Development and Validation of a Knowledge Management Questionnaire for Hospitals and Other Healthcare Organizations




Abstract
1. Introduction
2. Methods
2.1. Questionnaire Design
2.2. Ethical Issues
2.3. Research Tool
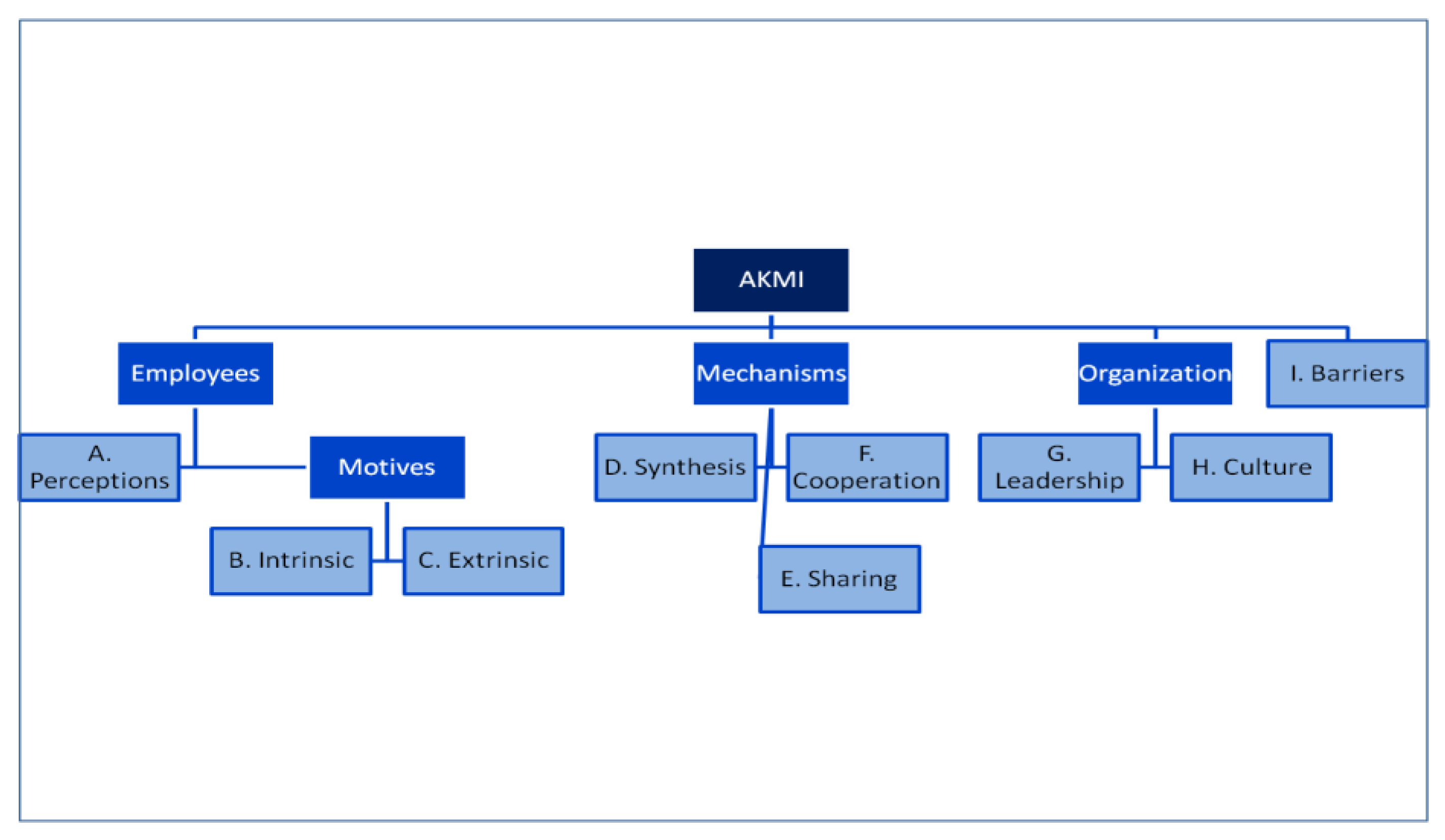
2.3.1. Selection of the Factors
2.3.2. Perceptions about Knowledge Management (KM)
2.3.3. Motives
2.3.4. Knowledge Synthesis
2.3.5. Knowledge Sharing and Collaboration
2.3.6. Leadership
2.3.7. Culture
2.3.8. Barriers
2.4. Pilot Study
2.5. Data Analysis
3. Results
3.1. Study Population
3.2. Validity
3.3. Exploratory Factor Analysis
4. Discussion
4.1. Knowledge Management and Sustainability
4.2. Knowledge Management and Human Resources
4.3. Knowledge Management and Organisational Learning
4.4. Knowledge Management and the Developed Questionnaire
5. Conclusions
Author Contributions
Funding
Acknowledgments
Conflicts of Interest
References
- Zins, C. Conceptual approaches for defining data, information, and knowledge. J. Am. Soc. Inf. Sci. Technol. 2007, 58, 479–493. [Google Scholar] [CrossRef]
- Ackoff, R.L. From Data to Wisdom. J. Appl. Syst. Anal. 1989, 16, 3–9. [Google Scholar]
- Smith, E.A. The role of tacit and explicit knowledge in the workplace. J. Knowl. Manag. 2001, 5, 311–321. [Google Scholar] [CrossRef]
- Collins, H. Tacit and Explicit Knowledge; University of Chicago Press: Chicago, IL, USA, 2010. [Google Scholar]
- Nonaka, I.; Takeuchi, H. The Knowledge-Creating Company: How Japanese Companies Create the Dynamics of Innovation; Oxford University Press: New York, NY, USA, 1995. [Google Scholar]
- Polanyi, M. The Tacit Dimension; Anchor Books: New York, NY, USA, 1967. [Google Scholar]
- Sanguankaew, P.; Vathanophas Ractham, V. Bibliometric review of research on knowledge management and sustainability, 1994–2018. Sustainability 2019, 11, 4388. [Google Scholar] [CrossRef]
- Tsoukas, H.; Vladimirou, E. What is organizational knowledge? J. Manag. Stud. 2001, 38, 973–993. [Google Scholar] [CrossRef]
- Guptill, J. Knowledge management in health care. J. Health Care Financ. 2005, 31, 10–14. [Google Scholar]
- Popa, I.; Ștefan, S.C. Modeling the Pathways of Knowledge Management Towards Social and Economic Outcomes of Health Organizations. Int. J. Environ. Res. Public Health 2019, 16, 1114. [Google Scholar] [CrossRef] [PubMed]
- Begoña Lloria, M. A review of the main approaches to knowledge management. Knowl. Manag. Res. Pract. 2008, 6, 77–89. [Google Scholar] [CrossRef]
- Hislop, D. Knowledge Management in Organizations: A Critical Introduction; Oxford University Press: Oxford, UK, 2013. [Google Scholar]
- Šajeva, S. The analysis of key elements of socio-technical knowledge management system. Econ. Manag. 2010, 15, 765–774. [Google Scholar]
- Drucker, P. Managing in the Next Society; Taylor & Francis Ltd.: Oxford, UK, 2007. [Google Scholar]
- Kothari, A.; Hovanec, N.; Hastie, R.; Sibbald, S. Lessons from the business sector for successful knowledge management in health care: A systematic review. BMC Health Serv. Res. 2011, 11, 173. [Google Scholar] [CrossRef]
- Karamitri, I.; Talias, M.A.; Bellali, T. Knowledge management practices in healthcare settings: A systematic review. Int. J. Health Plann. Manag. 2017, 32, 4–18. [Google Scholar] [CrossRef] [PubMed]
- Aharony, N. Librarians’ Attitudes toward Knowledge Management. Coll. Res. Libr. 2011, 72, 111–126. [Google Scholar] [CrossRef]
- Rattray, J.; Jones, M.C. Essential elements of questionnaire design and development. J. Clin. Nurs. 2007, 16, 234–243. [Google Scholar] [CrossRef] [PubMed]
- Bissett, A.F. Designing a questionnaire. Send a personal covering letter. BMJ 1994, 308, 202–203. [Google Scholar] [CrossRef]
- Duncan, A.; Bonetti, D.; Clarkson, J.; Ramsay, C. Improving trial questionnaire response rates using behaviour change theory. Trials 2015, 16, P92. [Google Scholar] [CrossRef]
- Fishbein, I.; Ajzen, I. Belief, Attitude, Intention and Behaviour: An Introduction to Theory and Research; Addison-Wesley: Boston, MA, USA, 1975. [Google Scholar]
- Chang, Y.-Y.; Hsu, P.-F.; Li, M.-H.; Chang, C.-C. Performance evaluation of knowledge management among hospital employees. Int. J. Health Care Qual. Assur. 2011, 24, 348–365. [Google Scholar] [CrossRef]
- Potgieter, A.; Dube, T.; Rensleigh, C. Knowledge management awareness in a research and development facility: Investigating employee perceptions. S. Afr. J. Inf. Manag. 2013, 15, 6. [Google Scholar] [CrossRef]
- Maslow, A.H. A theory of human motivation. Psychol. Rev. 1943, 50, 370–396. [Google Scholar] [CrossRef]
- Buchbinder, S.B.; Shanks, N.H. Introduction to Health Care Management, 2nd ed.; Jones & Bartlett Learning: Denver, CO, USA, 2011. [Google Scholar]
- Abbas, J. Impact of total quality management on corporate sustainability through the mediating effect of knowledge management. J. Clean. Prod. 2020, 244, 118806. [Google Scholar] [CrossRef]
- Thomas, K.W. Intrinsic Motivation at Work: What Really Drives Employee Engagement; Berrett-Koehler Publishers: San Francisco, CA, USA, 2009. [Google Scholar]
- Bednarczyk, T.K. Human resources and motivation in knowledge management. Manag. Prod. Eng. Rev. 2010, 1, 6. [Google Scholar]
- Skinner, B.F. Science and Human Behavior; New Impression edition; Free Press: New York, NY, USA, 1965. [Google Scholar]
- Lin, H.-F. Effects of extrinsic and intrinsic motivation on employee knowledge sharing intentions. J. Inf. Sci. 2007, 33, 135–149. [Google Scholar] [CrossRef]
- Colnar, S.; Dimovski, V.; Bogataj, D. Knowledge Management and the Sustainable Development of Social Work. Sustainability 2019, 11, 6374. [Google Scholar] [CrossRef]
- Ghosh, B.; Scott, J.E. Comparing knowledge management in health-care and technical support organizations. IEEE Trans. Inf. Technol. Biomed. 2005, 9, 162–168. [Google Scholar] [CrossRef] [PubMed]
- Orzano, A.J.; Ohman-Strickland, P.A.; Patel, M. What can family medicine practices do to facilitate knowledge management? Health Care Manag. Rev. 2008, 33, 216–224. [Google Scholar] [CrossRef] [PubMed]
- Gerrish, K.; McDonnell, A.; Nolan, M.; Guillaume, L.; Kirshbaum, M.; Tod, A. The role of advanced practice nurses in knowledge brokering as a means of promoting evidence-based practice among clinical nurses. J. Adv. Nurs. 2011, 67, 2004–2014. [Google Scholar] [CrossRef] [PubMed]
- Auernhammer, J.; Hall, H. Organizational culture in knowledge creation, creativity and innovation: Towards the Freiraum model. J. Inf. Sci. 2013, 40, 154–166. [Google Scholar] [CrossRef]
- Kumar, M. Effect of Leadership Behaviors on Knowledge Creation in Indian Organizations. Delhi Bus. Rev. 2013, 14, 25. [Google Scholar]
- Lee, H.S.; Hong, S.A. Factors affecting hospital employees‘ knowledge sharing intention and behavior, and innovation behavior. Osong Public Health Res. Perspect. 2014, 5, 148–155. [Google Scholar] [CrossRef]
- Nembhard, I.M. All teach, all learn, all improve?: The role of interorganizational learning in quality improvement collaboratives. Health Care Manag. Rev. 2012, 37, 154–164. [Google Scholar] [CrossRef]
- Williams, P.M. Integration of health and social care: A case of learning and knowledge management. Health Soc. Care Community 2012, 20, 550–560. [Google Scholar] [CrossRef]
- Pezeshki rad, G.; Alizadeh, N.; Zamani Miandashti, N.; Shabanali Fami, H. factors influencing knowledge sharing among personnel of agricultural extension and education organization in iranian ministry of jihad-e agriculture. J. Agric. Sci. Technol. 2011, 13, 491–501. [Google Scholar]
- Nguyen, H.; Mohamed, S. Leadership behaviors, organizational culture and knowledge management practices: An empirical investigation. J. Manag. Dev. 2011, 30, 206–221. [Google Scholar] [CrossRef]
- Liu, F.-C.; Cheng, K.-L.; Chao, M.; Tseng, H.-M. Team innovation climate and knowledge sharing among healthcare managers: Mediating effects of altruistic intentions. Chang. Gung Med. J. 2012, 35, 408–419. [Google Scholar] [CrossRef] [PubMed]
- Sánchez-Polo, M.T.; Cegarra-Navarro, J.G. Implementing Knowledge Management Practices in Hospital-in-the-Home Units. J. Nurs. Care Qual. 2008, 23, 18–22. [Google Scholar] [CrossRef]
- Alavi, M.; Kayworth, T.R.; Leidner, D.E. An Empirical Examination of the Influence of Organizational Culture on Knowledge Management Practices. J. Manag. Inf. Syst. 2005, 22, 191–224. [Google Scholar] [CrossRef]
- Sibbald, S.L.; Wathen, C.N.; Kothari, A. An empirically based model for knowledge management in health care organizations. Health Care Manag. Rev. 2016, 41, 64–74. [Google Scholar] [CrossRef]
- Karamat, J.; Shurong, T.; Ahmad, N.; Waheed, A.; Khan, S. Barriers to knowledge management in the health sector of Pakistan. Sustainability 2018, 10, 4155. [Google Scholar] [CrossRef]
- Dobbins, M.; DeCorby, K.; Twiddy, T. A knowledge transfer strategy for public health decision makers. Worldviews Evid. Based Nurs. 2004, 1, 120–128. [Google Scholar] [CrossRef]
- Lin, C.; Tan, B.; Chang, S. An exploratory model of knowledge flow barriers within healthcare organizations. Inf. Manag. 2008, 45, 331–339. [Google Scholar] [CrossRef]
- Woodward, C.A. Questionnaire construction and question writing for research in medical education. Med. Educ. 1988, 22, 345–363. [Google Scholar] [CrossRef]
- Shrout, P.E.; Fleiss, J.L. Intraclass correlations: Uses in assessing rater reliability. Psychol. Bull. 1979, 86, 420–428. [Google Scholar] [CrossRef] [PubMed]
- Cicchetti, D.V. Guidelines, criteria, and rules of thumb for evaluating normed and standardized assessment instruments in psychology. Psychol. Assess. 1994, 6, 284–290. [Google Scholar] [CrossRef]
- Cronbach, L.J. Coefficient alpha and the internal structure of tests. Psychometrika 1951, 16, 297–334. [Google Scholar] [CrossRef]
- Donders, A.R.T.; van der Heijden, G.J.M.G.; Stijnen, T.; Moons, K.G.M. Review: A gentle introduction to imputation of missing values. J. Clin. Epidemiol. 2006, 59, 1087–1091. [Google Scholar] [CrossRef] [PubMed]
- Tabachnick, B.G.; Fidell, L.S. Using Multivariate Statistics, 5th ed.; Pearson: London, UK, 2006. [Google Scholar]
- Hammer, A.; Ernstmann, N.; Ommen, O.; Wirtz, M.; Manser, T.; Pfeiffer, Y.; Pfaff, H. Psychometric properties of the Hospital Survey on Patient Safety Culture for hospital management (HSOPS_M). Bmc Health Serv. Res. 2011, 11, 165. [Google Scholar] [CrossRef] [PubMed]
- MacCallum, R.C.; Widaman, K.F.; Zhang, S.; Hong, S. Sample size in factor analysis. Psychol. Methods 1999, 4, 84–99. [Google Scholar] [CrossRef]
- Streiner, D.L.; Kottner, J. Recommendations for reporting the results of studies of instrument and scale development and testing. J. Adv. Nurs. 2014, 70, 1970–1979. [Google Scholar] [CrossRef]
- Weiner, I.B.; Craighead, W.E. The Corsini Encyclopedia of Psychology, 4th ed.; John Wiley & Sons: Hoboken, NJ, USA, 2010; Volume 2. [Google Scholar]
- Gotzamani Katerina, D. An empirical study of the ISO 9000 standards’ contribution towards total quality management. Int. J. Oper. Prod. Manag. 2001, 21, 1326–1342. [Google Scholar] [CrossRef]
- Windisch, W.; Freidel, K.; Schucher, B.; Baumann, H.; Wiebel, M.; Matthys, H.; Petermann, F. The Severe Respiratory Insufficiency (SRI) Questionnaire: A specific measure of health-related quality of life in patients receiving home mechanical ventilation. J. Clin. Epidemiol. 2003, 56, 752–759. [Google Scholar] [CrossRef]
- Karamat, J.; Shurong, T.; Ahmad, N.; Afridi, S.; Khan, S.; Mahmood, K. Promoting healthcare sustainability in developing countries: Analysis of knowledge management drivers in public and private hospitals of Pakistan. Int. J. Environ. Res. Public Health 2019, 16, 508. [Google Scholar] [CrossRef]
- Stefan, S.C.; Popa, I.; Dobrin, C.O. Towards a model of sustainable competitiveness of health organizations. Sustainability 2016, 8, 464. [Google Scholar] [CrossRef]
- Djukic, A.; Marić, J. Towards Socially sustainable Healthcare Facilities – the Role of Evidence-based Design in Regeneration of Existing Hospitals in Serbia. Procedia Environ. Sci. 2017, 38, 256–263. [Google Scholar] [CrossRef]
- Capolongo, S.; Gola, M.; Di Noia, M.; Nickolova, M.; Nachiero, D.; Rebecchi, A.; Settimo, G.; Vittori, G.; Buffoli, M. Social sustainability in healthcare facilities: A rating tool for analysing and improving social aspects in environments of care. Annali Dell’Istituto Superiore Sanita 2016, 52, 15–23. [Google Scholar]
- Hall, R.; Andriani, P. Managing knowledge associated with innovation. J. Bus. Res. 2003, 56, 145–152. [Google Scholar] [CrossRef]
- Abubakar, A.M.; Elrehail, H.; Alatailat, M.A.; Elçi, A. Knowledge management, decision-making style and organizational performance. J. Innov. Knowl. 2019, 4, 104–114. [Google Scholar] [CrossRef]
- Tursunbayeva, A. Human resource technology disruptions and their implications for human resources management in healthcare organizations. Bmc Health Serv. Res. 2019, 19, 268. [Google Scholar] [CrossRef] [PubMed]
- Singer, S.; Benzer, J.; Hamdan, S. Improving health care quality and safety: The role of collective learning. J. Healthc. Leadersh. 2015, 7, 91–107. [Google Scholar] [CrossRef] [PubMed]
- Levitt, B.; March, J.G. Organizational Learning. Annu. Rev. Sociol. 1988, 14, 319–338. [Google Scholar] [CrossRef]
- Khalil, C.; Dudezert, A. Knowledge management systems, Autonomy and control: How to regulate? A case-study in an industrial company. In Materiality, Rules and Regulation; Palgrave Macmillan: London, UK, 2015; pp. 143–153. [Google Scholar]
- Gagné, M.; Tian, A.W.; Soo, C.; Zhang, B.; Ho, K.S.B.; Hosszu, K. Different motivations for knowledge sharing and hiding: The role of motivating work design. J. Organ. Behav. 2019, 40, 783–799. [Google Scholar] [CrossRef]
- Steyn, P.D.; Du Toit, A.S.A. Perceptions on the use of a corporate business incubator to enhance knowledge management at Eskom. S. Afr. J. Econ. Manag. Sci. 2013, 10, 33–50. [Google Scholar] [CrossRef][Green Version]
- Forcada, N.; Fuertes, A.; Gangolells, M.; Casals, M.; Macarulla, M. Knowledge management perceptions in construction and design companies. Autom. Constr. 2013, 29, 83–91. [Google Scholar] [CrossRef]
- McAdam, R. SME and large organisation perceptions of knowledge management: Comparisons and contrasts. J. Knowl. Manag. 2001, 5, 231–241. [Google Scholar] [CrossRef]
- Harder, M. How Do Rewards and Management Styles Influence the Motivation to Share Knowledge? 2008. Available online: https://ssrn.com/abstract=1098881 (accessed on 31 March 2020).
- Singh Sanjay, K. Role of leadership in knowledge management: A study. J. Knowl. Manag. 2008, 12, 3–15. [Google Scholar] [CrossRef]
- Zheng, W.; Yang, B.; McLean, G.N. Linking organizational culture, structure, strategy, and organizational effectiveness: Mediating role of knowledge management. J. Bus. Res. 2010, 63, 763–771. [Google Scholar] [CrossRef]
- Dorothy, L.; Maryam, A.; Timothy, K. The Role of Culture in Knowledge Management: A Case Study of Two Global Firms. Int. J. E-Collab. 2006, 2, 17–40. [Google Scholar] [CrossRef]
- Lai, J.-Y. How reward, computer self-efficacy, and perceived power security affect knowledge management systems success: An empirical investigation in high-tech companies. J. Am. Soc. Inf. Sci. Technol. 2009, 60, 332–347. [Google Scholar] [CrossRef]
- Choo, A.S.; Linderman, K.W.; Schroeder, R.G. Method and psychological effects on learning behaviors and knowledge creation in quality improvement projects. Manag. Sci. 2007, 53, 437–450. [Google Scholar] [CrossRef]
- Kitsios, F.; Kamariotou, M.; Talias, M.A. Corporate Sustainability Strategies and Decision Support Methods: A Bibliometric Analysis. Sustainability 2020, 12, 521. [Google Scholar] [CrossRef]
- Yu, C.; Zhang, Z.; Lin, C.; Wu, Y.J. Knowledge creation process and sustainable competitive advantage: The role of technological innovation capabilities. Sustainability 2017, 9, 2280. [Google Scholar] [CrossRef]
- Parveen, F.; Jaafar Noor, I.; Ainin, S. Social media’s impact on organizational performance and entrepreneurial orientation in organizations. Manag. Decis. 2016, 54, 2208–2234. [Google Scholar] [CrossRef]



{kind=link}
{kind=link}
| Frequency | Percent | Valid Percent | Cumulative Percent | ||
|---|---|---|---|---|---|
| Gender | |||||
| Valid | Male | 75 | 28.7 | 29.1 | 29.1 |
| Female | 183 | 70.1 | 70.9 | 100 | |
| Total | 258 | 98.9 | 100 | ||
| Missing | |||||
| Total | |||||
| Professional status | |||||
| Valid | Physician | 47 | 18 | 18 | 18 |
| Nurse | 102 | 39.1 | 39.1 | 57.1 | |
| Administrative staff | 59 | 22.6 | 22.6 | 79.7 | |
| Paramedics | 21 | 8 | 8 | 87.7 | |
| Midwives - Health visitors | 7 | 2.7 | 2.7 | 90.4 | |
| Other | 25 | 9.6 | 9.6 | 100 | |
| Total | 261 | 100 | 100 | ||
| Educational status (in years of study) | |||||
| 9 years | 6 | 2.3 | 2.3 | 2.3 | |
| 12 years | 57 | 21.8 | 22.2 | 24.5 | |
| 107 | 98.9 | 100 | |||
| 16 years (technological orientation) | 107 | 98.9 | |||
| Missing | |||||
| Total | |||||
| N | Min | Max | Mean | Std. Dev. | |
| Age | 254 | 21 | 62 | 44.61 | 8.18 |
| Overall Working experience | 257 | 0.4 | 36 | 18.94 | 8.76 |
| Working experience | 256 | 0.4 | 36 | 14.17 | 9.18 |
| Loadings | ||||||||||
|---|---|---|---|---|---|---|---|---|---|---|
| Items | Communalities | 1 | 2 | 3 | 4 | 5 | 6 | 7 | 8 | 9 |
| Each hospital should implement KM politics KM is essential for the performance of the hospital. KM helps decrease errors. Knowledge acquisition helps the individual’s autonomy Knowledge recording helps employees adapt when they are transferred to different departments of the hospital. | 0.772 0.830 0.665 0.260 0.453 | 0.854 0.900 0.779 0.323 0.272 | ||||||||
| I feel content when I share my knowledge with others. | 0.579 | 0.668 | ||||||||
| When I know something is useful for my colleagues, I inform them. It is a matter of principle. | 0.575 | 0.675 | ||||||||
| I could participate in a seminar because I like knowledge even if I would not receive credit or a certificate | 0.433 | 0.531 | ||||||||
| Knowledge acquisition gives me the power | 0.466 | 0.381 | ||||||||
| When I share my knowledge, my colleagues respect me more. When I share my knowledge, I bond with my colleagues. When I help my colleagues, they help me, respectively. I have higher chances of promotion where I possess knowledge. | 0.703 0.788 0.600 0.529 | 0.790 0.860 0.736 0.366 | ||||||||
| I create knowledge through observation of the working environment. | 0.433 | 0.438 | ||||||||
| Knowledge is created during group meetings. | 0.698 | 0.512 | ||||||||
| Knowledge is created during group seminars. | 0.618 | 0.371 | ||||||||
| Knowledge is shared during group meetings. | 0.454 | 0.488 | ||||||||
| Knowledge is shared using electronic means (websites, wikis, forums). | 0.453 | 0.488 | ||||||||
| I share knowledge with colleagues who are my friends. | 0.319 | 0.514 | ||||||||
| I share knowledge with colleagues from my department. | 0.453 | 0.544 | ||||||||
| I share knowledge with colleagues of other professional groups at the hospital. | 0.714 | 0.200 | ||||||||
| I often cooperate with my colleagues to face a new situation | 0.359 | 0.411 | ||||||||
| When I come across difficulties, I ask my colleagues. | 0.497 | 0.487 | ||||||||
| When I know the work of others, it improves my performance | 0.319 | 0.301 | ||||||||
| Cooperation when creating new knowledge reduces the anxiety of responsibility in the case of an error | 0.391 | 0.241 | ||||||||
| My supervisor provides the required knowledge to solve problems. | 0.686 | 0.762 | ||||||||
| My supervisor rewards people who share their knowledge. | 0.727 | 0.793 | ||||||||
| Leadership creates channels of communication that help knowledge transfer. | 0.674 | 0.310 | ||||||||
| At this hospital, there are KM strategies. | 0.487 | 0.592 | ||||||||
| In this hospital, personnel are encouraged to innovate if they have a new idea. | 0.692 | 0.778 | ||||||||
| This hospital supports research. | 0.668 | 0.764 | ||||||||
| This hospital is a knowledge creation agency. | 0.589 | 0.726 | ||||||||
| This cooperation strengthens the knowledge culture of my department. | 0.572 | 0.275 | ||||||||
| In this hospital, there are commonly shared files to inform employees. | 0.484 | 0.594 | ||||||||
| Leadership at this hospital has not understood the importance of KM (reverse coding). | 0.522 | 0.680 | ||||||||
| There is no knowledge culture in this hospital (reverse coding) | 0.458 | 0.634 | ||||||||
| Most colleagues share their knowledge freely. | 0.507 | |||||||||
| Hospitals’ information system does not facilitate KM. | 0.514 | 0.409 | ||||||||
| I have no access to useful information for my work. | 0.658 | 0.727 | ||||||||
| I do not know very well where to find useful information for my work. | 0.725 | 0.838 | ||||||||
| Item | Dimensions | Mean | Median | Factor’s Mean | Cronbach Alpha |
|---|---|---|---|---|---|
| A. | PERCEPTIONS | ||||
| 1 | Each hospital should implement KM politics. | 4.26 | 4.00 | ||
| 2 | KM is essential for the performance of the hospital. | 4.30 | 4.00 | 4.19 | 0.724 |
| 3 | KM helps decrease errors. | 4.27 | 4.00 | ||
| 5 | Knowledge acquisition helps the individual’s autonomy. | 4.12 | 4.00 | ||
| 6 | Knowledge recording helps employees adapt when they are transferred to different departments of the hospital. | 3.99 | 4.00 | ||
| B. | INTRINSIC MOTIVATION | ||||
| 7 | I feel content when I share my knowledge with others. | 4.27 | 4.00 | ||
| 8 | When I know something is useful for my colleagues, I inform them. It is a matter of principle. | 4.42 | 4.00 | 4.33 | 0.626 |
| 9 | I could participate in a seminar because I like knowledge even if I would not receive credit or a certificate of participation. | 4.29 | 4.00 | ||
| 12 | Knowledge acquisition gives me power. | 4.35 | 4.00 | ||
| C. | EXTRINSIC MOTIVATION | ||||
| 13 | When I share my knowledge, my colleagues respect me more. | 3.56 | 4.00 | ||
| 14 | When I share my knowledge, I bond with my colleagues. | 3.64 | 4.00 | 3.55 | 0.739 |
| 15 | When I help my colleagues, they help me, respectively. | 3.59 | 4.00 | ||
| 17 | I have higher chances of promotion where I possess knowledge. | 3.39 | 4.00 | ||
| D. | SYNTHESIS | ||||
| 18 | I create knowledge through observation of the working environment | 3.91 | 4.00 | ||
| 19 | Knowledge is created during group meetings. | 3.68 | 4.00 | 3.85 | 0.652 |
| 20 | Knowledge is created during group seminars. | 3.95 | 4.00 | ||
| E. | SHARING | ||||
| 24 | Knowledge is shared during group meetings. | 3.65 | 4.00 | ||
| 25 | Knowledge is shared using electronic means (websites, wikis, forums). | 3.96 | 4.00 | ||
| 26 | I share knowledge with colleagues who are my friends | 3.44 | 4.00 | 3.74 | 0.570 |
| 27 | I share knowledge with colleagues from my department. | 3.91 | 4.00 | ||
| 28 | I share knowledge with colleagues of other professional groups at the hospital. | 3.76 | 4.00 | ||
| F. | COOPERATION | ||||
| 30 | I often cooperate with my colleagues to face a new situation. | 3.95 | 4.00 | ||
| 31 | When I come across difficulties, I ask my colleagues. | 4.18 | 4.00 | ||
| 33 | When I know the work of the others, it improves my performance. | 3.97 | 4.00 | 4.04 | 0.567 |
| 34 | Cooperation when creating new knowledge reduces the anxiety of responsibility in case of an error. | 4.05 | 4.00 | ||
| G. | LEADERSHIP | ||||
| 35 | My supervisor provides the required knowledge to solve problems. | 3.52 | 4.00 | ||
| 36 | My supervisor rewards people who share their knowledge. | 3.29 | 4.00 | 3.23 | 0.717 |
| 39 | Leadership creates channels of communication that help knowledge transfer. | 2.88 | 3.00 | ||
| H. | CULTURE | ||||
| 37 | Leadership at this hospital has not understood the importance of KM (reverse coding). | 2.61 | 3.00 | ||
| 38 | At this hospital, there are KM strategies. | 4.42 | 3.00 | ||
| 40 | In this hospital, personnel is encouraged to innovate if they have a new idea. | 4.29 | 3.00 | ||
| 41 | This hospital supports research. | 4.35 | 3.00 | 2.83 | 0.821 |
| 42 | This hospital is a knowledge creation agency. | 2.72 | 3.00 | ||
| 43 | This cooperation strengthens the knowledge culture of my department. | 3.68 | 4.00 | ||
| 44 | There is no knowledge culture in this hospital (reverse coding). | 2.95 | 3.00 | ||
| 45 | In this hospital, there are commonly shared files to inform employees. | 2.71 | 3.00 | ||
| 23 | Most colleagues share their knowledge freely. | 2.76 | 3.00 | ||
| I. | BARRIERS | 2.61 | |||
| 46 | The hospitals’ information system does not facilitate KM. | 3.19 | 3.00 | ||
| 52 | I have no access to useful information for my work. | 2.81 | 3.00 | 2.95 | 0.644 |
| 53 | I do not know very well where to find useful information for my work. | 2.84 | 3.00 |
| Factors | (1) | (2) | (3) | (4) | (5) | (6) | (7) | (8) | (9) |
|---|---|---|---|---|---|---|---|---|---|
| Perception (1) | 1.000 | ||||||||
| Intrinsic motives (2) | 0.059 | 1.000 | |||||||
| Extrinsic motives (3) | 0.110 | 1.054 *** | 1.000 | ||||||
| Synthesis (4) | 0.285 *** | 0.230 ** | 0.359 *** | 1.000 | |||||
| Sharing (5) | 0.201 * | 0.421 ** | 0.283 ** | 0.469 *** | 1.000 | ||||
| Cooperation (6) | 0.280 ** | 0.752 ** | 0.660 *** | 0.526 *** | 0.617 *** | 1.000 | |||
| Leadership (7) | –0.041 | 0.252 * | 0.098 | –0.059 | 0.101 | 0.096 | 1.000 | ||
| Culture (8) | –0.015 | 0.271 ** | 0.202 * | 0.018 | 0.151 | 0.056 | 0.949 *** | 1.000 | |
| Barrier (9) | 0.000 | –0.301 ** | –0.210 * | –0.098 | –0.223 | –0.173 ** | 0.501 *** | –0.486 *** | 1.000 |
© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Karamitri, I.; Kitsios, F.; Talias, M.A. Development and Validation of a Knowledge Management Questionnaire for Hospitals and Other Healthcare Organizations. Sustainability 2020, 12, 2730. https://doi.org/10.3390/su12072730
Karamitri I, Kitsios F, Talias MA. Development and Validation of a Knowledge Management Questionnaire for Hospitals and Other Healthcare Organizations. Sustainability. 2020; 12(7):2730. https://doi.org/10.3390/su12072730
Chicago/Turabian StyleKaramitri, Ioanna, Fotis Kitsios, and Michael A. Talias. 2020. "Development and Validation of a Knowledge Management Questionnaire for Hospitals and Other Healthcare Organizations" Sustainability 12, no. 7: 2730. https://doi.org/10.3390/su12072730
APA StyleKaramitri, I., Kitsios, F., & Talias, M. A. (2020). Development and Validation of a Knowledge Management Questionnaire for Hospitals and Other Healthcare Organizations. Sustainability, 12(7), 2730. https://doi.org/10.3390/su12072730