
Identification of BXDC2 as a Key Downstream Effector of the Androgen Receptor in Modulating Cisplatin Sensitivity in Bladder Cancer

 ,
, 
Abstract
Simple Summary
Abstract
1. Introduction
2. Results
2.1. Associations between AR and BXDC2 Expression
2.2. Associations between BXDC2 Expression and CDDP Sensitivity
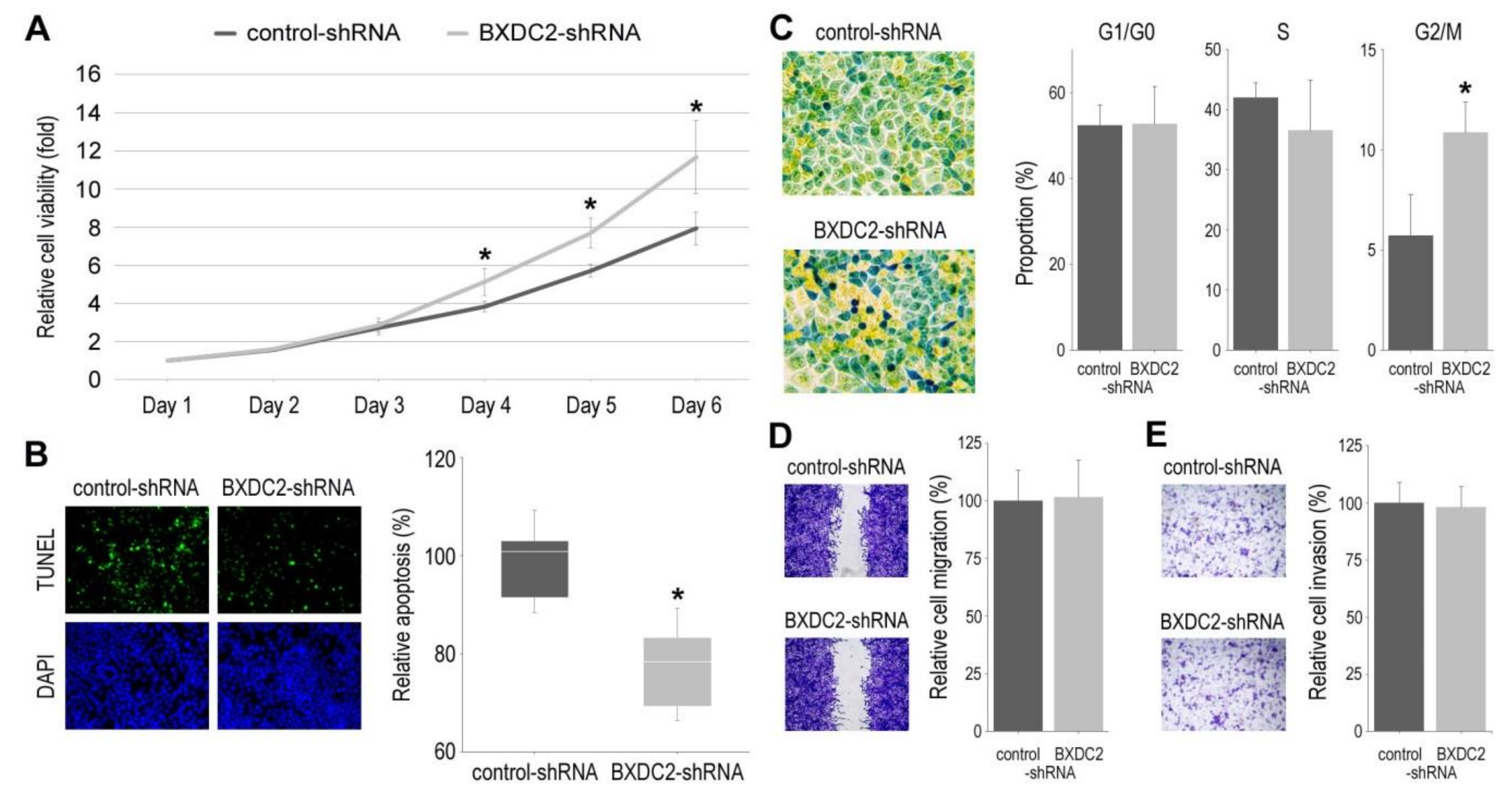
2.3. Role of BXDC2 in Cell Growth
2.4. Involvement of BXDC2 in AR-ERK Signaling
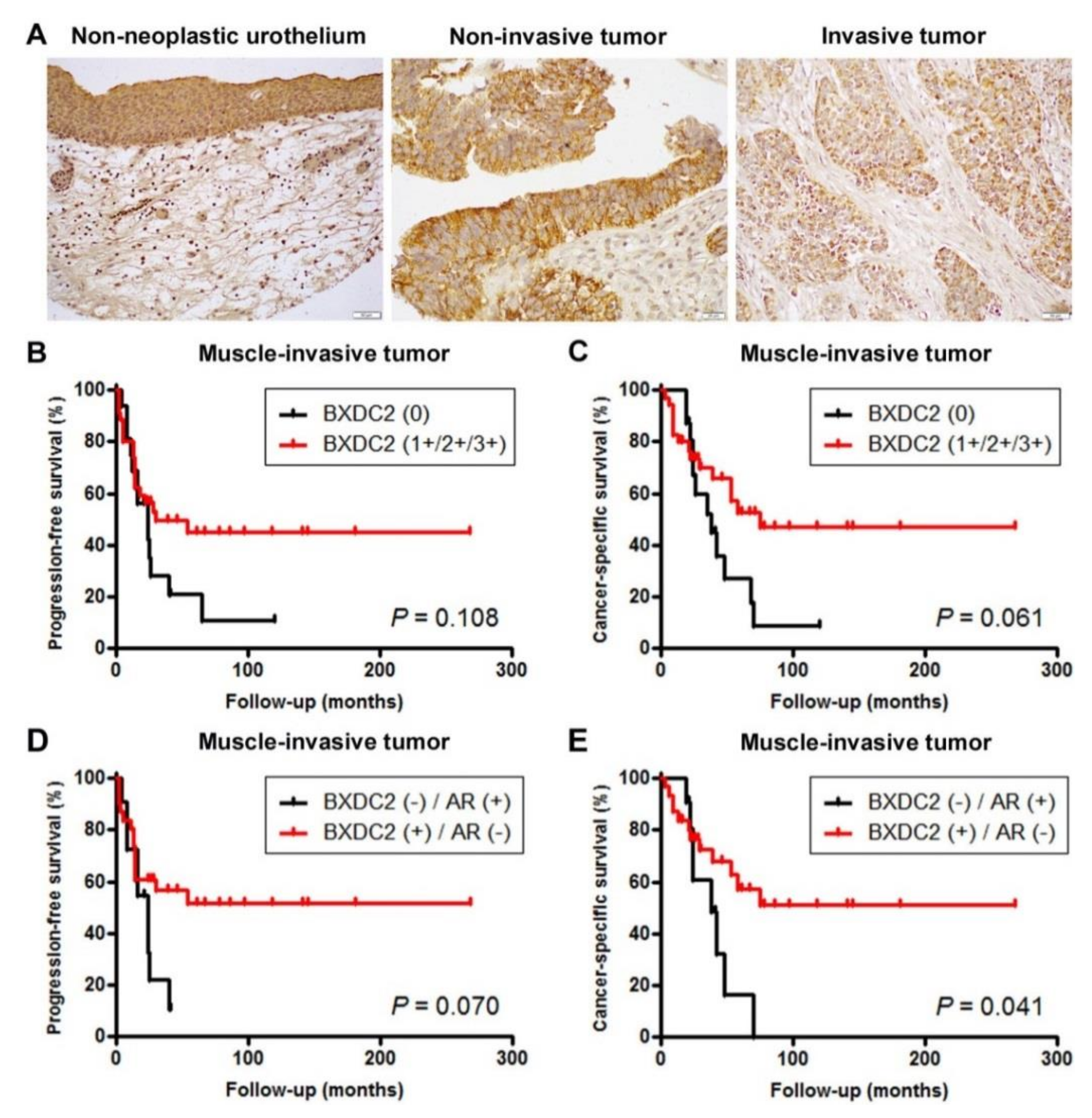
2.5. Expression of BXDC2 in Bladder Cancer Specimens
3. Discussion
4. Materials and Methods
4.1. Cell Lines
4.2. Antibodies and Chemicals
4.3. Western Blotting
4.4. Cell Proliferation
4.5. Apoptosis and Cell Cycle Analysis
4.6. Cell Migration
4.7. Bladder TMA and Immunohistochemistry
4.8. Statistical Analysis
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Torre, L.A.; Bray, F.; Siegel, R.L.; Ferlay, J.; Lortet-Tieulent, J.; Jemal, A. Global cancer statistics, 2012. CA Cancer J. Clin. 2015, 65, 87–108. [Google Scholar] [CrossRef]
- Bray, F.; Ferlay, J.; Soerjomataram, I.; Siegel, R.L.; Torre, L.A.; Jemal, A. Global cancer statistics 2018: GLOBOCAN estimates of incidence and mortality worldwide for 36 cancers in 185 countries. CA Cancer J. Clin. 2018, 68, 397–424. [Google Scholar] [CrossRef]
- SEER Cancer Stat Facts: Bladder Cancer. National Cancer Institute, Bethesda, MD. Available online: http://seer.cancer.gov/statfacts/html/urinb.html (accessed on 6 January 2021).
- Rouprêt, M.; Babjuk, M.; Compérat, E.; Zigeuner, R.; Sylvester, R.J.; Burger, M.; Cowan, N.C.; Gontero, P.; Van Rhijn, B.W.G.; Mostafid, A.H.; et al. European Association of Urology guidelines on upper urinary tract urothelial carcinoma: 2017 update. Eur. Urol. 2018, 73, 111–122. [Google Scholar] [CrossRef]
- Hanna, K.S. Updates and novel treatments in urothelial carcinoma. J. Oncol. Pharm. Pract. 2019, 25, 648–656. [Google Scholar] [CrossRef]
- Goto, T.; Miyamoto, H. Why has the prognosis for bladder cancer not significantly improved after decades of diagnostic and therapeutic advancements? Expert Rev. Anticancer Ther. 2020, 20, 229–231. [Google Scholar] [CrossRef]
- Kashiwagi, E.; Inoue, S.; Mizushima, T.; Chen, J.; Ide, H.; Kawahara, T.; Reis, L.O.; Baras, A.S.; Netto, G.J.; Miyamoto, H. Prostaglandin receptors induce urothelial tumourigenesis as well as bladder cancer progression and cisplatin resistance presumably via modulating PTEN expression. Br. J. Cancer 2018, 118, 213–223. [Google Scholar] [CrossRef]
- Sarin, N.; Engel, F.; Rothweiler, F.; Cinatl, J.; Michaelis, M.; Frötschl, R.; Fröhlich, H.; Kalayda, G.V. Key players of cisplatin resistance: Towards a systems pharmacology approach. Int. J. Mol. Sci. 2018, 19, 767. [Google Scholar] [CrossRef] [PubMed]
- Kashiwagi, E.; Ide, H.; Inoue, S.; Kawahara, T.; Zheng, Y.; Reis, L.O.; Baras, A.S.; Miyamoto, H. Androgen receptor activity modulates responses to cisplatin treatment in bladder cancer. Oncotarget 2016, 7, 49169–49179. [Google Scholar] [CrossRef]
- Li, P.; Chen, J.; Miyamoto, H. Androgen receptor signaling in bladder cancer. Cancers 2017, 9, 20. [Google Scholar] [CrossRef] [PubMed]
- Zheng, Y.; Izumi, K.; Yao, J.L.; Miyamoto, H. Dihydrotestosterone upregulates the expression of epidermal growth factor receptor and ERBB2 in androgen receptor-positive bladder cancer cells. Endocr. Relat. Cancer 2011, 18, 451–464. [Google Scholar] [CrossRef] [PubMed]
- Mizushima, T.; Jiang, G.; Kawahara, T.; Li, P.; Han, B.; Inoue, S.; Ide, H.; Kato, I.; Jalalizadeh, M.; Miyagi, E.; et al. Androgen receptor signaling reduces the efficacy of bacillus Calmette-Guѐrin therapy for bladder cancer via modulating Rab27b-induced exocytosis. Mol. Cancer Ther. 2020, 19, 1930–1942. [Google Scholar] [CrossRef]
- Ide, H.; Inoue, S.; Mizushima, T.; Jiang, G.; Chuang, K.H.; Oya, M.; Miyamoto, H. Androgen receptor signaling reduces radiosensitivity in bladder cancer. Mol. Cancer Ther. 2018, 17, 1566–1574. [Google Scholar] [CrossRef] [PubMed]
- Miyamoto, H.; Yang, Z.; Chen, Y.T.; Ishiguro, H.; Uemura, H.; Kubota, Y.; Nagashima, Y.; Chang, Y.J.; Hu, Y.C.; Tsai, M.Y.; et al. Promotion of bladder cancer development and progression by androgen receptor signals. J. Natl. Cancer Inst. 2007, 99, 558–568. [Google Scholar] [CrossRef]
- Inoue, S.; Mizushima, T.; Ide, H.; Jiang, G.; Goto, T.; Nagata, Y.; Netto, G.J.; Miyamoto, H. ATF2 promotes urothelial cancer outgrowth via cooperation with androgen receptor signaling. Endocr. Connect. 2018, 7, 1397–1408. [Google Scholar] [CrossRef] [PubMed]
- Miyamoto, H.; Yao, J.L.; Chaux, A.; Zheng, Y.; Hsu, I.; Izumi, K.; Chang, C.; Messing, E.M.; Netto, G.J.; Yeh, S. Expression of androgen and oestrogen receptors and its prognostic significance in urothelial neoplasm of the urinary bladder. BJU Int. 2012, 109, 1716–1726. [Google Scholar] [CrossRef] [PubMed]
- Shiota, M.; Takeuchi, A.; Yokomizo, A.; Kashiwagi, E.; Tatsugami, K.; Kuroiwa, K.; Naito, S. Androgen receptor signaling regulates cell growth and vulnerability to doxorubicin in bladder cancer cells. J. Urol. 2012, 188, 276–286. [Google Scholar] [CrossRef]
- Tyagi, A.; Chandrasekaran, B.; Kolluru, V.; Rai, S.; Jordan, A.C.; Houda, A.; Messer, J.; Ankem, M.; Damodaran, C.; Haddad, A. Combination of androgen receptor inhibitor and cisplatin, an effective treatment strategy for urothelial carcinoma of the bladder. Urol. Oncol. 2019, 37, 492–502. [Google Scholar] [CrossRef] [PubMed]
- Eisenhaber, F.; Wechselberger, C.; Kreil, G. The Brix domain protein family—A key to the ribosomal biogenesis pathway? Trends Biochem. Sci. 2001, 26, 345–347. [Google Scholar] [CrossRef]
- Wehner, K.A.; Baserga, S.J. The σ70-like motif: A eukaryotic RNA binding domain unique to a superfamily of proteins required for ribosome biogenesis. Mol. Cell 2002, 9, 329–339. [Google Scholar] [CrossRef]
- Bogengruber, E.; Briza, P.; Doppler, E.; Wimmer, H.; Koller, L.; Fasiolo, F.; Senger, B.; Hegemann, J.H.; Breitenbach, M. Functional analysis in yeast of the Brix protein superfamily involved in the biogenesis of ribosomes. FEMS Yeast Res. 2003, 3, 35–43. [Google Scholar] [CrossRef]
- Ebersberger, I.; Simm, S.; Leisegang, M.S.; Schmitzberger, P.; Mirus, O.; von Haeseler, A.; Bohnsack, M.T.; Schleiff, E. The evolution of the ribosome biogenesis pathway from a yeast perspective. Nucleic Acids Res. 2014, 42, 1509–1523. [Google Scholar] [CrossRef] [PubMed]
- Kovacevic, J.; Palm, D.; Jooss, D.; Bublak, D.; Simm, S.; Schleiff, E. Co-orthologues of ribosome biogenesis factors in A. thaliana are differentially regulated by transcription factors. Plant Cell Rep. 2019, 38, 937–949. [Google Scholar] [CrossRef] [PubMed]
- Yang, X.; Feng, L.; Zhang, Y.; Shi, Y.; Liang, S.; Zhao, T.; Sun, B.; Duan, J.; Sun, Z. Integrative analysis of methylome and transcriptome variation of identified cardiac disease-specific genes in human cardiomyocytes after PM2.5 exposure. Chemosphere 2018, 212, 915–926. [Google Scholar] [CrossRef]
- Zhu, B.; Li, Q.; Liu, R.; Zheng, M.; Wen, J.; Zhao, G. Genome-wide association study of H/L traits in chicken. Animals 2019, 9, 260. [Google Scholar] [CrossRef]
- Jung, H.M.; Choi, S.J.; Kim, J.K. Expression profiles of SV40-immortalization-associated genes upregulated in various human cancers. J. Cell. Biochem. 2009, 106, 703–713. [Google Scholar] [CrossRef]
- Goto, T.; Kashiwagi, E.; Jiang, G.; Nagata, Y.; Teramoto, Y.; Baras, A.S.; Yamashita, S.; Ito, A.; Arai, Y.; Miyamoto, H. Estrogen receptor-β signaling induces cisplatin resistance in bladder cancer. Am. J. Cancer Res. 2020, 10, 2523–2534. [Google Scholar] [PubMed]
- Kawahara, T.; Ide, H.; Kashiwagi, E.; El-Shishtawy, K.A.; Li, Y.; Reis, L.O.; Zheng, Y.; Miyamoto, H. Enzalutamide inhibits androgen receptor-positive bladder cancer cell growth. Urol. Oncol. 2016, 34, 432.e15–432.e23. [Google Scholar] [CrossRef]
- Kawahara, T.; Inoue, S.; Kashiwagi, E.; Chen, J.; Ide, H.; Mizushima, T.; Li, Y.; Zheng, Y.; Miyamoto, H. Enzalutamide as an androgen receptor inhibitor prevents urothelial tumorigenesis. Am. J. Cancer Res. 2017, 7, 2041–2050. [Google Scholar] [CrossRef] [PubMed]
- Li, Y.; Zheng, Y.; Izumi, K.; Ishiguro, H.; Ye, B.; Li, F.; Miyamoto, H. Androgen activates β-catenin signaling in bladder cancer cells. Endocr. Relat. Cancer 2013, 20, 293–304. [Google Scholar] [CrossRef] [PubMed]
- Kawahara, T.; Shareef, H.K.; Aljarah, A.K.; Ide, H.; Li, Y.; Kashiwagi, E.; Netto, G.J.; Zheng, Y.; Miyamoto, H. ELK1 is up-regulated by androgen in bladder cancer cells and promotes tumor progression. Oncotarget 2015, 6, 29860–29876. [Google Scholar] [CrossRef]
- Inoue, S.; Ide, H.; Mizushima, T.; Jiang, G.; Netto, G.J.; Gotoh, M.; Miyamoto, H. Nuclear factor-κB promotes urothelial tumorigenesis and cancer progression via cooperation with androgen receptor signaling. Mol. Cancer Ther. 2018, 17, 1303–1314. [Google Scholar] [CrossRef] [PubMed]
- Li, Y.; Ishiguro, H.; Kawahara, T.; Miyamoto, Y.; Izumi, K.; Miyamoto, H. GATA3 in the urinary bladder: Suppression of neoplastic transformation and down-regulation by androgens. Am. J. Cancer Res. 2014, 4, 461–473. [Google Scholar] [PubMed]
- Ide, H.; Mizushima, T.; Jiang, G.; Goto, T.; Nagata, Y.; Teramoto, Y.; Inoue, S.; Li, Y.; Kashiwagi, E.; Baras, A.S.; et al. FOXO1 as a tumor suppressor inactivated via AR/ERβ signals in urothelial cells. Endocr. Relat. Cancer 2020, 27, 231–244. [Google Scholar] [CrossRef] [PubMed]
- Izumi, K.; Zheng, Y.; Hsu, J.W.; Chang, C.; Miyamoto, H. Androgen receptor signals regulate UDP-glucuronosyltransferases in the urinary bladder: A potential mechanism of androgen-induced bladder carcinogenesis. Mol. Carcinogen. 2013, 52, 94–102. [Google Scholar] [CrossRef] [PubMed]
- Baras, A.S.; Gandhi, N.; Munari, E.; Faraj, S.; Shultz, L.; Marchionni, L.; Schoenberg, M.; Hahn, N.; Hoque, M.O.; Berman, D.; et al. Identification and validation of protein biomarkers of response to neoadjuvant platinum chemotherapy in muscle invasive urothelial carcinoma. PLoS ONE 2015, 10, e0131245. [Google Scholar]







{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Clinicopathology | n | Expression Levels of BXDC2 | p Value | |||
|---|---|---|---|---|---|---|
| Negative | Positive | |||||
| 0 | 1+ | 2+ | 3+ | 0 vs. 1+/2+/3+ | ||
| Tissues | 0.022 | |||||
| Non-neoplastic urothelium | 72 | 7 (10%) | 33 (46%) | 21 (29%) | 11 (15%) | |
| Urothelial neoplasm | 129 | 30 (23%) | 61 (47%) | 29 (22%) | 9 (7%) | |
| Tumor Grade | 0.056 | |||||
| PUNLMP + LG | 50 | 7 (14%) | 29 (58%) | 11 (22%) | 3 (6%) | |
| HG | 79 | 23 (29%) | 32 (41%) | 18 (23%) | 6 (8%) | |
| Pathologic Stage | 0.091 | |||||
| Non-muscle-invasive | 78 | 14 (18%) | 39 (50%) | 18 (23%) | 7 (9%) | |
| Muscle-invasive | 51 | 16 (31%) | 22 (43%) | 11 (22%) | 2 (4%) | |
| Lymph Node Involvement | 0.031 | |||||
| pN0 | 36 | 7 (19%) | 17 (47%) | 11 (31%) | 1 (3%) | |
| pN1-3 | 13 | 7 (54%) | 4 (31%) | 1 (8%) | 1 (8%) | |
| AR expression | 0.007 | |||||
| Negative | 71 | 10 (14%) | 43 (61%) | 13 (18%) | 5 (7%) | |
| Positive | 58 | 20 (34%) | 18 (31%) | 16 (28%) | 4 (7%) | |
| Chemoresponse | n | BXDC2 Expression | p Value | |
|---|---|---|---|---|
| 0 | 1+/2+/3+ | |||
| Responders | 17 | 4 (24%) | 13 (76%) | 0.083 |
| Non-responders | 26 | 13 (50%) | 13 (50%) | |
| Chemoresponse | n | BXDC2(−)/AR(+) | BXDC2 (+)/AR (−) | p Value |
|---|---|---|---|---|
| Responders | 13 | 2 (15%) | 11 (85%) | 0.047 |
| Non-responders | 18 | 9 (50%) | 9 (50%) |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Jiang, G.; Teramoto, Y.; Goto, T.; Mizushima, T.; Inoue, S.; Ide, H.; Nagata, Y.; Kashiwagi, E.; Baras, A.S.; Netto, G.J.; et al. Identification of BXDC2 as a Key Downstream Effector of the Androgen Receptor in Modulating Cisplatin Sensitivity in Bladder Cancer. Cancers 2021, 13, 975. https://doi.org/10.3390/cancers13050975
Jiang G, Teramoto Y, Goto T, Mizushima T, Inoue S, Ide H, Nagata Y, Kashiwagi E, Baras AS, Netto GJ, et al. Identification of BXDC2 as a Key Downstream Effector of the Androgen Receptor in Modulating Cisplatin Sensitivity in Bladder Cancer. Cancers. 2021; 13(5):975. https://doi.org/10.3390/cancers13050975
Chicago/Turabian StyleJiang, Guiyang, Yuki Teramoto, Takuro Goto, Taichi Mizushima, Satoshi Inoue, Hiroki Ide, Yujiro Nagata, Eiji Kashiwagi, Alexander S. Baras, George J. Netto, and et al. 2021. "Identification of BXDC2 as a Key Downstream Effector of the Androgen Receptor in Modulating Cisplatin Sensitivity in Bladder Cancer" Cancers 13, no. 5: 975. https://doi.org/10.3390/cancers13050975
APA StyleJiang, G., Teramoto, Y., Goto, T., Mizushima, T., Inoue, S., Ide, H., Nagata, Y., Kashiwagi, E., Baras, A. S., Netto, G. J., Yang, Z., & Miyamoto, H. (2021). Identification of BXDC2 as a Key Downstream Effector of the Androgen Receptor in Modulating Cisplatin Sensitivity in Bladder Cancer. Cancers, 13(5), 975. https://doi.org/10.3390/cancers13050975