Surgery for Unresectable Stage IIIC and IV Melanoma in the Era of New Systemic Therapy

 ,
, 
 ,
,  , ,
, ,  and
and
Abstract
1. Introduction
2. Patients and Methods
2.1. Patients
2.2. Statistical Analysis
3. Results
3.1. Patient and Tumor Characteristics
3.2. Treatment
3.3. Response
3.3.1. Best Response
3.3.2. Most Recent Disease Status Prior to Surgery
3.3.3. First Evaluation after Surgery
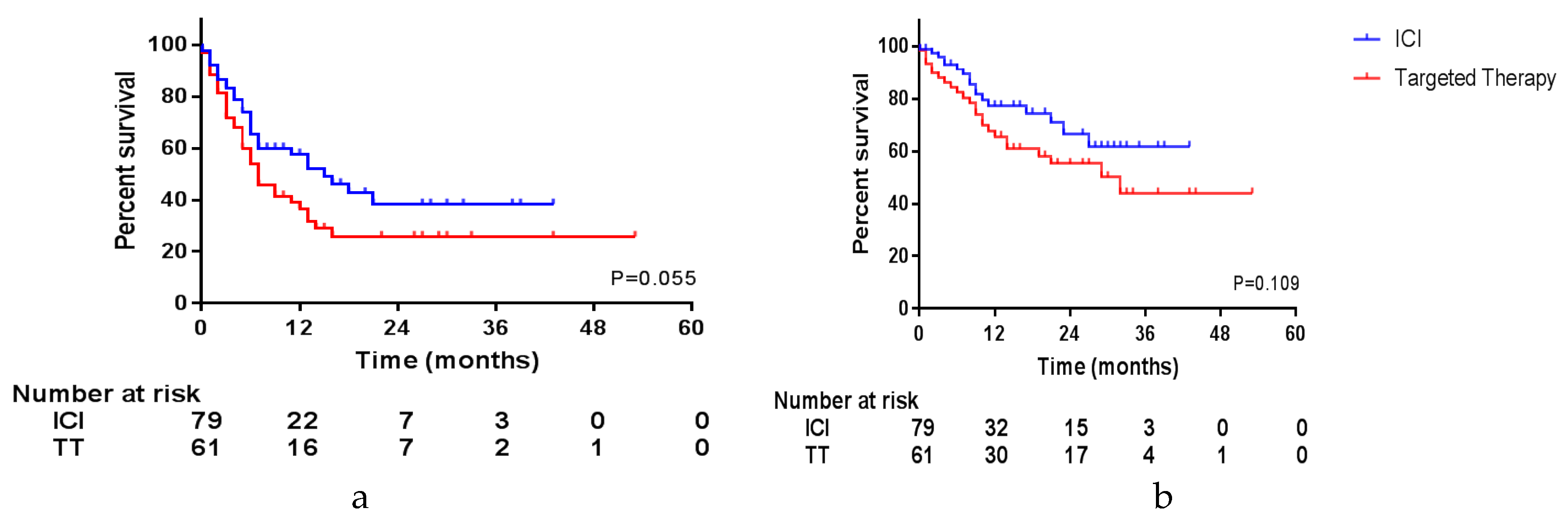
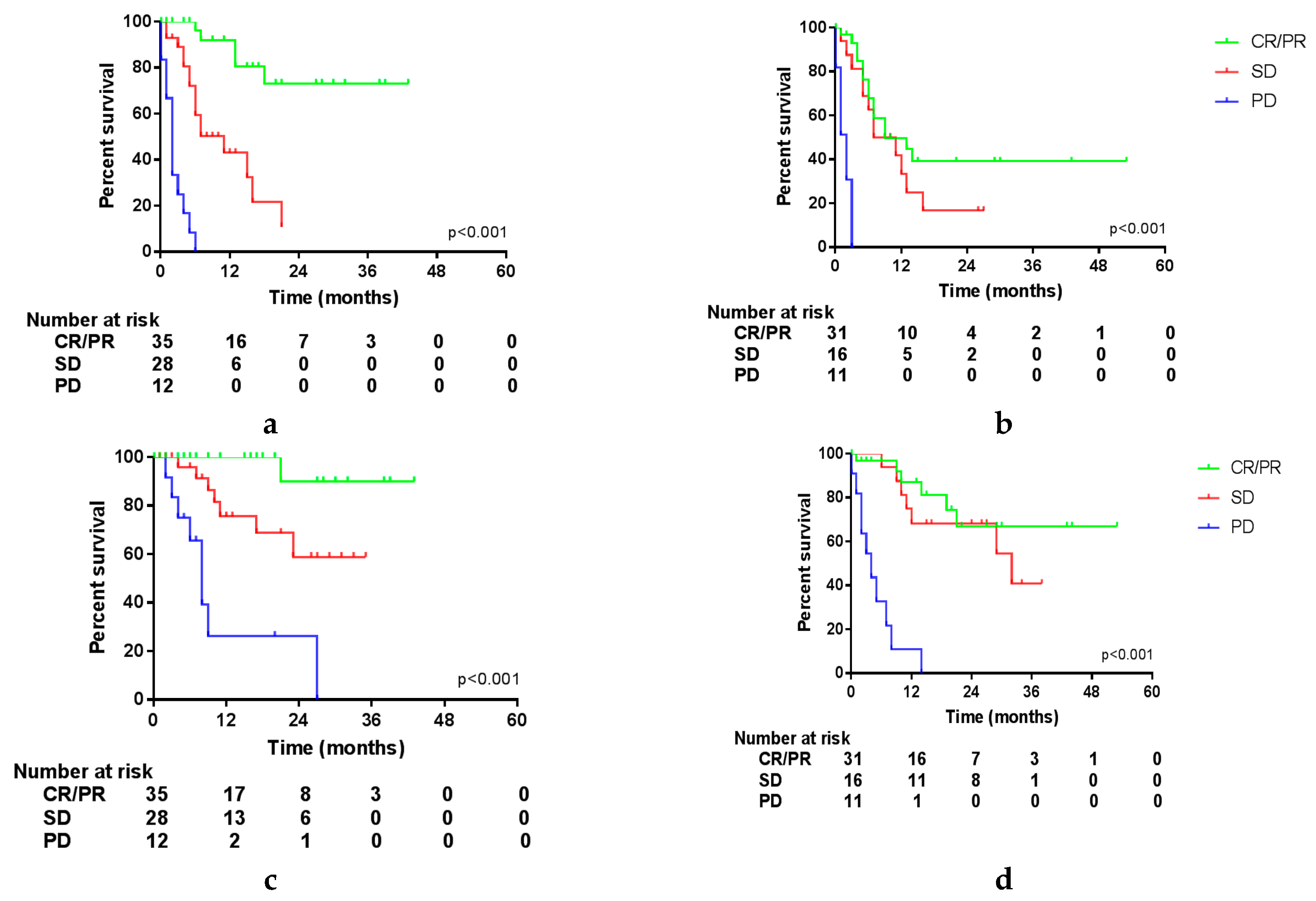
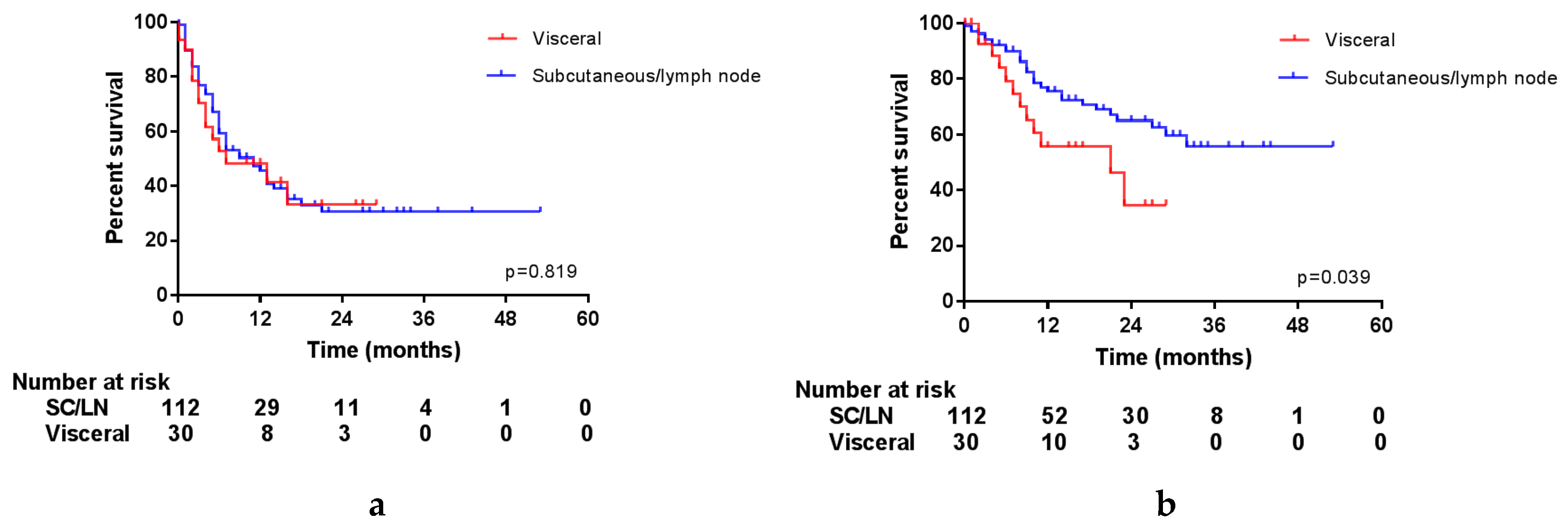
3.4. Survival Outcomes
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Acknowledgments
Conflicts of Interest
References
- Korn, E.L.; Liu, P.-Y.; Lee, S.J.; Chapman, J.-A.W.; Niedzwiecki, D.; Suman, V.J.; Moon, J.; Sondak, V.K.; Atkins, M.B.; Eisenhauer, E.A.; et al. Meta-analysis of phase II cooperative group trials in metastatic stage IV melanoma to determine progression-free and overall survival benchmarks for future phase II trials. J. Clin. Oncol. 2008, 26, 527–534. [Google Scholar] [CrossRef] [PubMed]
- Svedman, F.C.; Pillas, D.; Taylor, A.; Kaur, M.; Linder, R.; Hansson, J. Stage-specific survival and recurrence in patients with cutaneous malignant melanoma in Europe—A systematic review of the literature. Clin. Epidemiol. 2016, 8, 109–122. [Google Scholar] [CrossRef] [PubMed]
- Sosman, J.A.; Moon, J.; Tuthill, R.J.; Warneke, J.A.; Vetto, J.T.; Redman, B.G.; Liu, P.Y.; Unger, J.M.; Flaherty, L.E.; Sondak, V.K. A phase 2 trial of complete resection for stage IV melanoma: Results of Southwest Oncology Group Clinical Trial S9430. Cancer 2011, 117, 4740–4806. [Google Scholar] [CrossRef] [PubMed]
- Howard, J.H.; Thompson, J.F.; Mozzillo, N.; Nieweg, O.E.; Hoekstra, H.J.; Roses, D.F.; Sondak, V.K.; Reintgen, D.S.; Kashani-Sabet, M.; Karakousis, C.P.; et al. Metastasectomy for distant metastatic melanoma: Analysis of data from the first Multicenter Selective Lymphadenectomy Trial (MSLT-I). Ann. Surg. Oncol. 2012, 19, 2547–2555. [Google Scholar] [CrossRef] [PubMed]
- Ascierto, P.A.; Long, G.V.; Robert, C.; Brady, B.; Dutriaux, C.; Di Giacomo, A.M.; Mortier, L.; Hassel, J.C.; Rutkowski, P.; McNeil, C.; et al. Survival outcomes in patients with previously untreated BRAF wild-type advanced melanoma treated with nivolumab therapy: Three-year follow-up of a randomized phase 3 trial. JAMA Oncol. 2018. [Google Scholar] [CrossRef] [PubMed]
- Robert, C.; Long, G.V.; Brady, B.; Dutriaux, C.; Maio, M.; Mortier, L.; Hassel, J.C.; Rutkowski, P.; McNeil, C.; Kalinka-Warzocha, E.; et al. Nivolumab in previously untreated melanoma without BRAF mutation. N. Engl. J. Med. 2015, 372, 320–330. [Google Scholar] [CrossRef]
- Topalian, S.L.; Sznol, M.; McDermott, D.F.; Kluger, H.M.; Carvajal, R.D.; Sharfman, W.H.; Brahmer, J.R.; Lawrence, D.P.; Atkins, M.B.; Powderly, J.D.; et al. Survival, durable tumor remission, and long-term safety in patients with advanced melanoma receiving nivolumab. J. Clin. Oncol. 2014, 32, 1020–1030. [Google Scholar] [CrossRef]
- Weber, J.S.; D’Angelo, S.P.; Minor, D.; Hodi, F.S.; Gutzmer, R.; Neyns, B.; Hoeller, C.; Khushalani, N.I.; Miller, W.H., Jr.; Lao, C.D.; et al. Nivolumab versus chemotherapy in patients with advanced melanoma who progressed after anti-CTLA-4 treatment (CheckMate 037): A randomised, controlled, open-label, phase 3 trial. Lancet. Oncol. 2015, 16, 375–384. [Google Scholar] [CrossRef]
- Schachter, J.; Ribas, A.; Long, G.V.; Arance, A.; Grob, J.J.; Mortier, L.; Daud, A.; Carlino, M.S.; McNeil, C.; Lotem, M.; et al. Pembrolizumab versus ipilimumab for advanced melanoma: Final overall survival results of a multicentre, randomised, open-label phase 3 study (KEYNOTE-006). Lancet (Lond. Engl.) 2017, 390, 1853–1862. [Google Scholar] [CrossRef]
- Ascierto, P.A.; Del Vecchio, M.; Robert, C.; Mackiewicz, A.; Chiarion-Sileni, V.; Arance, A.; Lebbe, C.; Bastholt, L.; Hamid, O.; Rutkowski, P.; et al. Ipilimumab 10 mg/kg versus ipilimumab 3 mg/kg in patients with unresectable or metastatic melanoma: A randomised, double-blind, multicentre, phase 3 trial. Lancet. Oncol. 2017, 18, 611–622. [Google Scholar] [CrossRef]
- Hodi, F.S.; O’Day, S.J.; McDermott, D.F.; Weber, R.W.; Sosman, J.A.; Haanen, J.B.; Gonzalez, R.; Robert, C.; Schadendorf, D.; Hassel, J.C.; et al. Improved survival with ipilimumab in patients with metastatic melanoma. N. Engl. J. Med. 2010, 363, 711–723. [Google Scholar] [CrossRef] [PubMed]
- Robert, C.; Thomas, L.; Bondarenko, I.; O’Day, S.; Weber, J.; Garbe, C.; Lebbe, C.; Baurain, J.F.; Testori, A.; Grob, J.J.; et al. Ipilimumab plus dacarbazine for previously untreated metastatic melanoma. N. Engl. J. Med. 2011, 364, 2517–2526. [Google Scholar] [CrossRef]
- Hodi, F.S.; Chiarion-Sileni, V.; Gonzalez, R.; Grob, J.J.; Rutkowski, P.; Cowey, C.L.; Lao, C.D.; Schadendorf, D.; Wagstaff, J.; Dummer, R.; et al. Nivolumab plus ipilimumab or nivolumab alone versus ipilimumab alone in advanced melanoma (CheckMate 067): 4-year outcomes of a multicentre, randomised, phase 3 trial. Lancet Oncol. 2018, 19, 1480–1492. [Google Scholar] [CrossRef]
- Hodi, F.S.; Chesney, J.; Pavlick, A.C.; Robert, C.; Grossmann, K.F.; McDermott, D.F.; Linette, G.P.; Meyer, N.; Giguere, J.K.; Agarwala, S.S.; et al. Combined nivolumab and ipilimumab versus ipilimumab alone in patients with advanced melanoma: 2-year overall survival outcomes in a multicentre, randomised, controlled, phase 2 trial. Lancet Oncol. 2016, 17, 1558–1568. [Google Scholar] [CrossRef]
- Larkin, J.; Chiarion-Sileni, V.; Gonzalez, R.; Grob, J.J.; Cowey, C.L.; Lao, C.D.; Schadendorf, D.; Dummer, R.; Smylie, M.; Rutkowski, P.; et al. Combined nivolumab and ipilimumab or monotherapy in untreated melanoma. N. Engl. J. Med. 2015, 373, 23–34. [Google Scholar] [CrossRef]
- Postow, M.A.; Chesney, J.; Pavlick, A.C.; Robert, C.; Grossmann, K.; McDermott, D.; Linette, G.P.; Meyer, N.; Giguere, J.K.; Agarwala, S.S.; et al. Nivolumab and ipilimumab versus ipilimumab in untreated melanoma. N. Engl. J. Med. 2015, 372, 2006–2017. [Google Scholar] [CrossRef]
- Wolchok, J.D.; Chiarion-Sileni, V.; Gonzalez, R.; Rutkowski, P.; Grob, J.J.; Cowey, C.L.; Lao, C.D.; Wagstaff, J.; Schadendorf, D.; Ferrucci, P.F.; et al. Overall survival with combined nivolumab and ipilimumab in advanced melanoma. N. Engl. J. Med. 2017, 377, 1345–1356. [Google Scholar] [CrossRef]
- Wolchok, J.D.; Kluger, H.; Callahan, M.K.; Postow, M.A.; Rizvi, N.A.; Lesokhin, A.M.; Segal, N.H.; Ariyan, C.E.; Gordon, R.A.; Reed, K.; et al. Nivolumab plus ipilimumab in advanced melanoma. N. Engl. J. Med. 2013, 369, 122–133. [Google Scholar] [CrossRef]
- Dummer, R.; Ascierto, P.A.; Gogas, H.J.; Arance, A.; Mandala, M.; Liszkay, G.; Garbe, C.; Schadendorf, D.; Krajsova, I.; Gutzmer, R.; et al. Overall survival in patients with BRAF-mutant melanoma receiving encorafenib plus binimetinib versus vemurafenib or encorafenib (COLUMBUS): A multicentre, open-label, randomised, phase 3 trial. Lancet Oncol. 2018, 19, 1315–1327. [Google Scholar] [CrossRef]
- Dummer, R.; Ascierto, P.A.; Gogas, H.J.; Arance, A.; Mandala, M.; Liszkay, G.; Garbe, C.; Schadendorf, D.; Krajsova, I.; Gutzmer, R.; et al. Encorafenib plus binimetinib versus vemurafenib or encorafenib in patients with BRAF-mutant melanoma (COLUMBUS): A multicentre, open-label, randomised phase 3 trial. Lancet Oncol. 2018, 19, 603–615. [Google Scholar] [CrossRef]
- Larkin, J.; Ascierto, P.A.; Dreno, B.; Atkinson, V.; Liszkay, G.; Maio, M.; Mandala, M.; Demidov, L.; Stroyakovskiy, D.; Thomas, L.; et al. Combined vemurafenib and cobimetinib in BRAF-mutated melanoma. N. Engl. J. Med. 2014, 371, 1867–1876. [Google Scholar] [CrossRef] [PubMed]
- Long, G.V.; Flaherty, K.T.; Stroyakovskiy, D.; Gogas, H.; Levchenko, E.; de Braud, F.; Larkin, J.; Garbe, C.; Jouary, T.; Hauschild, A.; et al. Dabrafenib plus trametinib versus dabrafenib monotherapy in patients with metastatic BRAF V600E/K-mutant melanoma: Long-term survival and safety analysis of a phase 3 study. Ann. Oncol. 2017, 28, 1631–1639. [Google Scholar] [CrossRef] [PubMed]
- Long, G.V.; Stroyakovskiy, D.; Gogas, H.; Levchenko, E.; de Braud, F.; Larkin, J.; Garbe, C.; Jouary, T.; Hauschild, A.; Grob, J.J.; et al. Combined BRAF and MEK inhibition versus BRAF inhibition alone in melanoma. N. Engl. J. Med. 2014, 371, 1877–1888. [Google Scholar] [CrossRef] [PubMed]
- Long, G.V.; Stroyakovskiy, D.; Gogas, H.; Levchenko, E.; de Braud, F.; Larkin, J.; Garbe, C.; Jouary, T.; Hauschild, A.; Grob, J.J.; et al. Dabrafenib and trametinib versus dabrafenib and placebo for Val600 BRAF-mutant melanoma: A multicentre, double-blind, phase 3 randomised controlled trial. Lancet 2015, 386, 444–451. [Google Scholar] [CrossRef]
- Robert, C.; Karaszewska, B.; Schachter, J.; Rutkowski, P.; Mackiewicz, A.; Stroiakovski, D.; Lichinitser, M.; Dummer, R.; Grange, F.; Mortier, L.; et al. Improved overall survival in melanoma with combined dabrafenib and trametinib. N. Engl. J. Med. 2015, 372, 30–39. [Google Scholar] [CrossRef]
- Jochems, A.; Schouwenburg, M.G.; Leeneman, B.; Franken, M.G.; van den Eertwegh, A.J.; Haanen, J.B.; Gelderblom, H.; Uyl-de Groot, C.A.; Aarts, M.J.; van den Berkmortel, F.W.; et al. Dutch Melanoma Treatment Registry: Quality assurance in the care of patients with metastatic melanoma in the Netherlands. Eur. J. Cancer 2017, 72, 156–165. [Google Scholar] [CrossRef]
- Balch, C.M.; Gershenwald, J.E.; Soong, S.J.; Thompson, J.F.; Atkins, M.B.; Byrd, D.R.; Buzaid, A.C.; Cochran, A.J.; Coit, D.G.; Ding, S.; et al. Final version of 2009 AJCC melanoma staging and classification. J. Clin. Oncol. 2009, 27, 6199–6206. [Google Scholar] [CrossRef]
- Bello, D.M.; Panageas, K.S.; Hollmann, T.; Shoushtari, A.N.; Momtaz, P.; Chapman, P.B.; Postow, M.A.; Callahan, M.K.; Wolchok, J.D.; Brady, M.S.; et al. Survival outcomes after metastasectomy in melanoma patients categorized by response to checkpoint blockade. Ann. Surg. Oncol. 2019. [Google Scholar] [CrossRef]
- Klemen, N.D.; Wang, M.; Feingold, P.L.; Cooper, K.; Pavri, S.N.; Han, D.; Detterbeck, F.C.; Boffa, D.J.; Khan, S.A.; Olino, K.; et al. Patterns of failure after immunotherapy with checkpoint inhibitors predict durable progression-free survival after local therapy for metastatic melanoma. J. Immunother. Cancer 2019, 7, 196. [Google Scholar] [CrossRef]
- Tan, A.C.; Emmett, L.; Lo, S.; Liu, V.; Guminski, A.D.; Long, G.V.; Menzies, A.M. Utility of 1-year FDG-PET (PET) to determine outcomes from anti-PD-1 (PD1) based therapy in patients (pts) with metastatic melanoma (MM). J. Clin. Oncol. 2018, 36, 9517. [Google Scholar] [CrossRef]




{kind=link}
{kind=link}
{kind=link}
| Characteristic | Total (n = 154) n (%) | ICI (n = 79) n (%) | TT (n = 61) n (%) | p1 |
|---|---|---|---|---|
| Age, years | 0.452 | |||
| Median | 58 | 62 | 59 | |
| Range | 24–87 | 24–80 | 34–87 | |
| Sex | 0.444 | |||
| Female | 74 (48.1) | 35 (44.3) | 31 (50.8) | |
| Male | 80 (51.9) | 44 (55.7) | 30 (49.2) | |
| WHO performance status | 0.543 | |||
| 0 | 101 (65.6) | 52 (65.8) | 38 (62.3) | |
| 1 | 40 (26.0) | 21 (26.6) | 16 (26.2) | |
| 2 | 4 (2.6) | 3 (3.8) | 1 (1.6) | |
| 3 | 1 (0.6) | 0 (0.0) | 1 (1.6) | |
| Unknown | 8 (5.2) | 3 (3.8) | 5 (8.2) | |
| Location primary | 0.431 | |||
| Extremity | 61 (39.6) | 32 (40.5) | 23 (37.7) | |
| Trunk | 45 (29.2) | 20 (25.3) | 20 (32.8) | |
| Head/Neck | 10 (6.5) | 4 (5.1) | 6 (9.8) | |
| Acral | 9 (5.8) | 4 (5.1) | 4 (6.6) | |
| MUP 2 | 27 (17.5) | 17 (21.5) | 8 (13.1) | |
| Unknown | 2 (1.3) | 2 (2.5) | 0 (0.0) | |
| Type | 0.637 | |||
| Superficial spreading | 63 (40.9) | 27 (34.2) | 28 (45.9) | |
| Nodular | 27 (17.5) | 13 (16.5) | 10 (16.4) | |
| Acral lentiginous | 8 (5.2) | 5 (6.3) | 3 (4.9) | |
| Lentigo maligna | 1 (0.6) | 0 (0.0) | 1 (1.6) | |
| Desmoplastic | 1 (0.6) | 1 (1.3) | 0 (0.0) | |
| Other | 5 (3.2) | 4 (5.1) | 1 (1.6) | |
| Unknown | 20 (13.0) | 10 (12.7) | 10 (16.4) | |
| Missing (MUP 2) | 29 (18.8) | 19 (24.1) | 8 (13.1) | |
| Breslow thickness | 0.788 | |||
| ≤1.0 mm | 6 (3.9) | 2 (2.5) | 3 (4.9) | |
| 1.1–2.0 mm | 0 (0.0) | 0 (0.0) | 0 (0.0) | |
| 2.1–4.0 mm | 5 (3.2) | 2 (2.5) | 3 (4.9) | |
| >4.0 mm | 15 (9.6) | 5 (6.3) | 6 (9.8) | |
| Unknown | 128 (83.1) | 70 (88.6) | 49 (80.3) | |
| Ulceration | 0.639 | |||
| Yes | 38 (24.7) | 18 (22.8) | 13 (21.3) | |
| No | 58 (37.7) | 26 (32.9) | 28 (45.9) | |
| Unknown | 58 (37.7) | 35 (44.3) | 20 (32.8) | |
| Location metastases | 0.007 | |||
| Locoregional | 33 (21.4) | 9 (11.4) | 19 (31.1) | |
| Distant | 68 (44.2) | 42 (53.2) | 20 (32.8) | |
| Both | 53 (34.4) | 28 (35.4) | 22 (36.1) | |
| Number of metastases | 0.614 | |||
| 1 lesion | 10 (6.5) | 6 (7.6) | 3 (4.9) | |
| 2–5 lesions | 21 (13.6) | 13 (16.4) | 6 (9.8) | |
| 6–10 lesions | 3 (1.9) | 3 (3.8) | 0 (0.0) | |
| >10 lesions | 63 (40.9) | 35 (44.3) | 24 (39.3) | |
| Unknown | 57 (37.0) | 22 (27.8) | 28 (45.9) | |
| BRAF-mutation | <0.001 | |||
| Present | 106 (68.8) | 36 (45.6) | 61 (100.0) | |
| Absent | 45 (29.2) | 41 (51.9) | 0 (0.0) | |
| Unknown | 3 (1.9) | 2 (2.5) | 0 (0.0) | |
| LDH | 0.095 | |||
| ≤ULN 3 | 115 (74.7) | 62 (78.5) | 43 (70.5) | |
| >ULN (>250 U/L) | 34 (22.1) | 14 (17.7) | 18 (29.5) | |
| Unknown | 55 (35.7) | 30 (38.0) | 16 (26.2) | |
| S100 | 0.328 | |||
| ≤ULN | 40 (26.0) | 21 (26.6) | 18 (29.5) | |
| >ULN (>0.10 ug/L) | 59 (38.3) | 28 (35.4) | 27 (44.3) | |
| Unknown | 55 (35.7) | 30 (38.0) | 16 (26.2) | |
| Sequence systemic therapy | 0.006 | |||
| First Line | 107 (69.5) | 47 (59.5) | 49 (80.3) | |
| Second line | 29 (18.8) | 23 (29.1) | 5 (8.2) | |
| Third line | 11 (7.1) | 4 (5.1) | 6 (9.8) | |
| ≥ Fourth line | 7 (4.5) | 5 (6.3) | 1 (1.6) | |
| Type systemic therapy | ||||
| ICI | 79 (51.3) | |||
| Targeted therapy | 61 (39.6) | |||
| Other/unknown | 14 (9.1) | |||
| Best response to systemic therapy | 0.027 | |||
| Stable disease | 68 (44.2) | 33 (41.8) | 27 (44.3) | |
| Partial response | 71 (46.1) | 42 (53.2) | 25 (41.0) | |
| Complete response | 5 (3.2) | 3 (3.8) | 1 (1.6) | |
| Unknown | 9 (5.8) | 1 (1.3) | 8 (13.1) | |
| Status of disease prior to surgery | 0.007 | |||
| Progressive disease | 71 (46.1) | 45 (57.0) | 20 (32.8) | |
| Stable disease | 45 (29.2) | 19 (24.1) | 19 (31.1) | |
| Partial response | 29 (18.8) | 14 (17.7) | 15 (24.6) | |
| Unknown | 9 (5.8) | 1 (1.3) | 7 (11.5) | |
| Location surgery | 0.685 | |||
| (Sub)cutaneous/LN | 127 (82.5) | 56 (77.8) | 46 (80.7) | |
| Visceral | 27 (17.5) | 16 (22.2) | 11 (19.3) | |
| Complication surgery | 0.029 | |||
| None | 122 (79.2) | 67 (87.0) | 42 (68.9) | |
| Transient | 22 (14.3) | 6 (7.8) | 15 (24.6) | |
| Requiring intervention | 7 (4.5) | 4 (5.2) | 3 (4.9) | |
| Permanent damage | 1 (0.6) | 0 (0.0) | 1 (1.6) | |
| Death | 0 (0.0) | 0 (0.0) | 0 (0.0) | |
| Status of disease at first follow-up after surgery | 0.459 | |||
| Progressive disease | 26 (16.9) | 12 (15.4) | 11 (18.0) | |
| Stable disease | 49 (31.8) | 28 (35.9) | 16 (26.2) | |
| Partial response | 18 (11.7) | 18 (11.7) | 6 (9.8) | |
| Complete response | 49 (31.8) | 22 (28.2) | 25 (41.0) | |
| Unknown | 12 (7.8) | 4 (5.1) | 3 (4.9) | |
| a. Univariate Analyses (Significant Results). | ||||||
| Overall Survival | Progression-Free Survival | |||||
| Variable | HR | 95% CI | p | HR | 95% CI | p |
| Time between primary tumor and current episode | 0.030 | 0.476 | ||||
| ≤1 year | Ref | Ref | ||||
| >1 and ≤5 years | 0.32 | 0.15–0.71 | 0.005 | 0.65 | 0.36–1.17 | 0.150 |
| >5 and ≤10 years | 0.50 | 0.23–1.10 | 0.083 | 0.91 | 0.49–1.68 | 0.753 |
| >10 years | 0.59 | 0.25–1.39 | 0.224 | 0.85 | 0.43–1.69 | 0.650 |
| Systemic therapy | ||||||
| ICI | Ref | Ref | ||||
| Targeted therapy | 1.65 | 0.89–3.07 | 0.115 | 1.56 | 0.97–2.49 | 0.066 |
| Treatment sequence | 0.609 | 0.015 | ||||
| First line | Ref | Ref | ||||
| Second line | 0.67 | 0.30–1.51 | 0.334 | 0.42 | 0.21–0.86 | 0.017 |
| Third line | 1.42 | 0.55–3.64 | 0.465 | 1.79 | 0.88–3.65 | 0.109 |
| Fourth line or more | 0.73 | 0.10–5.40 | 0.761 | 0.53 | 0.13–2.18 | 0.380 |
| Duration of systemic treatment | ||||||
| ≤12 months | Ref | Ref | ||||
| >12 months | 0.60 | 0.24–1.53 | 0.288 | 0.40 | 0.18–0.86 | 0.020 |
| Status of disease prior to surgery | 0.003 | 0.004 | ||||
| PR | Ref | Ref | ||||
| SD | 1.93 | 0.54–6.96 | 0.313 | 1.19 | 0.55–2.54 | 0.663 |
| PD | 4.82 | 1.47–15.83 | 0.009 | 2.37 | 1.18–4.75 | 0.015 |
| Status of disease after surgery | <0.001 | <0.001 | ||||
| CR/PR | Ref | Ref | ||||
| SD | 3.08 | 1.29–7.38 | 0.012 | 2.95 | 1.66–5.23 | <0.001 |
| PD | 11.39 | 4.73–27.47 | <0.001 | 24.20 | 10.40–56.32 | <0.001 |
| Location surgery | ||||||
| Subcutaneous/LN | Ref | Ref | ||||
| Visceral | 2.02 | 1.02–3.94 | 0.045 | 1.07 | 0.60–1.88 | 0.825 |
| b. Multivariate analyses. | ||||||
| Overall Survival | Progression-free survival | |||||
| Variable | HR | 95% CI | p | HR | 95% CI | p |
| Systemic therapy | ||||||
| ICI | Ref | Ref | ||||
| Targeted therapy | 3.25 | 1.48–7.14 | 0.003 | 1.89 | 1.08–3.32 | 0.026 |
| Status of disease prior to surgery | 0.051 | 0.064 | ||||
| PR | Ref | Ref | ||||
| SD | 0.69 | 0.13–3.71 | 0.669 | 0.33 | 0.11–1.00 | 0.051 |
| PD | 2.87 | 0.55–15.02 | 0.212 | 0.69 | 0.23–2.08 | 0.514 |
| Status of disease after surgery | <0.001 | <0.001 | ||||
| CR/PR | Ref | Ref | ||||
| SD | 6.05 | 1.64–22.33 | 0.007 | 6.61 | 2.63–16.59 | <0.001 |
| PD | 18.62 | 4.54–76.42 | <0.001 | 37.46 | 12.25–114.51 | <0.001 |
| Duration of systemic treatment | ||||||
| ≤12 months | Ref | Ref | ||||
| >12 months | 0.34 | 0.09–1.32 | 0.119 | 0.40 | 0.17–0.97 | 0.042 |
© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Blankenstein, S.A.; Aarts, M.J.B.; van den Berkmortel, F.W.P.J.; Boers-Sonderen, M.J.; van den Eertwegh, A.J.M.; Franken, M.G.; de Groot, J.W.B.; Haanen, J.B.A.G.; Hospers, G.A.P.; Kapiteijn, E.; et al. Surgery for Unresectable Stage IIIC and IV Melanoma in the Era of New Systemic Therapy. Cancers 2020, 12, 1176. https://doi.org/10.3390/cancers12051176
Blankenstein SA, Aarts MJB, van den Berkmortel FWPJ, Boers-Sonderen MJ, van den Eertwegh AJM, Franken MG, de Groot JWB, Haanen JBAG, Hospers GAP, Kapiteijn E, et al. Surgery for Unresectable Stage IIIC and IV Melanoma in the Era of New Systemic Therapy. Cancers. 2020; 12(5):1176. https://doi.org/10.3390/cancers12051176
Chicago/Turabian StyleBlankenstein, Stephanie A., Maureen J. B. Aarts, Franchette W. P. J. van den Berkmortel, Marye J. Boers-Sonderen, Alfons J. M. van den Eertwegh, Margreet G. Franken, Jan Willem B. de Groot, John B. A. G. Haanen, Geke A. P. Hospers, Ellen Kapiteijn, and et al. 2020. "Surgery for Unresectable Stage IIIC and IV Melanoma in the Era of New Systemic Therapy" Cancers 12, no. 5: 1176. https://doi.org/10.3390/cancers12051176
APA StyleBlankenstein, S. A., Aarts, M. J. B., van den Berkmortel, F. W. P. J., Boers-Sonderen, M. J., van den Eertwegh, A. J. M., Franken, M. G., de Groot, J. W. B., Haanen, J. B. A. G., Hospers, G. A. P., Kapiteijn, E., Piersma, D., van Rijn, R. S., Suijkerbuijk, K. P. M., ten Tije, A. J., van der Veldt, A. A. M., Vreugdenhil, G., Wouters, M. W. J. M., & van Akkooi, A. C. J. (2020). Surgery for Unresectable Stage IIIC and IV Melanoma in the Era of New Systemic Therapy. Cancers, 12(5), 1176. https://doi.org/10.3390/cancers12051176