
Metabolic and Nutritional Issues after Lower Digestive Tract Surgery: The Important Role of the Dietitian in a Multidisciplinary Setting
 ,
, 
Abstract
1. Introduction
2. Small Bowel Surgery
3. Colectomy
3.1. Ileocecectomy
3.2. Low Anterior Resection and Abdominoperineal Resection
3.3. Proctocolectomy
4. Stoma Formation
4.1. Ileostomy
4.2. Colostomy
5. IBD Surgery
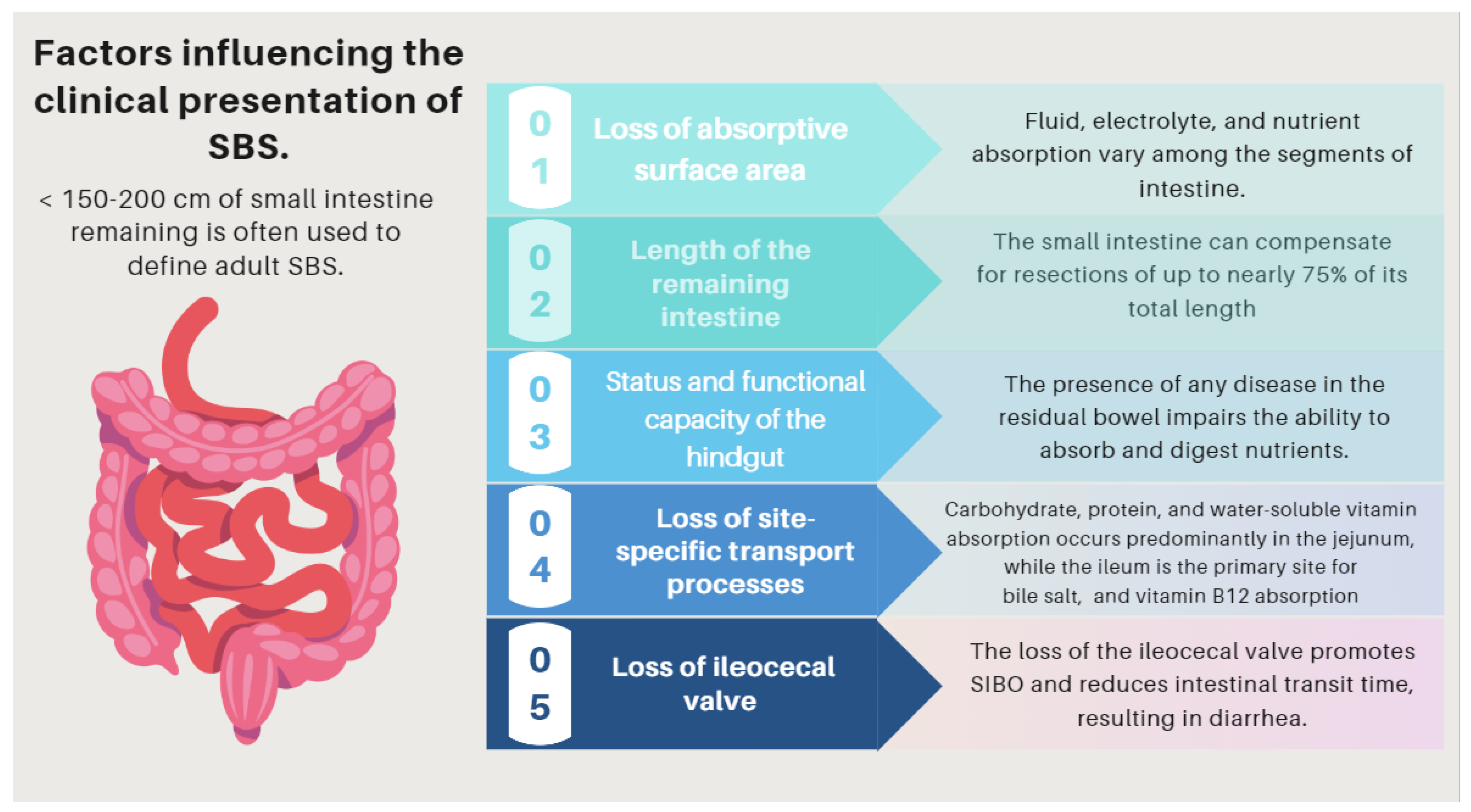
6. Short Bowel Syndrome (SBS)
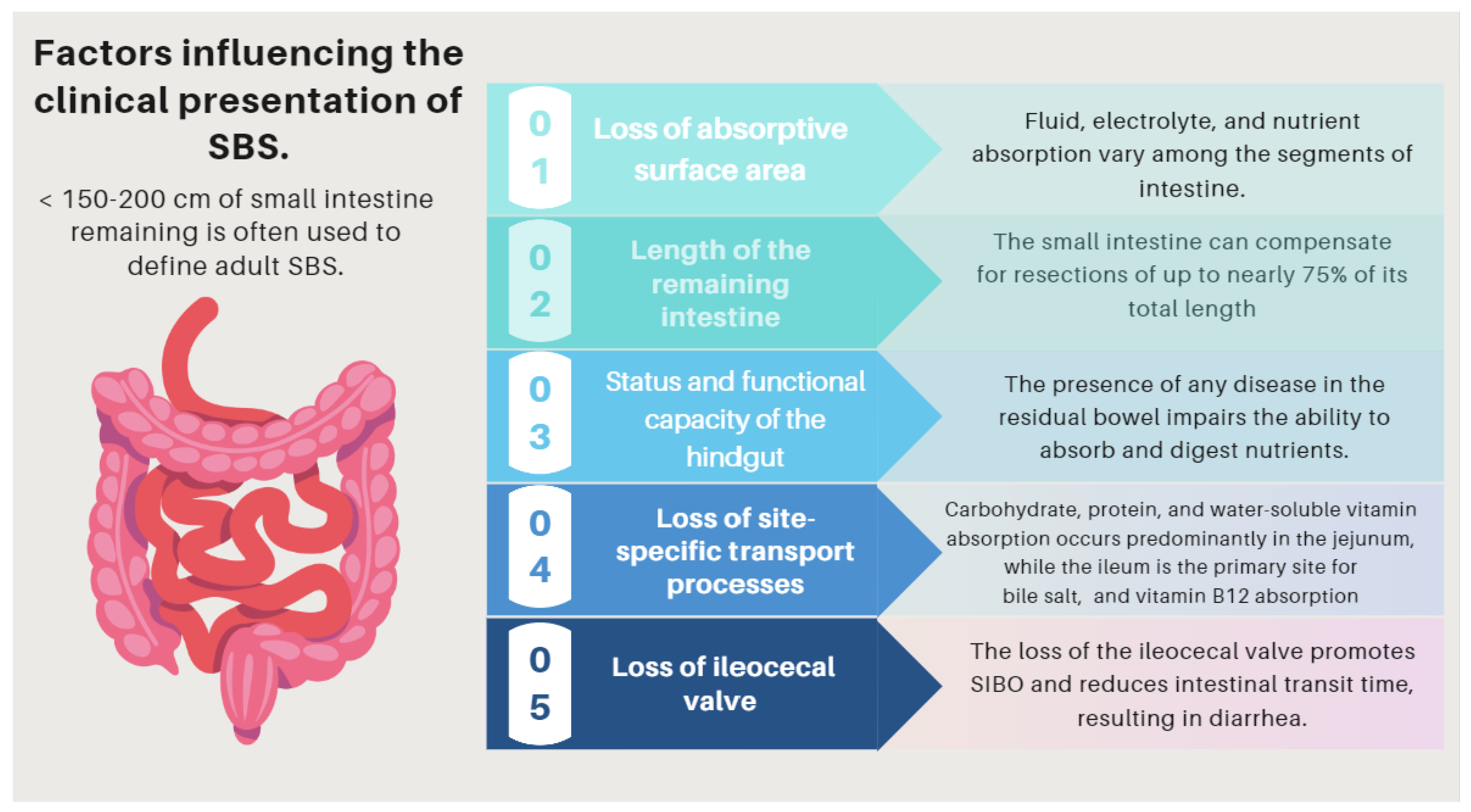
- (1)
- Loss of absorptive surface area and, crucially, the length of the remaining intestine.
- (2)
- Status and functional capacity of the intestinal mucosa.
- (3)
- Loss of site-specific transport processes.
- (4)
- Loss of site-specific endocrine cells and gastrointestinal (GI) hormones.
- (5)
- Loss of the ileocecal valve (Figure 3).
6.1. Clinical Presentation
6.1.1. Global Outlook

| Complications Related to SBS | Pathogenesis |
|---|---|
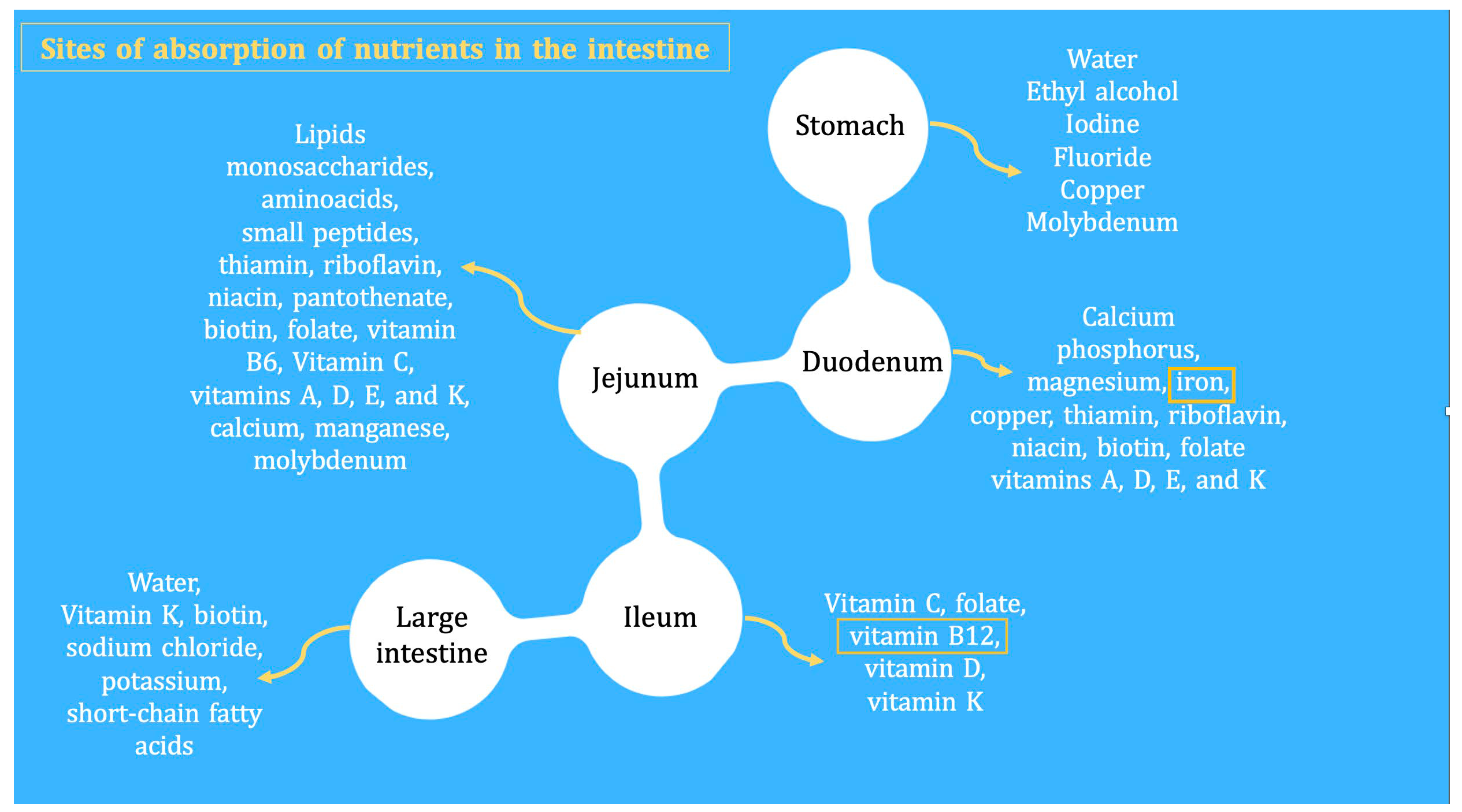
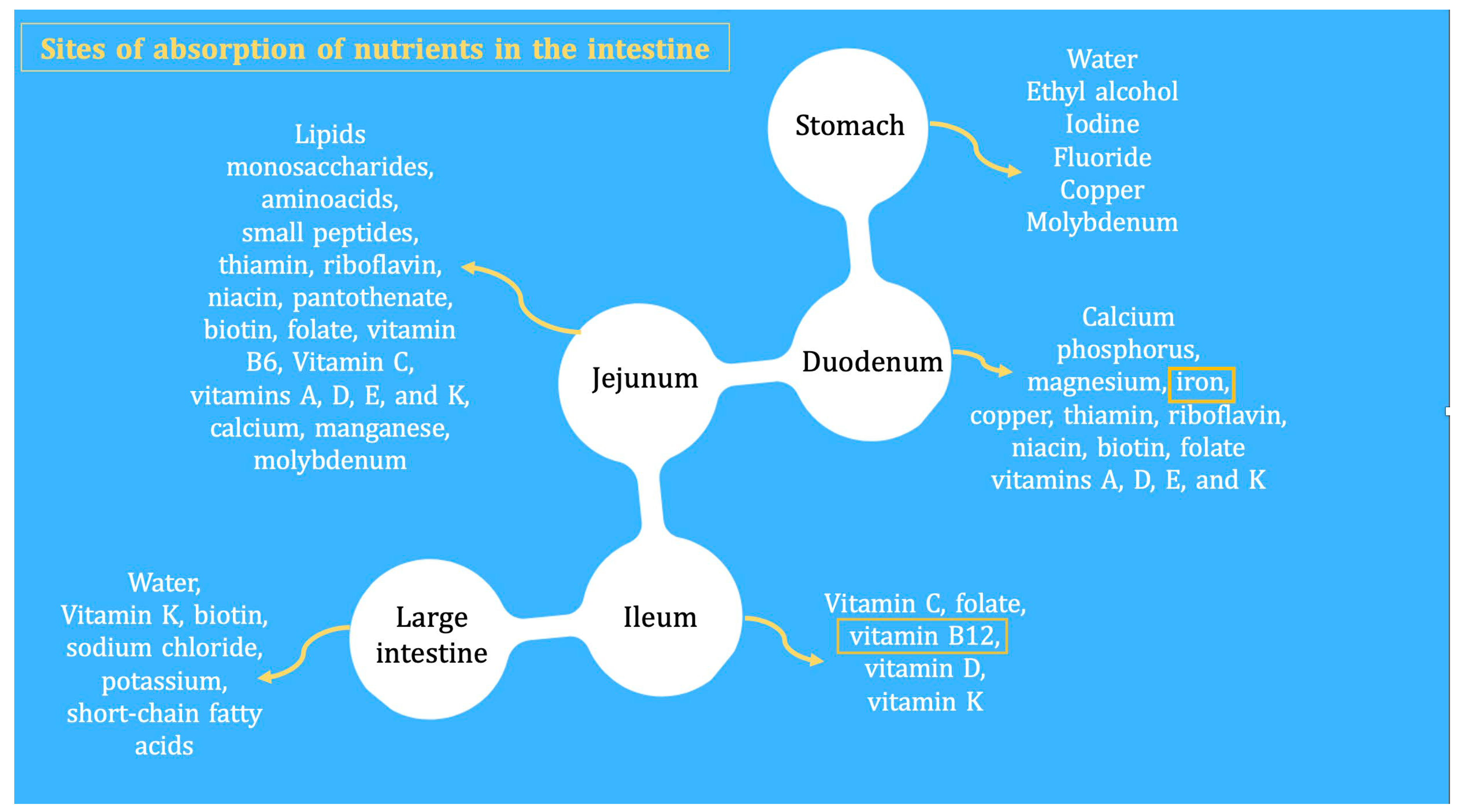
| (I) Complications related to SBS pathophysiology and its underlying pathology | The pattern of nutrient absorption native to the parts of the gastrointestinal tract is shown in Figure 1. |
| Peptic ulcer | Hypergastrinemia resulting from a failure of enterogastrone release (e.g., VIP, GIP, neurotensin, peptide YY, and GLP-1). Treatment with antisecretory drugs could also aggravate SIBO due to hipoclorhydria [73]. |
| Electrolyte disturbances: hypocalcemia, hypokalemia, and hypomagnesemia | Occur especially when large-volume diarrhea is present. (e.g., associated with an end jejunostomy). |
| D-lactic acidosis (D-LA) | The SBS microbiota, since it is rich in Lactobacillus, leads to the accumulation of fecal lactate. Lactate does not accumulate in healthy human feces because it is absorbed by intestinal cells, but in some SBS patients, the high amount of lactate found in feces indicates that production exceeds absorption capacities by the host. Excess lactate released into the colon is fermented by bacteria and converted into D-lactate, which has neuro-toxic effects [67,68,69]. |
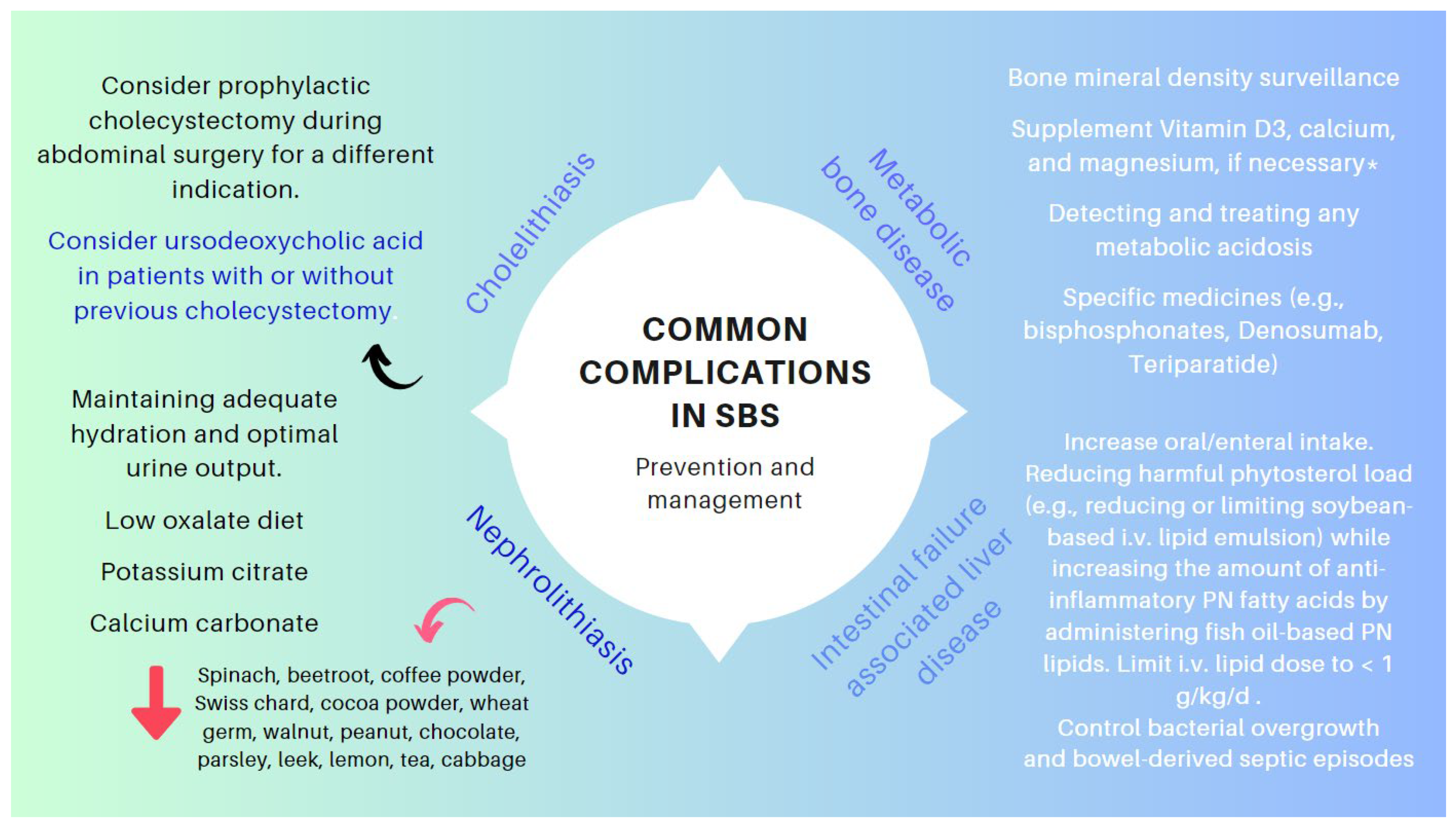
| Cholelithiasis | In the presence of an ileum resection, it breaks the enterohepatic circle of bile salts, causing a reduced biliary excretion and a marked decrease of the bile salt pool in the duodenal lumen. Consequently, cholesterol is oversaturated, favoring the formation of biliary stones [70,71]. |
| Nephrolithiasis | As a result of steatorrhea, increased free fatty acids are available to bind to calcium, resulting in an increased concentration of non-bound oxalate, which is easily absorbed across the colonic mucosa, where it is moving to the kidneys. Nephrolithiasis is more common among patients with an intact colon. The risk of nephrolithiasis is enhanced by volume depletion, metabolic acidosis, and hypomagnesemia, resulting in decreased renal perfusion, urine output, pH, and citrate excretion [72,73]. |
| Metabolic osteopathy | Metabolic changes that occur in SBS result in the depletion of calcium, magnesium, and vitamin D, which results in the demineralization of bone. The release of pro-inflammatory cytokines, steroid use, PN, chronic metabolic acidosis, and renal insufficiency may contribute to the development of metabolic osteopathy [74]. |
| (II) Complications related with nutritional therapy | Pathogenesis |
| Thrombus-associated venous occlusion | Central venous catheter (CVC)-related thrombosis (CRT) is a severe complication of parenteral nutrition (HPN), which increases its associated morbidity (due to pulmonary embolism) and mortality rates of this population [75,76]. |
| Catheter-associated central line bloodstream infections | Primary and intravascular catheter-associated bloodstream infections represent an important clinical entity in the intensive care unit (ICU) and has a poor effect on outcomes. Over-abundant levels of Proteobacteria have been found in the feces of patients with SBS presenting with Ca-CLBI [77,78,79,80]. |
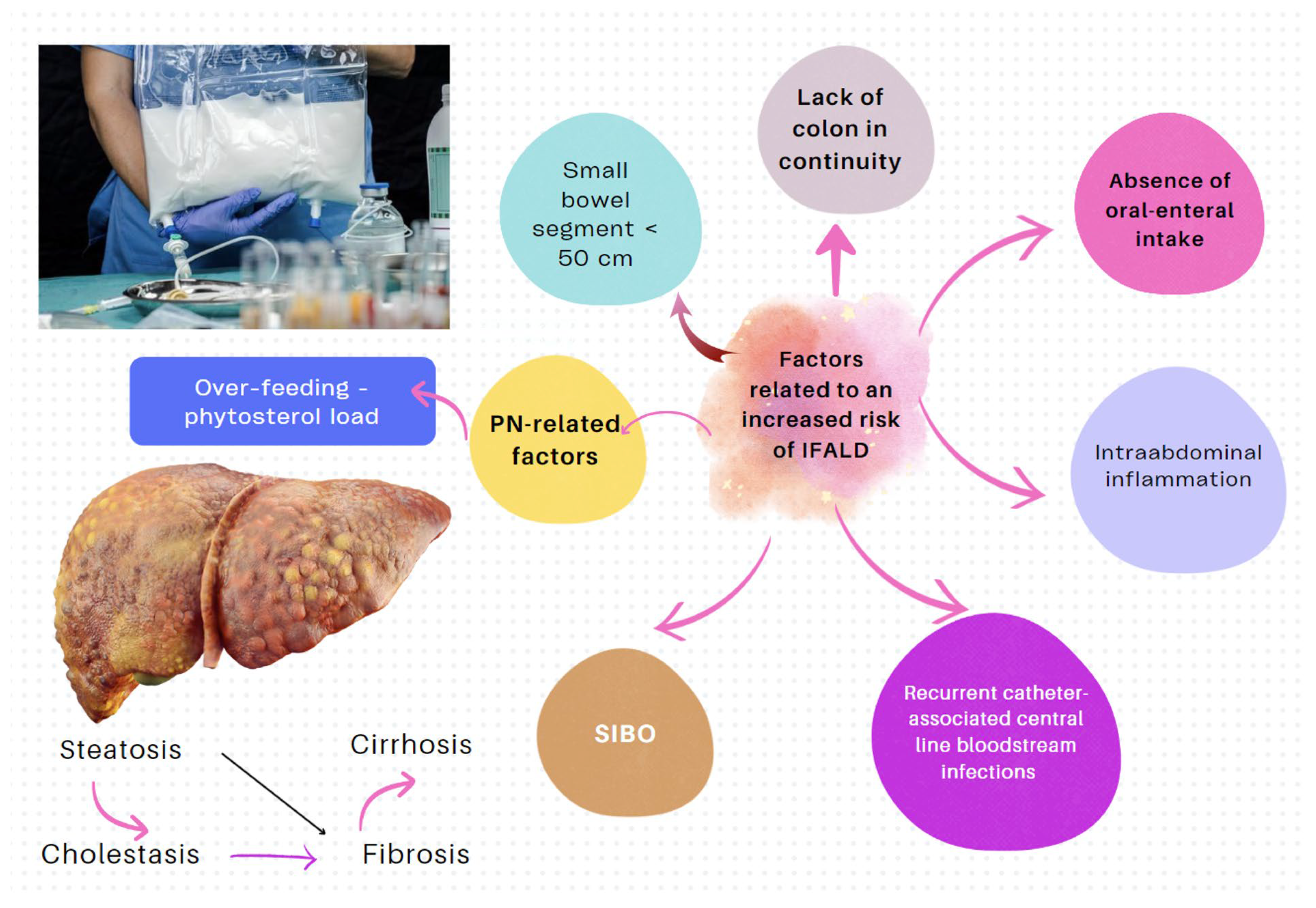
| IF-associated liver disease (IFALD) | IFALD is a possible complication in patients with IF who need intravenous support for survival due to severe intestinal dysfunction. An elevation of aminotransferases or cholestasis enzymes in this setting should raise clinical suspicion of this entity, which may progress from hepatic steatosis to cirrhosis. Some factors that increase the risk of this condition are shown in Figure 6. Liver cholestasis can be a life-threatening complication during HPN and may lead to a combined liver–intestinal transplantation (Figure 6) [17,79,81,82]. |
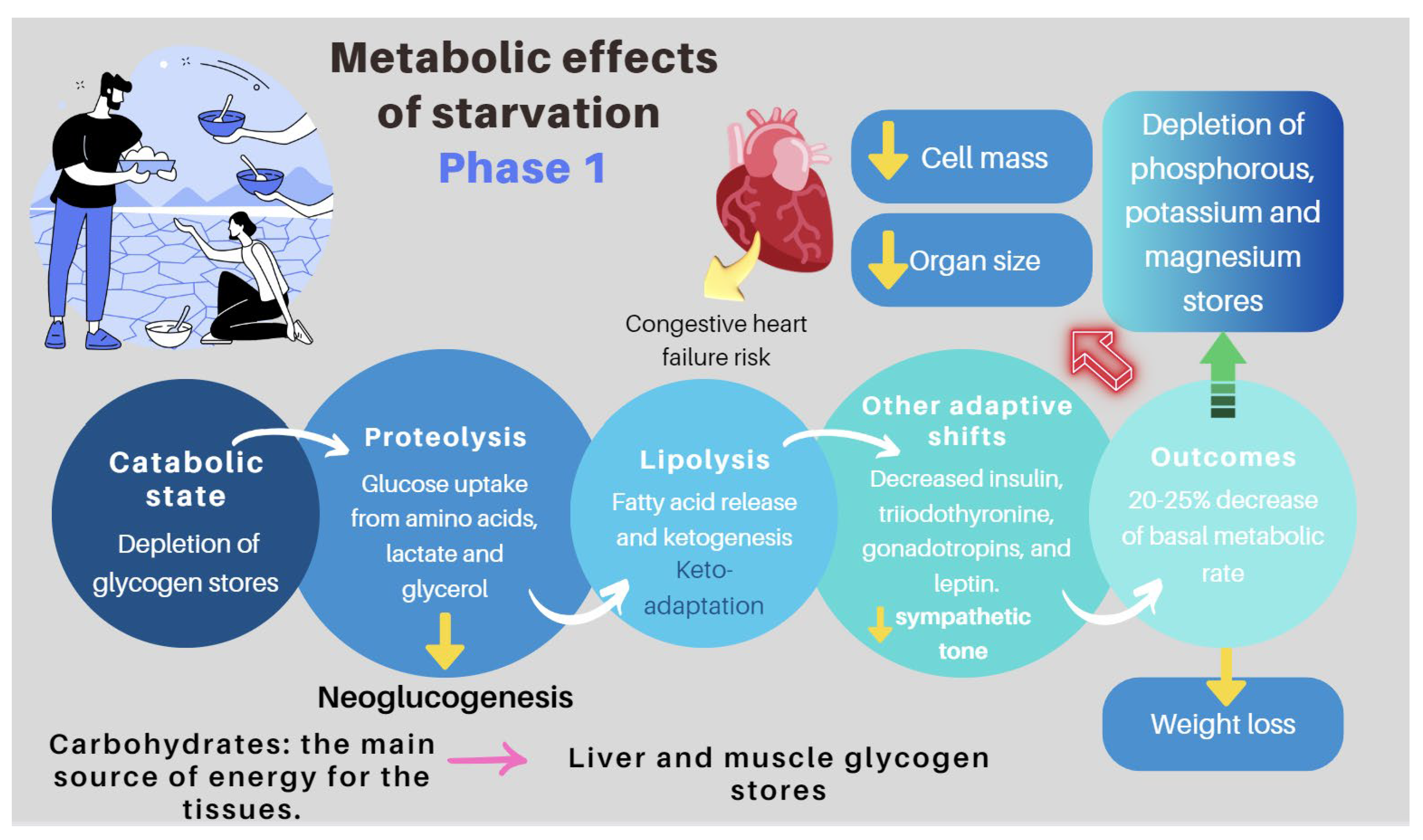
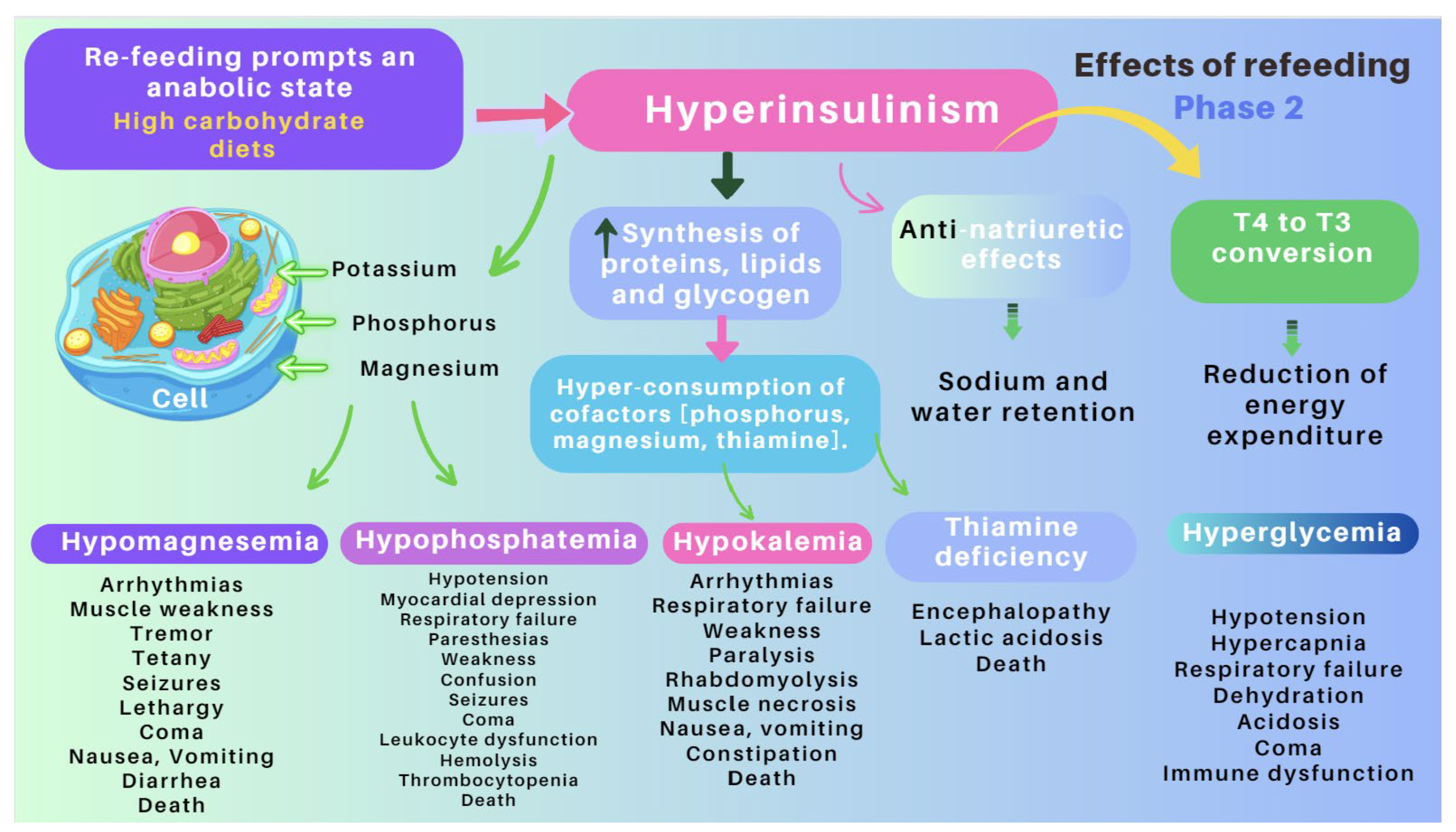
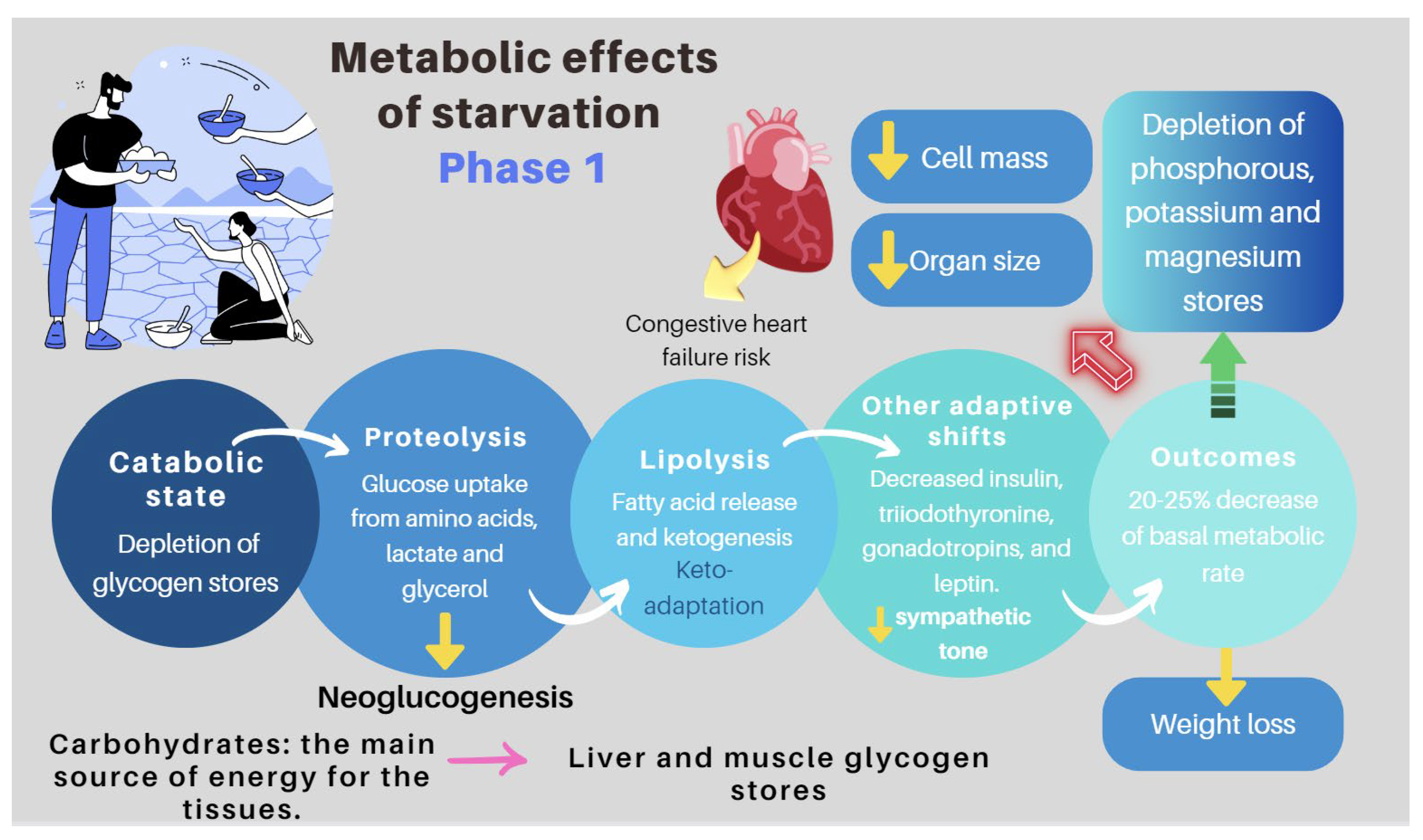
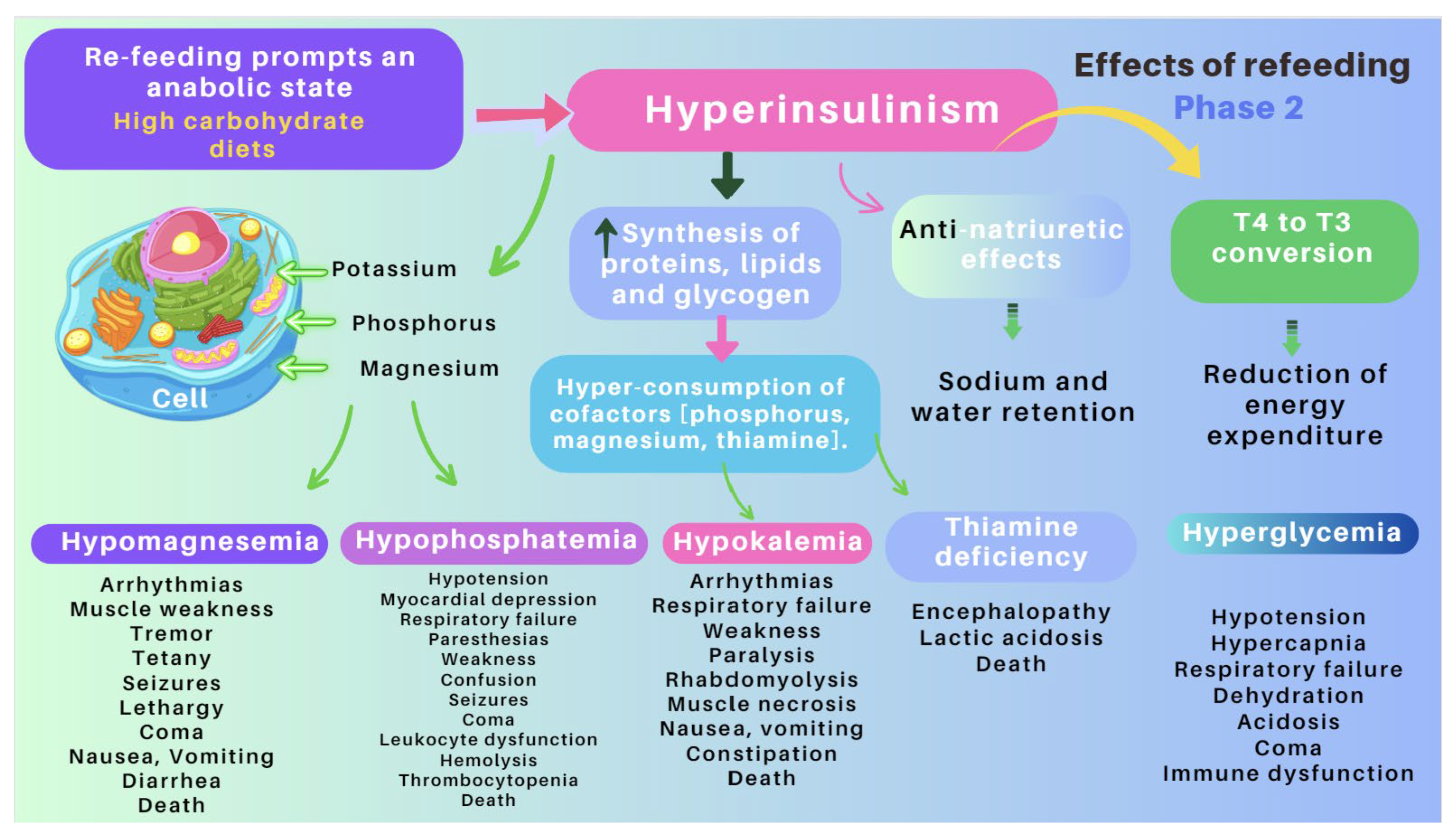
| Re-feeding syndrome (RFS) | The switch from a catabolic state to an anabolic state in malnourished patients undergoing refeeding (orally, enterally, or parenteral) may be the cause of all these clinical manifestations, which, in some cases, can lead to death. RS include a complex and extensive list of changes, such as hypophosphatemia, hypomagnesemia, hypokalemia, hyponatremia, hypocalcemia, hyperglycemia, and vitamin deficiency (especially thiamine deficiency), all of which are accompanied by clinical signs and symptoms, reflecting organ dysfunction (cardiovascular, renal, respiratory, and neurological manifestations, among others). Figure 7 and Figure 8 summarize the relationship between the pathophysiology of RS and its clinical presentation [83,84,85,86,87,88,89,90]. |

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
6.1.2. D-lactic Acidosis
6.1.3. Refeeding Syndrome (RS)
6.2. Basic Principles of Nutritional Management
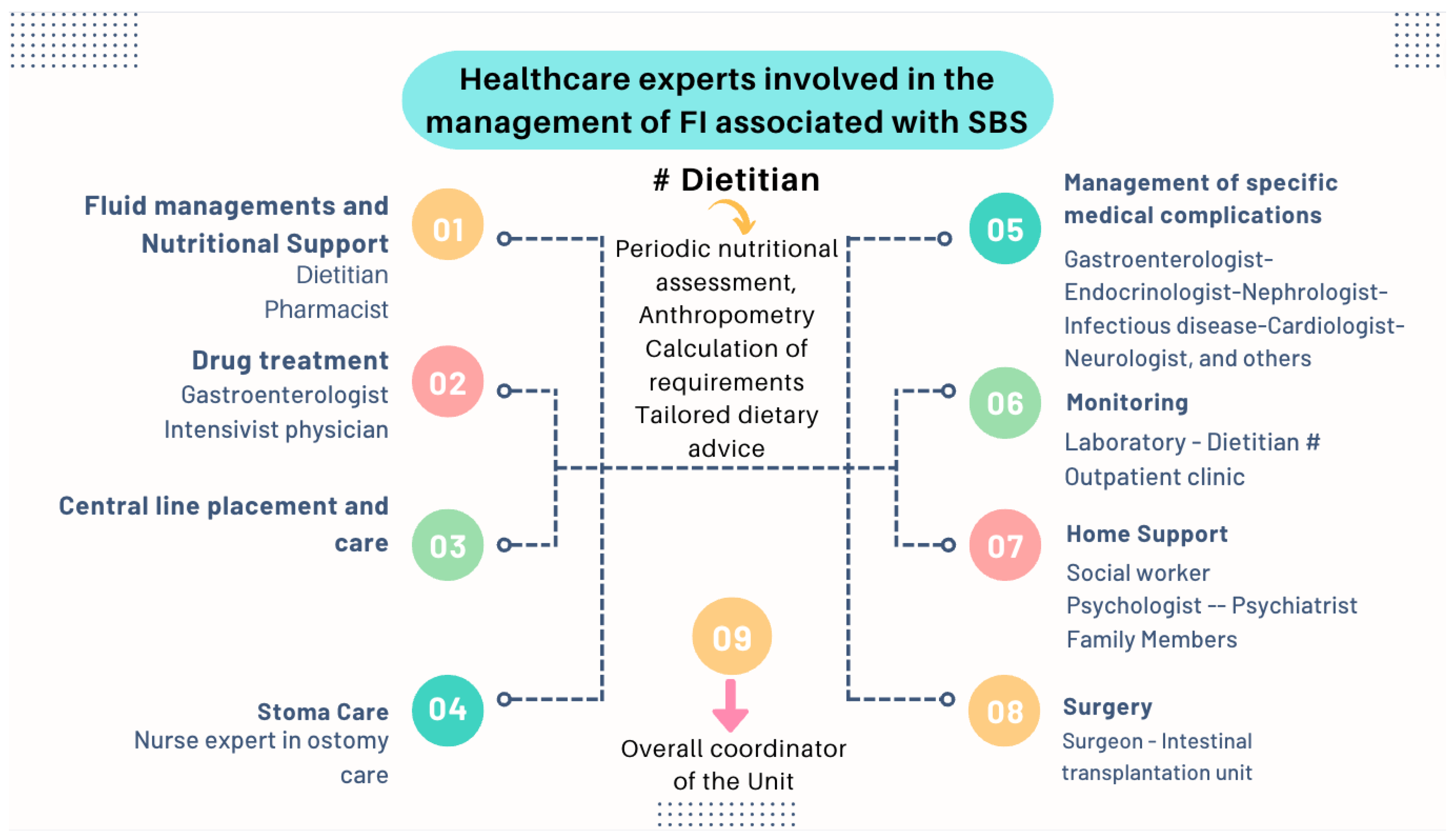
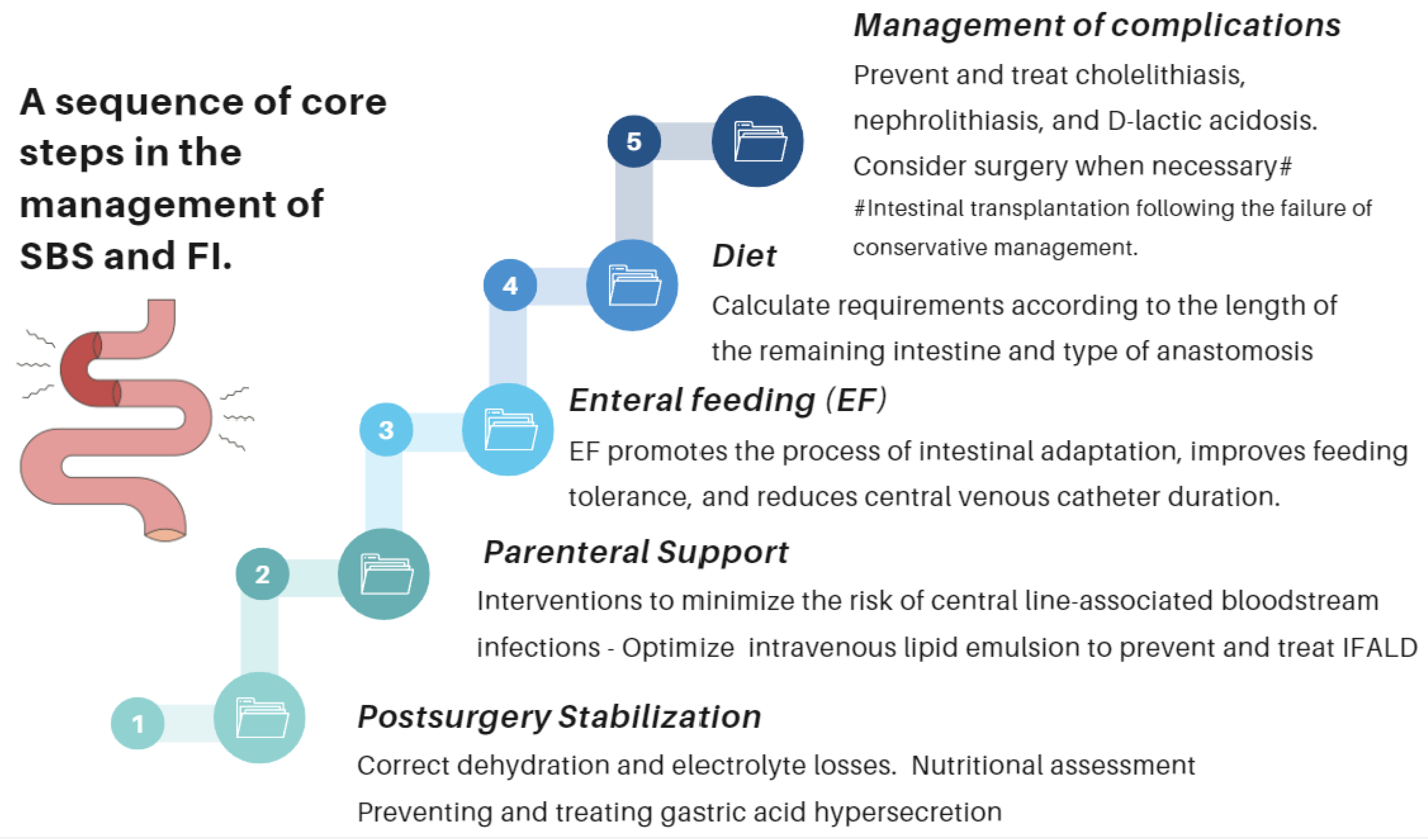
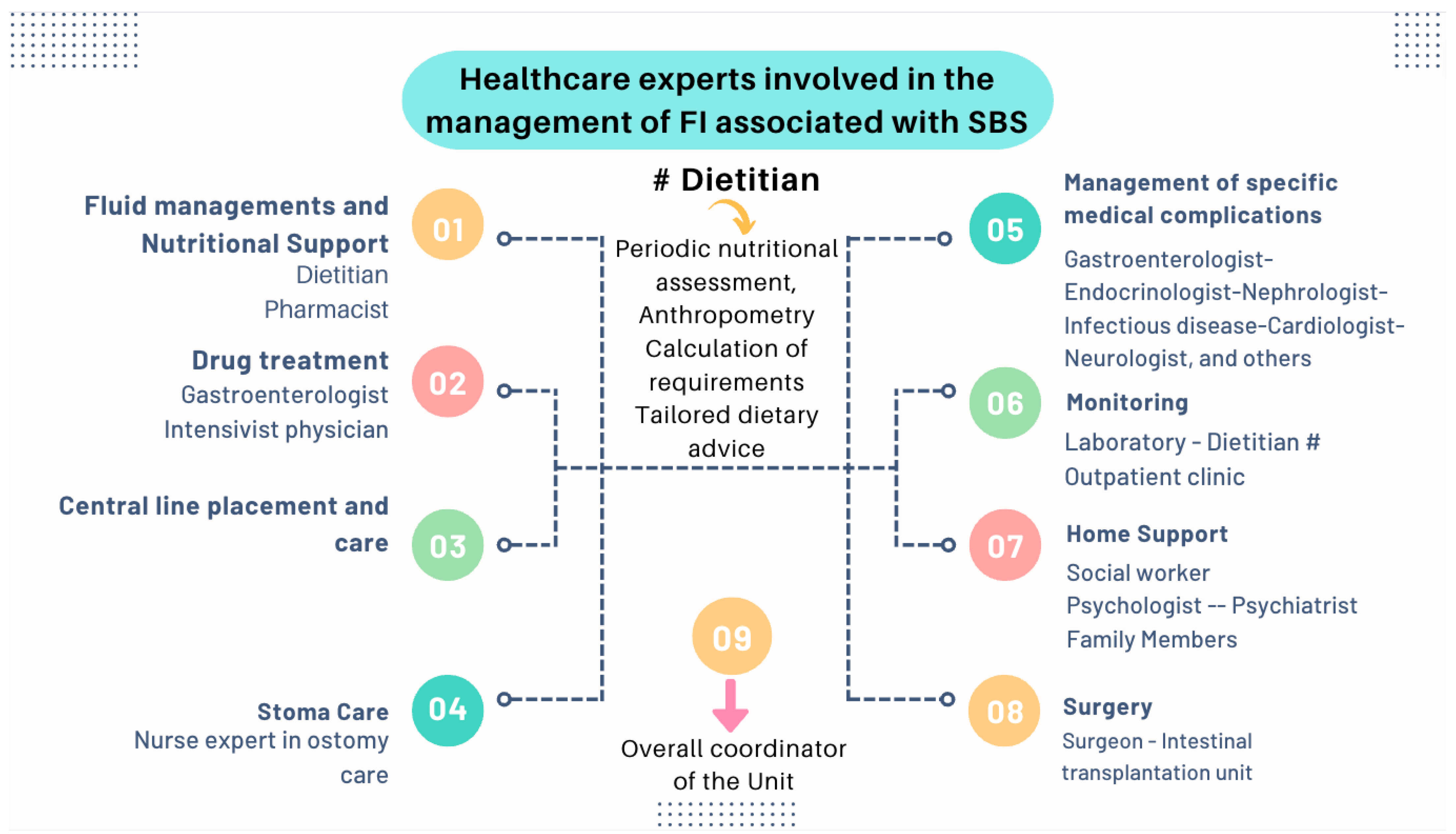
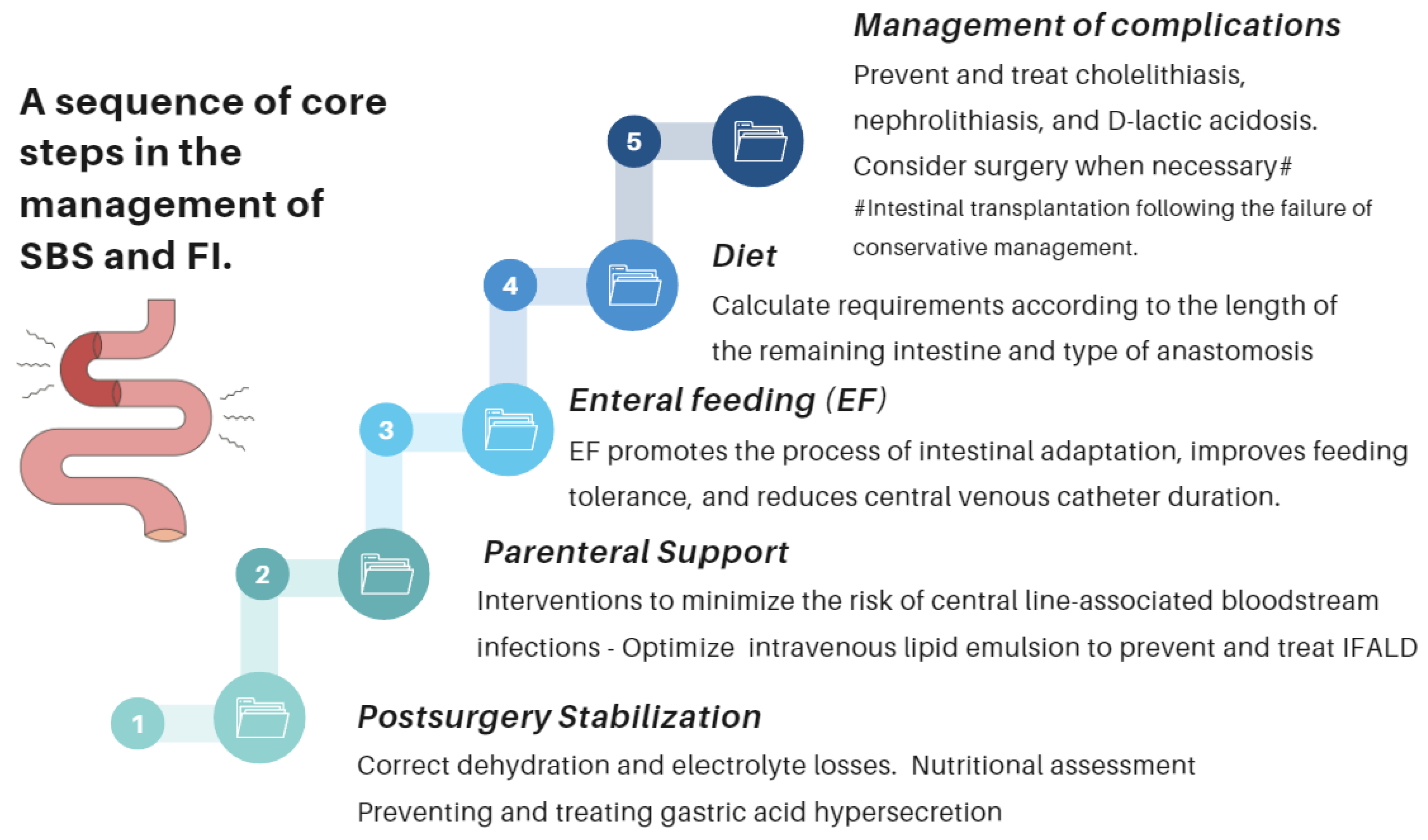
- Nutritional interventions to treat SBS include enteral and PN, intestinal rehabilitation techniques to increase the absorptive ability of the residual bowel, and surgical reconstruction designed to enhance the surface area for absorption [92,93,94]. Therefore, managing these patients requires a comprehensive and interdisciplinary approach in centers with proven experience in treating such challenging scenarios [93,94,95,96,97]. This issue is essential, as has been demonstrated by Geransar P et al., who reported a low level of awareness of chronic IF among non-specialist healthcare professionals [95]. Figure 9 highlights the components of a multidisciplinary team caring for these patients in a highly specialized center [93,96], and Figure 10 outlines the fundamental steps to be followed in the assessment and treatment of these patients [97].
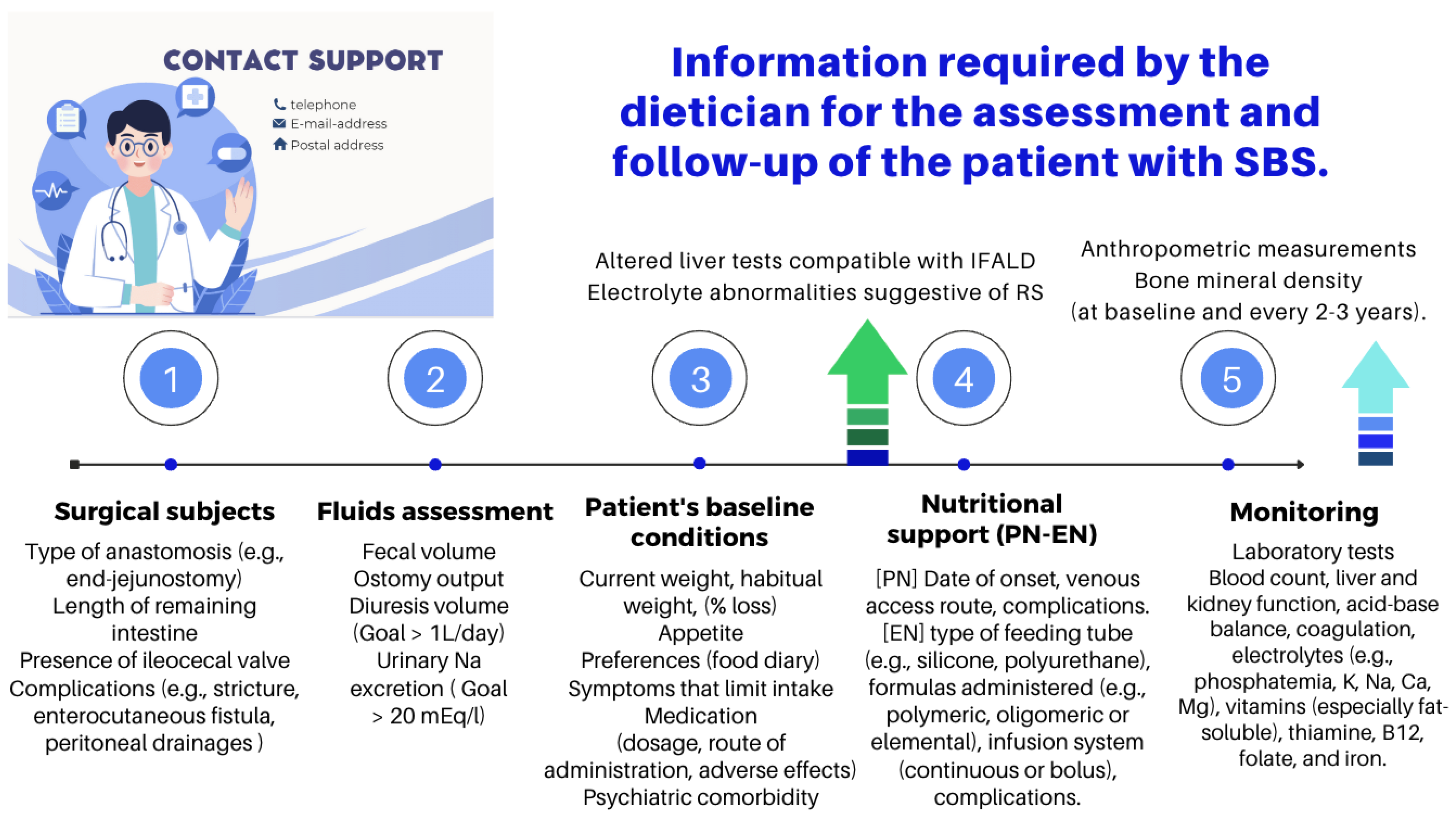
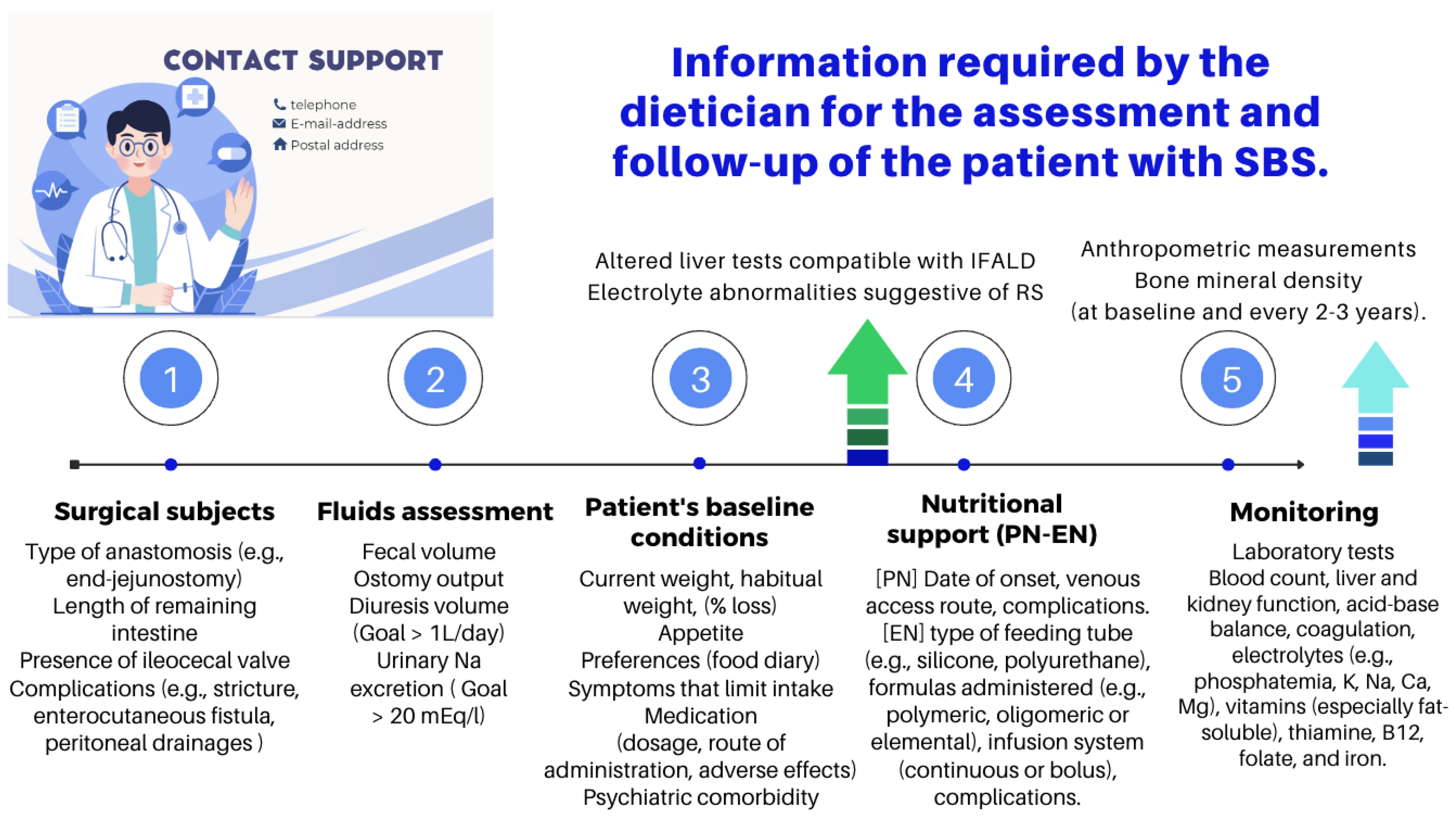
- The role of an experienced dietitian is also fundamental in the initial assessment and monitoring of the nutritional status of patients with SBS. Concerning this point, the dietitian should obtain information regarding multiple details related to the type of surgery performed, the patient’s baseline post-operative conditions (renal function, water–electrolyte, and acid–base balance), their degree of malnutrition, and the type of nutritional support received (enteral or parenteral), including access routes, as well as their associated complications (Figure 10 and Figure 11).
- Almost all patients with SBS need PN during the early period after a resection. PN should be initiated and adjusted to meet the patient’s fluid, electrolyte, energy, protein, and micronutrient needs. The literature provides excellent reviews of PN performance in this setting [98,99,100,101]. Although few patients with severe SBS can discontinue PN before hospital discharge, more than 50% of adults will be able to wean completely from PN within five years of their diagnosis. PN volume can be decreased when the patient begins to tolerate oral nutrition. This is possible if the volume or flow of feces from the rectum or through the ostomy is adequately reduced and the patient begins to gain weight. Enteral nutrition (EN) provides clear benefits, prevents villous atrophy, helps preserve the intestinal epithelial barrier, enhances the local immunity needed to avoid SIBO, and promotes the mechanisms of bowel adaptation, enhancing weaning from parenteral nutrition. The introduction of EN should always be prudent and judicious [100,101]. One approach is to start EN by providing 5% of the total calories and increasing this ratio every 3–7 days and assess tolerance. Patients who require long-term PN cannot be kept in hospital indefinitely, and thus transition to home PN when they are clinically stable. To maximize patient mobility and convenience at home, PN infusion time is minimized, and the solution is infused overnight. PN infusion time can typically be reduced (cycled) to 10–15 h, depending on patient tolerance [96,97]. Notably, the SBS patient receiving home PN is still at risk of micronutrient deficiencies, as well as liver and bone complications, and requires regular monitoring and supplementation with PN (Table 6).
- Many patients with less severe forms of SBS may be fed orally early. The dietary and nutritional management of these patients necessitate to understand the physiology and to consider the individual anatomy and adaptation phase. During the hypersecretory phase, fluid losses are usually the largest. Dehydration and saline depletion can occur during any phase, especially in patients without a colon, and particularly in case of an end jejunostomy [98].
6.3. Recommendations of Scientific Societies
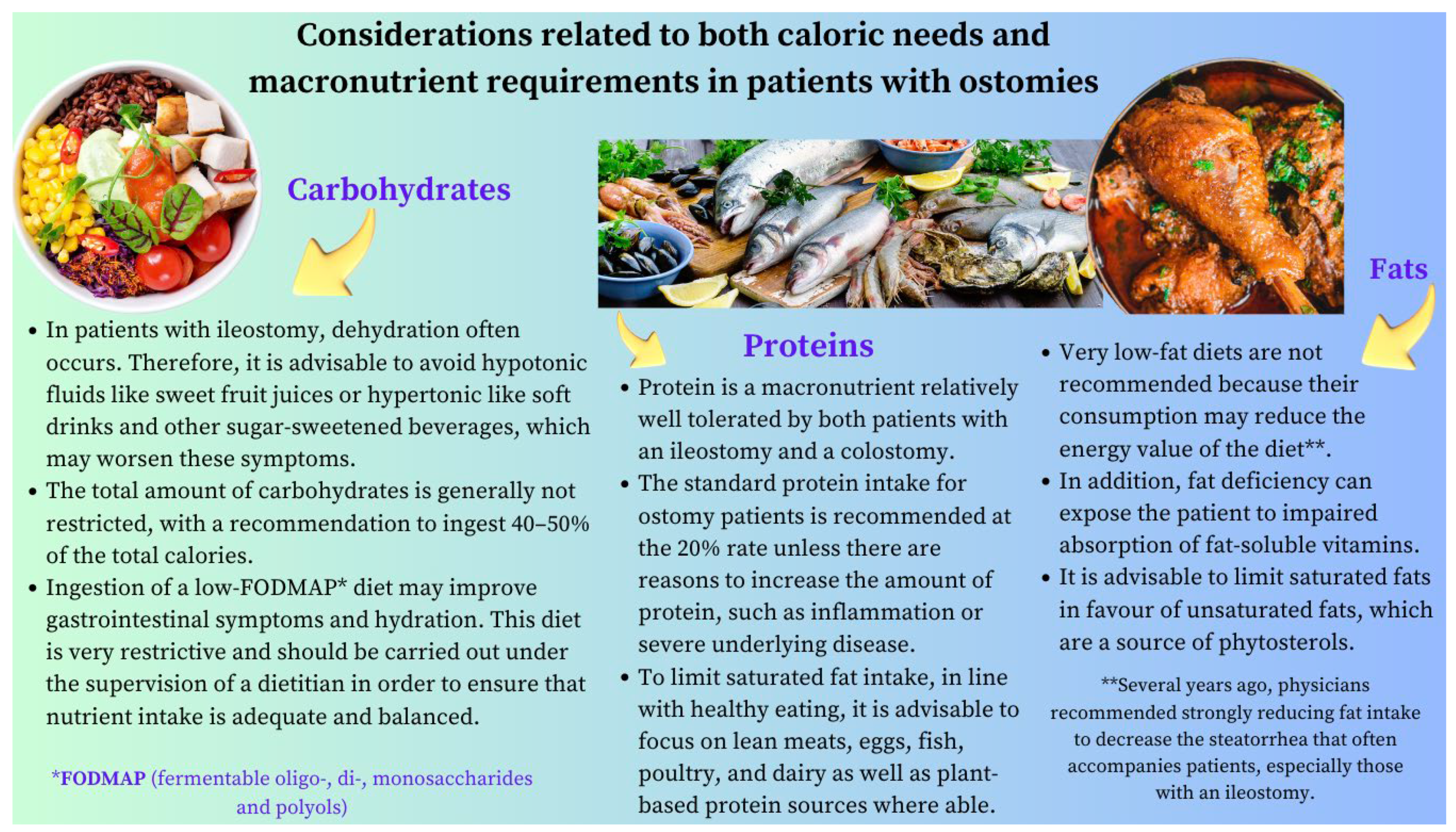
- Type 1: end jejunostomy. This is the most unfavorable phenotype, as malabsorption is more severe, and it presents with a high ostomy output. Patients without a colon and <100 cm of the jejunum have a higher risk of requiring long-term PN. Indeed, dehydration, hydroelectolytic abnormalities, acidosis, and renal failure are more likely in these patients [57]. Sodium absorption in the jejunum is dependent on water fluxes and is coupled to the absorption of glucose. For this reason, hydration with hypotonic solutions (e.g., water, tea, or coffee) should be discouraged, as they only exacerbate fluid losses through the stoma. Hypertonic drinks (e.g., fruit juices) should also not be recommended as they cause osmotic diarrhea. Some measures that may be useful for these patients are lowering the intake of sugars, decreasing the size of intakes, and take the oral rehydration solutions (ORSs) whose composition is best suited to promote the entry of sodium and water into the enterocytes [102,103]. Regarding calorie and macronutrient requirements, the recommendations are as follow (Table 6):
- Type 2: jejunocolic. It retains a portion of the jejunum anastomosed to a portion of the colon. In these patients, the clinical picture is dominated by diarrhea due to severe malabsorption, vitamin–mineral deficiencies, and subsequent malnutrition. Patients with jejunocolic anastomosis and <50 cm of the jejunum also have a higher risk of requiring long-term PN. The nutritional recommendations for those who recover intestinal autonomy are as follows (Table 7):
- Type 3: jejunoileocolic. These patients retain their entire colon and ileocecal valve along with a portion of their terminal ileum and jejunum. This is indeed the most advantageous phenotype, and these patients often do not require additional nutritional support because the ileum has a greater ability to adapt. This subgroup does not usually develop malnutrition, electrolyte disorders, or dehydration [57].
6.4. Common Recommendations for All Three Phenotypes
6.5. Vitamin and Mineral Replacement
6.6. Pharmacological Treatment
6.7. Management of Other Specific Conditions
6.8. Surgical Management
- (1)
- Preserving the existing intestine: It is common that after the initial resection, some patients need to be re-operated for various reasons (e.g., stenosis and perforations). In these scenarios, avoiding a resection and preserving the existing length of the intestinal remnant (e.g., serosal patching for certain strictures and chronic perforations) are essential. When carrying out a resection becomes unavoidable, an end-to-end anastomosis is preferred to prevent blind loops and, thus, optimize the functionality of the hindgut [58].
- (2)
- Restoration of intestinal continuity, elimination of a stoma with the aim of improving the patient’s quality of life and avoiding some of the complications associated with central venous catheters [57].
- (3)
- Tapering surgery when the remaining small bowel remains excessively dilated [153]. Intestinal tapering may be necessary in this context as a dilated intestine increases the risk of mucosal injury, bloodstream infections, and liver disease in patients with SBS [154]. Several techniques have been described to taper the dilated small bowel, including longitudinal intestinal lengthening and tapering, serial transverse enteroplasty, and spiral intestinal lengthening and tailoring [153,155].
- (4)
- Correction of stenoses, if possible, with stricturoplasties and with remodeling or intestinal plication if needed [156].
- (5)
- Serosal patching for chronic fistulae to prevent avoidable intestinal excisions [157].
- (6)
- Autologous gastrointestinal reconstruction operation: The aim of this procedure is to either enhance the mucosal surface area for absorption (e.g., lengthening procedures) or to slow intestinal transit to facilitate the assimilation of the nutrients or counterbalance stasis that cause gastrointestinal symptoms due to SIBO (e.g., reversing the segments of the intestine) [158,159], creating intestinal valves, or interposing a colonic segment in the mall intestinal remnant in either an isoperistaltic or antiperistaltic fashion [7,160,161,162]. These procedures should only be used in carefully selected patients and in centers with proven experience [163,164,165].
6.9. Intestinal Transplantation (ITx)
7. Anorectal Surgery
8. Conclusions and Highlights
8.1. Ileocecectomy
8.2. Low Anterior Resection and Abdominoperineal Resection
8.3. Proctocolectomy
8.4. Stoma Formation
8.4.1. Ileostomy
8.4.2. Colostomy
8.5. IBD Surgery
8.6. Short Bowel Syndrome
8.7. Anorectal Surgery
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
Abbreviations
References
- Lewis, S.J.; Egger, M.; Sylvester, P.A.; Thomas, S. Early enteral feeding versus “nil by mouth” after gastrointestinal surgery: Systematic review and meta-analysis of controlled trials. BMJ 2001, 323, 773–776. [Google Scholar] [CrossRef] [PubMed]
- Silk, D.B.; Gow, N.M. Postoperative starvation after gastrointestinal surgery. Early feeding is beneficial. BMJ 2001, 323, 761–762. [Google Scholar] [CrossRef] [PubMed]
- Canzan, F.; Caliaro, A.; Cavada, M.L.; Mezzalira, E.; Paiella, S.; Ambrosi, E. The effect of early oral postoperative feeding on the recovery of intestinal motility after gastrointestinal surgery: Protocol for a systematic review and meta-analysis. PLoS ONE 2022, 17, e0273085. [Google Scholar] [CrossRef] [PubMed]
- Shrestha, A.; Dani, M.; Kemp, P.; Fertleman, M. Acute Sarcopenia after Elective and Emergency Surgery. Aging Dis. 2022, 13, 1759–1769. [Google Scholar] [CrossRef] [PubMed]
- Tappenden, K.A. Anatomical and physiological considerations in short bowel syndrome: Emphasis on intestinal adaptation and the role of enterohormones. Nutr. Clin. Pract. 2023, 38 (Suppl. S1), S27–S34. [Google Scholar] [CrossRef] [PubMed]
- Hope, C.; Reill, J.; Lund, J.; Andreyev, H. Systematic review: The effect of right hemicolectomy for cancer on postoperative bowel function. Support. Care Cancer 2020, 28, 4549–4559. [Google Scholar] [CrossRef] [PubMed]
- Lauro, A.; Cirocchi, R.; Cautero, N.; Dazzi, A.; Pironi, D.; Di Matteo, F.M.; Santoro, A.; Pironi, L.; Pinna, A.D. Reconnection surgery in adult post-operative short bowel syndrome <100 cm: Is colonic continuity sufficient to achieve enteral autonomy without autologous gastrointestinal reconstruction? Report from a single center and systematic review of literature. G. Chir. 2017, 38, 163–175. [Google Scholar] [CrossRef]
- Hofmann, A.F. The syndrome of ileal disease and the broken enterohepatic circulation: Cholerheic enteropathy. Gastroenterology 1967, 52, 752–757. [Google Scholar] [CrossRef]
- Williams, A.J.K.; Merrick, M.V.; Eastwood, M.A. Idiopathic bile acid malabsorption a review of clinical presentation, diagnosis, and response to treatment. Gut 1991, 32, 1004–1006. [Google Scholar] [CrossRef]
- Hoffmann, A.F.; Poley, J.R. Cholestyramine treatment of diarrhea associated with ileal resection. N. Engl. J. Med. 1969, 281, 397–402. [Google Scholar] [CrossRef]
- Wu, E.H.; Guo, Z.; Zhu, W.M. Postoperative diarrhea in Crohn’s disease: Pathogenesis, diagnosis, and therapy. World J. Clin. Cases 2023, 11, 7–16. [Google Scholar] [CrossRef] [PubMed]
- Roediger, W.E. The starved colon--diminished mucosal nutrition, diminished absorption, and colitis. Dis. Colon Rectum 1990, 33, 858–862. [Google Scholar] [CrossRef] [PubMed]
- Glotzer, D.J.; Glick, M.E.; Goldman, H. Proctitis and colitis following diversion of the fecal stream. Gastroenterology 1981, 80, 438–441. [Google Scholar] [CrossRef] [PubMed]
- Lu, E.S.; Lin, T.; Harms, B.L.; Gaumnitz, E.A.; Singaram, C. A severe case of diversion colitis with large ulcerations. Am. J. Gastroenterol. 1995, 90, 1508–1510. [Google Scholar] [PubMed]
- Mohamed Elfadil, O.; Mundi, M.S.; Abdelmagid, M.G.; Patel, A.; Patel, N.; Martindale, R. Butyrate: More than a Short Chain Fatty Acid. Curr. Nutr. Rep. 2023, 12, 255–262. [Google Scholar] [CrossRef] [PubMed]
- Harig, J.M.; Soergel, K.H.; Komorowski, R.A.; Wood, C.M. Treatment of diversion colitis with short-chain-fatty acid irrigation. N. Engl. J. Med. 1989, 320, 23–28. [Google Scholar] [CrossRef] [PubMed]
- Rosen, H.; Sebesta, C.G.; Sebesta, C. Management of Low Anterior Resection Syndrome (LARS) following Resection for Rectal Cancer. Cancers 2023, 15, 778. [Google Scholar] [CrossRef]
- Keane, C.; Wells, C.; O’Grady, G.; Bissett, I.P. Defining low anterior resection syndrome: A systematic review of the literature. Color. Dis. 2017, 19, 713–722. [Google Scholar] [CrossRef]
- Chen, T.Y.; Emmertsen, K.J.; Laurberg, S. Bowel dysfunction after rectal cancer treatment: A study comparing the specialists versus patient’s perspective. BMJ Open 2014, 4, e003374. [Google Scholar] [CrossRef]
- Bazzell, A.; Madsen, L.T.; Dains, J. Clinical management of bowel dysfunction after low anterior resection for rectal cancer. J. Adv. Pract. Oncol. 2016, 7, 618–629. [Google Scholar]
- Colavita, K.; Andy, U.U. Role of diet in fecal incontinence: A systematic review of the literature. Int. Urogynecol. J. 2016, 27, 1805–1810. [Google Scholar] [CrossRef]
- Harji, D.; Fernandez, B.; Boissieras, L.; Berger, A.; Capdepont, M.; Zerbib, F.; Rullier, E.; Denost, Q. A novel bowel rehabilitation programme after total mesorectal excision for rectal cancer: The BOREAL pilot study. Color. Dis. 2021, 23, 2619–2626. [Google Scholar] [CrossRef] [PubMed]
- Staller, K.; Song, M.; Grodstein, F.; Whitehead, W.E.; Matthews, C.A.; Kuo, B.; Chan, A.T. Increased long-term dietary fiber intake is associated with a decreased risk of fecal incontinence in older women. Gastroenterology 2018, 155, 661–667. [Google Scholar] [CrossRef] [PubMed]
- Thiesen, A.; Drozdowski, L.; Iordache, C.; Neo, C.; Woudstra, T.D.; Xenodemetropoulos, T.; Keelan, M.; Clandinin, M.T.; Thomson, A.B.R.; Wild, G. Adaptation following intestinal resection: Mechanisms and signals. Best Pract. Res. Clin. Gastroenterol. 2003, 17, 981. [Google Scholar] [CrossRef] [PubMed]
- Dowling, R.H.; Booth, C.C. Structural and functional changes following small intestinal resection in the rat. Clin. Sci. 1967, 32, 139. [Google Scholar]
- Cisler, J.J.; Buchman, A.L. Intestinal adaptation in short bowel syndrome. J. Investig. Med. 2005, 53, 402–413. [Google Scholar] [CrossRef]
- Michońska, I.; Polak-Szczybyło, E.; Sokal, A.; Jarmakiewicz-Czaja, S.; Stępień, A.E.; Dereń, K. Nutritional Issues Faced by Patients with Intestinal Stoma: A Narrative Review. J. Clin. Med. 2023, 12, 510. [Google Scholar] [CrossRef]
- McCann, E. Routine assessment of the patient with an ostomy. In Wound, Ostomy, and Continence Nursing Secrets; Milne, C., Corbett, I., Dubuc, D., Eds.; Hanley and Belfus: Philadelphia, PA, USA, 2003. [Google Scholar]
- Messaris, E.; Sehgal, R.; Deiling, S.; Koltun, W.A.; David Stewart, D.; McKenna, K.; Poritz, L.S. Dehydration is the most common indication for readmission after diverting ileostomy creation. Dis. Colon Rectum 2012, 55, 175–180. [Google Scholar] [CrossRef]
- Paquette, I.M.; Solan, P.; Rafferty, J.F.; Ferguson, M.A.; Davis, B.R. Readmission for dehydration or renal failure after ileostomy creation. Dis. Colon Rectum 2013, 56, 974–979. [Google Scholar] [CrossRef]
- Borucki, J.P.; Schlaeger, S.; Crane, J.; Hernon, J.M.; Stearns, A.T. Risk and consequences of dehydration following colorectal cancer resection with diverting ileostomy. A systematic review and meta-analysis. Color. Dis. 2021, 23, 1721–1732. [Google Scholar] [CrossRef]
- Hayden, D.M.; Pinzon, M.C.; Francescatti, A.B.; Edquist, S.C.; Malczewski, M.R.; Jolley, J.M.; Brand, M.I.; Saclarides, T.J. Hospital readmission for fluid and electrolyte abnormalities following ileostomy construction: Preventable or unpredictable? J. Gastrointest. Surg. 2013, 17, 298–303. [Google Scholar] [CrossRef] [PubMed]
- McRorie, J.W., Jr. Evidence-Based Approach to Fiber Supplements and Clinically Meaningful Health Benefits, Part 2: What to Look for and How to Recommend an Effective Fiber Therapy. Nutr. Today 2015, 50, 90–97. [Google Scholar] [CrossRef] [PubMed]
- McRorie, J.W., Jr. Evidence-Based Approach to Fiber Supplements and Clinically Meaningful Health Benefits, Part 1: What to Look for and How to Recommend an Effective Fiber Therapy. Nutr. Today 2015, 50, 82–89. [Google Scholar] [CrossRef] [PubMed]
- McRorie, J.W., Jr.; McKeown, N.M. Understanding the Physics of Functional Fibers in the Gastrointestinal Tract: An Evidence-Based Approach to Resolving Enduring Misconceptions about Insoluble and Soluble Fiber. J. Acad. Nutr. Diet. 2017, 117, 251–264. [Google Scholar] [CrossRef]
- Crocetti, D.; Velluti, F.; La Torre, V.; Orsi, E.; De Anna, L.; La Torre, F. Psyllium fiber food supplement in the management of stoma patients: Results of a comparative prospective study. Tech. Coloproctol. 2014, 1, 595–596. [Google Scholar] [CrossRef]
- Garg, P. Psyllium Husk Should Be Taken at Higher Dose with Sufficient Water to Maximize Its Efficacy? J. Acad. Nutr. Diet. 2017, 117, 681. [Google Scholar] [CrossRef] [PubMed]
- Strong, C.; Hall, J.; Wilson, G.; Carney, K. Common intestinal stoma complaints. BMJ 2021, 374, n2310. [Google Scholar] [CrossRef]
- Bafford, A.C.; Irani, J.L. Management and complications of stomas. Surg. Clin. N. Am. 2013, 93, 145–166. [Google Scholar] [CrossRef]
- Erwin-Toth, P.; Doughty, D. Principles, and procedures of stomal management. In Ostomies and Continent Diversions: Nursing Management; Hampton, B., Bryant, R., Eds.; Mosby: St. Louis, MO, USA, 1992; p. 29. [Google Scholar]
- Floruta, C.V. Dietary choices of people with ostomies. J. Wound Ostomy Cont. Nurs. 2001, 28, 28–31. [Google Scholar] [CrossRef]
- Aronovitch, S.A.; Sharp, R.; Harduar-Morano, L. Quality of life for patients living with ostomies: Influence of contact with an ostomy nurse. J. Wound Ostomy Cont. Nurs. 2010, 37, 649–653. [Google Scholar] [CrossRef]
- Lomer, M.C.E.; Wilson, B.; Wall, C.L. British Dietetic Association consensus guidelines on the nutritional assessment and dietary management of patients with inflammatory bowel disease. J. Hum. Nutr. Diet. 2023, 36, 336–377. [Google Scholar] [CrossRef] [PubMed]
- Aluzaite, K.; Nuttall, J.W.; O’Connor, M.; Harvie, R.; Schultz, M. Quality of life in post ostomy surgery patients: A cross-sectional survey. JGH Open 2020, 4, 987–994. [Google Scholar] [CrossRef]
- Schiergens, T.S.; Hoffmann, V.; Schobel, T.N.; Englert, G.H.; Kreis, M.E.; Thasler, W.E.; Werner, J.; Kasparek, M.S. Long-term Quality of Life of Patients with Permanent End Ileostomy: Results of a Nationwide Cross-Sectional Survey. Dis. Colon Rectum 2017, 60, 51–60. [Google Scholar] [CrossRef] [PubMed]
- Fulham, J. Providing dietary advice for the individual with a stoma. Br. J. Nurs. 2008, 17, S22–S27. [Google Scholar] [CrossRef]
- Medlin, S. Nutritional, and fluid requirements: High-output stomas. Br. J. Nurs. 2012, 21, S22–S25. [Google Scholar] [CrossRef] [PubMed]
- Burch, J. Nutrition for people with stomas. 2: An overview of dietary advice. Nurs. Times 2008, 104, 26–27. [Google Scholar] [PubMed]
- Burch, J. Providing information and advice on diet to stoma patients. Br. J. Community Nurs. 2011, 16, 479–484. [Google Scholar] [CrossRef]
- Bischoff, S.C.; Bager, P.; Escher, J.; Forbes, A.; Hébuterne, X.; Hvas, C.L.; Joly, F.; Klek, S.; Krznaric, Z.; Ockenga, J. ESPEN guideline on Clinical Nutrition in inflammatory bowel disease. Clin. Nutr. 2023, 42, 352–379. [Google Scholar] [CrossRef]
- Dua, A.; Corson, M.; Sauk, J.S.; Jaffe, N.; Limketkai, B.N. Impact of malnutrition and nutrition support in hospitalized patients with inflammatory bowel disease. Aliment. Pharmacol. Ther. 2023, 57, 897–906. [Google Scholar] [CrossRef]
- O’Keefe, S.J.; Buchman, A.L.; Fishbein, T.M.; Jeejeebhoy, K.N.; Jeppesen, P.B.; Shaffer, J. Short bowel syndrome and intestinal failure: Consensus definitions and overview. Clin. Gastroenterol. Hepatol. 2006, 4, 6–10. [Google Scholar] [CrossRef]
- DiBaise, J.K.; Young, R.J.; Vanderhoof, J.A. Intestinal rehabilitation and the short bowel syndrome: Part 1. Am. J. Gastroenterol. 2004, 99, 186–195. [Google Scholar] [CrossRef]
- Thompson, J.S. Comparison of massive vs. repeated resection leading to the short bowel syndrome. J. Gastrointest. Surg. 2000, 4, 101–104. [Google Scholar] [CrossRef] [PubMed]
- Iyer, K.; DiBaise, J.K.; Rubio-Tapia, A. AGA clinical practice update on management of short bowel syndrome: Expert review. Clin. Gastroenterol. Hepatol. 2022, 20, 2185–2194. [Google Scholar] [CrossRef] [PubMed]
- Lakkasani, S.; Seth, D.; Khokhar, I.; Touza, M.; Dacosta, T.J. Concise review on short bowel syndrome: Etiology, pathophysiology, and management. World J. Clin. Cases 2022, 10, 11273–11282. [Google Scholar] [CrossRef] [PubMed]
- Bering, J.; DiBaise, J.K. Short bowel syndrome in adults. Am. J. Gastroenterol. 2022, 117, 876–883. [Google Scholar] [CrossRef]
- Seetharam, P.; Rodrigues, G. Short Bowel Syndrome. Saudi J. Gastroenterol. 2011, 17, 229–235. [Google Scholar] [CrossRef]
- Kumar, A.; Al-Hassi, H.O.; Jain, M.; Phipps, O.; Ford, C.; Gama, R.; Steed, H.; Butterworth, J.; McLaughlin, J.; Galbraith, N.; et al. A single faecal bile acid stool test demonstrates potential efficacy in replacing SeHCAT testing for bile acid diarrhoea in selected patients. Sci. Rep. 2022, 12, 8313. [Google Scholar] [CrossRef] [PubMed]
- Arasaradnam, R.P.; Steven Brown, S.; Forbes, A.; Fox, M.R.; Hungin, P.; Kelman, L.; Major, G.; O’Connor, M.; Dave SSanders, D.S.; Sinha, R.; et al. Guidelines for the investigation of chronic diarrhoea in adults: British Society of Gastroenterology, 3rd edition. Gut 2018, 67, 1380–1399. [Google Scholar] [CrossRef]
- Calzadilla, N.; Comiskey, S.M.; Dudeja, P.K.; Saksena, S.; Gill, R.K.; Alrefai, W.A. Bile acids as inflammatory mediators and modulators of intestinal permeability. Front. Immunol. 2022, 13, 1021924. [Google Scholar] [CrossRef]
- Kumar, A.; Galbraith, N.; Al-Hassi, H.O.; Jain, M.; Phipps, O.; Butterworth, J.; Steed, H.; McLaughlin, J.; Brookes, M.J. The impact of treatment with bile acid sequestrants on quality of life in patients with bile acid diarrhoea. BMC Gastroenterol. 2022, 22, 325. [Google Scholar] [CrossRef]
- Germani, P.; Zucca, A.; Giudici, F.; Terranova, S.; Troian, M.; Samardzic, N.; Greco, M.; Janez, J.; Gasparini, C.; Cagnazzo, E.; et al. Ileocecal valve syndrome and vitamin B12 deficiency after surgery: A multicentric prospective study. Updates Surg. 2021, 73, 569–580. [Google Scholar] [CrossRef]
- Fordtran, J.S.; Rector, F.C., Jr.; Ewton, M.F.; Soter, N.; Kinney, J. Permeability characteristics of the human small intestine. J. Clin. Investig. 1965, 44, 1935–1944. [Google Scholar] [CrossRef] [PubMed]
- Ziegler, T.R.; Cole, C.R. Small bowel bacterial overgrowth in adults: A potential contributor to intestinal failure. Curr. Gastroenterol. Rep. 2007, 9, 463–467. [Google Scholar] [CrossRef] [PubMed]
- Sorathia, S.J.; Chippa, V.; Rivas, J.M. Small Intestinal Bacterial Overgrowth. In StatPearls [Internet]; StatPearls Publishing: Treasure Island, FL, USA, 2023. [Google Scholar]
- Jain, A.; Jhinger, K.; Bellas, J. Recurrent Encephalopathy and Severe Anion Gap Metabolic Acidosis in a Patient with Short Bowel: It Is D-Lactic Acidosis. Case Rep. Gastroenterol. 2021, 15, 92–96. [Google Scholar] [CrossRef]
- Uribarri, J.; Oh, M.S.; Carroll, H.J. D-lactic acidosis. A review of clinical presentation, biochemical features, and pathophysiologic mechanisms. Medicine 1998, 77, 73–82. [Google Scholar] [CrossRef]
- Bianchetti, D.G.A.M.; Amelio, G.S.; Lava, S.A.G.; Bianchetti, M.G.; Simonetti, G.D.; Agostoni, C.; Fossali, E.F.; Milani, G.P. D-lactic acidosis in humans: Systematic literature review. Pediatr. Nephrol. 2018, 33, 673–681. [Google Scholar] [CrossRef] [PubMed]
- Gao, X.; Zhang, L.; Wang, S.; Xiao, Y.; Song, D.; Zhou, D.; Wang, X. Prevalence, Risk Factors, and Complications of Cholelithiasis in Adults with Short Bowel Syndrome: A Longitudinal Cohort Study. Front. Nutr. 2021, 8, 762240. [Google Scholar] [CrossRef]
- Thompson, J.S.; Rochling, F.A.; Lyden, E.; Merani, S.; Vargas, L.M.; Grant, W.J.; Langnas, A.N.; Mercer, D.F. Cholecystectomy prior to short bowel syndrome does not alter nutritional prognosis. Am. J. Surg. 2022, 224, 1285–1288. [Google Scholar] [CrossRef]
- Yang, J.; Sun, H.; Wan Mamtawla, G.; Gao, X.; Zhang, L.; Li, Y.; Wang, X.; Li, J. Risk Factors for Nephrolithiasis in Adults with Short Bowel Syndrome. Ann. Nutr. Metab. 2019, 75, 47–54. [Google Scholar] [CrossRef]
- Salazar, J.A.; Carey, A.N.; Duggan, C.P. Nutritional, and medical approaches to intestinal failure. Curr. Opin. Clin. Nutr. Metab. Care 2023, 26, 201–209. [Google Scholar] [CrossRef]
- Johnson, E.; Vu, L.; Matarese, L.E. Bacteria, Bones, and Stones: Managing Complications of Short Bowel Syndrome. Nutr. Clin. Pract. 2018, 33, 454–466. [Google Scholar] [CrossRef]
- Malec, L.M.; Cooper, J.; Rudolph, J.; Michaels, M.G.; Ragni, M.V. Prophylactic rtPA in the Prevention of Line-associated Thrombosis and Infection in Short Bowel Syndrome. J. Pediatr. Gastroenterol. Nutr. 2018, 66, 972–975. [Google Scholar] [CrossRef] [PubMed]
- Mundi, M.S.; Mohamed Elfadil, O.; Hurt, R.T.; Bonnes, S.; Salonen, B.R. Management of long-term home parenteral nutrition: Historical perspective, common complications, and patient education and training. JPEN J. Parenter. Enter. Nutr. 2023, 47 (Suppl. S1), S24–S34. [Google Scholar] [CrossRef]
- Stewart, A.G.; Laupland, K.B.; Tabah, A. Central line associated and primary bloodstream infections. Curr. Opin. Crit. Care 2023, 29, 423–429. [Google Scholar] [CrossRef]
- Alanazi, F.K.; Lapkin, S.; Molloy, L.; Sim, J. Healthcare-associated infections in adult intensive care units: A multisource study examining nurses’ safety attitudes, quality of care, missed care, and nurse staffing. Intensive Crit. Care Nurs. 2023, 78, 103480. [Google Scholar] [CrossRef] [PubMed]
- Wang, P.; Wang, Y.; Lu, L.; Yan, W.; Tao, Y.; Zhou, K.; Jia, J.; Cai, W. Alterations in intestinal microbiota relate to intestinal failure-associated liver disease and central line infections. J. Pediatr. Surg. 2017, 52, 1318–1326. [Google Scholar] [CrossRef] [PubMed]
- Gotchac, J.; Poullenot, F.; Guimber, D.; Ecochard-Dugelay, E.; Schneider, S.; Peretti, N.; Billiauws, L.; Borderon, C.; Breton, A.; Chaillou Legault, E.; et al. Management of Central Venous Catheters in Children and Adults on Home Parenteral Nutrition: A French Survey of Current Practice. Nutrients 2022, 14, 2532. [Google Scholar] [CrossRef]
- Cavicchi, M.; Beau, P.; Crenn, P.; Degott, C.; Messing, B. Prevalence of liver disease and contributing factors in patients receiving home parenteral nutrition for permanent intestinal failure. Ann. Intern. Med. 2000, 132, 525–532. [Google Scholar] [CrossRef]
- Mutanen, A.; Lohi, J.; Merras-Salmio, L.; Koivusalo, A.; Pakarinen, M.P. Prediction, identification, and progression of histopathological liver disease activity in children with intestinal failure. J. Hepatol. 2021, 74, 593–602. [Google Scholar] [CrossRef]
- Ponzo, V.; Pellegrini, M.; Cioffi, I.; Scaglione, L.; Bo, S. The Refeeding Syndrome: A neglected but potentially serious condition for inpatients. A narrative review. Intern. Emerg. Med. 2021, 16, 49–60. [Google Scholar] [CrossRef]
- Marinella, M.A. The refeeding syndrome and hypophosphatemia. Nutr. Rev. 2003, 61, 320–323. [Google Scholar] [CrossRef] [PubMed]
- Da Silva, J.S.V.; Seres, D.S.; Sabino, K.; Adams, S.C.; Berdahl, G.J.; Citty, S.W.; Cober, M.P.; Evans, D.C.; Greaves, J.R.; Gura, K.M.; et al. ASPEN Consensus Recommendations for Refeeding Syndrome. Nutr. Clin. Pract. 2020, 35, 178–195. [Google Scholar] [CrossRef] [PubMed]
- Araujo-Castro, M.; Vázquez-Martínez, C. The refeeding syndrome. Importance of phosphorus. Med. Clin. 2018, 150, 472–478. [Google Scholar] [CrossRef]
- Crook, M.A.; Hally, V.; Panteli, J.V. The importance of the refeeding syndrome. Nutrition 2001, 17, 632–637. [Google Scholar] [CrossRef] [PubMed]
- Pacei, F.; Tesone, A.; Laudi, N.; Laudi, E.; Cretti, A.; Pnini, S.; Varesco, F.; Colombo, C. The Relevance of Thiamine Evaluation in a Practical Setting. Nutrients 2020, 12, 2810. [Google Scholar] [CrossRef] [PubMed]
- Dos Santos, V.M.; Dos Santos, L.A.M.; Sugai, T.A.M. Refeeding syndrome: A challenging entity. An. Sist. Sanit. Navar. 2022, 45, e0995. [Google Scholar] [CrossRef] [PubMed]
- Wales, P.W.; Allen, N.; Worthington, P.; George, D.; Compher, C.; American Society for Parenteral and Enteral Nutrition; Teitelbaum, D. A.S.P.E.N. Clinical Guidelines: Support of Pediatric Patients With Intestinal Failure at Risk of Parenteral Nutrition–Associated Liver Disease. JPEN J. Parenter. Enter. Nutr. 2014, 38, 538–557. [Google Scholar] [CrossRef]
- Cuerda, C.; Pironi, L.; Arends, J.; Bozzetti, F.; Gillanders, L.; Jeppesen, P.B.; Joly, F.; Kelly, D.; Lal, S.; Staun, M.; et al. ESPEN practical guideline: Clinical nutrition in chronic intestinal failure. Clin. Nutr. 2021, 40, 5196–5220. [Google Scholar] [CrossRef]
- Matarese, L.E.; Harvin, G. Nutritional Care for Patients with Intestinal Failure. Gastroenterol. Clin. N. Am. 2021, 50, 201–216. [Google Scholar] [CrossRef]
- Matarese, L.E.; Jeppesen, P.B.; O’Keefe, S.J. Short bowel syndrome in adults: The need for an interdisciplinary approach and coordinated care. JPEN J. Parenter. Enter. Nutr. 2014, 38 (Suppl. S1), 60S–64S. [Google Scholar] [CrossRef]
- Wall, E.; Catron, H.; Delgado, A.; Greif, S.; Herlitz, J.; Moccia, L.; Lozano, E.; Mercer, D.; Vanuytsel, T.; Berner-Hansen, M.; et al. A multidisciplinary team evaluation of management guidelines for adult short bowel syndrome. Clin. Nutr. ESPEN 2023, 54, 41–44. [Google Scholar] [CrossRef]
- Geransar, P.; Lal, S.; Jeppesen, P.B.; Pironi, L.; Rzepa, E.; Schneider, S.M. Survey of healthcare professionals’ experiences of care delivery in patients with chronic intestinal failure: ATLAS of Variance. Clin. Nutr. ESPEN 2023, 54, 157–165. [Google Scholar] [CrossRef]
- Belcher, E.; Mercer, D.; Raphael, B.P.; Salinas, G.D.; Stacy, S.; Tappenden, K.A. Management of short-bowel syndrome: A survey of unmet educational needs among healthcare providers. JPEN J. Parenter. Enter. Nutr. 2022, 46, 1839–1846. [Google Scholar] [CrossRef]
- Premkumar, M.H.; Soraisham, A.; Bagga, N.; Adriana Massieu, L.; Maheshwari, A. Nutritional Management of Short Bowel Syndrome. Clin. Perinatol. 2022, 49, 557–572. [Google Scholar] [CrossRef]
- Bielawska, B.; Allard, J.P. Parenteral nutrition and intestinal failure. Nutrients 2017, 9, 466. [Google Scholar] [CrossRef]
- Bering, J.; DiBaise, J.K. Home Parenteral and Enteral Nutrition. Nutrients 2022, 14, 2558. [Google Scholar] [CrossRef]
- Doley, J. Enteral Nutrition Overview. Nutrients 2022, 14, 2180. [Google Scholar] [CrossRef]
- Avitzur, Y.; Courtney-Martin, G. Enteral approaches in malabsorption. Best Pract. Res. Clin. Gastroenterol. 2016, 30, 295–307. [Google Scholar] [CrossRef]
- Bonnes, S.L.; Salonen, B.R.; Hurt, R.T.; McMahon, M.T.; Mundi, M.S. Parenteral and Enteral Nutrition-from Hospital to Home: Will It Be Covered? Nutr. Clin. Pract. 2017, 32, 730–738. [Google Scholar] [CrossRef]
- Griffin, G.E.; Fagan, G.E.; Hodgson, H.J.; Chadwick, V.S. Enteral therapy in the management of massive gut resection complicated by chronic fluid and electrolyte depletion. Dig. Dis. Sci. 1982, 27, 902–908. [Google Scholar] [CrossRef]
- Gustafsson, U.O.; Ljungqvist, O. Perioperative nutritional management in digestive tract surgery. Curr. Opin. Clin. Nutr. Metab. Care 2011, 14, 504–509. [Google Scholar] [CrossRef] [PubMed]
- Berger, M.M.; Shenkin, A.; Schweinlin, A.; Amrein, K.; Augsburger, M.; Biesalski, H.K.; Bischoff, S.C.; Casaer, M.P.; Gundogan, K.; Lepp, H.L.; et al. ESPEN micronutrient guideline. Clin. Nutr. 2022, 41, 1357.e424. [Google Scholar] [CrossRef] [PubMed]
- Btaiche, I.F.; Carver, P.L.; Welch, K.B. Dosing and monitoring of trace elements in long-term home parenteral nutrition patients. JPEN J. Parenter. Enter. Nutr. 2011, 35, 736–747. [Google Scholar] [CrossRef]
- Jin, J.; Mulesa, L.; Carrilero Rouillet, M. Trace Elements in Parenteral Nutrition: Considerations for the Prescribing Clinician. Nutrients 2017, 9, 440. [Google Scholar] [CrossRef] [PubMed]
- McKeever, L. Vitamin and Trace Elements. In The ASPEN Adult Nutrition Support Core Curriculum, 3rd ed.; Mueller, C.M., Ed.; ASPEN: Silver Spring, MD, USA, 2017; pp. 139–184. [Google Scholar]
- Konrad, D.; Mitchell, R.; Hendrickson, E. Home nutrition support. In The ASPEN Adult Nutrition Support Core Curriculum, 3rd ed.; Mueller, C.M., Ed.; ASPEN: Silver Spring, MD, USA, 2017; pp. 765–784. [Google Scholar]
- Charney, P.; Malone, A. Biochemical Test, Medical Data, and Procedures. In Pocket Guide to Nutrition Assessment, 4th ed.; Charney, P., Malone, A., Eds.; Academy of Nutrition and Dietetics: Chicago, IL, USA, 2022; pp. 111–201. [Google Scholar]
- Williams, N.S.; Evans, P.; King, R.F. Gastric acid secretion and gastrin production in the short bowel syndrome. Gut 1985, 26, 914–919. [Google Scholar] [CrossRef] [PubMed]
- Thompson, J.S.; Langnas, A.N. Surgical approaches to improving intestinal function in the short bowel syndrome. Arch. Surg. 1999, 134, 706–711. [Google Scholar] [CrossRef] [PubMed]
- Kumpf, V.J. Pharmacologic management of diarrhea in patients with short bowel syndrome. JPEN J. Parenter. Enter. Nutr. 2014, 38 (Suppl. S1), 38S–44S. [Google Scholar] [CrossRef] [PubMed]
- Zafar, H.; Jimenez, B.; Schneider, A. Small intestinal bacterial overgrowth: Current update. Curr. Opin. Gastroenterol. 2023, 39, 522–528. [Google Scholar] [CrossRef]
- Larsen, H.M.; Krogh, K.; Borre, M.; Gregersen, T.; Mejlby Hansen, M.; Arveschoug, A.K.; Christensen, P.; Drewes, A.M.; Emmertsen, K.J.; Laurberg, S.; et al. Chronic loose stools following right-sided hemicolectomy for colon cancer and the association with bile acid malabsorption and small intestinal bacterial overgrowth. Color. Dis. 2023, 25, 600–607. [Google Scholar] [CrossRef]
- Korzilius, J.W.; Gompelman, M.; Wezendonk, G.T.J.; Jager, N.G.L.; Rovers, C.P.; Brüggemann, R.J.M.; Wanten, G.J.A. Oral antimicrobial agents in patients with short bowel syndrome: Worth a try! J. Antimicrob. Chemother. 2023, 78, 2008–2014. [Google Scholar] [CrossRef]
- Hofmann, A.F.; Poley, J.R. Role of bile acid malabsorption in pathogenesis of diarrhea and steatorrhea in patients with ileal resection. I. Response to cholestyramine or replacement of dietary long chain triglyceride by medium chain triglyceride. Gastroenterology 1972, 62, 918–934. [Google Scholar] [CrossRef] [PubMed]
- Scaldaferri, F.; Pizzoferrato, M.; Ponziani, F.R.; Gasbarrini, G.; Gasbarrini, A. Use and indications of cholestyramine and bile acid sequestrants. Intern. Emerg. Med. 2013, 8, 205–210. [Google Scholar] [CrossRef] [PubMed]
- Poley, J.R.; Hofmann, A.F. Role of fat maldigestion in pathogenesis of steatorrhea in ileal resection. Fat digestion after two sequential test meals with and without cholestyramine. Gastroenterology 1976, 71, 38–44. [Google Scholar] [CrossRef] [PubMed]
- DiBaise, J.K. Does my patient have bile acid malabsorption? Pract. Gastroenterol. 2020, 44, 10–24. [Google Scholar]
- Sainath, N.N.; Bales, C.; Brownell, J.N. Octavia Pickett-Blakely, Aisha Sattar, Virginia A Stallings. Impact of Pancreatic Enzymes on Enteral Fat and Nitrogen Absorption in Short Bowel Syndrome. J. Pediatr. Gastroenterol. Nutr. 2022, 75, 36–41. [Google Scholar] [CrossRef] [PubMed]
- Mouillot, T.; Beylot, M.; Drai, J.; Hillon, P.; Gelas, P.; Lauverjat, M.; Brondel, L.; Chambrier, C. Effect of bile acid supplementation on endogenous lipid synthesis in patients with short bowel syndrome: A pilot study. Clin. Nutr. 2020, 39, 928–934. [Google Scholar] [CrossRef] [PubMed]
- O’Keefe, S.J.; Haymond, M.W.; Bennet, W.M.; Oswald, B.; Nelson, D.K.; Shorter, R.G. Long-acting somatostatin analogue therapy and protein metabolism in patients with jejunostomies. Gastroenterology 1994, 107, 379–388. [Google Scholar] [CrossRef]
- Nightingale, J.M.D. How to manage a high-output stoma. Frontline Gastroenterol. 2021, 13, 140–151. [Google Scholar] [CrossRef]
- Kusuhara, K.; Kusunoki, M.; Okamoto, T.; Sakanoue, Y.; Utsunomiya, J. Reduction of the effluent volume in high- output ileostomy patients by a somatostatin analogue, SMS 201-995. Int. J. Color. Dis. 1992, 7, 202–205. [Google Scholar] [CrossRef]
- Shaffer, J.L.; O’Hanrahan, T.; Rowntree, S. Does somatostatin analogue (201-995) reduce high output stoma effluent? A controlled trial. Gut 1988, 29, A1432–A1433. [Google Scholar]
- Nightingale, J.M.; Walker, E.R.; Burnham, W.R.; Farthing, M.J.; Lennard-Jones, J.E. Octreotide (a somatostatin analogue) improves the quality of life in some patients with a short intestine. Aliment. Pharmacol. Ther. 1989, 3, 67–73. [Google Scholar] [CrossRef] [PubMed]
- Ladefoged, K.; Christensen, K.C.; Hegnhoj, J.; Jarnum, S. Effect of a long-acting somatostatin analogue SMS 201-995 on jejunostomy effluents in patients with severe short bowel syndrome. Gut 1989, 30, 943–949. [Google Scholar] [CrossRef]
- Lémann, M.; de Montigny, S.; Mahé, S. Effect of octreotide on water and electrolytes losses, nutrient absorption, and transit in short bowel syndrome. Eur. J. Gastroenterol. Hepatol. 1993, 5, 817–822. [Google Scholar]
- O’Keefe, S.J.; Peterson, M.E.; Fleming, C.R. Octreotide as an adjunct to home parenteral nutrition in the management of permanent end-jejunostomy syndrome. JPEN J. Parenter. Enter. Nutr. 1994, 18, 26–34. [Google Scholar] [CrossRef]
- Nightingale, J.M.; Lennard-Jones, J.E.; Gertner, D.J.; Wood, S.R.; Bartram, C.I. Colonic preservation reduces need for parenteral therapy, increases incidence of renal stones, but does not change high prevalence of gall stones in patients with a short bowel. Gut 1992, 33, 1493–1497. [Google Scholar] [CrossRef] [PubMed]
- Dowling, R.H.; Hussaini, S.H.; Murphy, G.M.; Wass, J.A. Gallstones during octreotide therapy. Digestion 1993, 54, 107–120. [Google Scholar] [CrossRef] [PubMed]
- Nehra, V.; Camilleri, M.; Burton, D.; Oenning, L.; Kelly, D.G. An open trial of octreotide long-acting release in the management of short bowel syndrome. Am. J. Gastroenterol. 2001, 96, 1494–1498. [Google Scholar] [CrossRef] [PubMed]
- Mesli, Y.; Holterbach, L.; Delhorme, J.B.; Lakkis, Z.; Ortega-Deballon, P.; Deguelte, S.; Rohr, S.; Brigand, C.; Meyer, N.; Romain, B. Is lanreotide useful in high output stoma? comparison between lanreotide to conventional antidiarrheal treatment alone. J. Investig. Surg. 2020, 4, 1312–1316. [Google Scholar] [CrossRef]
- Jeppesen, P.B.; Pertkiewicz, M.; Messing, B.; Iyer, K.; Seidner, D.L.; O’keefe, S.J.D.; Forbes, A.; Bo Joelsson, H.H. Teduglutide reduces need for parenteral support among patients with short bowel syndrome with intestinal failure. Gastroenterology 2012, 143, 1473–1481. [Google Scholar] [CrossRef]
- Jeppesen, P.B.; Pertkiewicz, M.; Forbes, A.; Pironi, L.; Gabe, S.M.; Joly, F.; Messing, B.; Loth, S.; Youssef, N.N.; Heinze, H.; et al. Quality of life in patients with short bowel syndrome treated with the new glucagon-like peptide-2 analogue teduglutide—Analyses from a randomised, placebo-controlled study. Clin. Nutr. 2013, 32, 713–721. [Google Scholar] [CrossRef]
- Jeppesen, P.B.; Gilroy, R.; Pertkiewicz, M.; Allard, J.P.; Messing, B.; O’Keefe, S.J. Randomised placebo-controlled trial of teduglutide in reducing parenteral nutrition and/or intravenous fluid requirements in patients with short bowel syndrome. Gut 2011, 60, 902–914. [Google Scholar] [CrossRef]
- Jeppesen, P.B.; Gabe, S.M.; Seidner, D.L.; Lee, H.M.; Olivier, C. Factors Associated with Response to Teduglutide in Patients with Short-Bowel Syndrome and Intestinal Failure. Gastroenterology 2018, 154, 874–885. [Google Scholar] [CrossRef] [PubMed]
- Jeppesen, P.B. Pharmacologic options for intestinal rehabilitation in patients with short bowel syndrome. JPEN J. Parenter. Enter. Nutr. 2014, 38 (Suppl. S1), 45S–52S. [Google Scholar] [CrossRef] [PubMed]
- Nørholk, L.M.; Holst, J.J.; Jeppesen, P.B. Treatment of adult short bowel syndrome patients with teduglutide. Expert Opin. Pharmacother. 2012, 13, 235–243. [Google Scholar] [CrossRef] [PubMed]
- Valiente, P.A.; Nim, S.; Kim, J.; Kim, P.M. Computational Design of Potent and Selective d-Peptide Agonists of the Glucagon-like Peptide-2 Receptor. J. Med. Chem. 2023, 66, 10342–10353. [Google Scholar] [CrossRef] [PubMed]
- de Dreuille, B.; Nuzzo, A.; Bataille, J.; Mailhat, C.; Billiauws, L.; Le Gall, M.; Joly, F. Post-Marketing Use of Teduglutide in a Large Cohort of Adults with Short Bowel Syndrome-Associated Chronic Intestinal Failure: Evolution and Outcomes. Nutrients 2023, 15, 2448. [Google Scholar] [CrossRef] [PubMed]
- Greif, S.; Maasberg, S.; Wehkamp, J.; Fusco, S.; Zopf, Y.; Herrmann, H.J.; Lamprecht, G.; Jacob, T.; Schiefke, I.; von Websky, M.W.; et al. Long-term results of teduglutide treatment for chronic intestinal failure—Insights from a national, multi-centric patient home-care service program. Clin. Nutr. ESPEN 2022, 51, 222–230. [Google Scholar] [CrossRef]
- Blüthner, E.; Pape, U.F.; Tacke, F.; Greif, S. Quality of Life in Teduglutide-Treated Patients with Short Bowel Syndrome Intestinal Failure-A Nested Matched Pair Real-World Study. Nutrients 2023, 15, 1949. [Google Scholar] [CrossRef]
- Joly, F.; Seguy, D.; Nuzzo, A.; Chambrier, C.; Beau, P.; Poullenot, F.; Thibault, R.; Armengol Debeir, L.; Layec, S.; Boehm, V.; et al. Six-month outcomes of teduglutide treatment in adult patients with short bowel syndrome with chronic intestinal failure: A real-world French observational cohort study. Clin. Nutr. 2020, 39, 2856–2862. [Google Scholar] [CrossRef]
- Pironi, L. Translation of Evidence into Practice with Teduglutide in the Management of Adults with Intestinal Failure due to Short-Bowel Syndrome: A Review of Recent Literature. JPEN J. Parenter. Enter. Nutr. 2020, 44, 968–978. [Google Scholar] [CrossRef]
- Kochar, B.; Herfarth, H.H. Teduglutide for the treatment of short bowel syndrome—A safety evaluation. Expert Opin. Drug Saf. 2018, 17, 733–739. [Google Scholar] [CrossRef] [PubMed]
- Chen, Y.; Tsai, Y.H.; Tseng, B.J.; Tseng, S.H. Influence of Growth Hormone and Glutamine on Intestinal Stem Cells: A Narrative Review. Nutrients 2019, 11, 1941. [Google Scholar] [CrossRef] [PubMed]
- Byrne, T.A.; Wilmore, D.W.; Iyer, K.; DiBaise, J.K.; Clancy, K.; Robinson, M.K.; Chang, P.; Gertner, J.M.; Lautz, D. Growth hormone, glutamine, and an optimal diet reduces parenteral nutrition in patients with short bowel syndrome: A prospective, randomized, placebo-controlled, double-blind clinical trial. Ann. Surg. 2005, 242, 655–661. [Google Scholar] [CrossRef]
- Ling, L.; Irving, M. The effectiveness of growth hormone, glutamine and a low-fat diet containing high carbohydrate on the enhancement of the function of remnant intestine among patients with short bowel syndrome: A review of published trials. Clin. Nutr. 2001, 20, 199–204. [Google Scholar] [CrossRef] [PubMed]
- Lauriti, G.; Zani, A.; Aufieri, R.; Cananzi, M.; Chiesa, P.L.; Eaton, S.; Pierro, A. Incidence, prevention, and treatment of parenteral nutrition-associated cholestasis and intestinal failure-associated liver disease in infants and children: A systematic review. JPEN J. Parenter. Enter. 2014, 38, 70–85. [Google Scholar] [CrossRef]
- Bond, A.; Huijbers, A.; Pironi, L.; Schneider, S.M.; Wanten, G.; Lal, S. Review article: Diagnosis and management of intestinal failure-associated liver disease in adults. Aliment. Pharmacol. Ther. 2019, 50, 640–653. [Google Scholar] [CrossRef]
- Cruz, R.J., Jr. Modified Antimesenteric Tapering Enteroplasty: An Alternative Technique for the Treatment of Dysfunctional Anastomosis in Patients with Short Bowel. Dis. Colon Rectum 2021, 64, e520–e525. [Google Scholar] [CrossRef] [PubMed]
- Hukkinen, M.; Mutanen, A.; Pakarinen, M.P. Small bowel dilation in children with short bowel syndrome is associated with mucosal damage, bowel-derived bloodstream infections, and hepatic injury. Surgery 2017, 162, 670–679. [Google Scholar] [CrossRef]
- Wendel, D.; Javid, P.J. Medical and Surgical Aspects of Intestinal Failure in the Child. Surg. Clin. N. Am. 2022, 102, 861–872. [Google Scholar] [CrossRef]
- Bueno, J. Surgical strategies in short bowel syndrome. Nutr. Hosp. 2007, 22 (Suppl. S2), 103–112. [Google Scholar]
- Carey, J.N.; Sheckter, C.C.; Watt, A.J.; Lee, G.K. Intra-abdominal pedicled rectus abdominis muscle flap for treatment of high-output enterocutaneous fistulae: Case reports and review of literature. J. Plast. Reconstr. Aesthet. Surg. 2013, 66, 1145–1148. [Google Scholar] [CrossRef] [PubMed]
- Beyer-Berjot, L.; Joly, F.; Maggiori, L.; Corcos, O.; Bouhnik, Y.; Bretagnol, F.; Panis, Y. Segmental reversal of the small bowel can end permanent parenteral nutrition dependency: An experience of 38 adults with short bowel syndrome. Ann. Surg. 2012, 256, 739–744. [Google Scholar] [CrossRef] [PubMed]
- Panis, Y.; Messing, B.; Rivet, P.; Coffin, B.; Hautefeuille, P.; Matuchansky, C.; Rambaud, J.C.; Valleur, P. Segment reversal of the small bowel as an alternative to intestinal transplantation in patients with short bowel syndrome. Ann. Surg. 1997, 225, 401–407. [Google Scholar] [CrossRef] [PubMed]
- Rege, A.S.; Sudan, D.L. Autologous gastrointestinal reconstruction: Review of the optimal nontransplant surgical options for adults and children with short bowel syndrome. Nutr. Clin. Pract. 2013, 28, 65–74. [Google Scholar] [CrossRef] [PubMed]
- Boroni, G.; Parolini, F.; Stern, M.V.; Moglia, C.; Alberti, D. Autologous Intestinal Reconstruction Surgery in Short Bowel Syndrome: Which, When, and Why. Front. Nutr. 2022, 9, 861093. [Google Scholar] [CrossRef] [PubMed]
- Thompson, J.S. Surgical approach to the short bowel syndrome: Procedures to slow intestinal transit. Eur. J. Pediatr. Surg. 1999, 9, 263–266. [Google Scholar] [CrossRef] [PubMed]
- Muff, J.L.; Sokolovski, F.; Walsh-Korb, Z.; Choudhury, R.A.; Dunn, J.C.Y.; Holland-Cunz, S.G.; Vuille-Dit-Bille, R.N. Surgical Treatment of Short Bowel Syndrome-The Past, the Present and the Future, a Descriptive Review of the Literature. Children 2022, 9, 1024. [Google Scholar] [CrossRef]
- Aubert, M.; Mege, D.; Billiauws, L.; Joly, F.; Panis, Y. State-of-the-art colorectal disease: Conservative surgical management of intestinal failure in adults. Int. J. Color. Dis. 2021, 36, 1597–1607. [Google Scholar] [CrossRef]
- Horslen, S.P.; Smith, J.M.; Ahn, Y.; Skeans, M.A.; Cafarella, M.; Noreen, S.M.; Snyder, J.J.; Israni, A.K. OPTN/SRTR 2019 annual data report: Intestine. Am. J. Transpl. 2021, 21 (Suppl. S2), 316–355. [Google Scholar] [CrossRef]
- Huynh, N.; Dubrovsky, G.; Rouch, J.D.; Scott, A.; Chiang, E.; Nguyen, T.; Wu, B.M.; Shekherdimian, S.; Krummel, T.M.; Dunn, J.C.Y. Three-Dimensionally Printed Surface Features to Anchor Endoluminal Spring for Distraction Enterogenesis. PLoS ONE 2018, 13, e0200529. [Google Scholar] [CrossRef]
- Sugimoto, S.; Kobayashi, E.; Fujii, M.; Ohta, Y.; Arai, K.; Matano, M.; Ishikawa, K.; Miyamoto, K.; Toshimitsu, K.; Takahashi, S.; et al. An Organoid-Based Organ-Repurposing Approach to Treat Short Bowel Syndrome. Nature 2021, 592, 99–104. [Google Scholar] [CrossRef] [PubMed]
- Huang, J.; Xu, Z.; Ren, J. Intestinalization Small of Colon Using Ileum Organoids. Trends Cell Biol. 2021, 31, 517–519. [Google Scholar] [CrossRef] [PubMed]
- Sugimoto, S.; Kobayashi, E.; Kanai, T.; Sato, T. In Vivo Intestinal Research Using Organoid Transplantation. Keio J. Med. 2022, 71, 73–81. [Google Scholar] [CrossRef] [PubMed]
- Kobayashi, E.A. New stage of experimental surgery for organoid based intestinal regeneration—A review of or-ganoid research and recent advance. Magy. Seb. 2022, 75, 261–264. [Google Scholar] [CrossRef] [PubMed]
- Nightingale, J.; Woodward, J.M. Small Bowel and Nutrition Committee of the British Society of Gastroenterology Guidelines for management of patients with a short bowel. Gut 2006, 55 (Suppl. S4), iv1–iv12. [Google Scholar] [CrossRef] [PubMed]
- Khalaf, R.T.; Sokol, R.J. New Insights into Intestinal Failure-Associated Liver Disease in Children. Hepatology 2020, 71, 1486–1498. [Google Scholar] [CrossRef]
- Lacaille, F.; Gupte, G.; Colomb, V.; D’Antiga, L.; Hartman, C.; Hojsak, I.; Kolacek, S.; Puntis, J.; Shamir, R. Intestinal failure associated liver disease: A position paper of the ESPGHAN Working Group of Intestinal Failure and Intestinal Transplantation. J. Pediatr. Gastroenterol. Nutr. 2015, 60, 272–283. [Google Scholar] [CrossRef]
- Secor, J.D.; Yu, L.; Tsikis, S.; Fligor, S.; Puder, M.; Gura, K.M. Current strategies for managing intestinal failure-associated liver disease. Expert Opin. Drug Saf. 2021, 20, 307–320. [Google Scholar] [CrossRef]
- Buchman, A.L.; Scolapio, J.; Fryer, J. AGA technical review on short bowel syndrome and intestinal transplantation. Gastroenterology 2003, 124, 1111–1134. [Google Scholar] [CrossRef]
- Kaufman, S.S.; Atkinson, J.B.; Bianchi, A.; Goulet, O.J.; Grant, D.; Langnas, A.N.; McDiarmid, S.V.; Mittal, N.; Reyes, J.; Tzakis, A.G. American Society of Transplantation. Indications for pediatric intestinal transplantation: A position paper of the American Society of Transplantation. Pediatr. Transpl. 2001, 5, 80–87. [Google Scholar] [CrossRef]
- Pironi, L.; Arends, J.; Bozzetti, F.; Cuerda, C.; Gillanders, L.; Jeppesen, P.B.; Joly, F.; Kelly, D.; Lal, S.; Staun, M.; et al. Home Artificial Nutrition & Chronic Intestinal Failure Special Interest Group of ESPEN. ESPEN guidelines on chronic intestinal failure in adults. Clin. Nutr. 2016, 35, 247–307. [Google Scholar] [CrossRef] [PubMed]
- Pironi, L.; Cuerda, C.; Jeppesen, P.B.; Joly, F.; Jonkers, C.; Krznarić, Ž.; Lal, S.; Lamprecht, G.; Lichota, M.M.; Mundi, M.S.; et al. ESPEN guideline on chronic intestinal failure in adults—Update 2023. Clin. Nutr. 2023, 42, 1940–2021. [Google Scholar] [CrossRef] [PubMed]
- Lal, S.; Pironi, L.; Wanten, G.; Arends, J.; Bozzetti, F.; Cuerda, C.; Joly, F.; Kelly, D.; Staun, M.; Szczepanek, K.; et al. Clinical approach to the management of Intestinal Failure Associated Liver Disease (IFALD) in adults: A position paper from the Home Artificial Nutrition and Chronic Intestinal Failure Special Interest Group of ESPEN. Clin. Nut 2018, 37 Pt A, 1794–1797. [Google Scholar] [CrossRef] [PubMed]
- Bettag, J.; Po, L.; Cunningham, C.; Tallam, R.; Kurashima, K.; Nagarapu, A.; Hutchinson, C.; Morfin, S.; Nazzal, M.; Lin, C.; et al. Novel Therapeutic Approaches for Mitigating Complications in Short Bowel Syndrome. Nutrients 2022, 14, 4660. [Google Scholar] [CrossRef] [PubMed]
- Parrish, A.B.; O’Neill, S.M.; Crain, S.R.; Russell, T.A.; Sonthalia, D.K.; Nguyen, V.T.; Aboulian, A. An Enhanced Recovery after Surgery (ERAS) Protocol for Ambulatory Anorectal Surgery Reduced Postoperative Pain and Unplanned Returns to Care After Discharge. World J. Surg. 2018, 42, 1929–1938. [Google Scholar] [CrossRef] [PubMed]
- Gudaityte, J.; Marchertiene, I.; Pavalkis, D. Anesthesia for ambulatory anorectal surgery. Medicina 2004, 40, 101–111. [Google Scholar] [PubMed]
- Heitmann, P.T.; Vollebregt, P.F.; Knowles, C.H.; Lunniss, P.J.; Dinning, P.G.; Scott, S.M. Understanding the physiology of human defaecation and disorders of continence and evacuation. Nat. Rev. Gastroenterol. Hepatol. 2021, 18, 751–769. [Google Scholar] [CrossRef]
- Jensen, S.L. Diet and other risk factors for fissure-in-ano. Prospective case control study. Dis. Colon Rectum 1988, 31, 770–773. [Google Scholar] [CrossRef]
- Kecmanovic, D.M.; Pavlov, M.J.; Ceranic, M.S.; Kerkez, M.D.; Rankovic, V.I.; Masirevic, V.P. Bulk agent Plantago ovata after Milligan-Morgan hemorrhoidectomy with Ligasure. Phytother. Res. 2006, 20, 655–658. [Google Scholar] [CrossRef]
- Urganci, N.; Akyildiz, B.; Polat, T.B. A comparative study: The efficacy of liquid paraffin and lactulose in management of chronic functional constipation. Pediatr. Int. 2005, 47, 15–19. [Google Scholar] [CrossRef]
- Nessim, A.; Wexner, S.D.; Agachan, F.; Alabaz, O.; Weiss, E.G.; Nogueras, J.J.; Daniel, N.; Billotti, V.L. Is bowel confinement necessary after anorectal reconstructive surgery? A prospective, randomized, surgeon-blinded trial. Dis. Colon Rectum 1999, 42, 16–23. [Google Scholar] [CrossRef] [PubMed]
- Johnson, C.D.; Budd, J.; Ward, A.J. Laxatives after hemorrhoidectomy. Dis. Colon Rectum 1987, 30, 780–781. [Google Scholar] [CrossRef] [PubMed]
- Joos, A.K.; Palma, P.; Jonescheit, J.O.; Hasenberg, T.; Herold, A. Enteral vs parenteral nutrition in reconstructive anal surgery—A prospective-randomized trial. Color. Dis. 2008, 10, 605–609. [Google Scholar] [CrossRef] [PubMed]
| Dietary Advice | Background and Potential Benefits |
|---|---|
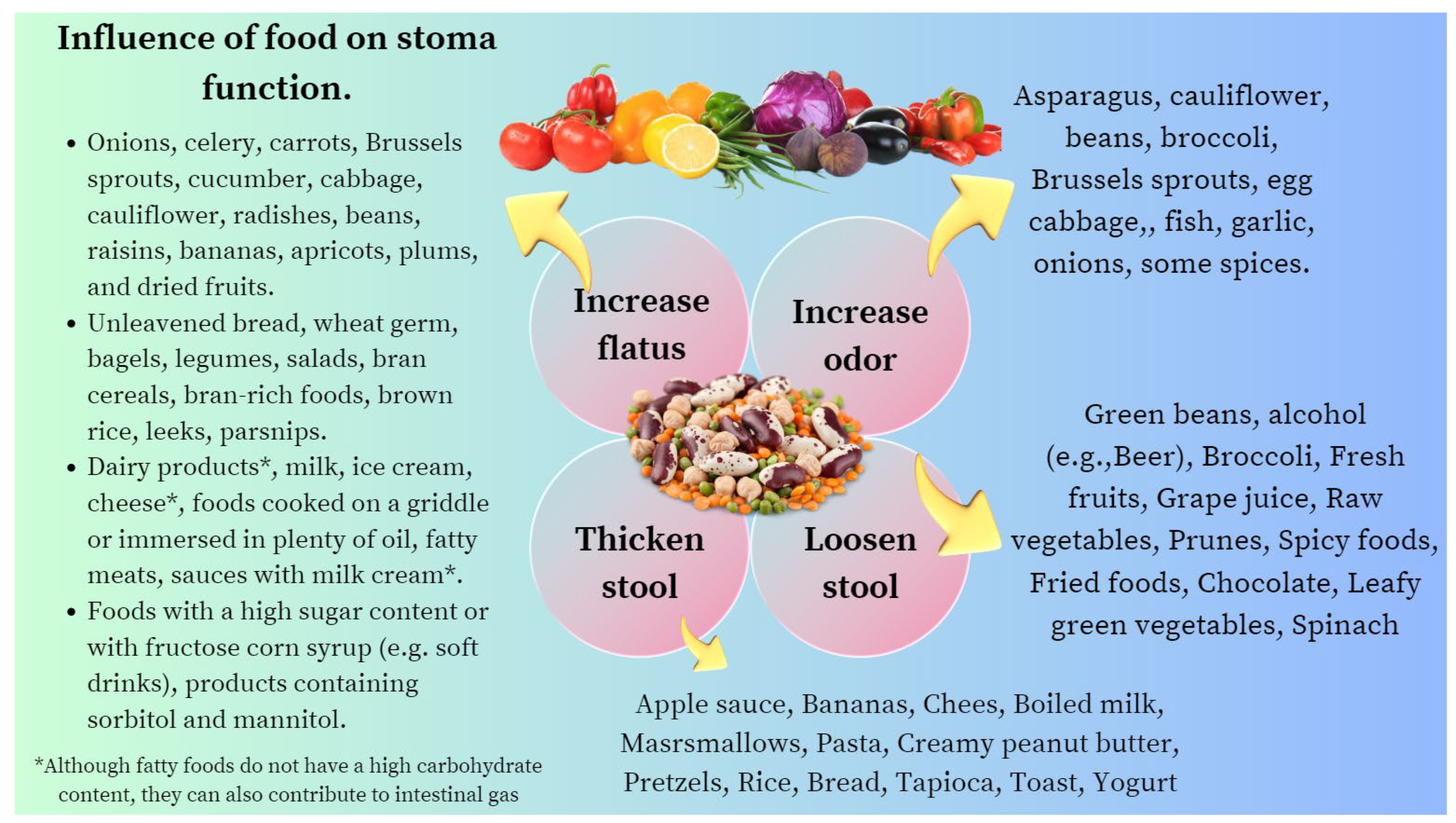
| Avoiding foods that contribute to decreased stool consistency (e.g., caffeine, plums or plum juice (both contain sorbitol), alcohol, and excessive fat). | Avoiding these foods helps to improve stool consistency (e.g., Bristol 6–7 to Bristol 5) and improves continence. |
| Intake of high-fiber foods. | High-fiber foods should lead to an increase in solid stool consistency, thus improving symptoms or incontinence due to diarrhea. |
| Avoiding an over-ingestion of insoluble fiber (e.g., wheat bran, some fruits (e.g., kiwi, grapes, raspberries, strawberries, rhubarb, pineapple, raisins, and blueberries), vegetables (e.g., green beans, corn, eggplant, broccoli, kale, spinach, and legumes like chickpeas or lentils), and whole grains). | Insoluble fibers add bulk to the stool and appears to help food pass more quickly through the stomach and intestines. However, they could lead to a deterioration of symptoms due to an increased number of spontaneous defecations as well as bloating #. |
| Preferably eat soluble fiber (bulking agents) (e.g., oat bran, nuts, barley, peas, seeds, beans, lentils, some fruits (e.g., guavas, apples, nectarines, pears, avocados, and apricots), and vegetables (e.g., brussels sprouts, broccoli, sweet potatoes, carrots, and turnips), as well as the psyllium, a common fiber supplement. | Soluble fibers attract water and turn into a gel during digestion. This slows digestion. In addition, soluble fibers should be recommended to achieve better stool consistency #. |
| Some Foods that Cause Abdominal Bloating due to Their Increased Production of Hydrogen, Carbon Dioxide, and Methane Gas. |
|---|
| Due to their high raffinose content: |
| beans, asparagus, soybeans, chickpeas, peanuts, peas, beans cabbage, cauliflower, brussels sprouts, and broccoli. Their consumption can cause flatulence because the tract does not synthesize α-galactosidase, the enzyme responsible for hydrolyzing these oligosaccharides. |
| Due to their high starch content: potatoes, corn, noodles, and wheat, but not rice. |
| Due to their high soluble fiber content: carrots, celery, onion, oat bran, peas, and most fruit, including apples, pears, peaches, plums, figs, cherries, and dates. |
| Some foods that decrease gas production, contributing to the attenuation of symptoms: Pineapples (for their bromelain content (a proteolytic enzyme)), papayas (contains papain), kiwis (actidine), and even figs, rich in ficin. |
| Mechanisms Involved in the Malnutrition of IBD Patients. |
|---|
| Limited intake caused by outbreaks of inflammatory activity (coexistence of limiting symptoms), and hypoorexia associated with the release of interleukins (e.g., IL-1 and IL-6) and tumor necrosis factor alpha. |
| Malabsorption caused by enteropathy (e.g., focal and segmental villous atrophy). |
| Maldigestion (e.g., steatorrhea due to malabsorption of bile salts after ileum resections >100 cm or secondary disaccharidase deficiency in the presence of severe enteropathy). |
| Bowel obstruction (nausea, vomiting, and inability to ingest food). |
| Protein-losing enteropathy due to malabsorption and mucosal ulceration (exudation of blood, mucus, and proteins) or high-output enterocutaneous fistulas. |
| The anatomical absorption surface is reduced after extensive small bowel resections, especially if the length of the removed ileum is beyond the critical point of 100 cm. |
| Increased basal energy expenditure due to transient states of catabolism (e.g., suppurative complications, such as fistulas and abscesses, leading to SIRS), severe outbreaks of ulcerative colitis with systemic toxicity, or major surgery. |
| Small intestine bacterial overgrowth (bacteria cause focal and segmental villous atrophy, deconjugation of bile salts, and excessive consumption of vitamin B12). |
| Glucocorticoids (interference with growth hormones, bone formation, nitrogen retention, and collagen synthesis). |
| Adverse effects of other drugs: metronidazole: decreased palatability; methotrexate/sulfasalazine: <bioavailability of folate). |
| Mechanism Explaining Diarrhea in SBS | Comment |
|---|---|
| Loss of the anatomical absorption surface. | The pattern of nutrient absorption native to the parts of the gastrointestinal tract is shown in Figure 1. |
| Increase in the volume of hydrochloride secretion due to a failure of gastric secretory inhibitory mechanisms via the defective release of enterogastrones (e.g., VIP, GIP, neurotensine, peptide YY, and GLP-1). | Adds a great volume of secretions to the upper digestive tract. An excessively acidic pH denatures pancreatic enzymes and interferes with the action of bile salts, causing maldigestion. |
| Accelerated gastric and intestinal transit by disrupting the feedback mechanism depends on hormone release from the ileum (see above). | Maldigestion due to inadequate mixing of pancreatic enzymes and biliary salts with the macronutrients. |
| Decreased bile salt pool in the intestinal lumen caused by the resection of the ileum and interruption of enterohepatic circulation. | Choleretic diarrhea if resection <100 cm #. Steatorrhea and malabsorption of liposoluble vitamins (e.g., vitamins A, D, K, and E) if resection >100 cm ǂ. |
| Small intestinal bacterial overgrowth (SIBO). | SIBO injures the enterocytes, causing focal and segmental villous atrophy and secondary lactase deficiency, resulting in osmotic and secretory diarrhea. |
| Presence of inflammation in the remaining intestine (e.g., IBD or radiation injury). | Inflammatory diarrhea with exudation of blood, mucus, and pus, as well as protein-losing enteropathy. |
| Clostridium difficile infection. | Substantial risk in patients who receive antibiotics due to central catheter infections and/or remain bedridden postoperatively. |
| Inappropriate intake of hypotonic solutions (e.g., water, tea, or caffeine) or hyperosmolar drinks (e.g., fruit juices or sports drinks) for thirst relief, especially in patients with an end jejunostomy. | Jejunal mucosa is “leaky” and rapid sodium. fluxes occur across it. If water or any solution with a sodium concentration of less than 90 mmol/L is drunk, there is a net efflux of sodium from the plasma into the bowel lumen, exacerbating diarrhea. |
| Diarrhea-causing drugs or oral nutritional supplements with high osmolarity. | E.g., omeprazole, non-steroidal anti-inflammatory drugs, psychotropic drugs, colchicine, or resin cholestyramine in patients with ileal resections >100 cm. |
| Requirement | Comment | |
|---|---|---|
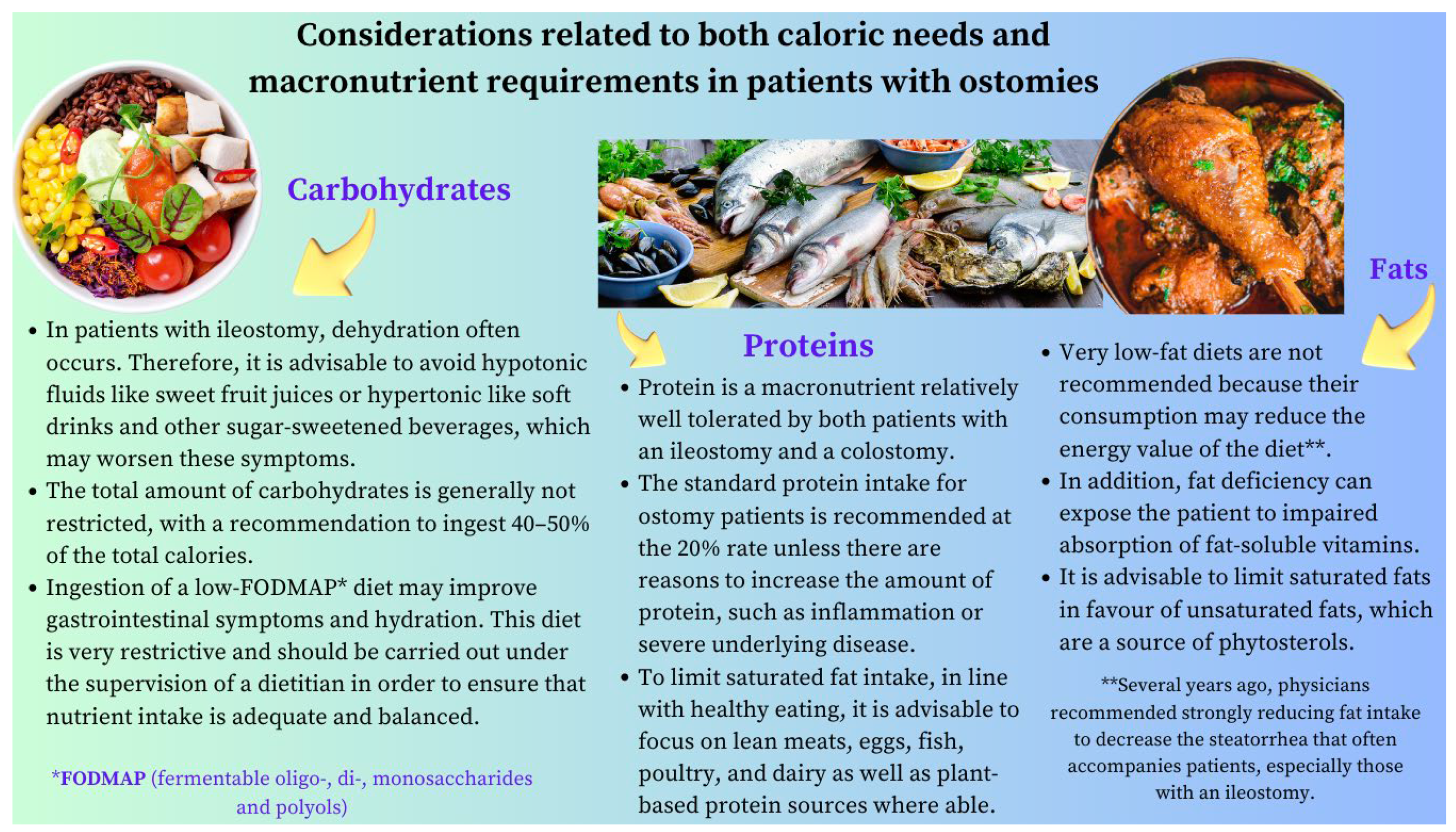
| Energy | 35–45 kcal/kg/day. In some cases, increasing the energy intake up to 60 kcal/kg/day may be necessary. | Patients with SBS develop compensatory hyperphagia, and it is advisable to take 5–6 meals spaced out during the day. |
| Carbohydrates | 20–40% of the daily energy target. | In the absence of a colon, it is not possible to rescue energy inherent in the production of short-chain fatty acids from the bacterial fermentation of sugars. |
| Protein | 1.5–2.0 g/kg/day or 20–30% of the daily energy target. | It is preferable to choose lean proteins of high biological value. |
| Fat | 40–60% of the daily energy target. | Choose essential fatty acids as the main component of fat intake. Consider MCTs in cases of malabsorption. |
| Fluids | Reduce oral hypotonic fluids to 500 mL/day #. Separating solids and liquids (i.e., do not drink anything for half an hour before or after a meal). | Add sodium chloride to any liquid feeds to make the sodium concentration near 100 mmol/L while keeping osmolality near 300 mOsmol/kg *. |
| Oxalate | The restriction is not necessary. | Calcium oxalate stones only occur in patients with a preserved colon. |
| Requirement | Comment | |
|---|---|---|
| Energy | 35–45 kcal/kg/day. In some cases, increasing the energy intake up to 60 kcal/kg/day may be necessary. | Patients with SBS develop compensatory hyperphagia, and it is advisable to take 5–6 meals spaced out during the day. |
| Carbohydrates | 50–60% of the daily energy target. | The colon provides energy (up to 1000 kcal/day) in SBS by releasing the SCFAs resulting from the fermentation of carbohydrates. In addition, it provides nutrition to the colonocytes. |
| Protein | 1.5–2.0 g/kg/day or 20–30% of the daily energy target. | It is preferable to choose lean proteins of high biological value. |
| Fluids | Isotonic/hypotonic #. | In SBS, the colon plays a vital role in fluid and electrolyte reabsorption, given the additional fluid that enters the colon with a capacity to absorb up to 6 L daily. |
| Fat | 20–30% of daily energy target. | In jejunum–colon patients, unabsorbed long-chain fatty acids in the colon are likely to reduce the transit time and reduce their water and sodium absorption, making their diarrhea worsen. Consider MCTs only in the case of severe malabsorption. MCT does not contain essential fatty acids. |
| Oxalate | The diet should be low in oxalate. | Nephrolithiasis only occurs in patients with a preserved large bowel. |
| Type of Micronutrient and Average Nutritional Intake Ranges | Clinical Signs Reflecting a Deficiency | Measurement | Typical Supplementation in SBS * |
|---|---|---|---|
| Water-soluble vitamins | Doses (all values per day) | ||
| Vitamin B1—thiamine (DRI: 1.1–1.2 mg/day) | Mental changes (apathy, decrease in short-term memory, confusion, and irritability), cognitive deficits, congestive heart failure, and metabolic lactic acidosis | Whole-blood ThDP or RBCs | Oral: 1–2 capsules daily (multivitamin: B1, B2, B3 B5, B6, and B7) |
| HPN and long-term PN: 2.5 mg/day | |||
| Vitamin B2—riboflavin (DRI: 1.3 mg/day—males. 1.1 mg/day—females) | Seborrheic dermatitis of the face, trunk, and scrotum, oral buccal lesions, ocular manifestations, marrow aplasia, and normochromic, normocytic anemia | Glutathione reductase activity in red blood cells | Oral: 1–2 capsules daily (multivitamin: B1, B2, B3 B5, B6, and B7) |
| HPN and long-term PN: 3.6 mg/day | |||
| Vitamin B3—niacin (DRI: 16 mg/day—adolescents and adult males > 14 years. 14 mg/day—females > 14 years) | Dementia, dermatitis, and diarrhea | Blood or tissue NAD | Oral: 1–2 capsules daily (multivitamin: B1, B2, B3 B5, B6, and B7) |
| HPN and long-term PN: 40 mg/day | |||
| Vitamin B5—pantothenic acid (DRI: 5 mg/day for 14 to over 70 years) | Fall in the diastolic and lability of systolic blood pressure, with postural hypotension, vertigo, and tachycardia. Gastrointestinal and neurological symptoms | Blood pantothenic acid | Oral: 1–2 capsules daily (multivitamin: B1, B2, B3 B5, B6, and B7) |
| HPN and long-term PN: 10 mg/day | |||
| Vitamin B6—pyridoxine (DRI: 1.3–1.7 mg/day for 14 to over 70 years) | Microcytic anemia, seborrheic dermatitis with cheilosis and glossitis, angular stomatitis, epileptiform convulsions, confusion, and/or depression | PLP levels. Red cell PLP in serious patients or in the presence of inflammation | Oral: 1–2 capsules daily (multivitamin: B1, B2, B3 B5, B6, and B7) |
| HPN and long-term PN: 4 mg/day | |||
| Vitamin B7—biotin (DRI: 40 μg/day) | Ataxia, dermatitis, and alopecia | Direct measure of urine and blood biotin that must be completed with the determination of biotin activity | Oral: 1–2 capsules daily (multivitamin: B1, B2, B3 B5, B6, and B7) |
| HPN and long-term PN: 60 μg/day | |||
| Vitamin B9—folic acid (DRI: 330 μg/day DFE) | Glossitis, megaloblastic anemia, pancytopenia, oral ulcers, angular stomatitis, and neuropsychiatric manifestations | Folate level in the plasma or serum—short-term status. In RBCs—long-term status | Oral: 1 mg daily |
| HPN and long-term PN: 400 μg/day | |||
| Vitamin B12—cobalamin (DRI: 2.4 μg/day) | Hematological, neurological, neuropsychiatric, and cognitive symptoms | Combination of at least two bio- markers (e.g., holo-TC and MMA), with serum cobalamin as a replacement for holo-TC when the measurement of this latter is unavailable | Oral: 1–2 capsules daily (multivitamin: B1, B2, B3 B5, B6, and B7) |
| HPN and long-term PN: 5 μg/day | |||
| Vitamin C—ascorbic acid (DRI: 90–100 mg/day) | Lassitude; shortness of breath; anemia; poor wound healing; myalgia and bone pain; loose teeth; spongy and purplish gums that are prone to bleeding; bulging eyes; scaly, dry, and brownish skin; dry hair that breaks; edema; petechiae; and easy bruising | Total plasma vitamin C (sum of AA and DHAA) or AA. | Oral: 200–500 mg daily ǂ |
| HPN and long-term PN: 100–200 mg/day | |||
| Fat-soluble vitamins | Doses (all values per day) | ||
| Vitamin A (DRI: 700–900 µg/day) | Night blindness, Bitot spots, foamy appearance on the conjunctiva, xerophthalmia, increased susceptibility to infections, and impairment of the intestinal immune and barrier function | Serum retinol | Oral: 5000–50,000 IU daily # |
| HPN and long-term PN: 800–1100 µg/day | |||
| Vitamin D (DRI: 15–20 µg/day) | Osteomalacia and nutritional rickets; increased susceptibility to infections | Serum 25-hydroxyvitamin D (25(OH)D) | <12 ng/mL: oral: 50,000 IU# once weekly (or calcitriol 0.25–2 mg daily), followed by maintenance:
|
| HPN and long-term PN: 200 IU/5 µg/day | |||
| Vitamin E (DRI: 15 mg/day) | Neurological symptoms (balance and coordination disorders and peripheral neuropathy) and muscle weakness | Serum alpha-tocopherol | Oral: 400 IU up to 3 times daily |
| HPN and long-term PN: 9–10 mg/day | |||
| Vitamin K (DRI: 90–120 µg/day) | Prolongation of prothrombin time with impaired clotting or bleeding, poor bone development, osteoporosis, and increased cardiovascular disease | Combination of biomarkers and dietary intake | Oral: 2.5 to 10 mg twice weekly to daily, or 10-mg single dose #; can be repeated 48–72 h later |
| HPN & long-term PN: 150 µg/day, usually provided by lipid emulsions | |||
| Trace mineral | Doses (all values per day) | ||
| Iron (DRI: 8 mg/day. 18 mg/day for female 19–50 years old) | Microcytic anemia | Serum ferritin, sideremia, and transferrin saturation (%) | Oral: 100–200 mg once daily or every other day # ǂ |
| HPN and long-term PN: 1.1 mg/day | |||
| Copper (DRI: 1.1–2 mg/day) | Microcytic anemia, neutropenia, osteoporosis, hair depigmentation, cardiac arrhythmias, delayed wound healing, and myeloneuropathy | Serum copper | Oral: 2 mg of elemental copper daily ǂ Higher doses may be needed |
| HPN and long-term PN: 0.3–0.5 mg/day- | |||
| Chromium (DRI: 20–35 µg/day) | Hyperglycemia, insulin resistance, elevated plasma fatty acids, weight loss, and peripheral neuropathy | Serum chromium | Oral: 100–200 mg up to 3 times daily |
| HPN and long-term PN: 10–15 µg/day | |||
| Zinc (DRI: 8–11 mg/day) | Impairment of immune defense, reduced growth rate, alopecia, skin rash of the face, groins, hands, and feet, delayed sexual development and bone maturation, impaired wound healing, diarrhea, and blunting of taste and smell | Serum zinc | Oral: 50 mg elemental zinc (once or twice daily) Dietary sources such as oysters and mussels can also be considered |
| HPN and long-term PN: 3–5 mg/day | |||
| Selenium (DRI: 55 µg/day) | Cardiomyopathy, skeletal muscle myopathy, and skin and nail impact | Serum selenium | Oral: 100–200 mg daily |
| HPN and long-term PN: 60–100 µg/day |
| Clinical Condition | Criteria | Comments |
|---|---|---|
| IAFLD | Forthcoming (total bilirubin above 3–6 mg/dL (54–108 μmol/L), progressive thrombocytopenia, and progressive splenomegaly) or overt liver failure (portal hypertension, hepatosplenomegaly, hepatic fibrosis, or cirrhosis because of IFALD). | Liver biopsy is the gold standard test to identify the stage of liver disease, the timing of transplantation, and the type of transplant required (isolated ITx or combined liver–ITx) It has been suggested that patients with METAVIR stage II fibrosis (perisinusoidal and portal/periportal fibrosis) should be considered for an isolated ITx, whereas those with stage III (bringing fibrosis) or IV (cirrhosis) should be considered for LITx. |
| Esophageal varices, ascites, and impaired synthetic function are not always present. | ||
| Central venous catheter-related thrombosis (CRVT) | Thrombosis of two or more central veins (loss of right and left internal jugular vein, right and left subclavian vein, or right and left femoral vein). | CRVT is a severe complication that is responsible for the loss of central venous accesses in patients on HPN and may be an indication for ITx if it affects two or more of the central venous vessels. For adults, this criterion is on a case-by-case basis. |
| Catheter-related bloodstream infection (CRBSI). | Frequent central line sepsis: two or more episodes per year of systemic sepsis secondary to line infections requiring hospitalization; a single episode of line-related fungemia; septic shock and/or acute respiratory distress syndrome. | Children: two admissions to an intensive care unit because of cardiorespiratory failure (mechanical ventilation or inotrope infusion) due to sepsis. For adults, this criterion is on a case-by-case basis, because recurrent episodes of CRBSI have been demonstrated to not be associated with an increased risk of death. |
| Other indications | Refractory electrolyte changes and frequent episodes of dehydration. High risk of death attributable to underlying diseases, such as congenital mucosal disorders, ultra-short bowel syndrome (gastrostomy; duodenostomy; residual small bowel <10 cm in infants and <20 cm in adults), and invasive intra-abdominal desmoid tumors; patients with high morbidity (frequent hospitalization, narcotic dependency, and inability to function (i.e., pseudo-obstruction; high output stoma)) or a low acceptance of long-term PN, especially in young patients. | |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Utrilla Fornals, A.; Costas-Batlle, C.; Medlin, S.; Menjón-Lajusticia, E.; Cisneros-González, J.; Saura-Carmona, P.; Montoro-Huguet, M.A. Metabolic and Nutritional Issues after Lower Digestive Tract Surgery: The Important Role of the Dietitian in a Multidisciplinary Setting. Nutrients 2024, 16, 246. https://doi.org/10.3390/nu16020246
Utrilla Fornals A, Costas-Batlle C, Medlin S, Menjón-Lajusticia E, Cisneros-González J, Saura-Carmona P, Montoro-Huguet MA. Metabolic and Nutritional Issues after Lower Digestive Tract Surgery: The Important Role of the Dietitian in a Multidisciplinary Setting. Nutrients. 2024; 16(2):246. https://doi.org/10.3390/nu16020246
Chicago/Turabian StyleUtrilla Fornals, Alejandra, Cristian Costas-Batlle, Sophie Medlin, Elisa Menjón-Lajusticia, Julia Cisneros-González, Patricia Saura-Carmona, and Miguel A. Montoro-Huguet. 2024. "Metabolic and Nutritional Issues after Lower Digestive Tract Surgery: The Important Role of the Dietitian in a Multidisciplinary Setting" Nutrients 16, no. 2: 246. https://doi.org/10.3390/nu16020246
APA StyleUtrilla Fornals, A., Costas-Batlle, C., Medlin, S., Menjón-Lajusticia, E., Cisneros-González, J., Saura-Carmona, P., & Montoro-Huguet, M. A. (2024). Metabolic and Nutritional Issues after Lower Digestive Tract Surgery: The Important Role of the Dietitian in a Multidisciplinary Setting. Nutrients, 16(2), 246. https://doi.org/10.3390/nu16020246