
Genetic Analysis and Operative Outcomes in Patients with Oncogene-Driven Advanced NSCLC Treated with Cytoreductive Surgery as a Component of Local Consolidative Therapy

 , , , and
, , , and
Abstract
Simple Summary
Abstract
1. Introduction
2. Patients and Methods
2.1. Patients
2.2. Molecular Analyses
2.3. Next-Generation Sequencing (NGS)
2.4. Statistical Analysis
3. Results
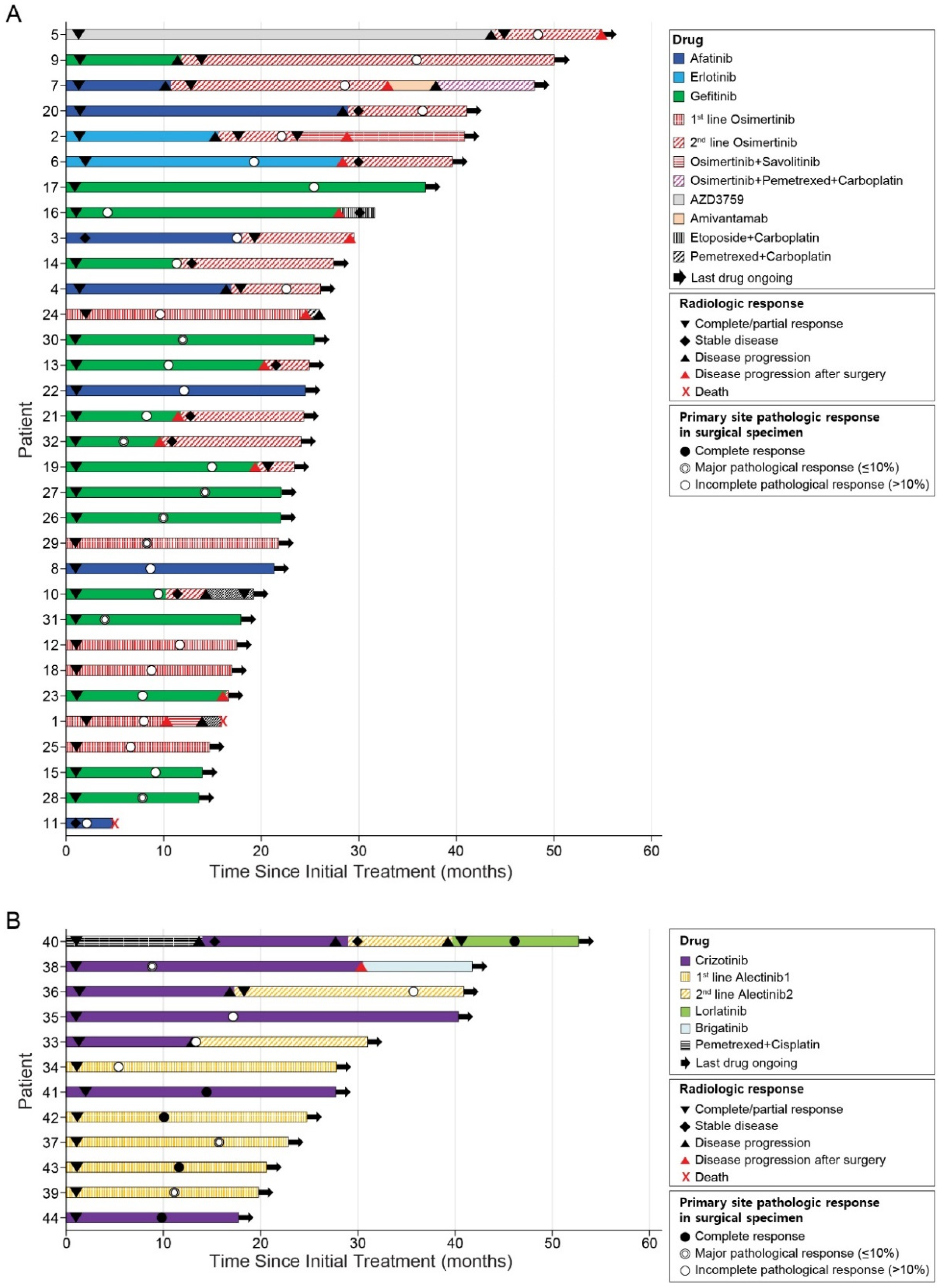
3.1. Baseline Characteristics and Treatments Prior to Surgery
3.2. Surgical Outcomes
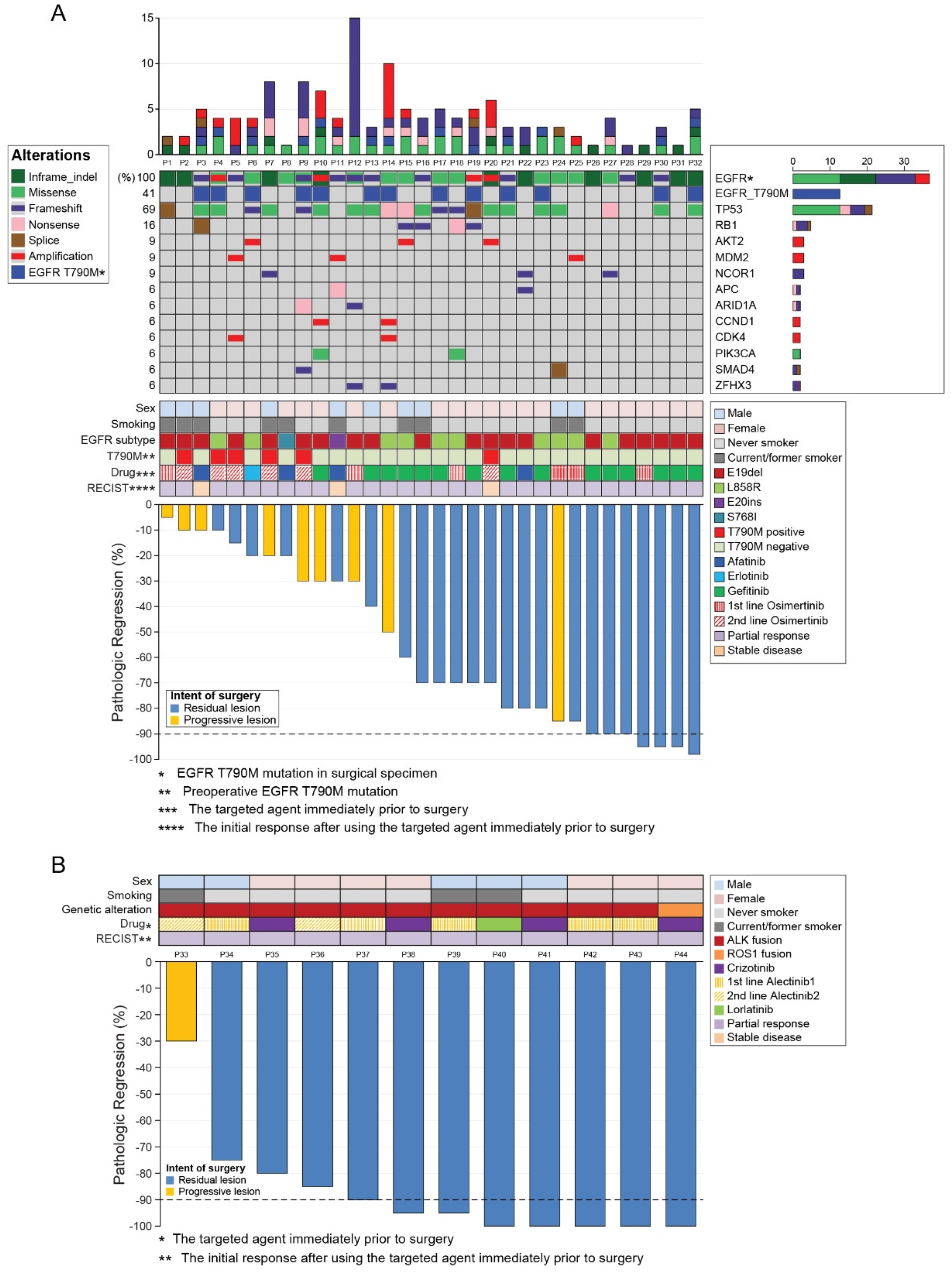
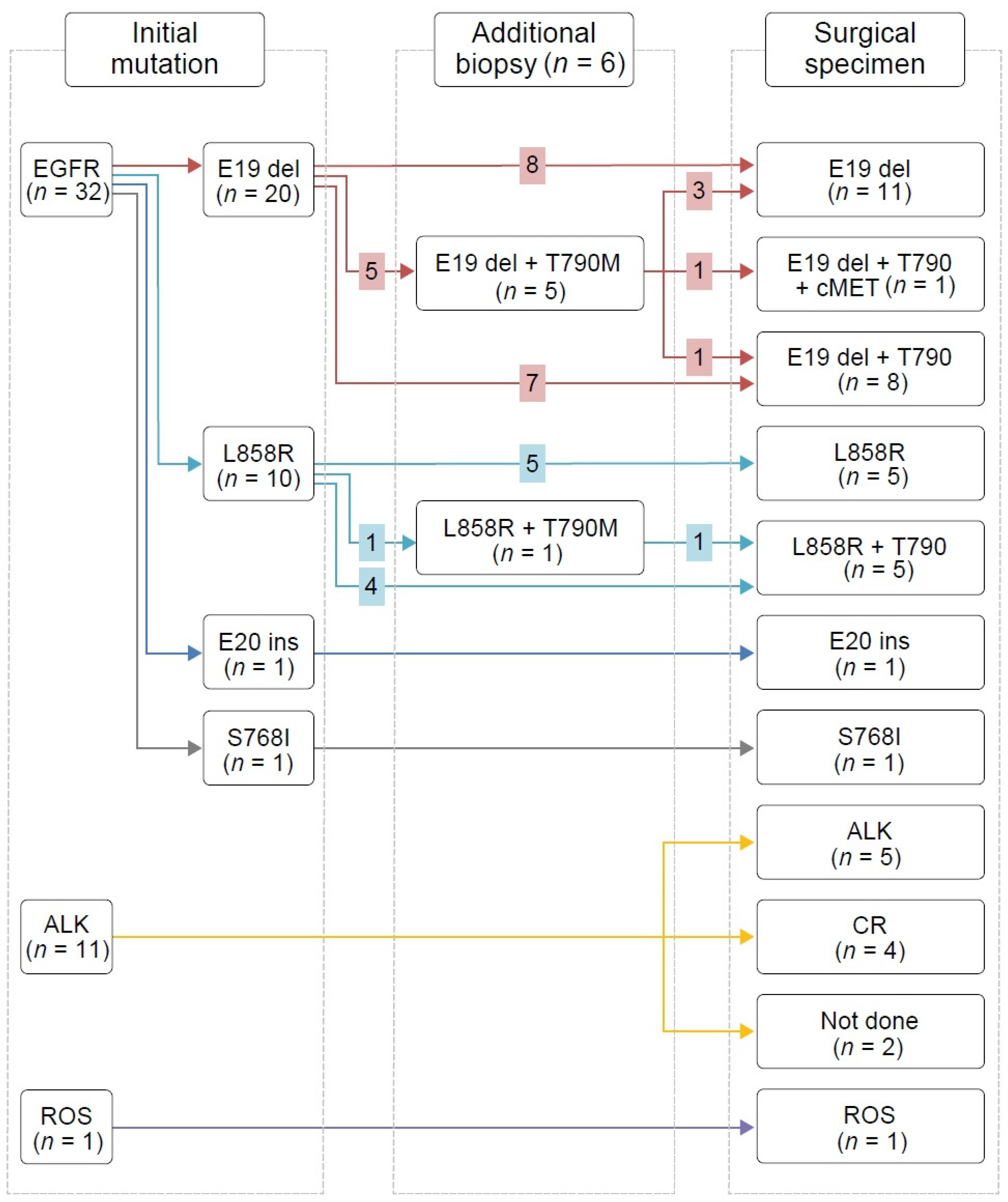
3.3. Pathologic Analysis of Surgical Specimens
3.4. NGS and Mutation Profiles
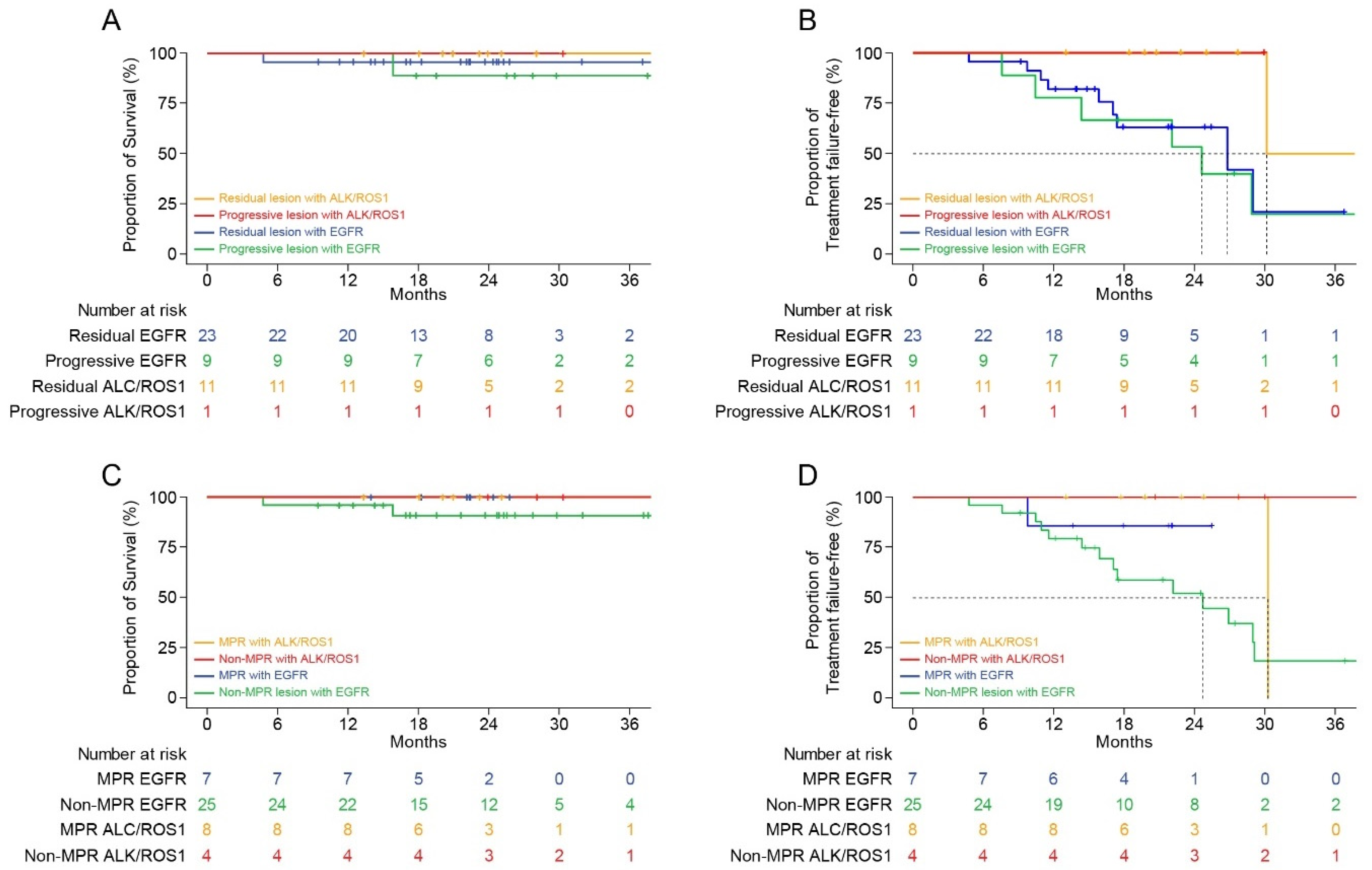
3.5. Survival Analysis
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Mok, T.S.; Wu, Y.L.; Thongprasert, S.; Yang, C.H.; Chu, D.T.; Saijo, N.; Sunpaweravong, P.; Han, B.; Margono, B.; Ichinose, Y.; et al. Gefitinib or carboplatin-paclitaxel in pulmonary adenocarcinoma. N. Engl. J. Med. 2009, 361, 947–957. [Google Scholar] [CrossRef]
- Solomon, B.J.; Mok, T.; Kim, D.W.; Wu, Y.L.; Nakagawa, K.; Mekhail, T.; Felip, E.; Cappuzzo, F.; Paolini, J.; Usari, T.; et al. First-line crizotinib versus chemotherapy in ALK-positive lung cancer. N. Engl. J. Med. 2014, 371, 2167–2177. [Google Scholar] [CrossRef] [PubMed]
- Zhong, W.Z.; Chen, K.N.; Chen, C.; Gu, C.D.; Wang, J.; Yang, X.N.; Mao, W.M.; Wang, Q.; Qiao, G.B.; Cheng, Y.; et al. Erlotinib Versus Gemcitabine Plus Cisplatin as Neoadjuvant Treatment of Stage IIIA-N2 EGFR-Mutant Non-Small-Cell Lung Cancer (EMERGING-CTONG 1103): A Randomized Phase II Study. J. Clin. Oncol. 2019, 37, 2235–2245. [Google Scholar] [CrossRef] [PubMed]
- Al-Halabi, H.; Sayegh, K.; Digamurthy, S.R.; Niemierko, A.; Piotrowska, Z.; Willers, H.; Sequist, L.V. Pattern of Failure Analysis in Metastatic EGFR-Mutant Lung Cancer Treated with Tyrosine Kinase Inhibitors to Identify Candidates for Consolidation Stereotactic Body Radiation Therapy. J. Thorac. Oncol. 2015, 10, 1601–1607. [Google Scholar] [CrossRef]
- Sorensen, B.S.; Wu, L.; Wei, W.; Tsai, J.; Weber, B.; Nexo, E.; Meldgaard, P. Monitoring of epidermal growth factor receptor tyrosine kinase inhibitor-sensitizing and resistance mutations in the plasma DNA of patients with advanced non-small cell lung cancer during treatment with erlotinib. Cancer 2014, 120, 3896–3901. [Google Scholar] [CrossRef]
- Gomez, D.R.; Blumenschein, G.R., Jr.; Lee, J.J.; Hernandez, M.; Ye, R.; Camidge, D.R.; Doebele, R.C.; Skoulidis, F.; Gaspar, L.E.; Gibbons, D.L.; et al. Local consolidative therapy versus maintenance therapy or observation for patients with oligometastatic non-small-cell lung cancer without progression after first-line systemic therapy: A multicentre, randomised, controlled, phase 2 study. Lancet Oncol. 2016, 17, 1672–1682. [Google Scholar] [CrossRef]
- Iyengar, P.; Wardak, Z.; Gerber, D.E.; Tumati, V.; Ahn, C.; Hughes, R.S.; Dowell, J.E.; Cheedella, N.; Nedzi, L.; Westover, K.D.; et al. Consolidative Radiotherapy for Limited Metastatic Non–Small-Cell Lung Cancer: A Phase 2 Randomized Clinical Trial. JAMA Oncol. 2018, 4, e173501. [Google Scholar] [CrossRef] [PubMed]
- Gomez, D.R.; Tang, C.; Zhang, J.; Blumenschein, G.R., Jr.; Hernandez, M.; Lee, J.J.; Ye, R.; Palma, D.A.; Louie, A.V.; Camidge, D.R.; et al. Local Consolidative Therapy Vs. Maintenance Therapy or Observation for Patients with Oligometastatic Non-Small-Cell Lung Cancer: Long-Term Results of a Multi-Institutional, Phase II, Randomized Study. J. Clin. Oncol. 2019, 37, 1558–1565. [Google Scholar] [CrossRef] [PubMed]
- Chan, O.S.H.; Lam, K.C.; Li, J.Y.C.; Choi, F.P.T.; Wong, C.Y.H.; Chang, A.T.Y.; Mo, F.K.F.; Wang, K.; Yeung, R.M.W.; Mok, T.S.K. ATOM: A phase II study to assess efficacy of preemptive local ablative therapy to residual oligometastases of NSCLC after EGFR TKI. Lung Cancer 2020, 142, 41–46. [Google Scholar] [CrossRef]
- Bivona, T.G.; Doebele, R.C. A framework for understanding and targeting residual disease in oncogene-driven solid cancers. Nat. Med. 2016, 22, 472–478. [Google Scholar] [CrossRef] [PubMed]
- Nahar, R.; Zhai, W.; Zhang, T.; Takano, A.; Khng, A.J.; Lee, Y.Y.; Liu, X.; Lim, C.H.; Koh, T.P.T.; Aung, Z.W.; et al. Elucidating the genomic architecture of Asian EGFR-mutant lung adenocarcinoma through multi-region exome sequencing. Nat. Commun. 2018, 9, 216. [Google Scholar] [CrossRef] [PubMed]
- Dindo, D.; Demartines, N.; Clavien, P.A. Classification of surgical complications: A new proposal with evaluation in a cohort of 6336 patients and results of a survey. Ann. Surg. 2004, 240, 205–213. [Google Scholar] [CrossRef]
- Li, M.M.; Datto, M.; Duncavage, E.J.; Kulkarni, S.; Lindeman, N.I.; Roy, S.; Tsimberidou, A.M.; Vnencak-Jones, C.L.; Wolff, D.J.; Younes, A.; et al. Standards and Guidelines for the Interpretation and Reporting of Sequence Variants in Cancer: A Joint Consensus Recommendation of the Association for Molecular Pathology, American Society of Clinical Oncology, and College of American Pathologists. J. Mol. Diagn. 2017, 19, 4–23. [Google Scholar] [CrossRef]
- Travis, W.D.; Dacic, S.; Wistuba, I.; Sholl, L.; Adusumilli, P.; Bubendorf, L.; Bunn, P.; Cascone, T.; Chaft, J.; Chen, G.; et al. IASLC Multidisciplinary Recommendations for Pathologic Assessment of Lung Cancer Resection Specimens After Neoadjuvant Therapy. J. Thorac. Oncol. 2020, 15, 709–740. [Google Scholar] [CrossRef] [PubMed]
- Eisenhauer, E.A.; Therasse, P.; Bogaerts, J.; Schwartz, L.H.; Sargent, D.; Ford, R.; Dancey, J.; Arbuck, S.; Gwyther, S.; Mooney, M.; et al. New response evaluation criteria in solid tumours: Revised RECIST guideline (version 1.1). Eur. J. Cancer 2009, 45, 228–247. [Google Scholar] [CrossRef] [PubMed]
- Ramirez, M.; Rajaram, S.; Steininger, R.J.; Osipchuk, D.; Roth, M.A.; Morinishi, L.S.; Evans, L.; Ji, W.; Hsu, C.H.; Thurley, K.; et al. Diverse drug-resistance mechanisms can emerge from drug-tolerant cancer persister cells. Nat. Commun. 2016, 7, 10690. [Google Scholar] [CrossRef] [PubMed]
- Wang, X.; Zeng, Z.; Cai, J.; Xu, P.; Liang, P.; Luo, Y.; Liu, A. Efficacy and acquired resistance for EGFR-TKI plus thoracic SBRT in patients with advanced EGFR-mutant non-small-cell lung cancer: A propensity-matched retrospective study. BMC Cancer 2021, 21, 482. [Google Scholar] [CrossRef] [PubMed]
- Yamamoto, Y.; Kodama, K.; Maniwa, T.; Takeda, M. Surgical resection of advanced non-small cell lung cancer after a response to EGFR-TKI: Presentation of two cases and a literature review. J. Cardiothorac. Surg. 2017, 12, 98. [Google Scholar] [CrossRef] [PubMed]
- Byun, C.S.; Lee, S.; Kim, D.J.; Lee, J.G.; Lee, C.Y.; Jung, I.; Chung, K.Y. Analysis of Unexpected Conversion to Thoracotomy During Thoracoscopic Lobectomy in Lung Cancer. Ann. Thorac. Surg. 2015, 100, 968–973. [Google Scholar] [CrossRef]
- Bott, M.J.; Yang, S.C.; Park, B.J.; Adusumilli, P.S.; Rusch, V.W.; Isbell, J.M.; Downey, R.J.; Brahmer, J.R.; Battafarano, R.; Bush, E.; et al. Initial results of pulmonary resection after neoadjuvant nivolumab in patients with resectable non-small cell lung cancer. J. Thorac. Cardiovasc. Surg. 2019, 158, 269–276. [Google Scholar] [CrossRef] [PubMed]
- Hishida, T.; Yoshida, J.; Aokage, K.; Nagai, K.; Tsuboi, M. Long-term outcome of surgical resection for residual or regrown advanced non-small cell lung carcinomas following EGFR-TKI treatment: Report of four cases. Gen. Thorac. Cardiovasc. Surg. 2016, 64, 429–433. [Google Scholar] [CrossRef] [PubMed]
- Ramalingam, S.S.; Vansteenkiste, J.; Planchard, D.; Cho, B.C.; Gray, J.E.; Ohe, Y.; Zhou, C.; Reungwetwattana, T.; Cheng, Y.; Chewaskulyong, B.; et al. Overall Survival with Osimertinib in Untreated, EGFR-Mutated Advanced NSCLC. N. Engl. J. Med. 2020, 382, 41–50. [Google Scholar] [CrossRef] [PubMed]
- Leonetti, A.; Sharma, S.; Minari, R.; Perego, P.; Giovannetti, E.; Tiseo, M. Resistance mechanisms to osimertinib in EGFR-mutated non-small cell lung cancer. Br. J. Cancer 2019, 121, 725–737. [Google Scholar] [CrossRef]
- Piper-Vallillo, A.J.; Sequist, L.V.; Piotrowska, Z. Emerging Treatment Paradigms for EGFR-Mutant Lung Cancers Progressing on Osimertinib: A Review. J. Clin. Oncol. 2020, 38, 2926–2936. [Google Scholar] [CrossRef] [PubMed]
- Hong, S.; Gao, F.; Fu, S.; Wang, Y.; Fang, W.; Huang, Y.; Zhang, L. Concomitant Genetic Alterations with Response to Treatment and Epidermal Growth Factor Receptor Tyrosine Kinase Inhibitors in Patients With EGFR-Mutant Advanced Non-Small Cell Lung Cancer. JAMA Oncol. 2018, 4, 739–742. [Google Scholar] [CrossRef]
- Lim, S.M.; Kim, H.R.; Cho, E.K.; Min, Y.J.; Ahn, J.S.; Ahn, M.J.; Park, K.; Cho, B.C.; Lee, J.H.; Jeong, H.C.; et al. Targeted sequencing identifies genetic alterations that confer primary resistance to EGFR tyrosine kinase inhibitor (Korean Lung Cancer Consortium). Oncotarget 2016, 7, 36311–36320. [Google Scholar] [CrossRef] [PubMed]
- Kim, Y.; Lee, B.; Shim, J.H.; Lee, S.H.; Park, W.Y.; Choi, Y.L.; Sun, J.M.; Ahn, J.S.; Ahn, M.J.; Park, K. Concurrent Genetic Alterations Predict the Progression to Target Therapy in EGFR-Mutated Advanced NSCLC. J. Thorac. Oncol. 2019, 14, 193–202. [Google Scholar] [CrossRef]
- Lee, J.K.; Lee, J.; Kim, S.; Kim, S.; Youk, J.; Park, S.; An, Y.; Keam, B.; Kim, D.W.; Heo, D.S.; et al. Clonal History and Genetic Predictors of Transformation Into Small-Cell Carcinomas From Lung Adenocarcinomas. J. Clin. Oncol. 2017, 35, 3065–3074. [Google Scholar] [CrossRef]
- Kim, J.O.; Shin, J.Y.; Kim, S.R.; Shin, K.S.; Kim, J.; Kim, M.Y.; Lee, M.R.; Kim, Y.; Kim, M.; Hong, S.H.; et al. Evaluation of Two EGFR Mutation Tests on Tumor and Plasma from Patients with Non-Small Cell Lung Cancer. Cancers 2020, 12, 785. [Google Scholar] [CrossRef]
- Wu, Y.L.; Yang, J.C.; Kim, D.W.; Lu, S.; Zhou, J.; Seto, T.; Yang, J.J.; Yamamoto, N.; Ahn, M.J.; Takahashi, T.; et al. Phase II Study of Crizotinib in East Asian Patients With ROS1-Positive Advanced Non-Small-Cell Lung Cancer. J. Clin. Oncol. 2018, 36, 1405–1411. [Google Scholar] [CrossRef]







{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Characteristic | N or Median | % or IQR |
|---|---|---|
| Age at operation, years | 59 | 53.8–65.3 |
| Sex | ||
| Male | 15 | 34.1% |
| Female | 29 | 65.9% |
| Smoking history | ||
| Never smoked | 31 | 70.5% |
| Former smoker | 12 | 27.3% |
| Current smoker | 1 | 2.3% |
| Smoking, pack-years | 0 | 0–19.3 |
| ECOG | ||
| 0 | 36 | 81.8% |
| 1 | 8 | 18.2% |
| PFT | ||
| FEV1, L | 2.27 | 2.0–2.7 |
| FEV1, % predicted | 92.0% | 83.5–101.0% |
| DLCO, mL/mmHg/min | 17.1 | 15.4–19.6 |
| DLCO, % predicted | 93.0% | 77.0–100.0% |
| Primary tumor location | ||
| RUL | 10 | 22.7% |
| RML | 3 | 6.8% |
| RLL | 14 | 31.8% |
| LUL | 6 | 13.6% |
| LLL | 11 | 25.0% |
| Clinical stage at diagnosis a | ||
| IIIB | 4 | 9.1% |
| IIIC | 1 | 2.3% |
| IVA | 15 | 34.1% |
| IVB | 24 | 54.5% |
| Metastasis sites at diagnosis | ||
| Brain | 10 | 22.7% |
| Bone | 6 | 13.6% |
| Lymph nodes | 6 | 13.6% |
| Intrathoracic organs | 5 | 11.4% |
| Multiple organs | 17 | 38.6% |
| Number of distant metastasis at diagnosis | ||
| 0 | 5 | 11.4% |
| 1–2 | 12 | 27.3% |
| 3–5 | 10 | 22.7% |
| >5 | 17 | 38.6% |
| Combined brain metastasis at diagnosis | 22 | 50.00% |
| Mutational profile at diagnosis | ||
| EGFR mutation | 32 | 72.7% |
| ALK fusion | 11 | 25.0% |
| ROS1 fusion | 1 | 2.3% |
| Variables | N or Median | % or IQR |
|---|---|---|
| Interval from the diagnosis to operation, months | 10.9 | 8.5–18.2 |
| Interval from the initiation of TKI immediately before surgery to the actual operation, months | 9.8 | 7.8–12.9 |
| TKI before surgery | ||
| Gefitinib | 15 | 34.1% |
| Afatinib | 4 | 9.1% |
| Erlotinib | 1 | 2.3% |
| Osimertinib | 12 | 27.3% |
| - First-line | 6 | 13.6% |
| - Later-line based on the acquired T790M mutation | 6 | 13.6% |
| Alectinib | 7 | 15.9% |
| - First-line | 5 | 11.4% |
| - Later-line | 2 | 4.5% |
| Crizotinib | 4 | 9.1% |
| Lorlatinib | 1 | 2.3% |
| Best response to TKI immediately before surgery | ||
| Partial response | 41 | 93.2% |
| Stable disease | 3 | 6.8% |
| Preoperative local control for metastatic site | 21 | 47.7% |
| Surgery | 4 | 9.1% |
| - Brain | 3 | 6.8% |
| - Lymph node | 1 | 2.3% |
| Radiation therapy | 15 | 34.1% |
| - Brain | 8 | 18.2% |
| - Bone | 5 | 11.4% |
| - Brain and bone | 2 | 4.5% |
| Surgery with radiation therapy | 2 | 4.5% |
| - Brain | 2 | 4.5% |
| Preoperative number of distant metastases | ||
| 0 | 22 | 50.0% |
| 1–2 | 9 | 20.5% |
| 3–5 | 6 | 13.6% |
| >5 | 7 | 15.9% |
| Preoperative primary lesion status | ||
| Partial response | 6 | 13.6% |
| Stable disease | 30 | 68.2% |
| Progressive disease | 8 | 18.2% |
| Preoperative metastatic lesion status | ||
| Radiologic “No-evidence-of-disease” status | 19 | 43.2% |
| Partial response | 2 | 4.5% |
| Stable disease | 21 | 47.7% |
| Progressive disease | 2 | 4.5% |
| Intent of surgery | ||
| Residual lesions | 34 | 77.3% |
| Progressive lesions | 10 | 22.7% |
| Variables | N or Median | % or IQR |
|---|---|---|
| Extent of pulmonary resection | ||
| Sub-lobar resection | 5 | 11.4% |
| Lobectomy | 37 | 84.1% |
| Bi-lobectomy | 2 | 4.5% |
| Surgical approach | ||
| Thoracotomy | 2 | 4.5% |
| VATS | 37 | 84.1% |
| Conversion to thoracotomy | 5 | 11.4% |
| - Difficult to dissect lymph node | 3 | 6.8% |
| - Difficult to dissect pulmonary artery | 2 | 4.5% |
| Combined surgical procedure | 20 | 45.5% |
| Neck lymph node dissection | 7 | 15.9% |
| Abdominal lymph node dissection | 1 | 2.3% |
| Separate pulmonary wedge resection | 4 | 9.1% |
| En-bloc resection of adjacent lobe | 5 | 11.4% |
| Other procedure | 3 | 6.8% |
| Duration of surgery, min | 108.5 | 92.0–136.3 |
| Duration of anesthesia, min | 160.0 | 135.0–191.3 |
| Estimated blood loss, mL | ||
| Minimal (≤50) | 29 | 65.9% |
| 50–200 | 12 | 27.3% |
| >200 | 3 | 6.8% |
| Complete resection (surgical field) | ||
| R0 | 41 | 93.2% |
| R1 | 1 | 2.3% |
| R2 | 2 | 4.5% |
| Intensive care unit stay (duration) | 1 (1 day) | 2.3% |
| Chest tube duration, days | 4 | 3.0–5.3 |
| Postoperative hospital stays, days | 5 | 4.0–7.3 |
| Complication (all) | 15 | 34.1% |
| Prolonged air leak (>5 days) | 5 | 11.4% |
| Chyle leakage | 3 | 6.8% |
| Vocal cord palsies | 2 | 4.5% |
| Bronchopleural fistula | 1 | 2.3% |
| Acute kidney injury | 1 | 2.3% |
| Acute lung injury | 1 | 2.3% |
| Pneumonia | 1 | 2.3% |
| Pneumothorax | 1 | 2.3% |
| Complication (Clavien–Dindo > Gr 3) | 4 | 9.1% |
| Chyle leakage | 1 | 2.3% |
| Vocal cord palsies | 1 | 2.3% |
| Broncho-pleural fistula | 1 | 2.3% |
| Pneumothorax | 1 | 2.3% |
| In-hospital mortality | 0 | 0.0% |
| Variables | N or Median | % or IQR |
|---|---|---|
| Postoperative ypStage | ||
| CR | 4 | 9.1% |
| I | 11 | 25.0% |
| II | 2 | 4.5% |
| III | 6 | 13.6% |
| IV | 21 | 47.7% |
| Primary site pathologic response | ||
| CR | 5 | 11.4% |
| Major pathologic response (≤10%) | 10 | 22.7% |
| Incomplete pathologic response (>10%) | 29 | 65.9% |
| Postoperative ypT-stage | ||
| CR | 5 | 11.4% |
| 1 | 23 | 52.3% |
| 2 | 7 | 15.9% |
| 3 | 5 | 11.4% |
| 4 | 4 | 9.1% |
| Postoperative ypN-stage | ||
| 0 | 22 | 50.0% |
| 1 | 6 | 13.6% |
| 2 | 16 | 36.4% |
| Additional mutations in surgical specimens | 12 | 27.3% |
| T790M | 11 | 25.0% |
| MET+ | 1 | 2.3% |
| Targeted agent change based on additional mutations in surgical specimens | 9 | 20.5% |
| Postoperative disease status | ||
| Radiologic “no-evidence-of-disease” status | 23 | 52.3% |
| Radiologic residual disease | 21 | 47.7% |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Park, B.J.; Shim, H.S.; Lee, C.Y.; Lee, J.G.; Kim, H.R.; Lee, S.H.; Hong, M.H.; Park, S.Y. Genetic Analysis and Operative Outcomes in Patients with Oncogene-Driven Advanced NSCLC Treated with Cytoreductive Surgery as a Component of Local Consolidative Therapy. Cancers 2021, 13, 2549. https://doi.org/10.3390/cancers13112549
Park BJ, Shim HS, Lee CY, Lee JG, Kim HR, Lee SH, Hong MH, Park SY. Genetic Analysis and Operative Outcomes in Patients with Oncogene-Driven Advanced NSCLC Treated with Cytoreductive Surgery as a Component of Local Consolidative Therapy. Cancers. 2021; 13(11):2549. https://doi.org/10.3390/cancers13112549
Chicago/Turabian StylePark, Byung Jo, Hyo Sup Shim, Chang Young Lee, Jin Gu Lee, Hye Ryun Kim, Sang Hoon Lee, Min Hee Hong, and Seong Yong Park. 2021. "Genetic Analysis and Operative Outcomes in Patients with Oncogene-Driven Advanced NSCLC Treated with Cytoreductive Surgery as a Component of Local Consolidative Therapy" Cancers 13, no. 11: 2549. https://doi.org/10.3390/cancers13112549
APA StylePark, B. J., Shim, H. S., Lee, C. Y., Lee, J. G., Kim, H. R., Lee, S. H., Hong, M. H., & Park, S. Y. (2021). Genetic Analysis and Operative Outcomes in Patients with Oncogene-Driven Advanced NSCLC Treated with Cytoreductive Surgery as a Component of Local Consolidative Therapy. Cancers, 13(11), 2549. https://doi.org/10.3390/cancers13112549