
Surgical Techniques and Outcomes of Colorectal Anastomosis after Left Hemicolectomy with Low Anterior Rectal Resection for Advanced Ovarian Cancer


Abstract
:Simple Summary
Abstract
1. Introduction
2. Materials and Methods
2.1. Patients
2.2. Surgery and Chemotherapy
2.3. Surgical Techniques for Colorectal Anastomosis after Low Anterior Rectal Resection and Right-Sided Colectomy
2.4. Surgical Techniques for Tension-Free Colorectal Anastomosis after Left Hemicolectomy with Low Anterior Rectal Resection
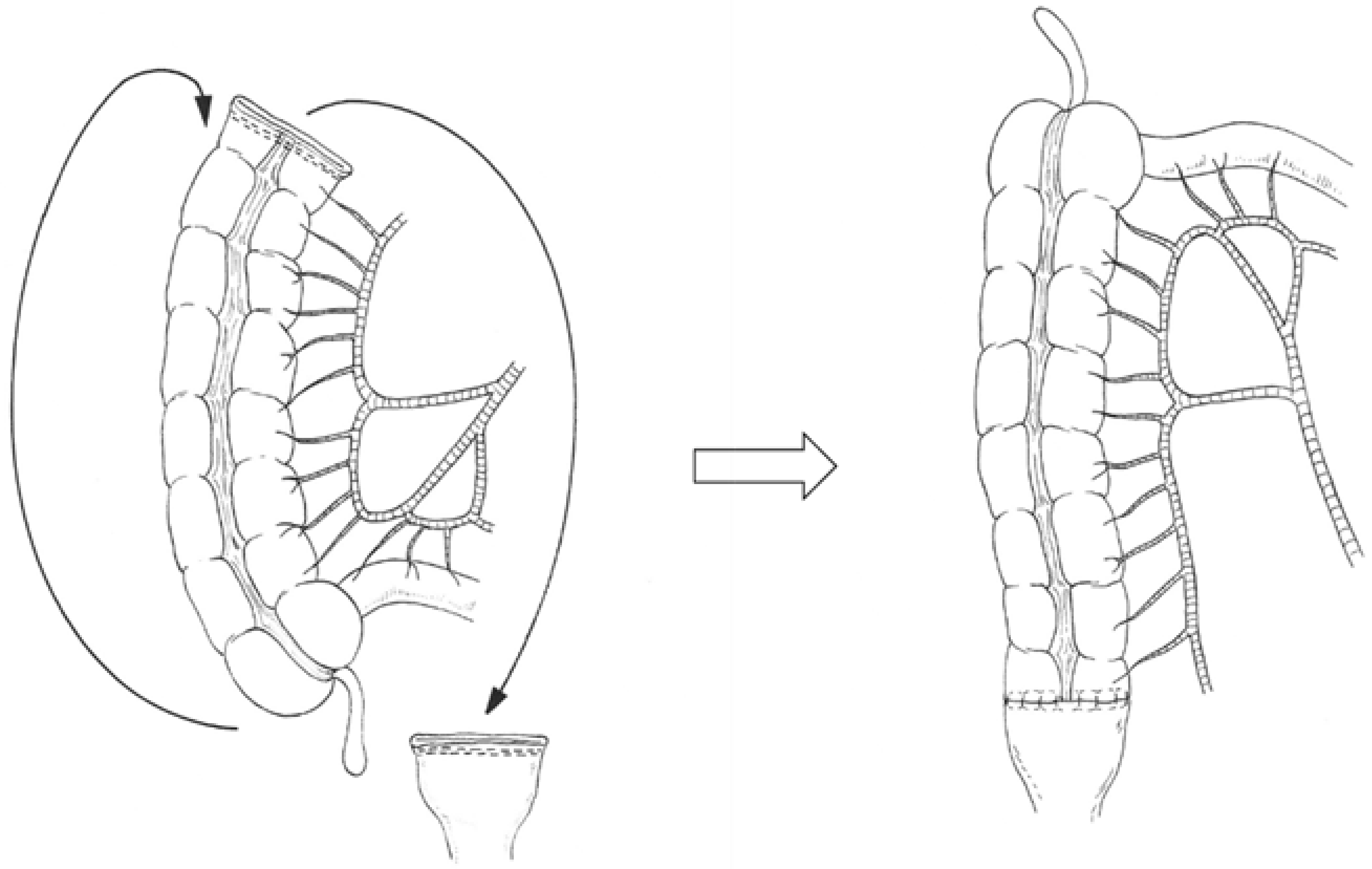
2.4.1. Right Colonic Transposition
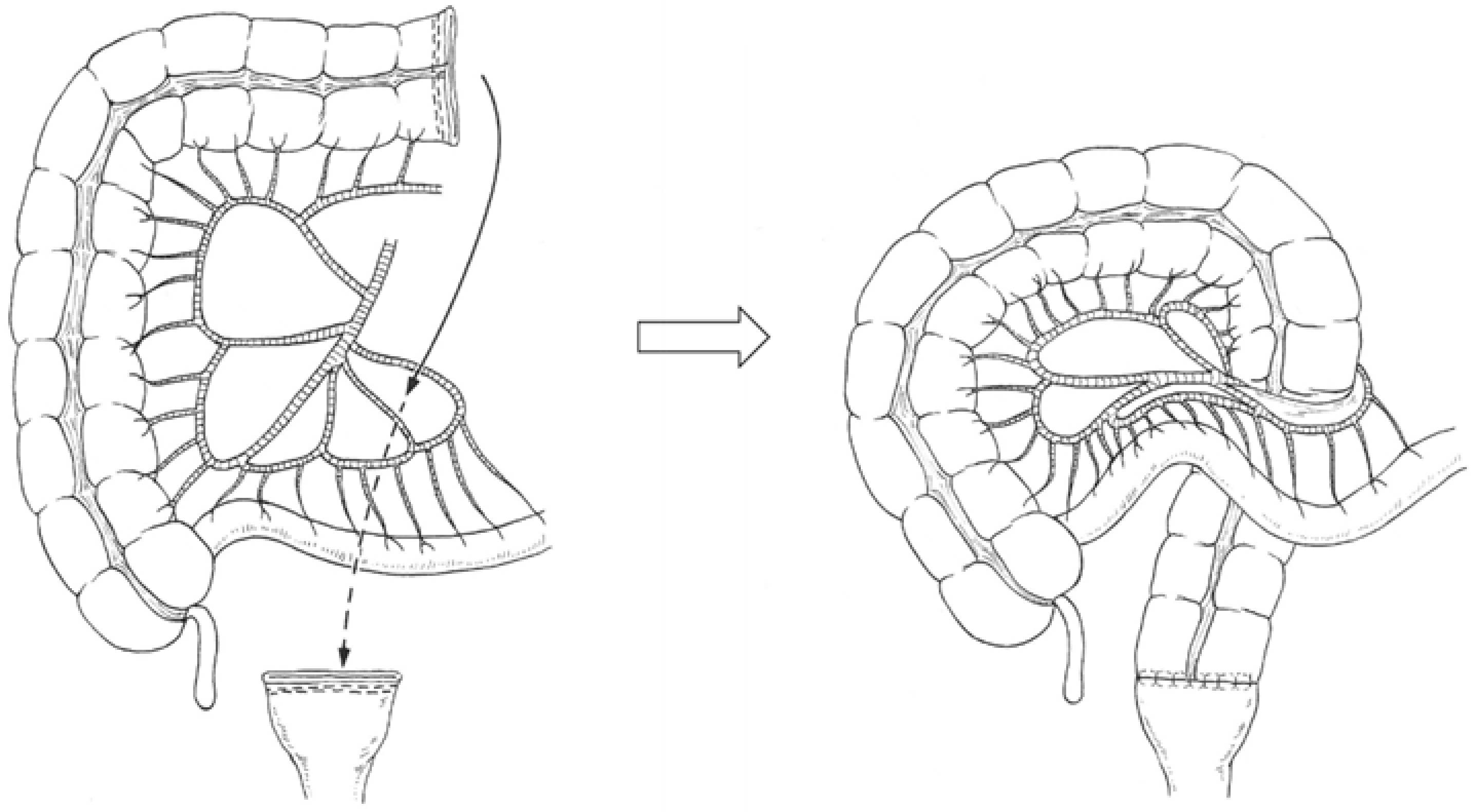
2.4.2. Retro-Ileal Anastomosis through an Ileal Mesenteric Defect
2.4.3. Additional Division of the Colic Artery
2.5. Definition and Management of Anastomotic Leakage
2.6. Surgical Outcomes
2.7. Statistical Analysis
3. Results
3.1. Patient Characteristics
3.2. Surgical Outcomes
3.3. Rate and Techniques of Colorectal Anastomosis after Left Hemicolectomy with Low Anterior Rectal Resection
3.4. Clinical Factors for Rectal Anastomotic Leakage
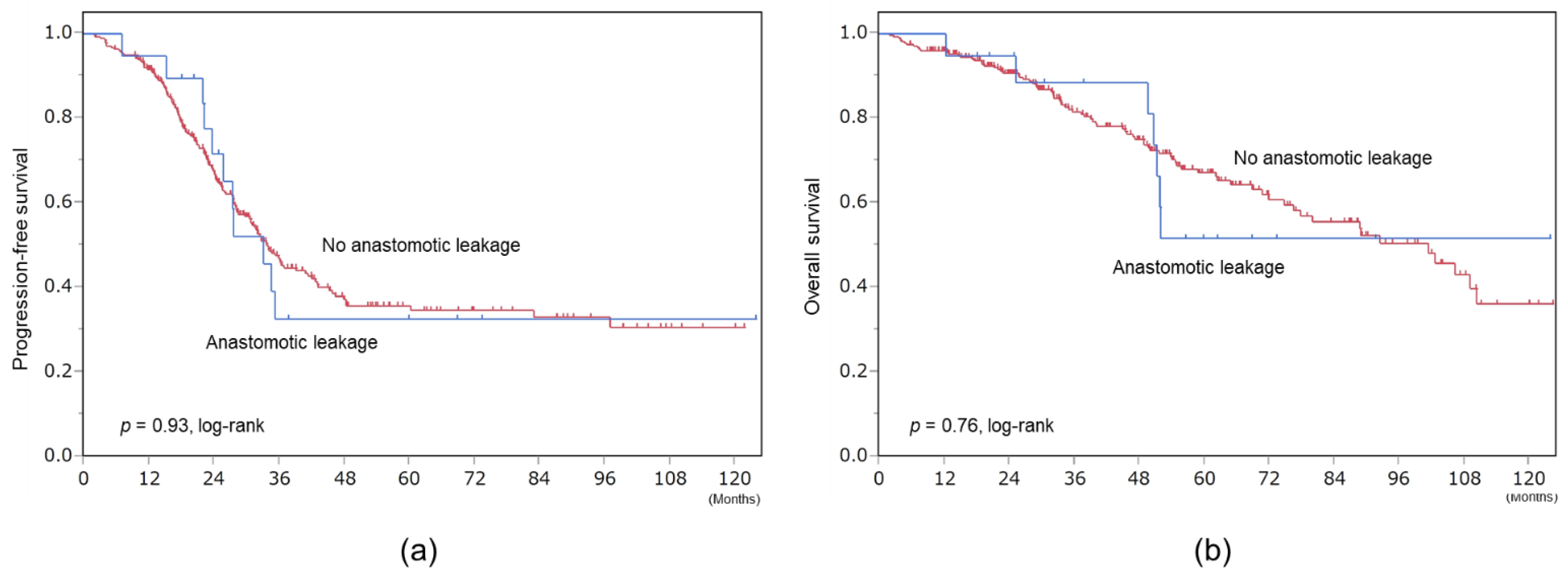
3.5. Survival
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Hoffman, M.S.; Griffin, D.; Tebes, S.; Cardosi, R.J.; Martino, M.A.; Fiorica, J.V.; Lockhart, J.L.; Grendys, E.C. Sites of bowel resected to achieve optimal ovarian cancer cytoreduction: Implications regarding surgical management. Am. J. Obstet. Gynecol. 2005, 193, 582–586, discussion 586–588. [Google Scholar] [CrossRef]
- Hoffman, M.S.; Zervose, E. Colon resection for ovarian cancer: Intraoperative decisions. Gynecol. Oncol. 2008, 111, S56–S65. [Google Scholar] [CrossRef]
- Kalogera, E.; Dowdy, S.C.; Mariani, A.; Weaver, A.L.; Aletti, G.; Bakkum-Gamez, J.N.; Cliby, W.A. Multiple large bowel resections: Potential risk factor for anastomotic leak. Gynecol. Oncol. 2013, 130, 213–218. [Google Scholar] [CrossRef] [Green Version]
- Grimm, C.; Harter, P.; Alesina, P.F.; Prader, S.; Schneider, S.; Ataseven, B.; Meier, B.; Brunkhorst, V.; Hinrichs, J.; Kurzeder, C.; et al. The impact of type and number of bowel resections on anastomotic leakage risk in advanced ovarian cancer surgery. Gynecol. Oncol. 2017, 146, 498–503. [Google Scholar] [CrossRef] [PubMed]
- Tseng, J.H.; Suidan, R.S.; Zivanovic, O.; Gardner, G.J.; Sonoda, Y.; Levine, D.A.; Abu-Rustum, N.R.; Tew, W.P.; Chi, D.S.; Roche, K.L. Diverting ileostomy during primary debulking surgery for ovarian cancer: Associated factors and postoperative outcomes. Gynecol. Oncol. 2016, 142, 217–224. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- O’Leary, D.P.; Fide, C.J.; Foy, C.; Lucarotti, E.M. Quality of life after low anterior resection with total mesorectal excision and temporary loop ileostomy for rectal carcinoma. BJS 2002, 88, 1216–1220. [Google Scholar] [CrossRef] [PubMed]
- Kim, H.S.; Kim, E.N.; Jeong, S.Y.; Chung, H.H.; Kim, Y.B.; Kim, J.W.; Park, K.J.; Park, N.H.; Song, Y.S.; Park, J.-G.; et al. Comparison of the efficacy of low anterior resection with primary anastomosis and Hartmann’s procedure in advanced primary or recurrent epithelial ovarian cancer. Eur. J. Obstet. Gynecol. Reprod. Biol. 2011, 156, 194–198. [Google Scholar] [CrossRef] [PubMed]
- Shariff, U.S.; Kullar, N.; Dorudi, S. Right Colonic Transposition Technique: When the Left Colon Is Unavailable for Achieving a Pelvic Anastomosis. Dis. Colon Rectum 2011, 54, 360–362. [Google Scholar] [CrossRef]
- Manceau, G.; Karoui, M.; Breton, S.; Blanchet, A.-S.; Rousseau, G.; Savier, E.; Siksik, J.-M.; Vaillant, J.-C.; Hannoun, L. Right Colon to Rectal Anastomosis (Deloyers Procedure) as a Salvage Technique for Low Colorectal or Coloanal Anastomosis: Postoperative and Long-Term Outcomes. Dis. Colon Rectum. 2012, 55, 363–368. [Google Scholar] [CrossRef]
- Deloyers, L. Suspension of the right colon permits without exception preservation of the anal sphincter after extensive colectomy of the transverse and left colon (including rectum). Technic-indications-immediate and late results. Lyon Chir. 1964, 60, 404–413. [Google Scholar] [PubMed]
- Rombeau, J.L.; Collins, J.P.; Turnbull, R.B., Jr. Left-sided colectomy with retroileal colorectal anastomosis. Arch Surg. 1978, 113, 1004–1005. [Google Scholar] [CrossRef] [PubMed]
- Le, T.H.; Gathright, J.B. Reconstitution of Intestinal Continuity after Extended Left Colectomy. Dis Colon Rectum. 1993, 36, 197–198. [Google Scholar] [CrossRef]
- Sakamoto, Y.; Tokunaga, R.; Miyamoto, Y.; Ohuchi, M.; Nakamura, K.; Kosumi, K.; Harada, K.; Shigaki, H.; Kurashige, J.; Iwatsuki, M.; et al. Retroileal colorectal anastomosis after extended left colectomy: Application for laparoscopic surgery. Surg. Today 2016, 46, 1476–1478. [Google Scholar] [CrossRef] [PubMed]
- Mike, M.; Kano, M. Reappraisal of the vascular anatomy of the colon and consequences for the definition of surgical resection. Dig Surg. 2013, 30, 383–392. [Google Scholar] [CrossRef]
- Tate, S.; Kato, K.; Nishikimi, K.; Matsuoka, A.; Shozu, M. Survival and safety associated with aggressive surgery for stage III/IV epithelial ovarian cancer: A single institution observation study. Gynecol. Oncol. 2017, 147, 73–80. [Google Scholar] [CrossRef]
- Nishikimi, K.; Tate, S.; Kato, K.; Matsuoka, A.; Shozu, M. Well-trained gynecologic oncologists can perform bowel resection and upper abdominal surgery safely. J. Gynecol. Oncol. 2020, 31, e3. [Google Scholar] [CrossRef]
- Tate, S.; Nishikimi, K.; Kato, K.; Matsuoka, A.; Kambe, M.; Kiyokawa, T.; Shozu, M. Microscopic diseases remain in initial disseminated sites after neoadjuvant chemotherapy for stage III/IV ovarian, tubal, and primary peritoneal cancer. J. Gynecol. Oncol. 2020, 31, e34. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Bristow, R.E.; Montz, F.J.; Lagasse, L.D.; Leuchter, R.S.; Karlan, B.Y. Survival Impact of Surgical Cytoreduction in Stage IV Epithelial Ovarian Cancer. Gynecol. Oncol. 1999, 72, 278–287. [Google Scholar] [CrossRef]
- Akahira, J.I.; Yoshikawa, H.; Shimizu, Y.; Tsunematsu, R.; Hirakawa, T.; Kuramoto, H.; Shiromizu, K.; Kuzuya, K.; Kamura, T.; Kikuchi, Y.; et al. Prognostic factors of stage IV epithelial ovarian cancer: A multicenter retrospective study. Gynecol. Oncol. 2001, 81, 398–403. [Google Scholar] [CrossRef]
- Winter, W.E., 3rd; Maxwell, G.L.; Tian, C.; Sundborg, M.J.; Rose, G.S.; Rose, P.G.; Rubin, S.C.; Muggia, F.; McGuire, W.P.; Gynecologic Oncology Group. Tumor residual after surgical cytoreduction in prediction of clinical outcome in stage IV epithelial ovarian cancer: A Gynecologic Oncology Group Study. J. Clin. Oncol. Off. J. Am. Soc. Clin. Oncol. 2008, 26, 83–89. [Google Scholar] [CrossRef]
- Ataseven, B.; Grimm, C.; Harter, P.; Heitz, F.; Traut, A.; Prader, S.; du Bois, A. Prognostic impact of debulking surgery and residual tumor in patients with epithelial ovarian cancer FIGO stage IV. Gynecol. Oncol. 2016, 140, 215–220. [Google Scholar] [CrossRef]
- Aletti, G.; Santillan, A.; Eisenhauer, E.L.; Hu, J.; Podratz, K.C.; Bristow, R.E.; Chi, D.S.; Cliby, W.A. A new frontier for quality of care in gynecologic oncology surgery: Multi-institutional assessment of short-term outcomes for ovarian cancer using a risk-adjusted model. Gynecol. Oncol. 2007, 107, 99–106. [Google Scholar] [CrossRef]
- Dindo, D.; Demartines, N.; Clavien, P.A. Classification of surgical complications: A new proposal with evaluation in a cohort of 6336 patients and results of a survey. Ann. Surg. 2004, 240, 205–213. [Google Scholar] [CrossRef] [PubMed]
- Sugarbaker, P.H.; Jablonski, K.A. Prognostic Features of 51 Colorectal and 130 Appendiceal Cancer Patients with Peritoneal Carcinomatosis Treated by Cytoreductive Surgery and Intraperitoneal Chemotherapy. Ann. Surg. 1995, 221, 124–132. [Google Scholar] [CrossRef] [PubMed]
- Jacquet, P.; Sugarbaker, P.H. Clinical research methodologies in diagnosis and staging of patients with peritoneal carcinomatosis. In Peritoneal Carcinomatosis: Principles of Management; Sugarbaker, P.H., Ed.; Springer US: Boston, MA, USA, 1996; pp. 359–374. [Google Scholar]
- Saunders, B.P.; Phillips, R.K.S.; Williams, C.B. Intraoperative measurement of colonic anatomy and attachments with relevance to colonoscopy. BJS 2005, 82, 1491–1493. [Google Scholar] [CrossRef] [PubMed]
- Gillette-Cloven, N.; Burger, A.R.; Monk, B.J.; McMeekin, D.; Vasilev, S.; DiSaia, P.J.; Kohler, M.F. Bowel resection at the time of primary cytoreduction for epithelial ovarian cancer. J. Am. Coll. Surg. 2001, 193, 626–632. [Google Scholar] [CrossRef]
- Tamussino, K.F.; Lim, P.C.; Webb, M.J.; Lee, R.A.; Lesnick, T.G. Gastrointestinal Surgery in Patients with Ovarian Cancer. Gynecol. Oncol. 2001, 80, 79–84. [Google Scholar] [CrossRef] [PubMed]
- Mourton, S.; Temple, L.; Aburustum, N.; Gemignani, M.; Sonoda, Y.; Bochner, B.; Barakat, R.; Chi, D. Morbidity of rectosigmoid resection and primary anastomosis in patients undergoing primary cytoreductive surgery for advanced epithelial ovarian cancer. Gynecol. Oncol. 2005, 99, 608–614. [Google Scholar] [CrossRef]
- Estes, J.M.; Leath, C.A.; Williams, S.; Modiano, M.R.; Sawyer, M.; Cohn, D.; Straughn, J.M.; Barnes, M.N.; Alvarez, R.D. Efficacy and toxicity of the novel chemotherapeutic agent KW-2170 in recurrent epithelial ovarian cancer. Gynecol. Oncol. 2006, 102, 338–342. [Google Scholar] [CrossRef] [PubMed]
- Silver, D.F.; Zgheib, N.B. Extended left colon resections as part of complete cytoreduction for ovarian cancer: Tips and considerations. Gynecol. Oncol. 2009, 114, 427–430. [Google Scholar] [CrossRef]
- Fournier, M.; Huchon, C.; Ngo, C.; Bensaid, C.; Bats, A.; Combe, P.; Belda, M.L.F.; Fournier, L.; Berger, A.; Lecuru, F.; et al. Morbidity of rectosigmoid resection in cytoreductive surgery for ovarian cancer. Risk factor analysis. Eur. J. Surg. Oncol. (EJSO) 2018, 44, 750–753. [Google Scholar] [CrossRef] [PubMed]
- Kang, S.; Jong, Y.H.; Hwang, J.H.; Lim, M.C.; Seo, S.-S.; Yoo, C.-W.; Park, S.-Y. Is Neo-adjuvant Chemotherapy a “Waiver” of Extensive Upper Abdominal Surgery in Advanced Epithelial Ovarian Cancer? Ann. Surg. Oncol. 2011, 18, 3824–3827. [Google Scholar] [CrossRef] [PubMed]
- Mueller, J.; Zhou, Q.C.; Iasonos, A.; O’Cearbhaill, R.E.; Alvi, F.A.; El Haraki, A.; Eriksson, A.G.Z.; Gardner, G.J.; Sonoda, Y.; Levine, D.A.; et al. Neoadjuvant chemotherapy and primary debulking surgery utilization for advanced-stage ovarian cancer at a comprehensive cancer center. Gynecol. Oncol. 2016, 140, 436–442. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Vergote, I.; Tropé, C.G.; Amant, F.; Kristensen, G.B.; Ehlen, T.; Johnson, N.; Verheijen, R.H.; Van Der Burg, M.E.; Lacave, A.J.; Panici, P.B.; et al. Neoadjuvant Chemotherapy or Primary Surgery in Stage IIIC or IV Ovarian Cancer. N. Engl. J. Med. 2010, 363, 943–953. [Google Scholar] [CrossRef] [Green Version]
- Kehoe, S.; Hook, J.; Nankivell, M.; Jayson, G.; Kitchener, H.; Lopes, A.D.B.; Luesley, D.; Perren, T.; Bannoo, S.; Mascarenhas, M.; et al. Primary chemotherapy versus primary surgery for newly diagnosed advanced ovarian cancer (CHORUS): An open-label, randomised, controlled, non-inferiority trial. Lancet 2015, 386, 249–257. [Google Scholar] [CrossRef]

{kind=link}
{kind=link}
{kind=link}
| Variables | All | Left Hemicolectomy with Low Anterior Rectal Resection | Right-Sided Colectomy with Low Anterior Rectal Resection | Transverse Colectomy with Low Anterior Rectal Resection or Total Colectomy | Low Anterior Rectal Resection Only |
|---|---|---|---|---|---|
| n = 295 | n = 40 | n = 105 | n = 5 | n = 145 | |
| Age, median (IQR) | 63 (51–71) | 65 (51–71) | 66 (54–72) | 62 (61–70) | 59 (50–69) |
| Primary site | |||||
| Ovary | 175 (59.3%) | 23 (57.5%) | 51 (48.6%) | 5 (100%) | 96 (66.2%) |
| Fallopian tube | 102 (34.6%) | 15 (37.5%) | 46 (43.8%) | 0 (0%) | 41 (28.3%) |
| Peritoneum | 18 (6.1%) | 2 (5.0%) | 8 (7.6%) | 0 (0%) | 8 (5.5%) |
| Performance status | |||||
| 0 | 69 (23.3%) | 8 (20.0%) | 20 (19.1%) | 0 (0%) | 41 (28.3%) |
| 1 | 135 (45.8%) | 24 (60.0%) | 43 (41.0%) | 2 (40.0%) | 66 (45.5%) |
| 2 | 66 (22.4%) | 8 (20.0%) | 31(30.0%) | 2 (40.0%) | 25(17.2%) |
| 3 | 25(8.5%) | 0(0%) | 11(10.5%) | 1 (20.0%) | 13(9.0%) |
| FIGO 2014 stage | |||||
| IVA | 28 (9.5%) | 0 (0%) | 1 (1.0%) | 0 (0%) | 27 (18.6%) |
| IVB | 15 (5.1%) | 0 (0%) | 1 (1.0%) | 0 (0%) | 14 (9.7%) |
| IVC | 131 (44.4%) | 18 (45.0%) | 55 (52.4%) | 4 (80.0%) | 54 (37.2%) |
| IIIA | 24 (8.1%) | 3 (7.5%) | 11 (10.5%) | 0 (0%) | 10(6.9%) |
| IIIB | 97 (32.9%) | 19 (47.5%) | 37 (35.2%) | 1 (20.0%) | 40 (27.6%) |
| Histology | |||||
| High-grade serous | 223 (75.6%) | 31 (77.5%) | 90 (85.7%) | 3 (60.0%) | 99 (68.3%) |
| Non high-grade serous | 72 (24.4%) | 9 (22.5%) | 12 (14.3%) | 2 (40.0%) | 45 (31.7%) |
| Clear | 25 (8.5%) | 5 (12.5%) | 5 (4.8%) | 0 (0%) | 15 (10.3%) |
| Endometrioid | 18 (6.1%) | 1 (2.5%) | 4 (3.8%) | 0 (0%) | 13 (8.9%) |
| Mucinous | 1 (0.3%) | 1 (2.5%) | 0 (0%) | 0 (0%) | 0 (0%) |
| Others | 28 (9.5%) | 2 (5.0%) | 6 (5.7%) | 2 (40.0%) | 18 (12.4%) |
| Timing of cytoreductive surgery | |||||
| Primary | 117 (39.7%) | 13 (32.5%) | 22 (21.0%) | 1 (20.0%) | 81 (55.9%) |
| Interval | 178 (60.3%) | 27 (67.5%) | 83 (79.1%) | 4 (80.0%) | 64 (44.1%) |
| Peritoneal cancer index, median (IQR) | 16 (8–21) | 23 (18–26) | 20 (16–23) | 20 (10–23) | 9 (5–16) |
| Variables | All | Left Hemicolectomy with Low Anterior Rectal Resection | Right-Sided Colectomy with Low Anterior Rectal Resection | Transverse Colectomy with Low Anterior Rectal Resection or Total Colectomy | Low Anterior Rectal Resection Only |
|---|---|---|---|---|---|
| n = 295 | n = 40 | n = 105 | n = 5 | n = 145 | |
| Permanent colostomy | 9 (3.1%) | 1 (0.3%) | 2 (2.0%) | 0(0%) | 6 (4.1%) |
| Protective ileostomy | 4 (1.4%) | 0 (0%) | 1 (0.1%) | 1 (20.0%) | 2 (1.4%) |
| Rectal anastomotic leakage | 19 (6.4%) | 3 (7.5%) | 9 (8.6%) | 0 (0%) | 7 (4.8%) |
| Conservative treatment with percutaneous drainage | 15 (5.1%) | 3 (7.5%) | 9 (8.6%) | 0 (0%) | 3 (2.1%) |
| Requiring re-operation | 4 (1.4%) | 0 (0%) | 0 (0%) | 0 (0%) | 4 (2.8%) |
| Surgical complexity score, median (IQR) | 13 [10,11,12,13,14,15] | 15 (13–16) | 15 (14–16) | 11 (9–16) | 11 (7–13) |
| Residual tumor | |||||
| 0 | 270 (91.5%) | 33 (82.5%) | 97 (92.4%) | 3 (60.0%) | 137 (94.5%) |
| 0.1–1.0 cm | 21 (7.1%) | 5 (12.5%) | 7 (6.7%) | 2 (40.0%) | 7 (4.8%) |
| >1.0 cm | 4 (1.4%) | 2 (5.0%) | 1 (1.0%) | 0 (0%) | 1 (0.7%) |
| Postoperative complications | |||||
| Clavien-Dindo IIIa | 61 (20.7%) | 15 (37.5%) | 30 (28.6%) | 0 (0%) | 16 (11.0%) |
| Clavien-Dindo IIIb-V | 11 (3.7%) | 1 (2.5%) | 1 (1.0%) | 0 (0%) | 9 (6.2%) |
| Time to initiation of adjuvant chemotherapy, median, day | 27 [21,22,23,24,25,26,27,28,29,30,31,32,33,34] | 27 (21–38) | 27 (22–35) | 29 (28–37) | 26 (20–32) |
| Length of hospitalization, median, day | 29 (23–40) | 28 (23–47) | 29 (23–38) | 29 (22–40) | 49 (21–51) |
| Variables | Rectal Anastomotic Leakage (+) | Rectal Anastomotic Leakage (−) | p Value |
|---|---|---|---|
| n = 19 | n = 276 | ||
| Age, median (IQR) | 62 (51–70) | 63 (51–71) | 0.86 |
| Performance status | 0.02 | ||
| 0–1 | 8 (42.1%) | 196 (71.0%) | |
| 2–3 | 11 (57.9%) | 80 (29.0%) | |
| FIGO 2014 stage | 0.92 | ||
| III | 11 (57.9%) | 163 (57.9%) | |
| IV | 8 (42.1%) | 113 (42.1%) | |
| Serum albumin before cytoreductive surgery (g/dL), median (IQR) | 3.9 (3.7–4.1) | 3.9 (3.5–4.2) | 0.98 |
| Timing of cytoreductive surgery | 0.03 | ||
| Primary | 3 (15.8%) | 114 (41.3%) | |
| Interval | 16 (84.2%) | 162 (58.7%) | |
| Peritoneal cancer index, median (IQR) | 16 (8–21) | 18 (16–25) | 0.06 |
| Surgical complexity score, median (IQR) | 13 (13–15) | 13 (10–15) | 0.16 |
| Residual tumor | 0.60 | ||
| Microscopic | 18 (94.7%) | 252 (91.3%) | |
| Macroscopic | 1 (5.3%) | 24 (8.7%) | |
| Type of large bowel resection | 0.61 | ||
| Left hemicolectomy with low anterior rectal resection | 3 (15.8%) | 37 (13.4%) | |
| Right-sided colectomy with low anterior rectal resection | 9 (47.4%) | 96 (34.8%) | |
| Transverse colectomy with low anterior rectal resection or total colectomy | 0 (0%) | 5 (1.8%) | |
| Low anterior rectal resection only | 7 (36.8%) | 138 (50.0%) | |
| Length that was continuously resected from the rectum to the colon (cm), median (IQR) | 21 (16–30) | 22 (17–29) | 0.79 |
| Number of intestinal anastomosis | 0.19 | ||
| 0 or 1 | 7 | 159 | |
| 2 or 3 | 11 | 117 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Nishikimi, K.; Tate, S.; Matsuoka, A.; Otsuka, S.; Shozu, M. Surgical Techniques and Outcomes of Colorectal Anastomosis after Left Hemicolectomy with Low Anterior Rectal Resection for Advanced Ovarian Cancer. Cancers 2021, 13, 4248. https://doi.org/10.3390/cancers13164248
Nishikimi K, Tate S, Matsuoka A, Otsuka S, Shozu M. Surgical Techniques and Outcomes of Colorectal Anastomosis after Left Hemicolectomy with Low Anterior Rectal Resection for Advanced Ovarian Cancer. Cancers. 2021; 13(16):4248. https://doi.org/10.3390/cancers13164248
Chicago/Turabian StyleNishikimi, Kyoko, Shinichi Tate, Ayumu Matsuoka, Satoyo Otsuka, and Makio Shozu. 2021. "Surgical Techniques and Outcomes of Colorectal Anastomosis after Left Hemicolectomy with Low Anterior Rectal Resection for Advanced Ovarian Cancer" Cancers 13, no. 16: 4248. https://doi.org/10.3390/cancers13164248
APA StyleNishikimi, K., Tate, S., Matsuoka, A., Otsuka, S., & Shozu, M. (2021). Surgical Techniques and Outcomes of Colorectal Anastomosis after Left Hemicolectomy with Low Anterior Rectal Resection for Advanced Ovarian Cancer. Cancers, 13(16), 4248. https://doi.org/10.3390/cancers13164248