
How about Levetiracetam in Glioblastoma? An Institutional Experience and Meta-Analysis

 , ,
, , 
 and
and
Abstract
:Simple Summary
Abstract
1. Introduction
2. Materials and Methods
2.1. Institutional Cohort
2.1.1. Patient Population
2.1.2. GBM Management
2.1.3. Epilepsy Treatment
2.1.4. Data Management
2.1.5. Study Endpoints and Statistical Analysis
2.2. Literature Review and Meta-Analysis
3. Results
3.1. Patient Population
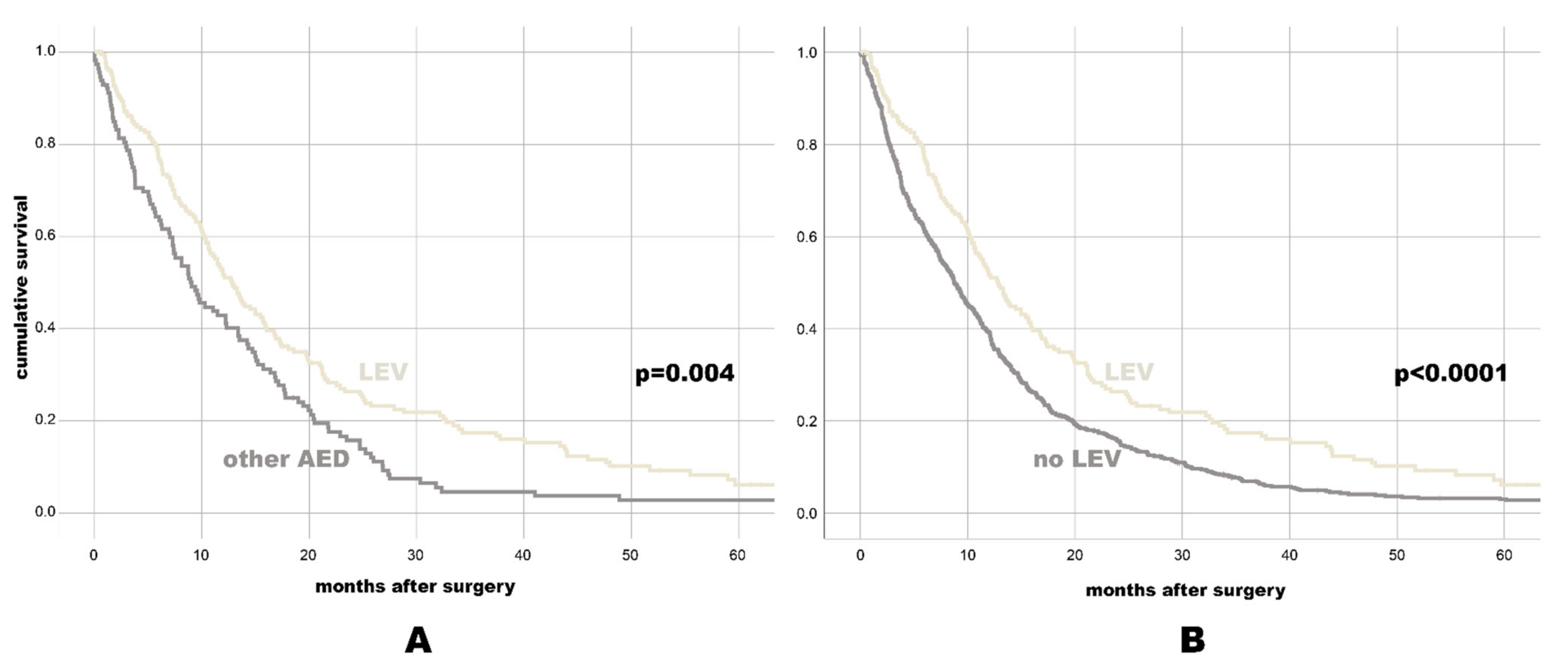
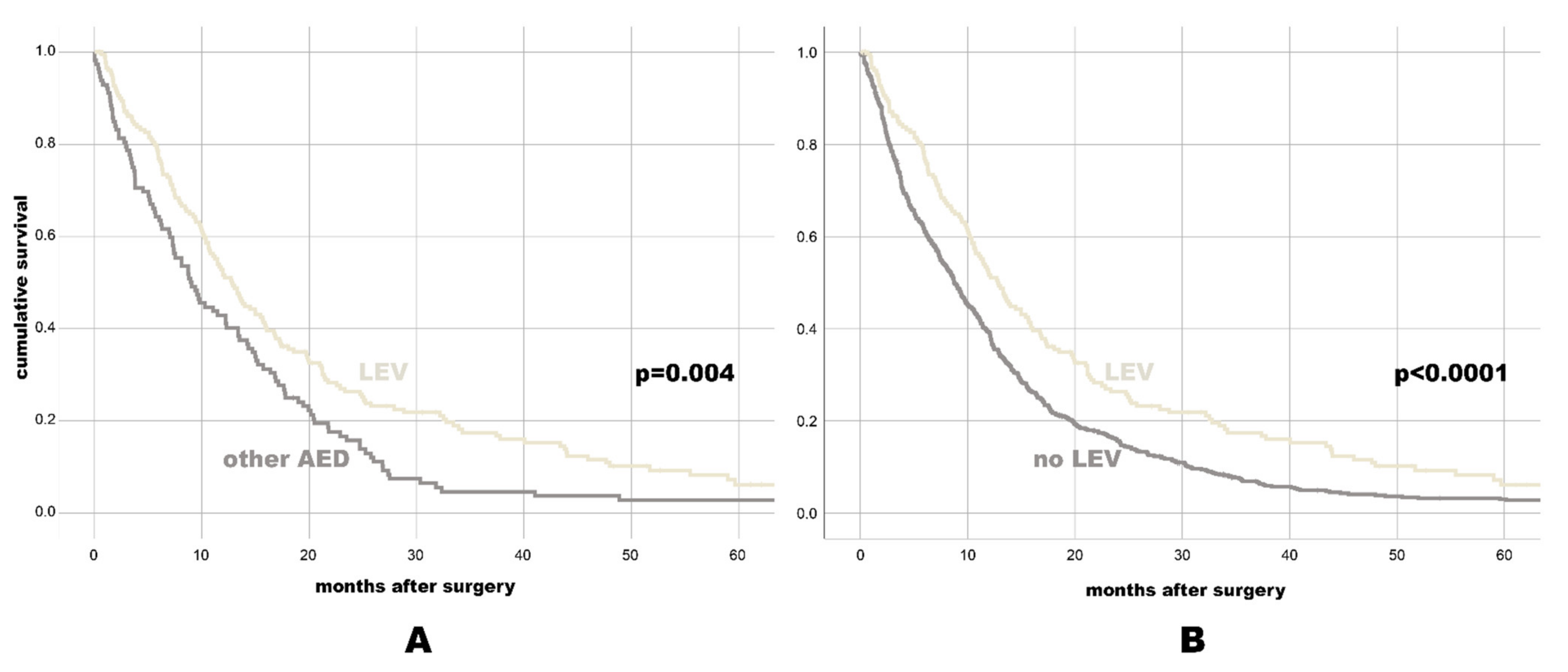
3.2. AED and OS
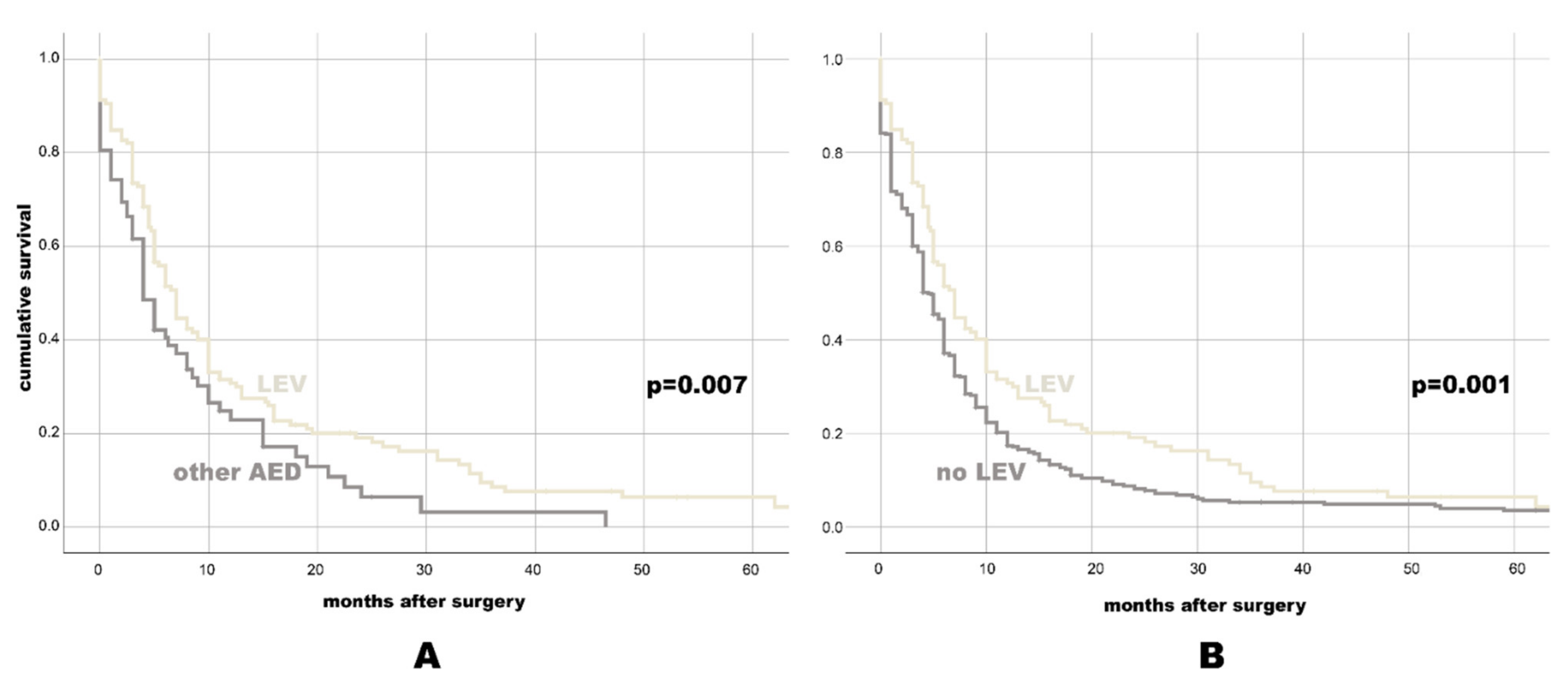
3.3. AED and PFS
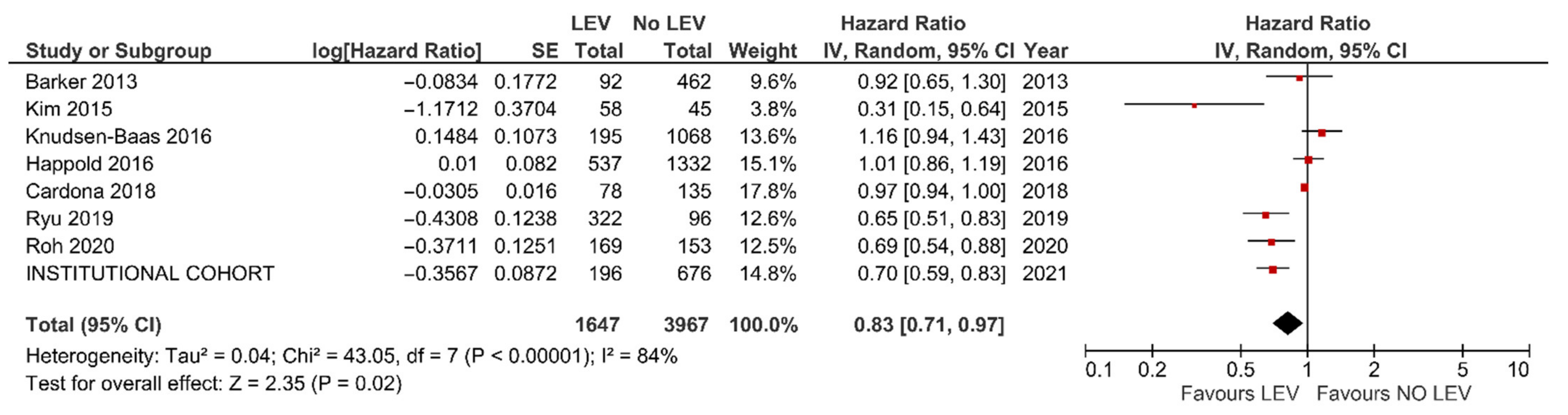
3.4. Meta-Analysis
4. Discussion
4.1. AED and GBM Prognosis: Direct or Indirect Antitumor Effect, Coincidence or Myth?
4.2. LEV: A Light at the End of the Tunnel?
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Maschio, M. Brain tumor-related epilepsy. Curr. Neuropharmacol. 2012, 10, 124–133. [Google Scholar] [CrossRef]
- Rigamonti, A.; Imbesi, F.; Silvani, A.; Gaviani, P.; Agostoni, E.; Porcu, L.; De Simone, I.; Torri, V.; Salmaggi, A. Antiepileptic treatment and survival in newly diagnosed glioblastoma patients: Retrospective multicentre study in 285 Italian patients. J. Neurol. Sci. 2018, 390, 14–19. [Google Scholar] [CrossRef] [PubMed]
- Stupp, R.; Mason, W.P.; van den Bent, M.J.; Weller, M.; Fisher, B.; Taphoorn, M.J.B.; Belanger, K.; Brandes, A.A.; Marosi, C.; Bogdahn, U.; et al. Radiotherapy plus concomitant and adjuvant temozolomide for glioblastoma. N. Engl. J. Med. 2005, 352, 987–996. [Google Scholar] [CrossRef]
- Domingo-Musibay, E.; Galanis, E. What next for newly diagnosed glioblastoma? Future Oncol. 2015, 11, 3273–3283. [Google Scholar] [CrossRef] [Green Version]
- Pierscianek, D.; Ahmadipour, Y.; Kaier, K.; Oppong, M.D.; Michel, A.; Kebir, S.; Stuschke, M.; Glas, M.; Sure, U.; Jabbarli, R. The SHORT score for preoperative assessment of the risk for short-term survival in glioblastoma. World Neurosurg. 2020, 138, e370–e380. [Google Scholar] [CrossRef]
- Flanigan, P.M.; Jahangiri, A.; Kuang, R.; Truong, A.; Choi, S.; Chou, A.; Rick, J.W.; Chang, S.M.; Molinaro, A.M.; McDermott, M.W.; et al. Improved survival with decreased wait time to surgery in glioblastoma patients presenting with seizure. Neurosurgery 2017, 81, 824–833. [Google Scholar] [CrossRef]
- Lorimer, C.F.; Hanna, C.; Saran, F.; Chalmers, A.; Brock, J. Challenges to Treating older glioblastoma patients: The influence of clinical and tumour characteristics on survival outcomes. Clin. Oncol. (R. Coll. Radiol.) 2017, 29, 739–747. [Google Scholar] [CrossRef] [PubMed]
- Lu, V.M.; Jue, T.R.; Phan, K.; McDonald, K.L. Quantifying the prognostic significance in glioblastoma of seizure history at initial presentation: A systematic review and meta-analysis. Clin. Neurol. Neurosurg. 2018, 164, 75–80. [Google Scholar] [CrossRef] [PubMed]
- Toledo, M.; Sarria-Estrada, S.; Quintana, M.; Maldonado, X.; Martinez-Ricarte, F.; Rodon, J.; Auger, C.; Salas-Puig, J.; Santamarina, E.; Martinez-Saez, E. Prognostic implications of epilepsy in glioblastomas. Clin. Neurol. Neurosurg. 2015, 139, 166–171. [Google Scholar] [CrossRef]
- Yuile, P.; Dent, O.; Cook, R.; Biggs, M.; Little, N. Survival of glioblastoma patients related to presenting symptoms, brain site and treatment variables. J. Clin. Neurosci. 2006, 13, 747–751. [Google Scholar] [CrossRef]
- Berendsen, S.; Varkila, M.; Kroonen, J.; Seute, T.; Snijders, T.J.; Kauw, F.; Spliet, W.G.; Willems, M.; Poulet, C.; Broekman, M.L.; et al. Prognostic relevance of epilepsy at presentation in glioblastoma patients. Neuro. Oncol. 2016, 18, 700–706. [Google Scholar] [CrossRef] [Green Version]
- Goldstein, E.D.; Feyissa, A.M. Brain tumor related-epilepsy. Neurol. Neurochir. Pol. 2018, 52, 436–447. [Google Scholar] [CrossRef]
- Ahmadipour, Y.; Rauschenbach, L.; Santos, A.; Darkwah Oppong, M.; Lazaridis, L.; Quesada, C.M.; Junker, A.; Pierscianek, D.; Dammann, P.; Wrede, K.H.; et al. Preoperative and early postoperative seizures in patients with glioblastoma—Two sides of the same coin? Neurooncol. Adv. 2021, 3. in press. [Google Scholar] [CrossRef] [PubMed]
- Happold, C.; Gorlia, T.; Chinot, O.; Gilbert, M.R.; Nabors, L.B.; Wick, W.; Pugh, S.L.; Hegi, M.; Cloughesy, T.; Roth, P.; et al. Does valproic acid or levetiracetam improve survival in glioblastoma? A pooled analysis of prospective clinical trials in newly diagnosed glioblastoma. J. Clin. Oncol. 2016, 34, 731. [Google Scholar] [CrossRef] [PubMed]
- Dobran, M.; Nasi, D.; Chiriatti, S.; Gladi, M.; di Somma, L.; Iacoangeli, M.; Scerrati, M. Prognostic factors in glioblastoma: Is there a role for epilepsy? Neurol. Med. Chir. 2018, 58, 110–115. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Dührsen, L.; Sauvigny, T.; Ricklefs, F.L.; Mende, K.C.; Schaper, M.; Matschke, J.; Goebell, E.; Westphal, M.; Martens, T. Seizures as presenting symptom in patients with glioblastoma. Epilepsia 2019, 60, 149–154. [Google Scholar] [CrossRef] [Green Version]
- Henker, C.; Kriesen, T.; Scherer, M.; Glass, Ä.; Von Deimling, A.; Bendszus, M.; Weber, M.A.; Herold-Mende, C.; Unterberg, A.; Piek, J. Association between tumor compartment volumes, the incidence of pretreatment seizures, and statin-mediated protective effects in glioblastoma. Neurosurgery 2019, 85, E722–E729. [Google Scholar] [CrossRef] [PubMed]
- Henker, C.; Kriesen, T.; Scherer, M.; Glass, Ä.; Von Deimling, A.; Bendszus, M.; Weber, M.A.; Herold-Mende, C.; Unterberg, A.; Piek, J. Correlation of enzyme-inducing anticonvulsant use with outcome of patients with glioblastoma. Neurology 2009, 85, E722–E729. [Google Scholar]
- Liang, S.; Zhang, J.; Zhang, S.; Fu, X. Epilepsy in adults with supratentorial glioblastoma: Incidence and influence factors and prophylaxis in 184 patients. PLoS ONE 2016, 11, e0158206. [Google Scholar] [CrossRef]
- Mineo, J.F.; Bordron, A.; Baroncini, M.; Ramirez, C.; Maurage, C.A.; Blond, S.; Dam-Hieu, P. Prognosis factors of survival time in patients with glioblastoma multiforme: A multivariate analysis of 340 patients. Acta Neurochir. 2007, 149, 245–253. [Google Scholar] [CrossRef]
- Rosati, A.; Poliani, P.L.; Todeschini, A.; Cominelli, M.; Medicina, D.; Cenzato, M.; Simoncini, E.L.; Magrini, S.M.; Buglione, M.; Grisanti, S.; et al. Glutamine synthetase expression as a valuable marker of epilepsy and longer survival in newly diagnosed glioblastoma multiforme. Neuro. Oncol. 2013, 15, 618–625. [Google Scholar] [CrossRef]
- Shin, J.Y.; Kizilbash, S.H.; Robinson, S.; Uhm, J.H.; Jatoi, A. Incidence, characteristics, and implications of seizures in patients with glioblastoma. Am. J. Hosp. Palliat. Care. 2017, 34, 650–653. [Google Scholar] [CrossRef] [PubMed]
- Salvati, M.; Bruzzaniti, P.; Relucenti, M.; Nizzola, M.; Familiari, P.; Giugliano, M.; Scafa, A.K.; Galletta, S.; Li, X.; Chen, R.; et al. Retrospective and randomized analysis of influence and correlation of clinical and molecular prognostic factors in a mono-operative series of 122 patients with glioblastoma treated with STR or GTR. Brain Sci. 2020, 10, 91. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Vecht, C.J.; Kerkhof, M.; Duran-Pena, A. Seizure prognosis in brain tumors: New insights and evidence-based management. Oncologist 2014, 19, 751. [Google Scholar] [CrossRef] [Green Version]
- Knudsen-Baas, K.M.; Engeland, A.; Gilhus, N.E.; Storstein, A.M.; Owe, J.F. Does the choice of antiepileptic drug affect survival in glioblastoma patients? J. Neurooncol. 2016, 129, 461–469. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Roh, T.H.; Moon, J.H.; Park, H.H.; Kim, E.H.; Hong, C.K.; Kim, S.H.; Kang, S.G.; Chang, J.H. Association between survival and levetiracetam use in glioblastoma patients treated with temozolomide chemoradiotherapy. Sci. Rep. 2020, 10, 10783. [Google Scholar] [CrossRef] [PubMed]
- Ryu, J.Y.; Min, K.L.; Chang, M.J. Effect of anti-epileptic drugs on the survival of patients with glioblastoma multiforme: A retrospective, single-center study. PLoS ONE 2019, 14, e0225599. [Google Scholar] [CrossRef] [Green Version]
- Louis, D.N.; Perry, A.; Reifenberger, G.; Von Deimling, A.; Figarella-Branger, D.; Cavenee, W.K.; Ohgaki, H.; Wiestler, O.D.; Kleihues, P.; Ellison, D.W. The 2016 world health organization classification of tumors of the central nervous system: A summary. Acta Neuropathol. 2016, 131, 803–820. [Google Scholar] [CrossRef] [Green Version]
- Leao, D.J.; Craig, P.G.; Godoy, L.F.; Leite, C.C.; Policeni, B. Response assessment in neuro-oncology criteria for gliomas: Practical approach using conventional and advanced techniques. AJNR Am. J. Neuroradiol. 2020, 41, 10–20. [Google Scholar] [CrossRef]
- Barker, C.A.; Bishop, A.J.; Chang, M.; Beal, K.; Chan, T.A. Valproic acid use during radiation therapy for glioblastoma associated with improved survival. Int. J. Radiat. Oncol. Biol. Phys. 2013, 86, 504–509. [Google Scholar] [CrossRef] [Green Version]
- Cardona, A.F.; Rojas, L.; Wills, B.; Bernal, L.; Ruiz-Patiño, A.; Arrieta, O.; Hakim, E.J.; Hakim, F.; Mejía, J.A.; Useche, N.; et al. Efficacy and safety of levetiracetam vs. other antiepileptic drugs in hispanic patients with glioblastoma. J. Neurooncol. 2018, 136, 363–371. [Google Scholar] [CrossRef] [PubMed]
- Kim, Y.H.; Kim, T.; Joo, J.D.; Han, J.H.; Kim, Y.J.; Kim, I.A.; Yun, C.H.; Kim, C.Y. Survival benefit of levetiracetam in patients treated with concomitant chemoradiotherapy and adjuvant chemotherapy with temozolomide for glioblastoma multiforme. Cancer 2015, 121, 2926–2932. [Google Scholar] [CrossRef] [PubMed]
- Kerkhof, M.; Dielemans, J.C.; van Breemen, M.S.; Zwinkels, H.; Walchenbach, R.; Taphoorn, M.J.; Vecht, C.J. Effect of valproic acid on seizure control and on survival in patients with glioblastoma multiforme. Neuro. Oncol. 2013, 15, 961–967. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Weller, M.; Gorlia, T.; Cairncross, J.G.; Van Den Bent, M.J.; Mason, W.; Belanger, K.; Brandes, A.A.; Bogdahn, U.; Macdonald, D.R.; Forsyth, P.; et al. Prolonged survival with valproic acid use in the EORTC/NCIC temozolomide trial for glioblastoma. Neurology 2011, 77, 1156–1164. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Tsai, H.C.; Wei, K.C.; Tsai, C.N.; Huang, Y.C.; Chen, P.Y.; Chen, S.M.; Lu, Y.J.; Lee, S.T. Effect of valproic acid on the outcome of glioblastoma multiforme. Br. J. Neurosurg. 2012, 26, 347–354. [Google Scholar] [CrossRef]
- Bobustuc, G.C.; Baker, C.H.; Limaye, A.; Jenkins, W.D.; Pearl, G.; Avgeropoulos, N.G.; Konduri, S.D. Levetiracetam enhances p53-mediated MGMT inhibition and sensitizes glioblastoma cells to temozolomide. Neuro. Oncol. 2010, 12, 917–927. [Google Scholar] [CrossRef] [Green Version]


{kind=link}
{kind=link}
{kind=link}
{kind=link}
| In the Whole Cohort | In the CCRT + TMZ-Subgroup | |||||||||
|---|---|---|---|---|---|---|---|---|---|---|
| Median | 95% CI | HR | 95% CI | p-Value | Median | 95% CI | HR | 95% CI | p-Value | |
| Mono AED vs. Combined AED | ||||||||||
| Mono AED | 15.0 | 13.01–16.99 | 1.23 | 0.65–2.33 | 0.532 | 15.0 | 13.01–16.99 | 1.23 | 0.65–2.33 | 0.532 |
| Combined AED | 10.27 | 7.94–12.59 | 10.27 | 7.94–12.59 | ||||||
| NEIAED vs. EIAED | ||||||||||
| NEIAED | 11.8 | 9.96–13.64 | 0.89 | 0.61–1.28 | 0.520 | 14.5 | 12.45–16.55 | 1.17 | 0.71–1.92 | 0.532 |
| EIAED | 9.67 | 4.67–14.67 | 15.07 | 11.42–18.72 | ||||||
| LEV vs. Any Other AED | ||||||||||
| LEV | 12.8 | 10.82–14.78 | 0.70 | 0.54–0.89 | 0.004 | 15 | 12.32–17.68 | 0.78 | 0.59–1.05 | 0.100 |
| Other AED | 9.07 | 6.68–11.46 | 14.23 | 10.27–18.19 | ||||||
| LEV vs. No LEV | ||||||||||
| LEV | 12.8 | 10.82–14.78 | 0.68 | 0.57–0.81 | <0.0001 | 15 | 12.32–17.68 | 0.73 | 0.60–0.89 | 0.002 |
| No LEV | 8.77 | 7.77–9.77 | 12.13 | 11.24–13.03 | ||||||
| Parameter | OS | PFS | ||||
|---|---|---|---|---|---|---|
| aHR | 95% CI | p-Value | aHR | 95% CI | p-Value | |
| LEV treatment | 0.76 | 0.59–0.97 | 0.030 | 0.69 | 0.51–0.93 | 0.015 |
| Age. per-year-increase | 1.03 | 1.02–1.03 | <0.0001 | 1.02 | 1.01–1.03 | <0.0001 |
| AED due to seizures | 1.10 | 0.89–1.36 | 0.381 | 1.21 | 0.93–1.58 | 0.161 |
| KPS < 80% | 1.40 | 1.18–1.65 | <0.0001 | 1.32 | 1.08–1.62 | 0.006 |
| Tumor location (midline) | 1.33 | 0.93–1.90 | 0.111 | 1.30 | 0.86–1.99 | 0.211 |
| EOR | 0.63 | 0.57–0.70 | <0.0001 | 0.73 | 0.64–0.82 | <0.0001 |
| MGMT-methylation | 0.68 | 0.57–0.81 | <0.0001 | 0.77 | 0.63–0.93 | 0.007 |
| IDH1-mutation | 0.76 | 0.38–1.54 | 0.388 | 0.99 | 0.43–2.30 | 0.984 |
| CCRT + TMZ | 0.38 | 0.31–0.47 | <0.0001 | 0.32 | 0.26–0.41 | <0.0001 |
| In the Whole Cohort | In the CCRT + TMZ-Subgroup | |||||||||
|---|---|---|---|---|---|---|---|---|---|---|
| Median | 95% CI | HR | 95% CI | p-Value | Median | 95% CI | HR | 95% CI | p-Value | |
| Mono AED vs. Combined AED | ||||||||||
| Mono AED | 8.0 | 6.4–9.6 | 1.33 | 0.62–2.86 | 0.464 | 8.0 | 6.4–9.6 | 1.33 | 0.62–2.86 | 0.464 |
| Combined AED | 4.0 | 1.52–6.48 | 4.0 | 1.52–6.48 | ||||||
| NEIAED vs. EIAED | ||||||||||
| NEIAED | 6.0 | 5.0–7.0 | 0.59 | 0.37–0.96 | 0.034 | 8.0 | 6.37–9.63 | 0.83 | 0.41–1.71 | 0.620 |
| EIAED | 4.0 | 1.43–6.57 | 5.0 | 3.54–6.46 | ||||||
| LEV vs. Any Other AED | ||||||||||
| LEV | 7.0 | 5.83–8.17 | 0.67 | 0.50–0.91 | 0.010 | 8.0 | 6.24–9.76 | 0.80 | 0.55–1.17 | 0.249 |
| Other AED | 4.0 | 2.79–5.21 | 7.0 | 3.32–10.68 | ||||||
| LEV vs. No LEV | ||||||||||
| LEV | 7.0 | 5.83–8.17 | 0.72 | 0.59–0.88 | 0.001 | 8.0 | 6.24–9.76 | 0.77 | 0.62–0.97 | 0.024 |
| No LEV | 4.5 | 3.86–5.14 | 6.0 | 5.46–6.54 | ||||||
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Jabbarli, R.; Ahmadipour, Y.; Rauschenbach, L.; Santos, A.N.; Darkwah Oppong, M.; Pierscianek, D.; Quesada, C.M.; Kebir, S.; Dammann, P.; Guberina, N.; et al. How about Levetiracetam in Glioblastoma? An Institutional Experience and Meta-Analysis. Cancers 2021, 13, 3770. https://doi.org/10.3390/cancers13153770
Jabbarli R, Ahmadipour Y, Rauschenbach L, Santos AN, Darkwah Oppong M, Pierscianek D, Quesada CM, Kebir S, Dammann P, Guberina N, et al. How about Levetiracetam in Glioblastoma? An Institutional Experience and Meta-Analysis. Cancers. 2021; 13(15):3770. https://doi.org/10.3390/cancers13153770
Chicago/Turabian StyleJabbarli, Ramazan, Yahya Ahmadipour, Laurèl Rauschenbach, Alejandro N. Santos, Marvin Darkwah Oppong, Daniela Pierscianek, Carlos M. Quesada, Sied Kebir, Philipp Dammann, Nika Guberina, and et al. 2021. "How about Levetiracetam in Glioblastoma? An Institutional Experience and Meta-Analysis" Cancers 13, no. 15: 3770. https://doi.org/10.3390/cancers13153770
APA StyleJabbarli, R., Ahmadipour, Y., Rauschenbach, L., Santos, A. N., Darkwah Oppong, M., Pierscianek, D., Quesada, C. M., Kebir, S., Dammann, P., Guberina, N., Scheffler, B., Kaier, K., Stuschke, M., Sure, U., & Wrede, K. H. (2021). How about Levetiracetam in Glioblastoma? An Institutional Experience and Meta-Analysis. Cancers, 13(15), 3770. https://doi.org/10.3390/cancers13153770