
Psychometric Properties of the Self-Compassion Scale—Short Form: Study of Its Role as a Protector of Spanish Nurses Professional Quality of Life and Well-Being during the COVID-19 Pandemic



Abstract
:1. Introduction
2. Materials and Methods
2.1. Study Design
2.2. Setting and Participants
2.3. Measures
2.4. Data Analysis
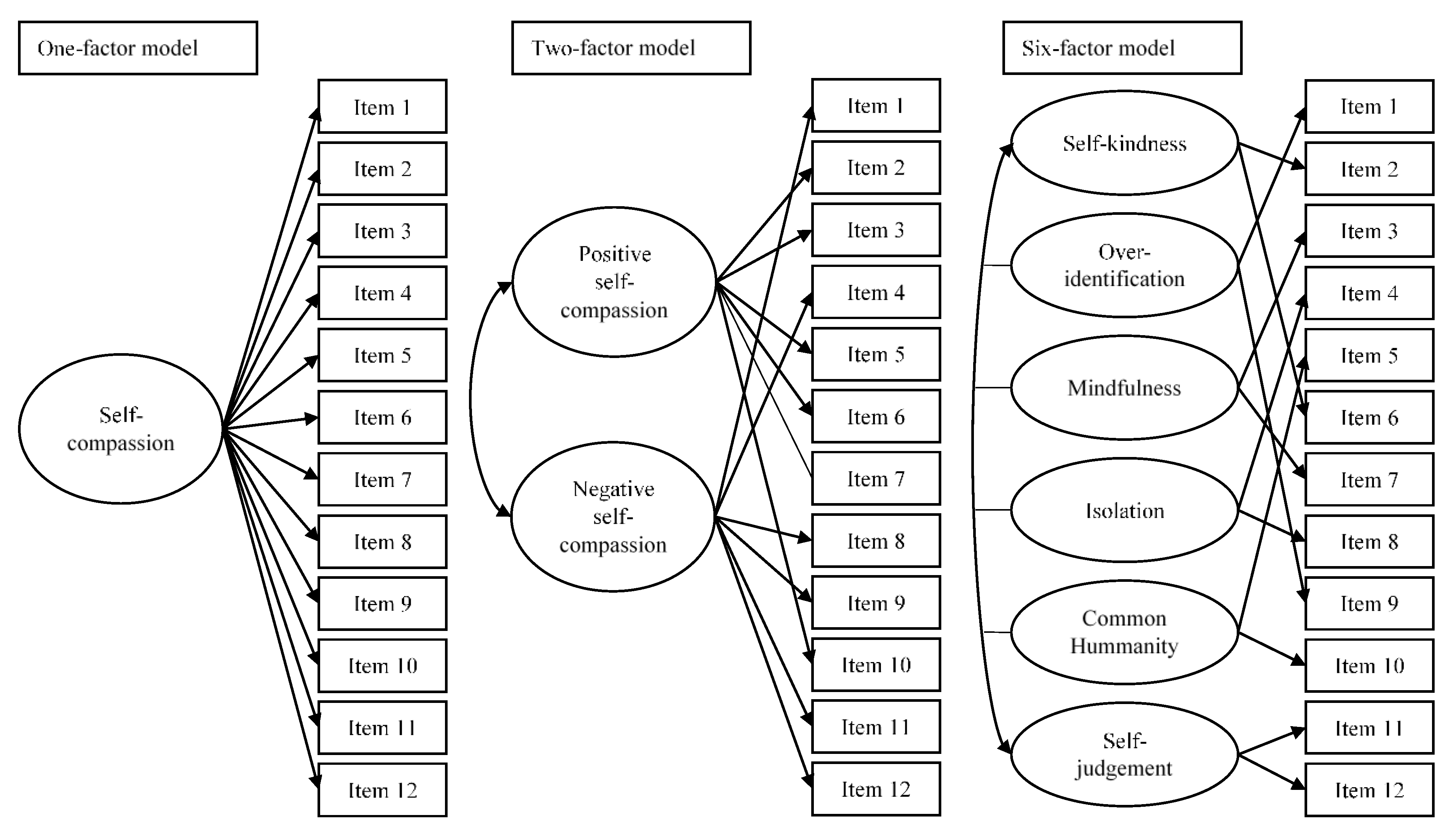
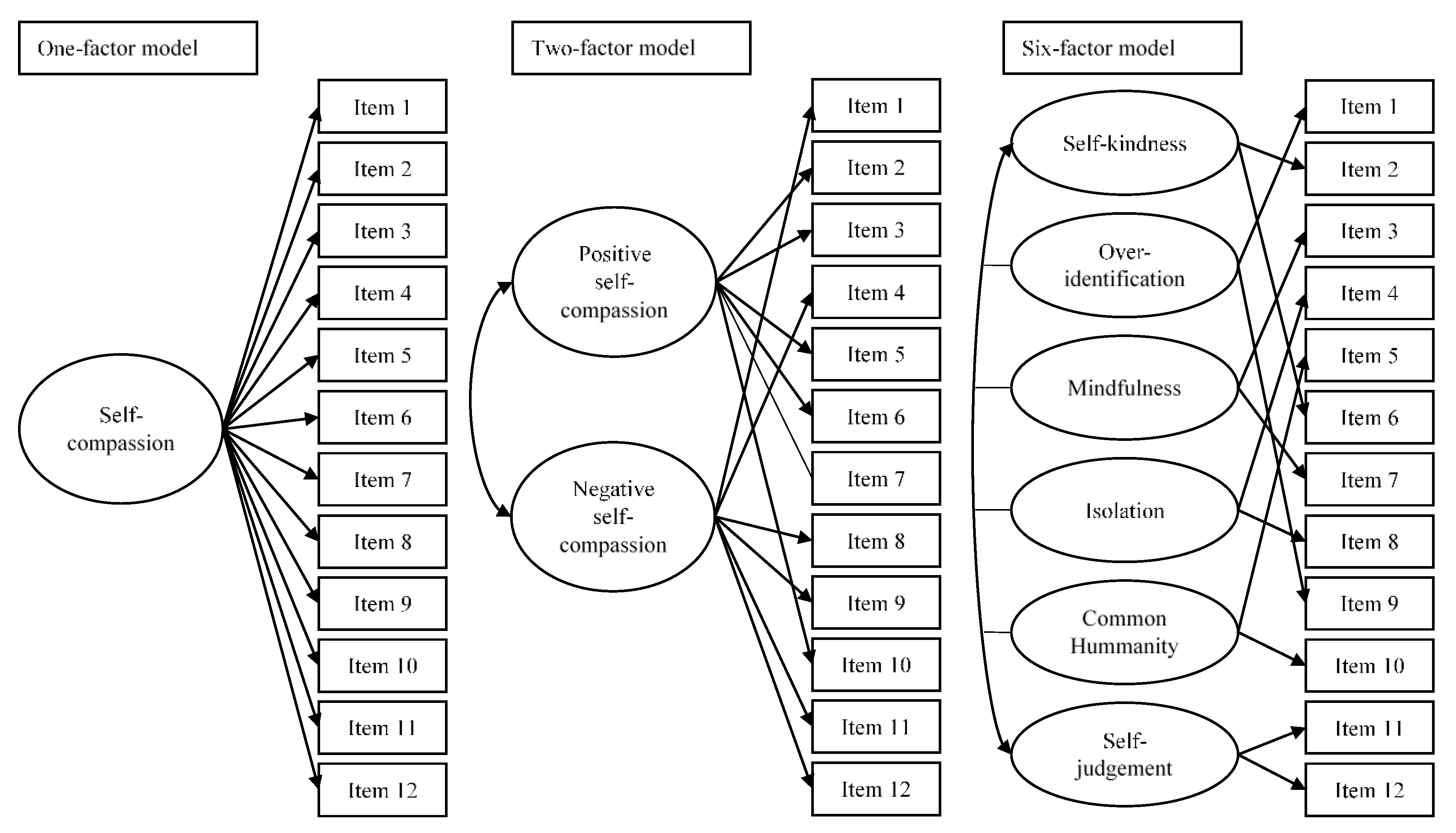
- One-factor model. This model is based on evidence provided by Deniz et al. [6], who tested a general factor of self-compassion that explained the 12 items of the SCS-SF, offering evidence that supported the unidimensional structure;
- Six-factor model. This model is based on the original results of Raes et al. [5], García-Campayo et al. [16], and Alabdulaziz et al. [18] and hypothesized six correlated factors, including self-kindness, common humanity, and mindfulness, which would represent compassionate behaviors, together with self-judgement, isolation, and over-identification, representing their opposite poles.
3. Results
4. Discussion
Limitations
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Neff, K.D. Self-compassion: An alternative conceptualization of a healthy attitude toward oneself. Self Identity 2003, 2, 85–101. [Google Scholar] [CrossRef] [Green Version]
- Neff, K.D. The development and validation of a scale to measure selfcompassion. Self Identity 2003, 2, 223–250. [Google Scholar] [CrossRef]
- Neff, K.D. The self-compassion scale is a valid and theoretically coherent measure of self-compassion. Mindfulness 2016, 7, 264–274. [Google Scholar] [CrossRef]
- Neff, K.D.; Dahm, K.A. Self-compassion: What it is, what it does, and how it relates to mindfulness. In Handbook of Mindfulness and Self-Regulation; Ostafin, B.D., Robinson, M.D., Meier, B.P., Eds.; Springer: New York, NY, USA, 2015; pp. 121–137. [Google Scholar]
- Raes, F.; Pommier, E.; Neff, K.D.; Van Gucht, D. Construction and factorial validation of a short form of the Self-Compassion Scale. Clin. Psychol. Psychother. 2011, 18, 250–255. [Google Scholar] [CrossRef]
- Deniz, M.; Kesici, Ş.; Sümer, A.S. The validity and reliability of the Turkish version of the self-compassion scale. Soc. Behav. Pers. 2008, 36, 1151–1160. [Google Scholar] [CrossRef]
- López, A.; Sanderman, R.; Smink, A.; Zhang, Y.; van Sonderen, E.; Ranchor, A.; Schroevers, M.J. A reconsideration of the selfcompassion scale’s total score: Self-compassion versus self-criticism. PLoS ONE 2015, 10, e0132940. [Google Scholar] [CrossRef] [Green Version]
- Costa, J.; Marôco, J.; Pinto-Gouveia, J.; Ferreira, C.; Castilho, P. Validation of the psychometric properties of the self-compassion scale. Testing the factorial validity and factorial invariance of the measure among borderline personality disorder, anxiety disorder, eating disorder and general populations. Clin. Psychol. Psychother. 2016, 23, 460–468. [Google Scholar] [CrossRef]
- Singer, T.; Bolz, M. Compassion: Bridging Practice and Science; Max Planck Institute for Human Cognitive and Brain Sciences: Leipzig, Germany, 2013. [Google Scholar]
- Mills, J.; Wand, T.; Fraser, J.A. On self-compassion and self-care in nursing: Selfish or essential for compassionate care? Int. J. Nurs. Stud. 2015, 52, 791–793. [Google Scholar] [CrossRef]
- Raab, K. Mindfulness, self-compassion, and empathy among health care professionals: A review of the literature. J. Health Care Chaplain 2014, 20, 95–108. [Google Scholar] [CrossRef]
- Gustin, L.; Wagner, L. The butterfly effect of caring—Clinical nursing teachers’ understanding of self-compassion as a source to compassionate care. Scand. J. Caring Sci. 2013, 27, 175–183. [Google Scholar] [CrossRef]
- Durkin, M.; Beaumont, E.; Hollins Martin, C.J.; Carson, J. A pilot study exploring the relationship between self-compassion, self-judgement, self-kindness, compassion, professional quality of life and wellbeing among UK community nurses. Nurse Educ. Today 2016, 46, 109–114. [Google Scholar] [CrossRef]
- Sansó, N.; Galiana, L.; González, B.; Sarmentero, J.; Reynes, M.; Oliver, A.; Garcia-Toro, M. Differential effects of two contemplative practice-based programs for health care professionals. Interv. Psicosoc. 2019, 28, 131–138. [Google Scholar] [CrossRef] [Green Version]
- Duarte, J.; Pinto-Gouveia, J.; Cruz, B. Relationships between nurses’ empathy, self-compassion and dimensions of professional quality of life: A cross-sectional study. Int. J. Nurs. Stud. 2016, 60, 1–11. [Google Scholar] [CrossRef] [Green Version]
- Garcia-Campayo, J.; Navarro-Gil, M.; Andrés, E.; Montero-Marin, J.; López-Artal, L.; Demarzo, M.M.P. Validation of the Spanish versions of the long (26 items) and short (12 items) forms of the Self-Compassion Scale (SCS). Health Qual. Life Outcomes 2014, 12, 1–9. [Google Scholar] [CrossRef] [Green Version]
- Meng, R.; Yu, Y.; Chai, S.; Luo, X.; Gong, B.; Liu, B.; Hu, Y.; Luo, Y.; Yu, C. Examining psychometric properties and measurement invariance of a Chinese version of the Self-Compassion Scale—Short Form (SCS-SF) in nursing students and medical workers. Psychol. Res. Behav. Manage. 2019, 12, 793–809. [Google Scholar] [CrossRef] [Green Version]
- Alabdulaziz, H.; Alquwez, N.; Almazan, J.U.; Albougami, A.; Alshammari, F.; Cruz, J.P. The Self-Compassion Scale Arabic version for baccalaureate nursing students: A validation study. Nurse Educ. Today 2020, 89, 104420. [Google Scholar] [CrossRef]
- Von Elm, E.; Altman, D.G.; Egger, M.; Pocock, S.J.; Gøtzsche, P.C.; Vandenbroucke, J.P. STROBE Initiative. The Strengthening the Reporting of Observational Studies in Epidemiology (STROBE) statement: Guidelines for reporting observational studies. J. Clin. Epidemiol. 2008, 61, 344–349. [Google Scholar] [CrossRef] [Green Version]
- Instituto Nacional de Estadística. Estadística de Profesionales Sanitarios Colegiados. Últimos Datos. 2021. Available online: https://www.ine.es/dyngs/INEbase/es/operacion.htm?c=Estadistica_C&cid=1254736176781&menu=ultiDatos&idp=1254735573175 (accessed on 1 February 2022).
- Galiana, L.; Oliver, A.; Arena, F.; De Simone, G.; Tomás, J.M.; Vidal-Blanco, G.; Muñoz-Martínez, I.; Sansó, N. Development and validation of the Short Professional Quality of Life Scale based on versions IV and V of the Professional Quality of Life Scale. Health Qual. Life Outcomes 2020, 18, 364. [Google Scholar] [CrossRef]
- Stamm, B.H. The Concise ProQOL Manual. 2010. Available online: https://proqol.org/uploads/ProQOLManual.pdf (accessed on 25 November 2020).
- Galiana, L.; Vidal-Blanco, G.; Oliver, A.; Sansó, N. Interpretación de las puntuaciones obtenidas con la Escala Breve de Calidad de Vida Profesional. Med. Pal. 2021. (accepted). [Google Scholar] [CrossRef]
- Pérez-Belmonte, S.; Galiana, L.; Fernández, I.; Vidal-Blanco, G.; Sansó, N. The Personal Wellbeing Index in Spanish Palliative Care Professionals: A Cross-Sectional Study of Wellbeing. Front. Psychol. 2021, 12, 672792. [Google Scholar] [CrossRef]
- Muthén, L.K.; Muthén, B.O. Mplus User’s Guide, 8th ed.; Muthén & Muthén: Los Angeles, CA, USA, 2017. [Google Scholar]
- Kline, R.B. Principles and Practice of Structural Equation Modeling; Guilford Press: New York, NY, USA, 2015. [Google Scholar]
- Hu, L.T.; Bentler, P.M. Cutoff criteria for fit indexes in covariance structure analysis: Conventional criteria versus new alternatives. Struct. Equ. Model. 1999, 6, 1–55. [Google Scholar] [CrossRef]
- Cheung, G.W.; Rensvold, R.B. Evaluating goodness-of-fit indexes for testing measurement invariance. Struct. Equ. Model. 2002, 9, 233–255. [Google Scholar] [CrossRef]
- Little, T.D. Mean and covariance structures (MACS) analyses of cross-cultural data: Practical and theoretical issues. Multivar. Behav. Res. 1997, 32, 53–76. [Google Scholar] [CrossRef]
- Kenny, D.A.; Kaniskan, B.; McCoach, D.B. The performance of RMSEA in models with small degrees of freedom. Sociol. Methods Res. 2015, 44, 486–507. [Google Scholar] [CrossRef]
- Wood, A.M.; Taylor, P.J.; Joseph, S. Does the CES-D measure a continuum from depression to happiness? Comparing substantive and artifactual models. Psychiatry Res. 2010, 177, 120–123. [Google Scholar] [CrossRef]
- Van Dam, N.T.; Hobkirk, A.L.; Danoff-Burg, S.; Earleywine, M. Mind your words: Positive and negative items create method effects on the Five Facet Mindfulness Questionnaire. Assessment 2012, 19, 123–130. [Google Scholar] [CrossRef] [Green Version]
- Tomás, J.M.; Oliver, A.; Galiana, L.; Sancho, P.; Lila, M. Explaining method effects associated with negatively worded items in trait and state global and domain-specific self-esteem scales. Struct. Equ. Model. 2013, 20, 299–313. [Google Scholar] [CrossRef]
- Galiana, L.; Gutiérrez, M.; Tomás, J.M.; Sancho, P. Validation of the Balanced Measure of Psychological Needs (BMPN) in Spanish and Portuguese: Method effects associated to negatively worded items. Psicol. Conductual. 2016, 24, 73–91. [Google Scholar]
- Neff, K.D.; Toth-Kiraly, I.; Colosimo, K. Self-compassion is best measured as a global construct and is overlapping with but distinct from neuroticism: A response to Pfattheicher, Geiger, Hartung, Weiss, and Schindler (2017). Eur. J. Pers. 2018, 32, 371–392. [Google Scholar] [CrossRef]
- Cicchetti, D.V. Guidelines, criteria, and rules of thumb for evaluating normed and standardized assessment instruments in psychology. Psychol. Assess. 1994, 6, 284–290. [Google Scholar] [CrossRef]
- Yarnell, L.M.; Stafford, R.E.; Neff, K.D.; Reilly, E.D.; Knox, M.C.; Mullarkey, M. Meta-analysis of gender differences in self-compassion. Self Identity 2015, 14, 499–520. [Google Scholar] [CrossRef]
- Souza, L.K.d.; Hutz, C.S. Self-compassion in relation to self-esteem, self-efficacy and demographical aspects. Paidéia 2016, 26, 181–188. [Google Scholar] [CrossRef] [Green Version]
- Sansó, N.; Galiana, L.; Oliver, A.; Tomás-Salvá, M.; Vidal-Blanco, G. Predicting Professional Quality of Life and Life Satisfaction in Spanish Nurses: A Cross-Sectional Study. Int. J. Environ. Res. Public Health 2020, 17, 4366. [Google Scholar] [CrossRef]
- Pfefferbaum, B.; North, C.S. Mental Health and the Covid-19 Pandemic. N. Engl. J. Med. 2020, 383, 510–512. [Google Scholar] [CrossRef]
- Shanafelt, T.; Ripp, J.; Trockel, M. Understanding and Addressing Sources of Anxiety Among Health Care Professionals During the COVID-19 Pandemic. JAMA 2020, 323, 2133–2134. [Google Scholar] [CrossRef]
- Liu, C.Y.; Yang, Y.Z.; Zhang, X.M.; Xu, X.; Dou, Q.L.; Zhang, W.W.; Cheng, A.S.K. The prevalence and influencing factors in anxiety in medical workers fighting COVID-19 in China: A cross-sectional survey. Epidemiol. Infect. 2020, 148, e98. [Google Scholar] [CrossRef]
- Rajkumar, R.P. COVID-19 and mental health: A review of the existing literature. Asian J. Psychiatr. 2020, 52, 102066. [Google Scholar] [CrossRef]
- Galli, F.; Pozzi, G.; Ruggiero, F.; Mameli, F.; Cavicchioli, M.; Barbieri, S.; Canevini, M.P.; Priori, A.; Pravettoni, G.; Sani, G.; et al. A Systematic Review and Provisional Metanalysis on Psychopathologic Burden on Health Care Workers of Coronavirus Outbreaks. Front. Psychiatry 2020, 11, 568664. [Google Scholar] [CrossRef]
- Samaniego, A.; Urzúa, A.; Buenahora, M.; Vera-Villarroel, P. Sintomatología asociada a trastornos de salud mental en trabajadores sanitarios en Paraguay: Efecto COVID-19. Interam. J. Psychol. 2020, 54, e1298. [Google Scholar] [CrossRef]
- Blanco-Donoso, L.M.; Moreno-Jiménez, J.; Amutio, A.; Gallego-Alberto, L.; Moreno-Jiménez, B.; Garrosa, E. Stressors, Job Resources, Fear of Contagion, and Secondary Traumatic Stress Among Nursing Home Workers in Face of the COVID-19: The Case of Spain. J. Appl. Gerontol. 2021, 40, 244–256. [Google Scholar] [CrossRef] [PubMed]
- Arpacioglu, S.; Gurler, M.; Cakiroglu, S. Secondary Traumatization Outcomes and Associated Factors Among the Health Care Workers Exposed to the COVID-19. Int. J. Soc. Psychiatry 2021, 67, 84–89. [Google Scholar] [CrossRef] [PubMed]
- Buselli, R.; Corsi, M.; Baldanzi, S.; Chiumiento, M.; Del Lupo, E.; Dell’Oste, V.; Bertelloni, C.A.; Massimetti, G.; Dell’Osso, L.; Cristaudo, A.; et al. Professional Quality of Life and Mental Health Outcomes among Health Care Workers Exposed to Sars-Cov-2 (Covid-19). Int. J. Environ. Res. Public Health 2020, 17, 6180. [Google Scholar] [CrossRef] [PubMed]
- Trumello, C.; Bramanti, S.M.; Ballarotto, G.; Candelori, C.; Cerniglia, L.; Cimino, S.; Crudele, M.; Lombardi, L.; Pignataro, S.; Viceconti, M.L.; et al. Psychological Adjustment of Healthcare Workers in Italy during the COVID-19 Pandemic: Differences in Stress, Anxiety, Depression, Burnout, Secondary Trauma, and Compassion Satisfaction between Frontline and Non-Frontline Professionals. Int. J. Environ. Res. Public Health 2020, 17, 8358. [Google Scholar] [CrossRef] [PubMed]
- Lizano, E.L. Examining the Impact of Job Burnout on the Health and Well-Being of Human Service Workers: A Systematic Review and Synthesis. Hum. Serv. Organ. Manage. Leadersh. Gov. 2015, 39, 167–181. [Google Scholar] [CrossRef] [Green Version]
- Galiana, L.; Sansó, N.; Muñoz-Martínez, I.; Vidal-Blanco, G.; Oliver, A.; Larkin, P.J. Palliative Care Professionals’ Inner Life: Exploring the Mediating Role of Self-Compassion in the Prediction of Compassion Satisfaction, Compassion Fatigue, Burnout and Wellbeing. J. Pain Symptom Manage. 2022, 63, 112–123. [Google Scholar] [CrossRef]

{kind=link}
{kind=link}
{kind=link}
| Variables | Categories | n | % |
|---|---|---|---|
| Sex | Men | 18 | 15.7 |
| Women | 97 | 84.3 | |
| Marital status | Single | 27 | 23.5 |
| Married/living as a couple | 74 | 64.3 | |
| Divorced | 14 | 12.2 | |
| Main activity | Care | 74 | 64.3 |
| Management | 4 | 3.5 | |
| Mixed | 37 | 32.2 |
| Variables | M | SD |
|---|---|---|
| Item 1 | 3.62 | 1.19 |
| Item 2 | 3.40 | 1.02 |
| Item 3 | 3.70 | 1.06 |
| Item 4 | 2.50 | 1.32 |
| Item 5 | 3.48 | 1.08 |
| Item 6 | 2.96 | 1.21 |
| Item 7 | 3.46 | 1.06 |
| Item 8 | 3.05 | 1.19 |
| Item 9 | 2.73 | 1.22 |
| Item 10 | 2.82 | 1.12 |
| Item 11 | 3.11 | 1.23 |
| Item 12 | 2.70 | 1.12 |
| Compassion satisfaction | 13.90 | 1.44 |
| Compassion fatigue | 8.30 | 2.37 |
| Burnout | 7.30 | 2.20 |
| χ2 | df | p | CFI | RMSEA (90% IC) | SRMR | ΔCFI | |
|---|---|---|---|---|---|---|---|
| One-factor model | 261.984 | 54 | <0.001 | 0.803 | 0.185 (0.163, 0.208) | 0.094 | -- |
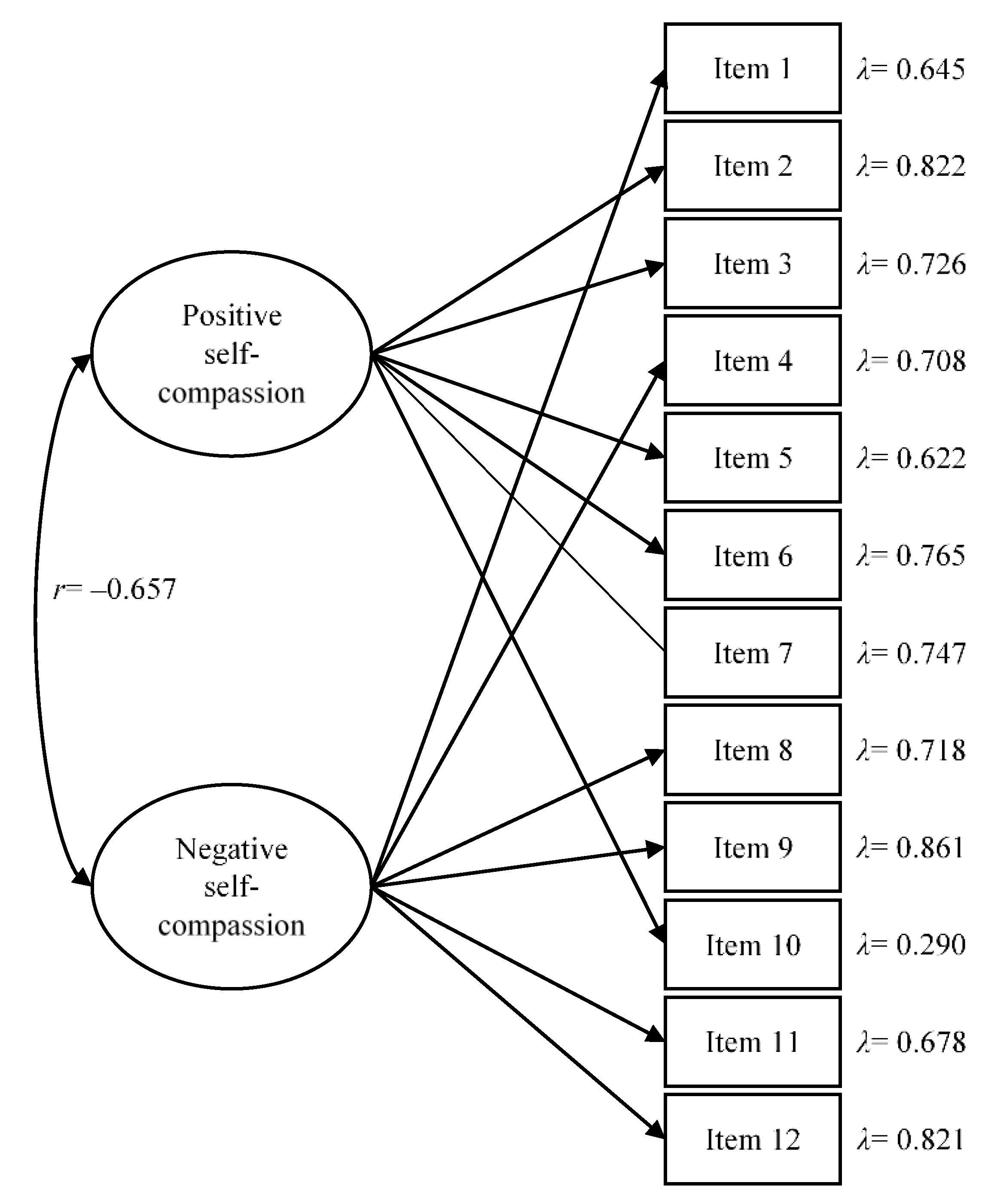
| Two-factor model | 154.819 | 53 | <0.001 | 0.903 | 0.131 (0.107, 0.155) | 0.068 | 0.100 |
| Six-factor model | 113.004 | 39 | <0.001 | 0.930 | 0.130 (0.103, 0.158) | 0.055 | 0.027 |
| Variables | Categories | Positive Self-Compassion | Negative Self-Compassion | ||
|---|---|---|---|---|---|
| M | SD | M | SD | ||
| Total sample | - | 3.30 | 0.78 | 2.96 | 0.91 |
| Sex | Men | 3.11 | 0.99 | 2.86 | 1.04 |
| Women | 3.33 | 0.74 | 2.97 | 0.89 | |
| Marital status | Single | 3.30 | 0.58 | 3.01 | 0.81 |
| Married/living with a couple | 3.34 | 0.79 | 2.88 | 0.96 | |
| Divorced | 3.10 | 1.08 | 3.27 | 0.73 | |
| Main activity | Care | 3.30 | 0.66 | 2.96 | 0.90 |
| Mixed | 3.27 | 0.99 | 2.92 | 0.97 | |
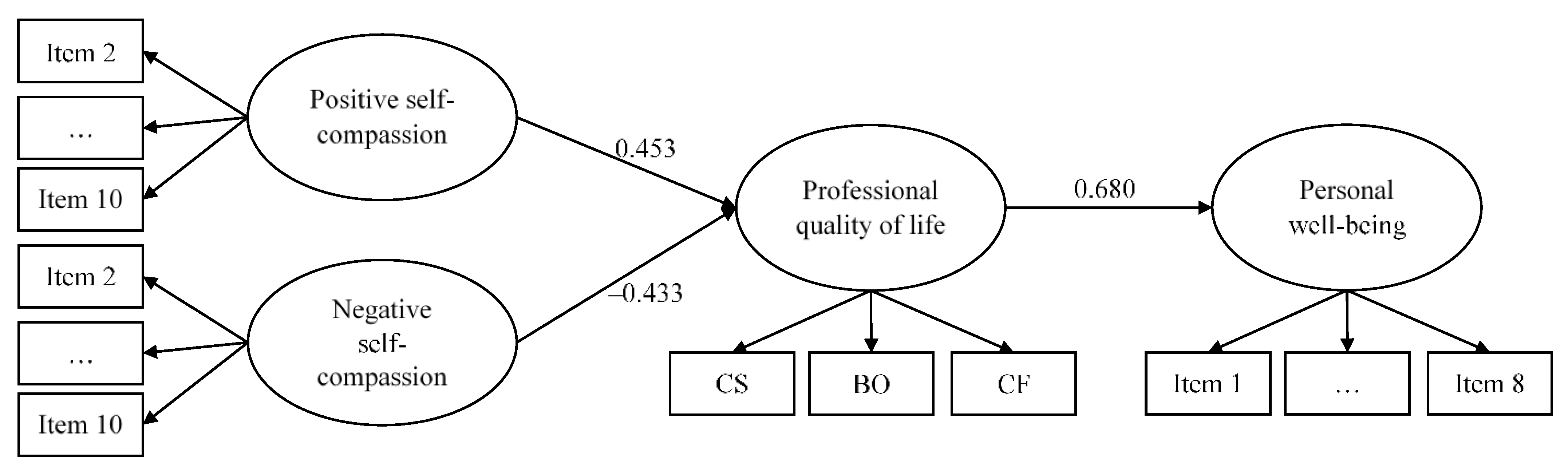
| Positive Self-Compassion | λ | Negative Self-Compassion | λ | Professional Quality of Life | λ | Personal Well-Being | λ |
|---|---|---|---|---|---|---|---|
| Item 2 | 0.810 | Item 1 | 0.608 | CS | 0.478 | Item 1 | 0.782 |
| Item 3 | 0.714 | Item 4 | 0.771 | BO | –0.529 | Item 2 | 0.590 |
| Item 5 | 0.617 | Item 8 | 0.678 | CF | –0.732 | Item 3 | 0.733 |
| Item 6 | 0.791 | Item 9 | 0.857 | Item 4 | 0.657 | ||
| Item 7 | 0.732 | Item 11 | 0.693 | Item 5 | 0.661 | ||
| Item 10 | 0.342 | Item 12 | 0.823 | Item 6 | 0.739 | ||
| Item 7 | 0.676 | ||||||
| Item 8 | 0.407 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Lluch-Sanz, C.; Galiana, L.; Vidal-Blanco, G.; Sansó, N. Psychometric Properties of the Self-Compassion Scale—Short Form: Study of Its Role as a Protector of Spanish Nurses Professional Quality of Life and Well-Being during the COVID-19 Pandemic. Nurs. Rep. 2022, 12, 65-76. https://doi.org/10.3390/nursrep12010008
Lluch-Sanz C, Galiana L, Vidal-Blanco G, Sansó N. Psychometric Properties of the Self-Compassion Scale—Short Form: Study of Its Role as a Protector of Spanish Nurses Professional Quality of Life and Well-Being during the COVID-19 Pandemic. Nursing Reports. 2022; 12(1):65-76. https://doi.org/10.3390/nursrep12010008
Chicago/Turabian StyleLluch-Sanz, Cristina, Laura Galiana, Gabriel Vidal-Blanco, and Noemí Sansó. 2022. "Psychometric Properties of the Self-Compassion Scale—Short Form: Study of Its Role as a Protector of Spanish Nurses Professional Quality of Life and Well-Being during the COVID-19 Pandemic" Nursing Reports 12, no. 1: 65-76. https://doi.org/10.3390/nursrep12010008
APA StyleLluch-Sanz, C., Galiana, L., Vidal-Blanco, G., & Sansó, N. (2022). Psychometric Properties of the Self-Compassion Scale—Short Form: Study of Its Role as a Protector of Spanish Nurses Professional Quality of Life and Well-Being during the COVID-19 Pandemic. Nursing Reports, 12(1), 65-76. https://doi.org/10.3390/nursrep12010008