

Post-Traumatic Stress Disorder Symptoms among Pediatric Healthcare Workers

 ,
,  ,
,  , , and
, , and 
Abstract
1. Introduction
2. Materials and Methods
2.1. Participants
2.2. Measures
2.2.1. Socio-Demographic Questionnaire
2.2.2. Post-Traumatic Stress Checklist (PCL-5) [29]
2.3. Statistical Analysis
3. Results
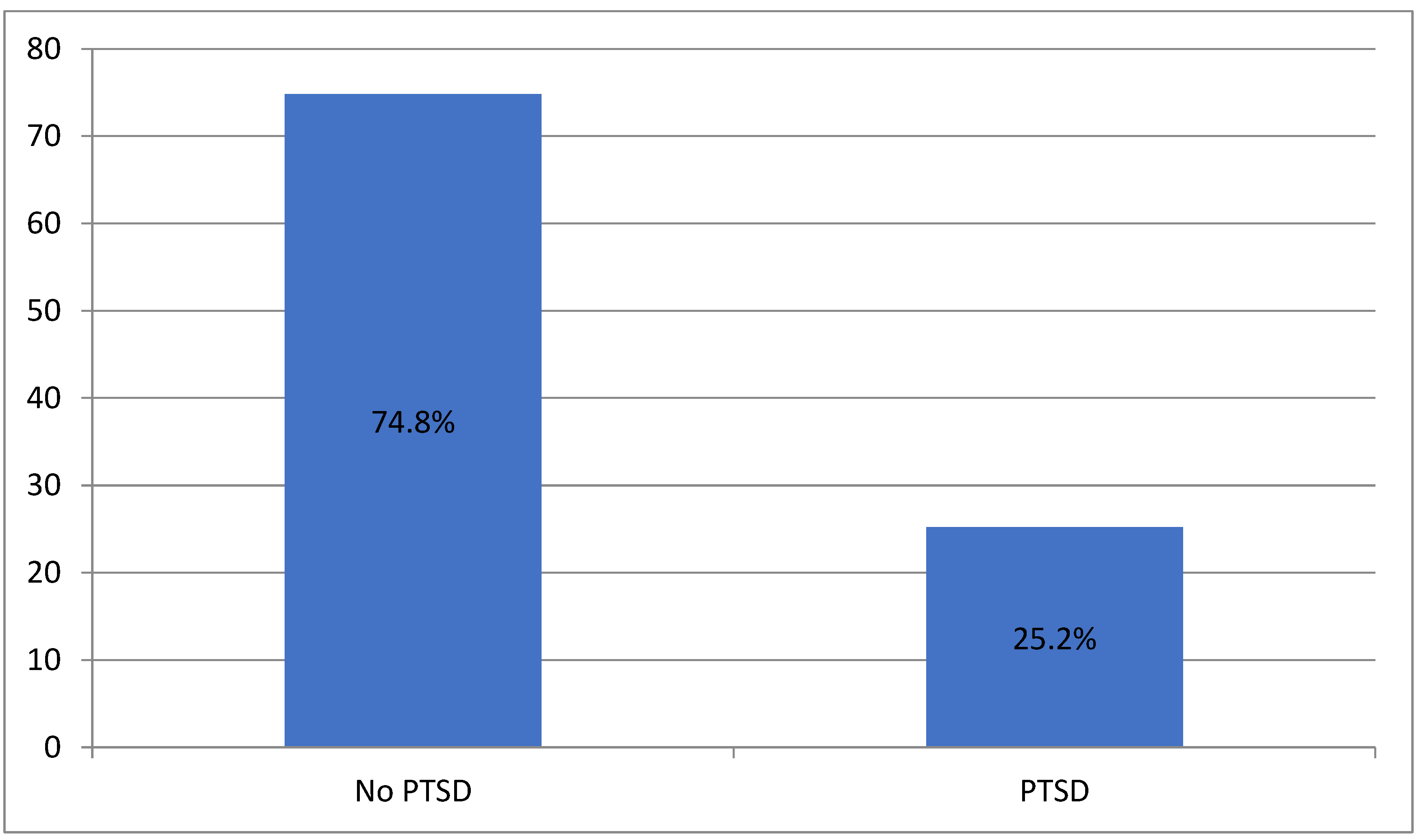
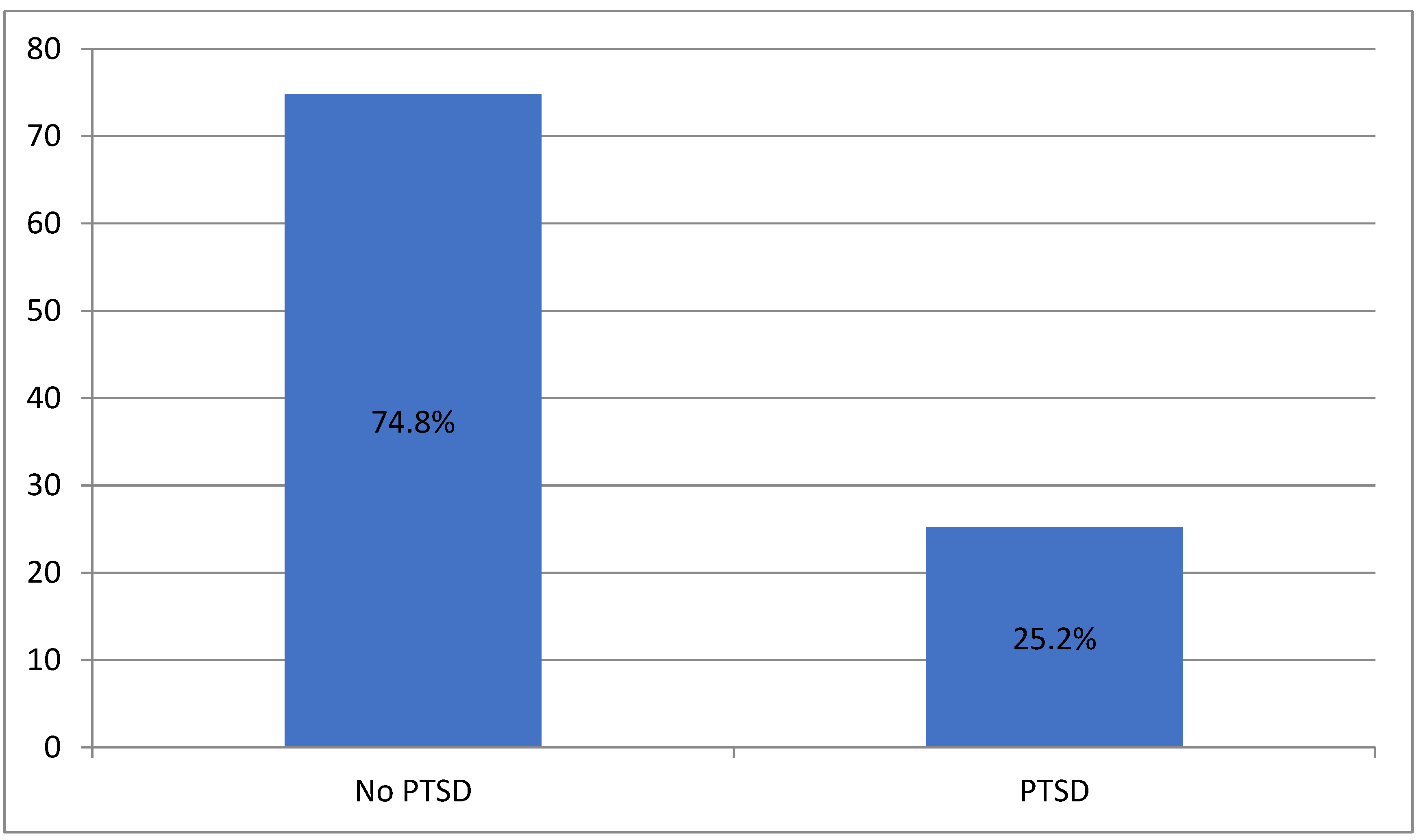
PTSD Levels in Pediatric Healthcare Workers
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Public Involvement Statement
Guidelines and Standards Statement
Conflicts of Interest
References
- Ferri, P.; Silvestri, M.; Artoni, C.; Di Lorenzo, R. Workplace Violence in Different Settings and among Various Health Professionals in an Italian General Hospital: A Cross-Sectional Study. Psychol. Res. Behav. Manag. 2016, 9, 263–275. [Google Scholar] [CrossRef] [PubMed]
- Czaja, A.S.; Moss, M.; Mealer, M. Symptoms of Post-Traumatic Stress Disorder among Pediatric Acute Care Nurses. J. Pediatr. Nurs. 2012, 27, 357–365. [Google Scholar] [CrossRef] [PubMed]
- PTSD: National Center for PTSD Home. Available online: https://www.ptsd.va.gov/ (accessed on 3 August 2022).
- DSM-5 Criteria for PTSD. BrainLine. Available online: https://www.brainline.org/article/dsm-5-criteria-ptsd (accessed on 23 September 2020).
- O’Connor, J.; Jeavons, S. Nurses’ Perceptions of Critical Incidents. J. Adv. Nurs. 2003, 41, 53–62. [Google Scholar] [CrossRef]
- Newsroom Feature: Health Worker Mental Health|NIOSH|CDC. Available online: https://www.cdc.gov/niosh/newsroom/feature/health-worker-mental-health.html (accessed on 9 August 2023).
- Ratrout, H.F.; Hamdan-Mansour, A.M. Secondary Traumatic Stress among Emergency Nurses: Prevalence, Predictors, and Consequences. Int. J. Nurs. Pract. 2020, 26, e12767. [Google Scholar] [CrossRef] [PubMed]
- Hapke, U.; Schumann, A.; Rumpf, H.-J.; John, U.; Meyer, C. Post-Traumatic Stress Disorder: The Role of Trauma, Pre-Existing Psychiatric Disorders, and Gender. Eur. Arch. Psychiatry Clin. Neurosci. 2006, 256, 299–306. [Google Scholar] [CrossRef]
- CWS. The Relationship between Secondary Trauma and Distress. Champions of Wellness. Available online: https://www.championsofwellness.com/blog-the-relationship-between-secondary-trauma-and-distress/ (accessed on 9 August 2023).
- Mealer, M.; Burnham, E.L.; Goode, C.J.; Rothbaum, B.; Moss, M. The Prevalence and Impact of Post Traumatic Stress Disorder and Burnout Syndrome in Nurses. Depress. Anxiety 2009, 26, 1118–1126. [Google Scholar] [CrossRef]
- NIHCM. Physician Burnout & Moral. Injury: The Hidden Health Care Crisis. Available online: https://nihcm.org/publications/physician-burnout-suicide-the-hidden-health-care-crisis (accessed on 9 August 2023).
- The Mental Health of Healthcare Workers in COVID-19. Mental Health America. Available online: https://mhanational.org/mental-health-healthcare-workers-covid-19 (accessed on 29 August 2023).
- Kim, W.; Bae, M.; Chang, S.-J.; Yoon, J.-H.; Jeong, D.Y.; Hyun, D.-S.; Ryu, H.-Y.; Park, K.-S.; Kim, M.-J.; Kim, C. Effect of Burnout on Post-Traumatic Stress Disorder Symptoms among Firefighters in Korea: Data from the Firefighter Research on Enhancement of Safety & Health (FRESH). J. Prev. Med. Public. Health 2019, 52, 345–354. [Google Scholar] [CrossRef]
- Liu, Y.; Zou, L.; Yan, S.; Zhang, P.; Zhang, J.; Wen, J.; Mao, J.; Li, L.; Wang, Y.; Fu, W. Burnout and Post-Traumatic Stress Disorder Symptoms among Medical Staff Two Years after the COVID-19 Pandemic in Wuhan, China: Social Support and Resilience as Mediators. J. Affect. Disord. 2023, 321, 126–133. [Google Scholar] [CrossRef]
- Lee, J.; Lim, N.; Yang, E.; Lee, S.M. Antecedents and Consequences of Three Dimensions of Burnout in Psychotherapists: A Meta-Analysis. Prof. Psychol. Res. Pract. 2011, 42, 252–258. [Google Scholar] [CrossRef]
- Maslach, C.; Schaufeli, W.B.; Leiter, M.P. Job Burnout. Annu. Rev. Psychol. 2001, 52, 397–422. [Google Scholar] [CrossRef]
- McManus, I.C.; Winder, B.C.; Gordon, D. The Causal Links between Stress and Burnout in a Longitudinal Study of UK Doctors. Lancet 2002, 359, 2089–2090. [Google Scholar] [CrossRef] [PubMed]
- Chirico, F.; Leiter, M. Tackling Stress, Burnout, Suicide and Preventing the “Great Resignation” Phenomenon among Healthcare Workers (during and after the COVID-19 Pandemic) for Maintaining the Sustainability of Healthcare Systems and Reaching the 2030 Sustainable Development Goals. J. Health Soc. Sci. 2022, 7, 9–13. [Google Scholar] [CrossRef]
- Lasalvia, A.; Amaddeo, F.; Porru, S.; Carta, A.; Tardivo, S.; Bovo, C.; Ruggeri, M.; Bonetto, C. Levels of Burn-out among Healthcare Workers during the COVID-19 Pandemic and Their Associated Factors: A Cross-Sectional Study in a Tertiary Hospital of a Highly Burdened Area of North-East Italy. BMJ Open 2021, 11, e045127. [Google Scholar] [CrossRef] [PubMed]
- Ogińska-Bulik, N.; Juczyński, Z. Burnout and Posttraumatic Stress Symptoms in Police Officers Exposed to Traumatic Events: The Mediating Role of Ruminations. Int. Arch. Occup. Environ. Health 2021, 94, 1201–1209. [Google Scholar] [CrossRef] [PubMed]
- Kellogg, M.B.; Knight, M.; Dowling, J.S.; Crawford, S.L. Secondary Traumatic Stress in Pediatric Nurses. J. Pediatr. Nurs. Nurs. Care Child. Fam. 2018, 43, 97–103. [Google Scholar] [CrossRef] [PubMed]
- Kleis, A.E.; Kellogg, M.B. Recalling Stress and Trauma in the Workplace: A Qualitative Study of Pediatric Nurses. Pediatr. Nurs. 2020, 46, 5–10. Available online: https://www.proquest.com/openview/1170ce23f0986503ad2645e4a2b85eee/1?cbl=47659&pq-origsite=gscholar (accessed on 29 December 2023).
- Park, E.; Meyer, R.M.L.; Gold, J.I. The Role of Medical Specialization on Posttraumatic Symptoms in Pediatric Nurses. J. Pediatr. Nurs. 2020, 53, 22–28. [Google Scholar] [CrossRef]
- Allen, J. Pediatric Intensive Care Nurses: Post-Traumatic Stress Disorder-Like Symptoms. Master’s Thesis, Loma Linda University, Loma Linda, CA, USA, 1996. [Google Scholar]
- Rodríguez-Rey, R.; Palacios, A.; Alonso-Tapia, J.; Pérez, E.; Álvarez, E.; Coca, A.; Mencía, S.; Marcos, A.; Mayordomo-Colunga, J.; Fernández, F.; et al. Are Pediatric Critical Personnel Satisfied with Their Lives? Prediction of Satisfaction with Life from Burnout, Posttraumatic Stress, and Posttraumatic Growth, and Comparison with Noncritical Pediatric Staff. Pediatr. Crit. Care Med. 2019, 20, e160–e169. [Google Scholar] [CrossRef]
- Rodríguez-Rey, R.; Palacios, A.; Alonso-Tapia, J.; Pérez, E.; Álvarez, E.; Coca, A.; Mencía, S.; Marcos, A.; Mayordomo-Colunga, J.; Fernández, F.; et al. Burnout and Posttraumatic Stress in Paediatric Critical Care Personnel: Prediction from Resilience and Coping Styles. Aust. Crit. Care 2019, 32, 46–53. [Google Scholar] [CrossRef]
- Jones, G.A.L.; Colville, G.A.; Ramnarayan, P.; Woolfall, K.; Heward, Y.; Morrison, R.; Savage, A.; Fraser, J.; Griksaitis, M.J.; Inwald, D.P. Psychological Impact of Working in Paediatric Intensive Care. A UK-Wide Prevalence Study. Arch. Dis. Child. 2020, 105, 470–475. [Google Scholar] [CrossRef]
- Price, J.L.; Mueller, C.W. A Causal Model of Turnover for Nurses. Acad. Manag. J. 1981, 24, 543–565. [Google Scholar] [CrossRef]
- PTSD Checklist for DSM-5 (PCL-5)-PTSD: National Center for PTSD. Available online: https://www.ptsd.va.gov/professional/assessment/adult-sr/ptsd-checklist.asp (accessed on 6 March 2020).
- American Psychiatric Association (Ed.) Diagnostic and Statistical Manual of Mental Disorders: DSM-5, 5th ed; American Psychiatric Association: Washington, DC, USA, 2013. [Google Scholar]
- Orovou, E.; Theodoropoulou, I.M.; Antoniou, E. Psychometric Properties of the Post Traumatic Stress Disorder Checklist for DSM-5 (PCL-5) in Greek Women after Cesarean Section. PLoS ONE 2021, 16, e0255689. [Google Scholar] [CrossRef] [PubMed]
- Sasidharan, S.; Dhillon, H.S. Intensive Care Unit Stress and Burnout among Health-Care Workers: The Wake-up Call Is Blaring! Indian. J. Psychiatry 2021, 63, 606–609. [Google Scholar] [CrossRef] [PubMed]
- Robins, P.M.; Meltzer, L.; Zelikovsky, N. The Experience of Secondary Traumatic Stress Upon Care Providers Working within a Children’s Hospital. J. Pediatr. Nurs. 2009, 24, 270–279. [Google Scholar] [CrossRef] [PubMed]
- Berger, J.; Polivka, B.; Smoot, E.A.; Owens, H. Compassion Fatigue in Pediatric Nurses. J. Pediatr. Nurs. Nurs. Care Child. Fam. 2015, 30, e11–e17. [Google Scholar] [CrossRef] [PubMed]
- Crilly, J.; Chaboyer, W.; Creedy, D. Violence towards Emergency Department Nurses by Patients. Accid. Emerg. Nurs. 2004, 12, 67–73. [Google Scholar] [CrossRef]
- Meadors, P.; Lamson, A.; Swanson, M.; White, M.; Sira, N. Secondary Traumatization in Pediatric Healthcare Providers: Compassion Fatigue, Burnout, and Secondary Traumatic Stress. Omega 2010, 60, 103–128. [Google Scholar] [CrossRef]
- Sekol, M.A.; Kim, S.C. Job Satisfaction, Burnout, and Stress among Pediatric Nurses in Various Specialty Units at an Acute Care Hospital. J. Nurs. Educ. Pract. 2014, 4, 115. [Google Scholar] [CrossRef]
- Branch, C.; Klinkenberg, D. Compassion Fatigue Among Pediatric Healthcare Providers. MCN Am. J. Matern./Child. Nurs. 2015, 40, 160. [Google Scholar] [CrossRef]
- Colville, G.A.; Smith, J.G.; Brierley, J.; Citron, K.; Nguru, N.M.; Shaunak, P.D.; Tam, O.; Perkins-Porras, L. Coping with Staff Burnout and Work-Related Posttraumatic Stress in Intensive Care. Pediatr. Crit. Care Med. 2017, 18, e267–e273. [Google Scholar] [CrossRef]
- Wu, A.W. Medical Error: The Second Victim: The Doctor Who Makes the Mistake Needs Help Too. BMJ 2000, 320, 726–727. [Google Scholar] [CrossRef] [PubMed]
- Robertson, J.J.; Long, B. Suffering in Silence: Medical Error and Its Impact on Health Care Providers. J. Emerg. Med. 2018, 54, 402–409. [Google Scholar] [CrossRef] [PubMed]
- Rassin, M.; Kanti, T.; Silner, D. Chronology of Medication Errors by Nurses: Accumulation of Stresses and PTSD Symptoms. Issues Ment. Health Nurs. 2005, 26, 873–886. [Google Scholar] [CrossRef] [PubMed]
- Bian, W.; Cheng, J.; Dong, Y.; Xue, Y.; Zhang, Q.; Zheng, Q.; Song, R.; Yang, H. Experience of Pediatric Nurses in Nursing Dying Children—A Qualitative Study. BMC Nurs. 2023, 22, 126. [Google Scholar] [CrossRef] [PubMed]
- Groves, K.A.; Adewumi, A.; Gerhardt, C.A.; Skeens, M.A.; Suttle, M.L. Grief in Critical Care Nurses after Pediatric Suffering and Death. Ann. Palliat. Med. 2022, 11, 1888–1899. [Google Scholar] [CrossRef] [PubMed]
- Chenevert, M.; Vignoli, M.; Conway, P.M.; Balducci, C. Workplace Bullying and Post-Traumatic Stress Disorder Symptomology: The Influence of Role Conflict and the Moderating Effects of Neuroticism and Managerial Competencies. Int. J. Environ. Res. Public Health 2022, 19, 10646. [Google Scholar] [CrossRef]
- Van den Brande, W.; Baillien, E.; De Witte, H.; Vander Elst, T.; Godderis, L. The Role of Work Stressors, Coping Strategies and Coping Resources in the Process of Workplace Bullying: A Systematic Review and Development of a Comprehensive Model. Aggress. Violent Behav. 2016, 29, 61–71. [Google Scholar] [CrossRef]
- Nadal, K.L. Microaggressions and Traumatic Stress: Theory, Research, and Clinical Treatment; American Psychological Association: Washington, DC, USA, 2018; p. xiv, 150. [Google Scholar] [CrossRef]
- Gemzøe Mikkelsen, E.; Einarsen, S. Relationships between Exposure to Bullying at Work and Psychological and Psychosomatic Health Complaints: The Role of State Negative Affectivity and Generalized Self–Efficacy. Scand. J. Psychol. 2002, 43, 397–405. [Google Scholar] [CrossRef]
- Maytum, J.C.; Heiman, M.B.; Garwick, A.W. Compassion Fatigue and Burnout in Nurses Who Work with Children with Chronic Conditions and Their Families. J. Pediatr. Health Care 2004, 18, 171–179. [Google Scholar] [CrossRef]
- Solomon, B.C.; Nikolaev, B.N.; Shepherd, D.A. Does Educational Attainment Promote Job Satisfaction? The Bittersweet Trade-Offs between Job Resources, Demands, and Stress. J. Appl. Psychol. 2022, 107, 1227–1241. [Google Scholar] [CrossRef]
- SHRM Online Staff. Survey: Salary Is Top. Cause of Dissatisfaction for U.S. Employees. SHRM. Available online: https://www.shrm.org/resourcesandtools/hr-topics/compensation/pages/dissatisfaction.aspx (accessed on 18 September 2023).
- Healthcare Workers with PTSD. Available online: https://nursesptsd.com (accessed on 18 September 2023).
- Stimpfel, A.W.; Sloane, D.M.; Aiken, L.H. The Longer the Shifts for Hospital Nurses, the Higher the Levels of Burnout and Patient Dissatisfaction. Health Aff. 2012, 31, 2501–2509. [Google Scholar] [CrossRef]
- Roman, P.; Perez-Cayuela, I.; Gil-Hernández, E.; Rodriguez-Arrastia, M.; Aparicio-Mota, A.; Ropero-Padilla, C.; Rueda-Ruzafa, L. Influence of Shift Work on the Health of Nursing Professionals. J. Personal. Med. 2023, 13, 627. [Google Scholar] [CrossRef]
- Hinderer, K.A.; VonRueden, K.T.; Friedmann, E.; McQuillan, K.A.; Gilmore, R.; Kramer, B.; Murray, M. Burnout, Compassion Fatigue, Compassion Satisfaction, and Secondary Traumatic Stress in Trauma Nurses. J. Trauma Nurs. 2014, 21, 160–169. [Google Scholar] [CrossRef]
- Schuster, B.L. Burnout, Posttraumatic Stress Disorder, or Both–Listen Carefully! Am. J. Med. 2021, 134, 705–706. [Google Scholar] [CrossRef]
- Msaouel, P.; Keramaris, N.C.; Tasoulis, A.; Kolokythas, D.; Syrmos, N.; Pararas, N.; Thireos, E.; Lionis, C. Burnout and Training Satisfaction of Medical Residents in Greece: Will the European Work Time Directive Make a Difference? Human. Resour. Health 2010, 8, 16. [Google Scholar] [CrossRef]
- Skefales, A.; Plakas, S.; Fouka, G.; Goni, M.; Vassiliadou, M.; Bergiannaki, J.-D. Burnout and Its Association with Working Conditions among Greek Hospital Nurses in a Time of Financial Crisis. Open J. Nurs. 2014, 2014. [Google Scholar] [CrossRef]
- Kaitelidou, D.; Konstantakopoulou, O.; Panteli, D.; Vildiridi, L. Testing the Resilience of the Greek Health System Faced by a Human Resources in Health (HRH) Shock Scenario. Eur. J. Public Health 2023, 33 (Suppl. 2), ckad160.391. [Google Scholar] [CrossRef]
- Sapountzi-Krepia, D.; Lavdaniti, M.; Psychogiou, M.; Arsenos, P.; Paralikas, T.; Triantafylidou, P.; Georgiadou, C. Nursing Staff Shortage and In-Hospital Informal Care in an Oncology Hospital in Greece: The Nursing Staff’s Perceptions. Int. J. Nurs. Pract. 2008, 14, 256–263. [Google Scholar] [CrossRef]

{kind=link}
| n | % | ||
|---|---|---|---|
| Gender | Man | 60 | 13.5% |
| Woman | 385 | 86.5% | |
| Specialty | Medical staff | 154 | 34.6% |
| Nursing staff | 291 | 65.4% | |
| Family status | Single | 160 | 36.0% |
| Married/In a relationship | 256 | 57.5% | |
| Divorced | 29 | 6.5% | |
| Education level | Secondary | 23 | 5.1% |
| University | 173 | 38.9% | |
| Master | 123 | 27.6% | |
| Ph.D. | 33 | 7.4% | |
| Specialty/Expertise | 93 | 20.9% | |
| Pediatric department | PICU | 155 | 34.8% |
| Emergencies | 50 | 11.2% | |
| Clinic | 240 | 53.9% | |
| Shift | Morning shift | 142 | 31.9% |
| Circular shift | 303 | 68.1% | |
| n | % | ||
|---|---|---|---|
| Choice to work in the specific department | Yours | 199 | 44.7% |
| Management | 246 | 55.3% | |
| If you were given the opportunity, would you change departments? | Yes | 109 | 24.5% |
| No | 336 | 75.5% | |
| Is your salary considered satisfactory in relation to your work and the responsibility it entails? | Yes | 43 | 9.7% |
| No | 402 | 90.3% | |
| Yes | No | |||
|---|---|---|---|---|
| n | % | n | % | |
| Nursing or medical error | 324 | 72.8% | 121 | 27.2% |
| Death or threat to the life of a child | 249 | 56.0% | 196 | 44.0% |
| Bullying | 247 | 55.5% | 198 | 44.5% |
| M | SD | |
|---|---|---|
| Re-experiencing the traumatic event (criterion B) | ||
| Are unwanted memories of the traumatic event recurring in a way that causes you to worry? | 0.9 | 1.1 |
| Are disturbing dreams related to the traumatic event recurring? | 0.8 | 1.0 |
| Do you feel and act as if the traumatic event is happening again and reliving it? | 0.8 | 1.0 |
| Do you get upset and agitated when something reminds you of a traumatic event of the past? | 1.2 | 1.1 |
| Do you feel like you have strange physical reactions, like a racing heart and sweating, every time you think about the traumatic event you experienced? | 1.0 | 1.1 |
| Avoidance of situations reminiscent of the traumatic experience (criterion C) | ||
| Do you avoid memories, thoughts, or feelings related to the specific traumatic event? | 1.3 | 1.3 |
| Do you avoid situations or activities that trigger memories and remind you of the traumatic event? | 1.1 | 1.2 |
| Negative feelings about the critical event (criterion D) | ||
| Do you have trouble remembering important elements of the traumatic event you experienced? | 0.7 | 0.9 |
| Do you have a negative belief about yourself, other people, and events happening in the world? (e.g., do you feel like everything is your fault, that you cannot trust anyone, or that the world is dangerous?) | 1.1 | 1.1 |
| Do you blame yourself or someone else for the traumatic experience, or what followed? | 0.8 | 1.1 |
| Do you feel strong negative emotions such as fear, terror, anger, guilt, or shame about the traumatic event you experienced? | 0.9 | 1.1 |
| Have you lost interest in activities you used to do in the past? | 1.1 | 1.1 |
| Do you feel distant or isolated from the people around you? | 0.9 | 1.1 |
| Do you feel emotionally apathetic or have difficulty expressing feelings of love to those close to you? | 0.8 | 1.0 |
| Increased arousal and reactivity (Criterion E) | ||
| Do you feel like you have irritability, outbursts of anger, or intense aggression? | 1.2 | 1.1 |
| Do you expose yourself to many risks or do things that can harm you? | 1.0 | 1.1 |
| Were you hypervigilant or alert (e.g., check to see who is around you, etc.)? | 0.8 | 1.4 |
| Do you feel startled or startled easily? | 1.0 | 1.1 |
| Do you find it difficult to concentrate on something? | 1.2 | 1.5 |
| Do you have trouble falling asleep or staying asleep? | 1.3 | 1.8 |
| M | SD | Min | Max | % | |
|---|---|---|---|---|---|
| PTSD | 19.73 | 15.03 | 0.0 | 64.0 | 25.2% |
| Criterion B | 4.76 | 4.48 | 0.0 | 19.0 | 48.5% |
| Criterion C | 2.45 | 2.39 | 0.0 | 8.0 | 44.3% |
| Criterion D | 6.16 | 5.58 | 0.0 | 25.0 | 41.6% |
| Criterion E | 6.37 | 5.09 | 0.0 | 20.0 | 44.5% |
| Diagnosis | χ2 | p | |||||
|---|---|---|---|---|---|---|---|
| No PTSD | PTSD | ||||||
| n | % | n | % | ||||
| Gender | Man | 44 | 73.3% | 16 | 26.7% | 0.083 | 0.774 |
| Woman | 289 | 75.1% | 96 | 24.9% | |||
| Specialty | Medical staff | 113 | 73.4% | 41 | 26.6% | 0.265 | 0.607 |
| Nursing staff | 220 | 75.6% | 71 | 24.4% | |||
| Education level | Secondary | 22 | 95.7% | 1 | 4.3% | 10.659 | 0.014 |
| University | 120 | 69.4% | 53 | 30.6% | |||
| Master/PhD | 118 | 75.6% | 38 | 24.4% | |||
| Specialty/Expertise | 73 | 78.5% | 20 | 21.5% | |||
| Shift | Morning | 115 | 81.0% | 27 | 19.0% | 4.343 | 0.037 |
| Circular | 218 | 71.9% | 85 | 28.1% | |||
| Department choice | Worker | 158 | 79.4% | 41 | 20.6% | 4.030 | 0.045 |
| Management | 175 | 71.1% | 71 | 28.9% | |||
| Intention to change department | Yes | 74 | 67.9% | 35 | 32.1% | 3.566 | 0.059 |
| No | 259 | 77.1% | 77 | 22.9% | |||
| Satisfaction with the salary | Yes | 40 | 93.0% | 3 | 7.0% | 10.506 | 0.001 |
| No | 293 | 72.9% | 109 | 27.1% | |||
| Pediatric department | PICU | 116 | 74.8% | 39 | 25.2% | 0.858 | 0.651 |
| Emergencies | 40 | 80.0% | 10 | 20.0% | |||
| Clinic | 177 | 73.8% | 63 | 26.3% | |||
| Area | Region | 142 | 76.8% | 43 | 23.2% | 0.627 | 0.429 |
| Athens | 191 | 73.5% | 69 | 26.5% | |||
| B | Typical Error | d.f. | p | Exp(B) | 95% CI | ||
|---|---|---|---|---|---|---|---|
| Lower | Upper | ||||||
| Shift | 0.507 | 0.249 | 1 | 0.042 | 1.661 | 1.019 | 2.706 |
| University | 2.274 | 1.036 | 1 | 0.028 | 9.717 | 1.276 | 73.977 |
| Master/PhD | 1.958 | 1.039 | 1 | 0.060 | 7.085 | 0.924 | 54.327 |
| Specialty/Expertise | 1.796 | 1.053 | 1 | 0.088 | 6.027 | 0.765 | 47.488 |
| Choice of department | 0.447 | 0.225 | 1 | 0.047 | 1.563 | 1.006 | 2.429 |
| Satisfaction with the salary | 1.601 | 0.609 | 1 | 0.009 | 4.960 | 1.503 | 16.365 |
| Diagnosis | χ2 | p | |||||
|---|---|---|---|---|---|---|---|
| No PTSD | PTSD | ||||||
| n | % | n | % | ||||
| Medical or nursing error | Yes | 227 | 70.1% | 97 | 29.9% | 15.928 | 0.000 |
| No | 106 | 87.6% | 15 | 12.4% | |||
| Death or threat to the life of a child | Yes | 175 | 70.3% | 74 | 29.7% | 6.320 | 0.012 |
| No | 158 | 80.6% | 38 | 19.4% | |||
| Bullying | Yes | 168 | 68.0% | 79 | 32.0% | 14.084 | 0.000 |
| No | 165 | 83.3% | 33 | 16.7% | |||
| B | Typical Error | d.f. | p | Exp(B) | 95% CI | ||
|---|---|---|---|---|---|---|---|
| Lower | Upper | ||||||
| Medical or nursing error | 1.105 | 0.301 | 1 | <0.001 | 3.020 | 1.673 | 5.451 |
| Death or threat to the life of a child | 0.564 | 0.228 | 1 | 0.013 | 1.758 | 1.125 | 2.747 |
| Bulling | 0.855 | 0.234 | 1 | <0.001 | 2.351 | 1.485 | 3.723 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Rigas, N.; Kyritsis, Z.; Dagla, M.; Soldatou, A.; Orovou, E.; Tzitiridou-Chatzopoulou, M.; Eskitzis, P.; Antoniou, E. Post-Traumatic Stress Disorder Symptoms among Pediatric Healthcare Workers. Nurs. Rep. 2024, 14, 115-127. https://doi.org/10.3390/nursrep14010010
Rigas N, Kyritsis Z, Dagla M, Soldatou A, Orovou E, Tzitiridou-Chatzopoulou M, Eskitzis P, Antoniou E. Post-Traumatic Stress Disorder Symptoms among Pediatric Healthcare Workers. Nursing Reports. 2024; 14(1):115-127. https://doi.org/10.3390/nursrep14010010
Chicago/Turabian StyleRigas, Nikolaos, Zacharias Kyritsis, Maria Dagla, Alexandra Soldatou, Eirini Orovou, Maria Tzitiridou-Chatzopoulou, Panagiotis Eskitzis, and Evangelia Antoniou. 2024. "Post-Traumatic Stress Disorder Symptoms among Pediatric Healthcare Workers" Nursing Reports 14, no. 1: 115-127. https://doi.org/10.3390/nursrep14010010
APA StyleRigas, N., Kyritsis, Z., Dagla, M., Soldatou, A., Orovou, E., Tzitiridou-Chatzopoulou, M., Eskitzis, P., & Antoniou, E. (2024). Post-Traumatic Stress Disorder Symptoms among Pediatric Healthcare Workers. Nursing Reports, 14(1), 115-127. https://doi.org/10.3390/nursrep14010010