


Mid-Term Evolution of the Serum Acylcarnitine Profile in Critically Ill Survivors: A Metabolic Insight into Survivorship
 ,
,
Abstract
:1. Introduction
2. Materials and Methods
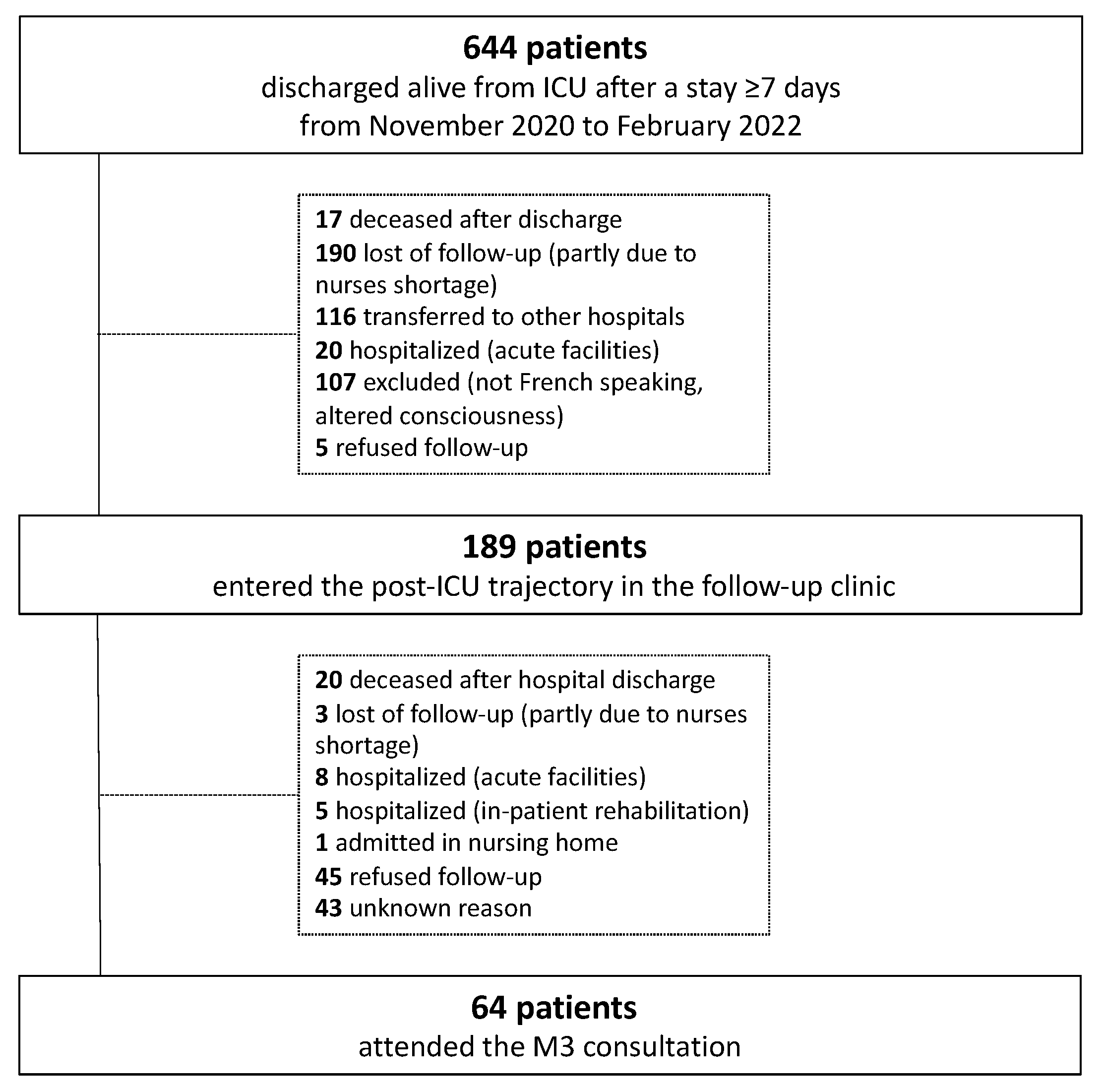
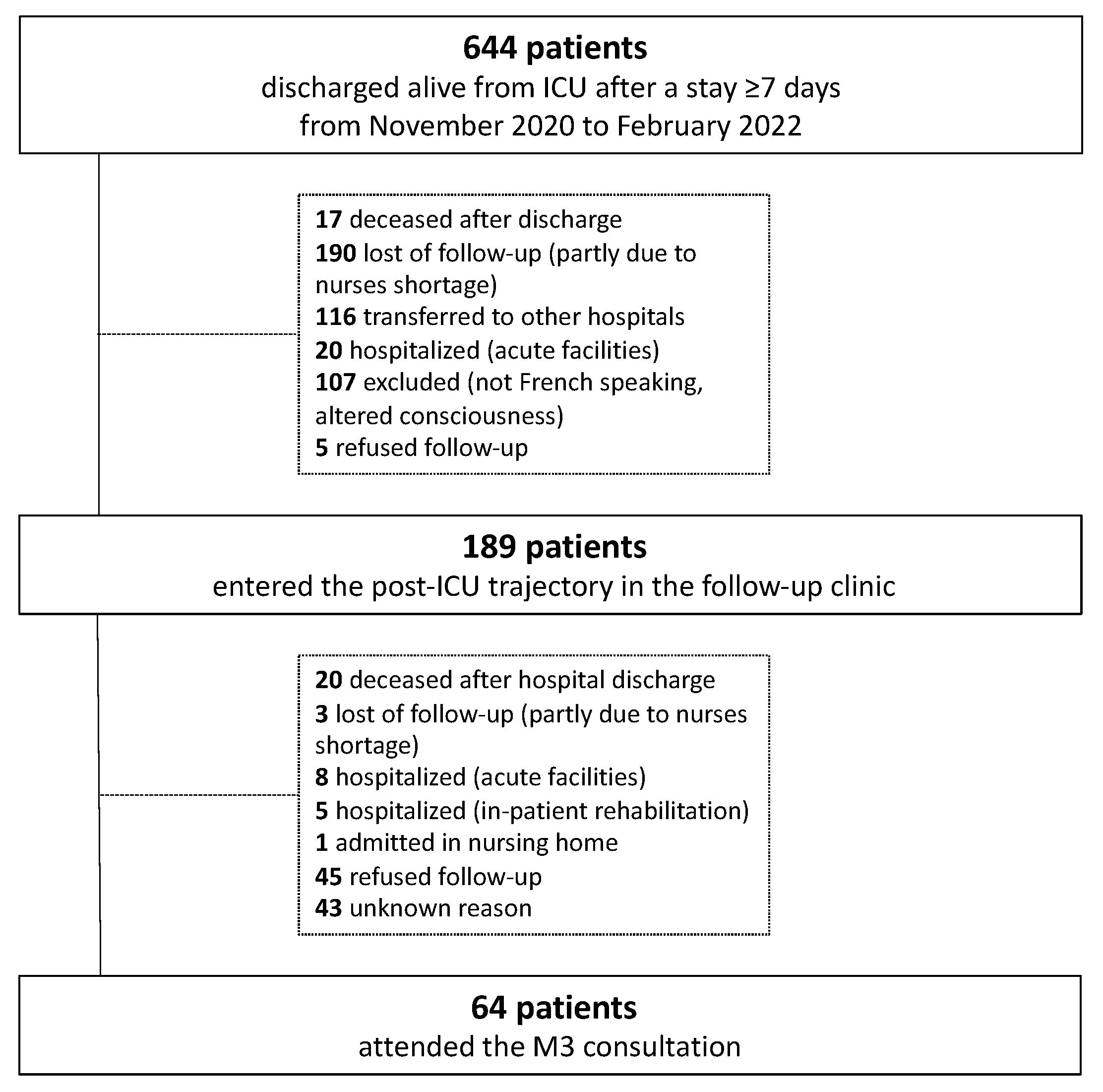
2.1. Patients
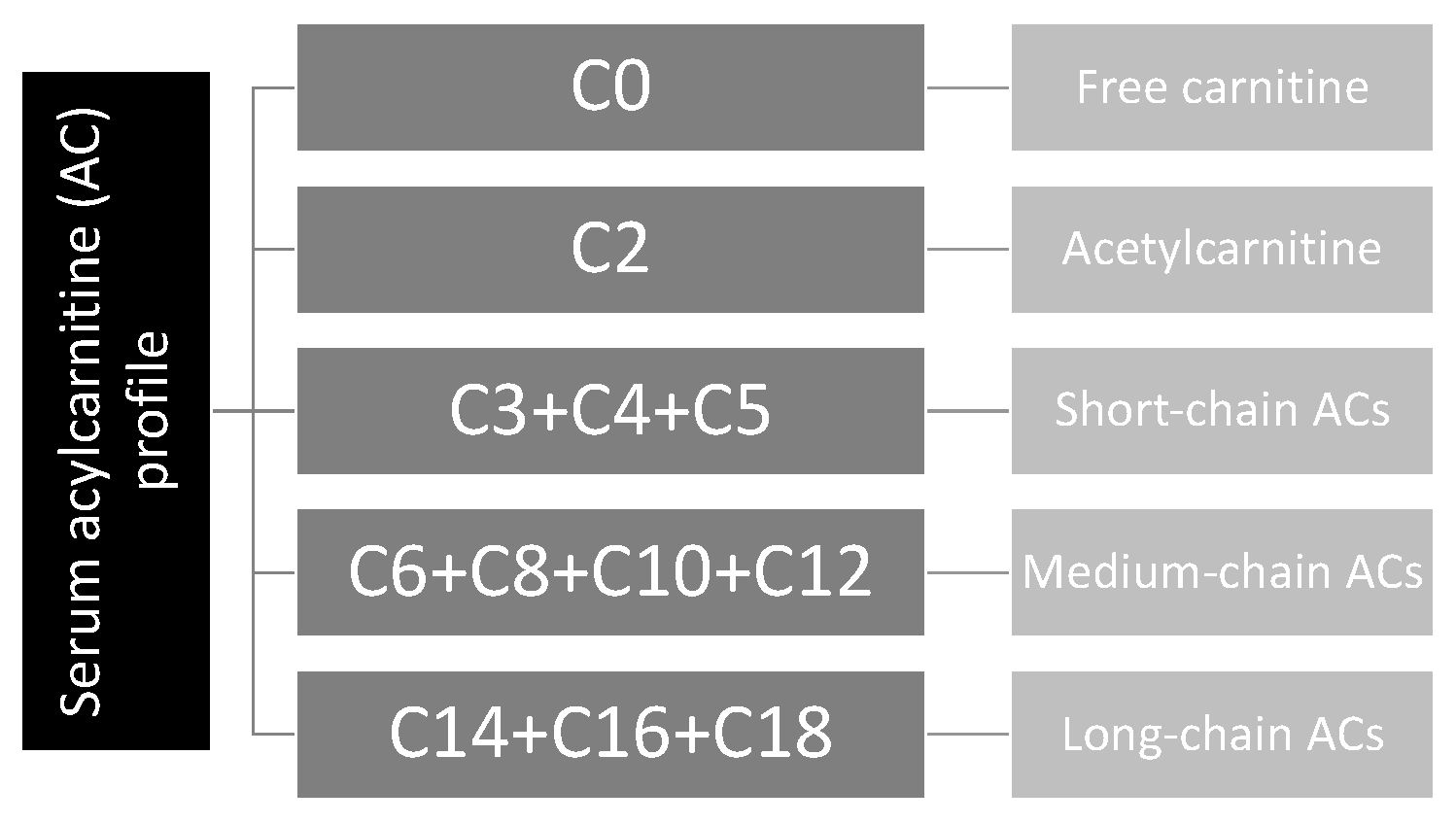
2.2. Serum Acylcarnitine Profiling
2.3. Other Data
2.4. Analysis
3. Results
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Rousseau, A.F.; Prescott, H.C.; Brett, S.J.; Weiss, B.; Azoulay, E.; Creteur, J.; Latronico, N.; Hough, C.L.; Weber-Carstens, S.; Vincent, J.L.; et al. Long-term outcomes after critical illness: Recent insights. Crit. Care 2021, 25, 108. [Google Scholar] [CrossRef] [PubMed]
- Rousseau, A.F.; Colson, C.; Minguet, P.; Kellens, I.; Collard, M.; Vancraybex, C.; Guiot, J.; Lambermont, B.; Misset, B. Characteristics of Mid-Term Post-Intensive Care Syndrome in Patients Attending a Follow-Up Clinic: A Prospective Comparison Between COVID-19 and Non-COVID-19 Survivors. Crit. Care Explor. 2023, 5, e0850. [Google Scholar] [CrossRef] [PubMed]
- Pfoh, E.R.; Wozniak, A.W.; Colantuoni, E.; Dinglas, V.D.; Mendez-Tellez, P.A.; Shanholtz, C.; Ciesla, N.D.; Pronovost, P.J.; Needham, D.M. Physical declines occurring after hospital discharge in ARDS survivors: A 5-year longitudinal study. Intensive Care Med. 2016, 42, 1557–1566. [Google Scholar] [CrossRef]
- Cavalleri, J.; Treguier, D.; Deliege, T.; Gurdebeke, C.; Ernst, M.; Lambermont, B.; Misset, B.; Rousseau, A.F. One-Year Functional Decline in COVID-19 and Non-COVID-19 Critically Ill Survivors: A Prospective Study Incorporating a Pre-ICU Status Assessment. Healthcare 2022, 10, 2023. [Google Scholar] [CrossRef] [PubMed]
- Vanhorebeek, I.; Latronico, N.; Van den Berghe, G. ICU-acquired weakness. Intensive Care Med. 2020, 46, 637–653. [Google Scholar] [CrossRef]
- Lad, H.; Saumur, T.M.; Herridge, M.S.; Dos Santos, C.C.; Mathur, S.; Batt, J.; Gilbert, P.M. Intensive Care Unit-Acquired Weakness: Not just Another Muscle Atrophying Condition. Int. J. Mol. Sci. 2020, 21, 7840. [Google Scholar] [CrossRef] [PubMed]
- Longo, N.; Frigeni, M.; Pasquali, M. Carnitine transport and fatty acid oxidation. Biochim. Biophys. Acta 2016, 1863, 2422–2435. [Google Scholar]
- Reuter, S.E.; Evans, A.M. Carnitine and acylcarnitines: Pharmacokinetic, pharmacological and clinical aspects. Clin. Pharmacokinet. 2012, 51, 553–572. [Google Scholar]
- McCann, M.R.; George De la Rosa, M.V.; Rosania, G.R.; Stringer, K.A. L-Carnitine and Acylcarnitines: Mitochondrial Biomarkers for Precision Medicine. Metabolites 2021, 11, 51. [Google Scholar] [CrossRef]
- Bonafe, L.; Berger, M.M.; Que, Y.A.; Mechanick, J.I. Carnitine deficiency in chronic critical illness. Curr. Opin. Clin. Nutr. Metab. Care 2014, 17, 200–209. [Google Scholar] [CrossRef]
- Berger, M.M.; Broman, M.; Forni, L.; Ostermann, M.; De Waele, E.; Wischmeyer, P.E. Nutrients and micronutrients at risk during renal replacement therapy: A scoping review. Curr. Opin. Crit. Care 2021, 27, 367–377. [Google Scholar] [CrossRef]
- Moonen, H.; Van Zanten, A.R.H. Mitochondrial dysfunction in critical illness during acute metabolic stress and convalescence: Consequences for nutrition therapy. Curr. Opin. Crit. Care 2020, 26, 346–354. [Google Scholar] [CrossRef] [PubMed]
- Owen, A.M.; Patel, S.P.; Smith, J.D.; Balasuriya, B.K.; Mori, S.F.; Hawk, G.S.; Stromberg, A.J.; Kuriyama, N.; Kaneki, M.; Rabchevsky, A.G.; et al. Chronic muscle weakness and mitochondrial dysfunction in the absence of sustained atrophy in a preclinical sepsis model. eLife 2019, 8, e49920. [Google Scholar]
- Mart, M.F.; Ely, E.W.; Tolle, J.J.; Patel, M.B.; Brummel, N.E. Physiologic responses to exercise in survivors of critical illness: An exploratory pilot study. Intensive Care Med. Exp. 2022, 10, 35. [Google Scholar] [CrossRef]
- Joris, M.; Pincemail, J.; Colson, C.; Joris, J.; Calmes, D.; Cavalier, E.; Misset, B.; Guiot, J.; Minguet, G.; Rousseau, A.F. Exercise Limitation after Critical Versus Mild COVID-19 Infection: A Metabolic Perspective. J. Clin. Med. 2022, 11, 4322. [Google Scholar] [CrossRef]
- Rousseau, A.F.; Schmitz, S.; Cavalier, E.; Misset, B.; Boemer, F. Altered Serum Acylcarnitines Profile after a Prolonged Stay in Intensive Care. Nutrients 2022, 14, 1122. [Google Scholar] [CrossRef] [PubMed]
- Rousseau, A.F.; Dongier, A.; Colson, C.; Minguet, P.; Defraigne, J.O.; Minguet, G.; Misset, B.; Boemer, F. Serum Acylcarnitines Profile in Critically Ill Survivors According to Illness Severity and ICU Length of Stay: An Observational Study. Nutrients 2023, 15, 2392. [Google Scholar] [CrossRef] [PubMed]
- Haines, R.W.; Zolfaghari, P.; Wan, Y.; Pearse, R.M.; Puthucheary, Z.; Prowle, J.R. Elevated urea-to-creatinine ratio provides a biochemical signature of muscle catabolism and persistent critical illness after major trauma. Intensive Care Med. 2019, 45, 1718–1731. [Google Scholar] [CrossRef] [PubMed]
- Kashani, K.B.; Frazee, E.N.; Kukralova, L.; Sarvottam, K.; Herasevich, V.; Young, P.M.; Kashyap, R.; Lieske, J.C. Evaluating Muscle Mass by Using Markers of Kidney Function: Development of the Sarcopenia Index. Crit. Care Med. 2017, 45, e23–e29. [Google Scholar] [CrossRef]
- Rousseau, A.F.; Lucania, S.; Fadeur, M.; Verbrugge, A.M.; Cavalier, E.; Colson, C.; Misset, B. Adequacy of Nutritional Intakes during the Year after Critical Illness: An Observational Study in a Post-ICU Follow-Up Clinic. Nutrients 2022, 14, 3797. [Google Scholar] [CrossRef] [PubMed]
- Alhasaniah, A.H. l-carnitine: Nutrition, pathology, and health benefits. Saudi J. Biol. Sci. 2023, 30, 103555. [Google Scholar]
- Rogers, A.J.; McGeachie, M.; Baron, R.M.; Gazourian, L.; Haspel, J.A.; Nakahira, K.; Fredenburgh, L.E.; Hunninghake, G.M.; Raby, B.A.; Matthay, M.A.; et al. Metabolomic derangements are associated with mortality in critically ill adult patients. PLoS ONE 2014, 9, e87538. [Google Scholar] [CrossRef] [PubMed]
- Chung, K.P.; Chen, G.Y.; Chuang, T.Y.; Huang, Y.T.; Chang, H.T.; Chen, Y.F.; Liu, W.L.; Chen, Y.J.; Hsu, C.L.; Huang, M.T.; et al. Increased Plasma Acetylcarnitine in Sepsis Is Associated With Multiple Organ Dysfunction and Mortality: A Multicenter Cohort Study. Crit. Care Med. 2019, 47, 210–218. [Google Scholar] [CrossRef] [PubMed]
- Yahyapoor, F.; Sedaghat, A.; Feizi, A.; Bagherniya, M.; Pahlavani, N.; Khadem-Rezaiyan, M.; Safarian, M.; Islam, M.S.; Zarifi, S.H.; Arabi, S.M.; et al. The effects of l-Carnitine supplementation on inflammatory markers, clinical status, and 28 days mortality in critically ill patients: A double-blind, randomized, placebo-controlled trial. Clin. Nutr. ESPEN 2022, 49, 61–67. [Google Scholar] [CrossRef] [PubMed]
- Haghighatdoost, F.; Jabbari, M.; Hariri, M. The effect of L-carnitine on inflammatory mediators: A systematic review and meta-analysis of randomized clinical trials. Eur. J. Clin. Pharmacol. 2019, 75, 1037–1046. [Google Scholar] [CrossRef] [PubMed]
- Chee, C.; Shannon, C.E.; Burns, A.; Selby, A.L.; Wilkinson, D.; Smith, K.; Greenhaff, P.L.; Stephens, F.B. Increasing skeletal muscle carnitine content in older individuals increases whole-body fat oxidation during moderate-intensity exercise. Aging Cell 2021, 20, e13303. [Google Scholar] [CrossRef]
- Platell, C.; Kong, S.E.; McCauley, R.; Hall, J.C. Branched-chain amino acids. J. Gastroenterol. Hepatol. 2000, 15, 706–717. [Google Scholar] [CrossRef]
- Roe, D.S.; Roe, C.R.; Brivet, M.; Sweetman, L. Evidence for a short-chain carnitine-acylcarnitine translocase in mitochondria specifically related to the metabolism of branched-chain amino acids. Mol. Genet. Metab. 2000, 69, 69–75. [Google Scholar] [CrossRef]
- Molinger, J.; Pastva, A.M.; Whittle, J.; Wischmeyer, P.E. Novel approaches to metabolic assessment and structured exercise to promote recovery in ICU survivors. Curr. Opin. Crit. Care 2020, 26, 369–378. [Google Scholar] [CrossRef]

{kind=link}
{kind=link}
| Data | n = 64 | |
|---|---|---|
| Male, n (%) | 44 (68.7) | |
| Age, y | 63 (50.2–68.7) Males: 63 (50.2–68.8) Females: 62 (50.5–69.2) | |
| Weight, kg | 77 (69.1–90) Males: 79.1 (69.6–95) Females: 74.2 (69–85.5) | |
| BMI, kg/m2 | 26.9 (23.8–30.6) Males: 26 (23.1–30.3) Females: 28.6 (25.3–33.2) | |
| Active smoking, n (%) | 10 (15.6) | |
| Admission category, n (%) | Medical | 30 (46.9) |
| Surgical | 34 (53.1) | |
| Primary dysfunction, n (%) | Cardiovascular | 24 (37.5) |
| Pulmonary | 15 (23.4) | |
| Neurologic | 6 (9.4) | |
| Digestive and hepatic | 8 (12.5) | |
| Polytrauma | 1 (1.6) | |
| Other | 10 (15.6) | |
| Simplified Acute Physiology Score II | 33.5 (26–53.7) | |
| Mechanical ventilation (MV) >24 h, n (%) | 48 (75) | |
| MV duration, d | 7 (2–16.8) | |
| Renal replacement therapy (RRT), n (%) | 4 (6.2) | |
| RRT duration, d | 10.5 (5.7–28) | |
| Extracorporeal membrane oxygenation, n (%) | 3 (4.7) | |
| Propofol-based sedation, n (%) | 46 (71.9) | |
| Propofol duration, d | 6 (2–12) | |
| Type of nutrition during ICU stay, n (%) | Oral nutrition | 34 (53.1) |
| Enteral nutrition | 40 (62.5) | |
| Parenteral nutrition | 10 (15.6) | |
| ICU LOS, d | 15 (9.2–23.8) | |
| Hospital LOS, d | 43 (26–67.5) | |
| Acylcarnitines (μmol/L) | Reference Range | T0 | M3 | p Value |
|---|---|---|---|---|
| C0 | 14.95–84.34 | 45.89 (35.8–127.5) | 28.73 (20.31–38.93) | <0.001 |
| C2 | 2.71–21.28 | 10.81 (7.48–14.85) | 8.61 (6.65–12.90) | 0.019 |
| Short-chain ACs | ||||
| C3 | 0.086–3.329 | 0.540 (0.431–0.809) | 0.337 (0.220–0.477) | <0.001 |
| C3-DC | 0.007–0.221 | 0.065 (0.037–0.106) | 0.060 (0.038–0.080) | 0.1465 |
| C4 | 0.038–0.400 | 0.235 (0.170–0.385) | 0.160 (0.112–0.240) | <0.001 |
| C5 | 0.024–0.202 | 0.100 (0.066–0.150) | 0.080 (0.059–0.110) | 0.002 |
| C5:1 | 0.004–0.043 | 0.020 (0.008–0.030) | 0.020 (0.010–0.030) | 0.913 |
| C5-OH | 0.011–0.073 | 0.050 (0.040–0.080) | 0.050 (0.032–0.060) | 0.011 |
| C5-DC | 0.021–0.267 | 0.150 (0.096–0.233) | 0.146 (0.110–0.200) | 0.719 |
| Medium-chain ACs | ||||
| C6 | 0.011–0.164 | 0.098 (0.066–0.148) | 0.053 (0.040–0.087) | <0.001 |
| C6-DC | 0.019–0.578 | 0.058 (0.030–0.114) | 0.045 (0.030–0.080) | 0.006 |
| C8 | 0.016–0.291 | 0.100 (0.070–0.138) | 0.086 (0.050–0.120) | 0.021 |
| C8:1 | 0.019–0.331 | 0.164 (0.114–0.287) | 0.152 (0.110–0.265) | 0.635 |
| C10 | 0.023–0.622 | 0.110 (0.081–0.187) | 0.100 (0.072–0.160) | 0.269 |
| C10:1 | 0.016–0.265 | 0.074 (0.085–0.099) | 0.062 (0.050–0.080) | 0.091 |
| C10:2 | 0.004–0.050 | 0.020 (0.010–0.029) | 0.020 (0.010–0.021) | 0.917 |
| C12 | 0.011–0.239 | 0.050 (0.040–0.067) | 0.058 (0.040–0.090) | 0.139 |
| C12:1 | 0.012–0.253 | 0.060 (0.040–0.094) | 0.047 (0.030–0.070) | 0.027 |
| Long-chain ACs | ||||
| C14 | 0.008–0.081 | 0.035 (0.027–0.050) | 0.040 (0.030–0.060) | 0.208 |
| C14:1 | 0.016–0.315 | 0.071 (0.050–0.101) | 0.060 (0.040–0.080) | 0.181 |
| C14:2 | 0.005–0.080 | 0.022 (0.020–0.031) | 0.020 (0.020–0.030) | 0.747 |
| C14-OH | 0.002–0.016 | 0.010 (0.007–0.014) | 0.010 (0.010–0.020) | 0.641 |
| C16 | 0.060–0.293 | 0.190 (0.140–0.267) | 0.190 (0.141–0.267) | 0.514 |
| C16:1 | 0.007–0.154 | 0.040 (0.030–0.056) | 0.035 (0.023–0.047) | 0.093 |
| C16-OH | 0.001–0.009 | 0.010 (0.004–0.020) | 0.010 (0.010–0.010) | 0.336 |
| C18 | 0.019–0.082 | 0.075 (0.040–0.110) | 0.086 (0.055–0.120) | 0.166 |
| C18:1 | 0.048–0.479 | 0.210 (0.151–0.317) | 0.210 (0.148–0.260) | 0.169 |
| C18:2 | 0.012–0.106 | 0.070 (0.046–0.110) | 0.070 (0.050–0.090) | 0.430 |
| C18:1-OH | 0.001–0.010 | 0.010 (0.004–0.020) | 0.010 (0.005–0.020) | 0.587 |
| C18:2-OH | 0.001–0.006 | 0.010 (0.002–0.010) | 0.010 (0.003–0.010) | 0.755 |
| Biomarkers | Reference Range | T0 | M3 | p Value |
|---|---|---|---|---|
| White blood cells (/mm3) | 103/mm3 | 9.57 (7.14–12.84) | 7.48 (6.25–9) | 0.004 |
| C-reactive protein (mg/L) | 0–5 | 33.1 (16.3–85.5) | 2.8 (1–10.9) | <0.001 |
| Albumin (g/L) | 32–46 | 32 (29–35) | 43 (39–44) | <0.001 |
| Prealbumin (g/L) | 0.2–0.4 | 0.20 (0.15–0.27) | 0.27 (0.24–0.31) | 0.075 |
| Triglycerides (mg/dL) | <175 | 143 (99–176) | 141.5 (102.8–242.5) | 0.277 |
| Urea (mg/dL) | 15–55 | 41.9 (29.1–55.7) | 34.1 (26.2–56.5) | 0.293 |
| Creatinine (mg/dL) | 0.55–1.02 (females) 0.55–1.18 (males) | 0.78 (0.59–1.27) | 0.95 (0.74–1.26) | 0.023 |
| eGFR (mL/min/1.73 m2) | >60 | 96.5 (55.5–114.3) | 75 (53.5–100) | 0.013 |
| Urea/Creatinine | 46.1 (35.6–69.5) | 37.8 (27.4–50.7) | 0.008 | |
| Cystatin C (mg/L) | 0.62–1.11 | 1.28 (1.03–1.59) | 1.38 (1.12–1.72) | 0.648 |
| Creatinine/Cystatin C | 52 (45–76) | 70 (59–85) | 0.057 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Rousseau, A.-F.; Ngongan, A.; Colson, C.; Minguet, P.; Neis-Gilson, S.; Cavalier, E.; Minguet, G.; Misset, B.; Boemer, F. Mid-Term Evolution of the Serum Acylcarnitine Profile in Critically Ill Survivors: A Metabolic Insight into Survivorship. Nutrients 2023, 15, 3595. https://doi.org/10.3390/nu15163595
Rousseau A-F, Ngongan A, Colson C, Minguet P, Neis-Gilson S, Cavalier E, Minguet G, Misset B, Boemer F. Mid-Term Evolution of the Serum Acylcarnitine Profile in Critically Ill Survivors: A Metabolic Insight into Survivorship. Nutrients. 2023; 15(16):3595. https://doi.org/10.3390/nu15163595
Chicago/Turabian StyleRousseau, Anne-Françoise, Arsène Ngongan, Camille Colson, Pauline Minguet, Sarah Neis-Gilson, Etienne Cavalier, Grégory Minguet, Benoit Misset, and François Boemer. 2023. "Mid-Term Evolution of the Serum Acylcarnitine Profile in Critically Ill Survivors: A Metabolic Insight into Survivorship" Nutrients 15, no. 16: 3595. https://doi.org/10.3390/nu15163595
APA StyleRousseau, A.-F., Ngongan, A., Colson, C., Minguet, P., Neis-Gilson, S., Cavalier, E., Minguet, G., Misset, B., & Boemer, F. (2023). Mid-Term Evolution of the Serum Acylcarnitine Profile in Critically Ill Survivors: A Metabolic Insight into Survivorship. Nutrients, 15(16), 3595. https://doi.org/10.3390/nu15163595