Abstract
To better engage with patients, nurses need employ various communication skills, particularly “engagement strategies” that enable them to understand, elicit or empathize with patients’ concerns. Such engagement is essential to delivering good patient-centered care. This paper describes one part of a mixed-methods needs analysis: the aim was to find and analyze illustrative examples of actual nursing communication in English that showed engagement with between nurses and patients within an intercultural/international context in mainland China, where nurses are increasingly needing to interact with patients in English due to globalization. To confirm and concretely illustrate previously established engagement strategies found in the literature, direct observations were made of a nurse’s authentic interactions with a non-Chinese patient, which were then complemented by a post-observation interview. A detailed linguistic analysis of the data yielded a rich qualitative description of how engagement was practiced, along with quantitative data on the typical distribution and variety of communication strategies in everyday nurse-patient interactions. Drawing on Systemic Functional Linguistics (SFL), this paper details how various strategies for different speech functions were used within the different discourse moves of the interactions, and argues for a more central focus on the teaching of these useful engagement strategies and their patterns of use. The pedagogical benefits and clinical implications of this study will be apparent to practitioners of English for specific purposes (ESP) and nurse educators around the world who are involved in teaching nursing communication in English-medium or international contexts.
1. Introduction
1.1. Background on Engagement in Nursing Communication
Sustainable higher education can be understood in different ways, but one aspect has to do with ensuring that courses are designed to properly meet the needs of graduates in an increasingly globalized world, where the transnational flow of peoples and resources means, among other things, that we can no longer be satisfied with graduates who are only monolingually and monoculturally competent. This paper reports on one part of a research project aimed at improving the syllabus of an English communication course for nursing students at a higher education institution to ensure that it better meets the workplace needs of its graduates. The paper reports, in particular, on how data for the improved, more sustainable course was developed through needs analysis coupled with direct observations of an experienced nurse involved in intercultural/international communication with a patient. The analysis of the data revealed that expert nurses typically deploy a complex assortment of communication strategies at various stages of their interaction with patients in order to effectively engage with them and ensure patient satisfaction and good outcomes. Current communication courses for nurses, however, inadequately train nursing students for this complex task of communicative engagement, instead focusing on basic language proficiency. This may be a reflection of the fact that research on communication in health care settings has, to date, rather neglected the views and practices of nurses, privileging, instead, those of clinicians (doctors). In this section, we present background information on the important roles that nurses play and explain why their communication needs should be given more attention.
Nurses play an essential role in patient care since they are present in everyday health care settings [1] and perform many clinical tasks, ranging from routine work, such as dealing with medication, recording patients’ conditions, administering patients’ injections and collecting vital signs, to more complex and skilled activities, such as minor surgery and patient counselling [2]. Nurses thus have many opportunities to interact with patients and need to learn how to communicate with patients on many different health care-related topics to provide adequate care [3]. When communicating with patients, nurse practitioners typically use two distinct approaches, viz., the biomedical and the biopsychosocial [4]. Nurses who use the biomedical approach, which is known as the traditional approach, focus only on the signs and symptoms of the patient. They typically ask closed-ended questions which may merely elicit a “yes” or “no” response, and give patients directions to follow with little or no additional patient input [5]. In contrast, nurses who employ the biopsychosocial style of communication, known as the patient-centered communication approach, engage with patients by encouraging the sharing of the patients’ thoughts, feelings, and social needs, and by asking open-ended questions to prompt patient participation [5]. Adopting patient-centered communication helps nurses to achieve patient-centered care, which is, “respecting and responding to patients’ wants, needs and preferences, so that they can make choices in their care that best fit their individual circumstances” [6]. Patient-centered care has been identified as a key element of high-quality care in health care settings worldwide, and patient-centered communication is the primary means by which patient-centered care is accomplished [7]. In many places across the globe, such as in Australia, the United Kingdom, Hong Kong, and mainland China, patient-centered communication is officially regarded as essential to effective communication in clinical settings (Australia: [8]; UK: [9]; Hong Kong: [10]; USA: [11]; mainland China: [12]).
A number of large-scale international studies have linked patient-centered communication with positive patient care outcomes, including patient satisfaction [5,13,14], patient safety [15], patient adherence to recommended treatments [16], and improved clinical outcomes, such as the better management of hypertension [17], oncology [18], and cancer [19,20]. Despite these findings, it remains a challenge for health care providers to always provide patient-centered communication because of the general belief that it is time-consuming and difficult, and health care settings have time constraints and stressful working conditions [21]. Inadequate communication, however, can lead to serious consequences, including patient complaints [22] and malpractice claims [23]. Owing to the importance and challenges of patient-centered communication, the mastery of patient-centered communication skills is essential for health care providers, including nurses.
One essential component of patient-centered communication is nursing engagement with patients [24,25]: a nurse’s active or proactive efforts to interact with a patient through two-way, patient-centered, communication in order to ensure that the nurse is understood by the patient, can assist the patient in revealing any concerns they may have, and provide empathy and rapport with the patient [26]. A nurse who is able to engage with a patient can understand and elicit that patient’s specific health needs and desired health outcomes, thus leading to patient-centered care [20]. Our previous work [26] has suggested that when given proper communication training, nurses are able to engage effectively and efficiently with patients regardless of time constraints and stressful conditions. Engagement with patients does not necessarily take any more time than usual, and nurses can make full use of effective communication strategies even under stressful conditions when they are well-trained and habituated into communicating that way [26].
1.2. Perceptions/Practices of Engagement in Nursing Communication
Due to the significant role that engagement plays in nurses’ communication with patients, some studies have been conducted in this area [24,27,28]. Our review of the literature, however, reveals that many previous studies on perceptions and/or practices of engagement have not focused on spoken interactions and related communication skills, which are the primary ways through which nurses interact with patients in high-risk and urgent clinical contexts [29], as most of the established research has only been conducted from the perspectives of patients or clinicians rather than nurses. The research findings so far suggest that, although patients value nurses’ engagement with them [24,25], the nurses’ behaviors that patients (and the studies’ authors) regard as engagement, such as nurse availability when required by the patient, and nurse friendliness and warmth [30], do not all relate to communication skills or language skills. Regarding clinicians, our search of the literature turned up only two studies, Bright et al. [24] and Roe et al. [25], that explored clinicians’ perceptions of engagement. All the involved clinicians attached great significance to engagement in their clinical work, and language was identified as an important factor in clinician-patient engagement. However, the actual language use or communication strategies were not specifically identified in these studies.
With regard to actual practices, Bright et al. [24] observed conversations between rehabilitation practitioners (including speech-language therapists, occupational therapists, physiotherapists, doctors, and nurses, and rehabilitation or health care assistants), and patients during stroke rehabilitation to explore the processes of engaging with people with communication disabilities. Their findings highlighted that relational dialogue and supportive/encouraging conversation were important in practitioner-patient interactions. However, the authors made only very brief comments in their analyses of the conversations, such as the fact that the clinicians used simple questions to support the patient. No elaboration on specific communication strategies was given by the authors.
In summary, previous studies on engagement have fundamentally neglected the perspectives of nurses, focusing only on concepts indirectly related to engagement. For example, Yam and Rossiter [28] and Freihat and Al-Makhzoomi [31] addressed nurses’ interpersonal communication, which is a broader concept than engagement (for example, assertiveness, which refers to how an individual gets his/her point across without offending the other party, was part of Freihat and Al-Makhzoomi’s [31] exploration of interpersonal communication practices, and is not directly related to patient engagement). Another related study is Dong et al. [27], which investigated emotional and expressive practices, which are a part of engagement. Drawing on survey and interview data, it was found that nurses in China and other countries are aware of the importance of interpersonal and emotional/expressive practices to the achievement of good clinical outcomes and high-quality nursing care [27,28,32,33]. However, many nurses, especially those in mainland China, admitted that in practice, they often paid more attention to providing physical comfort or to doing physical tasks (e.g., taking vital signs) than offering emotional support (e.g., showing empathy; [27,32]). It is therefore important for nurses to learn necessary communication skills and strategies to better engage with patients, and this starts with the training of nursing students during their higher education studies.
One basic problem with existing nursing communication skills courses is that, from the perspectives of nursing teachers, clinical supervisors, and nursing students, a theory-practice gap exists: there is a discrepancy between what nursing students are taught in the classroom and what they actually needed during clinical practice. As Corlett [34] reported, supervisors and teachers expressed that although nursing students were told about the need for effective nurse-patient communication, when they graduated and started working, they found it difficult to actually interact and engage with patients. This is in part due to the fact that sample nursing conversations in the teaching materials are too simplistic and not geared towards the teaching of how to use language to engage with patients, whereas real-life nursing practice is more complex, and requires the accomplishment of multiple clinical and communicative goals simultaneously. Thus, there is an urgent need for experience-informed communication courses.
1.3. Teaching Engagement in ESP Nursing Communication
In this era of globalization, nurses find themselves needing to communicate with ever-increasing numbers of patients in English rather than the local language. ESP courses aim to address the language skills that learners need in order to be effective in their professions, and ESP courses for trainee nurses in non-English-speaking countries such as China present the best opportunities for nurses to learn the relevant language and communication skills that will enable them to carry out their job professionally. However, a majority of the current ESP nursing courses focus almost exclusively on basic elements of language proficiency rather than communication skills. For example, they teach vocabulary [35,36,37,38] or pronunciation [39,40]. They do not teach communication strategies, and do not have engagement as a specific communicative goal.
Such an approach betrays a rather old-fashioned view of language and language mastery. In a classic paper, Canale and Swain [41] expanded on earlier descriptions of communicative competence [42] and argued that successfully learning a language involves learning not only the vocabulary and grammar of a language (“grammatical competence”), but, crucially, also the sociolinguistic competence to use language appropriately according to audience and context, and the discourse and strategic competence to use longer stretches of language and communication strategies to achieve discourse goals. In order for English-medium higher education courses for nursing students to be sustainable and successful in achieving their goal of turning out communicatively competent nurses able to actively engage with international patients in English, ESP courses need to be revamped, to more explicitly teach communication strategies for patient engagement instead of narrowly focusing on grammatical competence. In fact, such a course has the potential to benefit currently practising nurses as well, as part of continuing professional development (CPD) programs, if nursing managers feel the need for such training to plug a perceived gap in communicative skills.
For the current study, a list of communication strategies that lead to engagement was collated, sorted, and categorized from the literature in the field (mainly [43,44,45]). These are engagement strategies that have been discovered and validated by researchers (many through observations of nurse-patient interactions) and provide an operational framework for identifying and classifying engagement strategies. The current study involved direct observation of the clinical interactions of a hospital nurse to see how these strategies actually work in practice, to both verify and exemplify the established set of strategies, using the data as the basis for an evidence-based, globally sustainable, fit-for-purpose ESP course that can better meet the needs of nursing students.
2. Materials and Methods
The current study on ESP nursing course development focuses on engagement, the needs analysis consisted of two phases. The first phase concerned the hospital nurses’ and nursing students’ perceptions of engagement, and the results of this have been reported elsewhere (Huang and Pun [26]). Here, we report the second phase: the collection of examples of actual nursing engagement in clinical practice, and detailed analyses of those encounters, using a mixed-methods approach combining the qualitative and the quantitative methods [46]. The aim in this second phase was to answer the following research questions (RQs):
RQ1.
How is engagement actually practiced by hospital nurses in nursing communication?
RQ2.
What specific communication strategy does the nurse adopt at each stage of an encounter and for what specific effect or engagement function?
2.1. Needs Analysis
Needs analyses are typically conducted to inform the design of ESP curricula (as suggested in Hafner and Miller [47] and Woodrow [48]). Many existing ESP courses had needs analyses conducted before their creation to elicit the target learners’ specific professional language needs. For ESP nursing, various stakeholders such as nursing students, ESP teachers and medical specialists [31,40,49,50] have been consulted to inform researchers about the language skills nurses need to acquire and the most challenging language features for nursing clinical practice [31]. For example, Staples [40] elicited views from nurses about pronunciation issues (e.g., the correct pronunciation of work-related terms) and then developed an ESP course that taught the necessary skills. Similarly, Gass [49] reviewed what specific language expressions were related to clinical tasks and developed an ESP course that taught nursing students language expressions that are commonly used in carrying out nursing tasks. Other ESP studies also gathered specific perceptions from nurses about their jobs and then developed specific ESP courses to train nurses in particular nursing communication skills [31,50].
2.2. Participants
The needs analysis reported in the current study involved interviewing and observing frontline hospital nurses who have extensive working experience and professional knowledge of clinical tasks, so that their views (Phase 1) and practices (Phase 2) of engagement could generate valuable insights for developing an improved, engagement-focused ESP course. The insights from Phase 1, combined with findings from previous related studies, yielded a comprehensive framework of communication strategies for achieving engagement with patients. In Phase 2, the aim was to gather authentic nurse-patient dialogues that could be linguistically analyzed and used for ESP materials development and pedagogy. Due to practical constraints, it was possible to directly shadow and observe only one nurse at Central Hospital of Huizhou from 28 February to 4 March, 2019. Nurse Nana (a pseudonym) was chosen to be observed during her interactions with a non-Chinese patient, as she had a rich clinical working experience as a frontline nurse (19 years) at the observed hospital. Her nurse supervisor commented that she always worked hard and did well in engagement with her patients. Thus, Nana’s interactions with her patients were analyzed in this project to inform the development of pedagogical materials on engagement strategies, and at the same time served as authentic dialogic data for the purpose of illustrating engagement strategies in the teaching materials. During the given observation period, Nana cared for a non-Chinese patient in the intensive care unit (ICU) of this hospital. Basic information about the patient is given in Table 1.

Table 1.
Background information on the involved patient.
It should be pointed out that although only one nurse and one patient were directly observed for this phase of the study, the actual set of engagement-related communication strategies used in this study and implemented in the resulting teaching materials were collated and adapted from previous related studies, as mentioned earlier, which were also based on clinical practice. In addition, experienced nurses were interviewed for this study and were asked to examine and validate the strategies and the analyses of the observational data. The data from the direct observations were thus meant only to be illustrative—for purpose of developing an engagement-focused ESP course containing authentic nurse-patient interactions.
2.3. Data Collection
Nana’s communication with this patient was observed, and during the analysis particular focus was placed on her engagement behaviors. An established observation schedule on nurse-patient interactions [51] was adapted for this study (see Appendix A.1 for the current observation guide). Four common and recurrent clinical scenarios were observed: measuring vital signs, administering injections, patient hygiene, and patient education. From these communicative events, empirical data were collected which were likely to be useful in accurately identifying the authentic linguistic and pragmatic requirements of the target situation [48]. These data were eventually used to inform the ESP course development.
During the period of observation, field notes, including what both Nana and Tony said in their conversations, were recorded for further analysis according to the observation guide. Since direct audio-/video-recording of nurse-patient interactions was not allowed at the observed hospital, it was only possible to use written notes to record as much as possible about the interactions, along with contemporaneous voice memos by the researcher (i.e., the first author recorded herself summarizing key observations and reflections on the communication patterns). Based on the notes and memos, the first author subsequently made transcriptions of what was said during the observed interactions, which were all in English, and the transcriptions were later checked by Nana for accuracy. As the researcher and observer, the first author adopted the approach of “observer as participant’’, and thus interacted with the participating patient only when it was necessary to clarify a particular situation or interaction, or to make the participant feel more at ease with the observation process [52]. The Hawthorne effect, where individuals modify their behaviors in response to their awareness of being observed [53,54], was not judged to be a major issue in this situation, as patient care was the priority for the observed nurse in this high-stakes clinical context, and the patient was focused on the nurse who was attending to his needs.
After the observations, Nana was invited to express her thoughts and feelings about her engagement with the patient in a post-observation interview where open-ended questions were used (see Appendix A.2). The post-observation interview took place one day after the week of observations to facilitate Nana remembering the observed interactions, and lasted about an hour. It was conducted in a quiet office where only Nana and the first author were present, and was audio-recorded for further analysis. This interview was conducted in Mandarin because Nana, who was a Mandarin speaker, could express her ideas more clearly and fluently in her mother tongue. This interview complemented the observations, giving us a better picture of the nurse’s engagement practices.
2.4. Data Analysis
The analysis of engagement practices had qualitative and quantitative components. For the qualitative part, discourse analysis was conducted to investigate the communication strategies used by the nurse to engage with the patient. For the purposes of this study, “discourse” refers to all forms of spoken interaction that construct social reality [55]. A Systemic Functional Linguistics (SFL) approach was adopted as an analytic framework for the discourse analysis in the present study. The key SFL component for the current study is speech function analysis, a powerful tool in the analysis of interaction, as it demonstrates how an interaction progresses [56,57,58,59]. The analytical procedures drew on Halliday and Matthiessen’s [60], Martin’s [58] and Eggins and Slade’s [56] research. The texts were coded into ‘Initiation, Response, Follow-up/Feedback (IRF)’ sequences first [61], each set of sequences constituting a typical exchange move structure in clinical spoken interactions. Each move in the ‘IRF’ sequence was then coded for the type of speech function it realized. This framework was developed and tested in an analysis of health care communication in Australia and has been refined for use in Hong Kong [62,63,64]. The reconstructed transcripts of what nurse Nana and the patient said during their interactions were manually coded for three layers: moves (using the IRF framework), speech functions (e.g., Offer, Command, Statement, Question), and communication strategies (e.g., ‘Offering spoken reassurance’). This combination of analyses was aimed at capturing nurse’s communicative acts of engagement and contextualizing them as serving purposive speech acts (speech functions) during the flow of different sequences (moves) of the interaction.
The speech function categories adopted for the current study are shown below, and are based on Halliday and Matthiessen [60], Martin [58] and Eggins and Slade [56]: five initiating speech functions (i.e., offer, command, statement, question and greeting) and their expected responses (see Table 2) or discretionary responses (see Table 3).
Table 2.
Speech function diagram I.
Table 3.
Speech function diagram II.
The speech function analysis was used only for analyzing the difference in speech roles played by the two parties. The third layer of discourse analysis involved the classification of the spoken communication strategies of engagement used by the nurse. The engagement strategies were manually coded according to a typology of strategies previously identified in the literature, and further confirmed and validated for this study through interviews with hospital nurses, who reflected on their own experiences of engagement. (see [26] for details). All the transcriptions and coding of the nurse-patient communication were checked carefully by three parties: the first author who is an ESP educator, a researcher in discourse analysis, and the third author, who is a professor of nursing and a nurse supervisor. To ensure the reliability of the coding process, Cohen’s kappa coefficient (k) was calculated three times for different data. The second coder was asked to independently identify the different moves of the ‘IRF’ sequence in the data, and established an inter-rater reliability of (k > 0.8) with the first author. The second coder also identified the speech functions for each move, and established an inter-rater reliability of (k > 0.8) with the first author. The third author independently coded the engagement strategies, and established an inter-rater reliability of (k > 0.8) with the first author. Discrepancies were resolved through discussions until agreement was reached.
Table 4 below is presented as an example to show how the three-layered analytical framework was used to illuminate the nursing engagement practices. The interaction below represents a few minutes of a typical nursing scenario of a nurse administering an injection. This detailed analysis shows how the layers of analysis dovetailed with each other.
Table 4.
Selected nurse-patient conversations in administering injections.
For the quantitative arm of this study, statistical analysis was used to investigate the frequency and variety of engagement strategies used by the nurse in the data.
2.5. Ethical Consideration
Ethics approval for this project was obtained from the ethics committee of the authors’ institutions before the study began. The research project was explained to Nana beforehand, detailing the project objectives, research plan, and methods of data collection. Ethical requirements for this kind of observation were also explained in detail, including how participants’ confidentiality would be ensured and how participants could access the raw collected interactional data. Nana then explained the study to the involved patient, Tony, introducing the role of the observer and providing details about the aims of research and how his data would be used. Their written consent to participate in the research project and to have their conversations observed and studied was obtained before the observations began.
3. Results
3.1. Analysis of Engagement Strategies
The analysis of the data revealed that Nana adopted a wide variety of engagement strategies with the patient. These strategies were in line with what was established in the literature and can be classified as having three main purposes: improving patients’ understanding (e.g., through spontaneously offering information), eliciting patients’ concerns (e.g., by asking open-ended questions), and establishing empathy and rapport with patients (e.g., by stating an intention to help and support). Among these three types, Nana used the strategies for establishing empathy and rapport with the patient 99 times during the observations, making it the most frequent type of engagement (see Figure 1).
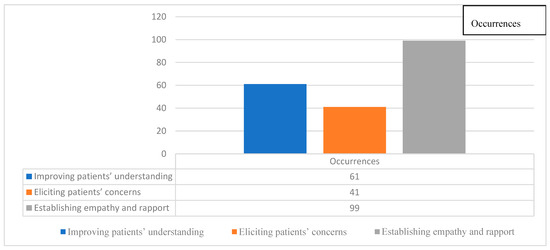
Figure 1.
Frequencies of communication strategies for different types of engagement.
Figure 2a,b and Table 5 show the communication strategies used, from the most to the least frequent. Overall, a total of seventeen different engagement strategies were adopted by Nana to engage with the patient. Table 5 classifies each of the identified strategies into one of the three main types or purposes of engagement and also includes an authentic example taken from the data. The utterances highlighted in bold are the ones that enact the engagement functions. For example, before taking his temperature, Nana said to the patient, “I will measure your axillary temperature, so first, I need to wipe off the sweat under your armpit.” In saying the highlighted utterance, she used the strategy of expressing care or/and concerns in the first person which falls under the engagement purpose category of “establishing empathy and rapport with the patient”.
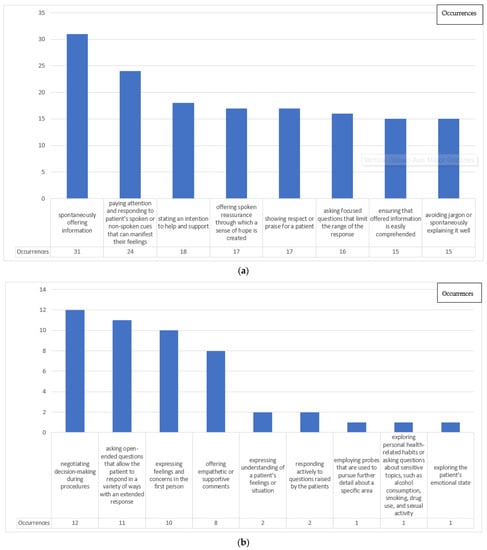
Figure 2.
(a,b) Frequencies of each engagement strategy.
Table 5.
Engagement strategies used to engage with the patient.
As Table 5 shows, the strategy of spontaneously offering information, which has the engagement function of improving patients’ understanding, was used most frequently among all seventeen strategies. Based on Nana’s post-observation interview, this high frequency is probably because of the fact that most patients come to the hospital in order to find out what is wrong with their bodies and thus are always anxious and eager to have as much information about their condition as they can, but they may not know how to ask questions due to the lack of medical knowledge. Thus, spontaneously offering all kinds of information is one of the nurse’s main roles [65]. Since this strategy aims mainly to provide information to patients, such as informing the patient of their body temperature, it does not belong to the most frequently used type of engagement practice: establishing empathy and rapport with patients (see Figure 1). Further, only four of the ten most frequently used strategies are for the most frequently used type of engagement practice, as shown in Table 5. That is, the most frequently used strategies do not necessarily concern the most frequently performed function of engagement, which is to establish empathy and rapport. This is possibly because there is a wider variety of communication strategies used to establish empathy and rapport, which altogether add up to make “establish empathy and rapport” the most common type of engagement.
With regard to the variety of communication strategies used by Nana, there were, respectively, 3, 5 and 9 different strategies used to improve patients’ understanding, elicit patients’ concerns and establish empathy and rapport (see Figure 3). She used the richest variety of communication strategies for establishing empathy and rapport with her patient. This category, mentioned earlier, is also Nana’s most frequently used type of engagement practice. Meanwhile, among these three functions of engagement, eliciting patients’ concerns happened least frequently (see Figure 1), although this engagement type included the second richest variety of communication strategies in the data (see Figure 3).
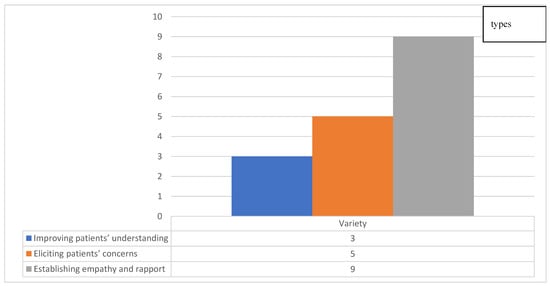
Figure 3.
Type of engagement versus variety of communication strategy.
3.2. Move Analysis
In terms of ‘IRF’ moves, the distribution of Nana’s engagement strategies was not even across the different moves, as shown in Table 6. The highest density of her engagement strategies was during the move of Initiation (76.74%), followed by Response (50%) and Follow-up (33.33%). That is, 76.74% of Nana’s Initiation moves showed engagement with the patient, or, from another angle, 80.5% of all her engagement-related moves (82) were during the Initiation stage of her exchanges (66). These results suggest that a nurse is more likely to construct engagement in his/her initiation moves.
Table 6.
Frequencies of engagement strategies in each move.
As for the moves that were Response, although half of hers concerned engagement, Nana only made 2 responses during the observations, while the other responses were all made by the patient. This indicates that, compared with the patient, the nurse is more likely to lead the interactions with the patient, possibly due to the nature of the job. According to the literature, one of the nurse’s roles is to be responsible for appropriate conduct of the interaction with the patient even though nurse-patient engagement is bidirectional during their communication [24,25], because the patient often enters the interaction while experiencing stress and anxiety [66] or without knowing enough to ask certain questions [67].This reason can also explain why nurses, as carers, are expected by patients to be the ones in charge in nurse-patient interactions. Such asymmetrical nurse-patient relationships, especially in Asian contexts, were also reflected in previous studies such as the research conducted by Ishikawa and Yamazaki [68]. Based on the above analyses, it makes sense to focus the teaching of engagement strategies on the moves of Initiation or Follow-up.
In the qualitative analyses of the moves, it was found that nurse always adopted more than one strategy to enact engagement within a move. For example, in an initiation move during the scenario of patient education, Nana said, “I will personally transfer you to the Department of Respiratory Medicine, and I will see you when I have time.” In this example, Nana simultaneously used three different communication strategies to engage with the patient. She stated an intention to help the patient transfer to another department, used the first person to express her concerns for the patient, and then offered spoken reassurance, telling the patient that she would visit him later.
3.3. Speech Function Analysis
As for speech functions, we report only on the most salient features. First, all Nana’s initiating open-ended questions, such as “How do you feel today?”, served to enact engagement (see Table 7), since the strategy of using such questions is to allow the patient to respond in a variety of ways with extended responses, and thus realize the purpose of eliciting patients’ concerns. Beyond this, some other strategies of engagement also involved open-ended questions. Table 8 presents these strategies and corresponding examples that include open-ended questions (see the words highlighted in bold). These examples are from different scenarios, labeled in square brackets, in the observed nurse-patient interactions.
Table 7.
Frequencies of engagement-oriented open and yes/no questions.
Table 8.
Engagement strategies that can use open-ended questions.
Second, as Table 7 shows, a large proportion of the yes/no questions initiated by Nana (88.89%) also concerned engagement. This suggests that, in addition to open-ended questions, yes/no questions can also be used to promote engagement (e.g., “Is it comfortable for you to lie like this?”), even though this type of question has been widely characterized as typically eliciting minimal information [5]. Table 9 shows the communication strategies that can involve the use of yes/no questions to engage with patients, and corresponding examples from the data.
Table 9.
Communication strategies using yes/no questions to engage with patients.
3.4. Post-Observation Comments
All of the findings discussed above were confirmed by Nana in the post-observation interview when she commented on her own performance of engagement in the observed scenarios. Overall, she was satisfied with how she engaged with the patient through the various communication strategies. Nana also saw a real need for students to learn related communication strategies that would help them engage more with patients, especially non-Chinese patients. As she said, They are more likely to feel anxious and lonely, being in a foreign country, and thus might appreciate a greater level of engagement with nurses.
For these reasons, she stressed the importance of ESP nursing courses having a focus on engagement, Such ESP courses represent the main opportunities for nursing students to learn about how to engage with non-Chinese patients in English.
Nana suggested that such courses should not focus on teaching words and phrases as things to only memorize in a context-free way, but as communication strategies embedded within the context of achieving the important nursing objectives of patient engagement and patient satisfaction. Such a course would show how each utterance or sentence serves to achieve specific engagement goals, thus better ensuring that our future nurses will not only survive but thrive in the workplace, which would be the goal of any sustainable ESP course: enabling nurses to consistently be good communicators who engage interactively with patients, instead of basic communicators who can just get by. Nana, along with other nurses interviewed for this project [26], also suggested that these strategies should be taught using authentic dialogues based on real-life interactions between experienced nurses and their patients, which is precisely what was collected in the current project.
4. Discussion
Through the above analyses, the actual engagement practices of an experienced nurse were explored both quantitatively and qualitatively. The quantitative analysis showed that, among the three types of communication strategies, the nurse used the strategies for establishing empathy and rapport with patients most frequently, and with the greatest variation in strategy. This result chimed with our previous study of nurses’ perceptions regarding engagement [26]. The nurse interviewees in that study also felt that the category of “establishing empathy and rapport with patients” had the widest variety of communication strategies [26]. This finding indicates that teaching strategies for establishing empathy and rapport with patients is more difficult and complicated because there are so many different ways/different strategies to achieve this end. This finding is also in line with the study by Shao et al. [69] who found that communicating empathetically was not always a straightforward undertaking for nurses. For example, nurses may lack the ability to recognize the emotional cues of patients in order to empathetically respond [70]. Several studies conducted at hospitals in China also reported that nurses often had limited ability to evaluate the emotional state of patients [71,72]. Moreover, communication may be adversely impacted if nurses miss or ignore the opportunity to express empathy owing to their busy work schedules [73]. In addition, patients under stress usually do not fully express their feelings to nurses [74]. These obstacles suggest that it is necessary to teach nurses to develop the habit of using proactive empathetic communication skills: perhaps they can learn to do more of “Eliciting patients’ concerns” during their initiation moves, to ensure that they do not miss these concerns, before they can respond with “Establishing empathy and rapport”. When nurses have the proper training, and start using the strategies as a matter of routine, the habitual nature of their use will help overcome the abovementioned obstacles. The evidence-based engagement strategies developed in the current study (as can be seen in Figure 2a,b or Table 5), therefore, will be a valuable contribution to the field, and will help not only novice nurses and nursing students but also currently practising nurses if taught as part of a professional development program.
The majority of the communication strategies identified in the observational data, such as showing respect or expressing praise for a patient [45,69], have been listed in existing literature. However, there appeared to be a new strategy not previously described. Consider the following scenario where the nurse is about to administer an injection (see Table 10).
Table 10.
An example of the observed nurse-patient conversation involving the new strategy.
In this example, the nurse asked the patient about his preference for an injection site, thus involving the patient in the decision-making process. This helped the nurse to elicit what could have been a concern of the patient, and encouraged him to express himself more and take a bigger role in what was happening. This strategy was also found in a previous study on effective communication between patients and clinicians in some Australian emergency departments, although that study was conducted on clinicians rather than nurses [75]. In the current study, this strategy was used by a nurse, and we have labelled this “negotiating decision-making during procedures”. It will be useful to teach this to nurses as strategy to engage with patients and elicit what their wishes are Patients will be encouraged to express themselves more and get more involved in their own health care.
5. Conclusions
The results of this needs analysis answered RQ1 and RQ2, by exploring a frontline hospital nurse’s current engagement practices and comparing it with what has been found in the literature. The multiple strategies the observed nurse used to engage with her non-Chinese patient in the hospital observations were identified, classified, and further examined using move analysis and speech function analysis. These analyses provide us with a detailed picture of the various speech functions that realize engagement and how they are used at various stages of nurse-patient interactions. The speech function analysis in conjunction with the identification of specific engagement strategies form a good organizing framework for a language syllabus [76] As part of this project, the detailed three-layered analyses were fed into the materials development of an ESP nursing course focused on engagement. Details on the development and post-implementation evaluation of that engagement-focused course will be published separately, but it can be noted here that a first trial run of the engagement-focused course on a group of nursing students resulted in a marked increase in awareness and appreciation of the importance of nurse-patient engagement, accompanied by a significant increase in the usage of engagement strategies by the students. Those results validate the usefulness of the needs analysis and discourse analyses of authentic interactions discussed in the current paper, where the focus was on showing the kinds of analysis can be done to plug a gap in current ESP courses on nursing communication to make them more sustainable and fit for purpose.
This study is one of the first to specifically focus on Chinese nurses’ engagement practices. The findings will have a positive influence on future nurses if implemented in ESP courses, as the use of engagement strategies can ensure patient-centered communication, which research has shown leads to positive clinical outcomes [14,77,78,79]. Further, the communication strategies and authentic examples provided in this study can help novice nurses quickly adapt to the real-world clinical environment and improve the quality of their nursing care. This is because the strategies are highly practical and authentic, being based on hospital observations.
The findings reported in this study are not limited to the specific research setting and participants: they are highly applicable to many other contexts, whatever the language situation or nurse-patient profile. Whether it is nurses in English-speaking countries speaking to patients from a non-English background, or nurses in China speaking Mandarin to Chinese patients, nurses can be trained to take a more proactive and active role in communicating with patients, deploying these strategies to better engage with patients from any background. It is hoped that future studies will apply these findings to new contexts, extending and adapting them to various national or intercultural situations, and provide further validation that such engagement-focused and workplace-relevant training can result in better, more sustainable higher education outcomes for nursing students.
Author Contributions
Conceptualization, Q.H., J.P. and S.H.; Methodology, Q.H. and J.P.; Software, Q.H.; Validation, Q.H., J.P. and S.H.; Formal Analysis, Q.H.; Investigation, Q.H. and S.H.; Data Curation, S.H.; Writing—Original Draft Preparation, Q.H.; Writing—Review & Editing, Q.H. and J.P. All authors have read and agreed to the published version of the manuscript.
Funding
This research received no external funding.
Institutional Review Board Statement
The study was conducted according to the guidelines of the Declaration of Helsinki, and approved by the Ethics Committees of Huizhou Health Sciences Polytechnic (2015003, approved December 2018) and City University of Hong Kong (53717971, approved 10 December 2018).
Informed Consent Statement
Informed consent was obtained from all subjects involved in the study.
Data Availability Statement
The data used during this study are available from the corresponding author, upon request by e-mail.
Acknowledgments
We would like to thank all the participants in this research, and Qianwen Joyce Yu from City University of Hong Kong and David Lee for their valuable advice on the manuscript.
Conflicts of Interest
The authors declare no conflict of interest.
Appendix A
Appendix A.1. The Observation Guide for Nursing Engagement with Patients
Table A1.
The Observation Guide for Nursing Engagement with Patients.
Table A1.
The Observation Guide for Nursing Engagement with Patients.
| Date: | |||||
|---|---|---|---|---|---|
| Time | Place | Clinical Tasks | Nurse/Patient’s Talk | Functions of Talk | Comments |
Appendix A.2. Post-Observation Interview Questions
- What was the purpose of your saying this?
- During this nurse-patient interaction, did you have any specific spoken strategy to better understand patients’ ideas?
- During this nurse-patient interaction, did you say anything to make yourself better understood by your patients?
- During this nurse-patient interaction, did you say anything to elicit as many patients’ concerns as possible, especially about their emotional needs?
- During this nurse-patient interaction, did you say anything to build empathy and rapport with the patient?
- Can you comment on your engagement practices during this nurse-patient interaction?
References
- Candlin, S.; Roger, P. Communication and Professional Relationships in Healthcare Practice; Equinox Publishing: Sheffield, UK, 2013. [Google Scholar]
- Harvey, K.; Koteyko, N. Exploring Health Communication: Language in Action; Routledge: New York, NY, USA, 2013. [Google Scholar]
- Fleischer, S.; Berg, A.; Zimmermann, M.; Wüste, K.; Behrens, J. Nurse-patient interaction and communication: A systematic literature review. J. Public Health 2009, 17, 339–353. [Google Scholar] [CrossRef]
- Charlton, C.R.; Dearing, K.S.; Berry, J.A.; Johnson, M.J. Nurse practitioners communication styles and their impact on patient outcomes: An integrated literature review. J. Am. Acad. Nurse Pract. 2008, 20, 382–388. [Google Scholar] [CrossRef] [PubMed]
- Anderson, E.B. Patient-centeredness: A new approach. Nephrol. News Issues 2002, 16, 80–82. [Google Scholar] [PubMed]
- Committee on Quality of Health Care in America. Crossing the Quality Chasm: A New Health System for the 21st Century; National Academies Press: Washington, DC, USA, 2001. [Google Scholar]
- McCormack, L.A.; Treiman, K.; Rupert, D.; Williams-Piehota, P.; Nadler, E.; Arora, N.K.; Lawrence, W.; Street, R.L. Measuring patient-centered communication in cancer care: A literature review and the development of a systematic approach. Soc. Sci. Med. 2011, 72, 1085–1095. [Google Scholar] [CrossRef] [PubMed]
- Australian Commission on Safety and Quality in Health Care. Patient-Centred Care: Improving Quality and Safety through Partnerships with Patients and Consumers. Available online: https://www.safetyandquality.gov.au/wp-content/uploads/2012/03/PCC_Paper_August.pdf (accessed on 18 June 2022).
- Department of Health. Treating Patients as People. Available online: https://www.gov.uk/government/speeches/treating-patients-as-people (accessed on 18 June 2022).
- Hospital Authority. Hospital Authority Strategic Plan 2017–2022. Available online: http://www.ha.org.hk/haho/ho/cad_bnc/AOM-P1236.pdf (accessed on 18 June 2022).
- National Academy of Medicine. Crossing the Quality Chasm: A New Health System for the 21st Century; National Academies Press: Washington, DC, USA, 2001. [Google Scholar]
- National Health Commission of the People’s Republic of China. Improving Patient Satisfaction with High-Quality Nursing Services. Available online: http://www.nhc.gov.cn/yzygj/s10006/201301/0b824411fa464505a9ed48de232c0be4.shtml (accessed on 18 June 2022).
- Fortin, A.H. Communication skills to improve patient satisfaction and quality of care. Ethn. Dis. 2002, 12, 58–61. [Google Scholar]
- Price, E.G.; Cooper, L.A. Hypertension in African Americans: Strategies to help achieve blood pressure goals. Consultant 2003, 43, 1330–1336. [Google Scholar]
- Anthony, M.K.; Preuss, G. Models of care: The influence of nurse communication on patient safety. Nurs. Econ. 2002, 20, 209–215. [Google Scholar]
- Nitzan, U.; Hirsch, E.; Walter, G.; Lurie, I.; Aviram, S.; Bloch, Y. Comprehension and companionship in the emergency department as predictors of treatment adherence. Australas. Psychiatry 2012, 20, 112–116. [Google Scholar] [CrossRef]
- Mead, N.; Bower, P. Patient-centred consultations and outcomes in primary care: A review of the literature. Patient Educ. Couns. 2002, 48, 51–61. [Google Scholar] [CrossRef]
- Bredart, A.; Bouleuc, C.; Dolbeault, S. Doctor-patient communication and satisfaction with care in oncology. Curr. Opin. Oncol. 2005, 17, 351–354. [Google Scholar] [CrossRef]
- Arora, N.K. Interacting with cancer patients: The significance of physicians’ communication behavior. Soc. Sci. Med. 2003, 57, 791–806. [Google Scholar] [CrossRef]
- Epstein, R.M.; Street, R.L. Patient-Centered Communication in Cancer Care: Promoting Healing and Reducing Suffering; National Cancer Institute: Bethesda, MD, USA, 2007. [Google Scholar]
- Sheldon, L.K.; Barrett, R.; Ellington, L. Difficult communication in nursing. J. Nurs. Scholarsh. 2006, 38, 141–147. [Google Scholar] [CrossRef] [PubMed]
- Kee, J.W.Y.; Khoo, H.S.; Lim, I.; Koh, M.Y.H. Communication skills in patient-doctor interactions: Learning from patient complaints. Health Prof. Educ. 2018, 4, 97–106. [Google Scholar] [CrossRef]
- Huntington, B.; Kuhn, N. Communication gaffes: A root cause of malpractice claims. Bayl. Univ. Med. Cent. Proc. 2003, 16, 157–161. [Google Scholar] [CrossRef] [PubMed]
- Bright, F.A.S.; Kayes, N.M.; McPherson, K.M.; Worrall, L.E. Engaging people experiencing communication disability in stroke rehabilitation: A qualitative study. Int. J. Lang. Commun. Disord. 2018, 53, 981–994. [Google Scholar] [CrossRef]
- Roe, Y.L.; Zeitz, C.J.; Fredericks, B. Study protocol: Establishing good relationships between patients and health care providers while providing cardiac care. Exploring how patient-clinician engagement contributes to health disparities between indigenous and non-indigenous Australians in South Australia. BMC Health Serv. Res. 2012, 12, 397. [Google Scholar] [CrossRef]
- Huang, Q.; Pun, J. Views of Hospital Nurses and Nursing Students on Nursing Engagement—Bridging the Gap Through Communication Courses. Front. Psychol. 2022, 13. [Google Scholar] [CrossRef]
- Dong, F.; Zheng, R.; Chen, X.; Wang, Y.; Zhou, H.; Sun, R. Caring for dying cancer patients in the Chinese cultural context: A qualitative study from the perspectives of physicians and nurses. Eur. J. Oncol. Nurs. 2016, 21, 189–196. [Google Scholar] [CrossRef]
- Yam, B.M.C.; Rossiter, J.C. Caring in nursing: Perceptions of Hong Kong nurses. J. Clin. Nurs. 2000, 9, 293–302. [Google Scholar] [CrossRef]
- Pangaltsos, A. Medical Thought; M. Barbounaki: Thessaloniki, Greece, 2011. [Google Scholar]
- Kralik, D.; Koch, T.; Wotton, K. Engagement and detachment: Understanding patients’ experiences with nursing. J. Adv. Nurs. 1997, 26, 399–407. [Google Scholar] [CrossRef]
- Freihat, P.S.; Al-Makhzoomi, K. An English for specific purposes (ESP) course for nursing students in Jordan and the role a needs analysis played. Int. J. Humanit. Soc. Sci. 2012, 2, 129–145. [Google Scholar]
- Pun, J.K.H.; Chan, E.A.; Murray, K.A.; Slade, D.; Matthiessen, C.M.I.M. Complexities of emergency communication: Clinicians’ perceptions of communication challenges in a trilingual emergency department. J. Clin. Nurs. 2016, 26, 3396–3407. [Google Scholar] [CrossRef] [PubMed]
- Pun, J.K.H.; Chan, E.A.; Wang, S.; Slade, D. Health professional-patient communication practices in East Asia: An integrative review of an emerging field of research and practice in Hong Kong, South Korea, Japan, Taiwan, and Mainland China. Patient Educ. Couns. 2018, 101, 1193–1206. [Google Scholar] [CrossRef] [PubMed]
- Corlett, J. The perceptions of nurse teachers, student nurses and preceptors of the theory-practice gap in nurse education. Nurse Educ. Today 2000, 20, 499–505. [Google Scholar] [CrossRef]
- Alfarania, A.; Su, S. Mobile assisted ESP vocabulary learning-A case study of a nursing english course. Taiwan Int. ESP J. 2016, 8, 66–88. [Google Scholar] [CrossRef]
- Chen, Y.; Lu, L.; Yang, X.Y.; Jian, Y.J.; Li, J. Attempt and result analysis of nursing speciality of the ESP teaching for high duty nurses specialized. Contin. Med. Educ. 2006, 20, 27–29. [Google Scholar] [CrossRef]
- Najafi, M.; Talebinezhad, M.R. The impact of teaching EFL medical vocabulary through collocations on vocabulary retention of EFL medical students. Adv. Lang. Lit. Stud. 2018, 9, 24–27. [Google Scholar] [CrossRef]
- Riahipour, P.; Saba, Z. ESP vocabulary instruction: Investigating the effect of using a game oriented teaching method for learners of english for nursing. J. Lang. Teach. Res. 2012, 3, 1258–1266. [Google Scholar] [CrossRef]
- Seibold, C.; Rolls, C.; Campbell, M. Nurses on the move: Evaluation of a program to assist international students undertaking an accelerated bachelor of nursing program. Contemp. Nurse 2007, 25, 63–71. [Google Scholar] [CrossRef]
- Staples, S. Using corpus-based discourse analysis for curriculum development: Creating and evaluating a pronunciation course for internationally educated nurses. Engl. Specif. Purp. 2019, 53, 13–29. [Google Scholar] [CrossRef]
- Canale, M.; Swain, M. Theoretical bases of communicative approaches to second language teaching and testing. Appl. Linguist. 1980, 1, 1–47. [Google Scholar] [CrossRef]
- Hymes, D. On Communicative Competence; University of Pennsylvania Press: Philadelphia, PA, USA, 1971. [Google Scholar]
- Bradley, J.; Edinberg, M. Communication in the Nursing Context; Pearson: Norwalk, CT, USA, 1990. [Google Scholar]
- Van Zanten, M.; Boulet, J.R.; McKinley, D. Using standardized patients to assess the interpersonal skills of physicians: Six years’ experience with a high-stakes certification examination. Health Commun. 2007, 22, 195–205. [Google Scholar] [CrossRef] [PubMed]
- Bays, A.M.; Engelberg, R.A.; Back, A.L.; Ford, D.W.; Downey, L.; Shannon, S.E.; Doorenbos, A.Z.; Edlund, B.; Christianson, P.; Arnold, R.W.; et al. Interprofessional communication skills training for serious illness: Evaluation of a small-group, simulated patient intervention. J. Palliat. Med. 2014, 17, 159–166. [Google Scholar] [CrossRef] [PubMed]
- Paltridge, B.; Phakiti, A. Research Methods in Applied Linguistics: A Practical Resource; Bloomsbury Academic: London, UK, 2015. [Google Scholar]
- Hafner, C.; Miller, L. English in the Disciplines: A Multidimensional Model for ESP Course Design; Routledge: New York, NY, USA, 2019. [Google Scholar]
- Woodrow, L. Introducing Course Design in English for Specific Purposes; Routledge: New York, NY, USA, 2018. [Google Scholar]
- Gass, J. Needs analysis and situational analysis: Designing an ESP curriculum for Thai nurses. Engl. Specif. Purp. World 2012, 12, 1–21. [Google Scholar]
- Bosher, S.; Smalkoski, K. From needs analysis to curriculum development. Engl. Specif. Purp. 2002, 21, 59–79. [Google Scholar] [CrossRef]
- Bolster, D.; Manias, E. Person-centred interactions between nurses and patients during medication activities in an acute hospital setting: Qualitative observation and interview study. Int. J. Nurs. Stud. 2010, 47, 154–165. [Google Scholar] [CrossRef]
- Manias, E.; Street, A. Legitimation of nurses’ knowledge through policies and protocols in clinical practice. J. Adv. Nurs. 2000, 32, 1467–1475. [Google Scholar] [CrossRef]
- Fox, N.S.; Brennan, J.S.; Chasen, S.T. Clinical estimation of fetal weight and the Hawthorne effect. Eur. J. Obstet. Gynecol. Reprod. Biol. 2008, 141, 111–114. [Google Scholar] [CrossRef]
- McCarney, R.; Warner, J.; Iliffe, S.; van Haselen, R.; Griffin, M.; Fisher, P. The Hawthorne effect: A randomised, controlled trial. BMC Med. Res. Methodol. 2007, 7, 30. [Google Scholar] [CrossRef]
- Potter, J.; Wetherell, M. Discourse and Social Psychology: Beyond Attitudes and Behaviour; Sage Publishing: Thousand Oaks, CA, USA, 1987. [Google Scholar]
- Eggins, M.; Slade, D. Analysing Casual Conversation; Equinox: London, UK, 1997. [Google Scholar]
- Halliday, M.A.K.; Matthiessen, C.M.I.M. An Introduction to Functional Grammar; Edward Arnold: London, UK, 2004. [Google Scholar]
- Martin, J.R. English Text: System and Structure; John Benjamins: Amsterdam, The Netherlands, 1992. [Google Scholar]
- Thornbury, S.; Slade, D. Conversation: From Description to Pedagogy; Cambridge University Press: Cambridge, MA, USA, 2006. [Google Scholar]
- Halliday, M.A.K.; Matthiessen, C.M.I.M. Halliday’s Introduction to Functional Grammar; Routledge: New York, NY, USA, 2013. [Google Scholar]
- Sinclair, J.M.; Coulthard, R.M. Towards an Analysis of Discourse: The English Used by Teachers and Pupils; Oxford University Press: London, UK, 1975. [Google Scholar]
- Pun, J.; Matthiessen, C.M.I.M.; Williams, G.; Slade, D. Using Ethnographic Discourse Analysis to Understand Doctor-Patient Interactions in Clinical Settings; Sage Publishing: Thousand Oaks, CA, USA, 2017. [Google Scholar]
- Slade, D.; Matthiessen, C.; Lock, G.; Pun, J.; Lam, M. Patterns of interaction in doctor-patient communication and their impact on health outcomes. In The Usage-Based Study of Language Learning and Multilingualism; Ortega, L., Tyler, A., Park, H., Uno, M., Eds.; Georgetown University Press: Washington, DC, USA, 2016; pp. 235–254. [Google Scholar]
- Slade, D.; Pun, J.; Lock, G.; Eggins, S. Potential risk points in doctor-patient communication: An analysis of Hong Kong emergency department medical consultations. In Language at Work: Analysing Language Use in Work, Education, Medical and Museum Contexts; Joyce, H.S., Ed.; Cambridge Scholars Publishing: Newcastle, UK, 2016; pp. 146–165. [Google Scholar]
- Candlin, S. Therapeutic Communication: A Lifespan Approach; Pearson Education: French’s Forest, NSW, Australia, 2008. [Google Scholar]
- Kourkouta, L.; Papathanasiou, I. Communication in Nursing Practice. Mater. Soc. Med. 2014, 26, 65–67. [Google Scholar] [CrossRef]
- Keating, N.L.; Green, D.C.; Kao, A.C.; Gazmararian, J.A.; Wu, V.Y.; Cleary, P.D. How are patients’ specific ambulatory care experiences related to trust, satisfaction, and considering changing physicians? J. Gen. Intern. Med. 2002, 17, 29–39. [Google Scholar] [CrossRef] [PubMed]
- Ishikawa, H.; Yamazaki, Y. How applicable are western models of patient-physician relationship in Asia? Changing patient-physician relationship in contemporary Japan. Int. J. Jpn. Sociol. 2005, 14, 84–93. [Google Scholar] [CrossRef]
- Shao, Y.N.; Sun, H.M.; Huang, J.W.; Li, M.L.; Huang, R.R.; Li, N. Simulation-based empathy training improves the communication skills of neonatal nurses. Clin. Simul. Nurs. 2018, 22, 32–42. [Google Scholar] [CrossRef]
- Morse, D.S.; Edwardsen, E.A.; Gordon, H.S. Missed opportunities for interval empathy in lung cancer communication. Arch. Intern. Med. 2015, 168, 1853–1865. [Google Scholar] [CrossRef] [PubMed]
- Wei, X.; Shi, Z. Nurses’ communication ability in nurse-patient conflict. J. Nurs. Sci. 2010, 25, 57–59. [Google Scholar]
- Ma, X.; Li, X. Investigation on influencing factors of nurse-patient communication competence of nursing staff. Chin. Nurs. Res. 2013, 27, 1951–1953. [Google Scholar]
- Hall, J.A. Clinicians’ accuracy in perceiving patients: Its relevance for clinical practice and a narrative review of methods and correlates. Patient Educ. Couns. 2011, 84, 319–324. [Google Scholar] [CrossRef]
- Wigert, H.; Dellenmark Blom, M.; Bry, K. Parents’ experiences of communication with neonatal intensive-care unit staff: An interview study. BMC Pediatr. 2014, 14, 304. [Google Scholar] [CrossRef]
- Slade, D.; Manidis, M.; McGregor, J.; Scheeres, H.; Chandler, E.; Stein-Parbury, J.; Dunston, R.; Herke, M.; Matthiessen, C.M.I.M. Communicating in Hospital Emergency Departments; Springer: Berlin/Heidelberg, Germany, 2015. [Google Scholar]
- Flowerdew, J. Discourse in English Language Education; Routledge: New York, NY, USA, 2013. [Google Scholar]
- Heisler, M.; Vijan, S.; Anderson, R.M.; Ubel, P.A.; Bernstein, S.J.; Hofer, T.P. When do patients and their physicians agree on diabetes treatment goals and strategies, and what difference does it make? J. Gen. Intern. Med. 2003, 18, 893–902. [Google Scholar] [CrossRef]
- Lobb, E.A.; Butow, P.N.; Barratt, A.; Meiser, B.; Gaff, C.; Young, M.A.; Haan, E.; Suthers, G.; Gattas, M.; Tucker, K. Communication and information-giving in high-risk breast cancer consultations: Influence on patient outcomes. Br. J. Cancer 2004, 90, 321–327. [Google Scholar] [CrossRef]
- Schrader, E.L.; Schrader, D.C. Health care provider communicator style and patient comprehension of oral contraceptive use. J. Am. Acad. Nurse Pract. 2001, 13, 80–83. [Google Scholar] [CrossRef] [PubMed]



Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).