


The Role of Energy Affordability in the Relationship between Poor Housing and Health Status



Abstract
1. Introduction
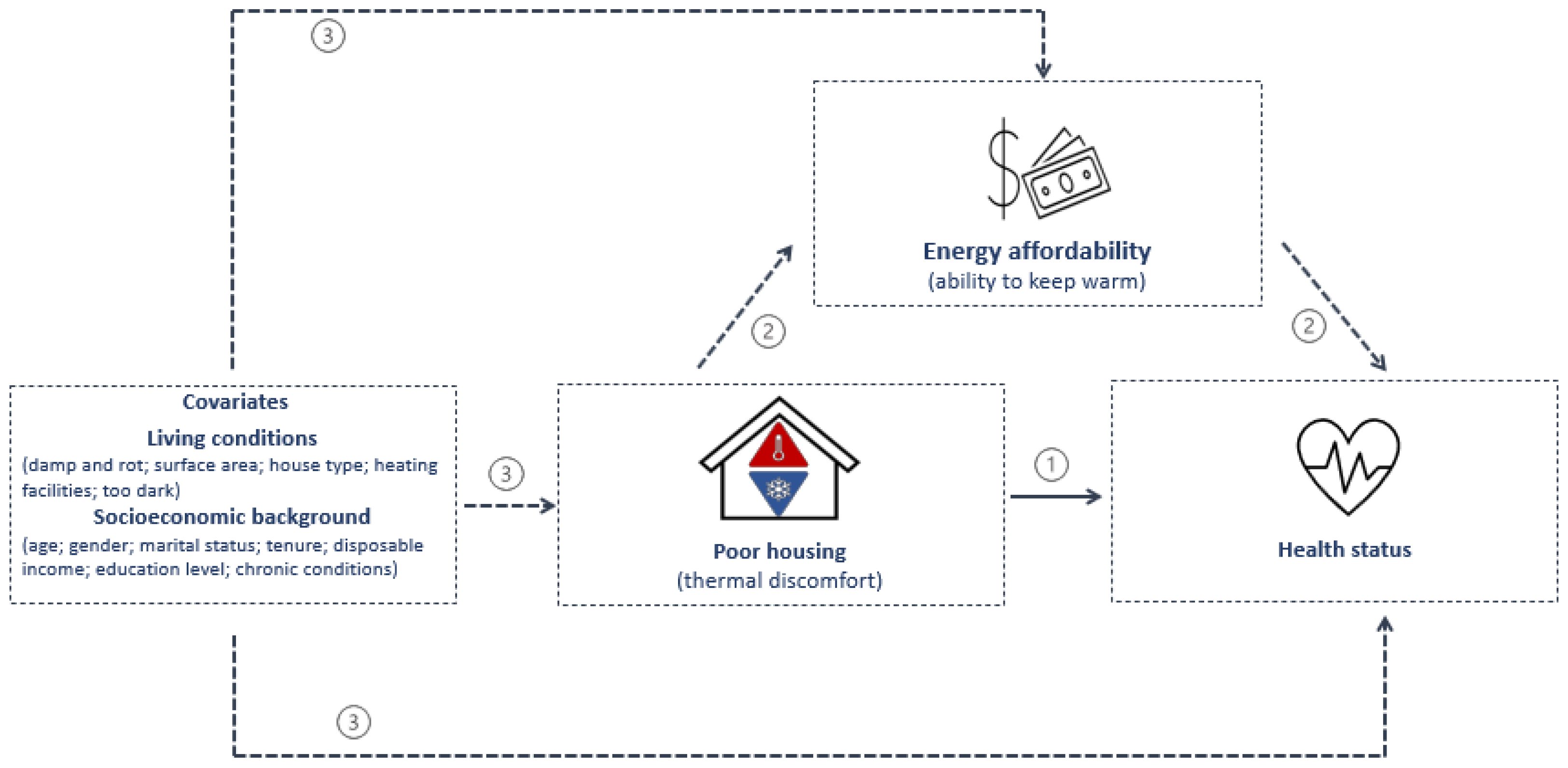
- What is the relationship between thermal discomfort and poor health status, according to socioeconomic background (e.g., age or income), using affordability as mediator?
- What is the portion of the overall effect that is allocated to each component of the ‘four-way decomposition’ analysis?
2. Literature Review
3. Materials and Methods
3.1. Dataset and Variables: Data Sources and Survey Description
3.2. Dataset and Variables: Dependent and Independent Variables and Summary Statistics
3.3. Model Specification
4. Results
5. Discussion
6. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- VELUX Group. Healthy Homes Barometer 2018: (Un)Healthy Homes, Offices, and Suburbanisation in Europe; VELUX: Hørsholm, Denmark, 2018. [Google Scholar]
- Bouzarovski, S.; Tirado Herrero, S. The energy divide: Integrating energy transitions, regional inequalities and poverty trends in the European Union. Eur. Urban Reg. Stud. 2017, 24, 69–86. [Google Scholar] [CrossRef] [PubMed]
- Petrova, S. Illuminating austerity: Lighting poverty as an agent and signifier of the Greek crisis. Eur. Urban Reg. Stud. 2017, 25, 360–372. [Google Scholar] [CrossRef] [PubMed]
- Ulucak, R.; Sari, R.; Erdogan, S.; Castanho, R.A. Bibliometric Literature Analysis of a Multi-Dimensional Sustainable Development Issue: Energy Poverty. Sustainability 2021, 13, 9780. [Google Scholar] [CrossRef]
- Al-Tal, R.; Murshed, M.; Ahmad, P.; Alfar, A.J.K.; Bassim, M.; Elheddad, M.; Nurmakhanova, M.; Mahmood, H. The Non-Linear Effects of Energy Efficiency Gains on the Incidence of Energy Poverty. Sustainability 2021, 13, 11055. [Google Scholar] [CrossRef]
- Stojilovska, A.; Guyet, R.; Mahoney, K.; Gouveia, J.P.; Castaño-Rosa, R.; Živčič, L.; Barbosa, R.; Tkalec, T. Energy poverty and emerging debates: Beyond the traditional triangle of energy poverty drivers. Energy Policy 2022, 169, 113181. [Google Scholar] [CrossRef]
- Magalhães, S.M.C.; Leal, V.M.S.; Horta, I.M. Predicting and characterizing indoor temperatures in residential buildings: Results from a monitoring campaign in Northern Portugal. Energy Build. 2016, 119, 293–308. [Google Scholar] [CrossRef]
- Simoes, S.; Gregório, V.; Seixas, J. Mapping Fuel Poverty in Portugal. Energy Procedia 2016, 106, 155–165. [Google Scholar] [CrossRef]
- Ramos, N.M.; Almeida, R.; Simões, M.L.; Delgado, J.; Pereira, P.F.; Curado, A.; Soares, S.; Fraga, S. Indoor hygrothermal conditions and quality of life in social housing: A comparison between two neighbourhoods. Sustain. Cities Soc. 2018, 38, 80–90. [Google Scholar] [CrossRef]
- Horta, A.; Gouveia, J.P.; Schmidt, L.; Sousa, J.C.; Palma, P.; Simões, S. Energy poverty in Portugal: Combining vulnerability mapping with household interviews. Energy Build. 2019, 203, 109423. [Google Scholar] [CrossRef]
- Energy Poverty Advisory Hub (EPAH). Introduction to the Energy Poverty Advisory Hub (EPAH) Handbooks: A Guide to Understanding and Addressing Energy Poverty; Energy Poverty Advisory Hub (EPAH): Brussels, Belgium, 2022. [Google Scholar]
- Vanderweele, T.J. A unification of mediation and interaction: A four-way decomposition. Epidemiology 2015, 25, 749–761. [Google Scholar] [CrossRef]
- European Commission. Methodological Guidelines And Description Of Eu-Silc Target Variables 2015 Operation, version 2014; European Commission: Brussels, Belgium, 2015. [Google Scholar]
- Eu-Silc Ad-Hoc Modules. AD-HOC MODULES. 2021. Available online: https://ec.europa.eu/eurostat/web/income-and-living-conditions/data/ad-hoc-modules (accessed on 6 May 2021).
- Santamouris, M.; Paravantis, J.A.; Founda, D.; Kolokotsa, D.; Michalakakou, P.; Papadopoulos, A.M.; Kontoulis, N.; Tzavali, A.; Stigka, E.K.; Ioannidis, Z.; et al. Financial crisis and energy consumption: A household survey in Greece. Energy Build. 2013, 65, 477–487. [Google Scholar] [CrossRef]
- Pevalin, D.J.; Reeves, A.; Baker, E.; Bentley, R. The impact of persistent poor housing conditions on mental health: A longitudinal population-based study. Prev. Med. 2017, 105, 304–310. [Google Scholar] [CrossRef] [PubMed]
- John, A.; Hermelink, A.; Galiotto, N.; Foldbjerg, P.; Eriksen KB, M.; Christoffersen, J. Study shows that unhealthy homes lead to reduced health. REHVA J. 2018, 3, 19–22. [Google Scholar]
- Fisk, W.J.; Singer, B.C.; Chan, W.R. Association of residential energy efficiency retrofits with indoor environmental quality, comfort, and health: A review of empirical data. Build. Environ. 2020, 180, 107067. [Google Scholar] [CrossRef]
- Ormandy, D.; Ezratty, V. Health and thermal comfort: From WHO guidance to housing strategies. Energy Policy 2011, 49, 116–121. [Google Scholar] [CrossRef]
- Heyman, B.; Harrington, B.E.; Merleau-Ponty, N.; Stockton, H.; Ritchie, N.; Allan, T.F. Keeping Warm and Staying Well Does Home Energy Efficiency Mediate the Relationship between Socio-economic Status and the Risk of Poorer Health? Hous. Stud. 2005, 20, 649–664. [Google Scholar] [CrossRef]
- Boomsma, C.; Pahl, S.; Jones, R.V.; Fuertes, A. “Damp in bathroom. Damp in back room. It’s very depressing!” exploring the relationship between perceived housing problems, energy affordability concerns, and health and well-being in UK social housing. Energy Policy 2017, 106, 382–393. [Google Scholar] [CrossRef]
- Chan, I.Y.; Liu, A.M. Effects of neighborhood building density, height, greenspace, and cleanliness on indoor environment and health of building occupants. Build. Environ. 2018, 145, 213–222. [Google Scholar] [CrossRef]
- Rodrigues, D.E.; César, C.C.; Xavier, C.C.; Caiaffa, W.T.; Proietti, F.A. Exploring neighborhood socioeconomic disparity in self-rated health: A multiple mediation analysis. Prev. Med. 2021, 145, 106443. [Google Scholar] [CrossRef]
- Hughes, C.; Natarajan, S.; Liu, C.; Chung, W.J.; Herrera, M. Winter thermal comfort and health in the elderly. Energy Policy 2019, 134, 110954. [Google Scholar] [CrossRef]
- Discacciati, A.; Bellavia, A.; Lee, J.J.; Mazumdar, M.; Valeri, L. Med4way: A Stata command to investigate mediating and interactive mechanisms using the four-way effect decomposition. Int. J. Epidemiol. 2019, 48, 15–20. [Google Scholar] [CrossRef] [PubMed]
- Lee, J.J.; Valeri, L.; Kapur, K.; Hasan, O.S.I.; Quamruzzaman, Q.; O Wright, R.; Bellinger, D.C.; Christiani, D.C.; Mazumdar, M. Growth parameters at birth mediate the relationship between prenatal manganese exposure and cognitive test scores among a cohort of 2- to 3-year-old Bangladeshi children. Int. J. Epidemiol. 2018, 47, 1169–1179. [Google Scholar] [CrossRef] [PubMed]
- Wolfson, J.; Stovitz, S.D.; Blair, S.N.; Sui, X.; Lee, D.-C.; Shrier, I. Decomposing the effects of physical activity and cardiorespiratory fitness on mortality. Glob. Epidemiol. 2019, 1, 100009. [Google Scholar] [CrossRef]
- Hallgren, M.; Vancampfort, D.; Owen, N.; Rossell, S.; Dunstan, D.W.; Bellocco, R.; Lagerros, Y.T. Prospective relationships of mentally passive sedentary behaviors with depression: Mediation by sleep problems. J. Affect. Disord. 2020, 265, 538–544. [Google Scholar] [CrossRef] [PubMed]
- Eurostat. EU-SILC Overview 2021. Available online: https://ec.europa.eu/eurostat/web/income-and-living-conditions (accessed on 6 May 2021).
- Instituto Nacional de Estatística. Inquérito às Despesas das Famílias 2015/2016; Instituto Nacional de Estatística: Madrid, Spain, 2017.
- European Commission Eurostat. Household Budget Survey: 2010 Wave EU Quality Report; European Commission Eurostat: Luxembourg, 2015. [Google Scholar]
- Kahouli, S. An economic approach to the study of the relationship between housing hazards and health: The case of residential fuel poverty in France. Energy Econ. 2019, 85, 104592. [Google Scholar] [CrossRef]
- Carmichael, L.; Prestwood, E.; Marsh, R.; Ige, J.; Williams, B.; Pilkington, P.; Eaton, E.; Michalec, A. Healthy buildings for a healthy city: Is the public health evidence base informing current building policies? Sci. Total Environ. 2020, 719, 137146. [Google Scholar] [CrossRef]
- Eurostat. Self-Perceived Health: Statistics Explained. 2021. Available online: https://ec.europa.eu/eurostat/statistics-explained/index.php?title=Glossary:Self-perceived_health (accessed on 6 July 2021).
- Angel, S.; Bittschi, B. Housing and Health. Rev. Income Wealth 2017, 65, 495–513. [Google Scholar] [CrossRef]
- Boch, S.J.; Taylor, D.M.; Danielson, M.L.; Chisolm, D.J.; Kelleher, K.J. ‘Home is where the health is’: Housing quality and adult health outcomes in the Survey of Income and Program Participation. Prev. Med. 2020, 132, 105990. [Google Scholar] [CrossRef]
- Lai, E.T.C.; Yu, R.; Woo, J. Social gradient of self-rated health in older people—the moderating/mediating role of sense of community. Age Ageing 2021, 50, 1283–1289. [Google Scholar] [CrossRef]
- Eurostat. EU-SILC: Data-Information on Data. 2021. Available online: https://ec.europa.eu/eurostat/web/income-and-living-conditions/data (accessed on 6 May 2021).
- Miguel-Bellod, J.S.; González-Martínez, P.; Sánchez-Ostiz, A. The relationship between poverty and indoor temperatures in winter: Determinants of cold homes in social housing contexts from the 40s–80s in Northern Spain. Energy Build. 2018, 173, 428–442. [Google Scholar] [CrossRef]
- Poortinga, W.; E Rodgers, S.; A Lyons, R.; Anderson, P.; Tweed, C.; Grey, C.; Jiang, S.; Johnson, R.; Watkins, A.; Winfield, T.G. The health impacts of energy performance investments in low-income areas: A mixed-methods approach. Public Health Res. 2018, 6, 1–182. [Google Scholar] [CrossRef] [PubMed]
- Eurostat. Equivalised Disposable Income: Statistics Explained. 2021. Available online: https://ec.europa.eu/eurostat/statistics-explained/index.php?title=Glossary:Equivalised_disposable_income (accessed on 6 June 2021).
- Eurostat. Income Quintile Group: Statistics Explained. 2021. Available online: https://ec.europa.eu/eurostat/statistics-explained/index.php?title=Glossary:Income_quintile_group (accessed on 6 June 2021).
- Miller, W.; Vine, D.; Amin, Z. Energy efficiency of housing for older citizens: Does it matter? Energy Policy 2017, 101, 216–224. [Google Scholar] [CrossRef]
- Arigoni, D. Preparing for an Aging Population: Factsheet; WHO Regional Office for the Western Pacific: Manila, Philippines, 2018. [Google Scholar]
- Vardoulakis, S.; Dimitroulopoulou, C.; Thornes, J.; Lai, K.-M.; Taylor, J.; Myers, I.; Heaviside, C.; Mavrogianni, A.; Shrubsole, C.; Chalabi, Z.; et al. Impact of climate change on the domestic indoor environment and associated health risks in the UK. Environ. Int. 2015, 85, 299–313. [Google Scholar] [CrossRef] [PubMed]
- Eurostat. EU-SILC: Metadata. 2021. Available online: https://ec.europa.eu/eurostat/cache/metadata/en/ilc_esms.htm (accessed on 6 May 2021).
- VanderWeele, T.J. Mediation Analysis: A Practitioner’s Guide. Annu. Rev. Public Health 2016, 37, 17–32. [Google Scholar] [CrossRef] [PubMed]
- SAS Institute Inc. SAS/STAT® 14.3 User’s Guide The CAUSALMED Procedure; SAS Institute: Cary, NC, USA, 2017. [Google Scholar]
- Russell, B.; Hemelrijck, M.V.; Gårdmark, T.; Holmberg, L.; Kumar, P.; Bellavia, A.; Häggström, C. A mediation analysis to explain socio-economic differences in bladder cancer survival. Cancer Med. 2020, 9, 7477–7487. [Google Scholar] [CrossRef]
- Bean, C.G.; Pingel, R.; Hallqvist, J.; Berg, N.; Hammarström, A. Poor peer relations in adolescence, social support in early adulthood, and depressive symptoms in later adulthood—evaluating mediation and interaction using four-way decomposition analysis. Ann. Epidemiol. 2019, 29, 52–59. [Google Scholar] [CrossRef]
- WHO. NCDs and Ageing; World Health Organisation: Geneva, Switzerland, 2021. Available online: https://www.who.int/westernpacific/about/governance/regional-director/ncds-and-ageing (accessed on 6 July 2021).
- WHO. World Health Organization—Noncommunicable Diseases (NCD) Country Profiles: Portugal; World Health Organisation: Geneva, Switzerland, 2018. Available online: https://www.who.int/nmh/countries/2018/prt_en.pdf?ua=1 (accessed on 5 October 2021).
- Palma, P.; Gouveia, J.P.; Simoes, S.G. Mapping the energy performance gap of dwelling stock at high-resolution scale: Implications for thermal comfort in Portuguese households. Energy Build. 2019, 190, 246–261. [Google Scholar] [CrossRef]
- Magalhães, S.A.; de Freitas, V.P. A complementary approach for energy efficiency and comfort evaluation of renovated dwellings in Southern Europe. Energy Procedia 2017, 132, 909–914. [Google Scholar] [CrossRef]
- Gouveia, J.P.; Seixas, J.; Long, G. Mining households’ energy data to disclose fuel poverty: Lessons for Southern Europe. J. Clean. Prod. 2018, 178, 534–550. [Google Scholar] [CrossRef]
- Delclós, C.; Vidal, L. Beyond renovation: Addressing Europe’s long housing crisis in the wake of the COVID-19 pandemic. Eur. Urban Reg. Stud. 2021, 28, 333–337. [Google Scholar] [CrossRef]
- Bulkeley, H.; Marvin, S.; Palgan, Y.V.; McCormick, K.; Breitfuss-Loidl, M.; Mai, L.; Von Wirth, T.; Frantzeskaki, N. Urban living laboratories: Conducting the experimental city? Eur. Urban Reg. Stud. 2018, 26, 317–335. [Google Scholar] [CrossRef]
- Ozarisoy, B.; Altan, H. Bridging the energy performance gap of social housing stock in south-eastern Mediterranean Europe: Climate change and mitigation. Energy Build. 2021, 258, 111687. [Google Scholar] [CrossRef]
- Barbosa, R.; Vicente, R.; Santos, R. Climate change and thermal comfort in Southern Europe housing: A case study from Lisbon. Build. Environ. 2015, 92, 440–451. [Google Scholar] [CrossRef]




{kind=link}
{kind=link}
{kind=link}
| Variables | General Health | House Type | Tenure status | Damp & Rot | Lack of Daylight | Ability to Keep Warm * | Heating Facilities | Warm during Winter ** | Cool during Summer | Surface Area | Urbanization Level | Gender | Age | Birthplace | Marital Status | Education Level | Household Size | Economic Status | Income Quintile | Chronic Conditions |
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Type | ||||||||||||||||||||
| Dependent | √ | |||||||||||||||||||
| Independent | √ | √ | √ | √ | √ | √ | √ | √ | √ | √ | √ | √ | √ | √ | √ | √ | √ | √ | √ | |
| Data collection | ||||||||||||||||||||
| Permanent | √ | √ | √ | √ | √ | √ | √ | √ | √ | √ | √ | √ | √ | √ | √ | √ | ||||
| Occasional | √ | √ | √ | √ | ||||||||||||||||
| * Proxy for energy affordability; ** Proxy for energy efficiency | ||||||||||||||||||||
| √ | poor housing conditions | √ socioeconomic conditions | ||||||||||||||||||
| Independent Variables | Categories | Percentage (%)/Mean | |
|---|---|---|---|
| Poor housing conditions | House type | Detached house * | 40.82 |
| Semi-detached or terraced house | 23.41 | ||
| Flat in a building ≤ 10 dwellings | 22.17 | ||
| Flat in a building ≥ 10 dwellings | 13.60 | ||
| Tenure status | Owner * | 50.90 | |
| Owner (mortgage) | 24.76 | ||
| Tenant (market rate) | 9.90 | ||
| Tenant (reduced rate) | 7.11 | ||
| Free accommodation | 7.33 | ||
| Damp and rot 1 | Yes * | 22.09 | |
| No | 77.91 | ||
| Too dark | Yes * | 10.94 | |
| No | 89.06 | ||
| Energy affordability | Yes * | 71.85 | |
| No | 28.15 | ||
| Heating facilities | Central heating * | 9.75 | |
| Other fixed heating | 33.99 | ||
| Non-fixed heating | 38.39 | ||
| No heating at all | 17.87 | ||
| Thermal comfort | Yes | 54.04 | |
| No * | 45.96 | ||
| Cool during summer | Yes | 66.14 | |
| No * | 33.86 | ||
| Surface area (m2) | continuous | 102.85 2 | |
| Urbanization level | Urban * | 34.29 | |
| Peri-urban | 28.24 | ||
| Rural | 37.47 | ||
| Socioeconomic background | Gender | Male * | 45.60 |
| Female | 54.40 | ||
| Age | (17–35) * | 9.35 | |
| (36/44) | 14.94 | ||
| (45/54) | 19.33 | ||
| (55/64) | 18.47 | ||
| (≥ 65) | 37.90 | ||
| Birthplace | Local * | 94.35 | |
| Other (EU) | 1.26 | ||
| Other (Non-EU) | 4.39 | ||
| Marital status | Never married * | 13.43 | |
| Married | 62.44 | ||
| Widowed | 15.90 | ||
| Divorced | 8.22 | ||
| Education level | Primary education * | 49.25 | |
| Secondary education | 24.85 | ||
| Tertiary education | 11.29 | ||
| No formal education | 14.61 | ||
| Household size (equivalized nº of household members) | continuous | 5.29 2 | |
| Economic status | Working full-time * | 32.58 | |
| Working part-time | 2.04 | ||
| Unemployed | 9.02 | ||
| Students | 1.72 | ||
| In retirement | 39.26 | ||
| Permanently disabled | 1.77 | ||
| Fulfilling domestic tasks and care responsibilities | 7.03 | ||
| Income quintile 3 | 1 (poorest) * | 13.73 | |
| 2 | 27.05 | ||
| 3 | 27.32 | ||
| 4 | 14.42 | ||
| 5 (richest) | 17.48 | ||
| Chronic disease | Yes * | 45.25 | |
| No | 54.75 |
| Decomposition Effect | Counterfactual Definition | Interpretation | Contextual Definition | |
|---|---|---|---|---|
| Total Effect (TE) | Total effect of exposure A (changing from ) on the outcome Y | Overall effect | What is the risk of poor health among those transitioning from thermal discomfort to thermal comfort? | |
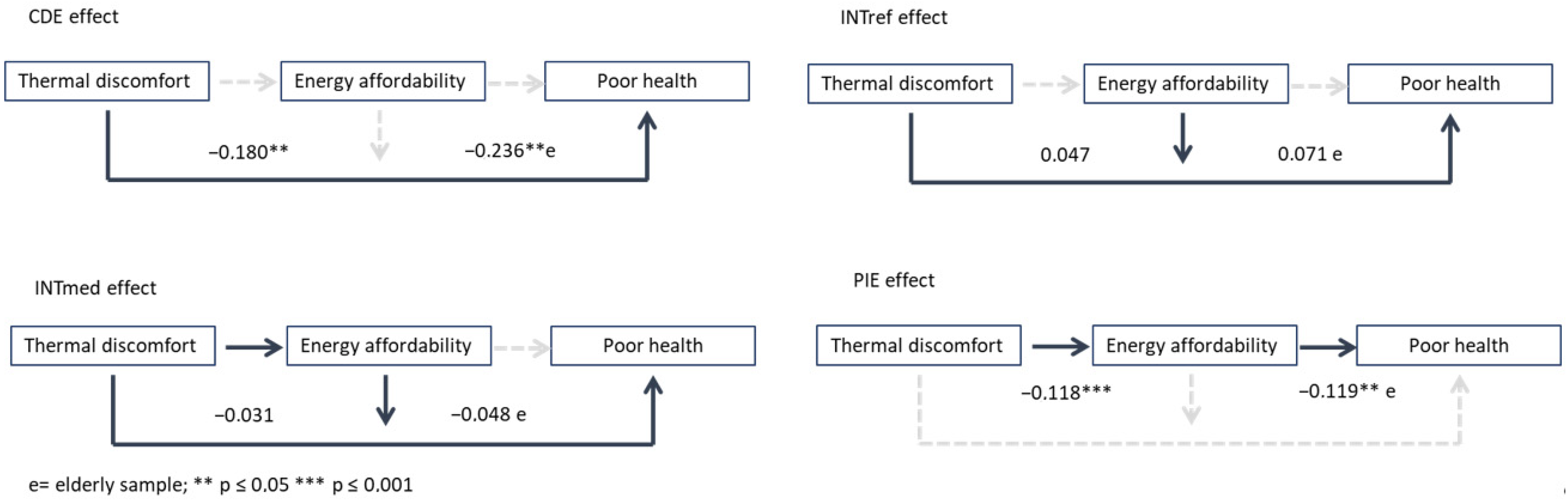
| Controlled Direct Effect (CDE) | ) | Effect of exposure A (changing from ) on the outcome Y, intervening to fix the mediator M to m | Due neither to mediation nor interaction | What is the risk of poor health among those transitioning from thermal discomfort to thermal comfort, if everyone is able to keep warm (has the same level of energy affordability)? |
| Reference Interaction ( | ) ( | An additive interaction that operates only if the mediator is present when exposure is a | Due to interaction only | What is the risk of poor health among those with thermal discomfort and affordability issues (inability to keep warm), if thermal discomfort does not have an effect on the energy affordability? |
| Mediated Interaction ( | ) ( | An additive interaction that operates only if the exposure A (changing from ) has an effect on the mediator M | Due to mediation and interaction | What is the combined risk of poor health among those with thermal discomfort and affordability issues (inability to keep warm), if thermal discomfort has an effect on the energy affordability? |
| Pure Indirect Effect (PIE) | )( | Effect of the mediator (changing from on the outcome Y when exposure A is a, multiplied by the effect of exposure A (changing from ) on the mediator M | Due to mediation only | What is the risk of poor health among those transitioning from thermal discomfort to thermal comfort and no affordability issues, if thermal discomfort has an effect on the energy affordability? |
| Overall Sample Decomposition Effects | β Coefficients (Std. Err.) | p-Value | PA (%) | Elderly Sample Decomposition Effects | β Coefficients (Std. Err.) | p-Value | PA (%) |
|---|---|---|---|---|---|---|---|
| Total effect (TE) | −0.282 (0.058) | ≤0.001 | 100 | Total effect (TE) | −0.332 (0.076) | ≤0.001 | 100 |
| Controlled direct effect (CDE) | −0.180 (0.069) | ≤0.008 | 64 | Controlled direct effect (CDE) | −0.236 (0.087) | ≤0.008 | 71 |
| ) | 0.047 (0.105) | ≤0.801 | −17 | ) | 0.071 (0.130) | ≤0.587 | −21 |
| ) | −0.031 (0.027) | ≤0.802 | 11 | ) | −0.048 (0.089) | ≤0.590 | 14 |
| Pure indirect effect (PIE) | −0.118 (0.030) | ≤0.001 | 42 | Pure indirect effect (PIE) | −0.119 (0.085) | ≤0.008 | 36 |
| Proportion attributable (PA) (%) | |||||||
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Lima, F.; Ferreira, P.; Leal, V. The Role of Energy Affordability in the Relationship between Poor Housing and Health Status. Sustainability 2022, 14, 14435. https://doi.org/10.3390/su142114435
Lima F, Ferreira P, Leal V. The Role of Energy Affordability in the Relationship between Poor Housing and Health Status. Sustainability. 2022; 14(21):14435. https://doi.org/10.3390/su142114435
Chicago/Turabian StyleLima, Fátima, Paula Ferreira, and Vítor Leal. 2022. "The Role of Energy Affordability in the Relationship between Poor Housing and Health Status" Sustainability 14, no. 21: 14435. https://doi.org/10.3390/su142114435
APA StyleLima, F., Ferreira, P., & Leal, V. (2022). The Role of Energy Affordability in the Relationship between Poor Housing and Health Status. Sustainability, 14(21), 14435. https://doi.org/10.3390/su142114435