Computer-Aided Diagnosis in Multiparametric MRI of the Prostate: An Open-Access Online Tool for Lesion Classification with High Accuracy

 ,
,  ,
, 
Abstract

1. Introduction
2. Results
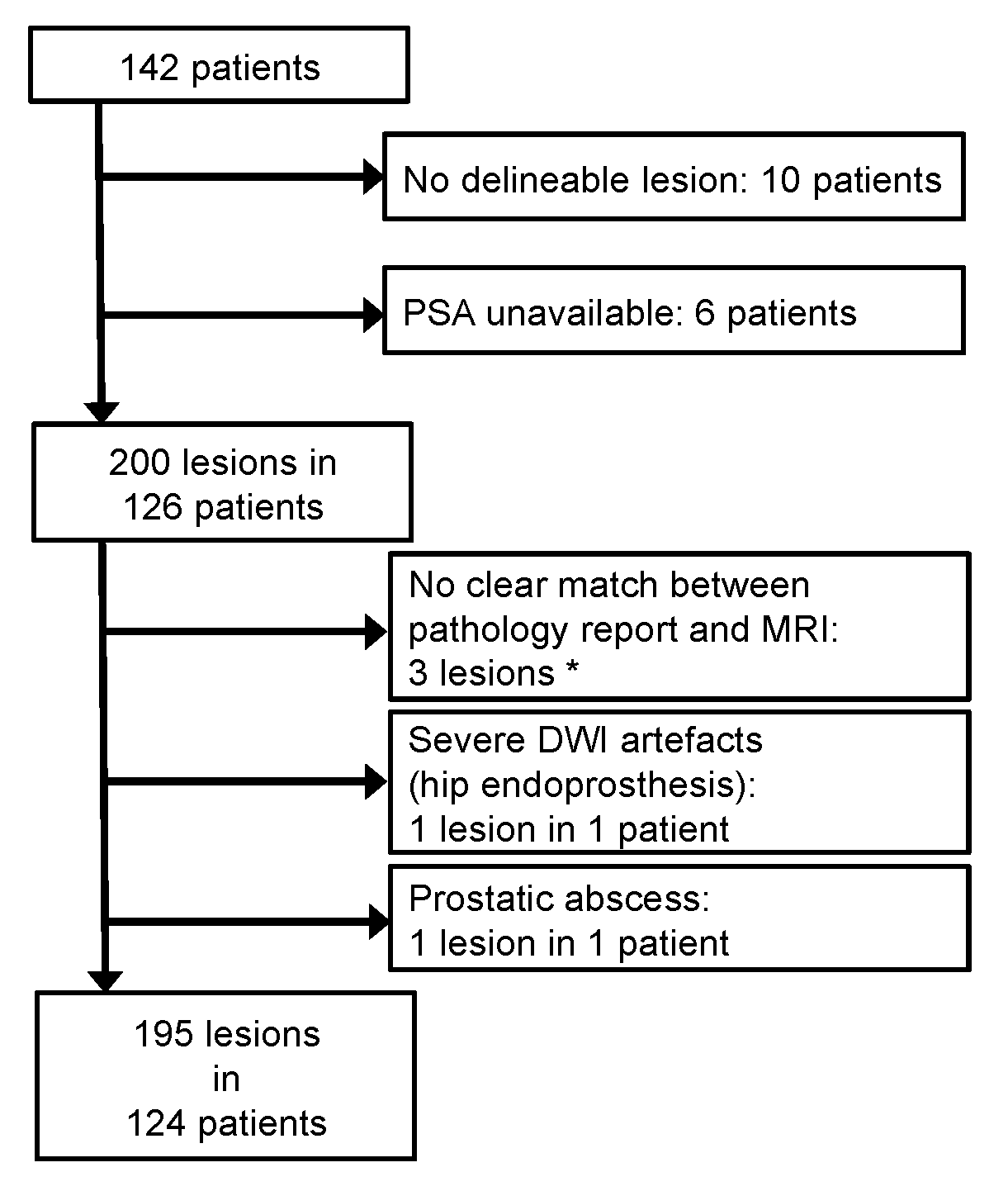
2.1. Patient Characteristics
2.2. Descriptive Statistics
2.3. CADx Development
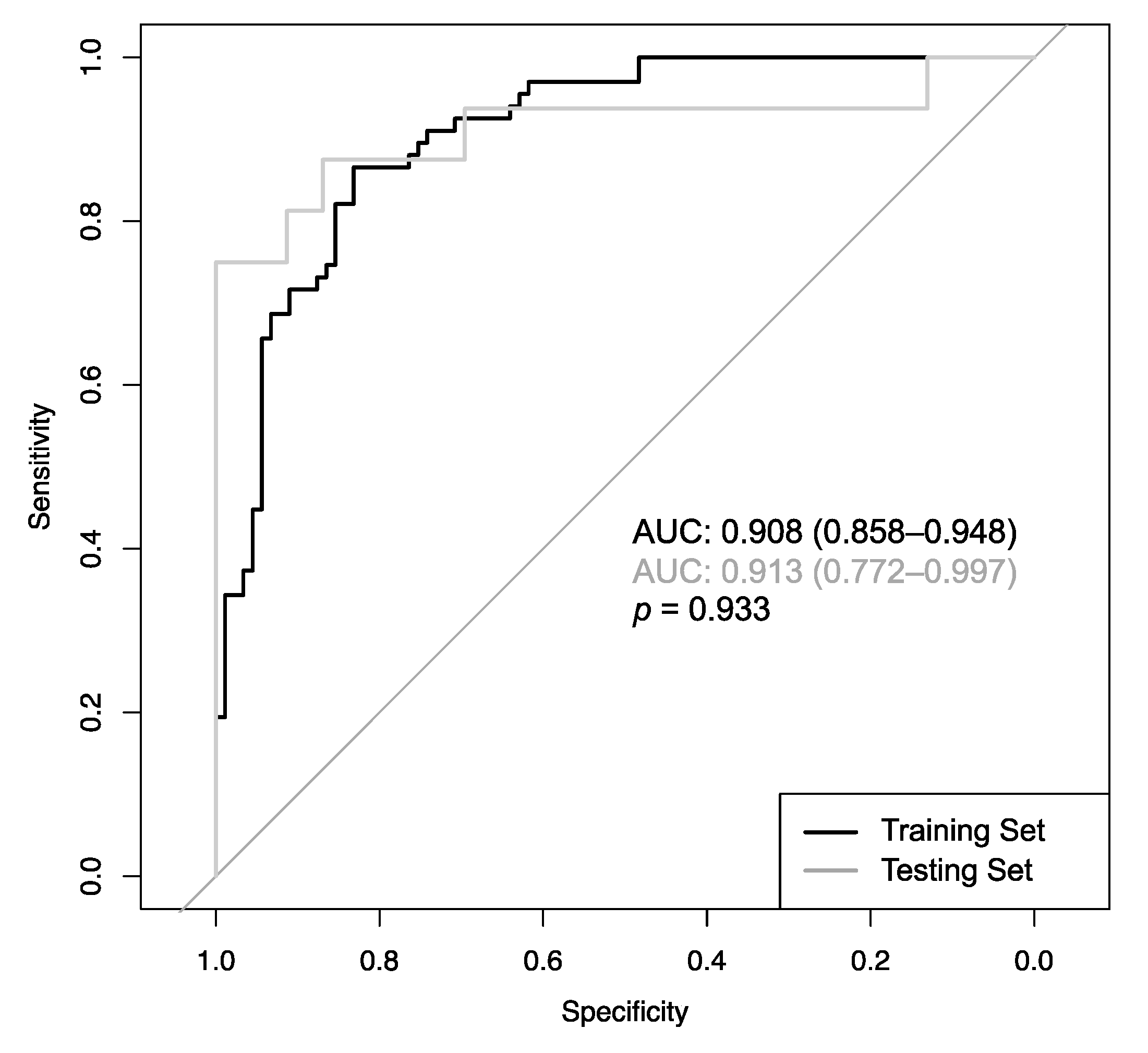
2.4. CADx Performance
3. Discussion
4. Materials and Methods
4.1. Patients
4.2. Imaging
4.2.1. Imaging Parameters
4.2.2. Image Assessment
- TTP (time from bolus arrival to end of wash in),
- AT (start of contrast enhancement),
- Wash in (slope of the line between bolus arrival and end of wash in),
- Wash out (slope of the line between start of wash out and end of measurement),
- PEI, and
- iAUC (in 60 s).
4.3. Histopathology
4.4. CADx Development, Statistics, and Open-Access Internet Application
4.4.1. CADx Development
4.4.2. Statistics
4.4.3. Open-Access Internet Application
5. Conclusions
Author Contributions
Funding
Acknowledgments
Conflicts of Interest
Appendix A

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Parameter | Value |
|---|---|
| subsample | 0.63 |
| nrounds | 121 |
| eta | 0.34 |
| gamma | 0.2 |
| max_depth | 8 |
| min_child_weight | 1.3 |
| colsample_bytree | 0.76 |
| rate_drop | 0.49 |
| skip_drop | 0.88 |
References
- Bray, F.; Ferlay, J.; Soerjomataram, I.; Siegel, R.L.; Torre, L.A.; Jemal, A. Global cancer statistics 2018: GLOBOCAN estimates of incidence and mortality worldwide for 36 cancers in 185 countries. CA Cancer J. Clin. 2018, 68, 394–424. [Google Scholar] [CrossRef]
- Hoeks, C.M.A.; Barentsz, J.O.; Hambrock, T.; Yakar, D.; Somford, D.M.; Heijmink, S.W.T.P.J.; Scheenen, T.W.J.; Vos, P.C.; Huisman, H.; van Oort, I.M.; et al. Prostate cancer: Multiparametric MR imaging for detection, localization, and staging. Radiology 2011, 261, 46–66. [Google Scholar] [CrossRef]
- EAU Guidelines: Prostate Cancer | Uroweb. Available online: https://uroweb.org/guideline/prostate-cancer/ (accessed on 28 July 2020).
- Litjens, G.; Debats, O.; Barentsz, J.; Karssemeijer, N.; Huisman, H. Computer-aided detection of prostate cancer in MRI. IEEE Trans. Med. Imag. 2014, 33, 1083–1092. [Google Scholar] [CrossRef]
- Weinreb, J.C.; Barentsz, J.O.; Choyke, P.L.; Cornud, F.; Haider, M.A.; Macura, K.J.; Margolis, D.; Schnall, M.D.; Shtern, F.; Tempany, C.M.; et al. PI-RADS Prostate Imaging—Reporting and Data System: 2015, Version 2. Eur. Urol. 2016, 69, 16–40. [Google Scholar] [CrossRef] [PubMed]
- Turkbey, B.; Rosenkrantz, A.B.; Haider, M.A.; Padhani, A.R.; Villeirs, G.; Macura, K.J.; Tempany, C.M.; Choyke, P.L.; Cornud, F.; Margolis, D.J.; et al. Prostate Imaging Reporting and Data System Version 2.1: 2019 Update of Prostate Imaging Reporting and Data System Version 2. Eur. Urol. 2019, 76, 340–351. [Google Scholar] [CrossRef] [PubMed]
- Woo, S.; Suh, C.H.; Kim, S.Y.; Cho, J.Y.; Kim, S.H. Diagnostic Performance of Prostate Imaging Reporting and Data System Version 2 for Detection of Prostate Cancer: A Systematic Review and Diagnostic Meta-analysis. Eur. Urol. 2017, 72, 177–188. [Google Scholar] [CrossRef] [PubMed]
- Zhang, L.; Tang, M.; Chen, S.; Lei, X.; Zhang, X.; Huan, Y. A meta-analysis of use of Prostate Imaging Reporting and Data System Version 2 (PI-RADS V2) with multiparametric MR imaging for the detection of prostate cancer. Eur. Radiol. 2017, 27, 5204–5214. [Google Scholar] [CrossRef] [PubMed]
- Rosenkrantz, A.B.; Ginocchio, L.A.; Cornfeld, D.; Froemming, A.T.; Gupta, R.T.; Turkbey, B.; Westphalen, A.C.; Babb, J.S.; Margolis, D.J. Interobserver Reproducibility of the PI-RADS Version 2 Lexicon: A Multicenter Study of Six Experienced Prostate Radiologists. Radiology 2016, 280, 793–804. [Google Scholar] [CrossRef]
- Fei, B. Computer-aided diagnosis of prostate cancer with MRI. Curr. Opin. Biomed. Eng. 2017, 3, 20–27. [Google Scholar] [CrossRef]
- Lemaître, G.; Martí, R.; Freixenet, J.; Vilanova, J.C.; Walker, P.M.; Meriaudeau, F. Computer-Aided Detection and diagnosis for prostate cancer based on mono and multi-parametric MRI: A review. Comput. Biol. Med. 2015, 60, 8–31. [Google Scholar] [CrossRef]
- Wang, S.; Burtt, K.; Turkbey, B.; Choyke, P.; Summers, R.M. Computer aided-diagnosis of prostate cancer on multiparametric MRI: A technical review of current research. BioMed Res. Int. 2014, 2014. [Google Scholar] [CrossRef] [PubMed]
- Langer, D.L.; van der Kwast, T.H.; Evans, A.J.; Trachtenberg, J.; Wilson, B.C.; Haider, M.A. Prostate cancer detection with multi-parametric MRI: Logistic regression analysis of quantitative T2, diffusion-weighted imaging, and dynamic contrast-enhanced MRI. J. Magn. Reson. Imaging 2009, 30, 327–334. [Google Scholar] [CrossRef] [PubMed]
- Lv, D.; Guo, X.; Wang, X.; Zhang, J.; Fang, J. Computerized characterization of prostate cancer by fractal analysis in MR images. J. Magn. Reson. Imaging 2009, 30, 161–168. [Google Scholar] [CrossRef] [PubMed]
- Viswanath, S.; Bloch, B.N.; Chappelow, J.; Patel, P.; Rofsky, N.; Lenkinski, R.; Genega, E.; Madabhushi, A. Enhanced multi-protocol analysis via intelligent supervised embedding (EMPrAvISE): Detecting prostate cancer on multi-parametric MRI. In Proceedings of the Medical Imaging 2011: Computer-Aided Diagnosis, SPIE Medical Imaging, Lake Buena Vista, FL, USA, 17 February 2011. [Google Scholar]
- Peng, Y.; Jiang, Y.; Yang, C.; Brown, J.B.; Antic, T.; Sethi, I.; Schmid-Tannwald, C.; Giger, M.L.; Eggener, S.E.; Oto, A. Quantitative analysis of multiparametric prostate MR images: Differentiation between prostate cancer and normal tissue and correlation with Gleason score—A computer-aided diagnosis development study. Radiology 2013, 267, 787–796. [Google Scholar] [CrossRef] [PubMed]
- Tamada, T.; Kido, A.; Takeuchi, M.; Yamamoto, A.; Miyaji, Y.; Kanomata, N.; Sone, T. Comparison of PI-RADS version 2 and PI-RADS version 2.1 for the detection of transition zone prostate cancer. Eur. J. Radiol. 2019, 121. [Google Scholar] [CrossRef] [PubMed]
- Smith, C.P.; Türkbey, B. PI-RADS v2: Current standing and future outlook. Turk. J. Urol. 2018, 44, 189–194. [Google Scholar] [CrossRef]
- Wei, C.; Zhang, Y.; Pan, P.; Chen, T.; Yu, H.; Dai, G.; Tu, J.; Yang, S.; Zhao, W.; Shen, J. Diagnostic Accuracy and Inter-observer Agreement of PI-RADS Version 2 and Version 2.1 for the Detection of Transition Zone Prostate Cancers. Am. J. Roentgenol. 2020. [Google Scholar] [CrossRef]
- Siddiqui, M.M.; Rais-Bahrami, S.; Turkbey, B.; George, A.K.; Rothwax, J.; Shakir, N.; Okoro, C.; Raskolnikov, D.; Parnes, H.L.; Linehan, W.M.; et al. Comparison of MR/ultrasound fusion-guided biopsy with ultrasound-guided biopsy for the diagnosis of prostate cancer. J. Am. Med. Assoc. 2015, 313, 390–397. [Google Scholar] [CrossRef]
- Rouvière, O.; Puech, P.; Renard-Penna, R.; Claudon, M.; Roy, C.; Mège-Lechevallier, F.; Decaussin-Petrucci, M.; Dubreuil-Chambardel, M.; Magaud, L.; Remontet, L.; et al. Use of prostate systematic and targeted biopsy on the basis of multiparametric MRI in biopsy-naive patients (MRI-FIRST): A prospective, multicentre, paired diagnostic study. Lancet Oncol. 2019, 20, 100–109. [Google Scholar] [CrossRef]
- Matoso, A.; Epstein, J.I. Defining clinically significant prostate cancer on the basis of pathological findings. Histopathology 2019, 74, 135–145. [Google Scholar] [CrossRef]
- Niaf, E.; Rouvière, O.; Mège-Lechevallier, F.; Bratan, F.; Lartizien, C. Computer-aided diagnosis of prostate cancer in the peripheral zone using multiparametric MRI. Phys. Med. Biol. 2012, 57, 3833–3851. [Google Scholar] [CrossRef] [PubMed]
- Kwak, J.T.; Sankineni, S.; Xu, S.; Turkbey, B.; Choyke, P.L.; Pinto, P.A.; Merino, M.; Wood, B.J. Correlation of magnetic resonance imaging with digital histopathology in prostate. Int. J. Comput. Assist. Radiol. Surg. 2016, 11, 657–666. [Google Scholar] [CrossRef]
- Ellmann, S.; Seyler, L.; Evers, J.; Heinen, H.; Bozec, A.; Prante, O.; Kuwert, T.; Uder, M.; Bäuerle, T. Prediction of early metastatic disease in experimental breast cancer bone metastasis by combining PET/CT and MRI parameters to a Model-Averaged Neural Network. Bone 2019, 120, 254–261. [Google Scholar] [CrossRef] [PubMed]
- Vos, E.K.; Litjens, G.J.S.; Kobus, T.; Hambrock, T.; de Kaa, C.A.H.; Barentsz, J.O.; Huisman, H.J.; Scheenen, T.W.J. Assessment of Prostate Cancer Aggressiveness Using Dynamic Contrast-enhanced Magnetic Resonance Imaging at 3 T. Eur. Urol. 2013, 64, 448–455. [Google Scholar] [CrossRef]
- Hegde, J.V.; Mulkern, R.V.; Panych, L.P.; Fennessy, F.M.; Fedorov, A.; Maier, S.E.; Tempany, C.M.C. Multiparametric MRI of prostate cancer: An update on state-of-the-art techniques and their performance in detecting and localizing prostate cancer. J. Magn. Reson. Imaging 2013, 37, 1035–1054. [Google Scholar] [CrossRef]
- Park, D.S.; Oh, J.J.; Hong, J.Y.; Hong, Y.K.; Choi, D.K.; Gong, I.H.; Hwang, J.H.; Kwon, S.W. Serum prostate-specific antigen as a predictor of prostate volume and lower urinary tract symptoms in a community-based cohort: A large-scale Korean screening study. Asian J. Androl. 2013, 15, 249–253. [Google Scholar] [CrossRef] [PubMed]
- Schoots, I.G.; Osses, D.F.; Drost, F.-J.H.; Verbeek, J.F.M.; Remmers, S.; van Leenders, G.J.L.H.; Bangma, C.H.; Roobol, M.J. Reduction of MRI-targeted biopsies in men with low-risk prostate cancer on active surveillance by stratifying to PI-RADS and PSA-density, with different thresholds for significant disease. Transl. Androl. Urol. 2018, 7, 132–144. [Google Scholar] [CrossRef]
- Barentsz, J.O.; Weinreb, J.C.; Verma, S.; Thoeny, H.C.; Tempany, C.M.; Shtern, F.; Padhani, A.R.; Margolis, D.; Macura, K.J.; Haider, M.A.; et al. Synopsis of the PI-RADS v2 Guidelines for Multiparametric Prostate Magnetic Resonance Imaging and Recommendations for Use. Eur. Urol. 2016, 69, 41–49. [Google Scholar] [CrossRef]
- Tofts, P. T1-weighted DCE Imaging Concepts: Modelling, Acquisition and Analysis. Available online: http://www.paul-tofts-phd.org.uk/DCE-MRI_siemens.pdf (accessed on 1 August 2020).
- Kuhn, M. CRAN—Pakage Caret. Available online: https://cran.r-project.org/web/packages/caret/index.html (accessed on 15 March 2017).
- Chen, T.; He, T.; Benesty, M.; Khotilovich, V.; Tang, Y.; Cho, H.; Chen, K.; Mitchell, R.; Cano, I.; Zhou, T.; et al. CRAN: Package xgboost—Extreme Gradient Boosting. Available online: https://cran.r-project.org/web/packages/xgboost/ (accessed on 16 July 2019).
- Cicchetti, D.V. Guidelines, criteria, and rules of thumb for evaluating normed and standardized assessment instruments in psychology. Psychol. Assess. 1994, 6, 284–290. [Google Scholar] [CrossRef]
- Dietzel, M.; Baltzer, P.A.T. How to use the Kaiser score as a clinical decision rule for diagnosis in multiparametric breast MRI: A pictorial essay. Insights Imaging 2018, 9, 325–335. [Google Scholar] [CrossRef]
- Baltzer, P.A.T.; Dietzel, M.; Kaiser, W.A. A simple and robust classification tree for differentiation between benign and malignant lesions in MR-mammography. Eur. Radiol. 2013, 23, 2051–2060. [Google Scholar] [CrossRef] [PubMed]
- Bruno, P. The importance of diagnostic test parameters in the interpretation of clinical test findings: The Prone Hip Extension Test as an example. J. Can. Chiropr. Assoc. 2011, 55, 69–75. [Google Scholar] [PubMed]
- Chang, W.; Cheng, J.; Allaire, J.; Xie, Y.; McPherson, J. Web Application Framework for R [R Package Shiny Version 1.0.0]. Available online: https://cran.r-project.org/web/packages/shiny/index.html (accessed on 15 March 2017).






| Parameter | Training Set | Testing Set | p-Value | ||
|---|---|---|---|---|---|
| Median | Range | Median | Range | ||
| Patient age [years] | 67 | 46–84 | 66 | 53–79 | 0.79 |
| Prostate volume [mL] | 46.0 | 15.6–180.8 | 41.8 | 22.5–173.5 | 0.29 |
| PSA [ng/mL] | 8.46 | 2.91–129 | 8.00 | 2.3–40 | 0.38 |
| T2w SI [A.U.] | 3.39 | 1.31–6.22 | 3.61 | 2.65–6.34 | 0.24 |
| ADC [10–6 mm2/s] | 1032.5 | 542–2267 | 1067 | 621–2151 | 0.76 |
| Long diameter [mm] | 12 | 4–45 | 13 | 4–28 | 0.51 |
| Short diameter [mm] | 9 | 4–32 | 8 | 2–24 | 0.60 |
| Wash in [mmol/min] | 0.419 | 0.032–1.423 | 0.483 | 0.07–0.926 | 0.51 |
| Wash out [mmol/min] | −0.009 | −0.087–0.048 | −0.017 | −0.059–0.021 | 0.29 |
| TTP [min] | 0.653 | 0.249–3.496 | 0.638 | 0.452–1.257 | 0.85 |
| AT [min] | 0.472 | 0–1.1 | 0.384 | 0–0.943 | 0.81 |
| PEI [mmol] | 0.326 | 0.079–0.809 | 0.360 | 0.109–0.598 | 0.45 |
| iAUC [mmol·min] | 0.230 | 0.035–0.912 | 0.261 | 0.04–0.472 | 0.68 |
| Gleason Score (PCa only) | 7 | 6–9 | 7 | 6–9 | 0.89 |
| Histopathology | PCa: n = 67; Benign: n = 89 | PCa: n = 16; Benign: n = 23 | 0.86 | ||
| Zone | PZ: n = 76; CG: n = 80 | PZ: n = 21; CG: n = 18 | 0.60 | ||
| Parameter | ICC | 95% CI |
|---|---|---|
| T2w SI | 0.88 | 0.78–0.93 |
| ADC | 0.87 | 0.72–0.94 |
| Long diameter | 0.87 | 0.76–0.93 |
| Short diameter | 0.90 | 0.80–0.95 |
| Wash in | 0.88 | 0.78–0.93 |
| Wash out | 0.93 | 0.88–0.96 |
| TTP | 0.93 | 0.88–0.96 |
| PEI | 0.88 | 0.79–0.94 |
| iAUC | 0.90 | 0.81–0.94 |
| Volume | 0.93 | 0.84–0.97 |
| Parameter | Training Set | Testing Set | p-Value | ||
|---|---|---|---|---|---|
| Estimation | 95% CI | Estimation | 95% CI | ||
| Sensitivity | 82.1% | 0.708–0.904% | 81.2% | 54.4–96.0% | 0.937 |
| Specificity | 85.4% | 0.763–0.92% | 82.6% | 61.2–95.0% | 0.759 |
| PPV | 80.9% | 0.695–0.894% | 76.5% | 50.1–93.2% | 0.703 |
| NPV | 86.4% | 0.774–0.928% | 86.4% | 65.1–97.1% | 1.000 |
| Accuracy | 84.0% | 0.773–0.894% | 82.1% | 66.5–92.5% | 0.787 |
| Positive Likelihood Ratio | 5.62 | 3.36–9.40 | 4.67 | 1.86–11.7 | 0.776 |
| Negative Likelihood Ratio | 0.21 | 0.13–0.35 | 0.23 | 0.08–0.64 | 0.901 |
| Error Rate | Rule In | Rule Out |
|---|---|---|
| <1% | 13/67 (19.4%) | 43/89 (48.3%) |
| <2% | 24/67 (35.8%) | 44/89 (49.4%) |
| <3% | 24/67 (35.8%) | 56/89 (62.9%) |
| <4% | 28/67 (41.8%) | 58/89 (65.2%) |
| <5% | 34/67 (50.7%) | 60/89 (67.4%) |
| Parameter | 1.5 T | 3 T | ||||||
|---|---|---|---|---|---|---|---|---|
| T2w TSE | DCE (VIBE) | T1w TSE | DWI | T2w TSE | DCE (VIBE) | T1w TSE | DWI | |
| TR [ms] | 7440 | 4.2 | 433 | 5300 | 4000 | 5.04 | 688 | 5090 |
| TE [ms] | 101 | 1.58 | 10 | 70 | 101 | 1.7 | 12 | 57 |
| ETL | 23 | 1 | 3 | 25 | 1 | 3 | ||
| Flip angle [°] | 160 | 12 | 154 | 18 | 150 | 15 | 140 | 180 |
| Field of view [mm2] | 200 × 200 | 259 × 259 | 200 × 200 | 200 × 200 | 200 × 200 | 200 × 200 | 308 × 380 | 200 × 200 |
| Matrix | 320 × 275 | 192 × 154 | 256 × 192 | 112 × 112 | 320 × 310 | 128 × 102 | 333 × 512 | 94 × 118 |
| Slice thickness [mm] | 3 | 3.5 | 3 | 3.5 | 3 | 3 | 5 | 3.5 |
| Number of slices | 28 | 22 | 28 | 20 | 26 | 24 | 40 | 25 |
| Averages | 3 | 1 | 1 | 1 | 3 | 1 | 1 | 1 |
| Duration [min:s] | 04:20 | 04:21 | 02:45 | 07:06 | 03:52 | 04:34 | 03:29 | 06:03 |
© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Ellmann, S.; Schlicht, M.; Dietzel, M.; Janka, R.; Hammon, M.; Saake, M.; Ganslandt, T.; Hartmann, A.; Kunath, F.; Wullich, B.; et al. Computer-Aided Diagnosis in Multiparametric MRI of the Prostate: An Open-Access Online Tool for Lesion Classification with High Accuracy. Cancers 2020, 12, 2366. https://doi.org/10.3390/cancers12092366
Ellmann S, Schlicht M, Dietzel M, Janka R, Hammon M, Saake M, Ganslandt T, Hartmann A, Kunath F, Wullich B, et al. Computer-Aided Diagnosis in Multiparametric MRI of the Prostate: An Open-Access Online Tool for Lesion Classification with High Accuracy. Cancers. 2020; 12(9):2366. https://doi.org/10.3390/cancers12092366
Chicago/Turabian StyleEllmann, Stephan, Michael Schlicht, Matthias Dietzel, Rolf Janka, Matthias Hammon, Marc Saake, Thomas Ganslandt, Arndt Hartmann, Frank Kunath, Bernd Wullich, and et al. 2020. "Computer-Aided Diagnosis in Multiparametric MRI of the Prostate: An Open-Access Online Tool for Lesion Classification with High Accuracy" Cancers 12, no. 9: 2366. https://doi.org/10.3390/cancers12092366
APA StyleEllmann, S., Schlicht, M., Dietzel, M., Janka, R., Hammon, M., Saake, M., Ganslandt, T., Hartmann, A., Kunath, F., Wullich, B., Uder, M., & Bäuerle, T. (2020). Computer-Aided Diagnosis in Multiparametric MRI of the Prostate: An Open-Access Online Tool for Lesion Classification with High Accuracy. Cancers, 12(9), 2366. https://doi.org/10.3390/cancers12092366