Abstract
Objective: To explore the relationship between physical activity intensity and depressive symptoms in Chinese middle-aged and elderly people, and to provide new evidence for the prevention and treatment of depression by physical activity. Methods: The data came from the 2018 China Health and Retirement Longitudinal Study. Using the PPS sampling method, a baseline survey was conducted among middle-aged and elderly people over the age of 45 across the country to investigate their demographics, health status, economic status, and other information. A total of 6128 people with complete information on depression and physical activity were included in the analysis. The Z-test, analysis of covariance, and logistic regression were performed on the data using SPSS 27.0 software. Results: In terms of depressive symptoms, the proportion of detected depressive symptoms was 33.6% and the proportion of no depressive symptoms was 69.4%, and the prevalence of males was higher than that of females. Participants with high physical activity accounted for 50.9%, participants with low physical activity accounted for 49.1%, and the physical activity of males was significantly higher than that of females. There was a significant relationship between physical activity and depressive symptoms in middle-aged and elderly people (p < 0.05), and after adjusting for demographic variables (location of residence, education level, gender, age, and widowed or not), health status characteristics and living habits (diabetes and disability), self-rated health status, hypertension, stroke, hyperlipidemia, arthritis, and walking 1 km, the association between physical activity and depressive symptoms remained statistically significant (p < 0.05). Conclusion: The proportion of Chinese middle-aged and elderly men suffering from depressive symptoms was slightly higher than that of women, and middle-aged and elderly people with high physical activity had a lower risk of developing depressive symptoms. Attention should be paid to middle-aged and elderly people who are older, have poor self-assessed health status, have disabilities, have high blood pressure, have arthritis, have low physical activity and cannot walk one kilometer, and have low physical activity. Scientific and effective exercise prescriptions should be explored to prevent and improve depressive symptoms in middle-aged and elderly people.
1. Introduction
Aging is a global problem. Japan has entered a hyper-aged culture and is one of the nations with the greatest rates of population aging in the world, with 27% of the population being over 65 [1]. Germany’s population is one of the oldest in Europe with a proportion of 21.12% [2]. China’s aging problem is equally serious. The National Bureau of Statistics predicts that by 2050, China will have 400 million people aged 65 and above, and China will become one of the countries with the highest proportion of elderly people in the world [3]. Among the elderly, 70–80% of senile diseases are significantly related to poor mental health [4], and one of the most common and harmful mental diseases is senile depression [5]. The main clinical features of depression are sadness, loss of interest, low self-worth, slow reaction, lack of sleep or appetite, inattention, and severe fatigue [6,7]. Depression can seriously damage a person’s ability to work, study, or cope with daily life [8]. As depression becomes more serious, it may lead to suicide [9]. The prevalence of senile depression in China is 22.7%. Depression not only damages the health of the elderly, but also reduces the quality of life of the elderly and their families [10,11]. These results show that effective prevention strategies are of great significance to reduce the prevalence of depressive symptoms in the elderly. Some studies have reported that depression symptoms are influenced by some factors, such as high BMI, little physical activity, skipping breakfast, poor sleep quality, and eating snacks before bed [12,13]. It is worth noting that more and more evidence shows that regular physical exercise can reduce the risk of depression in the elderly, and the risk of depression in the elderly who lack physical exercise is higher than that in the elderly who take regular physical exercise [14]. One study showed that high-intensity physical exercise had a positive effect on reducing depressive symptoms compared with low-intensity physical exercise [15]. Another study showed that high-intensity resistance training was more effective than low-intensity resistance training in improving depression in older adults [16]. However, some studies have shown that low-intensity physical activity and moderate-high-intensity physical activity can significantly improve the symptoms of the elderly and reduce the risk of depression in the elderly [17]. A study showed that compared with high-intensity physical exercise, moderate and low-intensity physical exercise can protect the elderly from depression. This study also believed that exercise that increases flexibility can also reduce the risk of depression in the elderly to some extent, such as yoga and Pilates [18]. These studies revealed the causal relationship between exercise and depressive symptoms of the elderly. However, in previous studies, the mixed effects of demographic variables, health status, physical activity, and depression have not been fully studied, and further research is needed. Therefore, the purpose of this study is to explore whether the depressive symptoms of middle-aged and elderly people in China are related to physical activity intensity after controlling for demographic variables and health status, and to provide new evidence for the prevention and treatment of depression by physical activity.
2. Methods
2.1. Participants and Data
CHARLS is a large-scale interdisciplinary survey project implemented by Peking University in China [19]. The purpose is to collect data on demographic information, physical and mental health, personal and family economic status, medical services, and insurance of middle-aged and elderly people aged 45 and above in China, for the analysis of China’s population aging and to promote interdisciplinary research on aging. CHARLS adopts the multi-stage probability scale proportional sampling method and conducts sampling through four stages of county (district)-village (resident)-household-individual. In our study, CHARLS 2018 data were used. A total of 6,128 respondents were included in this study. All data collected in CHARLS are kept in the CHARLS database of Peking University, China. All data can be found at http://charls.pku.edu.cn (accessed on 28 September 2022). This study was approved by the Ethics Review Board of Shenyang Normal University, China.
2.2. Variables
2.2.1. Demographic and Health Status Variables
Demographic variables include gender (male or female), age (50–59, 60–69, 70–79, 80–89, or 90 and above), household registration types (urban or rural), education level (below high school or above high school), and widowed (yes or no). Health status variables included self-rated health status (good or bad), high blood pressure (yes or no), disability (yes or no), hyperlipemia (yes or no), diabetes (yes or no), stroke (yes or no), arthritis (yes or no), asthma (yes or no), smoking (yes or no), and ability to walk 1 km (good or bad).
2.2.2. Physical Activities
Through the questionnaire survey, we know that the physical activities of middle-aged and elderly people include carrying heavy objects, digging, farming, and other activities that consume a lot of physical strength, including mopping the floor, playing Taijiquan, walking, entertainment, mahjong, and other low physical activities. Then, the number of days and the duration of daily activities of the participants for each physical activity for at least 10 min were evaluated. The duration of each physical activity was assessed as greater than or equal to 10 min but less than 0.5 h, greater than or equal to 0.5 h but less than 2 h, greater than or equal to 2 h but less than 4 h, and >4 h. According to the International Physical Activity Questionnaire (IPAQ), the PA level was estimated, and IPAQ has good reliability and validity [20]. Total PA per week was calculated by metabolic equivalent × hour/week and divided into 2 groups: ≥23 MET·h·week−1 (high physical activity) or <23 MET·h·week−1 (low physical activity).
2.2.3. Depression
The short version of the CES-D scale was used to assess the severity of depression in middle-aged and older adults [21]. Radloff (1977) confirmed that the CES-D scale has good reliability and validity in Chinese population studies [22]. The 10 questions of the short version of the CES-D scale in the CHARLS questionnaire are as follows: ① I am troubled by small things; ② I have difficulty concentrating when doing things; ③ I feel depressed; ④ I feel that doing everything is very difficult; ⑤ I am hopeful about the future; ⑥ I am afraid; ⑦ I do not sleep well; ⑧ I am happy; ⑨ I feel lonely; ⑩ I feel that I cannot go on with my life. The degree of depression reflected in each question is assigned a score of 0–3 from low to high, and the scores of ⑤ and ⑧ are calculated in reverse. If the total score reaches 10 points or more, the participant is evaluated as “depressed” and the total score is 10 points; if it is below, participants are rated as “not depressed”.
2.3. Statistical Analysis
All included variables were first described statistically. Multiple logistic regression analysis was performed on the variables, with depressive symptoms as the dependent variable and physical activity level as the independent variable, to estimate the relationship between physical activity and the risk of depressive symptoms. Multilevel linear regression analysis was used to estimate the association between physical activity and risk of depressive symptoms after adjusting for variables. In Model 1, an analysis of covariance was performed to calculate p-values. In Model 2, physical activity, household registration type, education level, gender, age, and widowhood were adjusted. In Model 3, adjustments were made for physical activity, hukou type, education level, gender, age, widowhood, diabetes, disability, self-rated health status, hypertension, stroke, hyperlipidemia, arthritis, and ability to walk one kilometer. For all statistical analyses, p-values < 0.05 were considered statistically significant. All statistical analyses were performed using IBM SPSS Statistics 27.0 software (IBM SPSS Inc., Chicago, IL, USA).
3. Results
3.1. Demographic Characteristics
A total of 6,128 respondents were included in this study. Among them, there were 3016 males (49.2%), less than 3112 females (50.8%), and there was no significant difference in the gender of participants (p = 0.220) through the Z-test. In terms of depressive symptoms, the proportion of depressive symptoms detected was 33.6% and the proportion of no depressive symptoms was 69.4%. Participants with high physical activity accounted for 50.9%, while those with low physical activity accounted for 49.1%. Through the Z-test, there was no significant difference in physical activity level (p = 0.153). Participants aged 50–59, 60–69, 70–79, 80–89, and 90 and above accounted for 5.6%, 16.9%, 36.2%, 35.1%, and 6.2%, respectively. In terms of household registration types, urban household registration accounted for 21.8% and rural household registration accounted for 78.2%. In terms of education level, junior high school and below accounted for 80.5%, and senior high school and above accounted for 19.5%. Widowed participants accounted for 10.7% and nonwidowed participants accounted for 89.3%. The proportion of participants who rated their health as good was 24.7%, while the proportion of participants who rated their health as bad was 75.3%. Participants with disabilities accounted for 3.6% and those without disabilities accounted for 96.4%. In terms of chronic diseases, 11.9% of participants had hypertension and 88.1% of participants did not; 12.6% had hyperlipidemia and 87.4% of the participants did not; 6.6% of participants had diabetes and 93.4% did not; 6.2% of participants had a stroke, 93.8% had no stroke; 1.8% of the participants had asthma and 98.2% had no asthma; arthritis was present in 7.1% of participants and absent in 92.9% of participants; 26.1% of the participants had a smoking habit and 73.9% did not; 79.8% were able to walk one kilometer and 20.2% of participants could not walk one kilometer. The Z-test showed that there were statistical differences among other variables except gender and physical activity (p < 0.05) (Figure 1 and Table 1).
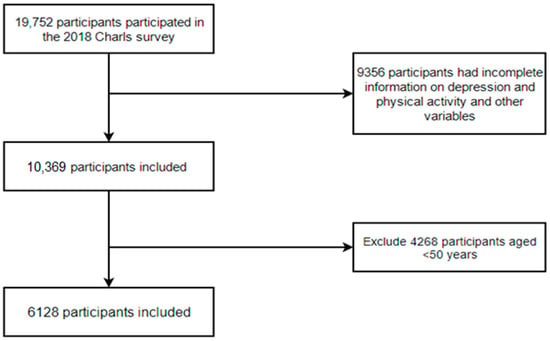
Figure 1.
Flow chart of participants screening.

Table 1.
Characteristics of middle-aged and elderly participants of the CHARLS in 2018.
3.2. Analysis of Influencing Factors of Depressive Symptoms
Gender, age, self-rated health status, disability, hypertension, arthritis, physical activity, and the ability to walk one kilometer are significantly related to depression (p < 0.05). Compared with middle-aged and elderly women, middle-aged and elderly men are more likely to suffer from depression (OR = 1.757; 95% CI = 1.552–1.990). With the increase in age, the risk of depression in middle-aged and elderly people decreases (OR = 0.675; 95% CI = 0.633–0.720). Middle-aged and elderly people with a worse self-rated health status have a higher risk of depression (OR = 0.801; 95% CI = 0.695–0.923). Middle-aged and elderly people with disability (OR = 1.957; 95% CI = 1.408–2.719), hypertension (OR = 1.216; 95% CI = 1.079–1.380), and arthritis (OR = 1.681; 95% CI = 1.539–1.861) are prone to depression symptoms. In terms of living habits, middle-aged and elderly people who have high physical activity momentum (OR = 5.719; 95% CI = 5.035–6.497) and can walk one kilometer (OR = 1.747; 95% CI = 1.506–2.027) are less likely to suffer from depressive symptoms (Table 2).
Table 2.
Influencing factors of depression among middle-aged and elderly participants in CHARLS in 2018.
3.3. Analysis of Influencing Factors of Physical Activity
Gender, age, disability, stroke, bad mood, arthritis, smoking, ability to walk one kilometer, and depression are significantly correlated with physical activity level (p < 0.05). Compared with middle-aged and old-aged women, the physical activity of middle-aged and old-aged men is higher (OR = 0.890; 95% CI = 0.792–0.999). With the increase in age, the physical activity momentum level of middle-aged and elderly people becomes lower (OR = 0.660; 95% CI = 0.515–0.845). Disability is negatively correlated with high physical activity of middle-aged and elderly people (OR = 0.491; 95% CI = 0.357–0.677). Middle-aged and elderly people with stroke (OR = 0.505; 95% CI = 0.391–0.652) and arthritis (OR = 0.440; 95% CI = 0.354–0.796) are significantly negatively correlated with high physical activity. The physical activity of middle-aged and elderly people with a smoking habit (OR = 1.257; 95% CI = 1.102–1.435) is significantly higher than that of middle-aged and elderly people without a smoking habit. The middle-aged and elderly people with no depressive symptoms (OR = 0.166; 95% CI = 0.146–0.189) and a good ability to walk 1 km (OR = 2.089; 95% CI = 1.796–2.431) are at a high level (Table 3).
Table 3.
Influencing factors of physical activity among middle-aged and elderly participants in CHARLS in 2018.
3.4. Analysis of Linear Hierarchical Regression Models between Participants’ Depressive Symptoms and Physical Activity Levels
Model 1 shows that there is a significant relationship between physical activity and depressive symptoms (p < 0.05). Model 2 adjusts the demographic variables (location of residence, education level, gender, age, whether or not you are widowed) on the basis of physical activity, and the results are also statistically significant (p < 0.05). On the basis of model 2, the model adjusts the characteristics of health status and living habits (diabetes, disability, self-rated health status, hypertension, stroke, hyperlipidemia, arthritis, and walking 1 km), and the results are still significant (p < 0.05) (Table 4).
Table 4.
Linear hierarchical regression model of depression symptoms and physical activity level of participants.
4. Discussion
This study demonstrates a negative correlation between depression symptoms and physical activity levels in middle-aged and elderly people. After adjusting for the demographic characteristics (registered residence type, education level, gender, age, and widows) and health status characteristics (diabetes, disability, self-rated health status, hypertension, stroke, hyperlipidemia, arthritis, and walking 1 km), this negative correlation still exists. This shows that high physical activity can reduce the risk of depressive symptoms in middle-aged and elderly people. This result is supported by a previous study by Overdorf et al. [23]. They recruited 65 women over 60 years old to evaluate the relationship between physical activity and depression symptoms of healthy elderly women. The results showed that there was a significant correlation between physical activity momentum and the score of the Beck Depression Scale, that is, the more active the physical activity of the elderly, the lower her self-reported depressive symptoms. Therefore, the elderly with low physical activity are more likely to suffer from depressive symptoms and may increase the severity of depressive symptoms. In addition, our survey shows that the level of physical activity is negatively correlated with depressive symptoms, which means that the elderly with high physical activity are less likely to have depressive symptoms. This result is consistent with the research results of Tapps et al. [24], who recruited 40 elderly people to evaluate the effect of resistance exercise for 12 weeks on the depression level of disabled elderly people. The results showed that compared with the control group, the depression level of the elderly who participated in the resistance exercise group was lower, which indicated that the resistance exercise had a positive effect on the depression of the elderly. Resistance exercise is a kind of high physical activity, so this study provides preliminary support for the curative effect of resistance exercise on depressive symptoms. According to the health characteristics of the elderly, making a scientific and systematic resistance exercise program may have a more powerful effect on the treatment of depression symptoms of the elderly.
Several possible mechanisms of the relationship between physical activity and depression have been proposed and tested. Physical activity may improve the physiological and psychological conditions of the elderly to prevent and improve depression. A study showed [25] that physical activity can change the control of the nervous system of the elderly, improve the plasticity of the brain of the elderly, improve the metabolism of the elderly, release dopamine, and then improve the symptoms of depression [26]. A study showed [27] that the injury of hippocampal nerve cells will increase the risk of depression in the elderly. Physical activity can enhance the oxygen content in blood, and nutritional factors of hippocampal nerve cells and stress-regulated cells. These nutritional factors can improve the brain metabolism of the elderly, nourish nerve cells, and then repair the damaged hippocampal nerve cells and other cells directly involved in stress regulation. A study showed [28] that physical activity can create an anti-inflammatory environment in the human body. The human body will stimulate the hypothalamus–pituitary–adrenal axis during physical activities, which can reduce the release of pro-inflammatory cytokines from hippocampal cells, increase the release of anti-inflammatory cytokines, and improve the inflammatory environment of the internal environment [29].
The results of our model also quantify the effects of demographic characteristics and health characteristics variables on physical activity and depressive symptoms. Considering the influence of gender, we find that the depression level of middle-aged and old-aged men is higher than that of middle-aged and old-aged women, which is inconsistent with the previous study of Blazer et al. [30], who evaluated the demographics, physical function, cognitive status, and depressive symptoms of 4162 elderly people aged 65+ in North Carolina, USA. The results showed that of the female elderly, those with low education level, physical dysfunction, and cognitive impairment are more likely to suffer from depression. However, the results of this study showed that middle-aged men are more prone to depression than middle-aged women. The subjects of this study were middle-aged and elderly people, and there were national and ethnic differences with the previous subjects, which may be one of the reasons for the inconsistency in the research results. Age is one of the important factors that affect the depressive symptoms of the elderly. This study found that the older the elderly, the higher the risk of depression. This result is consistent with the research results of Isik et al. [31], who recruited 501 elderly people and collected relevant data by questionnaires: the Loneliness Scale for the Elderly and Depression Scale for the Elderly. Statistical methods of regression analysis were used to analyze the factors influencing depressive symptoms. The results showed that loneliness, education level, and age of the elderly are the predictors of the increased risk of depression. People are a disgrace to aging. With the aging of middle-aged and elderly people, their ability of daily activities decreases significantly, which will lead to their mentality and mood becoming increasingly worse, which may lead to depression increasing with age. Therefore, with the increasingly serious aging problem in China, government and society should pay more attention to the mental health of the elderly, and it is necessary to publicize the aging culture among middle-aged and elderly people in the community so that they can realize that aging is a problem that everyone needs to face and that it is a process in which the middle-aged and elderly people must have a correct cognition of and accept. Let the elderly face the aging process with a positive and optimistic attitude.
The effects of health status (self-rated health status, disability, hypertension, and arthritis) of middle-aged and elderly people on physical activity and depressive symptoms were studied. We found that middle-aged and elderly people with poor health, disability, hypertension, and arthritis were more likely to suffer from depression symptoms and had a lower physical activity momentum. This result is partly in line with previous research by Tiong et al. [32]. They recruited 375 Singaporean elderly people aged 55 and above, used multivariate logistic regression analysis to evaluate the prevalence of depression among the elderly population in Singapore, and determined the risk factors related to depression. The results showed that the prevalence of depression in NH residents in Singapore was high. The important risk factors related to depression are chronic disease history, pain history, and lack of social contact. In order to provide the latest information on the prevalence and predictors of depression in the elderly Caucasian population, Djernes [33] conducted a research review. The results showed that gender, physical illness, cognitive impairment, physical dysfunction, lack of social contact, and depression history were all factors that increased the risk of depression symptoms. The research of Su et al. [34] showed that physical activity can alleviate depression by improving the function of the cardiovascular system. This study believed that compared with the elderly without chronic diseases, the middle-aged and elderly people with chronic diseases have a higher risk of depression. This finding is consistent with the research results of Schulz et al. [35]. They recruited 5201 elderly people aged 65 and above in a community in the United States to study the relationship between depression symptoms and mortality among the elderly, and controlled for social demographic factors, clinical diseases, subclinical diseases, and health risk factors. The results showed that the scores of high depressive symptoms were significantly correlated with high mortality. After controlling for social and demographic factors, epidemic clinical diseases, or biological or behavioral risk factors, the elderly with chronic diseases were found to be at higher risk of depression. Physical exercise has been proven to improve the function of the cardiovascular system [36], so it may also be one of the mechanisms that can improve depression symptoms of the elderly. The elderly should take regular physical exercise, which can not only reduce the risk of depression but also improve cardiovascular function.
In addition, this study shows that the risk of depression in middle-aged and elderly people who can walk one kilometer is significantly lower than that in middle-aged and elderly people who cannot walk one kilometer. One-kilometer walking ability represents the exercise ability of middle-aged and elderly people, which indicates that the stronger the exercise ability, the lower the risk of depression among middle-aged and elderly people. This finding is consistent with the research results of Xianqiang et al. [37], which showed that there is a significant relationship between exercise ability and depressive symptoms. One possible explanation for this result is that the stronger the exercise ability, the more physical activities will be carried out. Because high physical activity momentum is negatively correlated with depressive symptoms, the higher the exercise ability, the lower the risk of depressive symptoms for middle-aged and elderly people. Studies have shown that long-term sedentary behavior of the elderly will increase their risk of depression, and regular physical exercise will reduce the risk of depression [38]. It is found that high-intensity physical activity is more effective than low-intensity physical activity in relieving depression symptoms [39]. This finding is consistent with the research results of Satoru et al. [40], who considered that high-intensity resistance training is more effective than low-intensity resistance training in improving depression symptoms of the elderly. The above research is consistent with the conclusion of this study.
5. Conclusions and limitations
Depression symptoms of middle-aged and elderly people are closely related to physical activity, but at present, the research on physical activity and depression of middle-aged and elderly people in China is in the initial exploration stage. In this study, the middle-aged and elderly people with high physical activity have a lower risk of depression. Compared with middle-aged and elderly women, middle-aged and elderly men are more likely to suffer from depression (OR = 1.757; 95% CI = 1.552–1.990). With the increase in age, the risk of depression in middle-aged and elderly people decreases (OR = 0.675; 95% CI = 0.633–0.720). Middle-aged and elderly people with worse self-rated health status have a higher risk of depression (OR = 0.801; 95% CI = 0.695–0.923). Middle-aged and elderly people with disability (OR = 1.957; 95% CI = 1.408–2.719), hypertension (OR = 1.216; 95% CI = 1.079–1.380), and arthritis (OR = 1.681; 95% CI = 1.539–1.861) are prone to depression symptoms. This study is helpful to better understand the relationship between depression symptoms and physical activity in middle-aged and elderly people, and it has important reference significance for formulating accurate exercise prescriptions to prevent and improve depression symptoms in elderly people.
Our research is also affected by many limitations. First, this study only reveals the relationship between physical activity and depression, and also determines the relationship between physical activity level and depression after controlling for population characteristic variables and health status. However, it is impossible to determine the mechanism of physical activity affecting depressive symptoms, which needs to be verified by another experimental study. Secondly, we prove that the relationship between physical activity level and depressive symptoms of middle-aged and elderly people in China is limited. The relationship between physical activity and depressive symptoms may be different in different countries, so it is necessary to further study the relationship between physical activity and depressive symptoms in all countries of the world to determine the reliability of this research conclusion. Third, this study does not control the economic status of middle-aged and elderly people, which may affect the reliability of the results. Fourth, the lack of use of accelerometry to measure physical activity and the lack of a moderate intensity physical activity group are two other important limitations of this study. The use of accelerometers to measure physical activity in middle-aged and older adults is more accurate. The lack of a moderate-physical activity group would lead to the possibility that there is a boundary in the assessment of the high-intensity physical activity group versus the low-physical-activity group.
Author Contributions
Data curation: Y.Z. and Y.T.; formal analysis: Y.T.; methodology: Y.Z.; project administration: Y.T.; resources: Y.Z.; writing—original draft: Y.Z. and Y.T.; writing—review and editing: Y.Z. and Y.T. All authors have read and agreed to the published version of the manuscript.
Funding
This research received no external funding.
Institutional Review Board Statement
The study was conducted in accordance with the Declaration of Helsinki, and approved by the Institutional Review Board of College of Sports Science, Shenyang Normal University (protocol code 034, protocol approved on 2 June 2022).
Informed Consent Statement
Informed consent was obtained from all subjects involved in the study.
Data Availability Statement
All data collected in CHARLS are kept in the CHARLS database of Peking University, China. All data can be found at http://charls.pku.edu.cn (accessed on 28 September 2022).
Acknowledgments
The authors thank all the participants in the CHARLS team for their time and effort devoted to the project.
Conflicts of Interest
The authors declare no conflict of interest.
References
- Bessho, S. Local fiscal multipliers and population aging in Japan. Jpn. World Econ. 2021, 60, 101099. [Google Scholar] [CrossRef]
- Vanella, P.; Wilke, C.B.; Söhnlein, D. Prevalence and Economic Costs of Absenteeism in an Aging Population—A Quasi-Stochastic Projection for Germany. Forecasting 2022, 4, 371–393. [Google Scholar] [CrossRef]
- Liu, D. Current situation, causes and countermeasures of China’s aging population. Chin. J. Gerontol. 2022, 42, 4123–4126. [Google Scholar]
- Liu, J.K.; Li, S.; Lin, J.; Xu, F.S.; Zhang, Y.; Sun, L.; Xu, C.J.; Yang, H.X.; Wang, Y.G. Study on the relationship between the elderly’s ability of daily living and the coexistence of depression and anxiety symptoms. China Chronic Dis. Prev. Control. 2022, 30, 251–255. [Google Scholar]
- Yang, M.; Chen, X.; Fu, W.; Chen, C. Analysis of the current situation of depression symptoms and gender differences among middle-aged and elderly people in rural China. China Chronic Dis. Prev. Control. 2022, 30, 161–166+171. [Google Scholar]
- D’Errico, M.; Fessele, K. A Retrospective, Cross-Sectional Study of Self-Reported Physical Activity and Depression Among Breast, Gynecologic, and Thoracic Cancer Survivors. Oncol. Nurs. Forum 2021, 48, 59–64. [Google Scholar] [CrossRef] [PubMed]
- National Institute of Mental Health. Depression Basics. 2016. Available online: https://www.nimh.nih.gov/health/publications/depression/index.shtml (accessed on 25 May 2018).
- Ismail, Z.; Elbayoumi, H.; Fischer, C.E.; Hogan, D.B.; Millikin, C.P.; Schweizer, T.; Mortby, M.E.; Smith, E.E.; Patten, S.B.; Fiest, K.M. Prevalence of Depression in Patients with Mild Cognitive Impairment A Systematic Review and Meta-analysis. JAMA Psychiatry 2017, 1, 74. [Google Scholar] [CrossRef]
- Depressive Disorders. Diagnostic and Statistical Manual of Mental Disorders; American Psychiatric Association: Washington, DC, USA, 2013. [Google Scholar]
- Knapen, J.; Vancampfort, D.; Mori€en, Y.; Marchal, Y. Exercise therapy improves both mental and physical health in patients with major depression. Disabil. Rehabil. 2015, 37, 1490–1495. [Google Scholar] [CrossRef]
- Qin, X.; Wang, S.; Hsieh, C.R. The prevalence of depression and depressive symptoms among adults in China: Estimation based on a National Household Survey. China Econ. Rev. 2018, 51, 271–282. [Google Scholar] [CrossRef]
- Knepp, M.M.; Yoza, J.J.; Quandt, E.A. Higher modified beck depression inventory scores are associated with body, eating, and exercise comparisons but decreased exercise amounts. Percept. Mot. Skills. 2015, 120, 945–959. [Google Scholar] [CrossRef]
- Law, S.; Liu, P. Suicide in China: Unique demographic patterns and relationship to depressive disorder. Curr. Psychiatry Rep. 2008, 10, 80–86. [Google Scholar] [CrossRef]
- Dishman, R.K.; Mcdowell, C.P.; Herring, M.P. Customary physical activity and odds of depression: A systematic review and meta-analysis of 111 prospective cohort studies. Br. J. Sports Med. 2021, 55, 926–934. [Google Scholar] [CrossRef]
- Feng, G.; Ying, T.; Fei, Z.; Chunchun, W.; Yufei, C.; Cong, H. Intensity of Physical Activity and Depressive Symptoms in College Students: Fitness Improvement Tactics in Youth (FITYou) Project. Psychol. Res. Behav. Manag. 2020, 13, 787–796. [Google Scholar]
- Cui, Y.; Huang, C.; Gong, Q.; Guo, F.; Li, W.; Zhang, L.; Cai, X.; Wang, Y. Physical exercise behaviors and depressive symptoms among elderly Chinese women: Focus on exercise components. Risk Manag. Healthc. Policy 2021, 14, 2647–2655. [Google Scholar] [CrossRef]
- de Souto Araujo, Z.T.; de Miranda Silva Nogueira, P.A.; Cabral, E.E.A.; de Paula dos Santos, L.; da Silva, I.S.; Ferreira, G.M.H. Effectiveness of low-intensity aquatic exercise on COPD: A randomized clinical trial. Respir. Med. 2012, 106, 1535–1543. [Google Scholar] [CrossRef]
- Arrieta, H.; Rezola-Pardo, C.; Echeverria, I.; Iturburu, M.; Gil, S.M.; Yanguas, J.J.; Irazusta, J.; Rodriguez, L.A. Physical activity and fitness are associated with verbal memory, quality of life and depression among nursing home residents: Preliminary data of a randomized controlled trial. BMC Geriatr. 2018, 18, 80. [Google Scholar] [CrossRef]
- Yaohui, Z.; Strauss, J.; Xinxin, C.; Yafeng, W.; Jinquan, G.; Qinqin, M.; Gewei, W.; Huali, W. China Health and Retirement Longitudinal Study Wave 4 User’s Guide; National School of Development, Peking University: Beijing, China, 2020. [Google Scholar]
- van der Ploeg, H.P.; Tudor-Locke, C.; Marshall, A.L.; Craig, C.; Hagströmer, M.; Sjöström, M.; Bauman, A. Reliability and Validity of the International Physical Activity Questionnaire for Assessing Walking. Res. Q. Exerc. Sport 2010, 81, 97–101. [Google Scholar] [CrossRef]
- Aamir, S.; Winkel, C. The Impact of COVID-19 on Saudi Arabian Female Students: An Application of the CES-D Depression Scale. J. Educ. Soc. Res. 2021, 11, 23. [Google Scholar] [CrossRef]
- Mei, H.; Cunxian, J. Evaluation of reliability and validity of CES-D depression scale for different rural populations. China Public Health 2012, 28, 1265–1267. [Google Scholar]
- Overdorf, V.; Kollia, B.; Makarec, K.; Szeles, C.A. The Relationship Between Physical Activity and Depressive Symptoms in Healthy Older Women. Gerontol. Geriatr. Med. 2016, 2, 2333721415626859. [Google Scholar] [CrossRef]
- Tapps, T.N. An Investigation into the Effects of Resistance Exercise Participation on the Perceived Depression Levels of Older Adults Residing in a Long-Term Care Facility over Time; Oklahoma State University: Stillwater, OK, USA, 2009. [Google Scholar]
- Bruce, C.; Mcgregor, K.M.; Nocera, J.R.; Jonathan, H.D.; Stella, M.T.; Andrew, J.B. The relevance of aging-related changes in brain function to rehabilitation in aging-related disease. Front. Hum. Neurosci. 2015, 9, 307. [Google Scholar]
- Clark, B.C.; Manini, T.M. Functional consequences of sarcopenia and dynapenia in the elderly. Curr. Opin. Clin. Nutr. Metab. Care 2010, 13, 271–276. [Google Scholar] [CrossRef]
- Leal-Galicia, P.; Romo-Parra, H.; Rodríguez-Serrano, L.M.; Buenrostro-Jáuregui, M. Regulation of adult hippocampal neurogenesis exerted by sexual, cognitive and physical activity: An update. J. Chem. Neuroanat. 2019, 101, 101667. [Google Scholar] [CrossRef]
- Kitahara, C.; Trabert, B.; Katki, H.; Chaturvedi, A.K.; Kemp, T.J.; Pinto, L.A.; Moore, S.C.; Purdue, M.P.; Wentzensen, N.; Hildesheim, A.; et al. Body mass index, physical activity, and serum markers of inflammation, immunity, and insulin resistance. Cancer Epidemiol. Biomark. Prev. 2014, 12, 2480–2489. [Google Scholar] [CrossRef]
- Luan, H.; Huang, Y.; Li, J.; Sun, L.; Fan, Y. Effect of Local Vibration and Passive Exercise on the Hormones and Neurotransmitters of Hypothalamic–Pituitary–Adrenal Axis in Hindlimb Unloading Rats. Microgravity Sci. Technol. 2018, 30, 483–489. [Google Scholar] [CrossRef]
- Blazer, D.G.; Moody-Ayers, S.; Craft-Morgan, J.; Burchett, B. Depression in diabetes and obesity: Racial/ethnic/gender issues in older adults. J. Psychosom. Res. 2002, 53, 913–916. [Google Scholar] [CrossRef]
- Isik, K.; Başoğul, C.; Yildirim, H. The relationship between perceived loneliness and depression in the elderly and influencing factors. Perspect. Psychiatr. Care 2020, 57, 351–357. [Google Scholar] [CrossRef]
- Tiong, W.W.; Yap, P.; Koh, G.C.H.; Fong, N.P.; Luo, N. Prevalence and risk factors of depression in the elderly nursing home residents in Singapore. Aging Ment. Heal. 2013, 17, 724–731. [Google Scholar] [CrossRef]
- Djernes, J.K. Prevalence and predictors of depression in populations of elderly: A review. Acta Psychiatr. Scand. 2010, 113, 372–387. [Google Scholar] [CrossRef]
- Su, Z.A.; Kxb, C.; Sl, D.; Pan, H.F. Physical activity and depression in older adults: The knowns and unknowns. Psychiatry Res. 2021, 279, 113738. [Google Scholar]
- Schulz, R.; Beach, S.R.; Ives, D.G.; Martire, L.M.; Ariyo, A.A.; Kop, W.J. Association Between Depression and Mortality in Older Adults: The Cardiovascular Health Study. Arch. Intern. Med. 2000, 160, 1761–1768. [Google Scholar] [CrossRef] [PubMed]
- Ma, C.; Zhou, W.; Jia, Y.; Tang, Q. Effects of home-based Baduanjin combined with elastic band exercise in patients with chronic heart failure. Eur. J. Cardiovasc. Nurs. 2022, 21, 587–596. [Google Scholar] [CrossRef] [PubMed]
- Deng, X.; Xiao, L.; Kan, L. Exercise ability and influencing factors of senile depression patients. Chin. J. Gerontol. 2015, 35, 3107–3109. [Google Scholar]
- Teychenne, M.; Ball, K. Physical activity, sedentary behavior and depression among disadvantaged women. Health Educ. Res. 2010, 25, 632–644. [Google Scholar] [CrossRef]
- Yagi, A.; Kondo, k.; Hayasaka, S.; Ojima, T. The Association between Tub-Bathing Frequency and the Incidence of Depressive Symptoms among Older People in Japan: JAGES Longitudinal Study. Jpn. J. Health Res. 2019, 40, 67–73. [Google Scholar]
- Kanamori, S.; Takamiya, T.; Inoue, S.; Kai, Y.; Tsuji, T.; Kondo, K. Frequency and pattern of exercise and depression after two years in older Japanese adults: The JAGES longitudinal study. Entific Rep. 2018, 8, 11224. [Google Scholar] [CrossRef]
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).