Left Ventricular Assist Device Implantation in a Thrombosed Apical Aneurysm

 ,
, 
Abstract
:1. Introduction
2. Case Report
3. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Crespo-Leiro, M.G.; Metra, M.; Lund, L.H.; Milicic, D.; Costanzo, M.R.; Filippatos, G.; Gustafsson, F.; Tsui, S.; Barge-Caballero, E.; De Jonge, N.; et al. Advanced heart failure: A position statement of the Heart Failure Association of the European Society of Cardiology. Eur. J. Heart Fail. 2018, 20, 1505–1535. [Google Scholar] [CrossRef] [PubMed]
- Briasoulis, A.; Inampudi, C.; Akintoye, E.; Adegbala, O.; Alvarez, P.; Bhama, J. Trends in utilisation, mortality, major complications, and cost after left ventricular assist device implantation in the United States (2009 to 2014). Am. J. Cardiol. 2018, 121, 1214–1218. [Google Scholar] [CrossRef] [PubMed]
- Smith, J.W.; Pal, J.D.; Walters, D.; Mahr, C.M.; Mokadam, N.A. Left ventricular assist device placement with concomitant ventricular reconstruction for aneurismal disease. J. Heart Lung Transplant. 2016, 35, S372. [Google Scholar] [CrossRef] [Green Version]
- Potapov, E.V.; Antonides, C.; Crespo-Leiro, M.G.; Combes, A.; Färber, G.; Hannan, M.H.; Kukucka, M.; de Jonge, N.; Loforte, A.; Lund, L.H.; et al. 2019 EACTS Expert Consensus on long-term mechanical circulatory support. Eur. J. Cardio-Thorac. Surg. 2019, 56, 230–270. [Google Scholar] [CrossRef] [PubMed]

{kind=link}
{kind=link}
| March 2020 | Angina Episodes |
|---|---|
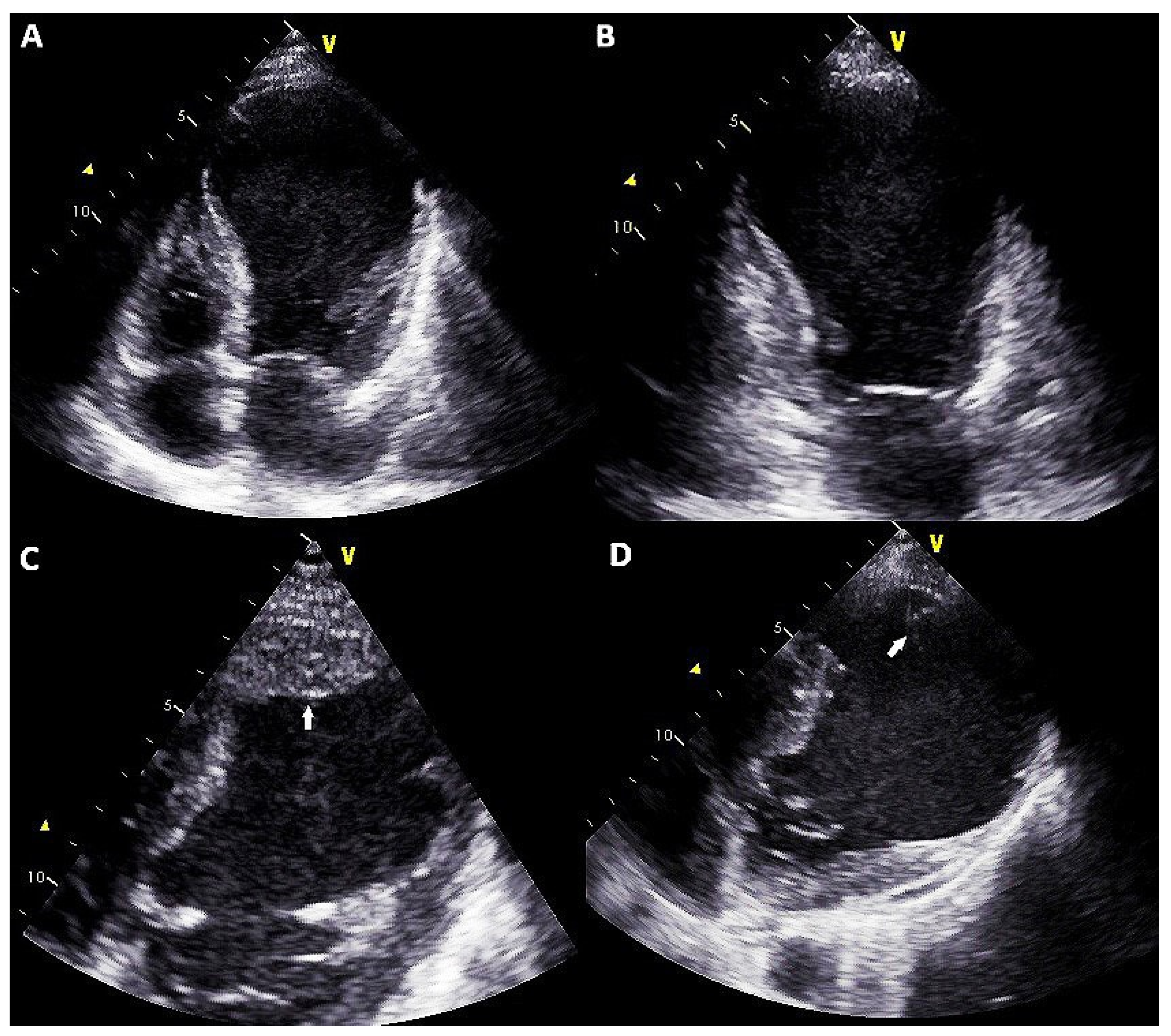
| 12 May 2020 | Hospitalization for acute heart failure with diagnosis of ischemic dilated cardiomyopathy with severe reduction of ejection fraction and thrombosed apical aneurysm Clinical presentation was complicated by acute kidney injury (eGFR at admission 38 mL/min/m2 vs. 57 mL/min/m2 of March 2020) and acute liver injury (biluribin 3.5 mg/dL, AST 560 UI/L, ALT 654 UI/L) High dose diuretics therapy (furosemide 250 mg bid plus spironolactone 200 mg/die) and levosimendan infusion was started (0.1 mcg/kg/min) |
| 13 May 2020 | 24 h diuresis 1100 mL; metolazone (5 mg bid) was added |
| 15 May 2020 | 24 h diuresis 1300 mL; enoximone infusion (5 mcg/kg/min) was started. Noradrenaline infusion (0.2 mcg/kg/min) was started. Episode of cardioembolic transitory ischemic attack occurs |
| 16 May 2020 | 24 h diuresis 1200 mL. Episode of cardioembolic transitory ischemic attack occurs |
| 17 May 2020 | Low cardiac output syndrome appears Heart team reunion and indication to LVAD |
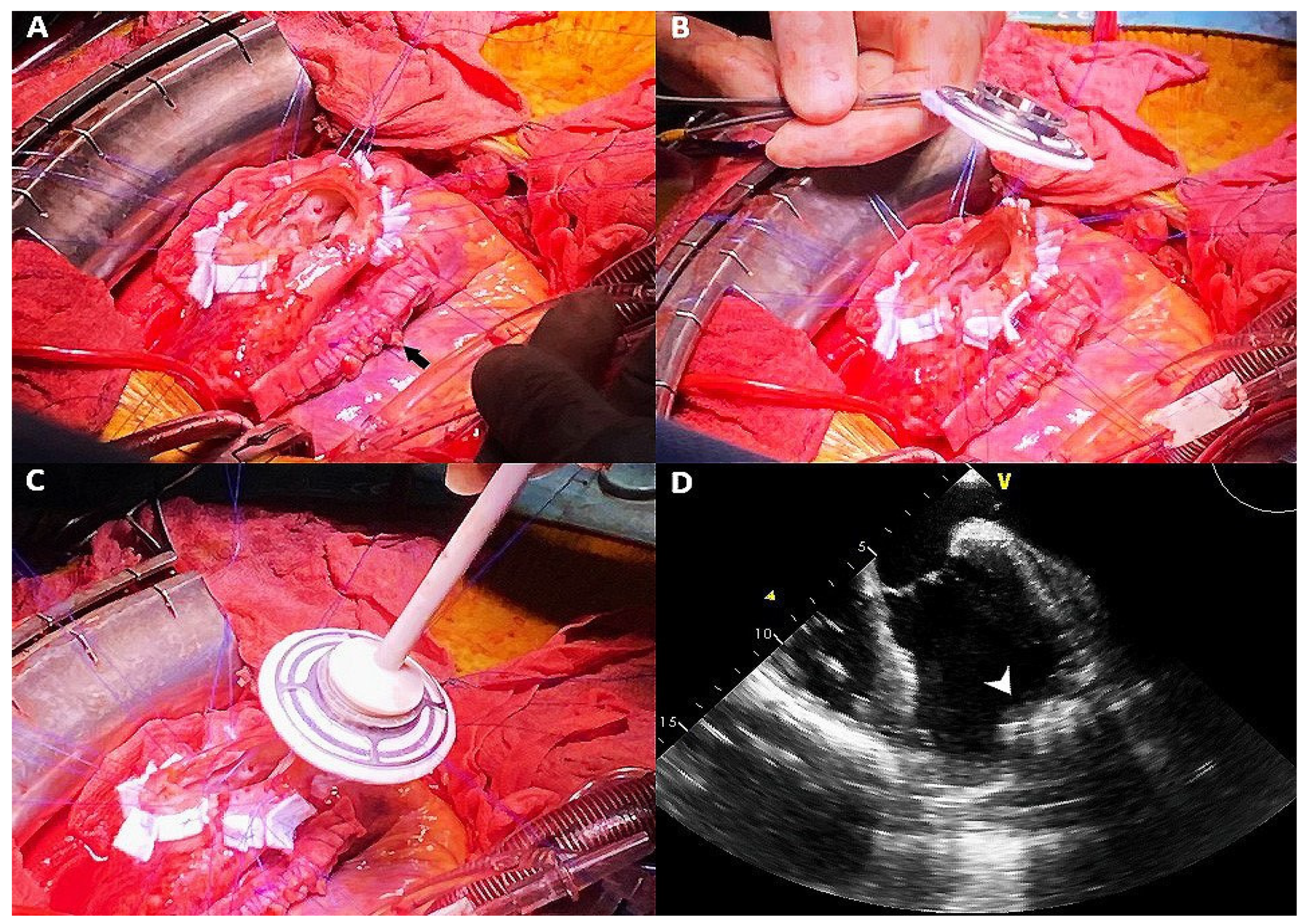
| 18 May 2020 | Heartmate III implantation with and concomitant surgical plication of the anterolateral wall pseudoaneurysm |
| 28 June 2020 | Patient discharged |
| 02 May 2021 | At follow-up non hospitalizations for heart failure and stable NYHA class |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Masarone, D.; Melillo, E.; Gravino, R.; Vastarella, R.; Caiazzo, A.; Ursomando, F.; Pacileo, G.; Petraio, A. Left Ventricular Assist Device Implantation in a Thrombosed Apical Aneurysm. Clin. Pract. 2021, 11, 430-434. https://doi.org/10.3390/clinpract11030057
Masarone D, Melillo E, Gravino R, Vastarella R, Caiazzo A, Ursomando F, Pacileo G, Petraio A. Left Ventricular Assist Device Implantation in a Thrombosed Apical Aneurysm. Clinics and Practice. 2021; 11(3):430-434. https://doi.org/10.3390/clinpract11030057
Chicago/Turabian StyleMasarone, Daniele, Enrico Melillo, Rita Gravino, Rossella Vastarella, Angelo Caiazzo, Fabio Ursomando, Giuseppe Pacileo, and Andrea Petraio. 2021. "Left Ventricular Assist Device Implantation in a Thrombosed Apical Aneurysm" Clinics and Practice 11, no. 3: 430-434. https://doi.org/10.3390/clinpract11030057
APA StyleMasarone, D., Melillo, E., Gravino, R., Vastarella, R., Caiazzo, A., Ursomando, F., Pacileo, G., & Petraio, A. (2021). Left Ventricular Assist Device Implantation in a Thrombosed Apical Aneurysm. Clinics and Practice, 11(3), 430-434. https://doi.org/10.3390/clinpract11030057