
The Dimensionality, Consistency, and Structural Validity of an Instrument Used to Measure Obesogenic Attitudes in Parents from Southern Spain (The PRELSA Scale)

 ,
,  , , and
, , and 
Abstract
1. Introduction
2. Materials and Methods
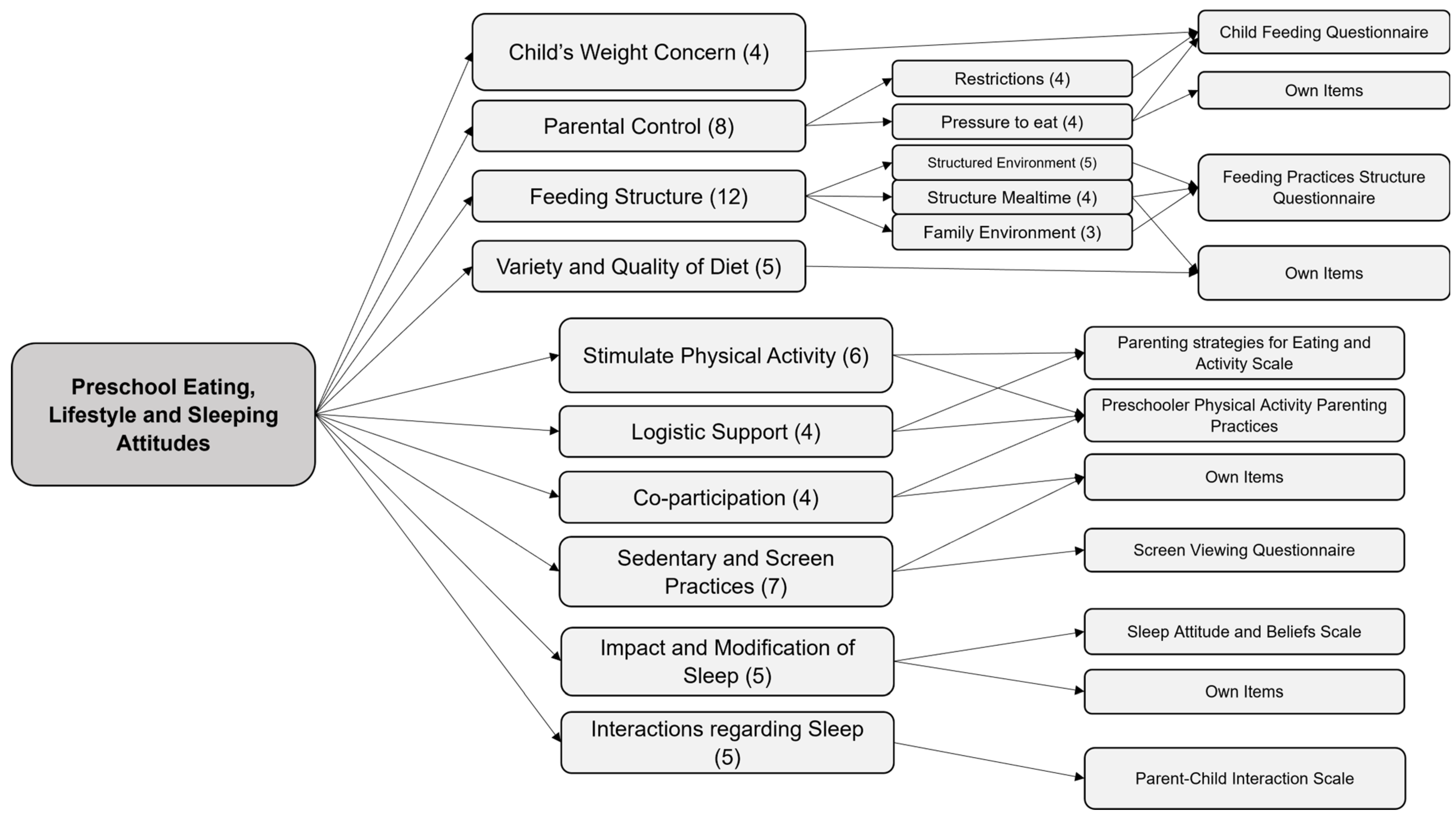
2.1. The PRELSA Scale
2.2. Participants and Data Collection
2.3. Data Analyses
3. Results
3.1. Dimensionality
3.2. Internal Consistency
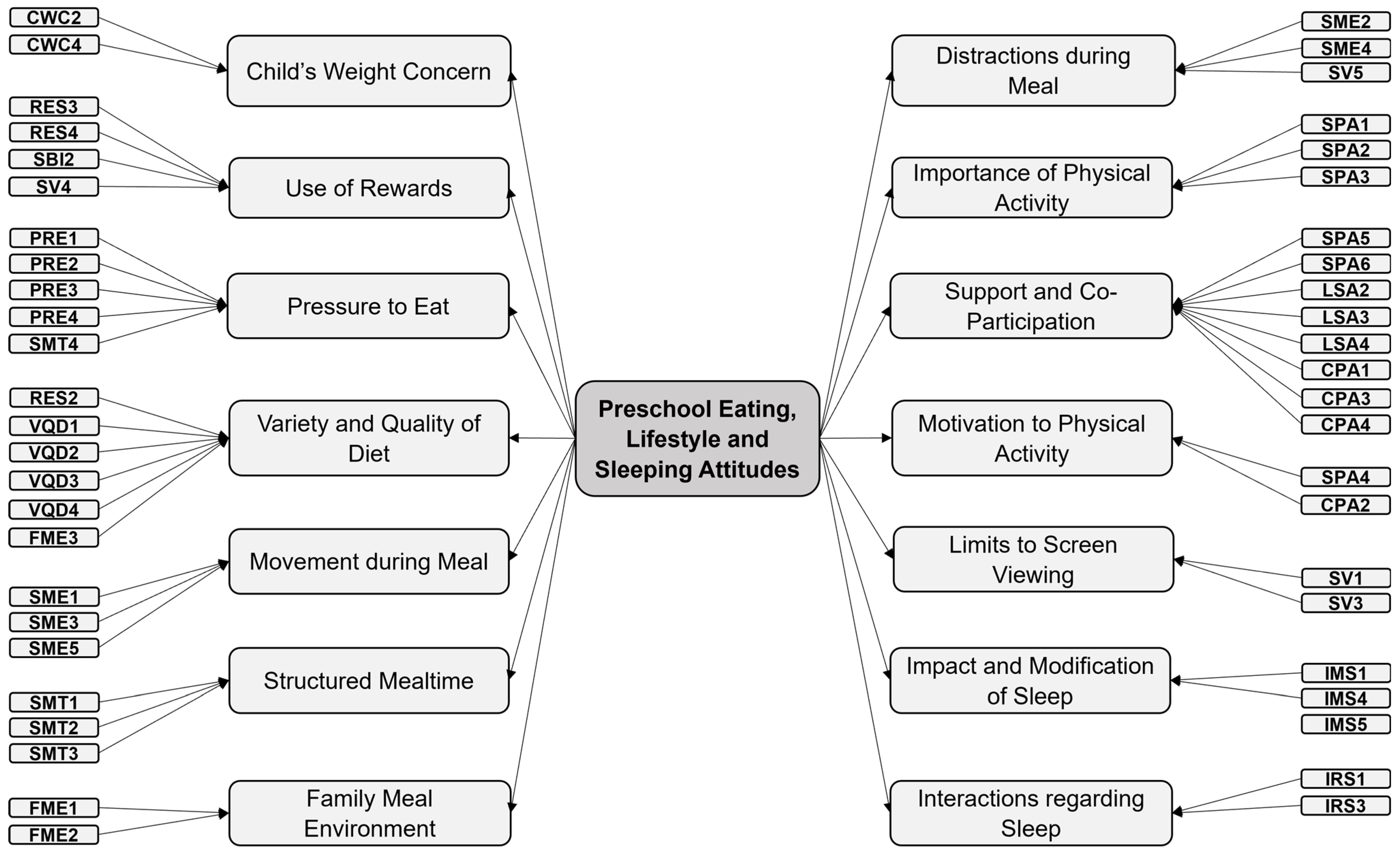
3.3. Structural Validity
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- World Obesity Federation. Global Atlas on Childhood Obesity; World Obesity Federation: London, UK, 2019. [Google Scholar]
- Kachur, S.; Lavie, C.J.; De Schutter, A.; Milani, R.V.; Ventura, H.O. Obesity and Cardiovascular Diseases. Minerva Med. 2017, 108, 212–228. [Google Scholar] [CrossRef] [PubMed]
- Garg, S.K.; Maurer, H.; Reed, K.; Selagamsetty, R. Diabetes and Cancer: Two Diseases with Obesity as a Common Risk Factor. Diabetes Obes. Metab. 2014, 16, 97–110. [Google Scholar] [CrossRef] [PubMed]
- Garrido-Migue, M.; Oliveira, A.; Cavero-Redondo, I.; Álvarez-Bueno, C.; Pozuelo-Carrascosa, D.P.; Soriano-Cano, A.; Martínez-Vizcaíno, V. Prevalence of Overweight and Obesity among European Preschool Children: A Systematic Review and Meta-Regression by Food Group Consumption. Nutrients 2019, 11, 1698. [Google Scholar] [CrossRef] [PubMed]
- AESAN. Estudio Aladino 2019—Estudio de Vigilancia del Crecimiento, Alimentación, Actividad Física, Desarrollo Infantil y Obesidad En España; AESAN: Madrid, Spain, 2019.
- Junta de Andalucía Plan Integral de Obesidad Infantil de Andalucía. Available online: https://www.juntadeandalucia.es/organismos/saludyfamilias/areas/planificacion/plan-integral/paginas/piobin.html (accessed on 11 February 2020).
- Agencia Española de Seguridad Alimentaria y Nutrición Estrategia NAOS. Available online: https://www.aesan.gob.es/AECOSAN/web/nutricion/seccion/estrategia_naos.htm (accessed on 28 January 2024).
- Rolland-Cachera, M.F.; Deheeger, M.; Maillot, M.; Bellisle, F. Early Adiposity Rebound: Causes and Consequences for Obesity in Children and Adults. Int. J. Obes. 2006, 30, S11–S17. [Google Scholar] [CrossRef] [PubMed]
- Pérez-Muñoz, C.; Carretero-Bravo, J.; Ortega-Martín, E.; Ramos-Fiol, B.; Ferriz-Mas, B.; Díaz-Rodríguez, M. Interventions in the First 1000 Days to Prevent Childhood Obesity: A Systematic Review and Quantitative Content Analysis. BMC Public Health 2022, 22, 2367. [Google Scholar] [CrossRef] [PubMed]
- Díaz-Rodríguez, M.; Pérez-Muñoz, C.; Carretero-Bravo, J.; Santi-Cano, M.J.; Carrasco-Sánchez, P.; Barroso-Chirino, C.; Ferriz-Mas, B.C. Impact of an Early 1000-Day Intervention for Obesity Prevention on Adiposity and BMI at Two Years of Age: A Quasi-Experimental Study. J. Glob. Health 2023, 13, 04145. [Google Scholar] [CrossRef] [PubMed]
- Rhodes, R.E.; Guerrero, M.D.; Vanderloo, L.M.; Barbeau, K.; Barbeau, K.; Birken, C.S.; Chaput, J.P.; Faulkner, G.; Janssen, I.; Madigan, S.; et al. Development of a Consensus Statement on the Role of the Family in the Physical Activity, Sedentary, and Sleep Behaviours of Children and Youth. Int. J. Behav. Nutr. Phys. Act. 2020, 17, 74. [Google Scholar] [CrossRef] [PubMed]
- McBride, B.; Fiese, B.; Dev, D.A.; Mcbride, B.A.; Fiese, B.H.; Jones, B.L.; Cho, H.; Harrison, K.; Bost, K.; Donovan, S.; et al. Risk Factors for Overweight/Obesity in Preschool Children: An Ecological Approach. Child. Obes. 2013, 9, 399–408. [Google Scholar] [CrossRef]
- Robinson, S.M.; Crozier, S.R.; Harvey, N.C.; Barton, B.D.; Law, C.M.; Godfrey, K.M.; Cooper, C.; Inskip, H.M. Modifiable Early-Life Risk Factors for Childhood Adiposity and Overweight: An Analysis of Their Combined Impact and Potential for Prevention. Am. J. Clin. Nutr. 2015, 101, 368–375. [Google Scholar] [CrossRef] [PubMed]
- Skouteris, H.; Mccabe, M.; Swinburn, B.; Newgreen, V.; Sacher, P.; Chadwick, P. Parental Influence and Obesity Prevention in Pre-Schoolers: A Systematic Review of Interventions. Obes. Rev. 2011, 12, 315–328. [Google Scholar] [CrossRef] [PubMed]
- Delisle Nyström, C.; Abbott, G.; Cameron, A.J.; Campbell, K.J.; Löf, M.; Salmon, J.; Hesketh, K.D. Maternal Knowledge Explains Screen Time Differences 2 and 3.5 Years Post-Intervention in INFANT. Eur. J. Pediatr. 2021, 180, 3391–3398. [Google Scholar] [CrossRef]
- Hesketh, K.D.; Kuswara, K.; Abbott, G.; Salmon, J.; Hnatiuk, J.A.; Campbell, K.J. How to Change Young Children’s Physical Activity and Sedentary Behavior: Mechanisms of Behavior Change in the INFANT Cluster Randomized Controlled Trial. Children 2021, 8, 470. [Google Scholar] [CrossRef]
- Ling, J.; Robbins, L.B.; Wen, F.; Zhang, N. Lifestyle Interventions in Preschool Children: A Meta-Analysis of Effectiveness. Am. J. Prev. Med. 2017, 53, 102–112. [Google Scholar] [CrossRef]
- He, B.; Long, W.; Li, X.; Yang, W.; Chen, Y.; Zhu, Y. Sugar-Sweetened Beverages Consumption Positively Associated with the Risks of Obesity and Hypertriglyceridemia among Children Aged 7–18 Years in South China. J. Atheroscler. Thromb. 2018, 25, 81–89. [Google Scholar] [CrossRef]
- Xu, H.; Ming Wen, L.; Rissel, C. Associations of Parental Influences with Physical Activity and Screen Time among Young Children: A Systematic Review. J. Obes. 2015, 2015, 546925. [Google Scholar] [CrossRef]
- Miller, A.L.; Miller, S.E.; LeBourgeois, M.K.; Sturza, J.; Rosenblum, K.L.; Lumeng, J.C. Sleep Duration and Quality Are Associated with Eating Behavior in Low-Income Toddlers. Appetite 2019, 135, 100–107. [Google Scholar] [CrossRef]
- Rodriguez-Ayllon, M.; Cornejo, I.E.; Verdejo-Román, J.; Muetzel, R.L.; Migueles, J.H.; Mora-Gonzalez, J.; Solis-Urra, P.; Erickson, K.I.; Hillman, C.H.; Catena, A.; et al. Physical Activity, Sedentary Behavior, and White Matter Microstructure in Children with Overweight or Obesity. Med. Sci. Sports Exerc. 2020, 52, 1218–1226. [Google Scholar] [CrossRef]
- Sleddens, E.F.C.; Kremers, S.P.J.; Hughes, S.O.; Cross, M.B.; Thijs, C.; De Vries, N.K.; O’Connor, T.M. Physical Activity Parenting: A Systematic Review of Questionnaires and Their Associations with Child Activity Levels. Obes. Rev. 2012, 13, 1015–1033. [Google Scholar] [CrossRef]
- Nascimento-Ferreira, M.V.; Collese, T.S.; de Moraes, A.C.F.; Rendo-Urteaga, T.; Moreno, L.A.; Carvalho, H.B. Validity and Reliability of Sleep Time Questionnaires in Children and Adolescents: A Systematic Review and Meta-Analysis. Sleep. Med. Rev. 2016, 30, 85–96. [Google Scholar] [CrossRef]
- Trost, S.G.; Loprinzi, P.D. Parental Influences on Physical Activity Behavior in Children and Adolescents: A Brief Review. Am. J. Lifestyle Med. 2011, 5, 171–181. [Google Scholar] [CrossRef]
- Rhodes, R.E.; Perdew, M.; Malli, S. Correlates of Parental Support of Child and Youth Physical Activity: A Systematic Review. Int. J. Behav. Med. 2020, 27, 636–646. [Google Scholar] [CrossRef] [PubMed]
- Anastasiou, C.A.; Fappa, E.; Zachari, K.; Mavrogianni, C.; Van Stappen, V.; Kivelä, J.; Virtanen, E.; González-Gil, E.M.; Flores-Barrantes, P.; Nánási, A.; et al. Development and Reliability of Questionnaires for the Assessment of Diet and Physical Activity Behaviors in a Multi-Country Sample in Europe the Feel4Diabetes Study. BMC Endocr. Disord. 2020, 20, 135. [Google Scholar] [CrossRef] [PubMed]
- Vioque, J.; Gimenez-Monzo, D.; Navarrete-Muñoz, E.M.; Garcia-De-la-hera, M.; Gonzalez-Palacios, S.; Rebagliato, M.; Ballester, F.; Murcia, M.; Iñiguez, C.; Granado, F. Reproducibility and Validity of a Food Frequency Questionnaire Designed to Assess Diet in Children Aged 4–5 Years. PLoS ONE 2016, 11, e0167338. [Google Scholar] [CrossRef] [PubMed]
- Dalmau, J.; Peña-Quintana, L.; Moráis, A.; Martínez, V.; Varea, V.; Martínez, M.J.; Soler, B. Análisis Cuantitativo de La Ingesta de Nutrientes En Niños Menores de 3 Años. Estudio ALSALMA. An. Pediatría (Engl. Ed.) 2015, 82, 255–266. [Google Scholar] [CrossRef] [PubMed]
- Figueroa, R.; Saltzman, J.A.; Aftosmes-Tobio, A.; Davison, K.K. The Obesity Parenting Intervention Scale: Factorial Validity and Invariance Among Head Start Parents. Am. J. Prev. Med. 2019, 57, 844–852. [Google Scholar] [CrossRef] [PubMed]
- Romanos-Nanclares, A.; Zazpe, I.; Santiago, S.; Marín, L.; Rico-Campà, A.; Martín-Calvo, N. Influence of Parental Healthy-Eating Attitudes and Nutritional Knowledge on Nutritional Adequacy and Diet Quality among Preschoolers: The SENDO Project. Nutrients 2018, 10, 1875. [Google Scholar] [CrossRef] [PubMed]
- Garcia-Conde, M.G.; Marin, L.; de Maya, S.R.; Cuestas, P.J. Parental Attitudes to Childhood Overweight: The Multiple Paths through Healthy Eating, Screen Use, and Sleeping Time. Int. J. Environ. Res. Public Health 2020, 17, 7885. [Google Scholar] [CrossRef] [PubMed]
- Lanzarote-Fernández, M.D.; Lozano-Oyola, J.F.; Gómez-De-Terreros-Guardiola, M.; Avilés-Carvajal, I.; Martínez-Cervantes, R.J.; Moreno, J.P. Spanish Version of the Family Health Behavior Scale: Adaptation and Validation. Int. J. Environ. Res. Public Health 2019, 16, 810. [Google Scholar] [CrossRef] [PubMed]
- Carretero-Bravo, J.; Díaz-Rodríguez, M.; Ferriz-Mas, B.C.; Pérez-Muñoz, C.; González-Caballero, J.L. The Preschool Eating, Lifestyle, and Sleeping Attitudes Scale (PRELSA Scale): Construction and Pilot Testing of a Tool to Measure Factors Associated with Childhood Obesity. Healthcare 2023, 11, 1365. [Google Scholar] [CrossRef] [PubMed]
- Birch, L.L.; Fisher, J.O.; Grimm-thomas, K.; Markey, C.N.; Sawyer, R.; Johnson, S.L. Confirmatory Factor Analysis of the Child Feeding Questionnaire: A Measure of Parental Attitudes, Beliefs and Practices about Child Feeding and Obesity Proneness. Appetite 2001, 36, 201–210. [Google Scholar] [CrossRef] [PubMed]
- Jansen, E.; Mallan, K.M.; Nicholson, J.M.; Daniels, L.A. The Feeding Practices and Structure Questionnaire: Construction and Initial Validation in a Sample of Australian First-Time Mothers and Their 2-Year Olds. Int. J. Behav. Nutr. Phys. Act. 2014, 11, 72. [Google Scholar] [CrossRef] [PubMed]
- Larios, S.E.; Ayala, G.X.; Arredondo, E.M.; Baquero, B.; Elder, J.P. Development and Validation of a Scale to Measure Latino Parenting Strategies Related to Children’s Obesigenic Behaviors. The Parenting Strategies for Eating and Activity Scale (PEAS). Appetite 2009, 52, 166–172. [Google Scholar] [CrossRef] [PubMed]
- O’Connor, T.M.; Cerin, E.; Hughes, S.O.; Robles, J.; Thompson, D.I.; Mendoza, J.A.; Baranowski, T.; Lee, R.E. Psychometrics of the Preschooler Physical Activity Parenting Practices Instrument among a Latino Sample. Int. J. Behav. Nutr. Phys. Act. 2014, 11, 3. [Google Scholar] [CrossRef] [PubMed]
- Määttä, S.; Kaukonen, R.; Vepsäläinen, H.; Lehto, E.; Ylönen, A.; Ray, C.; Erkkola, M.; Roos, E. The Mediating Role of the Home Environment in Relation to Parental Educational Level and Preschool Children’s Screen Time: A Cross-Sectional Study. BMC Public Health 2017, 17, 688. [Google Scholar] [CrossRef]
- Bessey, M.; Coulombe, J.A.; Smith, I.M.; Corkum, P. Assessing Parental Sleep Attitudes and Beliefs in Typically Developing Children and Children with ADHD and ASD. Child. Health Care 2013, 42, 116–133. [Google Scholar] [CrossRef]
- Alfano, C.A.; Smith, V.C.; Reynolds, K.C.; Reddy, R.; Dougherty, L.R. The Parent-Child Sleep Interactions Scale (PSIS) for Preschoolers: Factor Structure and Initial Psychometric Properties. J. Clin. Sleep Med. 2013, 9, 1153. [Google Scholar] [CrossRef] [PubMed]
- World Health Organization. WHO Guidelines on Physical Activity, Sedentary Behaviour; World Health Organization: Geneva, Switzerland, 2020; ISBN 9789241550536.
- Limesurvey GmbH. LimeSurvey: An Open Source Survey Tool 2023; Limesurvey GmbH: Hamburg, Germany, 2023. [Google Scholar]
- Mokkink, L.B.; Terwee, C.B.; Knol, D.L.; Stratford, P.W.; Alonso, J.; Patrick, D.L.; Bouter, L.M.; De Vet, H.C. The COSMIN Checklist for Evaluating the Methodological Quality of Studies on Measurement Properties: A Clarification of Its Content. BMC Med. Res. Methodol. 2010, 10, 22. [Google Scholar] [CrossRef] [PubMed]
- Drasgow, F. Polychoric and Polyserial Correlations. In Wiley StatsRef: Statistics Reference Online; Wiley: Hoboken, NJ, USA, 2014. [Google Scholar] [CrossRef]
- Streiner, D.; Norman, G.; Cairney, J. Health Measurement Scales, 15th ed.; Oxford University Press: Oxford, UK, 2015. [Google Scholar]
- Li, C.H. Confirmatory Factor Analysis with Ordinal Data: Comparing Robust Maximum Likelihood and Diagonally Weighted Least Squares. Behav. Res. Methods 2016, 48, 936–949. [Google Scholar] [CrossRef] [PubMed]
- Cronbach, L.J. Coefficient Alpha and the Internal Structure of Tests. Psychometrika 1951, 16, 297–334. [Google Scholar] [CrossRef]
- Terwee, C.B.; Bot, S.D.M.; de Boer, M.R.; van der Windt, D.A.W.M.; Knol, D.L.; Dekker, J.; Bouter, L.M.; de Vet, H.C.W. Quality Criteria Were Proposed for Measurement Properties of Health Status Questionnaires. J. Clin. Epidemiol. 2007, 60, 34–42. [Google Scholar] [CrossRef] [PubMed]
- Gadermann, A.M.; Guhn, M.; Zumbo, B.D. Estimating Ordinal Reliability for Likert-Type and Ordinal Item Response Data: A Conceptual, Empirical, and Practical Guide. Pract. Assess. Res. Eval. 2012, 17, 3. [Google Scholar] [CrossRef]
- Cheung, G.W.; Rensvold, R.B. Evaluating Goodness-of-Fit Indexes for Testing Measurement Invariance. Struct. Equ. Model. 2002, 9, 233–255. [Google Scholar] [CrossRef]
- Chen, F.F. Sensitivity of Goodness of Fit Indexes to Lack of Measurement Invariance. Struct. Equ. Model. 2007, 14, 464–504. [Google Scholar] [CrossRef]
- Rosseel, Y. Lavaan: An R Package for Structural Equation Modeling. J. Stat. Softw. 2012, 48, 1–36. [Google Scholar] [CrossRef]
- Litchford, A.; Savoie Roskos, M.R.; Wengreen, H. Influence of Fathers on the Feeding Practices and Behaviors of Children: A Systematic Review. Appetite 2020, 147, 104558. [Google Scholar] [CrossRef] [PubMed]
- Andrade, C. The Limitations of Online Surveys. Indian J. Psychol. Med. 2020, 42, 575–576. [Google Scholar] [CrossRef] [PubMed]
- Wang, Y.; Min, J.; Khuri, J.; Li, M. A Systematic Examination of the Association between Parental and Child Obesity across Countries. Adv. Nutr. 2017, 8, 436. [Google Scholar] [CrossRef] [PubMed]
- De Vet, H.; Terwee, C.; Mokkink, L.; Knol, D. Measurement in Medicine, 1st ed.; Cambridge University Press: Cambdridge, UK, 2011; ISBN 978-0-521-11820-0. [Google Scholar]
- Rea, C.J.; Smith, R.L.; Taveras, E.M. Associations of Parent Health Behaviors and Parenting Practices with Sleep Duration in Overweight and Obese Children. J. Clin. Sleep Med. 2016, 12, 1493. [Google Scholar] [CrossRef] [PubMed][Green Version]
- Musher-Eizenman, D.; Holub, S. Comprehensive Feeding Practices Questionnaire: Validation of a New Measure of Parental Feeding Practices. J. Pediatr. Psychol. 2007, 32, 960–972. [Google Scholar] [CrossRef]
- Canals-Sans, J.; Blanco-Gómez, A.; Luque, V.; Ferré, N.; Ferrando, P.J.; Gispert-Llauradó, M.; Escribano, J.; Closa-Monasterolo, R. Validation of the Child Feeding Questionnaire in Spanish Parents of Schoolchildren. J. Nutr. Educ. Behav. 2016, 48, 383–391.e1. [Google Scholar] [CrossRef] [PubMed]
- Kyriazos, T.A. Applied Psychometrics: Sample Size and Sample Power Considerations in Factor Analysis (EFA, CFA) and SEM in General. Psychology 2018, 09, 2207–2230. [Google Scholar] [CrossRef]
- Schumacker, R.E.; Lomax, R.G. A Beginner’s Guide to Structural Equation Modeling, 4th ed.; Taylor & Francis: Abingdon, UK, 2015. [Google Scholar] [CrossRef]
- Homs, C.; Berruezo, P.; Arcarons, A.; Wärnberg, J.; Osés, M.; González-Gross, M.; Gusi, N.; Aznar, S.; Marín-Cascales, E.; González-Valeiro, M.Á.; et al. Independent and Joined Association between Socioeconomic Indicators and Pediatric Obesity in Spain: The PASOS Study. Nutrients 2023, 15, 1987. [Google Scholar] [CrossRef] [PubMed]
- Moschonis, G.; Siopis, G.; Anastasiou, C.; Iotova, V.; Stefanova, T.; Dimova, R.; Rurik, I.; Radó, A.S.; Cardon, G.; De Craemer, M.; et al. Prevalence of Childhood Obesity by Country, Family Socio-Demographics, and Parental Obesity in Europe: The Feel4Diabetes Study. Nutrients 2022, 14, 1830. [Google Scholar] [CrossRef] [PubMed]



{kind=link}
{kind=link}
| Row | Missing | 1 | 2 | 3 | 4 | 5 | Mean | SD | SKEW |
|---|---|---|---|---|---|---|---|---|---|
| CWC1 | 0.00 | 0.86 | 6.65 | 90.39 | 1.97 | 0.12 | 2.94 | 0.34 | −2.34 |
| CWC2 | 0.00 | 66.63 | 18.47 | 8.87 | 3.69 | 2.34 | 1.57 | 0.97 | 1.82 |
| CWC3 | 0.00 | 39.66 | 16.87 | 16.13 | 11.45 | 15.89 | 2.49 | 1.5 | 0.5 |
| CWC4 | 0.00 | 30.05 | 15.15 | 17.49 | 13.18 | 24.14 | 2.88 | 1.56 | 0.12 |
| RES1 | 0.38 | 0.74 | 1.11 | 1.11 | 7.27 | 89.41 | 4.84 | 0.56 | −4.51 |
| RES2 | 0.25 | 0.99 | 1.23 | 1.97 | 8.13 | 87.44 | 4.8 | 0.63 | −3.99 |
| RES3 | 0.88 | 50.25 | 17.73 | 5.42 | 17.36 | 8.37 | 2.15 | 1.41 | 0.82 |
| RES4 | 0.51 | 78.69 | 11.33 | 2.96 | 5.05 | 1.48 | 1.39 | 0.89 | 2.5 |
| PRE1 | 0.38 | 47.91 | 18.35 | 4.19 | 21.55 | 7.64 | 2.21 | 1.42 | 0.7 |
| PRE2 | 0.88 | 14.04 | 8.99 | 2.34 | 25.25 | 48.52 | 3.85 | 1.47 | −1.01 |
| PRE3 | 0.63 | 48.03 | 21.67 | 1.48 | 18.97 | 9.24 | 2.18 | 1.43 | 0.82 |
| PRE4 | 1.14 | 27.09 | 10.84 | 1.85 | 25.25 | 33.87 | 3.29 | 1.66 | −0.37 |
| VQD1 | 0.38 | 1.48 | 2.34 | 0.99 | 6.90 | 87.93 | 4.79 | 0.71 | −3.93 |
| VQD2 | 0.38 | 62.32 | 24.88 | 2.34 | 7.88 | 2.09 | 1.62 | 1.01 | 1.76 |
| VQD3 | 0.76 | 3.57 | 6.77 | 2.22 | 25.74 | 60.96 | 4.35 | 1.06 | −1.82 |
| VQD4 | 0.51 | 0.62 | 1.11 | 0.86 | 9.61 | 87.32 | 4.83 | 0.55 | −4.26 |
| VQD5 | 1.39 | 31.77 | 24.01 | 3.08 | 24.51 | 15.15 | 2.67 | 1.52 | 0.28 |
| SME1 | 0.13 | 68.47 | 17.12 | 4.93 | 6.16 | 3.20 | 1.59 | 1.05 | 1.87 |
| SME2 | 0.25 | 58.13 | 19.70 | 7.51 | 10.84 | 3.57 | 1.81 | 1.18 | 1.3 |
| SME3 | 0.51 | 2.09 | 6.77 | 4.31 | 20.94 | 65.39 | 4.41 | 1.01 | −1.82 |
| SME4 | 0.13 | 67.61 | 15.02 | 5.30 | 9.61 | 2.34 | 1.63 | 1.08 | 1.65 |
| SME5 | 0.63 | 60.34 | 20.32 | 4.56 | 8.25 | 5.91 | 1.77 | 1.21 | 1.52 |
| SMT1 | 0.13 | 33.74 | 29.31 | 1.23 | 21.55 | 14.04 | 2.52 | 1.49 | 0.49 |
| SMT2 | 0.38 | 16.38 | 27.46 | 5.91 | 33.62 | 16.26 | 3.05 | 1.39 | −0.1 |
| SMT3 | 1.01 | 1.97 | 5.05 | 2.34 | 26.97 | 62.68 | 4.45 | 0.92 | −2.01 |
| SMT4 | 0.76 | 68.23 | 17.86 | 8.74 | 3.69 | 0.74 | 1.49 | 0.86 | 1.82 |
| FME1 | 0.76 | 1.11 | 1.72 | 4.06 | 13.55 | 78.82 | 4.69 | 0.73 | −2.85 |
| FME2 | 0.76 | 4.80 | 2.71 | 2.46 | 16.01 | 73.28 | 4.51 | 1.03 | −2.41 |
| FME3 | 0.88 | 1.23 | 3.08 | 5.42 | 19.95 | 69.46 | 4.55 | 0.83 | −2.17 |
| SPA1 | 0.51 | 0.12 | 0.49 | 0.74 | 7.27 | 90.89 | 4.89 | 0.4 | −4.81 |
| SPA2 | 0.63 | 0.86 | 1.97 | 1.72 | 16.50 | 78.33 | 4.7 | 0.69 | −3.01 |
| SPA3 | 1.01 | 0.37 | 0.49 | 0.74 | 9.24 | 88.18 | 4.86 | 0.46 | −4.53 |
| SPA4 | 1.77 | 2.59 | 5.05 | 6.16 | 35.34 | 49.14 | 4.25 | 0.97 | −1.56 |
| SPA5 | 0.88 | 0.37 | 0.00 | 2.09 | 11.95 | 84.73 | 4.82 | 0.49 | −3.53 |
| SPA6 | 1.01 | 2.34 | 4.06 | 3.33 | 21.18 | 68.10 | 4.5 | 0.92 | −2.22 |
| LSA1 | 0.25 | 0.00 | 0.37 | 0.37 | 5.79 | 93.23 | 4.92 | 0.32 | −5.16 |
| LSA2 | 0.76 | 0.00 | 1.23 | 2.83 | 12.07 | 83.13 | 4.78 | 0.55 | −2.87 |
| LSA3 | 0.88 | 0.37 | 1.35 | 2.34 | 14.66 | 80.42 | 4.75 | 0.6 | −3.07 |
| LSA4 | 1.14 | 1.72 | 2.71 | 3.94 | 16.38 | 74.14 | 4.6 | 0.83 | −2.52 |
| CPA1 | 0.76 | 0.25 | 0.12 | 1.35 | 9.11 | 88.42 | 4.87 | 0.43 | −4.2 |
| CPA2 | 1.39 | 1.11 | 5.67 | 9.36 | 39.66 | 42.86 | 4.19 | 0.91 | −1.21 |
| CPA3 | 0.88 | 0.62 | 2.71 | 5.54 | 25.62 | 64.66 | 4.53 | 0.77 | −1.92 |
| CPA4 | 0.51 | 0.49 | 1.35 | 1.48 | 10.84 | 85.34 | 4.8 | 0.58 | −3.72 |
| SBI1 | 1.39 | 46.92 | 30.54 | 6.03 | 9.61 | 5.30 | 1.94 | 1.19 | 1.24 |
| SBI2 | 0.51 | 73.40 | 16.75 | 2.46 | 4.80 | 2.09 | 1.45 | 0.92 | 2.37 |
| SV1 | 0.13 | 1.97 | 0.74 | 0.62 | 8.62 | 87.93 | 4.8 | 0.68 | −4.28 |
| SV2 | 0.13 | 52.71 | 26.97 | 3.20 | 12.19 | 4.80 | 1.9 | 1.22 | 1.26 |
| SV3 | 0.13 | 1.35 | 2.34 | 1.23 | 13.55 | 81.40 | 4.71 | 0.74 | −3.23 |
| SV4 | 0.38 | 44.58 | 18.84 | 1.85 | 26.72 | 7.64 | 2.34 | 1.46 | 0.52 |
| SV5 | 0.13 | 63.42 | 16.50 | 5.30 | 10.84 | 3.82 | 1.75 | 1.19 | 1.44 |
| IMS1 | 1.01 | 2.71 | 1.11 | 0.12 | 5.05 | 90.02 | 4.8 | 0.75 | −4.26 |
| IMS2 | 20.48 | 7.27 | 5.05 | 2.96 | 17.49 | 46.92 | 4.15 | 1.3 | −1.46 |
| IMS3 | 22.38 | 13.67 | 7.14 | 3.69 | 15.39 | 37.68 | 3.73 | 1.55 | −0.82 |
| IMS4 | 2.65 | 1.72 | 1.11 | 0.99 | 11.33 | 82.14 | 4.76 | 0.7 | −3.76 |
| IMS5 | 0.51 | 0.74 | 1.11 | 0.37 | 7.76 | 89.53 | 4.85 | 0.54 | −4.8 |
| IRS1 | 0.00 | 1.11 | 4.93 | 0.99 | 29.80 | 63.18 | 4.48 | 0.84 | −2.07 |
| IRS2 | 0.51 | 51.72 | 30.05 | 1.60 | 11.08 | 5.05 | 1.86 | 1.19 | 1.38 |
| IRS3 | 0.25 | 0.37 | 0.49 | 0.86 | 8.50 | 89.53 | 4.87 | 0.45 | −4.8 |
| IRS4 | 3.16 | 23.52 | 18.72 | 7.39 | 18.10 | 29.19 | 3.09 | 1.6 | −0.07 |
| IRS5 | 0.13 | 87.93 | 6.53 | 0.99 | 2.46 | 1.97 | 1.24 | 0.76 | 3.68 |
| Model | Chi2 Base | Chi2 | df | RMSEA | 90 CI | CFI | TLI | Variance Explained |
|---|---|---|---|---|---|---|---|---|
| EFA 55 ITEMS 12 FACTORS | 16,494.13 | 1101.928 | 891 | 0.017 | (0.014, 0.021) | 0.986 | 0.977 | 57.1% |
| EFA 55 ITEMS 13 FACTORS | 16,494.13 | 1001.915 | 848 | 0.015 | (0.011, 0.019) | 0.990 | 0.982 | 58.3% |
| EFA 55 ITEMS 14 FACTORS | 16,494.13 | 908.883 | 806 | 0.013 | (0.007, 0.017) | 0.993 | 0.987 | 59.7% |
| EFA 51 ITEMS 14 FACTORS | 14,310.81 | 708.764 | 652 | 0.011 | (0.004, 0.016) | 0.996 | 0.991 | 60.6% |
| EFA 48 ITEMS 14 FACTORS | 12,769.16 | 562.331 | 547 | 0.006 | (0.001, 0.012) | 0.998 | 0.996 | 61.3% |
| # Of Items | Range | Mean Item | Sum Mean | Alpha Cronbach | |
|---|---|---|---|---|---|
| F1 | 2 | 2–15 | 3.77 | 7.54 | 0.84 |
| F2 | 4 | 4–20 | 4.15 | 16.60 | 0.93 |
| F3 | 5 | 5–25 | 3.37 | 16.87 | 0.9 |
| F4 | 6 | 10–30 | 4.60 | 27.58 | 0.94 |
| F5 | 3 | 3–15 | 4.34 | 13.01 | 0.97 |
| F6 | 3 | 3–15 | 3.60 | 10.81 | 0.88 |
| F7 | 2 | 2–10 | 4.57 | 9.14 | 0.8 |
| F8 | 3 | 3–15 | 4.27 | 12.81 | 0.92 |
| F9 | 3 | 3–15 | 4.79 | 14.37 | 0.97 |
| F10 | 8 | 8–40 | 4.67 | 37.33 | 0.97 |
| F11 | 2 | 2–10 | 4.16 | 8.31 | 0.94 |
| F12 | 2 | 2–10 | 4.75 | 9.50 | 0.9 |
| F13 | 3 | 3–15 | 4.74 | 14.21 | 0.94 |
| F14 | 2 | 2–10 | 4.67 | 9.34 | 0.72 |
| TOTAL | 48 | 125–238 | 4.30 | 207.42 | 0.89 |
| CWC | REW | PRE | VQD | MOV | SMT | FME | DIS | IPA | SCP | MOT | LSV | IMS | IRS | R2 | |
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| CWC2 | 0.74 | 0.548 | |||||||||||||
| CWC4 | 0.661 | 0.437 | |||||||||||||
| RES3 | 0.726 | 0.527 | |||||||||||||
| RES4 | 0.707 | 0.5 | |||||||||||||
| SBI2 | 0.685 | 0.469 | |||||||||||||
| SV4 | 0.659 | 0.435 | |||||||||||||
| PRE1 | 0.766 | 0.587 | |||||||||||||
| PRE2 | 0.65 | 0.423 | |||||||||||||
| PRE3 | 0.795 | 0.632 | |||||||||||||
| PRE4 | 0.685 | 0.47 | |||||||||||||
| FME4 | 0.335 | 0.112 | |||||||||||||
| RES2 | 0.687 | 0.472 | |||||||||||||
| VQD1 | 0.55 | 0.303 | |||||||||||||
| VQD2 | −0.686 | 0.47 | |||||||||||||
| VQD3 | 0.603 | 0.364 | |||||||||||||
| VQD4 | 0.729 | 0.532 | |||||||||||||
| FME3 | 0.779 | 0.607 | |||||||||||||
| SME1 | 0.894 | 0.8 | |||||||||||||
| SME3 | −0.843 | 0.71 | |||||||||||||
| SME5 | 0.743 | 0.552 | |||||||||||||
| SMT1 | 0.824 | 0.68 | |||||||||||||
| SMT2 | 0.547 | 0.299 | |||||||||||||
| SMT3 | −0.557 | 0.311 | |||||||||||||
| FME1 | 0.715 | 0.511 | |||||||||||||
| FME2 | 0.718 | 0.516 | |||||||||||||
| SME2 | 0.867 | 0.751 | |||||||||||||
| SME4 | 0.648 | 0.419 | |||||||||||||
| SV5 | 0.914 | 0.835 | |||||||||||||
| SPA1 | 0.913 | 0.834 | |||||||||||||
| SPA2 | 0.798 | 0.636 | |||||||||||||
| SPA3 | 0.875 | 0.766 | |||||||||||||
| SPA5 | 0.856 | 0.732 | |||||||||||||
| SPA6 | 0.649 | 0.422 | |||||||||||||
| LSA2 | 0.697 | 0.486 | |||||||||||||
| LSA3 | 0.749 | 0.56 | |||||||||||||
| LSA4 | 0.54 | 0.291 | |||||||||||||
| CPA1 | 0.598 | 0.358 | |||||||||||||
| CPA3 | 0.698 | 0.487 | |||||||||||||
| CPA4 | 0.774 | 0.598 | |||||||||||||
| SPA4 | 0.762 | 0.58 | |||||||||||||
| CPA2 | 0.848 | 0.72 | |||||||||||||
| SV1 | 0.782 | 0.612 | |||||||||||||
| SV3 | 0.738 | 0.545 | |||||||||||||
| IMS1 | 0.687 | 0.472 | |||||||||||||
| IMS4 | 0.769 | 0.591 | |||||||||||||
| IMS5 | 0.91 | 0.829 | |||||||||||||
| IRS1 | 0.501 | 0.251 | |||||||||||||
| IRS3 | 0.694 | 0.481 | |||||||||||||
| Correlations between Factors | |||||||||||||||
| CWC | REW | PRE | VQD | MOV | SMT | FME | DIS | IPA | SCP | MOT | LSV | IMS | IRS | ||
| CWC | 1 | ||||||||||||||
| REW | 0.052 | 1 | |||||||||||||
| PRE | 0.101 | 0.563 * | 1 | ||||||||||||
| VQD | 0.083 | −0.528 * | −0.342 * | 1 | |||||||||||
| MOV | −0.088 | −0.081 | −0.388 * | −0.002 | 1 | ||||||||||
| SMT | −0.242 | −0.186 * | −0.549 * | 0.166 * | 0.648 * | 1 | |||||||||
| FME | 0.095 | −0.241 * | −0.104 | 0.493 * | −0.227 * | −0.079 | 1 | ||||||||
| DIS | −0.025 | 0.664 * | 0.399 * | −0.492 * | 0.027 | −0.105 | −0.294 * | 1 | |||||||
| IPA | 0.05 | −0.3 * | −0.228 * | 0.546 * | 0.037 | 0.059 | 0.345 * | −0.207 * | 1 | ||||||
| SCP | 0.09 | −0.273 * | −0.295 * | 0.61 * | −0.004 | 0.147 * | 0.41 * | −0.235 * | 0.828 * | 1 | |||||
| MOT | 0.121 * | −0.008 | 0.057 | 0.339 * | −0.029 | −0.06 | 0.237 * | −0.049 | 0.577 * | 0.675 * | 1 | ||||
| LSV | 0.112 * | −0.385 * | −0.255 * | 0.651 * | −0.046 | 0.074 | 0.417 * | −0.399 * | 0.513 * | 0.552 * | 0.224 * | 1 | |||
| IMS | 0.046 | −0.297 * | −0.166 * | 0.495 * | −0.11 * | 0.01 | 0.415 * | −0.299 * | 0.522 * | 0.643 * | 0.241 * | 0.581 * | 1 | ||
| IRS | 0.013 | −0.104 | 0.098 | 0.319 * | −0.299 * | −0.229 * | 0.416 * | −0.051 | 0.351 * | 0.405 * | 0.326 * | 0.359 * | 0.522 * | 1 | |
| Variable | Model | CFI | RMSEA | Cfi Diff | RMSEA Diff |
|---|---|---|---|---|---|
| Education | Configural Model | 0.932 | 0.031 | ||
| Metric Model | 0.932 | 0.031 | 0 | 0 | |
| Scalar Model | 0.932 | 0.030 | 0 | 0.001 | |
| Income | Configural Model | 0.935 | 0.031 | ||
| Metric Model | 0.937 | 0.030 | 0.002 | 0.001 | |
| Scalar Model | 0.937 | 0.030 | 0 | 0 | |
| Marital Status | Configural Model | 0.927 | 0.032 | ||
| Metric Model | 0.929 | 0.032 | 0 | 0 | |
| Scalar Model | 0.929 | 0.031 | 0 | 0.001 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Carretero-Bravo, J.; Díaz-Rodríguez, M.; Ferriz-Mas, B.C.; Pérez-Muñoz, C.; González-Caballero, J.L. The Dimensionality, Consistency, and Structural Validity of an Instrument Used to Measure Obesogenic Attitudes in Parents from Southern Spain (The PRELSA Scale). Nutrients 2024, 16, 1135. https://doi.org/10.3390/nu16081135
Carretero-Bravo J, Díaz-Rodríguez M, Ferriz-Mas BC, Pérez-Muñoz C, González-Caballero JL. The Dimensionality, Consistency, and Structural Validity of an Instrument Used to Measure Obesogenic Attitudes in Parents from Southern Spain (The PRELSA Scale). Nutrients. 2024; 16(8):1135. https://doi.org/10.3390/nu16081135
Chicago/Turabian StyleCarretero-Bravo, Jesús, Mercedes Díaz-Rodríguez, Bernardo Carlos Ferriz-Mas, Celia Pérez-Muñoz, and Juan Luis González-Caballero. 2024. "The Dimensionality, Consistency, and Structural Validity of an Instrument Used to Measure Obesogenic Attitudes in Parents from Southern Spain (The PRELSA Scale)" Nutrients 16, no. 8: 1135. https://doi.org/10.3390/nu16081135
APA StyleCarretero-Bravo, J., Díaz-Rodríguez, M., Ferriz-Mas, B. C., Pérez-Muñoz, C., & González-Caballero, J. L. (2024). The Dimensionality, Consistency, and Structural Validity of an Instrument Used to Measure Obesogenic Attitudes in Parents from Southern Spain (The PRELSA Scale). Nutrients, 16(8), 1135. https://doi.org/10.3390/nu16081135