

Joint Association of Dietary Protein Intake and Eating Habits with the Risk of Gestational Diabetes Mellitus: A Case-Control Study
Abstract
1. Introduction
2. Methods
2.1. Study Participants and Design
2.2. OGTT and Diagnosis of GDM
2.3. Maternal Dietary Assessment
2.4. Maternal Eating Habits
2.5. Covariates
2.6. Statistical Analysis
3. Results
3.1. Characteristics of the Study Population
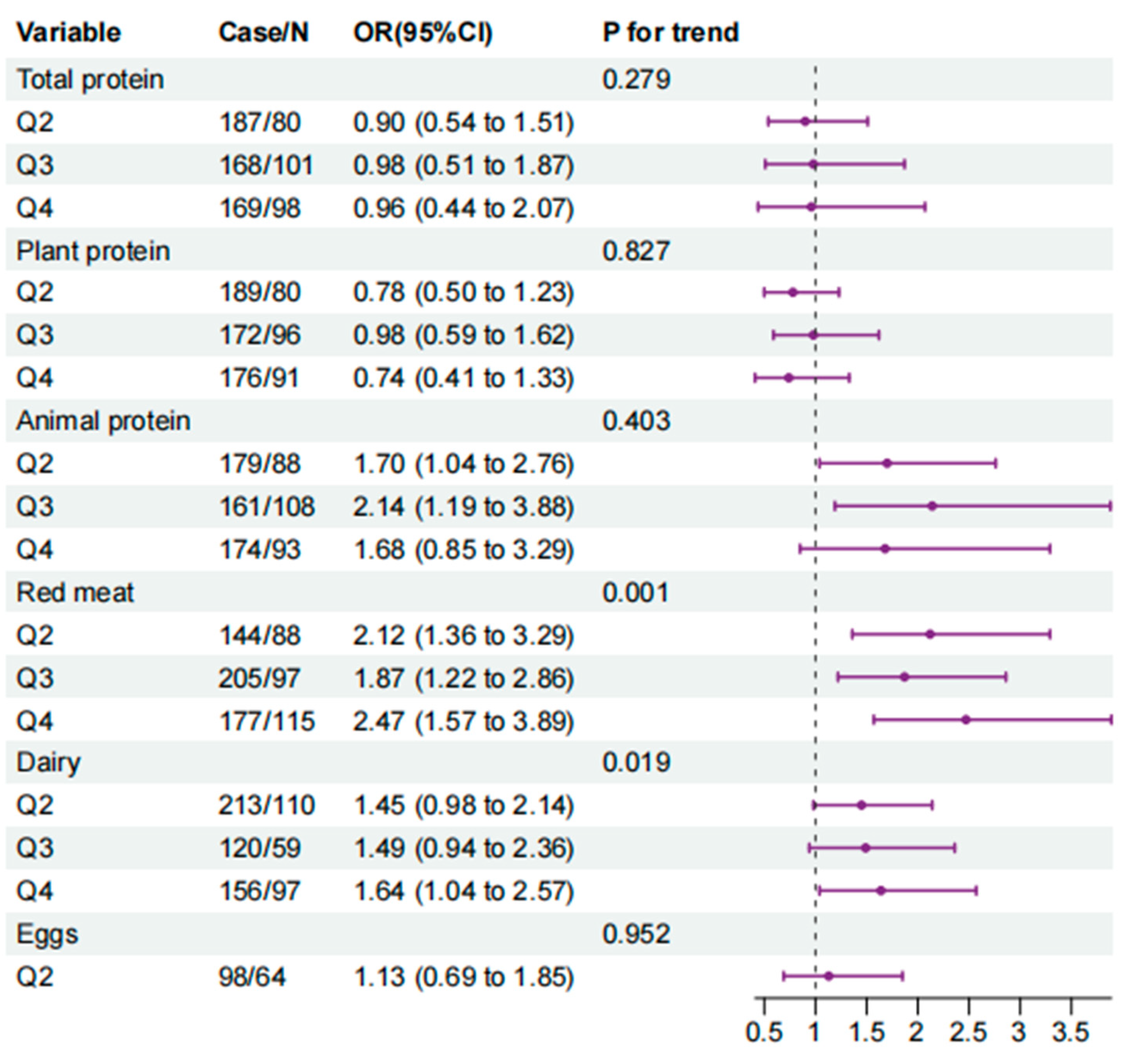
3.2. Associations between Dietary Protein Sources and Odds of GDM
3.3. Eating Habits with the Odds of GDM
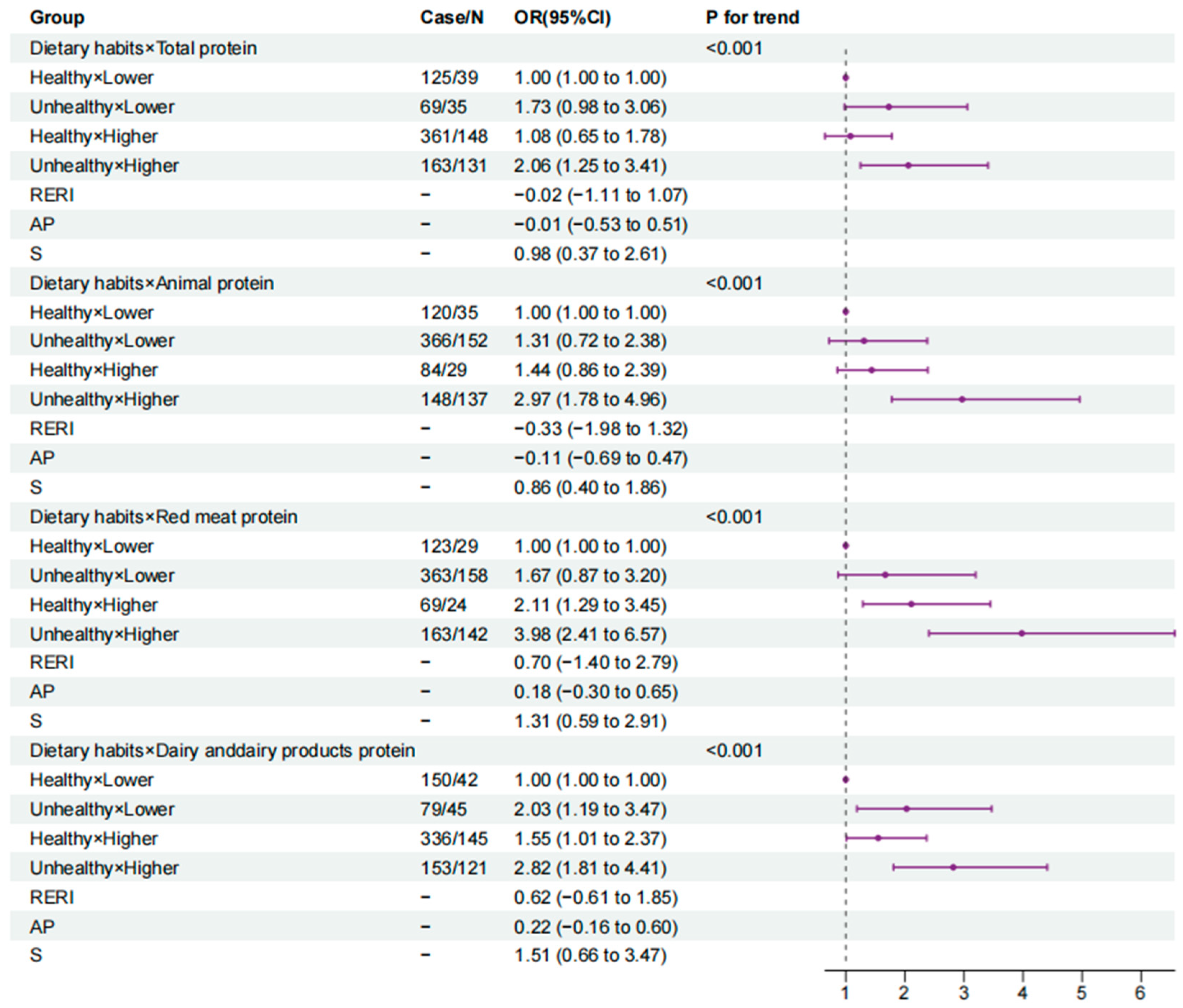
3.4. The Joint Association of Dietary Protein and Eating Habits with the Odds of GDM
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Billionnet, C.; Mitanchez, D.; Weill, A.; Nizard, J.; Alla, F.; Hartemann, A.; Jacqueminet, S. Gestational diabetes and adverse perinatal outcomes from 716,152 births in France in 2012. Diabetologia 2017, 60, 636–644. [Google Scholar] [PubMed]
- Sun, H.; Saeedi, P.; Karuranga, S.; Pinkepank, M.; Ogurtsova, K.; Duncan, B.B.; Stein, C.; Basit, A.; Chan, J.C.; Mbanya, J.C.; et al. IDF Diabetes Atlas: Global, regional and country-level diabetes prevalence estimates for 2021 and projections for 2045. Diabetes Res. Clin. Pract. 2021, 183, 109119. [Google Scholar] [PubMed]
- Li, Y.; Ren, X.; He, L.; Li, J.; Zhang, S.; Chen, W. Maternal age and the risk of gestational diabetes mellitus: A systematic review and meta-analysis of over 120 million participants. Diabetes Res. Clin. Pract. 2020, 162, 108044. [Google Scholar]
- Vounzoulaki, E.; Khunti, K.; Abner, S.C.; Tan, B.K.; Davies, M.J.; Gillies, C.L. Progression to type 2 diabetes in women with a known history of gestational diabetes: Systematic review and meta-analysis. BMJ 2020, 369, m1361. [Google Scholar] [PubMed]
- Westerterp-Plantenga, M.S.; Luscombe-Marsh, N.; Lejeune MP, G.M.; Diepvens, K.; Nieuwenhuizen, A.; Engelen MP, K.J.; Deutz, N.E.P.; Azzout-Marniche, D.; Tome, D.; Westerterp, K.R. Dietary protein, metabolism, and body-weight regulation: Dose-response effects. Int. J. Obes. Relat. Metab. Disord. 2006, 30, S16–S23. [Google Scholar]
- Mittendorfer, B.; Klein, S.; Fontana, L. A word of caution against excessive protein intake. Nat. Rev. Endocrinol. 2020, 16, 59–66. [Google Scholar]
- Rietman, A.; Schwarz, J.; Tome, D.; Kok, F.J.; Mensink, M. High dietary protein intake, reducing or eliciting insulin resistance? Eur. J. Clin. Nutr. 2014, 68, 973–979. [Google Scholar]
- Vasdev, S.; Gill, V.; Singal, P. Role of Advanced Glycation End Products in Hypertension and Atherosclerosis: Therapeutic Implications. Cell Biochem. Biophys. 2007, 49, 48–63. [Google Scholar]
- Ke, Q.; Chen, C.; He, F.; Ye, Y.; Bai, X.; Cai, L.; Xia, M. Association between dietary protein intake and type 2 diabetes varies by dietary pattern. Diabetol. Metab. Syndr. 2018, 10, 48. [Google Scholar]
- Bao, W.; Bowers, K.; Tobias, D.K.; Hu, F.B.; Zhang, C. Prepregnancy dietary protein intake, major dietary protein sources, and the risk of gestational diabetes mellitus: A prospective cohort study. Diabetes Care 2013, 36, 2001–2008. [Google Scholar]
- Pang, W.W.; Colega, M.; Cai, S.; Chan, Y.H.; Padmapriya, N.; Chen, L.-W.; Soh, S.-E.; Han, W.M.; Tan, K.H.; Lee, Y.S.; et al. Higher Maternal Dietary Protein Intake Is Associated with a Higher Risk of Gestational Diabetes Mellitus in a Multiethnic Asian Cohort. J. Nutr. 2017, 147, 653–660. [Google Scholar] [PubMed]
- Liang, Y.; Gong, Y.; Zhang, X.; Yang, D.; Zhao, D.; Quan, L.; Zhou, R.; Bao, W.; Cheng, G. Dietary Protein Intake, Meat Consumption, and Dairy Consumption in the Year Preceding Pregnancy and During Pregnancy and Their Associations with the Risk of Gestational Diabetes Mellitus: A Prospective Cohort Study in Southwest China. Front. Endocrinol. 2018, 9, 596. [Google Scholar] [CrossRef] [PubMed]
- Chen, L.; Du, S.; Song, H.; Chen, J.; Lv, C.; Li, C. The Effect of Dietary Protein Intake on the Risk of Gestational Diabetes. J. Food Qual. 2022, 2022, 8. [Google Scholar] [CrossRef]
- Brasington, N.; Bucher, T.; Beckett, E.L. Correlations between Convenience Cooking Product Use and Vegetable Intake. Nutrients 2022, 14, 848. [Google Scholar] [CrossRef] [PubMed]
- Garcidueñas-Fimbres, T.E.; Paz-Graniel, I.; Nishi, S.K.; Salas-Salvadó, J.; Babio, N. Eating Speed, Eating Frequency, and Their Relationships with Diet Quality, Adiposity, and Metabolic Syndrome, or Its Components. Nutrients 2021, 13, 1687. [Google Scholar] [CrossRef]
- Volta, U.; Pinto-Sanchez, M.I.; Boschetti, E.; Caio, G.; De Giorgio, R.; Verdu, E.F. Dietary Triggers in Irritable Bowel Syndrome: Is There a Role for Gluten? J. Neurogastroenterol. Motil. 2016, 22, 547–557. [Google Scholar] [CrossRef]
- Chapman-Kiddell, C.A.; Davies, P.S.W.; Gillen, L.; Radford-Smith, G.L. Role of diet in the development of inflammatory bowel disease. Inflamm. Bowel Dis. 2010, 16, 137–151. [Google Scholar] [CrossRef]
- Tucker, D.M.; Sandstead, H.H.; Logan, G.M.J.; Klevay, L.M.; Mahalko, J.; Johnson, L.K.; Inman, L.; Inglett, G.E. Dietary fiber and personality factors as determinants of stool output. Gastroenterology 1981, 81, 879–883. [Google Scholar] [CrossRef]
- Duncanson, K.R.; Talley, N.J.; Walker, M.M.; Burrows, T.L. Food and functional dyspepsia: A systematic review. J. Hum. Nutr. Diet. 2018, 31, 390–407. [Google Scholar] [CrossRef]
- Dong, J.-Y.; Ikehara, S.; Kimura, T.; Cui, M.; Kawanishi, Y.; Kimura, T.; Ueda, K.; Iso, H.; The Japan Environment and Children’s Study Group. Self-Reported Eating Speed and Incidence of Gestational Diabetes Mellitus: The Japan Environment and Children’s Study. Nutrients 2020, 12, 1296. [Google Scholar] [CrossRef]
- Metzger, B.E.; Gabbe, S.G.; Persson, B.; Lowe, L.P.; Dyer, A.R.; Oats, J.J.N.; Buchanan, T.A. International association of diabetes and pregnancy study groups recommendations on the diagnosis and classification of hyperglycemia in pregnancy. Diabetes Care 2010, 33, 676–682. [Google Scholar] [CrossRef] [PubMed]
- Zhang, H.; Qiu, X.; Zhong, C.; Zhang, K.; Xiao, M.; Yi, N.; Xiong, G.; Wang, J.; Yao, J.; Hao, L.; et al. Reproducibility and relative validity of a semi-quantitative food frequency questionnaire for Chinese pregnant women. Nutr. J. 2015, 14, 56. [Google Scholar] [CrossRef] [PubMed]
- Yang, Y.; Wang, G.; Pan, X. China Food Composition, 2nd ed.; Beijing Medical University Publishing House: Beijing, China, 2009. [Google Scholar]
- Fan, M.Y.; Lv, J.; He, P.P. Chinese guidelines for data processing and analysis concerning the International Physical Activity Questionnaire. Chin. J. Epidemiol. 2014, 35, 961–964. [Google Scholar]
- Andersson, T.; Alfredsson, L.; Källberg, H.; Zdravkovic, S.; Ahlbom, A. Calculating measures of biological interaction. Eur. J. Epidemiol. 2005, 20, 575–579. [Google Scholar] [CrossRef] [PubMed]
- Wu, Z.; Heng, J.; Tian, M.; Song, H.; Chen, F.; Guan, W.; Zhang, S. Amino acid transportation, sensing and signal transduction in the mammary gland: Key molecular signalling pathways in the regulation of milk synthesis. Nutr. Res. Rev. 2020, 33, 287–297. [Google Scholar] [CrossRef]
- Hertzler, S.R.; Lieblein-Boff, J.C.; Weiler, M.; Allgeier, C. Plant Proteins: Assessing Their Nutritional Quality and Effects on Health and Physical Function. Nutrients 2020, 12, 3704. [Google Scholar]
- Reddy, P.; Elkins, A.; Panozzo, J.; Rochfort, S.J. High-Throughput Analysis of Amino Acids for Protein Quantification in Plant and Animal-Derived Samples Using High Resolution Mass Spectrometry. Molecules 2021, 26, 7578. [Google Scholar] [CrossRef]
- White, P.J.; McGarrah, R.W.; Herman, M.A.; Bain, J.R.; Shah, S.H.; Newgard, C.B. Insulin action, type 2 diabetes, and branched-chain amino acids: A two-way street. Mol. Metab. 2021, 52, 101261. [Google Scholar]
- Zhou, M.; Shao, J.; Wu, C.-Y.; Shu, L.; Dong, W.; Liu, Y.; Chen, M.; Wynn, R.M.; Wang, J.; Wang, J.; et al. Targeting BCAA Catabolism to Treat Obesity-Associated Insulin Resistance. Diabetes 2019, 68, 1730–1746. [Google Scholar]
- Nie, C.; He, T.; Zhang, W.; Zhang, G.; Ma, X. Branched Chain Amino Acids: Beyond Nutrition Metabolism. Int. J. Mol. Sci. 2018, 19, 954. [Google Scholar] [CrossRef]
- Xu, L.; Lin, X.; Li, X.; Hu, Z.; Hou, Q.; Wang, Y.; Wang, Z. Integration of transcriptomics and metabolomics provides metabolic and functional insights into reduced insulin secretion in MIN6 beta-cells exposed to deficient and excessive arginine. FASEB J. 2022, 36, e22206. [Google Scholar] [PubMed]
- Halperin, F.; Mezza, T.; Li, P.; Shirakawa, J.; Kulkarni, R.N.; Goldfine, A.B. Insulin regulates arginine-stimulated insulin secretion in humans. Metabolism 2022, 128, 155117. [Google Scholar] [CrossRef] [PubMed]
- Würtz, A.M.L.; Jakobsen, M.U.; Bertoia, M.L.; Hou, T.; Schmidt, E.B.; Willett, W.C.; Overvad, K.; Sun, Q.; Manson, J.E.; Hu, F.B.; et al. Replacing the consumption of red meat with other major dietary protein sources and risk of type 2 diabetes mellitus: A prospective cohort study. Am. J. Clin. Nutr. 2021, 113, 612–621. [Google Scholar] [CrossRef] [PubMed]
- Aune, D.; Norat, T.; Romundstad, P.; Vatten, L.J. Dairy products and the risk of type 2 diabetes: A systematic review and dose-response meta-analysis of cohort studies. Am. J. Clin. Nutr. 2013, 98, 1066–1083. [Google Scholar] [CrossRef] [PubMed]
- Gao, D.; Ning, N.; Wang, C.; Wang, Y.; Li, Q.; Meng, Z.; Liu, Y.; Li, Q. Dairy products consumption and risk of type 2 diabetes: Systematic review and dose-response meta-analysis. PLoS ONE 2013, 8, e73965. [Google Scholar]
- Gholami, F.; Khoramdad, M.; Shakiba, E.; Alimohamadi, Y.; Shafiei, J.; Firouzi, A. Subgroup dairy products consumption on the risk of stroke and CHD: A systematic review and meta-analysis. Med. J. Islam. Repub. Iran 2017, 31, 143–149. [Google Scholar] [CrossRef][Green Version]
- Elbalshy, M.M.; Reynolds, A.N.; Mete, E.; Robinson, C.; Oey, I.; Silcock, P.; Haszard, J.J.; Perry, T.L.; Perry, J.; Morenga, L. Gelatinisation and milling whole-wheat increases postprandial blood glucose: Randomised crossover study of adults with type 2 diabetes. Diabetologia 2021, 64, 1385–1388. [Google Scholar]
- Reynolds, A.N.; Mann, J.; Elbalshy, M.; Mete, E.; Robinson, C.; Oey, I.; Silcock, P.; Downes, N.; Perry, T.; Te Morenga, L. Wholegrain Particle Size Influences Postprandial Glycemia in Type 2 Diabetes: A Randomized Crossover Study Comparing Four Wholegrain Breads. Diabetes Care 2019, 43, 476–479. [Google Scholar] [CrossRef]
- Collings, P.; Williams, C.; MacDonald, I. Effects of cooking on serum glucose and insulin responses to starch. Br. Med. J. 1981, 282, 1032. [Google Scholar]
- Jung, E.Y.; Suh, H.J.; Hong, W.S.; Kim, D.G.; Hong, Y.H.; Hong, I.S.; Chang, U.J. Uncooked rice of relatively low gelatinization degree resulted in lower metabolic glucose and insulin responses compared with cooked rice in female college students. Nutr. Res. 2009, 29, 457–461. [Google Scholar] [CrossRef]
- Andrici, J.; Eslick, G.D. Hot Food and Beverage Consumption and the Risk of Esophageal Cancer: A Meta-Analysis. Am. J. Prev. Med. 2015, 49, 952–960. [Google Scholar] [PubMed]
- Tang, L.; Xu, F.; Zhang, T.; Lei, J.; Binns, C.W.; Lee, A.H.-W. High Temperature of Food and Beverage Intake Increases the Risk of Oesophageal Cancer in Xinjiang, China. Asian Pac. J. Cancer Prev. 2013, 14, 5085–5088. [Google Scholar] [CrossRef] [PubMed][Green Version]
- Abedi-Ardekani, B.; Kamangar, F.; Sotoudeh, M.; Villar, S.; Islami, F.; Aghcheli, K.; Nasrollahzadeh, D.; Taghavi, N.; Dawsey, S.M.; Abnet, C.C.; et al. Extremely High Tp53 Mutation Load in Esophageal Squamous Cell Carcinoma in Golestan Province, Iran. PLoS ONE 2011, 6, e29488. [Google Scholar]



{kind=link}
{kind=link}
| Characteristic | Total (n = 1071) | Protein Intake Quartiles | p-Value b | |||
|---|---|---|---|---|---|---|
| Q1 (n = 268) | Q2 (n = 267) | Q3 (n = 269) | Q4 (n = 267) | |||
| Age (years) | 30.90 ± 3.93 | 30.37 ± 4.06 | 30.99 ± 3.63 | 31.06 ± 4.00 | 31.16 ± 4.02 | 0.086 |
| Pre-pregnancy BMI | 22.42 ± 3.82 | 22.85 ± 3.79 | 22.25 ± 3.69 | 22.13 ± 3.57 | 22.46 ± 4.18 | 0.140 |
| Ethnicity | 0.369 | |||||
| Han | 1052 (98.2) | 260 (97.0) | 264 (98.9) | 265 (98.5) | 263 (98.5) | |
| Other | 19 (1.8) | 8 (3.0) | 3 (1.1) | 4 (1.5) | 4 (1.5) | |
| Marital Status | 0.193 | |||||
| Married | 1059 (98.9) | 264 (98.5) | 267 (100.0) | 266 (98.9) | 262 (98.1) | |
| Unmarried or other | 12 (1.1) | 4 (1.5) | 0 (0.0) | 3 (1.1) | 5 (1.9) | |
| Annual household income (CNY) | 0.190 | |||||
| <50,000 | 159 (14.9) | 50 (18.7) | 33 (12.4) | 37 (13.8) | 39 (14.6) | |
| 50,000~99,900 | 369 (34.5) | 99 (37.1) | 96 (36.0) | 81 (30.1) | 93 (34.8) | |
| 100,000~199,900 | 387 (36.2) | 90 (33.7) | 93 (34.8) | 107 (39.8) | 97 (36.3) | |
| ≥200,000 | 155 (14.5) | 28 (10.5) | 45 (16.9) | 44 (16.4) | 38 (14.2) | |
| Education status | 0.826 | |||||
| Middle school and below | 176 (16.4) | 50 (18.7) | 46 (17.2) | 42 (15.6) | 38 (14.2) | |
| High school or technical secondary college | 223 (20.8) | 58 (21.6) | 52 (19.5) | 58 (21.6) | 55 (20.6) | |
| Junior college or regular college | 672 (62.7) | 160 (59.7) | 169 (63.3) | 169 (62.8) | 174 (65.2) | |
| Working Status | 0.296 | |||||
| Brain-based work | 585 (54.6) | 134 (50.0) | 159 (59.6) | 144 (53.5) | 148 (55.4) | |
| Physical-based work | 69 (6.4) | 18 (6.7) | 13 (4.9) | 16 (5.9) | 22 (8.2) | |
| Currently not working | 417 (38.9) | 116 (43.3) | 95 (35.6) | 109 (40.5) | 97 (36.3) | |
| Smoking | 0.266 | |||||
| Yes | 40 (3.7) | 14 (5.2) | 7 (2.6) | 7 (2.6) | 12 (4.5) | |
| No | 1031 (96.3) | 254 (94.8) | 260 (97.4) | 262 (97.4) | 255 (95.5) | |
| Drinking | 0.024 | |||||
| Yes | 172 (16.1) | 58 (21.6) | 42 (15.7) | 39 (14.5) | 33 (12.4) | |
| No | 899 (83.9) | 210 (78.4) | 225 (84.3) | 230 (85.5) | 234 (87.6) | |
| Age of menarche (years) | 0.801 | |||||
| 8~11 | 33 (3.1) | 7 (2.6) | 13 (4.9) | 8 (3.0) | 5 (1.9) | |
| 12 | 207 (19.3) | 58 (21.6) | 48 (18.0) | 53 (19.7) | 48 (18.0) | |
| 13 | 289 (27.0) | 68 (25.4) | 76 (28.5) | 68 (25.3) | 77 (28.8) | |
| 14 | 257 (24.0) | 64 (23.9) | 64 (24.0) | 62 (23.0) | 67 (25.1) | |
| ≥15 | 285 (26.6) | 71 (26.5) | 66 (24.7) | 78 (29.0) | 70 (26.2) | |
| Conception Season | <0.001 | |||||
| Spring | 287 (26.8) | 92 (34.3) | 84 (31.5) | 71 (26.4) | 40 (15.0) | |
| Autumn | 166 (15.5) | 53 (19.8) | 50 (18.7) | 41 (15.2) | 22 (8.2) | |
| Summer | 154 (14.4) | 30 (11.2) | 31 (11.6) | 34 (12.6) | 59 (22.1) | |
| Winter | 464 (43.3) | 93 (34.7) | 102 (38.2) | 123 (45.7) | 146 (54.7) | |
| Adverse maternal history | 0.069 | |||||
| No | 922 (86.1) | 242 (90.3) | 230 (86.1) | 230 (85.5) | 220 (82.4) | |
| Yes | 149 (13.9) | 26 (9.7) | 37 (13.9) | 39 (14.5) | 47 (17.6) | |
| Family history of diabetes | 0.236 | |||||
| No | 792 (73.9) | 195 (72.8) | 209 (78.3) | 192 (71.4) | 196 (73.4) | |
| Yes | 228 (21.3) | 56 (20.9) | 50 (18.7) | 60 (22.3) | 62 (23.2) | |
| Unclear | 51 (4.8) | 17 (6.3) | 8 (3.0) | 17 (6.3) | 9 (3.4) | |
| Family history of cardiovascular disease | 0.656 | |||||
| No | 833 (77.8) | 209 (78.0) | 201 (75.3) | 218 (81.0) | 205 (76.8) | |
| Yes | 175 (16.3) | 41 (15.3) | 50 (18.7) | 36 (13.4) | 48 (18.0) | |
| Unclear | 63 (5.9) | 18 (6.7) | 16 (6.0) | 15 (5.6) | 14 (5.2) | |
| Physical activity | 0.007 | |||||
| Low | 211 (19.7) | 52 (19.4) | 59 (22.1) | 52 (19.3) | 48 (18.0) | |
| Medium | 562 (52.5) | 119 (44.4) | 146 (54.7) | 140 (52.0) | 157 (58.8) | |
| High | 298 (27.8) | 97 (36.2) | 62 (23.2) | 77 (28.6) | 62 (23.2) | |
| Sleep quality | 0.141 | |||||
| Excellent | 19 (1.8) | 2 (0.7) | 6 (2.2) | 6 (2.2) | 5 (1.9) | |
| Good | 129 (12.0) | 34 (12.7) | 37 (13.9) | 38 (14.1) | 20 (7.5) | |
| Average | 923 (86.2) | 232 (86.6) | 224 (83.6) | 225 (83.6) | 242 (90.6) | |
| Nutrients | Total | GDM | Control | p Value a |
|---|---|---|---|---|
| (n = 1071) | (n = 353) | (n = 718) | ||
| Protein, g/day | ||||
| Total protein | 71.13 ± 26.66 | 73.52 ± 25.95 | 69.95 ± 26.94 | 0.040 |
| Plant protein | 30.65 ± 28.22 | 30.78 ± 13.75 | 30.59 ± 14.17 | 0.831 |
| Animal protein | 40.48 ± 20.29 | 42.74 ± 20.52 | 39.37 ± 20.10 | 0.011 |
| Protein sources | ||||
| Plant protein, g/day | ||||
| From grains | 21.43 ± 20.22 | 20.99 ± 8.55 | 21.65 ± 10.46 | 0.304 |
| From beans | 6.42 ± 4.00 | 6.95 ± 9.81 | 6.15 ± 7.87 | 0.151 |
| From nuts | 1.42 ± 1.03 | 1.44 ± 1.53 | 1.42 ± 1.56 | 0.840 |
| From soy milk | 1.38 ± 1.03 | 1.40 ± 1.67 | 1.37 ± 1.58 | 0.734 |
| Animal protein, g/day | ||||
| From red meat | 12.01 ± 11.50 | 12.90 ± 11.04 | 11.57 ± 11.70 | 0.075 |
| From poultry | 5.21 ± 2.86 | 5.24 ± 8.61 | 5.19 ± 7.53 | 0.916 |
| From eggs | 6.54 ± 6.65 | 6.95 ± 3.55 | 6.34 ± 4.04 | 0.017 |
| From dairy products | 7.41 ± 7.50 | 7.99 ± 4.58 | 7.13 ± 4.50 | 0.004 |
| From fish | 5.08 ± 2.53 | 5.26 ± 6.82 | 4.98 ± 6.56 | 0.519 |
| From shrimp | 4.25 ± 2.60 | 4.42 ± 4.92 | 4.16 ± 5.04 | 0.424 |
| Eating Habits | GDM (n = 353) | Model One | Model Two | Model Three |
|---|---|---|---|---|
| Food temperature | ||||
| Moderate | 272 (77.1) | 1.00 | 1.00 | 1.00 |
| Hot | 54 (15.3) | 2.14 (1.44, 3.20) | 2.16 (1.41, 3.31) | 1.72 (1.12, 2.66) |
| Cold | 27 (7.6) | 1.03 (0.64, 1.67) | 0.87 (0.52, 1.46) | 070 (0.41, 1.18) |
| Firmness | ||||
| Moderate | 209 (59.2) | 1.00 | 1.00 | 1.00 |
| Firm | 67 (19.0) | 1.78 (1.25, 2.54) | 1.82 (1.25, 2.65) | 1.71 (1.17, 2.51) |
| Soft | 77 (21.8) | 1.64 (1.18, 2.28) | 1.63 (1.14, 2.33) | 1.47 (1.04, 2.15) |
| Eating speed | ||||
| Moderate | 227 (64.3) | 1.00 | 1.00 | 1.00 |
| Fast | 90 (25.5) | 1.46 (1.07, 1.99) | 1.41 (1.01, 1.96) | 1.24 (0.88, 1.74) |
| Slow | 36 (10.2) | 0.84 (0.56, 1.28) | 0.96 (0.62, 1.49) | 0.84 (0.54, 1.31) |
| Group | Total (n = 1071) | GDM (n = 353) | Model One | Model Two | p for Trend |
|---|---|---|---|---|---|
| Cumulative score for three diabetes habits | <0.001 | ||||
| 0 | 673 (62.8) | 187 (53.0) | 1.00 | 1.00 | |
| 1 | 335 (31.3) | 134 (38.0) | 1.81 (1.38, 2.38) | 1.73 (1.29, 2.33) | |
| 2 | 63 (5.9) | 32 (9.1) | 2.81 (1.67, 4.73) | 2.88 (1.65, 5.04) |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Gong, K.; Xie, L.; Cao, Y.; Yu, X.; Qiang, W.; Fan, T.; Zhu, T.; Liu, J.; Tao, F.; Zhu, B. Joint Association of Dietary Protein Intake and Eating Habits with the Risk of Gestational Diabetes Mellitus: A Case-Control Study. Nutrients 2023, 15, 4332. https://doi.org/10.3390/nu15204332
Gong K, Xie L, Cao Y, Yu X, Qiang W, Fan T, Zhu T, Liu J, Tao F, Zhu B. Joint Association of Dietary Protein Intake and Eating Habits with the Risk of Gestational Diabetes Mellitus: A Case-Control Study. Nutrients. 2023; 15(20):4332. https://doi.org/10.3390/nu15204332
Chicago/Turabian StyleGong, Kexin, Lanci Xie, Yidan Cao, Xiayan Yu, Wenjing Qiang, Tuyan Fan, Tianli Zhu, Jingjing Liu, Fangbiao Tao, and Beibei Zhu. 2023. "Joint Association of Dietary Protein Intake and Eating Habits with the Risk of Gestational Diabetes Mellitus: A Case-Control Study" Nutrients 15, no. 20: 4332. https://doi.org/10.3390/nu15204332
APA StyleGong, K., Xie, L., Cao, Y., Yu, X., Qiang, W., Fan, T., Zhu, T., Liu, J., Tao, F., & Zhu, B. (2023). Joint Association of Dietary Protein Intake and Eating Habits with the Risk of Gestational Diabetes Mellitus: A Case-Control Study. Nutrients, 15(20), 4332. https://doi.org/10.3390/nu15204332