Towards an Algorithm-Based Tailored Treatment of Acute Neonatal Hyperammonemia

 , , , ,
, , , ,
Abstract
1. Introduction
2. Results
3. Discussion
4. Materials and Methods
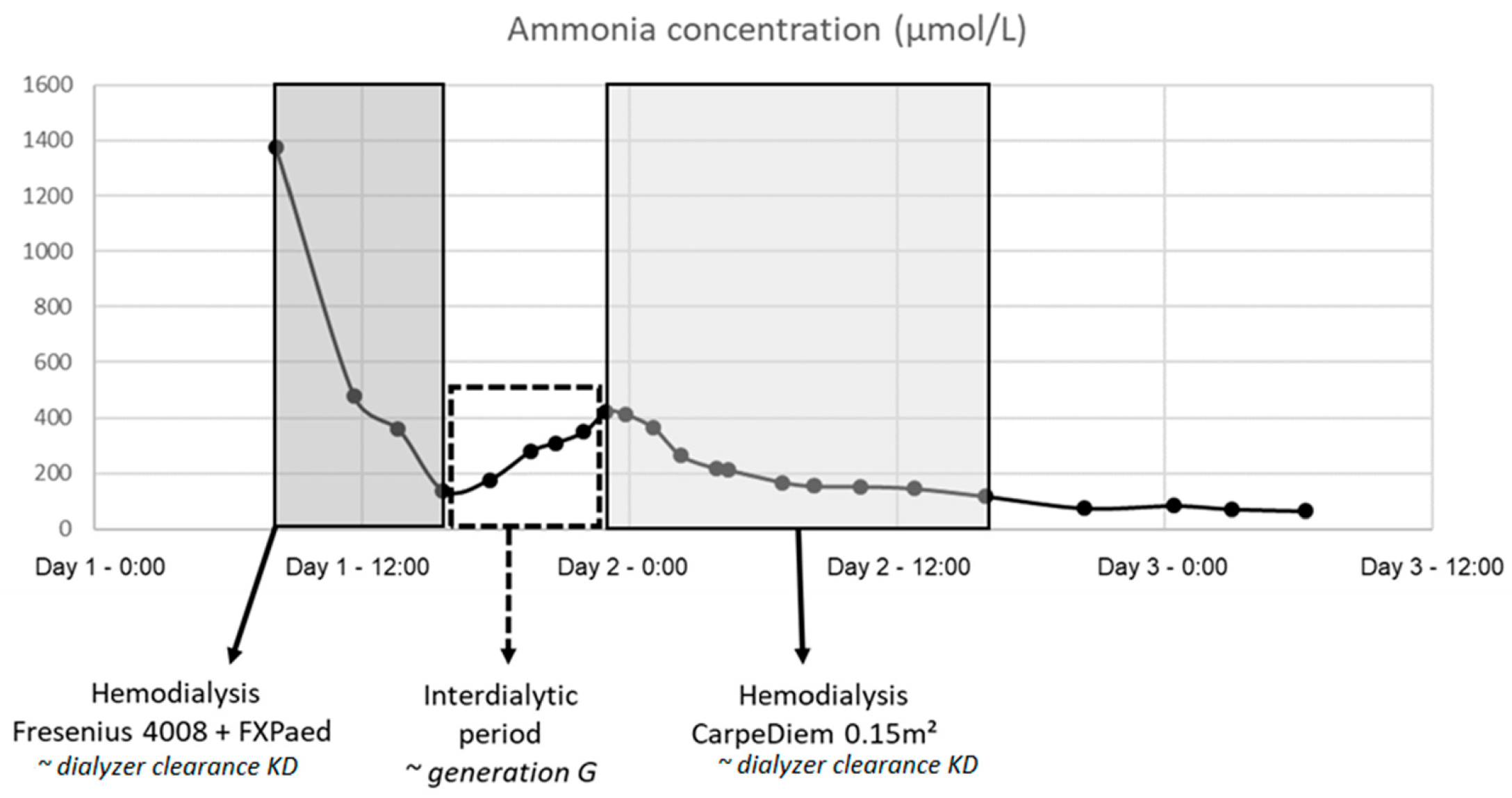
4.1. Patients, Dialyses and Blood Sampling
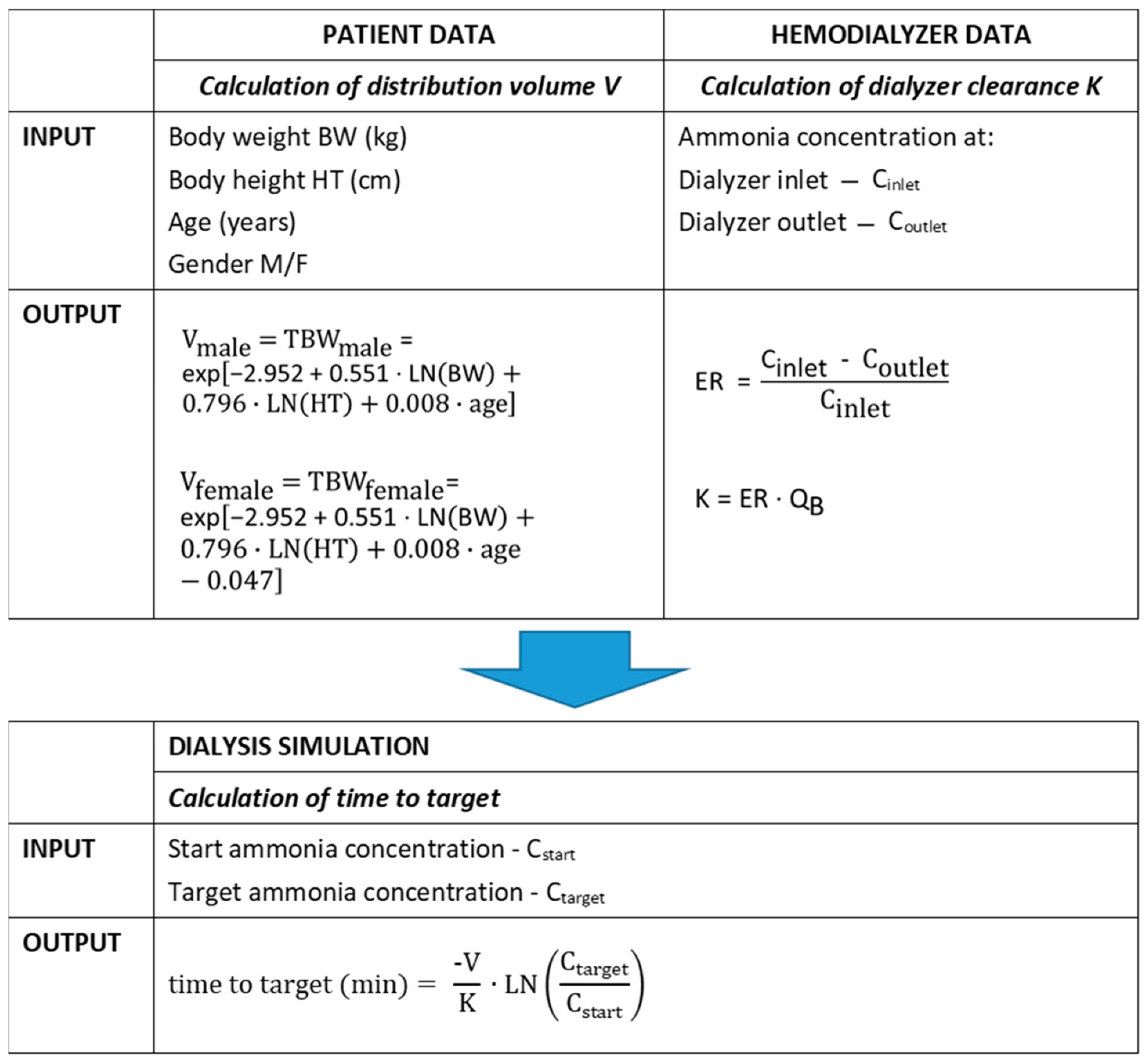
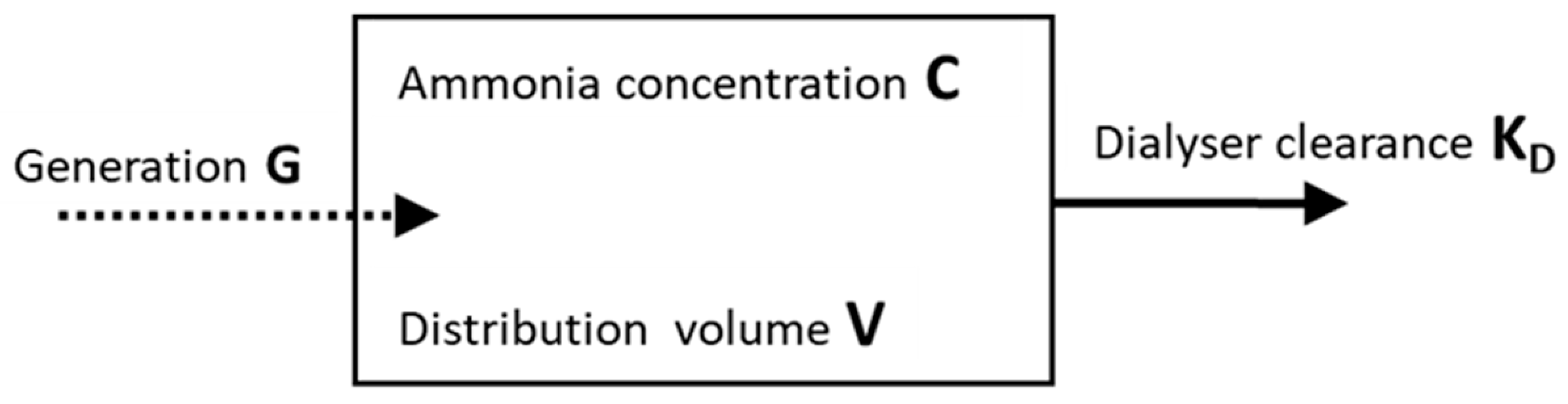
4.2. Calibration of the Kinetic Model
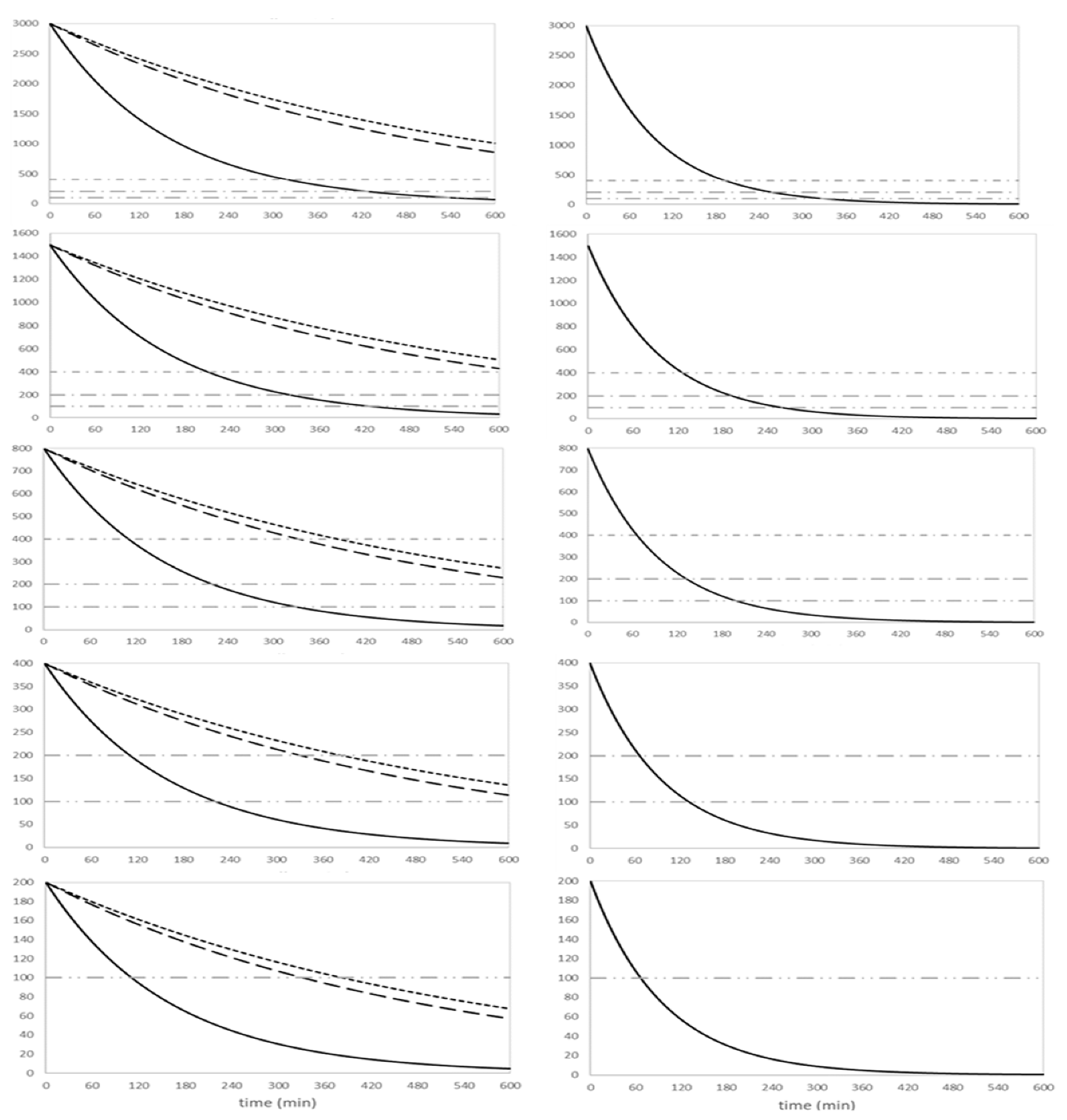
4.3. Kinetics Simulations
4.4. Optimized and Personalized Dialysis Protocol
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Enns, G.M.; Berry, S.A.; Berry, G.; Rhead, W.J.; Brusilow, S.W.; Hamosh, A. Survival after treatment with phenylacetate and benzoate for urea-cycle disorders. N. Engl. J. Med. 2007, 356, 2282–2292. [Google Scholar] [CrossRef]
- Haberle, J. Clinical practice: The management of hyperammonemia. Eur. J. Pediatr. 2011, 170, 21–34. [Google Scholar] [CrossRef]
- Häberle, J. Clinical and biochemical aspects of primary and secondary hyperammonemic disorders. Arch. Biochem. Biophys. 2013, 536, 101–108. [Google Scholar] [CrossRef]
- Häberle, J.; Chakrapani, A.; Mew, N.A.; Longo, N. Hyperammonaemia in classic organic acidaemias: A review of the literature and two case histories. Orphanet J. Rare Dis. 2018, 13, 219. [Google Scholar] [CrossRef]
- Bachmann, C. Outcome and survival of 88 patients with urea cycle disorders: A retrospective evaluation. Eur. J. Nucl. Med. Mol. Imaging 2003, 162, 410–416. [Google Scholar] [CrossRef]
- Nassogne, M.-C.; Héron, B.; Touati, G.; Rabier, D.; Saudubray, J.M. Urea cycle defects: Management and outcome. J. Inherit. Metab. Dis. 2005, 28, 407–414. [Google Scholar] [CrossRef]
- Cooper, A.J.; Plum, F. Biochemistry and physiology of brain ammonia. Physiol. Rev. 1987, 67, 440–519. [Google Scholar] [CrossRef]
- Batshaw, M.L. Hyperammonemia. Curr. Probl. Pediatr. 1984, 14, 6–69. [Google Scholar] [CrossRef]
- Batshaw, M.L.; Tuchman, M.; Summar, M.; Seminara, J. A longitudinal study of urea cycle disorders. Mol. Genet. Metab. 2014, 113, 127–130. [Google Scholar] [CrossRef]
- Enns, G.M. Neurologic damage and neurocognitive dysfunction in urea cycle disorders. Semin. Pediatr. Neurol. 2008, 15, 132–139. [Google Scholar] [CrossRef] [PubMed]
- Msall, M.; Batshaw, M.L.; Suss, R.; Brusilow, S.W.; Mellits, E.D. Neurologic Outcome in children with inborn errors of urea synthesis. N. Engl. J. Med. 1984, 310, 1500–1505. [Google Scholar] [CrossRef]
- Nicolaides, P.; Liebsch, D.; Dale, N.; Leonard, J.; Surtees, R. Neurological outcome of patients with ornithine carbamoyltransferase deficiency. Arch. Dis. Child. 2002, 86, 54–56. [Google Scholar] [CrossRef]
- Uchino, T.; Endo, F.; Matsuda, I. Neurodevelopmental outcome of long-term therapy of urea cycle disorders in Japan. J. Inherit. Metab. Dis. 1998, 21, 151–159. [Google Scholar] [CrossRef]
- Häberle, J.; Boddaert, N.; Burlina, A.; Chakrapani, A.; Dixon, M.; Huemer, M.; Karall, D.; Martinelli, D.; Crespo, P.S.; Santer, R.; et al. Suggested guidelines for the diagnosis and management of urea cycle disorders. Orphanet J. Rare Dis. 2012, 7, 32. [Google Scholar] [CrossRef]
- Häberle, J.; Burlina, A.; Chakrapani, A.; Dixon, M.; Karall, D.; Lindner, M.; Mandel, H.; Martinelli, D.; Pintos-Morell, G.; Santer, R.; et al. Suggested guidelines for the diagnosis and management of urea cycle disorders: First revision. J. Inherit. Metab. Dis. 2019, 42, 1192–1230. [Google Scholar] [CrossRef]
- Raina, R.; Bedoyan, J.K.; Lichter-Konecki, U.; Jouvet, P.; Picca, S.; Mew, N.A.; Machado, M.C.; Chakraborty, R.; Vemuganti, M.; Grewal, M.K.; et al. Consensus guidelines for management of hyperammonaemia in paediatric patients receiving continuous kidney replacement therapy. Nat. Rev. Nephrol. 2020, 16, 471–482. [Google Scholar] [CrossRef] [PubMed]
- Ronco, C.; Garzotto, F.; Brendolan, A.; Zanella, M.; Bellettato, M.; Vedovato, S.; Chiarenza, F.; Ricci, Z.; Goldstein, S.L. Continuous renal replacement therapy in neonates and small infants: Development and first-in-human use of a miniaturised machine (CARPEDIEM). Lancet 2014, 383, 1807–1813. [Google Scholar] [CrossRef]
- Vidal, E.; Cocchi, E.; Paglialonga, F.; Ricci, Z.; Garzotto, F.; Peruzzi, L.; Murer, L.; Ronco, C. Continuous veno-venous hemodialysis using the cardio-renal pediatric dialysis emergency machineTM: First clinical experiences. Blood Purif. 2019, 47, 149–155. [Google Scholar] [CrossRef] [PubMed]
- Picca, S.; Dionisi-Vici, C.; Bartuli, A.; De Palo, T.; Papadia, F.; Montini, G.; Materassi, M.; Donati, M.A.; Verrina, E.; Schiaffino, M.C.; et al. Short-term survival of hyperammonemic neonates treated with dialysis. Pediatr. Nephrol. 2015, 30, 839–847. [Google Scholar] [CrossRef] [PubMed]
- Schaefer, F.; Straube, E.; Oh, J.; Mehls, O.; Mayatepek, E. Dialysis in neonates with inborn errors of metabolism. Nephrol. Dial. Transplant. 1999, 14, 910–918. [Google Scholar] [CrossRef]
- Everdell, N.L.; Coulthard, M.G.; Crosier, J.; Keir, M.J. A machine for haemodialysing very small infants. Pediatr. Nephrol. 2005, 20, 636–643. [Google Scholar] [CrossRef] [PubMed]
- Davenport, A.; Will, E.J.; Davison, A.M. Early Changes in intracranial pressure during haemofiltration treatment in patients with grade 4 hepatic encephalopathy and acute oliguric renal failure. Nephrol. Dial. Transplant. 1990, 5, 192–198. [Google Scholar] [CrossRef] [PubMed]
- McBryde, K.D.; Kershaw, D.B.; Bunchman, T.E.; Maxvold, N.J.; Mottes, T.A.; Kudelka, T.L.; Brophy, P.D. Renal replacement therapy in the treatment of confirmed or suspected inborn errors of metabolism. J. Pediatr. 2006, 148, 770–778. [Google Scholar] [CrossRef] [PubMed]
- Wells, J.C.K.; Fewtrell, M.S.; Davies, P.S.W.; Williams, J.E.; Coward, W.A.; Cole, T.J. Prediction of total body water in infants and children. Arch. Dis. Child. 2005, 90, 965–971. [Google Scholar] [CrossRef] [PubMed]
- Fleming, G.M.; Walters, S.; Goldstein, S.L.; Alexander, S.R.; Baum, M.A.; Blowey, D.L.; Bunchman, T.E.; Chua, A.N.; Fletcher, S.A.; Flores, F.X.; et al. Nonrenal indications for continuous renal replacement therapy. Pediatr. Crit. Care Med. 2012, 13, e299–e304. [Google Scholar] [CrossRef] [PubMed]
- Spinale, J.M.; Laskin, B.L.; Sondheimer, N.; Swartz, S.J.; Goldstein, S.L. High-dose continuous renal replacement therapy for neonatal hyperammonemia. Pediatr. Nephrol. 2013, 28, 983–986. [Google Scholar] [CrossRef]
- Levesque, R. Haemodialysis for severe hyperammonaemic coma complicating urinary diversions. Nephrol. Dial. Transplant. 1999, 14, 458–461. [Google Scholar] [CrossRef]






{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Patient 1 | Patient 2 | Patient 3 | Patient 4 | |
|---|---|---|---|---|
| Patient characteristics at start hemodialysis | ||||
| Age (days) | 3 | 3 | 3 | 5 |
| Sex (F/M) | M | M | M | F |
| Body weight (kg) | 3.15 | 3.82 | 3.02 | 2.96 |
| Body length (cm) | 48 | 54 | 52 | 48.5 |
| Calculated TBW (L) | 2.14 | 2.62 | 2.23 | 2.04 |
| Diagnosed IEM | OTC | OTC | OTC | MMA |
| Serum ammonium (µmol/L) | 1377 | 729 | 3017 | 709 |
| Time from diagnosis to start hemodialysis | 06 h 10 min | 11 h 40 min | 15 h 20 min | 6 h 13 min |
| Dialysis prescription | ||||
| Vascular access | 6.5 Fr dL IJV | 6.5 Fr dL IJV | 6.5 Fr dL IJV | 6.5 Fr dL IJV |
| Fresenius 4008 (n = number of sessions) (priming: PC or S) | 1 (PC) | 1 (PC) + 1 (S) | 1 (PC) | 1 (PC) |
| CarpeDiem CD015 (n = number of sessions) (priming: PC or S) | 2 (S) | 0 | 0 | 0 |
| CarpeDiem CD025 (n = number of sessions) (priming: PC or S) | 1 (S) | 1 (S) + 2 (PC) | 0 | 0 |
| Anticoagulation | Heparin | Heparin | Heparin | Heparin |
| Therapy and outcome | ||||
| Duration medical management * prior to hemodialysis initiation | 01 h 23 min | 09 h 15 min | 13 h 15 min | 1 h 30 min |
| Time between arrival at our center and hemodialysis initiation | 01 h 23 min | 00 h 57 min | 01 h 14 min | 01 h 30 min |
| Time from HD initiation to serum ammonia <400 µmol/L | 04 h 06 min | 01 h 44 min | 06 h 43 min | 2 h 17 min |
| Time from diagnosis to reaching serum ammonia <400 µmol/L | 10 h 16 min | 13 h 24 min | 22 h 03 min | 8 h 30 min |
| Survival | Yes | Yes | Yes | No |
| Start Concentration | 3000 µmol/L | 1500 µmol/L | 800 µmol/L | 400 µmol/L | 200 µmol/L | ||||||
|---|---|---|---|---|---|---|---|---|---|---|---|
| Setup | Threshold | QB 30 | QB 50 | QB 30 | QB 50 | QB 30 | QB 50 | QB 30 | QB 50 | QB 30 | QB 50 |
| 4008 | 400 | 322 | 193 | 211 | 126 | 111 | 66 | - | - | - | - |
| 200 | 433 | 259 | 321 | 193 | 221 | 133 | 111 | 67 | - | - | |
| 100 | 546 | 326 | 431 | 259 | 330 | 199 | 221 | 133 | 110 | 65 | |
| CD025 | 400 | 965 | - | 632 | - | 332 | - | - | - | - | - |
| 200 | >> | - | 965 | - | 662 | - | 332 | - | - | - | |
| 100 | >> | - | >> | - | 995 | - | 665 | - | 330 | 200 | |
| CD015 | 400 | 1112 | - | 730 | - | 382 | - | - | - | - | - |
| 200 | >> | - | 1112 | - | 765 | - | 382 | - | - | - | |
| 100 | >> | - | >> | - | 1150 | - | 765 | - | 385 | 230 | |
| Start Concentration | 3000 µmol/L | 1500 µmol/L | 800 µmol/L | 400 µmol/L | 200 µmol/L | ||||||
|---|---|---|---|---|---|---|---|---|---|---|---|
| Setup | Threshold | QB 30 | QB 50 | QB 30 | QB 50 | QB 30 | QB 50 | QB 30 | QB 50 | QB 30 | QB 50 |
| 4008 | 400 | 471 | 283 | 309 | 186 | 162 | 97 | - | - | - | - |
| 200 | 632 | 380 | 471 | 282 | 324 | 194 | 162 | 97 | - | - | |
| 100 | 795 | 476 | 632 | 380 | 485 | 291 | 325 | 195 | 163 | 97 | |
| CD025 | 400 | 1414 | - | 926 | - | 486 | - | - | - | - | - |
| 200 | >> | - | 1413 | - | 972 | - | 485 | - | - | - | |
| 100 | >> | - | >> | - | >> | - | 970 | - | 485 | - | |
| CD015 | 400 | >> | - | 1070 | - | 560 | - | - | - | - | - |
| 200 | >> | - | >> | - | 1120 | - | 560 | - | - | - | |
| 100 | >> | - | >> | - | 1680 | - | 1120 | - | 560 | - | |
| Company | Fresenius Medical Care | Medtronic |
|---|---|---|
| Dialysis machine | 4008 | CarpeDiem |
| Blood flow (mL/min) | 30–100 | 5–50 |
| Dialysate flow (mL/min | 300–800 | 10 |
| Dialyzer | FXPaed | HCD 015/HCD 025 |
| Surface area (m2) | 0.20 | 0.17/0.29 |
| Fiber material | Helixone® | Polyethersulfon |
| Priming volume (mL) | 18 | 11/20 |
| Fiber diameter (µm) | 220 | 200 |
| Membrane thickness (µm) | 35 | 30 |
| Total priming volume (mL) | 53 | 32/41 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Eloot, S.; De Rudder, J.; Verloo, P.; Dhont, E.; Raes, A.; Van Biesen, W.; Snauwaert, E. Towards an Algorithm-Based Tailored Treatment of Acute Neonatal Hyperammonemia. Toxins 2021, 13, 484. https://doi.org/10.3390/toxins13070484
Eloot S, De Rudder J, Verloo P, Dhont E, Raes A, Van Biesen W, Snauwaert E. Towards an Algorithm-Based Tailored Treatment of Acute Neonatal Hyperammonemia. Toxins. 2021; 13(7):484. https://doi.org/10.3390/toxins13070484
Chicago/Turabian StyleEloot, Sunny, Jonathan De Rudder, Patrick Verloo, Evelyn Dhont, Ann Raes, Wim Van Biesen, and Evelien Snauwaert. 2021. "Towards an Algorithm-Based Tailored Treatment of Acute Neonatal Hyperammonemia" Toxins 13, no. 7: 484. https://doi.org/10.3390/toxins13070484
APA StyleEloot, S., De Rudder, J., Verloo, P., Dhont, E., Raes, A., Van Biesen, W., & Snauwaert, E. (2021). Towards an Algorithm-Based Tailored Treatment of Acute Neonatal Hyperammonemia. Toxins, 13(7), 484. https://doi.org/10.3390/toxins13070484