Mandibular Bone Loss after Masticatory Muscles Intervention with Botulinum Toxin: An Approach from Basic Research to Clinical Findings

 ,
, 

Abstract
1. Introduction
1.1. Bone Remodeling as an Integration Mechanism in the Masticatory Apparatus
1.2. Mechanism of Action and Treatment of Oral Muscular Disorders: The Use of Botulinum Toxin Type A in Dentistry
1.3. BoNT/A and Bone Loss at the Masticatory Apparatus
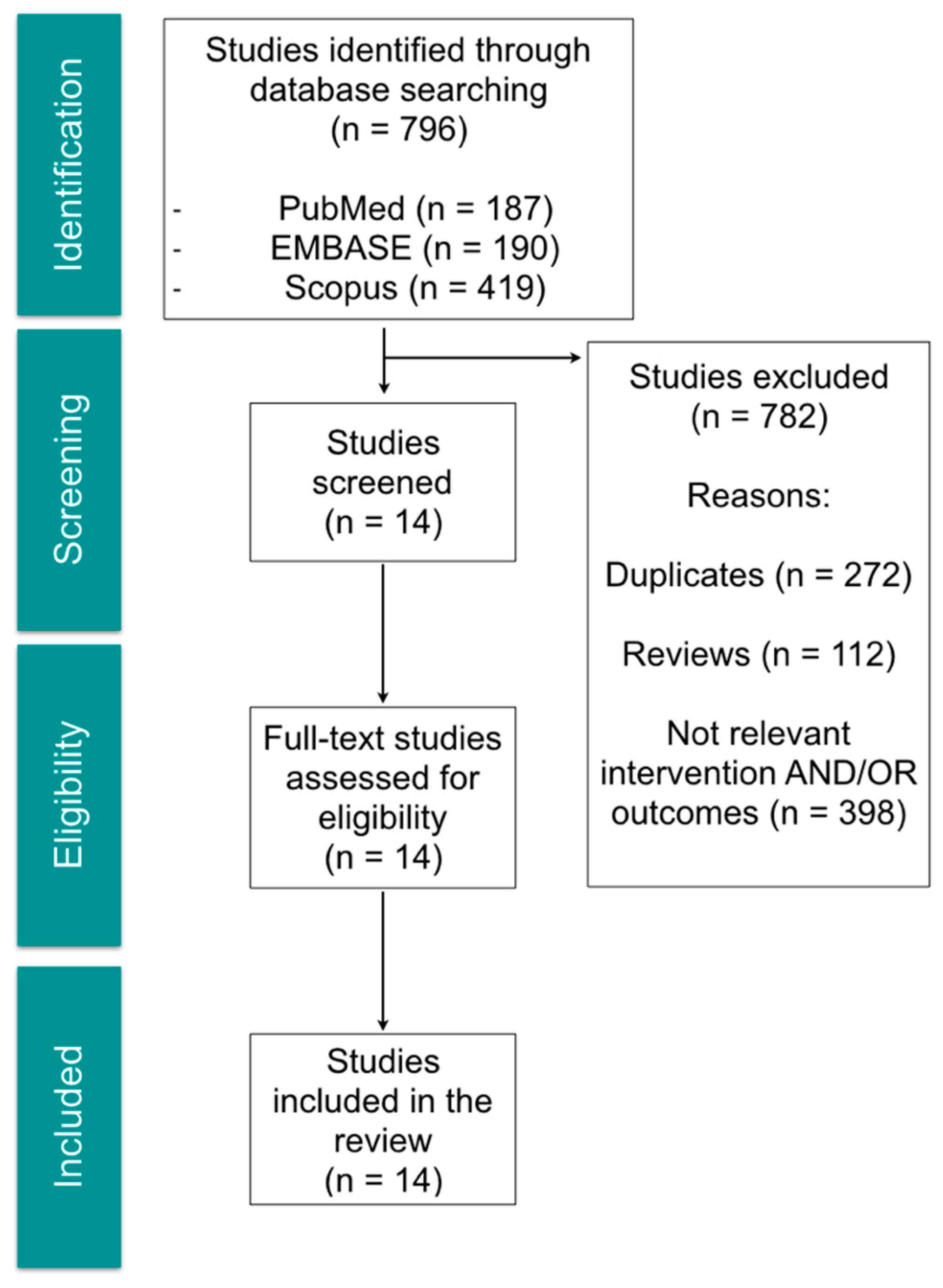
2. Methods
((((((((((("Mandible"[Mesh]) OR Mandib*[Title/Abstract]) OR "Temporomandibular Joint"[Mesh]) OR "Mandibular Condyle"[Mesh]) OR Mandibular head*[Title/Abstract]) OR Mandibular condyle*[Title/Abstract]) OR Subchondral bone*[Title/Abstract]) OR "Alveolar Bone Loss"[Mesh]) OR "Alveolar Process"[Mesh]) OR Alveolar bone*[Title/Abstract])) AND ((("Botulinum Toxins, Type A"[Mesh]) OR "Botulinum Toxins"[Mesh]) OR Botulinum toxin*[Title/Abstract])
3. Results
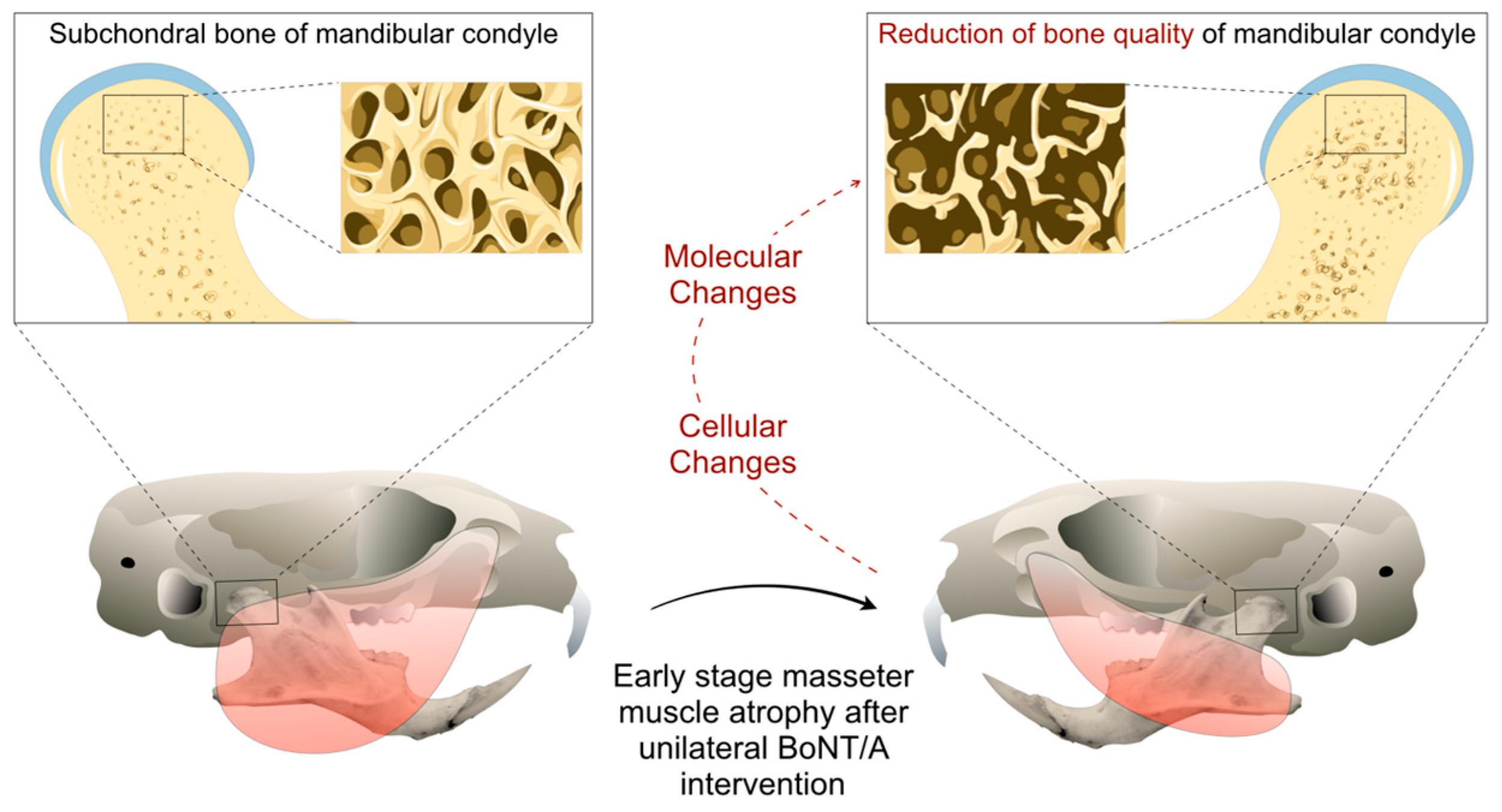
3.1. Cellular and Metabolic Changes
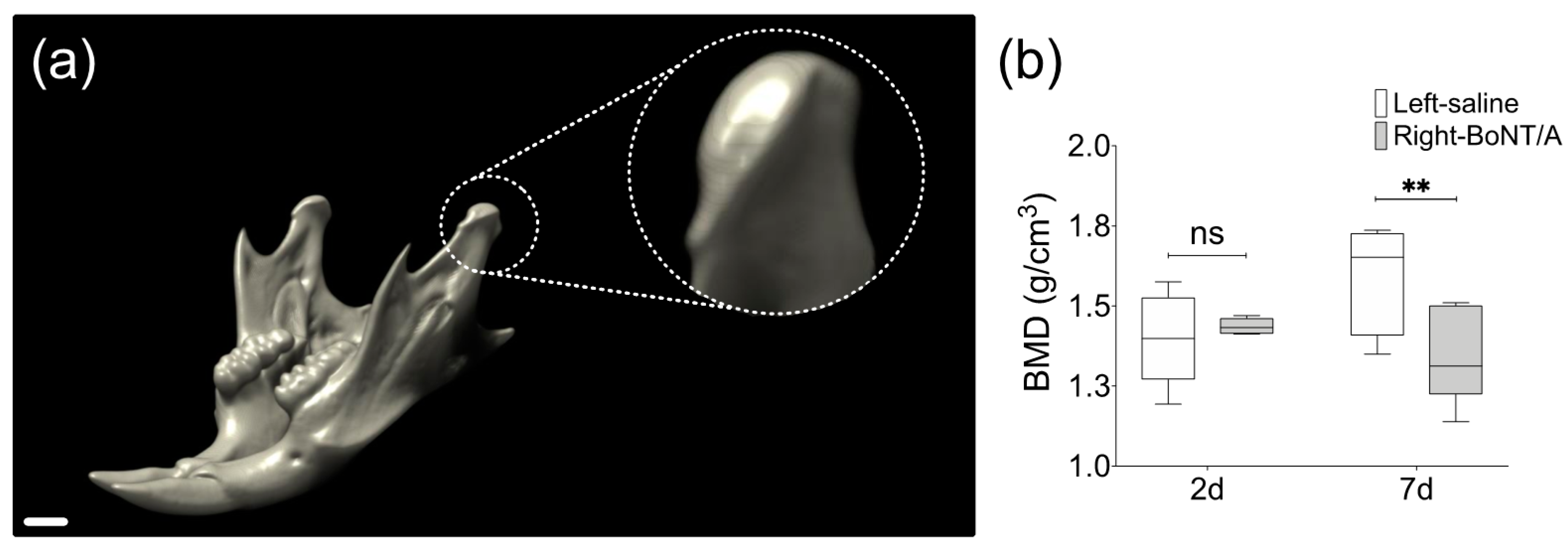
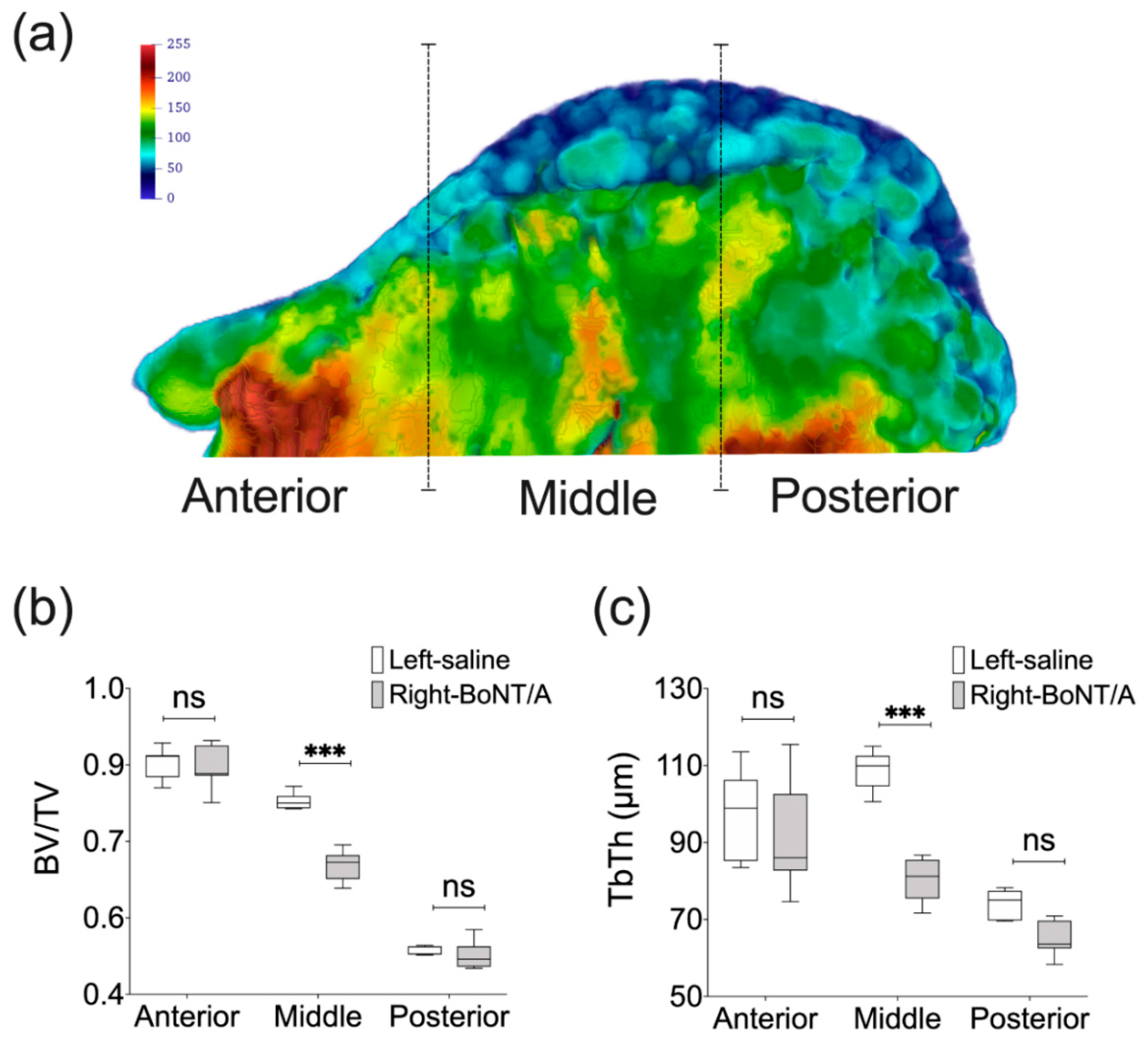
3.2. Microstructural Changes
3.3. Morphological Changes
4. Discussion
5. Conclusions
Author Contributions
Funding
Acknowledgments
Conflicts of Interest
References
- Miller, J.; Clarkson, E. Botulinum Toxin Type A: Review and Its Role in the Dental Office. Dent. Clin. North. Am. 2016, 60, 509–521. [Google Scholar] [CrossRef] [PubMed]
- Comella, C.L. Systematic review of botulinum toxin treatment for oromandibular dystonia. Toxicon 2018, 147, 96–99. [Google Scholar] [CrossRef] [PubMed]
- De la Torre Canales, G.; Camara-Souza, M.B.; do Amaral, C.F.; Garcia, R.C.; Manfredini, D. Is there enough evidence to use botulinum toxin injections for bruxism management? A systematic literature review. Clin. Oral Investig. 2017, 21, 727–734. [Google Scholar] [CrossRef] [PubMed]
- Fedorowicz, Z.; van Zuuren, E.J.; Schoones, J. Botulinum toxin for masseter hypertrophy. Cochrane Database Syst. Rev. 2013. [Google Scholar] [CrossRef] [PubMed]
- Aziz, J.; Awal, D.; Ayliffe, P. Resorption of the mandibular condyle after injections of botulinum toxin A. Br. J. Oral Maxillofac. Surg. 2017, 55, 987–988. [Google Scholar] [CrossRef] [PubMed]
- Balanta-Melo, J.; Buvinic, S. Mandibular bone loss: A hidden side effect of botulinum toxin type A injection in masticatory muscles. J. Oral Res. 2018, 7, 44–47. [Google Scholar] [CrossRef]
- Laskin, D.M. The Use of Botulinum Toxin for the Treatment of Myofascial Pain in the Masticatory Muscles. Oral Maxillofac. Surg. Clin. North. Am. 2018, 30, 287–289. [Google Scholar] [CrossRef] [PubMed]
- Lee, H.J.; Kim, S.J.; Lee, K.J.; Yu, H.S.; Baik, H.S. Repeated injections of botulinum toxin into the masseter muscle induce bony changes in human adults: A longitudinal study. Korean J. Orthod. 2017, 47, 222–228. [Google Scholar] [CrossRef] [PubMed]
- Santagati, F.; Rijli, F.M. Cranial neural crest and the building of the vertebrate head. Nat. Rev. Neurosci. 2003, 4, 806–818. [Google Scholar] [CrossRef] [PubMed]
- Baverstock, H.; Jeffery, N.S.; Cobb, S.N. The morphology of the mouse masticatory musculature. J. Anat. 2013, 223, 46–60. [Google Scholar] [CrossRef]
- Tzahor, E. Head muscle development. Results Probl. Cell. Differ. 2015, 56, 123–142. [Google Scholar] [CrossRef] [PubMed]
- Orset, E.; Chaffanjon, P.; Bettega, G. Temporomandibular joint model: anatomic and radiologic comparison between rat and human. Surg. Radiol. Anat. 2014, 36, 163–166. [Google Scholar] [CrossRef] [PubMed]
- Liang, W.; Li, X.; Gao, B.; Gan, H.; Lin, X.; Liao, L.; Li, C. Observing the development of the temporomandibular joint in embryonic and post-natal mice using various staining methods. Exp. Ther. Med. 2016, 11, 481–489. [Google Scholar] [CrossRef] [PubMed]
- Shibata, S.; Sato, R.; Murakami, G.; Fukuoka, H.; Francisco Rodríguez-Vázquez, J. Origin of mandibular condylar cartilage in mice, rats, and humans: Periosteum or separate blastema? J. Oral Biosci. 2013, 55, 208–216. [Google Scholar] [CrossRef]
- Mizoguchi, I.; Toriya, N.; Nakao, Y. Growth of the mandible and biological characteristics of the mandibular condylar cartilage. Jpn. Dent. Sci. Rev. 2013, 49, 139–150. [Google Scholar] [CrossRef]
- Dickinson, E.; Fitton, L.C.; Kupczik, K. Ontogenetic changes to muscle architectural properties within the jaw-adductor musculature of Macaca fascicularis. Am. J. Phys. Anthropol. 2018, 167, 291–310. [Google Scholar] [CrossRef] [PubMed]
- de Jong, W.C.; Korfage, J.A.; Langenbach, G.E. The role of masticatory muscles in the continuous loading of the mandible. J. Anat. 2011, 218, 625–636. [Google Scholar] [CrossRef] [PubMed]
- Tsouknidas, A.; Jimenez-Rojo, L.; Karatsis, E.; Michailidis, N.; Mitsiadis, T.A. A Bio-Realistic Finite Element Model to Evaluate the Effect of Masticatory Loadings on Mouse Mandible-Related Tissues. Front. Physiol. 2017, 8, 273. [Google Scholar] [CrossRef] [PubMed]
- Ahmad, M.; Schiffman, E.L. Temporomandibular Joint Disorders and Orofacial Pain. Dent. Clin. North. Am. 2016, 60, 105–124. [Google Scholar] [CrossRef]
- Okeson, J.P.; de Leeuw, R. Differential diagnosis of temporomandibular disorders and other orofacial pain disorders. Dent. Clin. North. Am. 2011, 55, 105–120. [Google Scholar] [CrossRef]
- List, T.; Jensen, R.H. Temporomandibular disorders: Old ideas and new concepts. Cephalalgia 2017, 37, 692–704. [Google Scholar] [CrossRef] [PubMed]
- Maixner, W.; Diatchenko, L.; Dubner, R.; Fillingim, R.B.; Greenspan, J.D.; Knott, C.; Ohrbach, R.; Weir, B.; Slade, G.D. Orofacial pain prospective evaluation and risk assessment study-the OPPERA study. J. Pain 2011, 12, T4–T11. [Google Scholar] [CrossRef] [PubMed]
- Yang, H.M.; Won, S.Y.; Kim, H.J.; Hu, K.S. Neurovascular structures of the mandibular angle and condyle: A comprehensive anatomical review. Surg. Radiol. Anat. 2015, 37, 1109–1118. [Google Scholar] [CrossRef] [PubMed]
- Bagi, C.M.; Berryman, E.; Moalli, M.R. Comparative bone anatomy of commonly used laboratory animals: Implications for drug discovery. Comp. Med. 2011, 61, 76–85. [Google Scholar] [PubMed]
- Chong, D.A.; Evans, C.A. Histologic study of the attachment of muscles to the rat mandible. Arch. Oral. Biol. 1982, 27, 519–527. [Google Scholar] [CrossRef]
- Kwan, P. Osteoporosis: From osteoscience to neuroscience and beyond. Mech. Ageing Dev. 2015, 145, 26–38. [Google Scholar] [CrossRef] [PubMed]
- Morrison, S.J.; Scadden, D.T. The bone marrow niche for haematopoietic stem cells. Nature 2014, 505, 327–334. [Google Scholar] [CrossRef] [PubMed]
- Laurent, M.R.; Dubois, V.; Claessens, F.; Verschueren, S.M.; Vanderschueren, D.; Gielen, E.; Jardi, F. Muscle-bone interactions: From experimental models to the clinic? A critical update. Mol. Cell. Endocrinol. 2016, 432, 14–36. [Google Scholar] [CrossRef] [PubMed]
- Pihut, M.; Ferendiuk, E.; Szewczyk, M.; Kasprzyk, K.; Wieckiewicz, M. The efficiency of botulinum toxin type A for the treatment of masseter muscle pain in patients with temporomandibular joint dysfunction and tension-type headache. J. Headache Pain 2016, 17, 29. [Google Scholar] [CrossRef]
- Oftadeh, R.; Entezari, V.; Sporri, G.; Villa-Camacho, J.C.; Krigbaum, H.; Strawich, E.; Graham, L.; Rey, C.; Chiu, H.; Muller, R.; et al. Hierarchical analysis and multi-scale modelling of rat cortical and trabecular bone. J. R. Soc. Interface 2015, 12. [Google Scholar] [CrossRef]
- Burr, D.B.; Akkus, O. Bone Morphology and Organization. In Basic and Applied Bone Biology; Academic Press: San Diego, CA, USA, 2014. [Google Scholar]
- Martin, R.B.; Burr, D.B.; Sharkey, N.A.; Fyhrie, D.P. Skeletal Biology. In Skeletal Tissue Mechanics; Martin, R.B., Burr, D.B., Sharkey, N.A., Fyhrie, D.P., Eds.; Springer: New York, NY, USA, 2015. [Google Scholar]
- Lai, X.; Price, C.; Lu, X.L.; Wang, L. Imaging and quantifying solute transport across periosteum: Implications for muscle-bone crosstalk. Bone 2014, 66, 82–89. [Google Scholar] [CrossRef] [PubMed]
- Bellido, T.; Plotkin, L.I.; Bruzzaniti, A. Bone Cells A2. In Basic and Applied Bone Biology; Allen, M.R., Burr, D.B., Eds.; Academic Press: San Diego, CA, USA, 2014. [Google Scholar]
- Sims, N.A.; Martin, T.J. Coupling the activities of bone formation and resorption: A multitude of signals within the basic multicellular unit. Bonekey Rep. 2014, 3, 481. [Google Scholar] [CrossRef] [PubMed]
- Xiao, W.; Wang, Y.; Pacios, S.; Li, S.; Graves, D.T. Cellular and Molecular Aspects of Bone Remodeling. Front Oral. Biol. 2016, 18, 9–16. [Google Scholar] [CrossRef]
- Cappariello, A.; Maurizi, A.; Veeriah, V.; Teti, A. Reprint of: The Great Beauty of the osteoclast. Arch. Biochem. Biophys. 2014, 561, 13–21. [Google Scholar] [CrossRef] [PubMed]
- Boyle, W.J.; Simonet, W.S.; Lacey, D.L. Osteoclast differentiation and activation. Nature 2003, 423, 337–342. [Google Scholar] [CrossRef] [PubMed]
- Takahashi, N.; Udagawa, N.; Suda, T. A new member of tumor necrosis factor ligand family, ODF/OPGL/TRANCE/RANKL, regulates osteoclast differentiation and function. Biochem. Biophys. Res. Commun. 1999, 256, 449–455. [Google Scholar] [CrossRef] [PubMed]
- Kim, J.H.; Kim, N. Signaling Pathways in Osteoclast Differentiation. Chonnam Med. J. 2016, 52, 12–17. [Google Scholar] [CrossRef]
- Long, F. Building strong bones: Molecular regulation of the osteoblast lineage. Nat. Rev. Mol. Cell. Biol. 2011, 13, 27–38. [Google Scholar] [CrossRef]
- Plotkin, L.I.; Bellido, T. Osteocytic signalling pathways as therapeutic targets for bone fragility. Nat. Rev. Endocrinol. 2016, 12, 593–605. [Google Scholar] [CrossRef]
- Bonewald, L.F. The amazing osteocyte. J. Bone Miner. Res. 2011, 26, 229–238. [Google Scholar] [CrossRef]
- Xiong, J.; Piemontese, M.; Onal, M.; Campbell, J.; Goellner, J.J.; Dusevich, V.; Bonewald, L.; Manolagas, S.C.; O’Brien, C.A. Osteocytes, not Osteoblasts or Lining Cells, are the Main Source of the RANKL Required for Osteoclast Formation in Remodeling Bone. PLoS ONE 2015, 10, e0138189. [Google Scholar] [CrossRef] [PubMed]
- Xiao, W.; Li, S.; Pacios, S.; Wang, Y.; Graves, D.T. Bone Remodeling Under Pathological Conditions. Front. Oral Biol. 2016, 18, 17–27. [Google Scholar] [CrossRef]
- Walsh, M.C.; Choi, Y. Biology of the RANKL-RANK-OPG System in Immunity, Bone, and Beyond. Front. Immunol. 2014, 5, 511. [Google Scholar] [CrossRef] [PubMed]
- Anderson, P.S.; Renaud, S.; Rayfield, E.J. Adaptive plasticity in the mouse mandible. BMC Evol. Biol. 2014, 14, 85. [Google Scholar] [CrossRef] [PubMed]
- Klingenberg, C.P.; Navarro, N. Development of the mouse mandible. In Evolution of the House Mouse; Macholán, M., Baird, S.J.E., Munclinger, P., Piálek, J., Eds.; Cambridge University Press: Cambridge, UK, 2012. [Google Scholar]
- Rossetto, O.; Pirazzini, M.; Montecucco, C. Botulinum neurotoxins: Genetic, structural and mechanistic insights. Nat. Rev. Microbiol. 2014, 12, 535–549. [Google Scholar] [CrossRef]
- Pirazzini, M.; Rossetto, O.; Eleopra, R.; Montecucco, C. Botulinum Neurotoxins: Biology, Pharmacology, and Toxicology. Pharmacol. Rev. 2017, 69, 200–235. [Google Scholar] [CrossRef] [PubMed]
- Balanta-Melo, J.; Toro-Ibacache, V.; Torres-Quintana, M.A.; Kupczik, K.; Vega, C.; Morales, C.; Hernandez-Moya, N.; Arias-Calderon, M.; Beato, C.; Buvinic, S. Early molecular response and microanatomical changes in the masseter muscle and mandibular head after botulinum toxin intervention in adult mice. Ann. Anat. 2018, 216, 112–119. [Google Scholar] [CrossRef]
- Brin, M.F.; James, C.; Maltman, J. Botulinum toxin type A products are not interchangeable: A review of the evidence. Biologics 2014, 8, 227–241. [Google Scholar] [CrossRef]
- Kane, C.D.; Nuss, J.E.; Bavari, S. Novel therapeutic uses and formulations of botulinum neurotoxins: A patent review (2012–2014). Expert Opin. Ther. Pat. 2015, 25, 675–690. [Google Scholar] [CrossRef]
- Jankovic, J. An update on new and unique uses of botulinum toxin in movement disorders. Toxicon 2018, 147, 84–88. [Google Scholar] [CrossRef]
- Chen, Z.; Chen, Z.; Zhao, N.; Shen, G. An Animal Model for Inducing Deviation of the Mandible. J. Oral Maxillofac. Surg. 2015, 73, 2207–2218. [Google Scholar] [CrossRef] [PubMed]
- Seok, H.; Kim, S.G.; Kim, M.K.; Jang, I.; Ahn, J. Effect of the masseter muscle injection of botulinum toxin A on the mandibular bone growth of developmental rats. Maxillofac. Plast. Reconstr. Surg. 2018, 40, 5. [Google Scholar] [CrossRef] [PubMed]
- Park, C.; Park, K.; Kim, J. Growth effects of botulinum toxin type A injected unilaterally into the masseter muscle of developing rats. J. Zhejiang Univ. Sci. B 2015, 16, 46–51. [Google Scholar] [CrossRef] [PubMed]
- Tsai, C.Y.; Yang, L.Y.; Chen, K.T.; Chiu, W.C. The influence of masticatory hypofunction on developing rat craniofacial structure. Int. J. Oral Maxillofac. Surg. 2010, 39, 593–598. [Google Scholar] [CrossRef] [PubMed]
- Kim, J.Y.; Kim, S.T.; Cho, S.W.; Jung, H.S.; Park, K.T.; Son, H.K. Growth effects of botulinum toxin type A injected into masseter muscle on a developing rat mandible. Oral Dis. 2008, 14, 626–632. [Google Scholar] [CrossRef] [PubMed]
- Kwon, T.G.; Park, H.S.; Lee, S.H.; Park, I.S.; An, C.H. Influence of unilateral masseter muscle atrophy on craniofacial morphology in growing rabbits. J. Oral Maxillofac. Surg. 2007, 65, 1530–1537. [Google Scholar] [CrossRef] [PubMed]
- Tsai, C.Y.; Chiu, W.C.; Liao, Y.H.; Tsai, C.M. Effects on craniofacial growth and development of unilateral botulinum neurotoxin injection into the masseter muscle. Am. J. Orthod. Dentofacial Orthop. 2009, 135, 142.e1–142.e6. [Google Scholar] [CrossRef] [PubMed]
- Balanta-Melo, J.; Torres-Quintana, M.A.; Bemmann, M.; Vega, C.; Gonzalez, C.; Kupczik, K.; Toro-Ibacache, V.; Buvinic, S. Masseter muscle atrophy impairs bone quality of the mandibular condyle but not the alveolar process early after induction. J. Oral. Rehabil. 2018. [Google Scholar] [CrossRef]
- Dutra, E.H.; O’Brien, M.H.; Logan, C.; Tadinada, A.; Nanda, R.; Yadav, S. Loading of the Condylar Cartilage Can Rescue the Effects of Botox on TMJ. Calcif. Tissue Int. 2018, 103, 71–79. [Google Scholar] [CrossRef]
- Shi, Z.; Lv, J.; Xiaoyu, L.; Zheng, L.W.; Yang, X.W. Condylar Degradation from Decreased Occlusal Loading following Masticatory Muscle Atrophy. Biomed. Res. Int. 2018, 2018, 1–11. [Google Scholar] [CrossRef]
- Kun-Darbois, J.D.; Manero, F.; Rony, L.; Chappard, D. Contrast enhancement with uranyl acetate allows quantitative analysis of the articular cartilage by microCT: Application to mandibular condyles in the BTX rat model of disuse. Micron 2017, 97, 35–40. [Google Scholar] [CrossRef] [PubMed]
- Dutra, E.H.; MH, O.B.; Lima, A.; Kalajzic, Z.; Tadinada, A.; Nanda, R.; Yadav, S. Cellular and Matrix Response of the Mandibular Condylar Cartilage to Botulinum Toxin. PLoS ONE 2016, 11, e0164599. [Google Scholar] [CrossRef]
- Matthys, T.; Ho Dang, H.A.; Rafferty, K.L.; Herring, S.W. Bone and cartilage changes in rabbit mandibular condyles after 1 injection of botulinum toxin. Am. J. Orthod. Dentofacial Orthop. 2015, 148, 999–1009. [Google Scholar] [CrossRef] [PubMed]
- Kun-Darbois, J.D.; Libouban, H.; Chappard, D. Botulinum toxin in masticatory muscles of the adult rat induces bone loss at the condyle and alveolar regions of the mandible associated with a bone proliferation at a muscle enthesis. Bone 2015, 77, 75–82. [Google Scholar] [CrossRef] [PubMed]
- Raphael, K.G.; Tadinada, A.; Bradshaw, J.M.; Janal, M.N.; Sirois, D.A.; Chan, K.C.; Lurie, A.G. Osteopenic consequences of botulinum toxin injections in the masticatory muscles: A pilot study. J. Oral Rehabil. 2014, 41, 555–563. [Google Scholar] [CrossRef]
- Rafferty, K.L.; Liu, Z.J.; Ye, W.; Navarrete, A.L.; Nguyen, T.T.; Salamati, A.; Herring, S.W. Botulinum toxin in masticatory muscles: Short- and long-term effects on muscle, bone, and craniofacial function in adult rabbits. Bone 2012, 50, 651–662. [Google Scholar] [CrossRef]
- Chang, C.S.; Bergeron, L.; Yu, C.C.; Chen, P.K.; Chen, Y.R. Mandible changes evaluated by computed tomography following Botulinum Toxin A injections in square-faced patients. Aesthetic Plast. Surg. 2011, 35, 452–455. [Google Scholar] [CrossRef]
- Tsai, C.Y.; Huang, R.Y.; Lee, C.M.; Hsiao, W.T.; Yang, L.Y. Morphologic and bony structural changes in the mandible after a unilateral injection of botulinum neurotoxin in adult rats. J. Oral Maxillofac. Surg. 2010, 68, 1081–1087. [Google Scholar] [CrossRef]
- Fonseca, H.; Moreira-Goncalves, D.; Coriolano, H.J.; Duarte, J.A. Bone quality: The determinants of bone strength and fragility. Sports Med. 2014, 44, 37–53. [Google Scholar] [CrossRef]
- Balanta-Melo, J.; Toro-Ibacache, V.; Torres-Quintana, M.A.; Kupczik, K.; Buvinic, S. Mandibular condyle osteopenia after botulinum toxin type A intervention in the mouse masseter muscle. In preparation.
- Sinclair, C.F.; Gurey, L.E.; Blitzer, A. Oromandibular dystonia: Long-term management with botulinum toxin. Laryngoscope 2013, 123, 3078–3083. [Google Scholar] [CrossRef]
- Jilka, R.L. The relevance of mouse models for investigating age-related bone loss in humans. J. Gerontol. A Biol. Sci. Med. Sci. 2013, 68, 1209–1217. [Google Scholar] [CrossRef] [PubMed]
- Piemontese, M.; Almeida, M.; Robling, A.G.; Kim, H.N.; Xiong, J.; Thostenson, J.D.; Weinstein, R.S.; Manolagas, S.C.; O’Brien, C.A.; Jilka, R.L. Old age causes de novo intracortical bone remodeling and porosity in mice. JCI Insight 2017. [Google Scholar] [CrossRef] [PubMed]
- Okayasu, I.; Yamada, Y.; Kohno, S.; Yoshida, N. New animal model for studying mastication in oral motor disorders. J. Dent. Res. 2003, 82, 318–321. [Google Scholar] [CrossRef] [PubMed]
- Yoshimi, T.; Koga, Y.; Nakamura, A.; Fujishita, A.; Kohara, H.; Moriuchi, E.; Yoshimi, K.; Tsai, C.Y.; Yoshida, N. Mechanism of motor coordination of masseter and temporalis muscles for increased masticatory efficiency in mice. J. Oral Rehabil. 2017, 44, 363–374. [Google Scholar] [CrossRef] [PubMed]
- Lodberg, A.; Vegger, J.B.; Jensen, M.V.; Larsen, C.M.; Thomsen, J.S.; Bruel, A. Immobilization induced osteopenia is strain specific in mice. Bone Rep. 2015, 2, 59–67. [Google Scholar] [CrossRef] [PubMed]
- Rinotas, V.; Niti, A.; Dacquin, R.; Bonnet, N.; Stolina, M.; Han, C.Y.; Kostenuik, P.; Jurdic, P.; Ferrari, S.; Douni, E. Novel genetic models of osteoporosis by overexpression of human RANKL in transgenic mice. J. Bone Miner. Res. 2014, 29, 1158–1169. [Google Scholar] [CrossRef] [PubMed]
- Wang, X.D.; Zhang, J.N.; Gan, Y.H.; Zhou, Y.H. Current understanding of pathogenesis and treatment of TMJ osteoarthritis. J. Dent. Res. 2015, 94, 666–673. [Google Scholar] [CrossRef] [PubMed]
- Van Eijden, T.M.; Korfage, J.A.; Brugman, P. Architecture of the human jaw-closing and jaw-opening muscles. Anat. Rec. 1997, 248, 464–474. [Google Scholar] [CrossRef]





{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Author | Individuals | Intervention | Time after Intervention and Bone Evaluation Methods |
|---|---|---|---|
| Balanta-Melo et al. 2018 [62] | Adult male BALB/c mice (8–9 weeks-old) | Experimental group: 0.2 U BoNT/A in the right masseter and saline solution in the left masseter Control group: without intervention | 2 weeks; 3D bone parameters from mandibular condyle and alveolar process, and shape analysis of mandibular condyle using microCT |
| Dutra et al. 2018 [63] | Young adult female C57BL/6J mice (6 weeks-old) | Experimental group: 0.3 U BoNT/A in the right masseter and no intervention in the left masseter Control group: without intervention | 4 weeks; 3D bone parameters using microCT, BMD and histomorphometry from mandibular condyle |
| Shi et al. 2018 [64] | Young adult female Sprague-Dawley rats (5 weeks-old) | Experimental group: 2 U BoNT/A bilateral in both masseter muscles Control group: without intervention | 4 weeks; 3D bone parameters using microCT and histomorphometry from mandibular condyle |
| Balanta-Melo et al. 2018 [51] | Adult male BALB/c mice (8 weeks-old) | Experimental group: 0.2 U BoNT/A in the right masseter and saline solution in the left masseter | 2 weeks; bone histomorphometry and mRNA quantification from mandibular condyle |
| Aziz et al. 2017 [5] | Adult woman (55 years-old) | 140 U BoNT/A quarterly in the left masseter | Morphology of the mandibular condyle (qualitative description) using diagnostic imaging (Dynamic Magnetic Resonance Imaging) |
| Lee et al. 2017 [8] | Adult men and women (28–48 years-old) | Experimental group I: 25 U BoNT/A bilaterally in the masseter muscles Experimental group II: 25 U BoNT/A bilaterally in the masseter muscles; repetition 4 months after the first intervention | 6 months after first intervention; evaluation of bone volume in the mandibular angle using CBCT |
| Kün-Darbois et al. 2017 [65] | Adult male Sprague–Dawley rats (18 weeks-old) | Experimental group: 1 U BoNT/A unilaterally in the masseter and temporalis muscles Control group: unilateral injection of saline solution in the masseter and temporalis muscles | 4 weeks; 3D bone parameters using microCT of mandibular condyles |
| Dutra et al. 2016 [66] | Young adult female transgenic mice (Col10a1) on a CD-1 background (5 weeks-old) | Experimental group: 0.3 U BoNT/A in the right masseter and no intervention in the left masseter | 4 weeks; 3D bone parameters using microCT, BMD and histomorphometry of mandibular condyles |
| Matthys et al. 2015 [67] | Adult New Zeland white female rabbits (5 months-old) | Experimental group: 10 U BoNT/A unilateral in the masseter muscle Control group: unilateral injection of saline solution in the masseter muscle | 4 weeks and 12 weeks; bone histomorphometry of mandibular condyles |
| Kün-Darbois et al. 2015 [68] | Adult male Sprague–Dawley rats (18 weeks-old) | Experimental group: 1 U BoNT/A unilateral in the masseter and the temporalis muscles Control group: unilateral injection of saline solution in the masseter and the temporalis muscles | 4 weeks; 2D analysis of microCT slices from mandibular condyles and alveolar bone |
| Raphael et al. 2014 [69] | Adult women (Mean age 45 years-old) | Exposed group: Adult women with myofascial pain exposed to BoNT/A for treatment. No dose of BoNT/A reported. Unexposed group: Adult women with myofascial pain with no previous exposure to BoNT/A | CBCT 6-10 weeks after exposure to BoNT/A intervention |
| Rafferty et al. 2012 [70] | Adult New Zeland white female rabbits (5 months-old) | Experimental group: 10 U BoNT/A unilateral in the masseter muscle Control group: unilateral injection of saline solution in the masseter muscle | 4 weeks and 12 weeks; 2D and 3D evaluation using microCT of mandibular condyles and alveolar bone |
| Chang et al. 2011 [71] | Adult women | Bilateral injection of 120 U BoNT/A in both masseter muscles | 3 months; 3D analysis of cortical thickness of the mandibular ramus using CT |
| Tsai et al. 2010 [72] | Adult male Sprague-Dawley rats (8 weeks-old) | Experimental group: 7.5 U BoNT/A in the left masseter and saline solution in the right masseter | 3 months; Linear measurements and BMD of mandibles 2D histomorphometry of slices at first molar and coronoid levels |
| Individual | Average Masseter Mass (g) | Generic Name/Brand | Dose/Volume (U/ml) | Average BoNT/A Dose Per Masseter Mass (U/g) |
|---|---|---|---|---|
| Mouse [51,62,63,66] | 0.075 [51] | Onabotulinumtoxin A; Botox®, Allergan Chile, Santiago, Chile [51,62] Onabotulinumtoxin A; Botox®, Allergan, Plc, Parsippany-Troy Hills, NJ, USA [63,66] | 0.2–0.3/0.01–0.03 | 3.3 |
| Rat [64,65,68,72] | 1.1 [64] | Onabotulinumtoxin A; Botox®, Allergan Inc., Irvine, CA, USA [64,65,68] Onabotulinumtoxin A; Botox®, Allergan Pharmaceuticals, Dublin, Ireland [72] | 1–7.5/0.1–0.3 | 4.3 |
| Rabbit [67,70] | 7.9 [70] | Onabotulinumtoxin A; Botox®, Allergan Inc., Irvine, CA, USA [67,70] | 10/0.25 | 1.2 |
| Human [8,71] | 20.14 [83] | Onabotulinumtoxin A; Neuronox®, Medytox Inc., Seoul, Korea [8] Abobotulinum A; Dysport®, Ipsen Biopharm Ltd, Wrexham, UK [71] | 25/0.5 [8] 120/0.6 [71] | 3.6 |
© 2019 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Balanta-Melo, J.; Toro-Ibacache, V.; Kupczik, K.; Buvinic, S. Mandibular Bone Loss after Masticatory Muscles Intervention with Botulinum Toxin: An Approach from Basic Research to Clinical Findings. Toxins 2019, 11, 84. https://doi.org/10.3390/toxins11020084
Balanta-Melo J, Toro-Ibacache V, Kupczik K, Buvinic S. Mandibular Bone Loss after Masticatory Muscles Intervention with Botulinum Toxin: An Approach from Basic Research to Clinical Findings. Toxins. 2019; 11(2):84. https://doi.org/10.3390/toxins11020084
Chicago/Turabian StyleBalanta-Melo, Julián, Viviana Toro-Ibacache, Kornelius Kupczik, and Sonja Buvinic. 2019. "Mandibular Bone Loss after Masticatory Muscles Intervention with Botulinum Toxin: An Approach from Basic Research to Clinical Findings" Toxins 11, no. 2: 84. https://doi.org/10.3390/toxins11020084
APA StyleBalanta-Melo, J., Toro-Ibacache, V., Kupczik, K., & Buvinic, S. (2019). Mandibular Bone Loss after Masticatory Muscles Intervention with Botulinum Toxin: An Approach from Basic Research to Clinical Findings. Toxins, 11(2), 84. https://doi.org/10.3390/toxins11020084