
Managing Female Athlete Health: Auditing the Representation of Female versus Male Participants among Research in Supplements to Manage Diagnosed Micronutrient Issues

 , , and
, , and
Abstract
1. Introduction
2. Materials and Methods
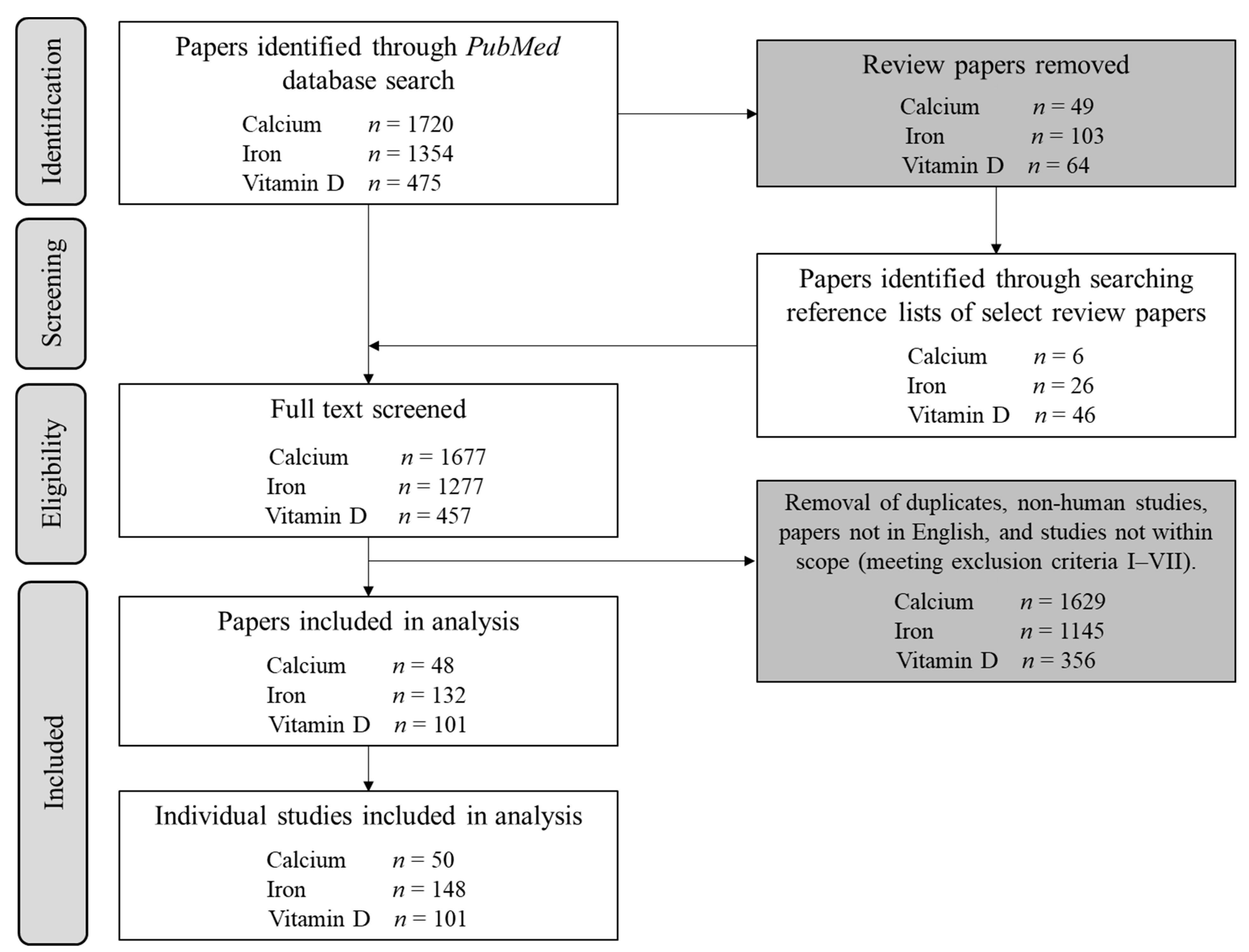
2.1. Search Strategy
2.2. Data Extraction
2.3. Statistical Analysis
3. Results
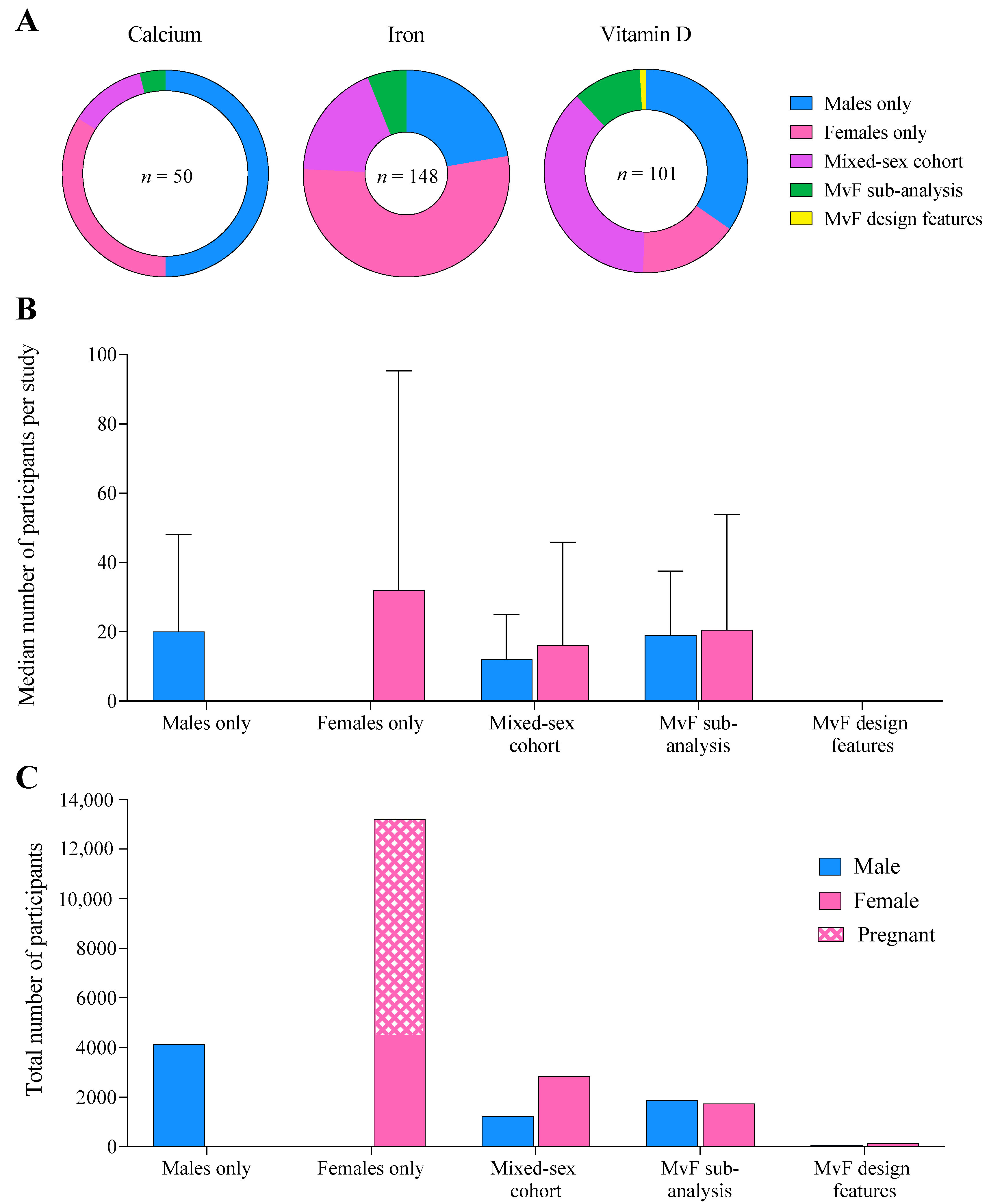
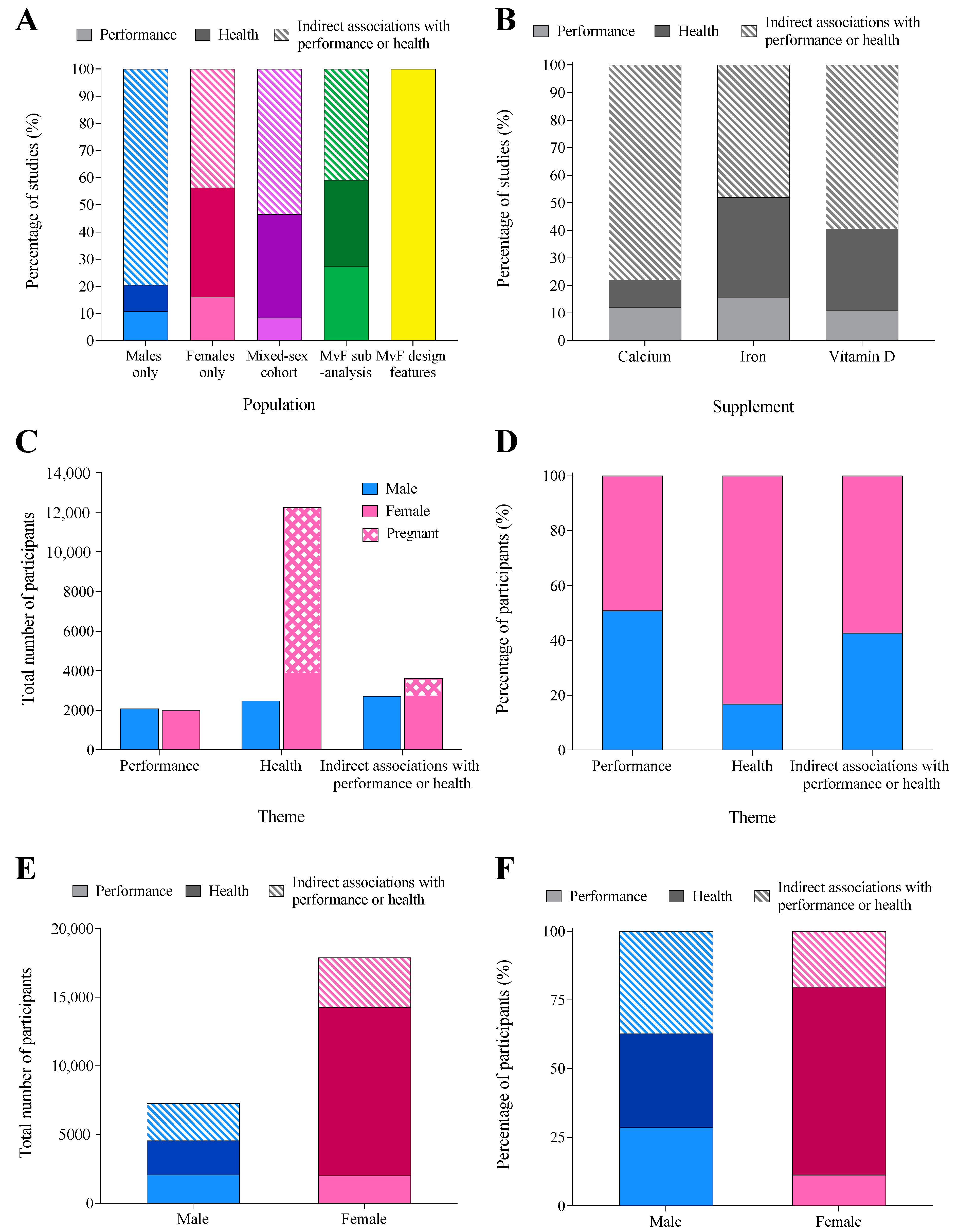
3.1. Population and Sample Size
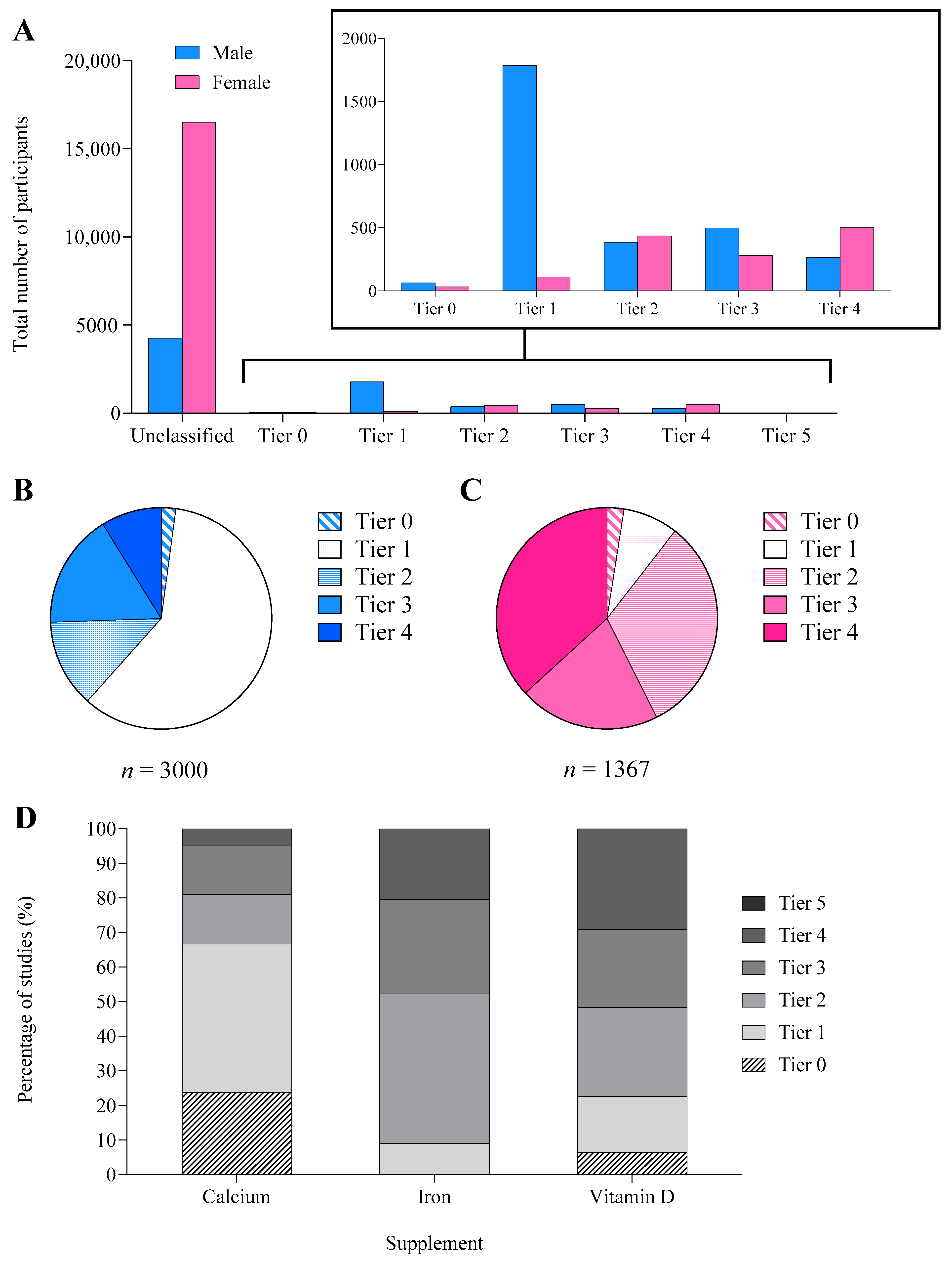
3.2. Athletic Calibre
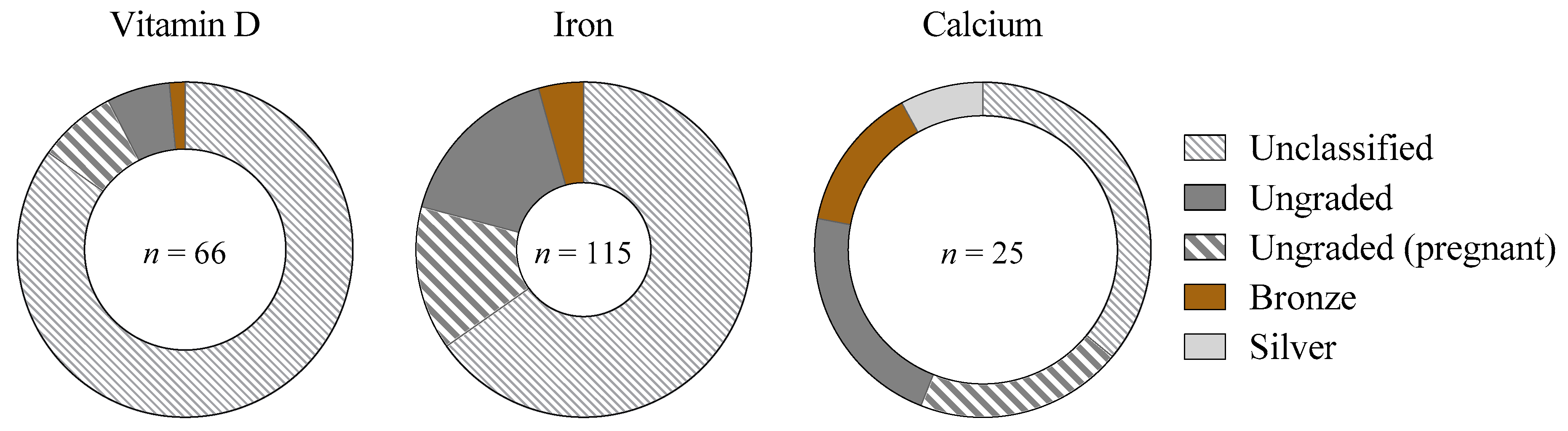
3.3. Menstrual Status
3.4. Performance vs. Health Research Themes
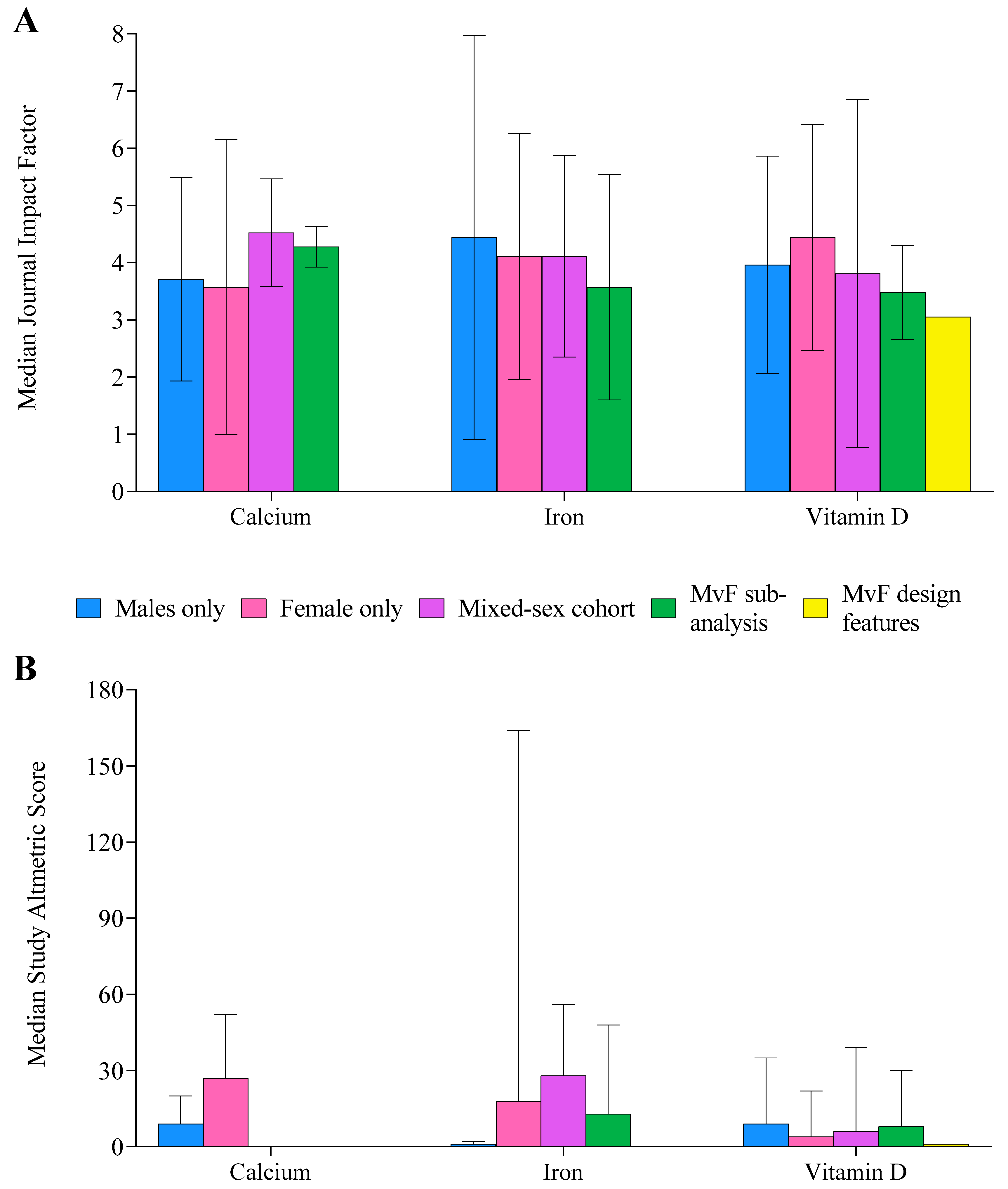
3.5. Journal and Study Impact
3.6. Supplement-Specific
3.7. Athlete-Specific Literature
4. Discussion
4.1. Calcium
4.2. Iron
4.3. Vitamin D
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Australian Institute of Sport; Australian Sports Commission. The AIS Sports Supplement Framework; Australian Institute of Sport: Bruce, Australia, 2021.
- Garthe, I.; Maughan, R.J. Athletes and supplements: Prevalence and perspectives. Int. J. Sport Nutr. Exerc. Metab. 2018, 28, 126–138. [Google Scholar] [CrossRef] [PubMed]
- Maughan, R.J.; Burke, L.M.; Dvorak, J.; Larson-Meyer, D.E.; Peeling, P.; Phillips, S.M.; Rawson, E.S.; Walsh, N.P.; Garthe, I.; Geyer, H. IOC consensus statement: Dietary supplements and the high-performance athlete. Int. J. Sport Nutr. Exerc. Metab. 2018, 28, 104–125. [Google Scholar] [CrossRef] [PubMed]
- Wiens, K.; Erdman, K.A.; Stadnyk, M.; Parnell, J.A. Dietary supplement usage, motivation, and education in young, Canadian athletes. Int. J. Sport Nutr. Exerc. Metab. 2014, 24, 613–622. [Google Scholar] [CrossRef] [PubMed]
- Bird, J.K.; Murphy, R.A.; Ciappio, E.D.; McBurney, M.I. Risk of deficiency in multiple concurrent micronutrients in children and adults in the United States. Nutrients 2017, 9, 655. [Google Scholar] [CrossRef] [PubMed]
- Jordan, S.L.; Albracht-Schulte, K.; Robert-McComb, J.J. Micronutrient deficiency in athletes and inefficiency of supplementation: Is low energy availability a culprit? PharmaNutrition 2020, 14, 100229. [Google Scholar] [CrossRef]
- Hossein-Nezhad, A.; Holick, M.F. Vitamin D for health: A global perspective. Mayo Clin. Proc. 2013, 88, 720–755. [Google Scholar] [CrossRef]
- Close, G.L.; Kasper, A.M.; Walsh, N.P.; Maughan, R.J. “Food first but not always food only”: Recommendations for using dietary supplements in sport. Int. J. Sport Nutr. Exerc. Metab. 2022, 1, 1–16. [Google Scholar] [CrossRef]
- Bermon, S.; Castell, L.M.; Calder, P.C.; Bishop, N.C.; Blomstrand, E.; Mooren, F.C.; Kruger, K.; Kavazis, A.N.; Quindry, J.C.; Senchina, D.S.; et al. Consensus statement immunonutrition and exercise. Exerc. Immunol. Rev. 2017, 23, 8–50. [Google Scholar]
- Walsh, N.P. Nutrition and athlete immune health: New perspectives on an old paradigm. Sports Med. 2019, 49, 153–168. [Google Scholar] [CrossRef]
- DellaValle, D.M.; Haas, J.D. Impact of iron depletion without anemia on performance in trained endurance athletes at the beginning of a training season: A study of female collegiate rowers. Int. J. Sport Nutr. Exerc. Metab. 2011, 21, 501–506. [Google Scholar] [CrossRef]
- DellaValle, D.M.; Haas, J.D. Iron supplementation improves energetic efficiency in iron-depleted female rowers. Med. Sci. Sports Exerc. 2014, 46, 1204–1215. [Google Scholar] [CrossRef] [PubMed]
- Haas, J.D.; Brownlie, T., IV. Iron deficiency and reduced work capacity: A critical review of the research to determine a causal relationship. J. Nutr. 2001, 131, 676S–688S, discussion 688S–690S. [Google Scholar] [CrossRef] [PubMed]
- Smith, E.S.; McKay, A.K.A.; Kuikman, M.; Ackerman, K.E.; Harris, R.; Elliott-Sale, K.J.; Stellingwerff, T.; Burke, L.M. Auditing the representation of female versus male athletes in sports science and sports medicine research: Evidence-based performance supplements. Nutrients 2022, 14, 953. [Google Scholar] [CrossRef] [PubMed]
- Smith, E.S.; McKay, A.K.A.; Ackerman, K.E.; Harris, R.; Elliott-Sale, K.J.; Stellingwerff, T.; Burke, L.M. Methodology review: A protocol to audit the representation of female athletes in sports science and sports medicine research. Int. J. Sport Nutr. Exerc. Metab. 2022, 32, 114–127. [Google Scholar] [CrossRef] [PubMed]
- Ouzzani, M.; Hammady, H.; Fedorowicz, Z.; Elmagarmid, A. Rayyan—A Web and Mobile App for Systematic Reviews. Available online: https://www.rayyan.ai/ (accessed on 1 February 2022).
- McKay, A.K.A.; Stellingwerff, T.; Smith, E.S.; Martin, D.T.; Mujika, I.; Goosey-Tolfrey, V.L.; Sheppard, J.; Burke, L.M. Defining training and performance caliber: A participant classification framework. Int. J. Sports Physiol. Perform. 2022, 17, 317–331. [Google Scholar] [CrossRef] [PubMed]
- Altmetric. Putting the Altmetric Attention Score in Context. Available online: https://help.altmetric.com/support/solutions/articles/6000233313-putting-the-altmetric-attention-score-in-context (accessed on 1 March 2022).
- Elliott-Sale, K.J.; Minahan, C.L.; de Jonge, X.; Ackerman, K.E.; Sipila, S.; Constantini, N.W.; Lebrun, C.M.; Hackney, A.C. Methodological Considerations for Studies in Sport and Exercise Science with Women as Participants: A Working Guide for Standards of Practice for Research on Women. Sports Med. 2021, 51, 843–861. [Google Scholar] [CrossRef] [PubMed]
- Campbell, C.G.; Chew, B.P.; Luedecke, L.O.; Shultz, T.D. Yogurt consumption does not enhance immune function in healthy premenopausal women. Nutr. Cancer 2000, 37, 27–35. [Google Scholar] [CrossRef]
- Brookshire, B. Women in sports are often underrepresented in science. Sci. News 2016, 1, 847–851. [Google Scholar]
- Cowley, E.S.; Olenick, A.A.; McNulty, K.L.; Ross, E.Z. “Invisible sportswomen”: The sex data gap in sport and exercise science research. Women Sport Phys. Act. J. 2021, 29, 146–151. [Google Scholar] [CrossRef]
- Hutchins, K.P.; Borg, D.N.; Bach, A.J.E.; Bon, J.J.; Minett, G.M.; Stewart, I.B. Female (Under) Representation in Exercise Thermoregulation Research. Sports Med. Open 2021, 7, 43. [Google Scholar] [CrossRef]
- Costello, J.T.; Bieuzen, F.; Bleakley, C.M. Where are all the female participants in Sports and Exercise Medicine research? Eur. J. Sport Sci. 2014, 14, 847–851. [Google Scholar] [CrossRef] [PubMed]
- Pasricha, S.-R.; Tye-Din, J.; Muckenthaler, M.U.; Swinkels, D.W. Iron deficiency. Lancet 2021, 397, 233–248. [Google Scholar] [CrossRef]
- Sim, M.; Garvican-Lewis, L.A.; Cox, G.R.; Govus, A.; McKay, A.K.A.; Stellingwerff, T.; Peeling, P. Iron considerations for the athlete: A narrative review. Eur. J. Appl. Physiol. 2019, 119, 1463–1478. [Google Scholar] [CrossRef] [PubMed]
- Badenhorst, C.E.; Dawson, B.; Cox, G.R.; Laarakkers, C.M.; Swinkels, D.W.; Peeling, P. Acute dietary carbohydrate manipulation and the subsequent inflammatory and hepcidin responses to exercise. Eur. J. Appl. Physiol. 2015, 115, 2521–2530. [Google Scholar] [CrossRef] [PubMed]
- Goto, K.; Kojima, C.; Kasai, N.; Sumi, D.; Hayashi, N.; Hwang, H. Resistance exercise causes greater serum hepcidin elevation than endurance (cycling) exercise. PLoS ONE 2020, 15, e0228766. [Google Scholar] [CrossRef]
- Peeling, P.; Dawson, B.; Goodman, C.; Landers, G.; Wiegerinck, E.T.; Swinkels, D.W.; Trinder, D. Training surface and intensity: Inflammation, hemolysis, and hepcidin expression. Med. Sci. Sports Exerc. 2009, 41, 1138–1145. [Google Scholar] [CrossRef]
- Haakonssen, E.C.; Ross, M.L.; Knight, E.J.; Cato, L.E.; Nana, A.; Wluka, A.E.; Cicuttini, F.M.; Wang, B.H.; Jenkins, D.G.; Burke, L.M. The effects of a calcium-rich pre-exercise meal on biomarkers of calcium homeostasis in competitive female cyclists: A randomised crossover trial. PLoS ONE 2015, 10, e0123302. [Google Scholar] [CrossRef]
- Barry, D.W.; Hansen, K.C.; Van Pelt, R.E.; Witten, M.; Wolfe, P.; Kohrt, W.M. Acute calcium ingestion attenuates exercise-induced disruption of calcium homeostasis. Med. Sci. Sports Exerc. 2011, 43, 617. [Google Scholar] [CrossRef]
- Guillemant, J.; Accarie, C.; Peres, G.; Guillemant, S. Acute effects of an oral calcium load on markers of bone metabolism during endurance cycling exercise in male athletes. Calcif. Tissue Int. 2004, 74, 407–414. [Google Scholar] [CrossRef]
- Kuikman, M.A.; Smith, E.S.; McKay, A.K.A.; Ackerman, K.E.; Harris, R.; Elliott-Sale, K.J.; Stellingwerff, T.; Burke, L.M. Fuelling the female athlete: Auditing her representation in studies of acute carbohydrate intake for exercise. Eur. J. Sport Sci. 2022, 22, 684–696. [Google Scholar]
- Dusek, T. Influence of high intensity training on menstrual cycle disorders in athletes. Croat. Med. J. 2001, 42, 79–82. [Google Scholar] [PubMed]
- Martin, D.; Sale, C.; Cooper, S.B.; Elliott-Sale, K.J. Period Prevalence and Perceived Side Effects of Hormonal Contraceptive Use and the Menstrual Cycle in Elite Athletes. Int. J. Sports Physiol. Perform. 2018, 13, 926–932. [Google Scholar] [CrossRef] [PubMed]
- Redman, L.M.; Loucks, A.B. Menstrual disorders in athletes. Sports Med. 2005, 35, 747–755. [Google Scholar] [CrossRef] [PubMed]
- Torstveit, M.; Sundgot-Borgen, J. Participation in leanness sports but not training volume is associated with menstrual dysfunction: A national survey of 1276 elite athletes and controls. Br. J. Sports Med. 2005, 39, 141–147. [Google Scholar] [CrossRef]
- Martínez-Rosales, E.; Hernández-Martínez, A.; Sola-Rodríguez, S.; Esteban-Cornejo, I.; Soriano-Maldonado, A. Representation of women in sport sciences research, publications, and editorial leadership positions: Are we moving forward? J. Sci. Med. Sport 2021, 24, 1093–1097. [Google Scholar] [CrossRef]
- Thomas, D.T.; Erdman, K.A.; Burke, L.M. American College of Sports Medicine joint position statement. Nutrition and athletic performance. Med. Sci. Sports Exerc. 2016, 48, 543–568. [Google Scholar] [CrossRef]
- Lundy, B.; McKay, A.K.A.; Fensham, N.C.; Tee, N.; Anderson, B.; Morabito, A.; Ross, M.L.R.; Sim, M.; Ackerman, K.E.; Burke, L.M. The impact of acute calcium intake on bone markers during a training day in elite male rowers. Med. Sci. Sports Exerc. 2022; in review. [Google Scholar]
- Kohrt, W.M.; Wolfe, P.; Sherk, V.D.; Wherry, S.J.; Wellington, T.; Melanson, E.L.; Swanson, C.M.; Weaver, C.M.; Boxer, R.S. Dermal calcium loss is not the primary determinant of PTH secretion during exercise. Med. Sci. Sports Exerc. 2019, 51, 2117. [Google Scholar] [CrossRef]
- Haakonssen, E.C.; Ross, M.L.; Cato, L.E.; Nana, A.; Knight, E.J.; Jenkins, D.G.; Martin, D.T.; Burke, L.M. Dairy-based preexercise meal does not affect gut comfort or time-trial performance in female cyclists. Int. J. Sport Nutr. Exerc. Metab. 2014, 24, 553–558. [Google Scholar] [CrossRef]
- Mehlenbeck, R.S.; Ward, K.D.; Klesges, R.C.; Vukadinovich, C.M. A pilot intervention to increase calcium intake in female collegiate athletes. Int. J. Sport Nutr. Exerc. Metab. 2004, 14, 18–29. [Google Scholar] [CrossRef][Green Version]
- McCormick, R.; Sim, M.; Dawson, B.; Peeling, P. Refining treatment strategies for iron deficient athletes. Sports Med. 2020, 50, 2111–2123. [Google Scholar] [CrossRef] [PubMed]
- Ashenden, M.J.; Dobson, G.P.; Hahn, A.G. Sensitivity of reticulocyte indices to iron therapy in an intensely training athlete. Br. J. Sports Med. 1998, 32, 259–260. [Google Scholar] [CrossRef] [PubMed]
- Harris Rosenzweig, P.; Volpe, S.L. Effect of iron supplementation on thyroid hormone levels and resting metabolic rate in two college female athletes: A case study. Int. J. Sport Nutr. Exerc. Metab. 2000, 10, 434–443. [Google Scholar] [CrossRef] [PubMed]
- Ashenden, M.; Pyne, D.; Parisotto, R.; Dobson, G.; Hahn, A. Can reticulocyte parameters by of use in detecting iron deficient erythropoiesis in female athletes? J. Sports Med. Phys. Fit. 1999, 39, 140. [Google Scholar]
- Powell, P.D.; Tucker, A. Iron supplementation and running performance in female cross-country runners. Int. J. Sports Med. 1991, 12, 462–467. [Google Scholar] [CrossRef]
- Risser, W.L.; Lee, E.J.; Poindexter, H.B.; West, M.S.; Pivarnik, J.M.; Risser, J.M.; Hickson, J.F. Iron deficiency in female athletes: Its prevalence and impact on performance. Med. Sci. Sports Exerc. 1988, 20, 116–121. [Google Scholar] [CrossRef]
- Sandroni, A.; House, E.; Howard, L.; DellaValle, D.M. Synbiotic supplementation improves response to iron supplementation in female athletes during training. J. Diet. Suppl. 2022, 19, 366–380. [Google Scholar] [CrossRef]
- Burden, R.J.; Pollock, N.; Whyte, G.P.; Richards, T.; Moore, B.; Busbridge, M.; Srai, S.K.; Otto, J.; Pedlar, C.R. Effect of intravenous iron on aerobic capacity and iron metabolism in elite athletes. Med. Sci. Sports Exerc. 2015, 47, 1399–1407. [Google Scholar] [CrossRef]
- Blee, T.; Goodman, C.; Dawson, B.; Stapff, A. The effect of intramuscular iron injections on serum ferritin levels and physical performance in elite netballers. J. Sci. Med. Sport 1999, 2, 311–321. [Google Scholar] [CrossRef]
- Ishizaki, S.; Koshimizu, T.; Yanagisawa, K.; Akiyama, Y.; Mekada, Y.; Shiozawa, N.; Takahaski, N.; Yamakawa, J.; Kawano, Y. Effects of a fixed dietary intake on changes in red blood cell delta-aminolevulinate dehydratase activity and hemolysis in female rhythmic gymnasts: A two-year follow-up study. Int. J. Sport Nutr. Exerc. Metab. 2006, 16, 597–610. [Google Scholar] [CrossRef]
- Govus, A.D.; Garvican-Lewis, L.A.; Abbiss, C.R.; Peeling, P.; Gore, C.J. Pre-altitude serum ferritin levels and daily oral iron supplement dose mediate iron parameter and hemoglobin mass responses to altitude exposure. PLoS ONE 2015, 10, e0135120. [Google Scholar] [CrossRef] [PubMed]
- Okazaki, K.; Stray-Gundersen, J.; Chapman, R.F.; Levine, B.D. Iron insufficiency diminishes the erythropoietic response to moderate altitude exposure. J. Appl. Physiol. 2019, 127, 1569–1578. [Google Scholar] [CrossRef] [PubMed]
- Hall, R.; Peeling, P.; Nemeth, E.; Bergland, D.; McCluskey, W.T.P.; Stellingwerff, T. Single versus split dose of iron optimizes hemoglobin mass gains at 2106 m altitude. Med. Sci. Sports Exerc. 2019, 51, 751–759. [Google Scholar] [CrossRef] [PubMed]
- Tsalis, G.; Nikolaidis, M.; Mougios, V. Effects of iron intake through food or supplement on iron status and performance of healthy adolescent swimmers during a training season. Int. J. Sports Med. 2004, 25, 306–313. [Google Scholar] [PubMed]
- Owens, D.J.; Allison, R.; Close, G.L. Vitamin D and the Athlete: Current Perspectives and New Challenges. Sports Med. 2018, 48, 3–16. [Google Scholar] [CrossRef]
- Aydin, C.G.; Dincel, Y.M.; Arikan, Y.; Tas, S.K.; Deniz, S. The effects of indoor and outdoor sports participation and seasonal changes on vitamin D levels in athletes. SAGE Open Med. 2019, 7, 2050312119837480. [Google Scholar] [CrossRef]
- Fishman, M.P.; Lombardo, S.J.; Kharrazi, F.D. Vitamin D deficiency among professional basketball players. Orthop. J. Sports Med. 2016, 4, 2325967116655742. [Google Scholar] [CrossRef]
- Ksiazek, A.; Zagrodna, A.; Slowinska-Lisowska, M. Vitamin D, skeletal muscle function and athletic performance in athletes—A narrative review. Nutrients 2019, 11, 1800. [Google Scholar] [CrossRef]
- Heaney, R.P.; Recker, R.R.; Grote, J.; Horst, R.L.; Armas, L.A. Vitamin D3 is more potent than vitamin D2 in humans. J. Clin. Endocrinol. Metab. 2011, 96, E447–E452. [Google Scholar] [CrossRef]
- Lehmann, U.; Hirche, F.; Stangl, G.I.; Hinz, K.; Westphal, S.; Dierkes, J. Bioavailability of vitamin D2 and D3 in healthy volunteers, a randomized placebo-controlled trial. J. Clin. Endocrinol. Metab. 2013, 98, 4339–4345. [Google Scholar] [CrossRef]
- Trang, H.M.; Cole, D.; Rubin, L.A.; Pierratos, A.; Siu, S.; Vieth, R. Evidence that vitamin D3 increases serum 25-hydroxyvitamin D more efficiently than does vitamin D2. Am. J. Clin. Nutr. 1998, 68, 854–858. [Google Scholar] [CrossRef] [PubMed]
- AlQuaiz, A.M.; Kazi, A.; Fouda, M.; Alyousefi, N. Age and gender differences in the prevalence and correlates of vitamin D deficiency. Arch. Osteoporos. 2018, 13, 49. [Google Scholar] [CrossRef] [PubMed]
- Sanghera, D.K.; Sapkota, B.R.; Aston, C.E.; Blackett, P.R. Vitamin D status, gender differences, and cardiometabolic health disparities. Ann. Nutr. Metab. 2017, 70, 79–87. [Google Scholar] [CrossRef] [PubMed]
- Vitale, J.A.; Lombardi, G.; Cavaleri, L.; Graziani, R.; Schoenhuber, H.; Torre, A.L.; Banfi, G. Rates of insufficiency and deficiency of vitamin D levels in elite professional male and female skiers: A chronobiologic approach. Chronobiol. Int. 2018, 35, 441–449. [Google Scholar] [CrossRef]








{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Supplement | Daily Oral Supplementation | Bolus Supplementation | Food Fortification/Food Only | ||||
|---|---|---|---|---|---|---|---|
| Mean Dose | No. of Studies | Mean Dose | Dosing Method | No. of Studies | Mean Dose | No. of Studies | |
| Calcium | 1264 mg | 16 | - | - | - | 798 mg | 9 |
| Iron | 100 mg | 100 | 846 mg | IV (n = 16) IM (n = 3) | 19 | 9.2 mg | 23 |
| Vitamin D | 2754 IU | 54 | 83,709 IU | Oral (n = 38) IV (n = 2) IM (n = 2) | 42 | 731 IU | 8 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Smith, E.S.; McKay, A.K.A.; Kuikman, M.; Ackerman, K.E.; Harris, R.; Elliott-Sale, K.J.; Stellingwerff, T.; Burke, L.M. Managing Female Athlete Health: Auditing the Representation of Female versus Male Participants among Research in Supplements to Manage Diagnosed Micronutrient Issues. Nutrients 2022, 14, 3372. https://doi.org/10.3390/nu14163372
Smith ES, McKay AKA, Kuikman M, Ackerman KE, Harris R, Elliott-Sale KJ, Stellingwerff T, Burke LM. Managing Female Athlete Health: Auditing the Representation of Female versus Male Participants among Research in Supplements to Manage Diagnosed Micronutrient Issues. Nutrients. 2022; 14(16):3372. https://doi.org/10.3390/nu14163372
Chicago/Turabian StyleSmith, Ella S., Alannah K. A. McKay, Megan Kuikman, Kathryn E. Ackerman, Rachel Harris, Kirsty J. Elliott-Sale, Trent Stellingwerff, and Louise M. Burke. 2022. "Managing Female Athlete Health: Auditing the Representation of Female versus Male Participants among Research in Supplements to Manage Diagnosed Micronutrient Issues" Nutrients 14, no. 16: 3372. https://doi.org/10.3390/nu14163372
APA StyleSmith, E. S., McKay, A. K. A., Kuikman, M., Ackerman, K. E., Harris, R., Elliott-Sale, K. J., Stellingwerff, T., & Burke, L. M. (2022). Managing Female Athlete Health: Auditing the Representation of Female versus Male Participants among Research in Supplements to Manage Diagnosed Micronutrient Issues. Nutrients, 14(16), 3372. https://doi.org/10.3390/nu14163372