Abstract
Although significant strides have been made in cardiac pacing, the field is still evolving. While transvenous permanent pacing is highly effective in the management of bradyarrhythmias, it is not risk free and may result in significant morbidity and, rarely, mortality. Transvenous leads are often the weakest link in a pacing system. They may dislodge, fracture, or suffer breaches in their insulation. This review was undertaken to clarify leadless risks, benefits, and alternatives to transvenous cardiac pacing for bradyarrhythmias and heart failure management. In order to clarify the role(s) of leadless pacing, this narrative review was undertaken by searching MEDLINE to identify peer-reviewed clinical trials, randomized controlled trials, meta-analyses, and review articles, as well as other clinically relevant reports and studies. The search was limited to English-language reports published between 1932 and 2024. Leadless pacing was searched using the terms Micra™, Nanostim™, AVEIR™, single-chamber leadless pacemaker, dual-chamber leadless pacemaker, cardiac resynchronization therapy (CRT), cardiac physiological pacing (CPP) and biventricular pacing (BiV). Google and Google Scholar, as well as bibliographies of identified articles were also reviewed for additional references. The advantages and limitations of leadless pacing as well as options that are under investigation are discussed in detail.
1. Introduction
The rich history of cardiac pacing began more than 90 years ago. Its evolution has resulted from a combination of creative thought and dramatic advances in technology. Table 1 summarizes key developments in transvenous cardiac pacing (additional details are available in Supplement S1) [1,2,3,4,5,6,7,8,9,10,11,12,13,14,15,16,17,18,19]. This manuscript aims to provide a review of the structure, function, and limitations of transvenous cardiac pacemaker leads, the development of leadless pacemakers, the structural characteristics of leadless pacemakers, clinical trials that investigated the safety and efficacy of leadless pacing, implantation techniques, indications for leadless pacing, risks and complications of leadless pacing, advantages and disadvantages of leadless pacing, investigational devices (those without U.S. Food and Drug Administration [FDA] approval, without CE Mark or without both), and final conclusions.

Table 1.
Evolving concepts in cardiac pacing [1,2,3,4,5,6,7,8,9,10,11,12,13,14,15,16].
2. Structure, Function, and Limitations of Transvenous Cardiac Pacemaker Leads
Transvenous pacemaker systems consist primarily of a hermitically sealed can, placed in the pre-pectoral region, containing the battery and all circuitry. The can is connected to the myocardial tissue by a pacemaker lead or leads. The leads contain conductor coils to the distal electrodes separated by insulation material [20] (Figure 1). Over the last three to four decades, the basic material used for most conductors has been MP-35N (SPS Technologies, Cleveland, OH, USA), an alloy of nickel, cobalt, chromium, and molybdenum. High electrical resistance has been overcome with the development of composite-wire conductors that incorporate low-resistance metals such as silver and stainless steel, with high-strength materials such as titanium, platinum, and platinum–iridium alloy. The leads are of coaxial (coil within a coil) or coradial (side-by-side coils) design, depending on the arrangement of the conductor coils. Lead tips are attached to the myocardium by a penetrating helix (active fixation) or by tines that embed in the myocardial trabeculations (passive fixation) [20]. Standardization of pacemaker leads has allowed global compatibility across manufacturers. The international standard-1 (IS-1) terminal ring and pin arrangement allows (with some exceptions) connection to pacemaker generators from different manufacturers [21].
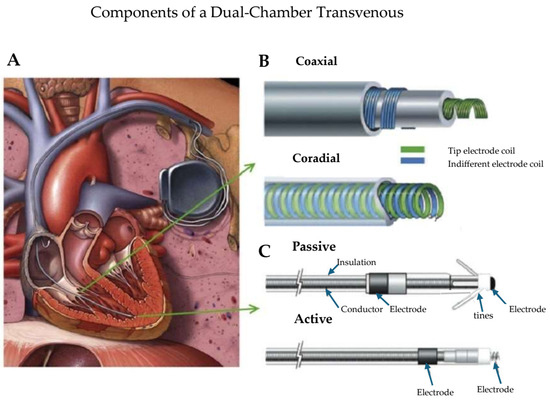
Figure 1.
(A) Transvenous pacemaker systems primarily consisting of a hermetically encased can (also known as a generator) containing the battery and its circuitry placed subcutaneously (in the pre-pectoral region) or submuscularly between the pectoral muscles. The can is connected to the myocardial tissue by a pacemaker lead (or leads). The leads contain conductor coils to the distal electrodes separated by insulation material. (B) The leads are of coaxial (coil within a coil) or coradial (side-by-side coils) design depending on the arrangement of the conductor coils. (C) The lead tips are attached to the myocardium by a screw-like penetrating helix (active fixation) or by tines that embed in the myocardial trabeculations (passive fixation). Adapted from reference [20] with permission.
Despite advances made in cardiac pacing, lead-related issues remain the “Achilles heel” of cardiac pacing. Apart from infection, there is a greater incidence of lead-related complications compared with issues related to pulse generators.
Early lead-related issues include dislodgement resulting in loss of capture, as well as under-sensing due to an acute inflammatory response. The latter is usually remediable via reprogramming.
Lead insulation provides physical and electrical shielding of the conductor elements. In addition, insulation contributes significantly to the structural strength of the entire lead body [22]. Among the problems with the major materials used for lead insulation (polyurethane, silicone rubber, fluoropolymers) is that they were not originally specifically designed for this purpose. Each has disadvantages when used as part of a biological pacing system. Because leads are subject to repetitive mechanical stress during each cardiac cycle and by shoulder girdle movement in the body, leads are the most common pacemaker components to fail. Insulation breaks result in low impedance measurements and oversensing of signals generated by surrounding muscle structures because the conductors are exposed [22].
Over the last three to four decades, the basic material used for most conductors has been MP-35N (SPS Technologies, Cleveland), an alloy of nickel, cobalt, chromium, and molybdenum. The main advantage of MP-35N is high strength and resistance to corrosion [23]. Its main disadvantage is its high electrical resistance. This has been overcome with the development of composite-wire conductors that incorporate low-resistance metals such as silver and stainless steel with high-strength materials such as titanium, platinum, and platinum–iridium alloy [23]. Conductor fracture typically results in non-physiologic signals (“noise”) caused by the lead. This noise consists of high-frequency, saturated electrograms generated by intermittent contact between disrupted conductor elements (called filars) and can be associated with elevated lead impedance and loss of capture. Chronic inflammation (at times due to an underlying primary cardiomyopathic process) may result in loss of capture. Acute venous entry angles, medial venous access near the costoclavicular ligament, sharp turns in the pocket, young age, subpectoral device placement, tight sutures, and silicone insulation are risk factors associated with insulation breaks and lead fractures [20]. Other lead problems include infection/endocarditis, venous thrombosis and emboli, and tricuspid regurgitation [20].
In addition to the problems noted above, leads may be misplaced in the left chamber of the heart. Although inadvertent malpositioning of cardiac implantable electronic device leads into the left ventricle is an uncommon complication of transvenous pacing and defibrillation, it may result in serious consequences. In 2016, Ohlow et al. reported a 3.4% incidence of inadvertent lead placement into the left heart; however, this included the cardiac veins [18]. Inadvertent endocardial left ventricular (LV) lead placement creates a nidus for thrombus formation and possible embolization. Treatment of LV lead misplacement discovered late after implantation includes lead removal or chronic anticoagulation with warfarin to prevent thromboemboli. Although LV lead extraction was first described in 1991 [19], procedural safety remains uncertain. Because use of dabigatran in patients with mechanical heart valves was associated with increased rates of thromboembolic and bleeding complications compared with warfarin, substituting a direct oral anticoagulant for warfarin in the setting of malpositioned left ventricular leads is not recommended [24].
Rapid identification of lead position is critical during implantation and just after the procedure, with immediate correction required if malpositioning is detected. If lead misplacement is discovered late after implantation, the lead should be surgically removed or chronic anticoagulation with warfarin should be initiated [24].
3. Development of Leadless Pacemakers (LPs)
Leadless cardiac pacing has been developed in response to lead-related problems and the desire to reduce the incidence of device-related infection. Because leads have long been considered the weakest link of cardiac pacing systems, a totally self-contained cardiac pacing system was conceptualized more than 50 years ago. In 1970, Spickler and associates reported totally self-contained leadless cardiac pacing in a canine model. Nevertheless, this concept has become a reality only recently as a result of technological advancements in battery energy, endocardial fixation and delivery systems [25]. The first report of leadless pacing in humans was published in 2014 [26].
4. Structure of Leadless Pacemakers
The newest versions of leadless pacemakers available from Medtronic (Minneapolis, MN, USA) are Micra AV and Micra VR2. Each has a length of 25.9 mm, an outer diameter of 6.7 mm, and a mass of 1.75 g. Materials in chronic contact with human tissue include titanium, titanium nitride, parylene C, PEEK, nitinol, platinum–iridium alloy, and silicone rubber. Nitonal FlexFixTM tines are used for fixation. A monolithic controlled release device (MCRD) provides steroid elution to help maintain acceptable pacing thresholds. The nominal pacing cathode measures 2.5 mm2, is point-sintered and coated with titanium nitride. The minimum pacing anode measures 22 mm2 and is coated with titanium nitride. The cathode-to-anode spacing is 18 mm. Both have a 3.2-volt lithium-hybrid CFx silver vanadium oxide battery [27,28].
The AVEIR leadless ventricular pacemaker has a length of 38 mm, a diameter of 6.5 mm. and a mass of 2.4 g. The outer shell/can of the device is composed of titanium. Fixation is achieved via a nonretractable helix. Its tip electrode is a titanium nitride-coated, platinum–iridium disk located at the center of the fixation helix, which measures about 2.2 mm2. The tip electrode includes a single dose of dexamethasone sodium phosphate (DSP) intended to reduce inflammation. The ring electrode is the uncoated part of the titanium pacemaker case, and its surface area measures > 127 mm2. The inter-electrode space is >24 mm [29].
The AVEIR leadless atrial pacemaker has a length of 32.2 mm, a diameter of 6.5 mm. and a mass of 2.1 g. The LP distal tip electrode comprises a titanium nitride-coated, platinum–iridium helix (LSP201A) or disk (LSP202V) located at the center of the fixation helix. The tip electrode includes a single dose of dexamethasone sodium phosphate (DSP) intended to reduce inflammation. The ring electrode is the uncoated part of the titanium pacemaker case, and its surface area measures ~124 mm2. The inter-electrode space is >24 mm [29]. All leadless conductors use MP-35N alloys. Table 2 provides additional comprehensive details of leadless pacing devices [30].
Table 2.
Characteristics of leadless pacemakers.
5. Clinical Trials Investigating Leadless Pacing’s Safety and Efficacy
LEADLESS was a prospective, non-randomized, single-arm multicenter study of the safety and clinical performance of a completely self-contained leadless cardiac pacemaker (Nanostim Inc., Sunnyvale, CA, USA). The 33 patients enrolled had a mean age of 77 ± 8 years, and 67% of the patients were male. Implantation was successful in 97% (32/33) of the cohort. Five patients (15%) required the use of more than one pacing device due to inadvertent LV placement, malfunction of the release knob, delivery catheter damage, damage to the device’s helix, and difficulty with the delivery catheter’s wire deflection mechanism. The one inadvertent device placement in the LV (via a patent foramen ovale) was successfully retrieved without sequelae. A new device was implanted in the RV apex. Another patient developed cardiac tamponade. He underwent emergent median sternotomy on cardiopulmonary bypass and surgical repair of an RV apical perforation. Despite gradual recovery, he suffered left-sided hemiplegia attributable to a right-sided main cerebral artery ischemic infarct and died on post-procedure day 18 [26].
Follow-up of the other 31 patients who underwent successful implantation revealed no pacemaker-related adverse events reported between 3 and 12 months of follow-up. At 6 and 12 months of follow-up, the pacing performance results were as follows: mean pacing threshold (at a 0.4 ms pulse width), 0.40 ± 0.26 Volts [V] and 0.43 ± 0.30 V; R-wave amplitude 10.6 ± 2.6 millivolts [mV] and 10.3 ± 2.2 mV; and impedance 625 ± 205 Ohms [Ω] and 627 ± 209 Ω. At the 12-month follow-up, 61% of the patients had their rate response sensor activated. Adequate rate response was observed in all of these patients [26,31].
A subsequent report from the Leadless II study [32] reviewed data from the first 300 Nanostim (acquired by St. Jude Medical, Sylmar, CA, USA) device recipients followed for 6 months as well as the entire cohort of 526 patients enrolled as of June 2015. The primary composite efficacy end point was an acceptable pacing capture threshold (≤2.0 V at 0.4 ms) and an acceptable sensing amplitude (R wave ≥ 5.0 mV, or a value equal to or greater than the value at implantation) through 6 months.
Implantation was successful in 289 of the initial 300 patients (96.3%) and 270 patients (90%) had an acceptable primary composite end point. Inadequate pacing capture thresholds were noted in 4 patients. Inadequate sensing was noted in 14 patients and one patient had inadequate pacing and sensing parameters [32].
The primary safety end point was freedom from serious device-related adverse events during the initial 6 months post-implantation. Twenty-two serious device-related adverse events occurred in 20 patients (6.7%). Included among these complications were cardiac perforation (4 [1.3%]), device dislodgement (5 [1.7%], elevated pacing thresholds requiring device replacement (4 [1.3%]) and vascular complications in 4 [1.3%] patients [32].
There were 28 deaths (5.3%) in the total cohort, 19 (68%) occurred within 6 months, 8 (29%) between 6 and 12 months, and 1 (3%) after 12 months. The mean age of patients who died was 79.1±10.9 years. Two deaths (0.4%) were classified by the clinical events committee as procedure-related [32].
St. Jude Medical (now Abbott) halted implantation of its Nanostim leadless pacemaker in October 2016, due to reports of battery malfunction resulting in loss of telemetry and pacing output. St. Jude Medical had previously halted implantations of the Nanostim leadless pacemaker after reports surfaced of problems with the device’s docking button, which was designed to connect with the retrieval catheter, allowing the Nanostim device to be retrieved and removed after implantation.
The redesigned version of Nanostim, Aveir LP (Abbott Cardiovascular, Plymouth, MN, USA) incorporated important design improvements, including the use of standard transvenous pacemaker lithium carbon-monofluoride battery chemistry with a 12% (1.1 years) longer battery life (up to 10.4 years), an altered form factor (10% shorter, 1.5-F wider, to 19.5-F), a modified docking button (facilitating retrievability), a modified delivery system with an ergonomic design, and a new application-specific integrated circuit (ASIC) chip designed to support a dual-chamber pacing system once approved [33].
The LEADLESS II–Phase 2 trial evaluated the efficacy and safety of the AVEIR LP system in 200 patients with standard VVI(R) pacing indications. The primary efficacy end point was a composite score of acceptable pacing thresholds (≤2.0 V at 0.4 ms) and R-wave amplitudes (≥5.0 mV) at implantation through six weeks of follow-up.
The implant success rate was 98% and 83.2% did not require repositioning. The primary safety end point “serious complications” occurred in eight patients. The most common complications were cardiac tamponade and premature device deployment. The primary efficacy end point was achieved in 188 of 196 (95.9%) patients who underwent successful device implantation [33].
Shortly before the time when implantation of Nanostim was halted, Ritter and colleagues reported early experience with implantation of the Micra transcatheter [leadless] pacing system (TPS, Model MC1VR01, Medtronic plc, Mounds View, MN, USA) [34]. Micra (physical characteristics noted above) was a single-chamber ventricular pacemaker (Figure 2) [34]. A total of 140 patients underwent device implantation. The prespecified safety goal was >85% freedom from unanticipated serious adverse device-related events and efficacy was assessed via the mean 3-month pacing capture threshold. During a mean follow-up of 1.9 ± 1.8 months, there were no unanticipated serious adverse events. However, 30 adverse events related to the system or procedure occurred (primarily transient arrhythmias or femoral access complications) [34]. Among patients followed for 3 months (n = 60), the mean pacing threshold was 0.51 ± 0.22 V, and none exceeded 2 V. The mean R-wave amplitude was 16.1 ± 5.2 mV, and the mean impedance was 650.7 ± 130 Ω [34].
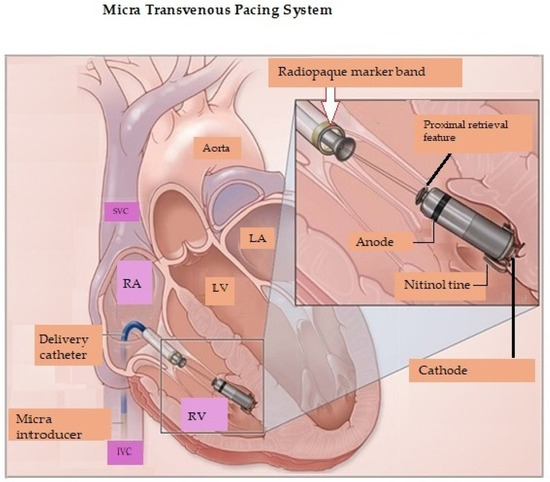
Figure 2.
Micra transvenous pacing system positioned in the right ventricle. RA = Right atrium; RV = Right ventricle; LA = Left atrium; LV = Left ventricle; SVC = Superior vena cava; IVC = Inferior vena cava. Reproduced from reference [35] with permission.
In 2016, Reynolds et al. reported an interim (6-month) analysis of the safety and efficacy of the Micra transcatheter pacing system. The device was successfully implanted in 719 of 725 patients (99.2%). The primary efficacy end point was the percentage of patients with low (≤2 V at a pulse width of 0.24 ms) and stable pacing thresholds (an increase of ≤1.5 V from the time of implantation) at 6 months post-implantation. The primary safety end point was freedom from system-related or procedure-related major complications [35].
The primary efficacy goal was evaluated in 297 patients and was achieved in 292 (98.3%). In comparison to a historical (transvenous pacing) cohort, the safety profile was comparable to that of a transvenous system while providing low and stable pacing thresholds [35].
There were 28 major complications in 25 patients (4%), including four of six patients who underwent unsuccessful attempts at implantation. Among these, one death occurred, eleven patients had cardiac perforation or pericardial effusions, two patients had venous thrombosis (one also had a pulmonary embolus), two had elevated pacing thresholds and five developed arteriovenous fistulae at their femoral venous entry site [35].
For Micra™, the long term (12 months) safety objective of freedom from major complications was achieved in 96%. Four new major complications occurred. Three patients developed heart failure and one was associated with pacemaker syndrome (atrioventricular dyssynchrony associated with a constellation of symptoms such as dyspnea, fatigue, and exercise intolerance) [36,37]. Although there were 26 patients with 33 systemic infectious events during the trial, none were attributed to implantation of the device.
Among the 630 patients with pacing threshold data available at 12 months, 93% had a threshold of ≤1 V (mean 0.60 ± 0.38 V) at 0.24 ms pulse duration, and out of the 58 patients with available pacing threshold data at 24 months, 97% had a pacing threshold of ≤1 V (mean 0.53 ± 0.23 V) also at 0.24 ms. Pacing thresholds tended to decrease after implant and subsequently remained stable [36]. R-waves (ventricular sensing) were 15.1 mV at 12 months and 15.5 mV at 24 months [36].
In 2017, the acute performance of the Micra transcatheter pacemaker was reported from a worldwide post-approval registry. Performance of the Micra transcatheter pacemaker in the real-world setting demonstrated a high rate (99.6%) of implant success and low rate (1.51%) of major complications over 30 days post-implant. The rates of pericardial effusion, device dislodgement, and infection were low, reinforcing the results of the investigational study [38].
The Longitudinal Coverage With Evidence Development Study on Micra Leadless Pacemakers (Micra CED) is a continuously enrolling observational cohort study evaluating complications, utilization, and outcomes of leadless VVI pacemakers in the US Medicare fee-for-service population. At a 5-year follow-up, data from the post-approval registry on 1809 patients enrolled between July 2015 and March 2018 revealed that Micra leadless pacemaker outcomes continued to demonstrate low rates of major complications and system revisions as well as an extremely low incidence of infection. There were no Micra removals due to infection. At 36 months, system revision rates were significantly lower with Micra compared to transvenous systems (3.2% vs. 6.6%, p < 0.001) [39].
Because single-chamber ventricular pacemakers do not provide atrial pacing or consistent atrioventricular synchrony, implantation is limited to approximately 20% of patients who have indications for a pacemaker [40,41]. In 2023, Knops and colleagues reported 90-day results from 300 patients who received a dual-chamber leadless pacing system AVEIR DR (Abbott Cardiovascular, Plymouth, MN, USA) [40]. The system consisted of two devices implanted percutaneously (in a single procedure), one in the right atrium and one in the right ventricle. AVEIR AR LP was designed to accommodate the right atrial size and sensitivity, with unique features designed to achieve implant stability and optimization. A 1.63 mm inactive outer helix provide primary fixation while the recessed inner helix acts as the pacing electrode while also providing additional fixation and electrical stability [30,40]. As previously noted, the atrial leadless pacemaker is shorter (32.2 mm in length). The right ventricular leadless pacemaker is physically identical to the commercially available single-chamber leadless device. Both leadless devices are 6.5 mm in diameter (Figure 3). The leadless pacemakers wirelessly communicated bidirectionally (implant-to-implant), on a beat-to-beat basis via a series of short pulses delivered through the blood and myocardial tissue after each locally paced or sensed event, thus maintaining atrioventricular synchrony [40].
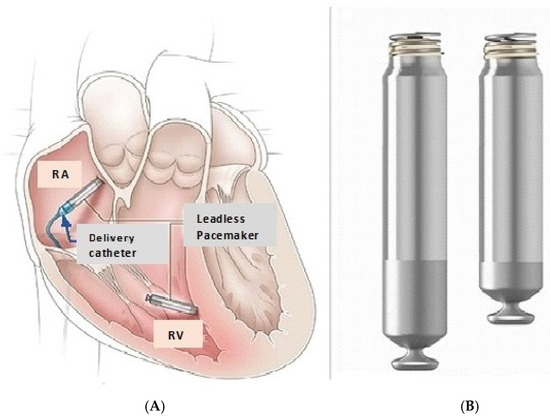
Figure 3.
(A) Device placement. The RV LP is positioned at the interventricular septum aiming to reduce the risk of perforation. (B) The RA LP measures 5.8 mm and is shorter than the RV LP. It is ideally positioned at the ostium of the RA appendage. RA = Right atrium; RV = Right ventricle. Adapted from reference [40] with permission.
Procedural success was attained in 295 of 300 patients (98.3%). The atrial pacing device was not implanted in 2 patients, and 3 had inadequate implant-to-implant communication. Intraprocedural device dislodgment (6; 5 atrial) was successfully managed with retrieval and repositioning. Five additional dislodgements occurred at 26 ± 17 days post procedure. Another atrial device was implanted in three patients. The authors recommended targeting the ostium of the appendage to optimize implant-to-implant communication and possibly limit atrial lead dislodgement [40]. Eight revision procedures were performed. The indications for these revisions were atrial dislodgement (6), suboptimal implant-to-implant communication (1), and intermittent ventricular capture (1). Successful percutaneous retrieval was achieved in each instance. Six new leadless pacemakers were implanted successfully. At the discretion of the investigator, two patients did not receive a replacement atrial leadless pacemaker [40].
Four patients died. The deaths were adjudicated (by an independent clinical events committee) to be unrelated to the device or the procedure [40].
The first primary performance end point, a combination of adequate atrial capture threshold (≤3.0 V at 0.4 ms) and atrial sensing amplitude (P wave of ≥1.0 mV) at the 3-month visit was achieved in 90.2%. The second primary performance end point was AV synchrony at the 3-month visit, defined as a paced or sensed ventricular beat within 300 ms of a paced or sensed atrial beat in ≥70% of the cardiac cycles evaluated during a 5 min seated recording, and was found in 97.3% [40]. The FDA-approved the AVEIR™ dual chamber (DR) leadless pacemaker system on 5 July 2023 [42,43].
Unlike traditional dual-chamber transvenous permanent pacemakers, which sense atrial electrical activity directly through a lead implanted in the right atrium, the Micra AV algorithm (Medtronic, Inc., Minneapolis, MN, USA) identifies mechanical atrial contraction, detected by the device implanted in the ventricle, and allows AV synchronous pacing. The algorithm relies on a three-axis accelerometer to detect atrial contraction [44]. Micra AV accelerometer signals and their relationship to surface ECG waves are depicted in Figure 4. The A1 signal corresponds to closure of the tricuspid and mitral valves and the onset of ventricular isovolumic contraction. Hence, A1 falls at the end of the electrocardiographic (ECG) QRS complex (electrical systole precedes mechanical systole). The A2 signal corresponds to aortic and pulmonic valve closures, corresponding to the end of ventricular systole. Hence, the A2 signal typically falls at the end of T wave. The A3 signal corresponds to passive ventricular filling while the A4 signal corresponds to atrial contraction. These (A3 and A4) signals correspond to the E and A mitral inflow echocardiographic measurements [44]. In Micra AV2, the AV conduction mode switch to a lower rate is programmable to facilitate AV conduction. A3 and A4 thresholds were improved. The Auto+ A3 adjusts the A3 threshold more appropriately to facilitate tracking at higher sinus rates. The auto A4 threshold could be adjusted too high in Micra AV. Therefore, a programmable max A4 threshold was added in Micra AV2 with a nominal value of 3.0 m/s2 (meters per second squared). A change in battery composition and a decrease in current drain increased longevity by 4+ years for Micra AV2 and Micra VR2 devices. Micra AV2 and Micra VR2 have expanded labeling for MRI scans < 1.5T [45].
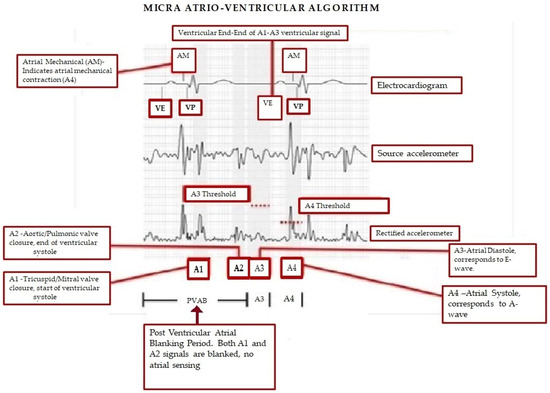
Figure 4.
Micra AV accelerometer signals and their relationship to surface ECG wave. AM, atrial mechanical; AV, atrioventricular; ECG, electrocardiography; PVAB, post-ventricular atrial blanking; VE, end of ventricular ectopy. Reproduced from reference [44] with permission.
The MARVEL 2 (Micra Atrial tRacking using a Ventricular accELerometer 2, Minneapolis, MN, USA) study assessed the ability to provide AV synchronous pacing by mechanically sensing atrial contractions via a right ventricular Micra leadless pacemaker [46]. The algorithm facilitated AV synchrony ≥ 70% at rest in 95% of patients with complete atrioventricular block (AVB) [46]. Micra AV2 was approved by the FDA in 2020 based on the results of the MARVEL 2 study [45].
The AccelAV study was a prospective, non-randomized, multicenter clinical trial conducted in the United States and Hong Kong and reported in 2023 [47]. The primary aim of the AccelAV study was to characterize chronic atrioventricular synchrony in patients implanted with Micra AV (Model MC1AVR1, Medtronic, Inc., Minneapolis, MN, USA). As noted above, Micra AV is implanted in the RV and uses the device’s accelerometer to mechanically sense atrial contractions and facilitate VDD pacing. In this mode, V = ventricular pacing, D = sensing in the atrium and ventricle, D = an intrinsic QRS can inhibit ventricular pacing, and an intrinsic P-wave can trigger an AV delay resulting in P-wave tracking and maintenance of AV synchrony via RV pacing [48]. In complete AV block, the intrinsic P-wave does not conduct to the ventricle and the end of the AV delay is followed by a paced ventricular complex [48].
Among 54 patients with normal sinus node function and complete AVB, Micra AV mean resting AV synchrony was 85.4% at 1 month, and ambulatory AV synchrony was 74.8%. In a subset of 20 patients with programming optimization, mean ambulatory AV synchrony was 82.6% [47]. Medtronic received the CE mark for these devices in January 2024 [49].
6. Implantation Techniques
The vast majority of leadless pacemakers have been implanted via the following sequence: Right femoral vein access, introduction and advancement of a large (e.g., 27 F) sheath under fluoroscopy navigating the delivery system to superior vena cava and the right interventricular septum, deployment, and fixation. If difficulty with venous stenosis, occlusion, or severe tortuosity of the right femoral vein is encountered, a left femoral venous approach may also be used [50]. As previously noted, right atrial devices are ideally advanced to the ostium of the right atrial appendage [40].
In addition to the difficulties noted above, femoral vein access may be accompanied by complications in the groin area, such as hematomas, arteriovenous fistulae, or arterial pseudoaneurysms, each occurring with an approximate risk of 1%. Moreover, stenosis or a tortuous anatomy of the inferior vena cava (IVC) may hinder the successful implantation of a femoral leadless pacemaker. Therefore, Molitor et al. compared peri-procedural safety and efficacy in the first 100 consecutive patients who underwent Micra™ leadless pacemaker implantation via the right internal jugular vein (at two centers) to the first 100 patients using a femoral implantation approach at the University Hospital Zurich. The mean procedure (35.63 ± 10.29 versus 48.9 ± 21.0 min; p < 0.01) and fluoroscopy times (4.66 ± 5.16 min versus 7.7 ± 7.8 min; p < 0.01) were shorter compared to the femoral approach. Electrical parameters were similar between the two techniques. Two complications occurred during jugular veinous implantation (1 pericardial effusion and 1 dislocation), versus 16 complications using the femoral approach (1 pericardial effusion, 2 femoral artery injuries, and 13 major groin hematomas). This difference was statistically significant (p= 0.0005) [51]. Additional experience with this technique is needed to shed further light on its efficacy and safety.
El-Chami and Shah have suggested ways to avoid ventricular perforation (see Section 8, below). They suggest: (1) Always advancing the delivery system over a stiff wire under fluoroscopic guidance; (2) Withdrawing the delivery sheath in the right atrium rather than advancing the delivery system out of the sheath; (3) Avoiding traumatic manipulation of the delivery system by starting counter-clockwise rotation in the lower one-third of the RA to steer the delivery system anteriorly toward the tricuspid valve; (4) Avoiding suddenly popping the delivery system across the tricuspid valve and into the right ventricle; (5) Making sure the delivery system is free in the right ventricle and applying clockwise torque toward the right ventricular septum (to avoid the risk of perforation [see below] in the inferior right ventricular recess and apex); and (6) Avoiding frequent deployments (>5) if a good position or electrical characteristics are not achieved [50].
7. Indications for Leadless Pacing
Transvenous permanent pacing is typically performed by accessing the subclavian and axillary veins via puncture, or the cephalic vein via cutdown to implant transvenous leads [52]. Common acute transvenous system-related issues include lead dislodgement, thoracic trauma, vascular injury, pocket hematoma, and infection. Common long-term transvenous pacemaker complications (which may require transvenous lead extraction) include lead conductor fractures, abnormal lead sensing or pacing values, insulation failures, device header or connector problems, premature battery depletion, and pocket infection [53]. Leadless permanent pacing was developed to bypass the two major weaknesses of the transvenous systems, the lead(s) and the subcutaneous (or submuscular) pocket [54,55,56]. They are an excellent alternative approach in case of specific comorbidities, such as limited upper venous access, transvenous pacemaker infection (see below) and kidney failure patients receiving hemodialysis (who are also likely to have limited central venous access) [54,56]. While femoral implantation of transvenous leads is possible, it is technically challenging and is a far less desirable option [57].
The initial indication for leadless pacing therapy was mainly limited to patients who had persistent or permanent AF with a slow ventricular response. Single chamber ventricular leadless pacing may also be indicated in patients with paroxysmal atrioventricular (AV) block, sinus node disease or syncope, in which infrequent ventricular pacing is expected [54]. A European Heart Rhythm Association (EHRA) survey regarding the use of leadless pacing in Europe revealed that, among 52 centers from 21 countries, the most common indications for leadless pacing were permanent AF (83%), a history of complications with a conventional pacemaker (87%), anticipated difficult vascular access (91%) and an expected higher risk of infection (70%) [54,58].
The 2021 European Society of Cardiology (ESC) guidelines on cardiac pacing and cardiac resynchronization therapy provided similar recommendations for leadless pacing. As noted above, the guidelines recommended patients without upper-extremity venous access (making the usual transvenous pacing approaches impossible or, at least, impractical) as the most appropriate candidates (ESC Class IIa-B). The low infection rates associated with leadless pacing were noted to make LP attractive for patients on hemodialysis and those with a previous history of a pacemaker infection (ESC Class IIa-B). These guidelines also recommended that LP be considered in all single-lead pacemaker candidates, such as those with permanent atrial fibrillation and patients likely to have a low pacing burden (ESC Class IIb-C). Given the uncertainty surrounding the optimal LP replacement strategy, older patients (with a limited life expectancy) may be more suitable candidates for leadless pacing [30,59].
In the previously noted prospective, multicenter, single-group study to evaluate the safety and performance of a dual-chamber leadless pacemaker system, the most common indications for dual-chamber pacemaker implantation were sinus-node dysfunction (190 patients [63.3%]) and atrioventricular block (100 patients [33.3%]) [40].
8. Risks and Complications of Leadless Pacing
Despite the potential advantages of leadless pacing (see below), the risk of procedural complications is far from insignificant. In 2022, Haddadin et al. reported the rate of complications in 7821 patients who underwent leadless pacemaker implantation (Table 3) [60]. Immediate procedure-related complications occurred in 7.5% of patients. Pericardial effusion that did not require pericardiocentesis occurred in 1.9% of patients, and pericardiocentesis was performed in 1.0%. Vascular complications occurred in 2.3% of patients (0.33% required repair), and device dislodgment occurred in 0.51%. The most significant predictors of procedural complications were end-stage renal disease (odds ratio [OR] 1.65; 95% confidence interval [CI] 1.17–2.32; p = 0.004), congestive heart failure (OR 1.28; 95% CI 1.01–1.62; p = 0.04), and coagulopathy (OR 1.77; 95% CI 1.34–2.34; p < 0.001). All-cause readmission occurred in 17.9% of patients within 30 days of device implantation, and 1.36% were procedure-related. At 30 days post-implant, 0.25% of patients needed a new pacemaker, and 0.18% had pericardial complications [60]. It is important to understand that these data were extracted from the United States National Readmission Database (NRD), between 2016 and 2018. Therefore, it is likely that this study reflects a relatively early clinical experience. A substantial operator learning curve exists for LP implantations, and the implanters might not have been at the end of their learning phase. Additional safety data from large (>500 patients) single-chamber LP large registries and regulatory trials is summarized in Table 4 [30]. Table 5 compares complication rates between patients implanted with leadless versus transvenous pacemakers
Table 3.
Leadless pacemaker implant complications. In-hospital clinical and procedural outcomes.
Table 4.
Short-term and long-term complications of leadless pacing.
Table 5.
Complications between cohorts patients implanted with a leadless pacemaker compared to patients implanted with a transvenous pacemaker.
9. Advantages and Disadvantages of LPs
Table 6 [61,62,63,64,65,66,67,68,69,70,71,72,73] contrasts the advantages and disadvantages of leadless pacing. One of the major drawbacks of LPs is the higher rate of perforation and pericardial effusion at implantation compared to transvenous pacing systems. LP-related perforations are not only more common, but also more severe [30]. LP-related perforations are associated with a high number of deaths, tamponades, and rescue thoracotomies. A 2021 analysis from the MAUDE database revealed that 96% of reported major adverse events with LPs were related to perforation and 27% of major adverse events required a sternotomy [69]. Patient characteristics associated with an increased risk of cardiac perforation included advanced age, female sex, low body mass index (<20), chronic obstructive pulmonary disease, heart failure, prior myocardial infarction, COPD, absence of prior cardiothoracic surgery, and dialysis [30,70]. A recent position paper recommended that LP implantation should preferably be performed at centers with on-site cardiothoracic surgery support [30,71]. For RV pacing, placement of the device at the interventricular septum rather than the apex may reduce the likelihood of perforation (see Figure 2 and Figure 3).
Table 6.
Strengths and weaknesses of leadless pacing.
Despite their potential problems, LPs are associated with a substantially lower overall complication rate, mainly caused by a low rate of long-term complications [30]. The major advantage of LPs is the elimination of lead and pocket-related complications. Avoiding pocket and lead revision reduces the rate of infection. This predominantly reflects the lack of a subcutaneous pocket (the major source of device-related infection) and to a lesser extent the absence of transvenous leads [30]. In a sub-analysis of Micra PAR, 105 patients had Micra LP implanted after extraction of an infected TV-PPM (37% of Micra were implanted the same day as device removal and lead extraction) [65,69]. No reinfection of the Micra LP was seen [65].
10. Investigational Devices *
* = Without FDA approval, without CE mark or without both.
Boston Scientific has investigated the use of a Modular CRM (modular cardiac rhythm) management system (mCRM™). The system combines use of a subcutaneous ICD (EMBLEM™ S-ICD) and a leadless pacemaker EMPOWER™ LP. Modular CRM therapy aims to reduce the risk of transvenous leads while providing the option to pace for bradycardia or receive antitachycardia pacing (ATP) for ventricular tachyarrhythmias [66].
Knops et al. recently reported results from a multinational, single-group study that enrolled patients at risk of sudden death from ventricular arrhythmias and followed them for six months after implantation of the modular pacemaker–defibrillator system [67]. The investigators enrolled 293 patients and 151 completed the 6-month follow-up period. Wireless device communication was successful in 98.8% of communication tests and 97.5% were free from leadless pacemaker-related major complications. Pacing thresholds ≤ 2.0 V were achieved in 97.4% [67].
The combined system exceeded performance goals for freedom from major complications. Eight patients died. None of the deaths were judged to be related to arrhythmias or the implantation procedure [67]. Boston Scientific will pursue FDA approval for the EMPOWER leadless pacemaker and mCRM system in 2025 [73].
The subcutaneous ICD (S-ICD) was developed to avoid the vascular risks of transvenous ICDs. The first S-ICD, the SQRX (Cameron Health, San Clemente, CA, USA), was approved by the United States Food and Drug Administration in 2012. Cameron Health was acquired by Boston Scientific (Natick, MA, USA) and the second and third generations of the device were released in 2015 and 2016 [74]. In a secondary analysis of the PRAETORIAN trial, significantly fewer lead-related complications and systemic infections occurred in the S-ICD group compared with the TV-ICD group (p < 0.001, p = 0.03, respectively). In addition, more complications required invasive interventions in the TV-ICD group compared with the S-ICD group (8.3% vs. 4.3%, HR: 0.59; p = 0.047) [75]. Medtronic has developed an extravascular implantable cardioverter-defibrillator (ICD) that has a substernally implanted single lead to enable pause-prevention pacing, antitachycardia pacing, and defibrillation energy, similar to transvenous ICDs [76]. While none of these devices are leadless, they send a clear message that transvenous leads are an imperfect option.
Cardiac physiological pacing (CPP) refers to any form of cardiac pacing intended to restore or preserve synchrony of ventricular contraction. Biventricular (BiV) pacing is the most common method used to achieve resynchronization. Left ventricular leads are usually implanted epicardially via the coronary sinus (CS) into the cardiac veins (Figure 5), ideally targeting areas of late activation (most often the lateral or posterolateral wall) [77,78]. When CRT cannot be obtained with a CS LV lead due to anatomical or functional considerations, options include surgical placement of an epicardial lead, His-bundle pacing and left bundle branch pacing [77]. His-bundle pacing has been limited by relatively high pacing thresholds and lead instability. Left bundle branch pacing has been increasingly used because it overcomes those issues and is more likely to result in the narrowing of the QRS complex when conduction disease is more distal [79].
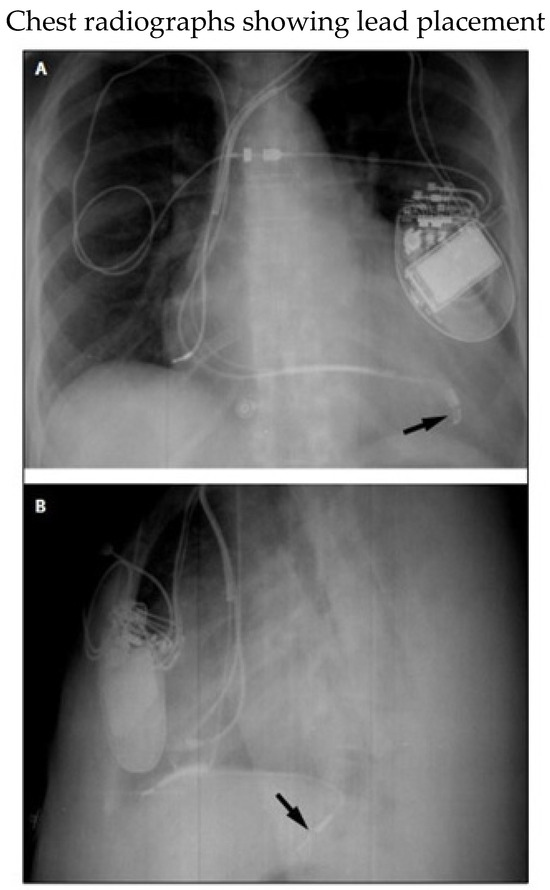
Figure 5.
(A) Posteroanterior and (B) lateral radiographs showing tip of left ventricular lead (arrows) in a tributary of the middle cardiac vein. Despite proximity to the left hemidiaphragm, phrenic near stimulation did not take place. The right ventricular lead points anteriorly toward the rib cage. Reproduced from reference [78] with permission.
Reasons for failure or abandonment of CRT with BiV pacing include: venous inaccessibility (subclavian, innominate vein, or superior vena cava occlusion), CS inaccessibility (occlusion, dissection, perforation, obstructive Thebesian valve), cardiac vein inaccessibility (small, angulated, or tortuous vein branches), suboptimal vein location (non-lateral vein, anterior interventricular vein), persistent SVC, poor lead stability (prone to dislodgment), high-capture thresholds, diaphragmatic stimulation, and major complications such as pericardial effusion/tamponade, CS or vascular dissection, sustained ventricular tachyarrhythmias/cardiac arrest, pulmonary embolism, respiratory failure or stroke [77]. These issues make potential leadless options exciting.
The Wireless Stimulation Endocardial for Cardiac Resynchronization (WiSE-CRT) system (EBR Systems, Sunnyvale, CA, USA) includes a receiver electrode (9.1 mm × 2.7 mm) that can be implanted (via a retrograde aortic or transseptal approach) in the left ventricular endocardium, a transmitter implanted in the intercostal space that detects RV pacing and delivers ultrasound energy to the receiver electrode, and a battery. The receiver electrode transforms ultrasound energy into electrical energy which results in LV pacing [69,80] (Figure 6).
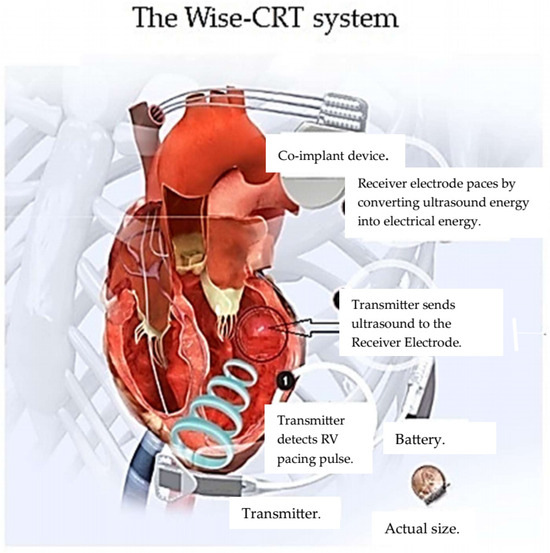
Figure 6.
Adapted from reference [81] with permission.
In the SELECT-LV (Safety and Performance of Electrodes implanted in the Left Ventricle) multi-center non-randomized trial, 35 patients received the new WiSE-CRT system after failing conventional CRT. Implantation was successful in 34 patients (97.1%). Biventricular pacing was seen in 33 patients (97.1%) at one month. Clinical improvement was achieved in 84.8% of patients. An improvement > 5% in left ventricular ejection fraction was noted in 66%. Serious complications within 24 h occurred in 3 patients. Additional complications occurred in 8 patients after 24 h. These included VF during implantation in one patient, electrode embolization, groin complications, pocket complications, and one cerebrovascular accident [69,81].
Subsequently, 90 patients from 14 European centers underwent WiSE-CRT system implantation. The system was successfully implanted in 85 (94.4%) patients. Improvement in heart failure symptoms occurred in seventy percent of patients. However, acute (<24 h), 1- to 30-day, and 1- to 6-month complications rates were 4.4%, 18.8%, and 6.7%, respectively. Five deaths (5.6%) occurred within 6 months (three were procedure-related). Because 76% of complications occurred within centers’ first 10 procedures, the authors speculated that a learning curve was likely involved in implantation outcomes [69,82].
Data presented at a late-breaking session at Heart Rhythm Society 2023 from the SOLVE-CRT study revealed that the safety and efficacy end points were met with a 16.4% improvement in cardiac function (p = 0.003) and an absence of device and procedure-related complications in 80.9 percent of patients (p < 0.001) [83,84,85]. The FDA granted the WiSE-CRT system a Breakthrough Device designation, supporting priority review and paving the way for premarket approval [85]. The WiSE-CRT system received European CE mark approval in 2015.
In 2019, Funasako and colleagues reported two cases of a totally leadless biventricular pacing approach. The Micra Transcatheter Pacemaker System was used for RV pacing and was combined with the WiSE-CRT wireless endocardial pacing system to achieve their goal [86].
The first patient had long-standing persistent atrial fibrillation (AF) with a rapid ventricular response. Following Micra implantation, AV junction ablation was performed. Unfortunately, the patient developed LV systolic dysfunction (EF 33%) and heart failure. Subsequently, the WiSE-CRT system was added. At a 6-month follow-up, the patient reported symptomatic improvement and transthoracic echocardiography revealed normalization of the LV ejection fraction [86].
The second patient had previously undergone mitral and tricuspid annuloplasty along with a bilateral maze procedure for persistent AF. However, AF continued, and the patient suffered episodes of complete AV block. A Micra device was implanted 1-year post-cardiac surgery. Due to progressive LV dysfunction (EF 25%), a WiSE LV system was implanted [86].
One week after a WiSE LV system was implanted, the patient’s symptoms of heart failure resolved. At a 6-month follow-up, the patient was completely asymptomatic and reported large increases in exercise tolerance and quality of life [86].
In 2021, Carabelli et al. reported eight patients with indications for both Micra and WiSE-CRT systems due to one of the following: (a) heart failure related to a high burden of RV pacing by Micra; (b) the need to remove a previously infected CRT system and/or perceived persistent high risk of further system infection; or (c) anatomical conditions such as venous obstruction or difficult coronary sinus anatomy that resulted in failed attempts at conventional CRT system implantation [69,87].
Similarly to the procedure described in Funasako’s report [86], the WiSE system was implanted in two steps. The battery was implanted subcutaneously at the midaxillary line and connected to the transmitter. The transmitter was placed in the fourth to sixth intercostal spaces lateral to the left parasternal border at a site (confirmed by echocardiography) with a lung- and bone-free acoustic window to the left ventricle [87]. Subsequently, a combination of fluoroscopy, echocardiography, electrical timing and pacing thresholds was used to identify an appropriate endocardial LV pacing site. Once this was determined, the electrode was deployed and anchored into the LV endocardium [87].
Seven patients reached the 6-month follow-up (one died at 4 months due to acute heart failure). The others had significant improvement in left ventricular EF (+11.29 ± 8.46%; p = 0.018) and four patients had an improvement in LVEF ≥10% [87]. In both studies, QRS duration decreased after the WiSE system was turned on [86,87].
11. Conclusions
Leadless pacing is an exciting clinical option and is associated with rapidly evolving technology. It offers physicians and many patients a viable alternative to transvenous pacing. It is particularly enticing as a way to reduce procedural morbidity, particularly the risk of infection, because pocket formation is not needed. It offers an opportunity to replace an infected transvenous device and minimize or eliminate recurrent infection. It is clear that implanters require a learning curve, and lack of experience may result in more complications. Cardiac perforation and pericardial effusions/cardiac tamponade remain the most problematic issues. Although likely to be controversial, recommendations suggest that leadless device implantation should not take place in centers that do not perform cardiac surgery. Optimal management of these devices at end of life remains uncertain and time will tell whether extraction or simply adding a new device is more advantageous.
Supplementary Materials
The following supporting information can be downloaded at: https://www.mdpi.com/article/10.3390/mi16010089/s1. The supplement is referenced independently of the main text.
Funding
This research received no external funding.
Conflicts of Interest
Richard G. Trohman reported serving as an advisor to Boston Scientific/Guidant; receiving research grants from Boston Scientific/Guidant, Medtronic Inc, St Jude Medical (Abbott), Vitatron, and Wyeth- Ayerst/Wyeth Pharmaceuticals; serving as a consultant for Biosense Webster, Alta Thera Pharmaceuticals and Newron Pharmaceuticals P.s.A.; and receiving speakers fees or honoraria Boston Scientific/Guidant CRM, Medtronic Inc, Daiichi Sankyo, Alta Thera Pharmaceuticals and St Jude Medical (Abbott). Richard G. Trohman was not involved in the selection of peer reviewers for the manuscript nor any of the subsequent editorial decisions. Richard G. Trohman attests that these potential conflicts of interest did not influence the contents of this manuscript.
References
- Hyman, A.S. Resuscitation of the Stopped Heart by Intracardial Therapy: II. Experimental use of an Artificial Pacemaker. Arch. Intern. Med. 1932, 50, 283–305. [Google Scholar] [CrossRef]
- Furman, S. Early history of cardiac pacing and defibrillation. Indian Pacing Electrophysiol. J. 2002, 2, 2–3. [Google Scholar] [PubMed] [PubMed Central]
- Madias, C.; Trohman, R.G. Cardiac resynchronization therapy: The state of the art. Expert. Rev. Cardiovasc. Ther. 2014, 12, 573–587. [Google Scholar] [CrossRef] [PubMed]
- Bigelow, W.G.; Callaghan, J.C.; Hopps, J.A. General hypothermia for experimental intracardiac surgery; the use of electrophrenic respirations, an artificial pacemaker for cardiac standstill and radio-frequency rewarming in general hypothermia. Ann. Surg. 1950, 132, 531–539. [Google Scholar] [CrossRef]
- Zoll, P.M. Resuscitation of the heart in ventricular standstill by external electric stimulation. N. Engl. J. Med. 1952, 247, 768–771. [Google Scholar] [CrossRef]
- Lemberg, L.; Castellanos, A., Jr.; Berkovits, B.V. Pacemaking on Demand in AV Block. JAMA 1965, 191, 12–14. [Google Scholar] [CrossRef] [PubMed]
- Sutton, R.F.J.; Linde, C.; Benditt, D.G. History of electrical therapy for the heart. Eur. Heart J. Suppl. 2007, 9 (Suppl. SI), I3–I10. [Google Scholar] [CrossRef][Green Version]
- Rickards, A.F.; Norman, J. Relation between QT interval and heart rate. New design of physiologically adaptive cardiac pacemaker. Br. Heart J. 1981, 45, 56–61. [Google Scholar] [CrossRef] [PubMed] [PubMed Central]
- Cazeau, S.; Ritter, P.; Bakdach, S.; Lazarus, A.; Limousin, M.; Henao, L.; Mundler, O.; Daubert, J.C.; Mugica, J. Four chamber pacing in dilated cardiomyopathy. Pacing Clin. Electrophysiol. 1994, 17 Pt 2, 1974–1979. [Google Scholar] [CrossRef] [PubMed]
- Daubert, J.C.; Ritter, P.; Le Breton, H.; Gras, D.; Leclercq, C.; Lazarus, A.; Mugica, J.; Mabo, P.; Cazeau, S. Permanent left ventricular pacing with transvenous leads inserted into the coronary veins. Pacing Clin. Electrophysiol. 1998, 21 Pt 2, 239–245. [Google Scholar] [CrossRef] [PubMed]
- Nichols, M. European Perspectives. Spotlight: Angelo Auricchio, MD, PhD, FESC. Circulation 2009, 120, f85–f90. [Google Scholar]
- Auricchio, A.; Klein, H.; Tockman, B.; Sack, S.; Stellbrink, C.; Neuzner, J.; Kramer, A.; Ding, J.; Pochet, T.; Maarse, A.; et al. Transvenous biventricular pacing for heart failure: Can the obstacles be overcome? Am. J. Cardiol. 1999, 83, 136–142. [Google Scholar] [CrossRef] [PubMed]
- Sharma, P.S.; Vijayaraman, P. His Bundle Pacing Or Biventricular Pacing For Cardiac Resynchronization Therapy In Heart Failure: Discovering New Methods For An Old Problem. J. Atr. Fibrillation 2016, 9, 1501. [Google Scholar] [CrossRef] [PubMed] [PubMed Central]
- Arnold, A.D.; Shun-Shin, M.J.; Keene, D.; Howard, J.P.; Sohaib, S.M.A.; Wright, I.J.; Cole, G.D.; Qureshi, N.A.; Lefroy, D.C.; Koa-Wing, M.; et al. His Resynchronization Versus Biventricular Pacing in Patients With Heart Failure and Left Bundle Branch Block. J. Am. Coll. Cardiol. 2018, 72, 3112–3122. [Google Scholar] [CrossRef] [PubMed] [PubMed Central]
- Ponnusamy, S.S.; Arora, V.; Namboodiri, N.; Kumar, V.; Kapoor, A.; Vijayaraman, P. Left bundle branch pacing: A comprehensive review. J. Cardiovasc. Electrophysiol. 2020, 31, 2462–2473. [Google Scholar] [CrossRef] [PubMed]
- Vijayaraman, P.; Zalavadia, D.; Haseeb, A.; Dye, C.; Madan, N.; Skeete, J.R.; Vipparthy, S.C.; Young, W.; Ravi, V.; Rajakumar, C.; et al. Clinical outcomes of conduction system pacing compared to biventricular pacing in patients requiring cardiac resynchronization therapy. Heart Rhythm. 2022, 19, 1263–1271. [Google Scholar] [CrossRef] [PubMed]
- Link, M.S. Pacing System Malfunction: Evaluation and Management. Available online: https://www.uptodate.com/contents/pacing-system-malfunction-evaluation-and-management?search=pacing%20lead%20problems&source=search_result&selectedTitle=3%7E150&usage_type=default&display_rank=3 (accessed on 5 July 2024).
- Ohlow, M.A.; Roos, M.; Lauer, B.; Von Korn, H.; Geller, J.C. Incidence, predictors, and outcome of inadvertent malposition of transvenous pacing or defibrillation lead in the left heart. Europace 2016, 18, 1049–1054. [Google Scholar] [CrossRef]
- Trohman, R.G.; Wilkoff, B.L.; Byrne, T.; Cook, S. Successful percutaneous extraction of a chronic left ventricular pacing lead. Pacing Clin. Electrophysiol. 1991, 14, 1448–1451. [Google Scholar] [CrossRef] [PubMed]
- Mulpuru, S.K.; Madhavan, M.; McLeod, C.J.; Cha, Y.-M.; Friedman, P.A. Cardiac Pacemakers: Function, Troubleshooting, and Management: Part 1 of a 2-Part Series. J. Am. Coll. Cardiol. 2017, 69, 189–210. [Google Scholar] [CrossRef]
- Knight, B.P. Subtle Differences in IS-1 Pacing Leads from Different Companies Result in a New Lead-Device Compatibility Problem. EP Lab. Digest. 2018, 18. Available online: https://www.hmpgloballearningnetwork.com/site/eplab/articles/subtle-differences-1-pacing-leads-different-companies-results-new-lead-device (accessed on 5 July 2024).
- Pfensig, S.; Arbeiter, D.; Stiehm, M.; Grabow, N.; Schmitz, K.-P.; Siewert, S. In vitro biostability of cardiac pacemaker lead insulations under static mechanical loading. Curr. Dir. Biomed. Eng. 2022, 8, 447–450. [Google Scholar] [CrossRef]
- Haqqani, H.M.; Epstein, L.M.; Cooper, J.M. Engineering and Construction of Pacemaker and ICD Leads. Available online: https://Clinicalgate.com/ (accessed on 11 June 2024).
- Trohman, R.G.; Sharma, P.S. Detecting and managing device leads inadvertently placed in the left ventricle. Cleve Clin. J. Med. 2018, 85, 69–75. [Google Scholar] [CrossRef] [PubMed]
- Spickler, J.W.; Rasor, N.S.; Kezdi, P.; Misra, S.N.; Robins, K.E.; LeBoeuf, C. Totally self-contained intracardiac pacemaker. J. Electrocardiol. 1970, 3, 325–331. [Google Scholar] [CrossRef] [PubMed]
- Reddy, V.Y.; Knops, R.E.; Sperzel, J.; Miller, M.A.; Petru, J.; Simon, J.; Sediva, L.; de Groot, J.R.; Tjong, F.V.; Jacobson, P.; et al. Permanent leadless cardiac pacing: Results of the LEADLESS trial. Circulation 2014, 129, 1466–1471. [Google Scholar] [CrossRef] [PubMed]
- Micra™. AV Product Specifications. Available online: https://www.medtronic.com/content/dam/medtronic-wide/public/united-states/products/cardiac-vascular/cardiac-rhythm/pacing-systems/micra-av2-spec-sheet.pdf (accessed on 24 November 2024).
- Micra™. VR2 Leadless Pacemaker. Available online: https://www.medtronic.com/en-us/healthcare-professionals/products/cardiac-rhythm/pacing-systems/pacemakers/micra-vr2-leadless-pacemaker.html (accessed on 24 November 2024).
- Aveir™. Leadless Pacemaker, Model LSP201A, LSP202V Specifications and Characterisitics. Available online: https://www.accessdata.fda.gov/cdrh_docs/pdf15/P150035S003B.pdf (accessed on 24 November 2024).
- Breeman, K.T.N.; Tjong, F.V.Y.; Miller, M.A.; Neuzil, P.; Dukkipati, S.; Knops, R.E.; Reddy, V.Y. Ten Years of Leadless Cardiac Pacing. J. Am. Coll. Cardiol. 2024, 84, 2131–2147. [Google Scholar] [CrossRef] [PubMed]
- Knops, R.E.; Tjong, F.V.; Neuzil, P.; Sperzel, J.; Miller, M.A.; Petru, J.; Simon, J.; Sediva, L.; de Groot, J.R.; Dukkipati, S.R.; et al. Chronic performance of a leadless cardiac pacemaker: 1-year follow-up of the LEADLESS trial. J. Am. Coll. Cardiol. 2015, 65, 1497–1504. [Google Scholar] [CrossRef] [PubMed]
- Reddy, V.Y.; Exner, D.V.; Cantillon, D.J.; Doshi, R.; Bunch, T.J.; Tomassoni, G.F.; Friedman, P.A.; Estes, N.A., 3rd; Ip, J.; Niazi, I.; et al. Percutaneous Implantation of an Entirely Intracardiac Leadless Pacemaker. N. Engl. J. Med. 2015, 373, 1125–1135. [Google Scholar] [CrossRef] [PubMed]
- Reddy, V.Y.; Exner, D.V.; Doshi, R.; Tomassoni, G.; Bunch, T.J.; Estes, N.M.; Neužil, P.; Paulin, F.L.; Guerrero, J.J.G.; Cantillon, D.J. Primary Results on Safety and Efficacy From the LEADLESS II–Phase 2 Worldwide Clinical Trial. J. Am. Coll. Cardiol. EP 2022, 8, 115–117. [Google Scholar] [CrossRef]
- Ritter, P.; Duray, G.Z.; Steinwender, C.; Soejima, K.; Omar, R.; Mont, L.; Boersma, L.V.; Knops, R.E.; Chinitz, L.; Zhang, S.; et al. Early performance of a miniaturized leadless cardiac pacemaker: The Micra Transcatheter Pacing Study. Eur. Heart J. 2015, 36, 2510–2519. [Google Scholar] [CrossRef] [PubMed] [PubMed Central]
- Reynolds, D.; Duray, G.Z.; Omar, R.; Soejima, K.; Neuzil, P.; Zhang, S.; Narasimhan, C.; Steinwender, C.; Brugada, J.; Lloyd, M.; et al. A Leadless Intracardiac Transcatheter Pacing System. N. Engl. J. Med. 2016, 374, 533–541. [Google Scholar] [CrossRef] [PubMed]
- Duray, G.Z.; Ritter, P.; El-Chami, M.; Narasimhan, C.; Omar, R.; Tolosana, J.M.; Zhang, S.; Soejima, K.; Steinwender, C.; Rapallini, L.; et al. Long-term performance of a transcatheter pacing system: 12-Month results from the Micra Transcatheter Pacing Study. Heart Rhythm. 2017, 14, 702–709. [Google Scholar] [CrossRef] [PubMed]
- Soto, G.E. Pacemaker syndrome: Thinking beyond atrioventricular dyssynchrony. HeartRhythm Case Rep. 2024, 10, 273–275. [Google Scholar] [CrossRef] [PubMed] [PubMed Central]
- Roberts, P.R.; Clementy, N.; Al Samadi, F.; Garweg, C.; Martinez-Sande, J.L.; Iacopino, S.; Johansen, J.B.; Vinolas Prat, X.; Kowal, R.C.; Klug, D.; et al. A leadless pacemaker in the real-world setting: The Micra Transcatheter Pacing System Post-Approval Registry. Heart Rhythm. 2017, 14, 1375–1379. [Google Scholar] [CrossRef] [PubMed]
- El-Chami, M.F.; Garweg, C.; Clementy, N.; Al-Samadi, F.; Iacopino, S.; Martinez-Sande, J.L.; Roberts, P.R.; Tondo, C.; Johansen, J.B.; Vinolas-Prat, X.; et al. Leadless pacemakers at 5-year follow-up: The Micra transcatheter pacing system post-approval registry. Eur. Heart J. 2024, 45, 1241–1251. [Google Scholar] [CrossRef] [PubMed] [PubMed Central]
- Knops, R.E.; Reddy, V.Y.; Ip, J.E.; Doshi, R.; Exner, D.V.; Defaye, P.; Canby, R.; Bongiorni, M.G.; Shoda, M.; Hindricks, G.; et al. A Dual-Chamber Leadless Pacemaker. N. Engl. J. Med. 2023, 388, 2360–2370. [Google Scholar] [CrossRef] [PubMed]
- Mond, H.G.; Proclemer, A. The 11th world survey of cardiac pacing and implantable cardioverter-defibrillators: Calendar year 2009--a World Society of Arrhythmia’s project. Pacing Clin. Electrophysiol. 2011, 34, 1013–1027. [Google Scholar] [CrossRef] [PubMed]
- Unmatched Innovation: Setting the Pace with FDA-Approved AVEIR™ AR Atrial Leadless Pacemaker. Available online: https://www.cardiovascular.abbott/us/en/hcp/products/cardiac-rhythm-management/blog/unmatched-innovation-setting-pace-with-fda-approved-aveir-ar.html (accessed on 23 July 2024).
- Abbott Receives FDA Approval for World’s First Dualchamber Leadless Pacemaker. Available online: https://abbott.mediaroom.com/2023-07-05-Abbott-Receives-FDA-Approval-for-Worlds-First-Dual-Chamber-Leadless-Pacemaker (accessed on 23 July 2024).
- El-Chami, M.F.; Bhatia, N.K.; Merchant, F.M. Atrio-ventricular synchronous pacing with a single chamber leadless pacemaker: Programming and trouble shooting for common clinical scenarios. J. Cardiovasc. Electrophysiol. 2021, 32, 533–539. [Google Scholar] [CrossRef] [PubMed] [PubMed Central]
- Micra AV2 and Micra VR2 Pacemakers-Updated Features. Available online: https://www.medtronicacademy.com/en-us/learning-plan/micra-leadless-pacing-systems (accessed on 31 July 2024).
- Steinwender, C.; Khelae, S.K.; Garweg, C.; Chan, J.Y.S.; Ritter, P.; Johansen, J.B.; Sagi, V.; Epstein, L.M.; Piccini, J.P.; Pascual, M.; et al. Atrioventricular Synchronous Pacing Using a Leadless Ventricular Pacemaker: Results From the MARVEL 2 Study. JACC Clin. Electrophysiol. 2020, 6, 94–106. [Google Scholar] [CrossRef] [PubMed]
- Chinitz, L.A.; El-Chami, M.F.; Sagi, V.; Garcia, H.; Hackett, F.K.; Leal, M.; Whalen, P.; Henrikson, C.A.; Greenspon, A.J.; Sheldon, T.; et al. Ambulatory atrioventricular synchronous pacing over time using a leadless ventricular pacemaker: Primary results from the AccelAV study. Heart Rhythm. 2023, 20, 46–54. [Google Scholar] [CrossRef] [PubMed]
- Puette, J.A.; Malek, R.; Ellison, M.B. Pacemaker. In StatPearls [Internet]; StatPearls Publishing: Treasure Island, FL, USA, 2024; Available online: https://www.ncbi.nlm.nih.gov/books/NBK526001/ (accessed on 12 September 2022).
- Medtronic Receives CE Mark for Its Next Generation Micra Leadless Pacing Systems. Available online: https://news.medtronic.com/2024-01-05-Medtronic-receives-CE-Mark-for-its-next-generation-Micra-leadless-pacing-systems (accessed on 25 July 2024).
- Molitor, N.; Saleem-Talib, S.; Ramanna, H.; Hofer, D.; Breitenstein, A.; Steffel, J. Leadless pacemaker implantation via the internal jugular vein. Europace 2024, 26, euae199. [Google Scholar] [CrossRef] [PubMed] [PubMed Central]
- El-Chami, M.F.; Shah, A.D. How to implant leadless pacemakers and mitigate major complications. Heart Rhythm. 2023, 20, 754–759. [Google Scholar] [CrossRef] [PubMed]
- Atti, V.; Turagam, M.K.; Garg, J.; Koerber, S.; Angirekula, A.; Gopinathannair, R.; Natale, A.; Lakkireddy, D. Subclavian and Axillary Vein Access Versus Cephalic Vein Cutdown for Cardiac Implantable Electronic Device Implantation: A Meta-Analysis. JACC Clin. Electrophysiol. 2020, 6, 661–671. [Google Scholar] [CrossRef] [PubMed]
- Cantillon, D.J.; Exner, D.V.; Badie, N.; Davis, K.; Gu, N.Y.; Nabutovsky, Y.; Doshi, R. Complications and Health Care Costs Associated With Transvenous Cardiac Pacemakers in a Nationwide Assessment. JACC Clin. Electrophysiol. 2017, 3, 1296–1305. [Google Scholar] [CrossRef] [PubMed]
- Vouliotis, A.I.; Roberts, P.R.; Dilaveris, P.; Gatzoulis, K.; Yue, A.; Tsioufis, K. Leadless Pacemakers: Current Achievements and Future Perspectives. Eur. Cardiol. 2023, 18, e49. [Google Scholar] [CrossRef] [PubMed] [PubMed Central]
- Malaczynska-Rajpold, K.; Elliot, M.; Wijesuriya, N.; Mehta, V.; Wong, T.; Rinaldi, C.A.; Behar, J.M. Leadless Cardiac Pacing: New Horizons. Cardiol. Ther. 2023, 12, 21–33. [Google Scholar] [CrossRef] [PubMed] [PubMed Central]
- Della Rocca, D.G.; Gianni, C.; Di Biase, L.; Natale, A.; Al-Ahmad, A. Leadless Pacemakers: State of the Art and Future Perspectives. Card. Electrophysiol. Clin. 2018, 10, 17–29. [Google Scholar] [CrossRef] [PubMed]
- Gupta, A.; Halleran, S.M.; Krishnan, K.; Trohman, R.G. Rescue permanent iliac vein pacing after epicardial lead failure: An unusual reversal of pacing fortune. Europace 2008, 10, 1236–1238. [Google Scholar] [CrossRef] [PubMed]
- Boveda, S.; Lenarczyk, R.; Haugaa, K.H.; Iliodromitis, K.; Finlay, M.; Lane, D.; Prinzen, F.W.; Dagres, N. Use of leadless pacemakers in Europe: Results of the European Heart Rhythm Association survey. Europace 2018, 20, 555–559. [Google Scholar] [CrossRef] [PubMed]
- Glikson, M.; Nielsen, J.C.; Kronborg, M.B.; Michowitz, Y.; Auricchio, A.; Barbash, I.M.; Barrabés, J.A.; Boriani, G.; Braunschweig, F.; Brignole, M.; et al. 2021 ESC Guidelines on cardiac pacing and cardiac resynchronization therapy: Developed by the Task Force on cardiac pacing and cardiac resynchronization therapy of the European Society of Cardiology (ESC) With the special contribution of the European Heart Rhythm Association (EHRA). Eur. Heart J 2021, 42, 3427–3520, Corrigendum at Eur. Heart J. 2021, 42, 4901https://doi.org/10.1093/eurheartj/ehab670.. [Google Scholar] [CrossRef]
- Haddadin, F.; Majmundar, M.; Jabri, A.; Pecha, L.; Scott, C.; Daher, M.; Kumar, A.; Kalra, A.; Fram, R.; Haddadin, F.; et al. Clinical outcomes and predictors of complications in patients undergoing leadless pacemaker implantation. Heart Rhythm. 2022, 19, 1289–1296. [Google Scholar] [CrossRef] [PubMed]
- Leadless Pacemaker. Available online: https://my.clevelandclinic.org/health/treatments/17166-pacemakers-leadless-pacemaker (accessed on 2 November 2024).
- Aveir DR Dual-Chamber Leadless Pacemaker Looks Solid at 1 Year. Available online: https://www.tctmd.com/news/aveir-dr-dual-chamber-leadless-pacemaker-looks-solid-1-year#:~:text=Knops%20acknowledged%20that%20all%20of%20that%20communication%20between,device%20and%2011.3%20years%20for%20the%20ventricular%20device (accessed on 2 November 2024).
- Pasupula, D.K.; Rajaratnam, A.; Rattan, R.; Munir, M.B.; Ahmad, S.; Adelstein, E.; Jain, S.; Wang, N.C.; Saba, S. Trends in hospital admissions for and readmissions after cardiac implantable electronic device procedures in the United States: An analysis from 2010 to 2014 using the National Readmission Database. Mayo. Clin. Proc. 2019, 94, 588–598. [Google Scholar] [CrossRef] [PubMed]
- El-Chami, M.F.; Clementy, N.; Garweg, C.; Omar, R.; Duray, G.Z.; Gornick, C.C.; Leyva, F.; Sagi, V.; Piccini, J.P.; Soejima, K.; et al. Leadless pacemaker implantation in hemodialysis patients: Experience with the Micra Transcatheter Pacemaker. J. Am. Coll. Cardiol. EP 2019, 5, 162–170. [Google Scholar]
- El-Chami, M.F.; Johansen, J.B.; Zaidi, A.; Faerestrand, S.; Reynolds, D.; Garcia-Seara, J.; Mansourati, J.; Pasquie, J.L.; McElderry, H.T.; Roberts, P.R.; et al. Leadless pacemaker implant in patients with pre-existing infections: Results from the Micra postapproval registry. J. Cardiovasc. Electrophysiol. 2019, 30, 569–574. [Google Scholar] [CrossRef] [PubMed] [PubMed Central]
- Modular CRM (mCRM™) System. Available online: https://www.bostonscientific.com/en-US/products/defibrillators/emblem-s-icd-system/modular-crm-system.html (accessed on 24 July 2024).
- Knops, R.E.; Lloyd, M.S.; Roberts, P.R.; Wright, D.J.; Boersma, L.V.; Doshi, R.; Friedman, P.A.; Neuzil, P.; Blomström-Lundqvist, C.; Bongiorni, M.G.; et al. A Modular Communicative Leadless Pacing-Defibrillator System. N. Engl. J. Med. 2024. Epub ahead of print. [Google Scholar] [CrossRef] [PubMed]
- Tjong, F.V.; Reddy, V.Y. Permanent Leadless Cardiac Pacemaker Therapy: A Comprehensive Review. Circulation 2017, 135, 1458–1470. [Google Scholar] [CrossRef] [PubMed]
- Ibrahim, R.; Khoury, A.; El-Chami, M.F. Leadless Pacing: Where We Currently Stand and What the Future Holds. Curr. Cardiol. Rep. 2022, 24, 1233–1240. [Google Scholar] [CrossRef] [PubMed]
- Hauser, R.G.; Gornick, C.C.; Abdelhadi, R.H.; Tang, C.Y.; Casey, S.A.; Sengupta, J.D. Major adverse clinical events associated with implantation of a leadless intracardiac pacemaker. Heart Rhythm. 2021, 18, 1132–1139. [Google Scholar] [CrossRef] [PubMed]
- Piccini, J.P.; Cunnane, R.; Steffel, J.; El-Chami, M.F.; Reynolds, D.; Roberts, P.R.; Soejima, K.; Steinwender, C.; Garweg, C.; Chinitz, L.; et al. Development and validation of a risk score for predicting pericardial effusion in patients undergoing leadless pacemaker implantation: Experience with the Micra transcatheter pacemaker. Europace 2022, 24, 1119–1126. [Google Scholar] [CrossRef] [PubMed] [PubMed Central]
- Boersma, L.V.; El-Chami, M.; Steinwender, C.; Lambiase, P.; Murgatroyd, F.; Mela, T.; Theuns, D.A.M.J.; Khelae, S.K.; Kalil, C.; Zabala, F.; et al. Practical considerations, indications, and future perspectives for leadless and extravascular cardiac implantable electronic devices: A position paper by EHRA/HRS/LAHRS/APHRS. Europace 2022, 24, 1691–1708. [Google Scholar] [CrossRef] [PubMed]
- MODULAR ATP Trial: Evaluating Safety, Effectiveness and Performance of the Modular CRM (mCRM™) System and EMPOWER™ Leadless Pacemaker (LP). Available online: https://www.bostonscientific.com/en-US/products/defibrillators/emblem-s-icd-system/clinical-data/appraise-modular-trials.html (accessed on 25 July 2024).
- Zeineh, N.S.; Prutkin, J.M. The Subcutaneous Implantable Cardioverter-defibrillator: New Features and Implant Techniques and Future Developments. J. Innov. Card. Rhythm. Manag. 2018, 9, 3417–3424. [Google Scholar] [CrossRef] [PubMed] [PubMed Central]
- Knops, R.E.; Pepplinkhuizen, S.; Delnoy, P.P.H.M.; Boersma, L.V.A.; Kuschyk, J.; El-Chami, M.F.; Bonnemeier, H.; Behr, E.R.; Brouwer, T.F.; Kaab, S.; et al. Device-related complications in subcutaneous versus transvenous ICD: A secondary analysis of the PRAETORIAN trial. Eur. Heart J. 2022, 43, 4872–4883. [Google Scholar] [CrossRef] [PubMed] [PubMed Central]
- Friedman, P.; Murgatroyd, F.; Boersma, L.V.; Manlucu, J.; O’donnell, D.; Knight, B.P.; Clémenty, N.; Leclercq, C.; Amin, A.; Merkely, B.P.; et al. Efficacy and Safety of an Extravascular Implantable Cardioverter-Defibrillator. N. Engl. J. Med. 2022, 387, 1292–1302. [Google Scholar] [CrossRef] [PubMed]
- Chung, M.K.; Patton, K.K.; Lau, C.-P.; Forno, A.R.D.; Al-Khatib, S.M.; Arora, V.; Birgersdotter-Green, U.M.; Cha, Y.-M.; Chung, E.H.; Cronin, E.M.; et al. 2023 HRS/APHRS/LAHRS guideline on cardiac physiologic pacing for the avoidance and mitigation of heart failure. Heart Rhythm 2023, 20, e17–e91. [Google Scholar] [CrossRef] [PubMed] [PubMed Central]
- Trohman, R.G.; Kim, M.H.; Pinski, S.L. Cardiac pacing: The state of the art. Lancet 2004, 364, 1701–1719. [Google Scholar] [CrossRef] [PubMed]
- Upadhyay, G.A.; Cherian, T.; Shatz, D.Y.; Beaser, A.D.; Aziz, Z.; Ozcan, C.; Broman, M.T.; Nayak, H.M.; Tung, R. Intracardiac delineation of septal conduction in left bundle-branch block patterns: Mechanistic evidence of left intrahisian block circumvented by His bundle pacing. Circulation 2019, 139, 1876–1888. [Google Scholar] [CrossRef]
- Reddy, V.Y.; Miller, M.A.; Neuzil, P.; Søgaard, P.; Butter, C.; Seifert, M.; Delnoy, P.P.; van Erven, L.; Schalji, M.; Boersma, L.V.A.; et al. Cardiac Resynchronization Therapy With Wireless Left Ventricular Endocardial Pacing: The SELECT-LV Study. J. Am. Coll. Cardiol. 2017, 69, 2119–2129. [Google Scholar] [CrossRef] [PubMed]
- Okabe, T.; Hummel, J.D.; Bank, A.J.; Niazi, I.K.; McGrew, F.A.; Kindsvater, S.; Oza, S.R.; Scherschel, J.A.; Walsh, M.N.; Singh, J.P. Leadless left ventricular stimulation with WiSE-CRT System—Initial experience and results from phase I of SOLVE-CRT Study (nonrandomized, roll-in phase). Heart Rhythm. 2022, 19, 22–29. [Google Scholar] [CrossRef] [PubMed]
- Sieniewicz, B.J.; Betts, T.R.; James, S.; Turley, A.; Butter, C.; Seifert, M.; Boersma, L.V.A.; Riahi, S.; Neuzil, P.; Biffi, M.; et al. Real-world experience of leadless left ventricular endocardial cardiac resynchronization therapy: A multicenter international registry of the WiSE-CRT pacing system. Heart Rhythm. 2020, 17, 1291–1297. [Google Scholar] [CrossRef] [PubMed] [PubMed Central]
- EBR Systems’ Pivotal SOLVE-CRT Trial Meets Endpoints: Excellent Interim Analysis Results Lead to Early Trial Halt for Success. Available online: https://www.prnewswire.com/news-releases/ebr-systems-pivotal-solve-crt-trial-meets-endpoints-excellent-interim-analysis-results-lead-to-early-trial-halt-for-success-301830654.html (accessed on 25 July 2024).
- Pivotal SOLVE-CRT Trial Meets Endpoints: Excellent Interim Analysis Results Lead to Early Trial Halt for Success. Available online: https://www.ebrsystemsinc.com/blog/pivotal-solve-crt-trial-meets-endpoints-excellent-interim-analysis-results-lead-to-early-trial-halt-for-success (accessed on 8 August 2024).
- Singh, J.P.; Rinaldi, C.A.; Sanders, P.; Kubo, S.H.; James, S.; Niazi, I.K.; Betts, T.R.; Butter, C.; Okabe, T.; Latacha, M.P.; et al. LB-456088-4 Safety and efficacy of a leadless ultrasound-based cardiac resynchronization pacing system in heart failure—Results from the SOLVE-CRT study. Heart Rhythm 2023, 20, 1096–1097. [Google Scholar] [CrossRef]
- Funasako, M.; Neuzil, P.; Dujka, L.; Petru, J.; Sediva, L.; Simon, J.; Hauser, T.; Baroch, J.; Reddy, V.Y. Successful implementation of a totally leadless biventricular pacing approach. HeartRhythm Case Rep. 2019, 6, 153–157. [Google Scholar] [CrossRef] [PubMed] [PubMed Central]
- Carabelli, A.; Jabeur, M.; Jacon, P.; Rinaldi, C.A.; Leclercq, C.; Rovaris, G.; Arnold, M.; Venier, S.; Neuzil, P.; Defaye, P. European experience with a first totally leadless cardiac resynchronization therapy pacemaker system. EP Europace 2021, 23, 740–747. [Google Scholar] [CrossRef]






Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2025 by the author. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).