
Effect of Fortification with Multiple Micronutrient Powder on the Prevention and Treatment of Iron Deficiency and Anaemia in Brazilian Children: A Randomized Clinical Trial

 ,
,
Abstract
1. Introduction
2. Materials and Methods
2.1. Study Design and Eligibility
2.2. Sampling and Randomization
2.3. Intervention
2.4. Variables Recorded
2.5. Data Collection
2.6. Statistical Analyses
2.7. Ethical Considerations
3. Results
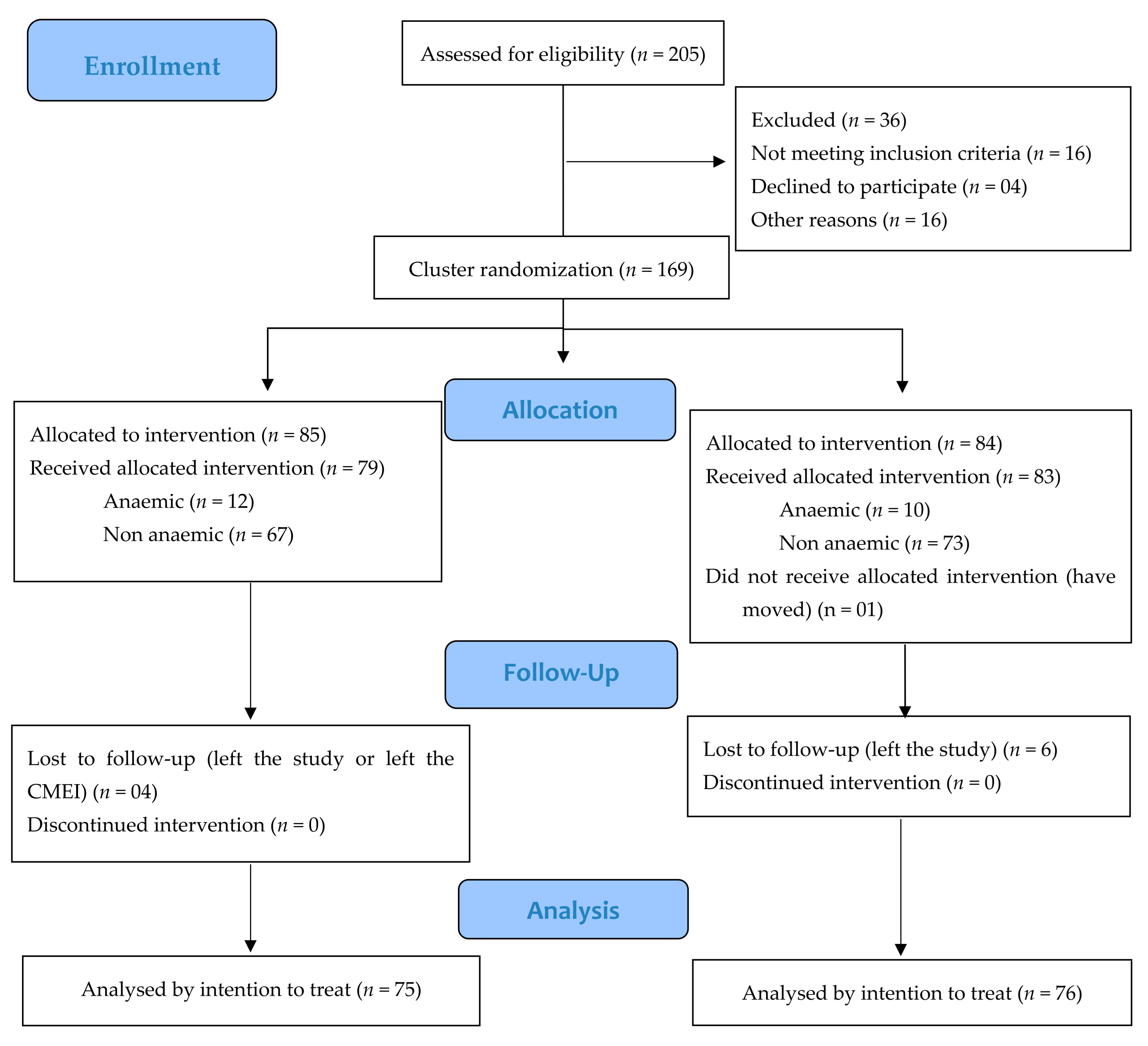
3.1. Participants
3.2. Prevalence of Anaemia and Iron Deficiency
3.3. Random Effects
3.4. Effect of Baseline Intervention
3.5. Delta Analyses
3.6. Adverse Reactions
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Stevens, G.A.; Finucane, M.M.; De-Regil, L.M.; Paciorek, C.J.; Flaxman, S.R.; Branca, F.; Peña-Rosas, J.P.; Bhutta, Z.A.; Ezzati, M.; Nutrition Impact Model Study Group. Behalf of Nutrition Impact Model Study Group Anaemia. Global, regional, and national trends in haemoglobin concentration and prevalence of total and severe anaemia in children and pregnant and non-pregnant women for 1995–2011: A systematic analysis of population-representative data. Lancet Glob. Health 2013, 1, e16–e25. [Google Scholar] [CrossRef]
- De-Regil, L.M.; Jefferds, M.E.D.; Peña-Rosas, J.P. Point-of-use fortification of foods with micronutrient powders containing iron in children of preschool and school-age. Cochrane Database Syst. Rev. 2017, 11, 1–142. [Google Scholar] [CrossRef] [PubMed]
- World Health Organizaton. World Health Data Platform. Prevalence of Anaemia in Children under 5 Years (%) [internet]. Geneva. Available online: https://www.who.int/data/gho/data/indicators/indicator-details/GHO/prevalence-of-anaemia-in-children-under-5-years-(-) (accessed on 4 February 2021).
- Ministério da Saúde (Brasil). NutriSUS. Guia de evidências: Estratégia de Fortificação da Alimentação Infantil com Micronutrientes (Vitaminas e Minerais) em pó; Ministério da Saúde, Ministério da Educação: Brasília, Brazil, 2015; 50p. [Google Scholar]
- World Health Organization. Comprehensive Implementation Plan on Maternal, Infant, and Young Child Nutrition; WHO: Geneva, Switzerland, 2014. [Google Scholar]
- De-Regil, L.M.; Suchdev, P.S.; Vist, G.E.; Walleser, S.; Peña-Rosas, J. Home fortification of foods with multiple micronutrient powders for health and nutrition in children under two years of age. Cochrane Database Syst. Rev. 2011, 9, 1–87. [Google Scholar] [CrossRef]
- Tam, E.; Keats, E.C.; Rind, F.; Das, J.K.; Bhutta, Z.A. Micronutrient supplementation and fortification interventions on health and development outcomes among children under-five in low- and middle-income countries: A systematic review and meta-analysis. Nutrients 2020, 12, 289. [Google Scholar] [CrossRef]
- Suchdev, P.S.; Jefferds, M.E.D.; Ota, E.; Lopes, K.S.; De-Regil, L.M. Home Fortification of Foods with Multiple Micronutrient Powders for Health and Nutrition in Children under Two Years of Age (Review); World Health Organization: Geneva, Switzerland, 2020; 162p. [Google Scholar] [CrossRef]
- Christofides, A.; Asante, K.P.; Schauer, C.; Sharieff, W.; Owusu-Agyei, S.; Zlotkin, S. Multi-micronutrient Sprinkles including a low dose of iron provided as microencapsulated ferrous fumarate improves haematologic indices in anaemic children: A randomized clinical trial. Matern. Child Nutr. 2006, 2, 169–180. [Google Scholar] [CrossRef] [PubMed]
- Hirve, S.; Bhave, S.; Bavdekar, A.; Naik, S.; Pandit, A.; Schauer, C.; Christofides, A.; Hyder, Z.; Zlotkin, S. Low dose ’Sprinkles’—An innovative approach to treat iron deficiency anemia in infants and young children. Indian Pediatr. 2007, 44, 91–100. [Google Scholar]
- Young, M.F.; Girard, A.W.; Mehta, R.; Srikantiah, S.; Gosdin, L.; Menon, P.; Ramakrishnan, U.; Martorell, R.; Avula, R. Acceptability of multiple micronutrient powders and iron syrup in Bihar, India. Matern. Child Nutr. 2018, 14, e12572. [Google Scholar] [CrossRef]
- Inayati, D.A.; Scherbaum, V.; Purwestri, R.C.; Wirawan, N.N.; Suryantan, J.; Hartono, S.; Bloem, M.A.; Pangaribuan, R.V.; Biesalski, H.K.; Bellows, A.C.; et al. Combined intensive nutrition education and micronutrient powder supplementation improved nutritional status of mildly wasted children on Nias Island, Indonesia. Asia Pac. J. Clin. Nutr. 2012, 21, 361–373. [Google Scholar]
- Kounnavong, S.; Sunahara, T.; Mascie-Taylor, C.N.; Hashizume, M.; Okumura, J.; Moji, K.; Boupha, B.; Yamamoto, T. Effect of daily versus weekly home fortification with multiple micronutrient powder on haemoglobin concentration of young children in a rural area, Lao People’s Democratic Republic: A randomised trial. Nutr. J. 2011, 10, 1–11. [Google Scholar] [CrossRef] [PubMed]
- Lundeen, E.; Schueth, T.; Toktobaev, N.; Zlotkin, S.; Hyder, S.M.Z.; Houser, R. Daily use of Sprinkles micronutrient powder for 2 months reduces anemia among children 6 to 36 months of age in the Kyrgyz Republic: A cluster-randomized trial. Food Nutr. Bull. 2010, 31, 446–460. [Google Scholar] [CrossRef] [PubMed]
- Macharia-Mutie, C.W.; Moretti, D.; Van den Briel, N.; Omusundi, A.M.; Mwangi, A.M.; Kok, F.J.; Zimmermann, M.B.; Brouwer, I.D. Maize porridge enriched with a micronutrient powder containing low-dose iron as NaFeEDTA but not amaranth grain flour reduces anemia and iron deficiency in Kenyan preschool children. J. Nutr. 2012, 142, 1756–1763. [Google Scholar] [CrossRef] [PubMed]
- Luo, R.; Yue, A.; Zhou, H.; Shi, Y.; Zhang, L.; Martorell, R.; Medina, A.; Rozelle, S.; Sylvia, S. The effect of a micronutrient powder home fortification program on anemia and cognitive outcomes among young children in rural China: A cluster randomized trial. BMC Public Health 2017, 17, 738–752. [Google Scholar] [CrossRef]
- Somassè, Y.E.; Dramaix, M.; Traoré, B.; Ngabonziza, I.; Touré, O.; Konaté, M.; Diallo, M.; Donnen, P. The WHO recommendation of home fortification of foods with multiple-micronutrient powders in children under 2 years of age and its effectiveness on anaemia and weight: A pragmatic cluster-randomized controlled trial. Public Health Nutr. 2018, 21, 1350–1358. [Google Scholar] [CrossRef]
- Lanou, H.B.; Osendarp, S.J.M.; Argaw, A.; Polnay k Ouédraogo, C.; Kouanda, S.; Kolsteren, P. Micronutrient powder supplements combined with nutrition education marginally improve growth amongst children aged 6–23 months in rural Burkina Faso: A cluster randomized controlled trial. Matern. Child Nutr. 2019, 15, e12820. [Google Scholar] [CrossRef]
- Larson, L.M.; Young, M.F.; Bauer, P.J.; Mehta, R.; Girard, A.W.; Ramakrishnan, U.; Verma, P.; Chaudhuri, I.; Srikantiah, S.; Martorell, R. Effectiveness of a home fortification programme with multiple micronutrients on infant and young child development: A cluster-randomised trial in rural Bihar, India. Br. J. Nutr. 2018, 120, 176–187. [Google Scholar] [CrossRef] [PubMed]
- Roschnik, N.; Diarra, H.; Dicko, Y.; Diarra, S.; Stanley, I.; Moestue, H.; McClean, J.; Verhoef, H.; Clarke, S.E. Adherence and acceptability of community-based distribution of micronutrient powders in Southern Mali. Matern. Child Nutr. 2019, 15, e12831. [Google Scholar] [CrossRef] [PubMed]
- Ministério da Saúde (Brasil). NutriSUS. Manual Operacional: Estratégia de Fortificação da Alimentação Infantil com Micronutrientes (Vitaminas e Minerais) em pó; Ministério da Saúde, Ministério da Educação: Brasília, Brazil, 2015; 52p. [Google Scholar]
- Cardoso, M.A.; Augusto, R.A.; Bortolini, G.A.; Oliveira, C.S.; Tietzman, D.C.; Sequeira, L.A.; Hadler, M.C.; do Rosario, G.; Peixoto, M.; Muniz, P.T.; et al. Effect of providing multiple micronutrients in powder through primary healthcare on anemia in young brazilian children: A multicentre pragmatic controlled trial. PLoS ONE 2016, 11, e0151097. [Google Scholar] [CrossRef]
- Hadler, M.C.C.M.; Sigulem, D.M.; Alves, M.F.C.; Torres, V.M. Treament and prevention of anemia with ferrous sulfate plus folic acid in children attending daycare centers in Goiânia, Goiás State, Brazil: A randomized controlled trial. Cad. Saúde Públic 2008, 24 (Suppl. 2), S259–S271. [Google Scholar] [CrossRef]
- HF-TAG—Home Fortification Technical Advisory Group. Manual on Micronutrient Powder (MNPs) Composition; Home Fortification Technical Advisory Group: Geneva, Switzerland, 2013. [Google Scholar]
- Associação Brasileira de Empresas de Pesquisas (ABEP). Critério de classificação econômica Brasil; Associação Brasileira de Empresas de Pesquisa (ABEP): São Paulo, Brazil, 2015. [Google Scholar]
- World Health Organization. Haemoglobin Concentrations for the Diagnosis of Anaemia and Assessment of Severity; WHO: Geneva, Switzerland, 2011. [Google Scholar]
- Lundeen, E.A.; Lind, J.N.; Clarke, K.E.; Aburto, N.J.; Imanalieva, C.; Mamyrbaeva, T.; Ismailova, A.; Timmer, A.; Whitehead, R.D.; Serdula, M.K.; et al. Four years after implementation of a national micronutrient powder program in Kyrgyzstan, prevalence of iron deficiency and iron deficiency anemia is lower, but prevalence of vitamin A deficiency is higher. Eur. J. Clin. Nutr. 2018, 73, 416–423. [Google Scholar] [CrossRef] [PubMed]
- World Health Organization. Guideline on Use of Ferritin Concentrations to Assess Iron Status in Individuals and Populations; World Health Organization: Geneva, Switzerland, 2020; 82p. [Google Scholar]
- Agência Nacional de Vigilância Sanitária—ANVISA. Aprovação do Regulamento Técnico para a Fortificação das Farinhas de Trigo e das Farinhas de Milho com Ferro e Ácido Fólico; RDC Nº 344, de 13 de dezembro de 2002; Diário Oficial da União nº 244 18 de dez; ANVISA: Brasília, Brazil, 2002.
- Ministério da Saúde (Brasil). Instituir o Componente I do Programa de Humanização no Pré-natal e Nascimento—Incentivo à Assistência Pré-natal no âmbito do Sistema Único de Saúde; Portaria nº 570, de 1º de junho de 2000; Diário Oficial da União, Brasília: 1º de jun; Ministério da Saúde: Brasília, Brazil, 2000. [Google Scholar]
- Figueredo, S.F.; Mattar, M.J.G.; Abrao, A.C.F.V. Iniciativa Hospital Amigo da Criança: Uma política de promoção, proteção e apoio ao aleitamento materno. Acta Paul. Enferm. 2012, 25, 459–463. [Google Scholar] [CrossRef][Green Version]
- Ministério da Saúde (Brasil). Programa Nacional de Suplementação de Ferro: Manual de condutas gerais; Secretaria de Atenção à Saúde, Departamento de Atenção Básica, Ministério da Saúde: Brasília, Brazil, 2013; 24p, ISBN 978-85-334-2042-7. [Google Scholar]
- Ministério da Saúde (Brasil). Manual de condutas gerais do Programa Nacional de Suplementação de Vitamina A; Secretaria de Atenção à Saúde, Departamento de Atenção Básica, Ministério da Saúde: Brasília, Brazil, 2013; 34p, ISBN 987-85-334-2021-2. [Google Scholar]
- Ministério da Saúde (Brasil). Bases para a discussão da Política Nacional de Promoção, Proteção e Apoio ao Aleitamento Materno; Secretaria de Atenção à Saúde, Departamento de Ações Programáticas Estratégicas, Ministério da Saúde: Brasília, Brazil, 2017; 68p, ISBN 978-85-334-2531-6. [Google Scholar]
- WHO—World Health Organization. O clampeamento tardio do cordão umbilical reduz a anemia infantil; WHO/RHR/14.19; WHO: Geneva, Switzerland, 2013; 5p. [Google Scholar]
- Giovannini, M.; Sala, D.; Usuelli, M.; Livio, L.; Francescato, G.; Braga, M.; Radaelli, G.; Riva, E. Double-blind, placebo-controlled trial comparing effects of supplementation with two different combinations of micronutrients delivered as sprinkles on growth, anemia, and iron deficiency in cambodian infants. J. Pediatr. Gastroenterol. Nutr. 2006, 42, 306–312. [Google Scholar] [CrossRef] [PubMed]
- Menon, P.; Ruel, M.T.; Loechl, C.U.; Arimond, M.; Habicht, J.P.; Pelto, G.; Michaud, L. Micronutrient sprinkles reduce anemia among 9- to 24-mo-old children when delivered through an integrated health and nutrition program in rural Haiti. J. Nutr. 2007, 137, 1023–1030. [Google Scholar] [CrossRef] [PubMed]
- Adu-Afarwuah, S.; Lartey, A.; Brown, K.H.; Zlotkin, S.; Briend, A.; Dewey, K.G. Randomized comparison of 3 types of micronutrient supplements for home fortification of complementary foods in Ghana: Effects on growth and motor development. Am. J. Clin. Nutr. 2007, 86, 412–420. [Google Scholar] [CrossRef] [PubMed]
- Hyder, S.M.Z.; Haseen, F.; Rahman, M.; Tondeur, M.; Zlotkin, S.H. Effect of daily versus once-weekly home fortification with micronutrient sprinkles on hemoglobin and iron status among young children in rural Bangladesh. Food Nutr. Bull. 2007, 28, 156–164. [Google Scholar] [CrossRef] [PubMed]
- Garcia-Casal, M.N.; Pasricha, S.R.; Sharma, A.J.; Peña-Rosas, J.P. Use and interpretation of hemoglobin concentrations for assessing anemia status in individuals and populations: Results from a WHO technical meeting. Ann. N. Y. Acad. Sci. 2019, 1450, 5–14. [Google Scholar] [CrossRef]
- Kejo, D.; Petrucka, P.; Martin, H.; Mosha, T.C.E.; Kimanya, M.E. Efficacy of Different Doses of Multiple Micronutrient Powder on Haemoglobin Concentration in Children Aged 6–59 Months in Arusha District. Scientifica 2019, 3, 1–7. [Google Scholar] [CrossRef]
- Carter, R.C.; Jacobson, J.L.; Burden, M.J.; Armony-Sivan, R.; Dodge, N.C.; Angelilli, M.L.; Lozoff, B.; Jacobson, S.W. Iron deficiency anemia and cognitive function in infancy. Pediatrics 2010, 126, e427–e434. [Google Scholar] [CrossRef]
- Tang, M.; Frank, D.N.; Hendricks, A.E.; Ir, D.; Esamai, F.; Liechty, E.; Hambidge, K.M.; Krebs, N.F. Iron in micronutrient powder promotes an unfavorable gut microbiota in Kenyan infants. Nutrients 2017, 9, 776. [Google Scholar] [CrossRef] [PubMed]




{kind=link}
{kind=link}
{kind=link}
| Variables 1 | Total (n = 162) | MNP 2 (n = 79) | FS_FA 3 (n = 83) | p Value 4 |
|---|---|---|---|---|
| Gender (female %) | 83 (51.23) | 41 (49.40) | 42 (50.60) | 0.869 |
| Child’s age (months) | 24 (14–35) | 24 (16–35) | 24 (13–35) | 0.975 |
| <24 months | 73 (45.06) | 36 (49.32) | 37 (50.68) | 0.899 |
| ≥24 months | 89 (54.94) | 43 (48.31) | 46 (51.69) | |
| Child skin color n (%) | 0.598 | |||
| White | 73 (45.06) | 39 (53.42) | 34 (46.58) | |
| Brown | 80 (49.38) | 36 (45.00) | 44 (55.00) | |
| Black | 9 (5.56) | 4 (44.44) | 5 (55.56) | |
| Day care time (months) | 14 (4–24) | 15 (4–24) | 14 (4–24) | 0.584 |
| Maternal age (years) | 29.99 ± 5.96 | 30.44 ± 6.03 | 29.56 ± 5.88 | 0.349 |
| Mother’s schooling (complete years) | 12 (12–15) | 12 (12–15) | 12 (12–16) | 0.826 |
| Father’s schooling (complete years) | 12 (10–12) | 12 (10–12) | 12 (10–13) | 0.818 |
| Economic class 5 | 0.912 | |||
| A or B | 54 (33.33) | 26 (48.15) | 28 (51.85) | |
| C, D, or E | 108 (66.67) | 53 (49.07) | 55 (50.93) | |
| Per capita income (Real 6) | 750 (500–1000) | 670.83 (500–1000) | 750 (450–1000) | 0.893 |
| Variable | MNP 3 | FS_FA 4 | p Value | |
|---|---|---|---|---|
| Iron deficiency 2 (n = 108) | Baseline | 72.09% (n = 54) | 70.12% (n = 54) | 0.821 |
| After intervention | 39.17% (n = 28) | 31.76% (n = 25) | 0.417 | |
| p value | <0.001 | <0.001 | ||
| Anaemia 1 (n = 22) | Baseline | 15.09% (n = 12) | 11.89% (n = 10) | 0.737 |
| After intervention | 1.30% (n = 1) | 1.34% (n = 1) | 0.339 | |
| p value | <0.001 | <0.001 |
| Variables | Time | Baseline | After Intervention | ||||
|---|---|---|---|---|---|---|---|
| Groups | MNP 1 | FS_FA 2 | p Value | MNP 1 | FS_FA 2 | p Value | |
| Hemoglobin (g/dL) (ni = 162; nf = 151) | Global | 11.68 ± 0.13 (n = 79) | 11.64 ± 0.14 (n = 83) | 0.909 3 | 12.90 ± 0.11 (n = 75) | 12.53 ± 0.12 (n = 76) | 0.142 3 |
| Anaemic | 10.78 ± 0.24 (n = 12) | 10.80 ± 0.27 (n = 10) | <0.001 4 | 13.17 ± 0.23 (n = 11) | 12.51 ± 0.24 (n = 10) | 0.080 4 | |
| Non anaemic | 12.58 ± 0.09 (n = 67) | 12.48 ± 0.09 (n = 73) | 12.62 ± 0.08 (n = 64) | 12.54 ± 0.08 (n = 66) | |||
| Serum ferritin (ng/mL) (ni = 161; nf = 152) | Global | 25.97 ± 2.29 (n = 78) | 26.13 ± 2.65 (n = 83) | 0.378 3 | 35.60 ± 2.33 (n = 76) | 33.14 ± 2.48 (n = 76) | 0.228 3 |
| Anaemic | 22.85 ± 4.29 (n = 12) | 21.07 ± 5.11 (n = 10) | 0.096 4 | 38.90 ± 4.36 (n = 11) | 29.36 ± 4.68 (n = 10) | 0.112 4 | |
| Non anaemic | 29.09 ± 1.77 (n = 66) | 31.19 ± 1.67 (n = 73) | 32.31 ± 1.76 (n = 65) | 36.93 ± 1.71 (n = 66) | |||
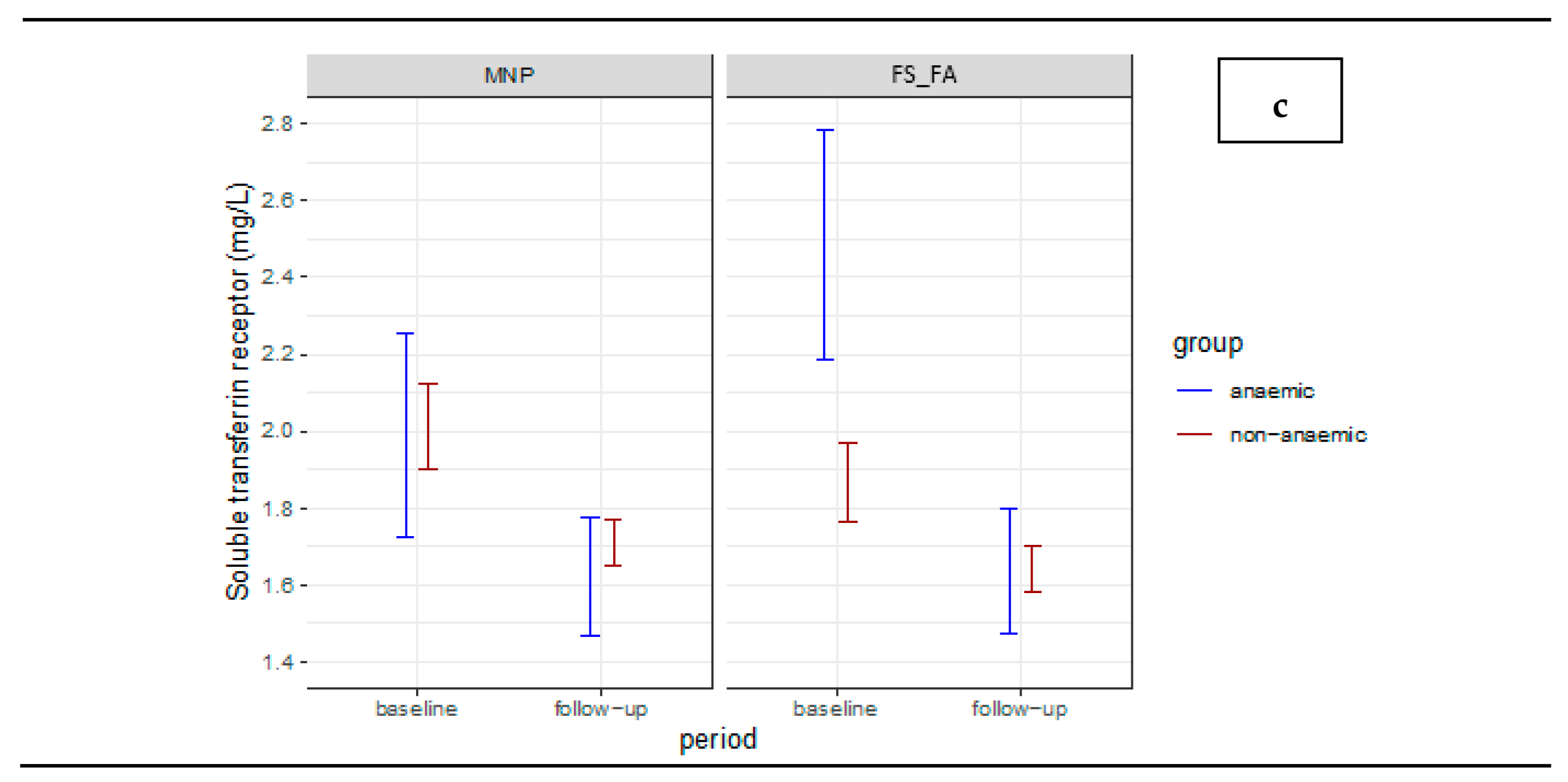
| Soluble transferrin receptor (mg/L) (ni = 161; nf = 150) | Global | 2.00 ± 0.07 (n = 78) | 2.18 ± 0.08 (n = 83) | 0.294 3 | 1.67 ± 0.04 (n = 74) | 1.64 ± 0.04 (n = 76) | 0.156 3 |
| Anaemic | 1.99 ± 0.13 (n = 12) | 2.48 ± 0.15 (n = 10) | <0.001 4 | 1.62 ± 0.07 (n = 10) | 1.64 ± 0.08 (n = 10) | 0.600 4 | |
| Non anaemic | 2.01 ± 0.05 (n = 66) | 1.87 ± 0.05 (n = 73) | 1.71 ± 0.03 (n = 64) | 1.64 ± 0.03 (n = 66) | |||
| Variables | MNP 2 | FS_FA 3 | p Value 4 | |
|---|---|---|---|---|
| Hemoglobin (g/dL) 5 | Global | 0.86 ± 0.17 (n = 75) d = 0.58 | 0.51 ± 0.18 (n = 76) d = 0.33 | |
| Anaemic | 1.52 ± 0.25 (n = 11) d = 1.83 | 0.87 ± 0.27 (n = 10) d = 1.02 | <0.001 | |
| Non anaemic | 0.19 ± 0.15 (n = 64) d = 0.16 | 0.17 ± 0.15 (n = 66) d = 0.14 | ||
| p value 6 | 0.382 | |||
| Serum ferritin (ng/mL) 7 (n = 143) | Global | 7.84 ± 2.59 (n = 75) d = 0.35 | 3.52 ± 2.77 (n = 76) d = 0.15 | |
| Anaemic | 12.01 ± 4.86 (n = 11) d = 0.75 | −0.24 ± 5.22 (n = 10) d = −0.01 | 0.107 | |
| Non anaemic | 3.67 ± 1.96 (n = 64) d = 0.23 | 7.29 ± 1.91 (n = 66) d = 0.47 | ||
| p value 6 | 0.558 | |||
| Soluble transferrin receptor (mg/L) 7 (n = 141) | Global | −0.30 ± 0.06 (n = 73) d = −0.59 | −0.44 ± 0.06 (n = 76) d = −0.84 | |
| Anaemic | −0.32 ± 0.12 (n = 10) d = −0.84 | −0.65 ± 0.12 (n = 10) d = −1.71 | 0.011 | |
| Non anaemic | −0.29 ± 0.05 (n = 63) d = −0.73 | −0.24 ± 0.05 (n = 66) d = −0.59 | ||
| p value 6 | 0.962 | |||
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Machado, M.M.A.; Lopes, M.d.P.; Schincaglia, R.M.; da Costa, P.S.S.; Coelho, A.S.G.; Hadler, M.C.C.M. Effect of Fortification with Multiple Micronutrient Powder on the Prevention and Treatment of Iron Deficiency and Anaemia in Brazilian Children: A Randomized Clinical Trial. Nutrients 2021, 13, 2160. https://doi.org/10.3390/nu13072160
Machado MMA, Lopes MdP, Schincaglia RM, da Costa PSS, Coelho ASG, Hadler MCCM. Effect of Fortification with Multiple Micronutrient Powder on the Prevention and Treatment of Iron Deficiency and Anaemia in Brazilian Children: A Randomized Clinical Trial. Nutrients. 2021; 13(7):2160. https://doi.org/10.3390/nu13072160
Chicago/Turabian StyleMachado, Malaine Morais Alves, Mirella de Paiva Lopes, Raquel Machado Schincaglia, Paulo Sérgio Sucasas da Costa, Alexandre Siqueira Guedes Coelho, and Maria Claret Costa Monteiro Hadler. 2021. "Effect of Fortification with Multiple Micronutrient Powder on the Prevention and Treatment of Iron Deficiency and Anaemia in Brazilian Children: A Randomized Clinical Trial" Nutrients 13, no. 7: 2160. https://doi.org/10.3390/nu13072160
APA StyleMachado, M. M. A., Lopes, M. d. P., Schincaglia, R. M., da Costa, P. S. S., Coelho, A. S. G., & Hadler, M. C. C. M. (2021). Effect of Fortification with Multiple Micronutrient Powder on the Prevention and Treatment of Iron Deficiency and Anaemia in Brazilian Children: A Randomized Clinical Trial. Nutrients, 13(7), 2160. https://doi.org/10.3390/nu13072160