial. JMIR Res. Protoc. 2020, 9, e21693. [Google Scholar] [CrossRef] [PubMed]
- El Shafie, R.A.; Weber, D.; Bougatf, N.; Sprave, T.; Oetzel, D.; Huber, P.E.; Debus, J.; Nicolay, N.H. Supportive Care in Radiotherapy Based on a Mobile App: Prospective Multicenter Survey. JMIR Mhealth Uhealth 2018, 6, e10916. [Google Scholar] [CrossRef]
- Denis, F.; Lethrosne, C.; Pourel, N.; Molinier, O.; Pointreau, Y.; Domont, J.; Bourgeois, H.; Senellart, H.; Trémolières, P.; Lizée, T.; et al. Randomized Trial Comparing a Web-Mediated Follow-up with Routine Surveillance in Lung Cancer Patients. J. Natl. Cancer Inst. 2017, 109, djx029. [Google Scholar] [CrossRef]
- Basch, E.; Deal, A.M.; Dueck, A.C.; Scher, H.I.; Kris, M.G.; Hudis, C.; Schrag, D. Overall Survival Results of a Trial Assessing Patient-Reported Outcomes for Symptom Monitoring During Routine Cancer Treatment. JAMA 2017, 318, 197–198. [Google Scholar] [CrossRef]
- Hofstede, G. The cultural relativity of the quality of life concept. Acad. Manag. Rev. 1984, 9, 389–398. [Google Scholar] [CrossRef]
- Morton, R.P. Studies in the quality of life of head and neck cancer patients: Results of a two-year longitudinal study and a comparative cross-sectional cross-cultural survey. Laryngoscope 2003, 113, 1091–1103. [Google Scholar] [CrossRef] [PubMed]
- Haehl, E.; Ruhle, A.; David, H.; Kalckreuth, T.; Sprave, T.; Stoian, R.; Becker, C.; Knopf, A.; Grosu, A.L.; Nicolay, N.H. Radiotherapy for geriatric head-and-neck cancer patients: What is the value of standard treatment in the elderly? Radiat. Oncol. 2020, 15, 31. [Google Scholar] [CrossRef]
- Sprave, T.; Rühle, A.; Stoian, R.; Weber, A.; Zamboglou, C.; Nieder, C.; Grosu, A.-L.; Nicolay, N.H. Radiotherapy for nonagenarians: The value of biological versus chronological age. Radiat. Oncol. 2020, 15, 113. [Google Scholar] [CrossRef] [PubMed]
- Schmidt, J.; Lamprecht, F.; Wittmann, W. Satisfaction with inpatient management. Development of a questionnaire and initial validity studies. Psychother. Psychosom. Med. Psychol. 1989, 39, 248–255. [Google Scholar] [PubMed]






{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Global QoL (QLQ-C30) | p-Value | ZUF-8 | p-Value | |
|---|---|---|---|---|
| 0 (n = 2) | 66.7 | 26.5 | ||
| 1 (n = 14) | 70.9 | 30.5 | ||
| 2 (n = 27) | 66.7 | 29.0 | ||
| 3 (n = 7) | 66.7 | 0.640 | 29.0 | 0.517 |
| Definitive (chemo)radiotherapy | Adjuvant (chemo)radiotherapy | p-Value | |
|---|---|---|---|
| No pain killer usage | 19 | 21 | |
| Pain killer usage | 4 | 6 | 0.736 |
| No nutritional supplement intake | 19 | 21 | |
| Nutritional supplement intake | 4 | 6 | 0.736 |
| No feeding tube dependence | 23 | 23 | |
| Feeding tube dependence | 0 | 4 | 0.115 |
| Parameter | Median (Range) | ||
|---|---|---|---|
| Age at Radiotherapy | 69 Years (65–82) | ||
| n | % | ||
| Gender | male | 32 | 64 |
| female | 18 | 36 | |
| Smoking | non-smoker | 19 | 38 |
| smoker | 24 | 48 | |
| missing | 7 | 14 | |
| Karnofsky performance status | 100% | 8 | 16 |
| 90% | 25 | 50 | |
| 80% | 13 | 26 | |
| 70% | 3 | 6 | |
| 60% | 1 | 2 | |
| CCI | 2 | 10 | 20 |
| 3 | 17 | 34 | |
| 4 | 9 | 18 | |
| 5 | 5 | 10 | |
| 6 | 7 | 14 | |
| 9 | 1 | 2 | |
| 10 | 1 | 2 | |
| Localization | nasopharynx | 1 | 2 |
| oropharynx | 26 | 52 | |
| hypopharynx | 1 | 2 | |
| oral cavity | 9 | 18 | |
| larynx | 6 | 12 | |
| multi-level | 3 | 6 | |
| others | 4 | 8 | |
| T stage | T1 | 12 | 24 |
| T2 | 17 | 34 | |
| T3 | 12 | 24 | |
| T4 | 9 | 18 | |
| n stage | N0 | 16 | 32 |
| N1 | 11 | 22 | |
| N2 | 18 | 36 | |
| N3 | 5 | 10 | |
| Grading | G1 | 2 | 4 |
| G2 | 23 | 46 | |
| G3 | 24 | 48 | |
| missing | 1 | 2 | |
| HPV | HPV-negative | 16 | 32 |
| HPV-positive | 18 | 36 | |
| missing | 16 | 32 | |
| Radiotherapy completion | completed | 48 | 96 |
| discontinued | 2 | 4 | |
| Chemotherapy completion (n = 31) | completed | 30 | 97 |
| discontinued | 1 | 3 | |
| Treatment concept | definitive radiotherapy | 3 | 6 |
| definitive chemoradiotherapy | 20 | 40 | |
| adjuvant radiotherapy | 16 | 32 | |
| adjuvant chemoradiotherapy | 11 | 22 | |
| Chemotherapy (n = 31) | platinum agents | 29 | 94 |
| nivolumab | 2 | 6 | |
| Median (range) | |||
| Radiation dose (definitive treatment) in EQD2 | 70 Gy (55–72) | ||
| Radiation dose (adjuvant treatment) in EQD2 | 66 Gy (59–66) | ||
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Rühle, A.; Haehl, E.; Kalckreuth, T.; Stoian, R.; Spohn, S.K.B.; Sprave, T.; Zamboglou, C.; Gkika, E.; Knopf, A.; Grosu, A.-L.; et al. Surviving Elderly Patients with Head-and-Neck Squamous Cell Carcinoma—What Is the Long-Term Quality of Life after Curative Radiotherapy? Cancers 2021, 13, 1275. https://doi.org/10.3390/cancers13061275
Rühle A, Haehl E, Kalckreuth T, Stoian R, Spohn SKB, Sprave T, Zamboglou C, Gkika E, Knopf A, Grosu A-L, et al. Surviving Elderly Patients with Head-and-Neck Squamous Cell Carcinoma—What Is the Long-Term Quality of Life after Curative Radiotherapy? Cancers. 2021; 13(6):1275. https://doi.org/10.3390/cancers13061275
Chicago/Turabian StyleRühle, Alexander, Erik Haehl, Tobias Kalckreuth, Raluca Stoian, Simon K. B. Spohn, Tanja Sprave, Constantinos Zamboglou, Eleni Gkika, Andreas Knopf, Anca-Ligia Grosu, and et al. 2021. "Surviving Elderly Patients with Head-and-Neck Squamous Cell Carcinoma—What Is the Long-Term Quality of Life after Curative Radiotherapy?" Cancers 13, no. 6: 1275. https://doi.org/10.3390/cancers13061275
APA StyleRühle, A., Haehl, E., Kalckreuth, T., Stoian, R., Spohn, S. K. B., Sprave, T., Zamboglou, C., Gkika, E., Knopf, A., Grosu, A.-L., & Nicolay, N. H. (2021). Surviving Elderly Patients with Head-and-Neck Squamous Cell Carcinoma—What Is the Long-Term Quality of Life after Curative Radiotherapy? Cancers, 13(6), 1275. https://doi.org/10.3390/cancers13061275