
Antibody-Drug Conjugates in Solid Tumor Oncology: An Effectiveness Payday with a Targeted Payload

 , ,
, , 
Abstract
:1. Introduction
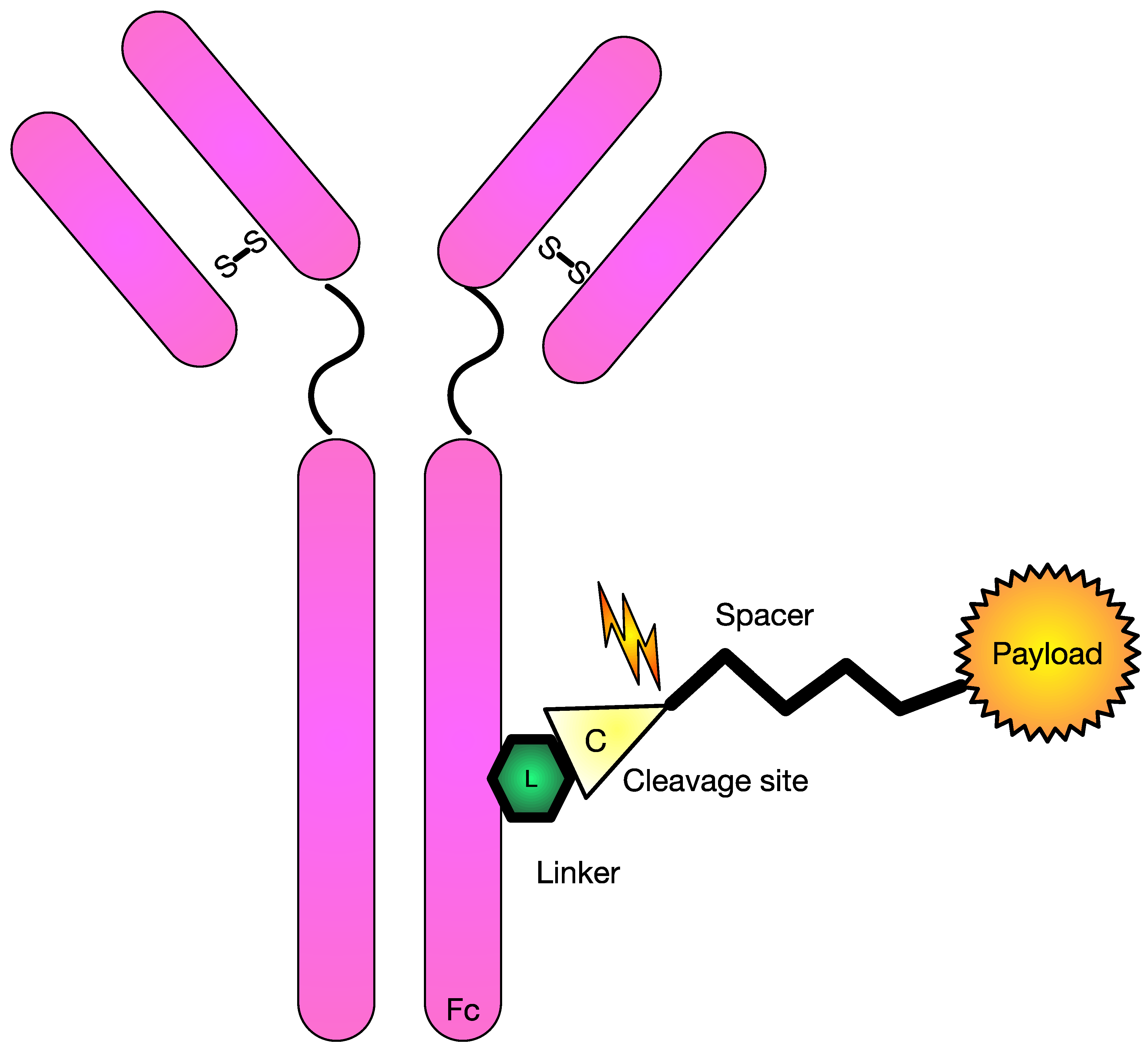
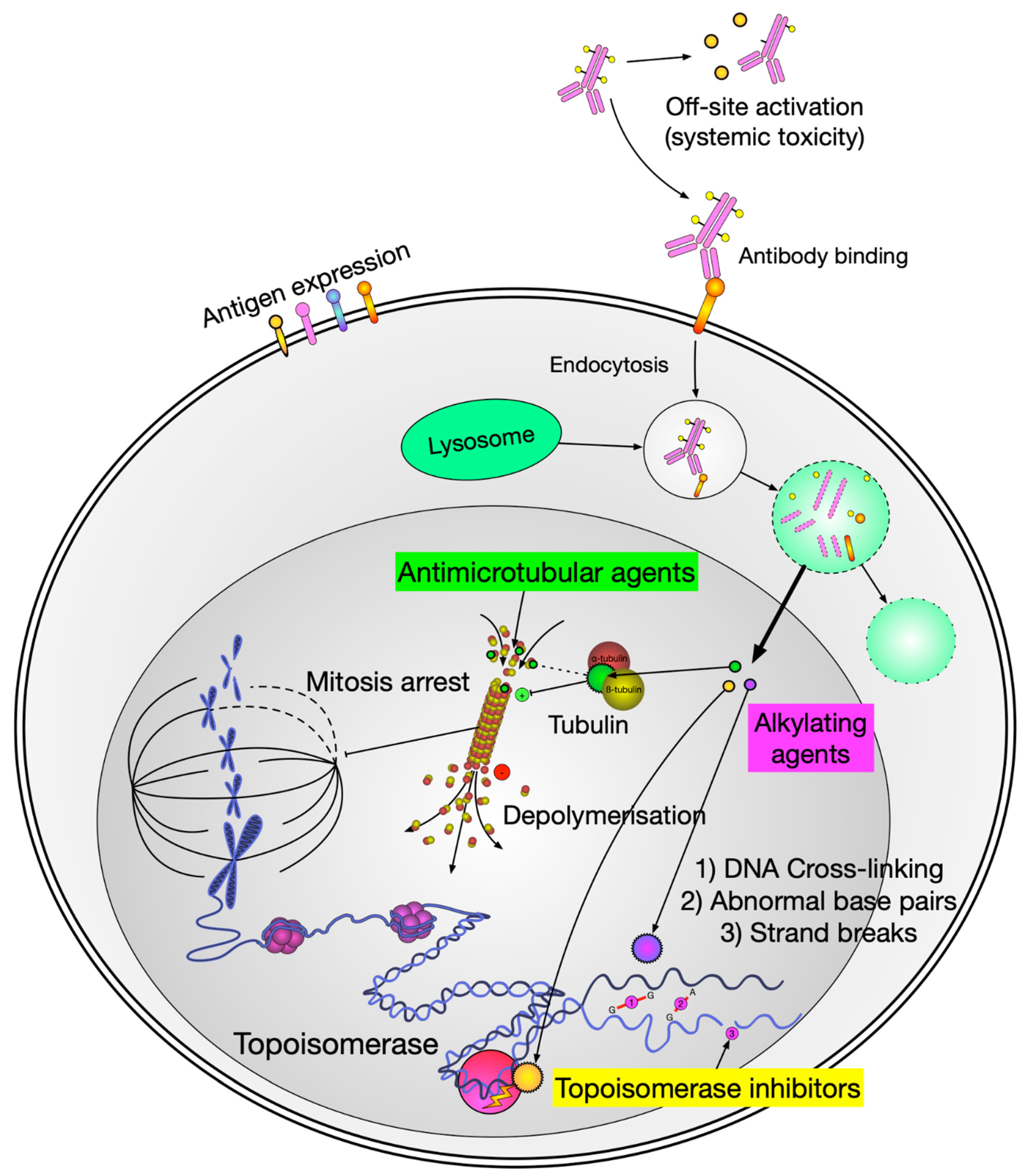
2. General ADC Structure
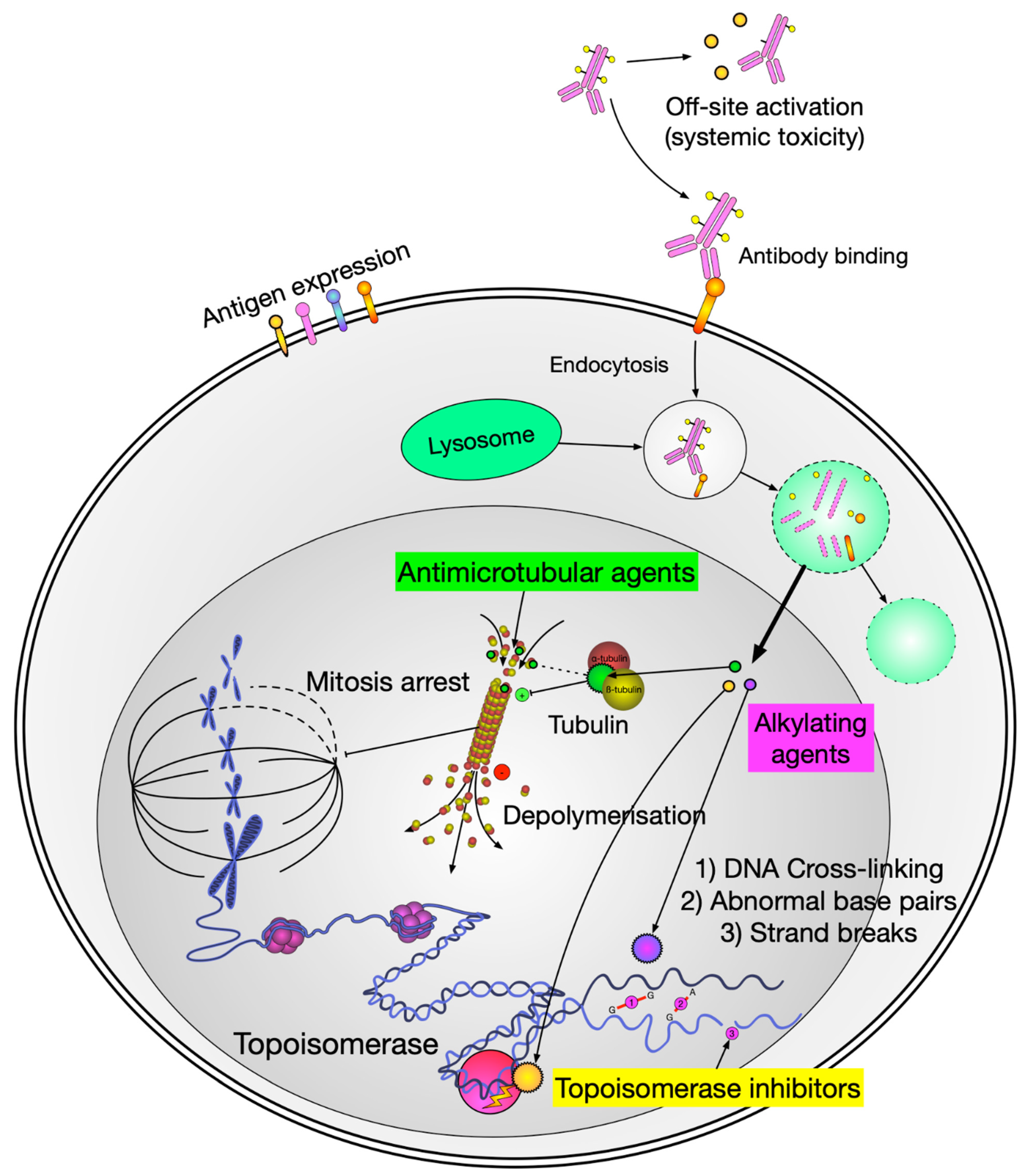
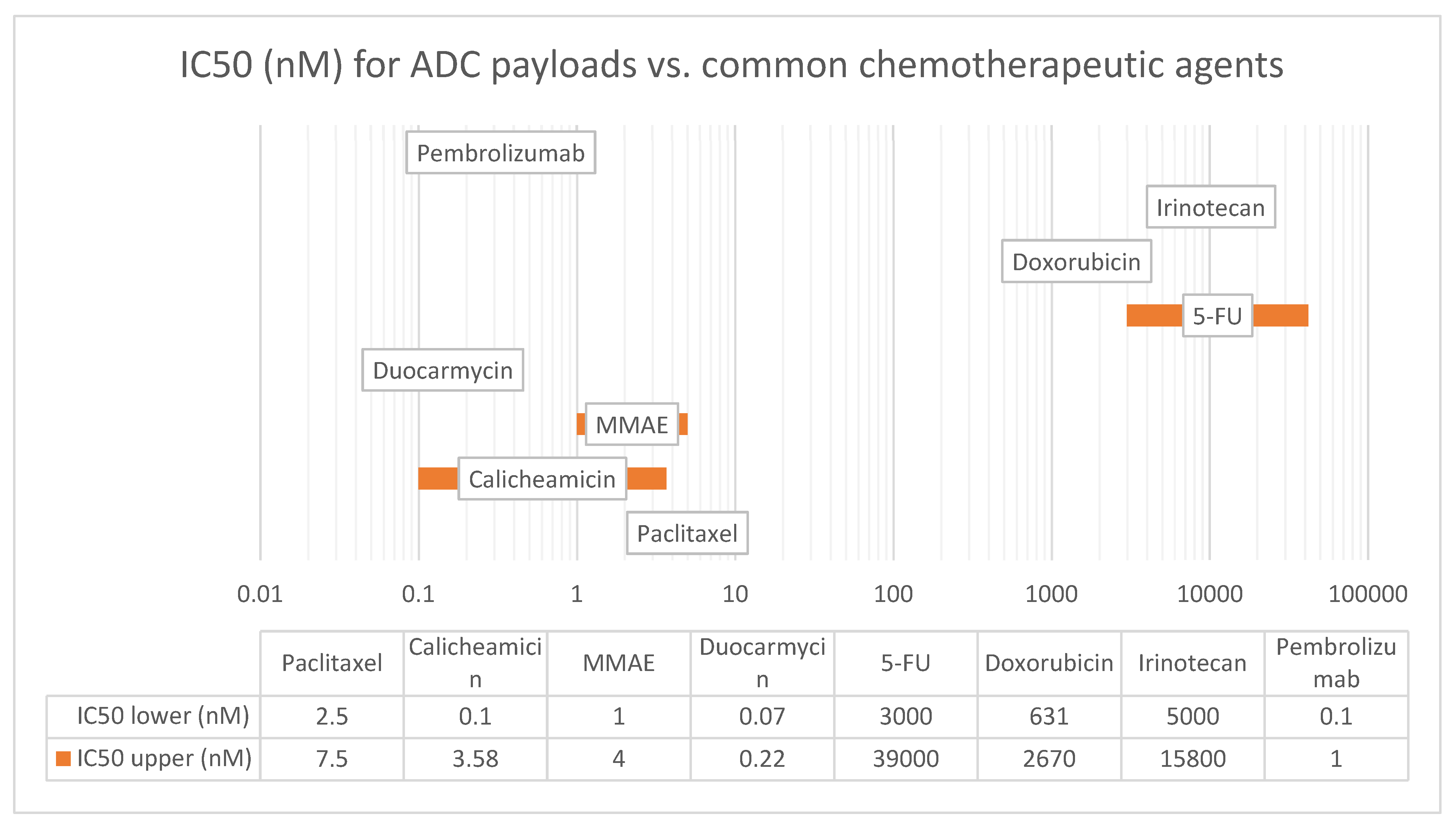
2.1. Payload Types
2.1.1. Auristatins
2.1.2. Maytansinoids (DM1 and DM4)
2.1.3. Calicheamicin
2.1.4. Duocarmycins
2.2. Linkers
2.3. Spacers
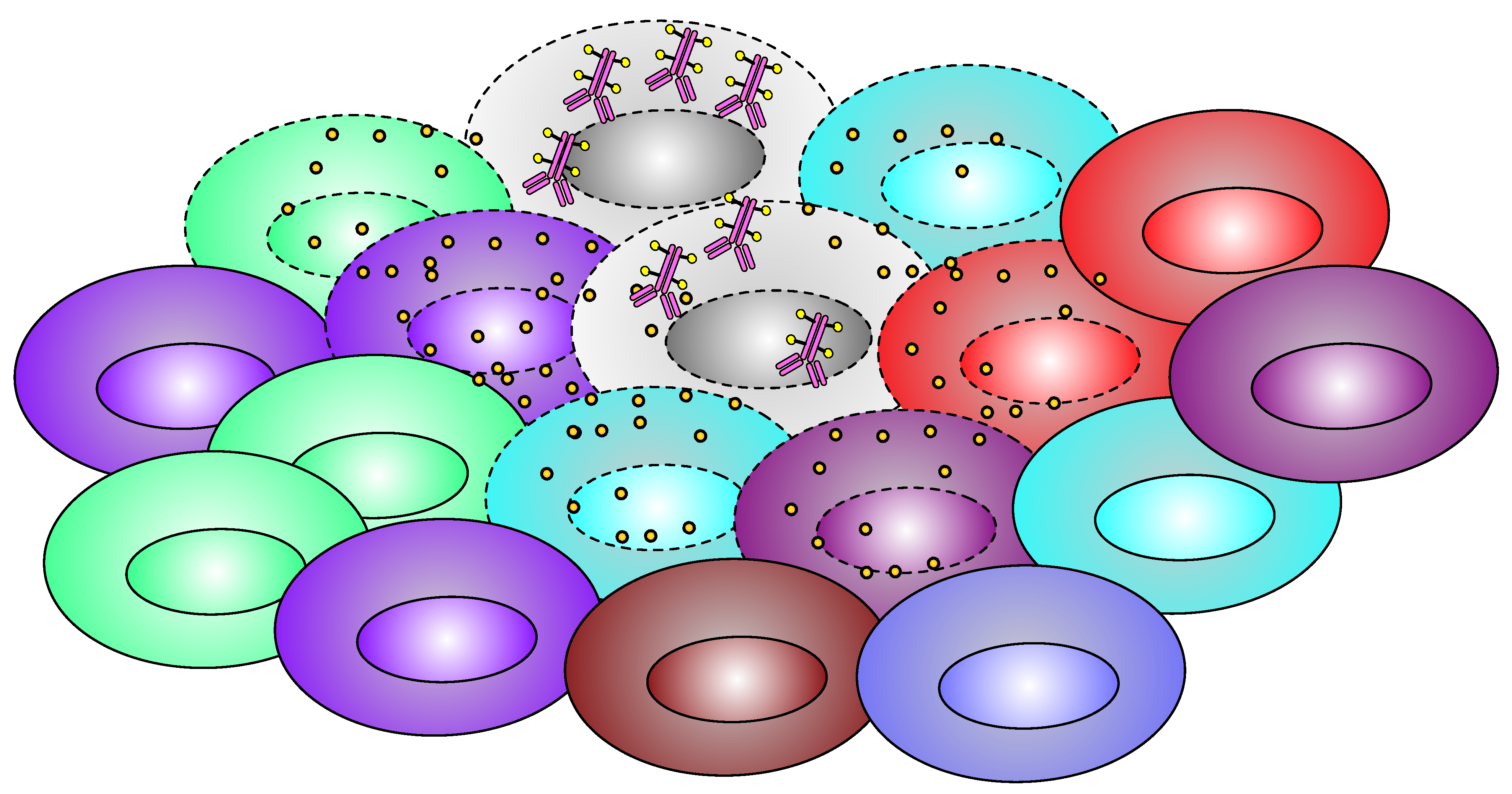
2.4. Bystander Effect
2.4.1. List of Currently FDA-Approved ADC Therapies and Their Clinical Efficacy in Solid Tumors
2.4.2. Ado-Trastuzumab Emtansine (Kadcyla®), or T-DM1
2.4.3. Trastuzumab Deruxtecan (Enhertu®) or T-Dxd
- Breast Cancer
- Gastric Cancer
- Lung Cancer
3. Enfortumab Vedotin (Padcev®)
4. Sacituzuzmab Govitecan (Trodelvy®)
- Triple-negative breast cancer
- Hormone receptor-positive, HER2-negative breast cancer
5. Tisotumab Vedotin (Tivdak®) or TV
6. Mirvetuximab Soravtansine (Elahere™)
6.1. Solid Tumor ADCs in the Pipeline
- RC48-ADC, also known as disitamab vedotin, is a newly developed ADC drug targeting HER2. It is comprised of hertuzumab coupling MMAE via a cleavable linker. It has demonstrated promising anti-tumor activity in pre-clinical and early clinical studies (phase II, single arm, n-43), showing ORR of 51.2% (35.5–66.7%) as a second line treatment of patients with HER2+ locally advanced or metastatic urothelial cancer previously treated platinum-containing chemotherapy. The agent has already been approved for use in China in June 2021 [67,68]. Currently, there are three active phase III clinical trials for RC-48 for its use in HER2-positive breast cancer, HER2-low metastatic breast cancer, and urothelial carcinoma.
- MRG002 is a novel HER2-targeting ADC with potent antitumor activity against HER2-positive solid tumors. It is composed of a modified (hyper-fucosylated) trastuzumab, MMAE payload and a cleavable vc-linker, similar to T-DM1, but with favorable toxicity profile according to preclinical data [69]. A phase I trial in HER-2-positive breast carcinoma showed ORR of 34.7% and DCR of 75.5%, with n-17 PR, 20 SD, and 12 PD [70]. There are 11 ongoing clinical trials for breast, lung, and gastric carcinomas, including two phase III trials: NCT04924699 for HER2-positive unresectable locally advanced or metastatic breast cancer and NCT05754853 for HER-2-positive unresectable or advanced metastatic urothelial cancer.
- ARX788 is an anti-HER2 ADC that utilizes a unique nonnatural amino acid-enabled conjugation technology and a noncleavable drug-linker amberstatin (AS269), a potent tubulin inhibitor. The special drug-linker structure is designed to increase drug serum stability and to decrease off-site activation. In preclinical data on mice, ARX788 showed a half-life of 12.5 days [71]. It received fast track designation from the FDA in early 2021 based on phase I trial (CTR20171162/ACE-Breast-01) data in HER-2 positive breast cancer, with ORR of 19/29 or 66% (45.7–82.1%) [72]. There is currently ongoing phase II trial ACE-Breast03 (NCT04829604). ARX788 is also being studied for advanced gastric and gastrojejunal junction adenocarcinoma patients, with preliminary phase I trial data showing ORR of 45.5% (9/23) [73].
- SYD985, also known as trastuzumab duocarmazine, is another HER2-targeting ADC with a cleavable linker-duocarmycin payload. As mentioned in the payload section, duocarmazine-based ADCs have been extensively studied over the past 50 years, but none of them have been FDA approved in oncology so far. Trastuzumab duocarmazine received FDA fast track designation in 2018 based on early clinical data [74,75]. It is currently undergoing a phase III trial (TULIP/NCT03262935, n-437), where trastuzumab duocarmazine was compared to physician’s choice of treatment in patients with heavily pre-treated HER-2 locally advanced or metastatic breast cancer. Primary outcome analysis results published in 2021 showed a difference in PFS of 7.0 months (5.4–7.2) for SYD985 compared 4.9 months (4.0–5.5) for PC [76].
- XMT-1536 also known as upifitamab rilsodotin (UpRi), is a first-in-class dolaflexin (dolastatin/MMAE family) ADC targeting sodium-dependent phosphate transporter NaPi2b, linked with proprietary DolaLock payload auristatin F-hydroxypropylamide (AF-HPA). F-hydroxyprolylamide was designed to be lipophilic with intracellular metabolic conversion into a less lipophilic metabolite to balance bystander killing and intracellular trapping [77]. NaPi2b is broadly expressed in solid tumors such as serous epithelial ovarian cancer and NCLSC. Some limited clinical data released by the company showed an ORR of 32% and disease control rate of 74% in ovarian cancer patients (n = 31) with NaPi2b overexpression [78].
- Datopotamab deruxtecan, also known as Dato-DXd, is another Trop2-directed ADC being jointly developed by AstraZeneca and Daiichi Sankyo. It is made up of a humanized anti-Trop2 IgG1 mAb attached to a deruxtecan payload via a stable tetrapeptide-based cleavable linker. The agent is being studied in a series of TROPION trials series. Data from TROPION-PanTumor01 (NCT03401385) has been published. A total of 24 patients with triple negative breast cancer were treated with Dato-Dxd, with an overall response rate of 43% and a disease control rate of 95%. The most common side effects (any grade) were nausea, stomatitis, fatigue, and vomiting. Thirty-three percent of patients experienced grade 3 or higher treatment-emergent adverse events. Yet, no patients discontinued treatment, and no cases of drug-related interstitial lung disease were reported [79]. More recently, AstraZeneca made an announcement on their website that Dato-DXd met dual primary endpoint in the TROPION-Lung01 phase III trial, but no details have been published yet [80].
6.2. ADC Limitations and Side Effects
7. Conclusions
Supplementary Materials
Author Contributions
Funding
Conflicts of Interest
References
- Strebhardt, K.; Ullrich, A. Paul Ehrlich’s magic bullet concept: 100 years of progress. Nat. Rev. Cancer 2008, 8, 473–480. [Google Scholar] [CrossRef] [PubMed]
- Qi, X.; Li, Y.; Liu, W.; Wang, Y.; Chen, Z.; Lin, L. Research Trend of Publications Concerning Antibody-Drug Conjugate in Solid Cancer: A Bibliometric Study. Front. Pharmacol. 2022, 13, 921385. [Google Scholar] [CrossRef]
- Norsworthy, K.J.; Ko, C.W.; Lee, J.E.; Liu, J.; John, C.S.; Przepiorka, D.; Farrell, A.T.; Pazdur, R. FDA Approval Summary: Mylotarg for Treatment of Patients with Relapsed or Refractory CD33-Positive Acute Myeloid Leukemia. Oncologist 2018, 23, 1103–1108. [Google Scholar] [CrossRef]
- Fu, Z.; Li, S.; Han, S.; Shi, C.; Zhang, Y. Antibody drug conjugate: The “biological missile” for targeted cancer therapy. Signal Transduct. Target Ther. 2022, 7, 93. [Google Scholar] [CrossRef] [PubMed]
- Li, B.T.; Smit, E.F.; Goto, Y.; Nakagawa, K.; Udagawa, H.; Mazieres, J.; Nagasaka, M.; Bazhenova, L.; Saltos, A.N.; Felip, E.; et al. Trastuzumab Deruxtecan in HER2-Mutant Non-Small-Cell Lung Cancer. N. Engl. J. Med. 2022, 386, 241–251. [Google Scholar] [CrossRef] [PubMed]
- Shitara, K.; Bang, Y.J.; Iwasa, S.; Sugimoto, N.; Ryu, M.H.; Sakai, D.; Chung, H.C.; Kawakami, H.; Yabusaki, H.; Lee, J.; et al. Trastuzumab Deruxtecan in Previously Treated HER2-Positive Gastric Cancer. N. Engl. J. Med. 2020, 382, 2419–2430. [Google Scholar] [CrossRef] [PubMed]
- Modi, S.; Jacot, W.; Yamashita, T.; Sohn, J.; Vidal, M.; Tokunaga, E.; Tsurutani, J.; Ueno, N.T.; Prat, A.; Chae, Y.S.; et al. Trastuzumab Deruxtecan in Previously Treated HER2-Low Advanced Breast Cancer. N. Engl. J. Med. 2022, 387, 9–20. [Google Scholar] [CrossRef]
- Zhu, Y.; Liu, K.; Wang, M.; Wang, K.; Zhu, H. Trastuzumab deruxtecan versus trastuzumab emtansine for patients with human epidermal growth factor receptor 2-positive metastatic breast cancer: A cost-effectiveness analysis. Breast 2022, 66, 191–198. [Google Scholar] [CrossRef] [PubMed]
- Jin, Y.; Edalatian Zakeri, S.; Bahal, R.; Wiemer, A.J. New Technologies Bloom Together for Bettering Cancer Drug Conjugates. Pharmacol. Rev. 2022, 74, 680–711. [Google Scholar] [CrossRef]
- Chalouni, C.; Doll, S. Fate of Antibody-Drug Conjugates in Cancer Cells. J. Exp. Clin. Cancer Res. 2018, 37, 20. [Google Scholar] [CrossRef] [PubMed]
- Santi, D.V.; Cabel, L.; Bidard, F.C. Does sacituzumab-govitecan act as a conventional antibody drug conjugate (ADC), a prodrug of SN-38 or both? Ann. Transl. Med. 2021, 9, 1113. [Google Scholar] [CrossRef] [PubMed]
- Manzano, A.; Ocana, A. Antibody-Drug Conjugates: A Promising Novel Therapy for the Treatment of Ovarian Cancer. Cancers 2020, 12, 2223. [Google Scholar] [CrossRef]
- Lambert, J.M.; Berkenblit, A. Antibody-Drug Conjugates for Cancer Treatment. Annu. Rev. Med. 2018, 69, 191–207. [Google Scholar] [CrossRef]
- Vidarsson, G.; Dekkers, G.; Rispens, T. IgG subclasses and allotypes: From structure to effector functions. Front. Immunol. 2014, 5, 520. [Google Scholar] [CrossRef]
- National Center for Biotechnology Information. PubChem Compound Summary for CID 11542188, Monomethyl Auristatin E. 2023. Available online: https://pubchem.ncbi.nlm.nih.gov/compound/Monomethyl-auristatin-E (accessed on 28 July 2023).
- National Center for Biotechnology Information. PubChem Compound Summary for CID 46944733, VcMMAE. 2023. Available online: https://pubchem.ncbi.nlm.nih.gov/compound/VcMMAE (accessed on 28 July 2023).
- Mahmood, I. Clinical Pharmacology of Antibody-Drug Conjugates. Antibodies 2021, 10, 20. [Google Scholar] [CrossRef] [PubMed]
- Sun, X.; Ponte, J.F.; Yoder, N.C.; Laleau, R.; Coccia, J.; Lanieri, L.; Qiu, Q.; Wu, R.; Hong, E.; Bogalhas, M.; et al. Effects of Drug-Antibody Ratio on Pharmacokinetics, Biodistribution, Efficacy, and Tolerability of Antibody-Maytansinoid Conjugates. Bioconjug. Chem. 2017, 28, 1371–1381. [Google Scholar] [CrossRef] [PubMed]
- Satomaa, T.; Pynnonen, H.; Vilkman, A.; Kotiranta, T.; Pitkanen, V.; Heiskanen, A.; Herpers, B.; Price, L.S.; Helin, J.; Saarinen, J. Hydrophilic Auristatin Glycoside Payload Enables Improved Antibody-Drug Conjugate Efficacy and Biocompatibility. Antibodies 2018, 7, 15. [Google Scholar] [CrossRef]
- Ducry, L.; Stump, B. Antibody-drug conjugates: Linking cytotoxic payloads to monoclonal antibodies. Bioconjug. Chem. 2010, 21, 5–13. [Google Scholar] [CrossRef]
- Barok, M.; Joensuu, H.; Isola, J. Trastuzumab emtansine: Mechanisms of action and drug resistance. Breast Cancer Res. 2014, 16, 209. [Google Scholar] [CrossRef]
- von Minckwitz, G.; Huang, C.S.; Mano, M.S.; Loibl, S.; Mamounas, E.P.; Untch, M.; Wolmark, N.; Rastogi, P.; Schneeweiss, A.; Redondo, A.; et al. Trastuzumab Emtansine for Residual Invasive HER2-Positive Breast Cancer. N. Engl. J. Med. 2019, 380, 617–628. [Google Scholar] [CrossRef]
- Powles, T.; Rosenberg, J.E.; Sonpavde, G.P.; Loriot, Y.; Duran, I.; Lee, J.L.; Matsubara, N.; Vulsteke, C.; Castellano, D.; Wu, C.; et al. Enfortumab Vedotin in Previously Treated Advanced Urothelial Carcinoma. N. Engl. J. Med. 2021, 384, 1125–1135. [Google Scholar] [CrossRef] [PubMed]
- Modi, S.; Saura, C.; Yamashita, T.; Park, Y.H.; Kim, S.B.; Tamura, K.; Andre, F.; Iwata, H.; Ito, Y.; Tsurutani, J.; et al. Trastuzumab Deruxtecan in Previously Treated HER2-Positive Breast Cancer. N. Engl. J. Med. 2020, 382, 610–621. [Google Scholar] [CrossRef]
- Bardia, A.; Hurvitz, S.A.; Tolaney, S.M.; Loirat, D.; Punie, K.; Oliveira, M.; Brufsky, A.; Sardesai, S.D.; Kalinsky, K.; Zelnak, A.B.; et al. Sacituzumab Govitecan in Metastatic Triple-Negative Breast Cancer. N. Engl. J. Med. 2021, 384, 1529–1541. [Google Scholar] [CrossRef]
- Rugo, H.S.; Bardia, A.; Marmé, F.; Cortes, J.; Schmid, P.; Loirat, D.; Tredan, O.; Ciruelos, E.; Dalenc, F.; Pardo, P.G.; et al. Primary results from TROPiCS-02: A randomized phase 3 study of sacituzumab govitecan (SG) versus treatment of physician’s choice (TPC) in patients (Pts) with hormone receptor–positive/HER2-negative (HR+/HER2-) advanced breast cancer. J. Clin. Oncol. 2022, 40 (Suppl. S17), LBA1001. [Google Scholar] [CrossRef]
- Coleman, R.L.; Lorusso, D.; Gennigens, C.; Gonzalez-Martin, A.; Randall, L.; Cibula, D.; Lund, B.; Woelber, L.; Pignata, S.; Forget, F.; et al. Efficacy and safety of tisotumab vedotin in previously treated recurrent or metastatic cervical cancer (innovaTV 204/GOG-3023/ENGOT-cx6): A multicentre, open-label, single-arm, phase 2 study. Lancet Oncol. 2021, 22, 609–619. [Google Scholar] [CrossRef]
- Matulonis, U.A.; Lorusso, D.; Oaknin, A.; Pignata, S.; Dean, A.; Denys, H.; Colombo, N.; Van Gorp, T.; Konner, J.A.; Marin, M.R.; et al. Efficacy and Safety of Mirvetuximab Soravtansine in Patients With Platinum-Resistant Ovarian Cancer with High Folate Receptor Alpha Expression: Results From the SORAYA Study. J. Clin. Oncol. 2023, 41, 2436–2445. [Google Scholar] [CrossRef] [PubMed]
- Goundry, W.R.F.; Parker, J.S. Payloads for Antibody–Drug Conjugates. Org. Process Res. Dev. 2022, 26, 2121–2123. [Google Scholar] [CrossRef]
- Conilh, L.; Sadilkova, L.; Viricel, W.; Dumontet, C. Payload diversification: A key step in the development of antibody-drug conjugates. J. Hematol. Oncol. 2023, 16, 3. [Google Scholar] [CrossRef]
- Li, W.; Veale, K.H.; Qiu, Q.; Sinkevicius, K.W.; Maloney, E.K.; Costoplus, J.A.; Lau, J.; Evans, H.L.; Setiady, Y.; Ab, O.; et al. Synthesis and Evaluation of Camptothecin Antibody-Drug Conjugates. ACS Med. Chem. Lett. 2019, 10, 1386–1392. [Google Scholar] [CrossRef]
- Fuentes-Antras, J.; Genta, S.; Vijenthira, A.; Siu, L.L. Antibody-drug conjugates: In search of partners of choice. Trends Cancer 2023, 9, 339–354. [Google Scholar] [CrossRef]
- Nguyen, T.D.; Bordeau, B.M.; Balthasar, J. Mechanisms of ADC Toxicity and Strategies to Increase ADC Tolerability. Cancers 2023, 15, 713. [Google Scholar] [CrossRef]
- Thurston, D.E.; Jackson, P.J.M. Cytotoxic Payloads for Antibody—Drug Conjugates; Royal Society of Chemistry: Cambridge, UK, 2019; 71p. [Google Scholar]
- Kreitman, R.J.; Pastan, I. Antibody fusion proteins: Anti-CD22 recombinant immunotoxin moxetumomab pasudotox. Clin. Cancer Res. 2011, 17, 6398–6405. [Google Scholar] [CrossRef]
- He, L.; Wang, L.; Wang, Z.; Li, T.; Chen, H.; Zhang, Y.; Hu, Z.; Dimitrov, D.S.; Du, J.; Liao, X. Immune Modulating Antibody-Drug Conjugate (IM-ADC) for Cancer Immunotherapy. J. Med. Chem. 2021, 64, 15716–15726. [Google Scholar] [CrossRef]
- Hong, K.B.; An, H. Degrader-Antibody Conjugates: Emerging New Modality. J. Med. Chem. 2023, 66, 140–148. [Google Scholar] [CrossRef] [PubMed]
- Xu, Z.; Ma, J.; Chen, T.; Yang, Y. Case report: The remarkable response of pembrolizumab combined with RC48 in the third-line treatment of metastatic urothelial carcinoma. Front. Immunol. 2022, 13, 978266. [Google Scholar] [CrossRef]
- Emens, L.A.; Esteva, F.J.; Beresford, M.; Saura, C.; De Laurentiis, M.; Kim, S.B.; Im, S.A.; Wang, Y.; Salgado, R.; Mani, A.; et al. Trastuzumab emtansine plus atezolizumab versus trastuzumab emtansine plus placebo in previously treated, HER2-positive advanced breast cancer (KATE2): A phase 2, multicentre, randomised, double-blind trial. Lancet Oncol. 2020, 21, 1283–1295. [Google Scholar] [CrossRef]
- Akaiwa, M.; Dugal-Tessier, J.; Mendelsohn, B.A. Antibody-Drug Conjugate Payloads; Study of Auristatin Derivatives. Chem. Pharm. Bull. 2020, 68, 201–211. [Google Scholar] [CrossRef]
- Kumar, A.; White, J.; James Christie, R.; Dimasi, N.; Gao, C. Antibody-Drug Conjugates. In Platform Technologies in Drug Discovery and Validation; Academic Press: Cambridge, MA, USA, 2017; pp. 441–480. [Google Scholar]
- Takahashi, I.; Takahashi, K.; Ichimura, M.; Morimoto, M.; asano, K.; Kawamoto, I.; Tomita, F.; Nakano, H. Duocarmycin A, a new antitumor antibiotic from Streptomyces. J. Antibiot. 1988, 41, 1915–1917. [Google Scholar] [CrossRef]
- Yao, H.-P.; Zhao, H.; Hudson, R.; Tong, X.-M.; Wang, M.-H. Duocarmycin-based antibody–drug conjugates as an emerging biotherapeutic entity for targeted cancer therapy: Pharmaceutical strategy and clinical progress. Drug Discov. Today 2021, 26, 1857–1874. [Google Scholar] [CrossRef]
- Verkade, J.M.M.; Wijdeven, M.A.; Van Geel, R.; Janssen, B.M.G.; Van Berkel, S.S.; Van Delft, F.L. A Polar Sulfamide Spacer Significantly Enhances the Manufacturability, Stability, and Therapeutic Index of Antibody-Drug Conjugates. Antibodies 2018, 7, 12. [Google Scholar] [CrossRef]
- Guo, J.; Kumar, S.; Chipley, M.; Marcq, O.; Gupta, D.; Jin, Z.; Tomar, D.S.; Swabowski, C.; Smith, J.; Starkey, J.A.; et al. Characterization and Higher-Order Structure assessment of an Interchain Cysteine-Based ADC: Impact of Drug Loading and Distribution on the Mechanism of Aggregation. Bioconjug. Chem. 2016, 27, 604–615. [Google Scholar] [CrossRef] [PubMed]
- Tedeschini, T.; Campara, B.; Grigoletto, A.; Bellini, M.; Salvalaio, M.; Matsuno, Y.; Suzuki, A.; Yoshioka, H.; Pasut, G. Polyethylene glycol-based linkers as hydrophilicity reservoir for antibody-drug conjugates. J. Control Release 2021, 337, 431–447. [Google Scholar] [CrossRef] [PubMed]
- Di, X.; Bright, A.T.; Bellott, R.; Gaskins, E.; Robert, J.; Holt, S.; Gewirtz, D.; Elmore, L. A chemotherapy-associated senescence bystander effect in breast cancer cells. Cancer Biol. Ther. 2008, 7, 864–872. [Google Scholar] [CrossRef] [PubMed]
- Daguenet, E.; Louati, S.; Wozny, A.S.; Vial, N.; Gras, M.; Guy, J.B.; Vallard, A.; Rodriguez-Lafrasse, C.; Magne, N. Radiation-induced bystander and abscopal effects: Important lessons from preclinical models. Br. J. Cancer 2020, 123, 339–348. [Google Scholar] [CrossRef] [PubMed]
- Jin, C.; Wu, S.; Lu, X.; Liu, Q.; Qi, M.; Lu, S.; Xi, Q.; Cai, Y. Induction of the bystander effect in Chinese hamster V79 cells by actinomycin D. Toxicol. Lett. 2011, 202, 178–185. [Google Scholar] [CrossRef] [PubMed]
- Alexandre, J.; Hu, Y.; Lu, W.; Pelicano, H.; Huang, P. Novel action of paclitaxel against cancer cells: Bystander effect mediated by reactive oxygen species. Cancer Res. 2007, 67, 3512–3517. [Google Scholar] [CrossRef] [PubMed]
- Basheerudeen, S.A.; Mani, C.; Kulkarni, M.A.; Pillai, K.; Rajan, A.; Venkatachalam, P. Human brain glioblastoma cells do not induce but do respond to the bleomycin-induced bystander response from lung adenocarcinoma cells. Mutat. Res. 2013, 757, 114–119. [Google Scholar] [CrossRef]
- Li, F.; Emmerton, K.K.; Jonas, M.; Zhang, X.; Miyamoto, J.B.; Setter, J.R.; Nicholas, N.D.; Okeley, N.M.; Lyon, R.P.; Benjamin, D.R.; et al. Intracellular Released Payload Influences Potency and Bystander-Killing Effects of Antibody-Drug Conjugates in Preclinical Models. Cancer Res. 2016, 76, 2710–2719. [Google Scholar] [CrossRef] [PubMed]
- Erickson, H.K.; Park, P.U.; Widdison, W.C.; Kovtun, Y.V.; Garrett, L.M.; Hoffman, K.; Lutz, R.J.; Goldmacher, V.S.; Blattler, W.A. Antibody-maytansinoid conjugates are activated in targeted cancer cells by lysosomal degradation and linker-dependent intracellular processing. Cancer Res. 2006, 66, 4426–4433. [Google Scholar] [CrossRef] [PubMed]
- Wu, S.; Shah, D.K. Determination of ADC Cytotoxicity in Immortalized Human Cell Lines. Methods Mol. Biol. 2020, 2078, 329–340. [Google Scholar] [PubMed]
- Singh, A.P.; Sharma, S.; Shah, D.K. Quantitative characterization of in vitro bystander effect of antibody-drug conjugates. J. Pharmacokinet. Pharmacodyn. 2016, 43, 567–582. [Google Scholar] [CrossRef] [PubMed]
- Verma, S.; Miles, D.; Gianni, L.; Krop, I.E.; Welslau, M.; Baselga, J.; Pegram, M.; Oh, D.Y.; Dieras, V.; Guardino, E.; et al. Trastuzumab emtansine for HER2-positive advanced breast cancer. N. Engl. J. Med. 2012, 367, 1783–1791. [Google Scholar] [CrossRef] [PubMed]
- National Institute of Diabetes and Digestive and Kidney Diseases. Trastuzumab and Ado-Trastuzumab Emtansine. In LiverTox: Clinical and Research Information on Drug-Induced Liver Injury; National Institute of Diabetes and Digestive and Kidney Diseases: Bethesda, MD, USA, 2012. [Google Scholar]
- Thuss-Patience, P.C.; Shah, M.A.; Ohtsu, A.; Van Cutsem, E.; Ajani, J.A.; Castro, H.; Mansoor, W.; Chung, H.C.; Bodoky, G.; Shitara, K.; et al. Trastuzumab emtansine versus taxane use for previously treated HER2-positive locally advanced or metastatic gastric or gastro-oesophageal junction adenocarcinoma (GATSBY): An international randomised, open-label, adaptive, phase 2/3 study. Lancet Oncol. 2017, 18, 640–653. [Google Scholar] [CrossRef]
- FDA Approves Fam-Trastuzumab Deruxtecan-Nxki for HER2-Low Breast Cancer. 2022. Available online: https://www.fda.gov/drugs/resources-information-approved-drugs/fda-approves-fam-trastuzumab-deruxtecan-nxki-her2-low-breast-cancer (accessed on 28 July 2023).
- Ogitani, Y.; Hagihara, K.; Oitate, M.; Naito, H.; Agatsuma, T. Bystander killing effect of DS-8201a, a novel anti-human epidermal growth factor receptor 2 antibody-drug conjugate, in tumors with human epidermal growth factor receptor 2 heterogeneity. Cancer Sci. 2016, 107, 1039–1046. [Google Scholar] [CrossRef] [PubMed]
- FDA DISCO. Burst Edition: FDA Approvals of Enhertu (Fam-Trastuzumab Deruxtecan-Nxki) for Unresectable or Metastatic HER2-Low Breast Cancer, and Nubeqa (Darolutamide) in Combination with Docetaxel for Metastatic Hormone-Sensitive Prostate Cancer. Available online: https://www.fda.gov/drugs/resources-information-approved-drugs/fda-disco-burst-edition-fda-approvals-enhertu-fam-trastuzumab-deruxtecan-nxki-unresectable-or#:~:text=On%20August%205%2C%202022%2C%20the,six%20months%20of%20completing%20adjuvant (accessed on 28 July 2023).
- FDA Approves Fam-Trastuzumab Deruxtecan-Nxki for HER2-Positive Gastric Adenocarcinomas. 2021. Available online: https://www.fda.gov/drugs/resources-information-approved-drugs/fda-approves-fam-trastuzumab-deruxtecan-nxki-her2-positive-gastric-adenocarcinomas (accessed on 28 July 2023).
- Shvartsur, A.; Bonavida, B. Trop2 and its overexpression in cancers: Regulation and clinical/therapeutic implications. Genes Cancer 2015, 6, 84–105. [Google Scholar] [CrossRef] [PubMed]
- FDA Grants Accelerated Approval to Tisotumab Vedotin-Tftv for Recurrent or Metastatic Cervical Cancer. 2021. Available online: https://www.fda.gov/drugs/resources-information-approved-drugs/fda-grants-accelerated-approval-tisotumab-vedotin-tftv-recurrent-or-metastatic-cervical-cancer (accessed on 28 July 2023).
- FDA Grants Accelerated Approval to Mirvetuximab Soravtansine-Gynx for FRα Positive, Platinum-Resistant Epithelial Ovarian, Fallopian Tube, or Peritoneal Cancer. Available online: https://www.fda.gov/drugs/resources-information-approved-drugs/fda-grants-accelerated-approval-mirvetuximab-soravtansine-gynx-fra-positive-platinum-resistant (accessed on 28 July 2023).
- Moore, K.N.; Martin, L.P.; O’Malley, D.M.; Matulonis, U.A.; Konner, J.A.; Perez, R.P.; Bauer, T.M.; Ruiz-Soto, R.; Birrer, M.J. Safety and Activity of Mirvetuximab Soravtansine (IMGN853), a Folate Receptor Alpha-Targeting Antibody-Drug Conjugate, in Platinum-Resistant Ovarian, Fallopian Tube, or Primary Peritoneal Cancer: A Phase I Expansion Study. J. Clin. Oncol. 2017, 35, 1112–1118. [Google Scholar]
- Peng, Z.; Liu, T.; Wei, J.; Wang, A.; He, Y.; Yang, L.; Zhang, X.; Fan, N.-F.; Luo, S.; Gong, J.; et al. A phase II study of efficacy and safety of RC48-ADC in patients with locally advanced or metastatic HER2-overexpressing gastric or gastroesophageal junction cancers. J. Clin. Oncol. 2020, 38 (Suppl. S15), 4560. [Google Scholar] [CrossRef]
- Shi, F.; Liu, Y.; Zhou, X.; Shen, P.; Xue, R.; Zhang, M. Disitamab vedotin: A novel antibody-drug conjugates for cancer therapy. Drug Deliv. 2022, 29, 1335–1344. [Google Scholar] [CrossRef]
- Li, H.; Zhang, X.; Xu, Z.; Li, L.; Liu, W.; Dai, Z.; Zhao, Z.; Xiao, L.; Li, H.; Hu, C. Preclinical evaluation of MRG002, a novel HER2-targeting antibody-drug conjugate with potent antitumor activity against HER2-positive solid tumors. Antib. Ther. 2021, 4, 175–184. [Google Scholar] [CrossRef]
- Jiang, Z.; Sun, T.; Wang, X.; Liu, Q.; Yan, M.; Tong, Z.; Geng, C.; Tang, J.; Yin, Y.; Yu, G.; et al. A multiple center, open-label, single-arm, phase II clinical trial of MRG002, an HER2-targeted antibody-drug conjugate, in patients with HER2-low expressing advanced or metastatic breast cancer. J. Clin. Oncol. 2022, 40 (Suppl. S16), 1102. [Google Scholar] [CrossRef]
- Skidmore, L.; Sakamuri, S.; Knudsen, N.A.; Hewet, A.G.; Milutinovic, S.; Barkho, W.; Biroc, S.L.; Kirtley, J.; Marsden, R.; Storey, K.; et al. ARX788, a Site-specific Anti-HER2 Antibody-Drug Conjugate, Demonstrates Potent and Selective Activity in HER2-low and T-DM1-resistant Breast and Gastric Cancers. Mol. Cancer Ther. 2020, 19, 1833–1843. [Google Scholar] [CrossRef] [PubMed]
- Zhang, J.; Ji, D.; Shen, W.; Xiao, Q.; Gu, Y.; O’Shaughnessy, J.; Xia, G.; Ji, Y.; Xiong, G.; Li, M.; et al. Abstract PD8-04: Safety and anti-tumor activity of ARX788 in HER2-positive metastatic breast cancer patients whose disease is resistant/refractory to HER2 targeted agents (trastuzumab, ADCs, TKIs, and bispecific antibodies): ACE-Breast-01 trial results. Cancer Res. 2022, 82 (Suppl. S4), PD8-04. [Google Scholar] [CrossRef]
- Zhang, Y.; Qiu, M.; Wang, J.; Zhang, Y.; Yuan, X.; Zhang, T.; Yan, J.; Xiong, G.; Ji, Y.; Liang, X.; et al. A phase 1 multicenter, dose expansion study of ARX788 as monotherapy in patients with HER2-positive advanced gastric and gastroesophageal junction adenocarcinoma (ACE-Gastric-01). J. Clin. Oncol. 2021, 39 (Suppl. S15), e16059. [Google Scholar] [CrossRef]
- Saura, C.; Thistlethwaite, F.; Banerji, U.; Lord, S.; Moreno, V.; MacPherson, I.; Boni, V.; Rolfo, C.D.; Vries, E.G.E.D.; Herpen, C.M.L.-V.; et al. A phase I expansion cohorts study of SYD985 in heavily pretreated patients with HER2-positive or HER2-low metastatic breast cancer. J. Clin. Oncol. 2018, 36 (Suppl. S15), 1014. [Google Scholar] [CrossRef]
- Black, J.; Menderes, G.; Bellone, S.; Schwab, C.L.; Bonazzoli, E.; Ferrari, F.; Predolini, F.; De Haydu, C.; Cocco, E.; Buza, N.; et al. SYD985, a Novel Duocarmycin-Based HER2-Targeting Antibody-Drug Conjugate, Shows Antitumor Activity in Uterine Serous Carcinoma with HER2/Neu Expression. Mol. Cancer Ther. 2016, 15, 1900–1909. [Google Scholar] [CrossRef]
- Saura Manich, C.; O’Shaughnessy, J.; Aftimos, P.G.; van den Tweel, E.; Oesterholt, M.; Escrivá-de-Romaní, S.I.; Quenel Tueux, N.; Tan, T.J.; Lim, J.S.; Ladoire, S.; et al. LBA15 Primary outcome of the phase III SYD985.002/TULIP trial comparing [vic-]trastuzumab duocarmazine to physician’s choice treatment in patients with pre-treated HER2-positive locally advanced or metastatic breast cancer. Ann. Oncol. 2021, 32, S1288. [Google Scholar]
- Yurkovetskiy, A.V.; Bodyak, N.D.; Yin, M.; Thomas, J.D.; Clardy, S.M.; Conlon, P.R.; Stevenson, C.A.; Uttard, A.; Qin, L.; Gumerov, D.R.; et al. Dolaflexin: A Novel Antibody-Drug Conjugate Platform Featuring High Drug Loading and a Controlled Bystander Effect. Mol. Cancer Ther. 2021, 20, 885–895. [Google Scholar] [CrossRef]
- Richardson, D.L.; Hamilton, E.P.; Oaknin, A.; Randall, L.M.; Banerjee, S.N.; Taylor, S.K.; Mileshkin, L.R.; Coleman, R.L.; Monk, B.J.; Mirza, M.R.; et al. Uplift (ENGOT-ov67): A pivotal cohort to evaluate XMT-1536 (upifitamab rilsodotin), a NaPi2b-directed antibody drug conjugate for platinum-resistant ovarian cancer. J. Clin. Oncol. 2021, 39 (Suppl. S15), TPS5607. [Google Scholar] [CrossRef]
- Meric-Bernstam, F.; Spira, A.I.; Lisberg, A.E.; Sands, J.; Yamamoto, N.; Johnson, M.L.; Yoh, K.; Garon, E.B.; Heist, R.S.; Petrich, A.; et al. TROPION-PanTumor01: Dose analysis of the TROP2-directed antibody-drug conjugate (ADC) datopotamab deruxtecan (Dato-DXd, DS-1062) for the treatment (Tx) of advanced or metastatic non-small cell lung cancer (NSCLC). J. Clin. Oncol. 2021, 39 (Suppl. S15), 9058. [Google Scholar] [CrossRef]
- Datopotamab Deruxtecan Met Dual Primary Endpoint of Progression-Free Survival in Patients with Advanced Non-Small Cell Lung Cancer in TROPION-Lung01 Phase III trial. 2023. Available online: https://www.astrazeneca-us.com/media/press-releases/2023/datopotamab-deruxtecan-met-dual-primary-endpoint-of-progression-free-survival-in-patients-with-advanced-non-small-cell-lung-cancer-in-tropion-lung01-phase-iii-trial.html (accessed on 28 July 2023).
- Damelin, M.; Zhong, W.; Myers, J.; Sapra, P. Evolving Strategies for Target Selection for Antibody-Drug Conjugates. Pharm. Res. 2015, 32, 3494–3507. [Google Scholar] [CrossRef]
- Khera, E.; Dong, S.; Huang, H.; de Bever, L.; van Delft, F.L.; Thurber, G.M. Cellular-Resolution Imaging of Bystander Payload Tissue Penetration from Antibody-Drug Conjugates. Mol. Cancer Ther. 2022, 21, 310–321. [Google Scholar] [CrossRef] [PubMed]
- Matsumura, Y. Barriers to antibody therapy in solid tumors, and their solutions. Cancer Sci. 2021, 112, 2939–2947. [Google Scholar] [CrossRef] [PubMed]
- Tsumura, R.; Manabe, S.; Takashima, H.; Koga, Y.; Yasunaga, M.; Matsumura, Y. Influence of the dissociation rate constant on the intra-tumor distribution of antibody-drug conjugate against tissue factor. J. Control Release 2018, 284, 49–56. [Google Scholar] [CrossRef] [PubMed]
- Sorkin, M.R.; Walker, J.A.; Kabaria, S.R.; Torosian, N.P.; Alabi, C.A. Responsive Antibody Conjugates Enable Quantitative Determination of Intracellular Bond Degradation Rate. Cell Chem. Biol. 2019, 26, 1643–1651.e4. [Google Scholar] [CrossRef] [PubMed]
- Krop, I.E.; Kim, S.B.; Martin, A.G.; LoRusso, P.M.; Ferrero, J.M.; Badovinac-Crnjevic, T.; Hoersch, S.; Smitt, M.; Wildiers, H. Trastuzumab emtansine versus treatment of physician’s choice in patients with previously treated HER2-positive metastatic breast cancer (TH3RESA): Final overall survival results from a randomised open-label phase 3 trial. Lancet Oncol. 2017, 18, 743–754. [Google Scholar] [CrossRef]
- Parslow, A.C.; Parakh, S.; Lee, F.T.; Gan, H.K.; Scott, A.M. Antibody-Drug Conjugates for Cancer Therapy. Biomedicines 2016, 4, 14. [Google Scholar] [CrossRef]
- Schwaederle, M.; Parker, B.A.; Schwab, R.B.; Daniels, G.A.; Piccioni, D.E.; Kesari, S.; Helsten, T.L.; Bazhenova, L.A.; Romero, J.; Fanta, P.T.; et al. Precision Oncology: The UC San Diego Moores Cancer Center PREDICT Experience. Mol. Cancer Ther. 2016, 15, 743–752. [Google Scholar] [CrossRef]
- Adashek, J.J.; Sapkota, S.; de Castro Luna, R.; Seiwert, T.Y. Complete response to alectinib in ALK-fusion metastatic salivary ductal carcinoma. npj Precis. Oncol. 2023, 7, 36. [Google Scholar] [CrossRef]
- Tateo, V.; Marchese, P.V.; Mollica, V.; Massari, F.; Kurzrock, R.; Adashek, J.J. Agnostic Approvals in Oncology: Getting the Right Drug to the Right Patient with the Right Genomics. Pharmaceuticals 2023, 16, 614. [Google Scholar] [CrossRef]
- Kurzrock, R. Selpercatinib Aimed at RET-Altered Cancers. N. Engl. J. Med. 2020, 383, 868–869. [Google Scholar] [CrossRef]
- Cobain, E.F.; Wu, Y.M.; Vats, P.; Chugh, R.; Worden, F.; Smith, D.C.; Schuetze, S.M.; Zalupski, M.M.; Sahai, V.; Alva, A.; et al. assessment of Clinical Benefit of Integrative Genomic Profiling in Advanced Solid Tumors. JAMA Oncol. 2021, 7, 525–533. [Google Scholar] [CrossRef] [PubMed]
- Flaherty, K.T.; Gray, R.; Chen, A.; Li, S.; Patton, D.; Hamilton, S.R.; Williams, P.M.; Mitchell, E.P.; Iafrate, A.J.; Sklar, J.; et al. The Molecular Analysis for Therapy Choice (NCI-MATCH) Trial: Lessons for Genomic Trial Design. J. Natl. Cancer Inst. 2020, 112, 1021–1029. [Google Scholar] [CrossRef] [PubMed]
- Kato, S.; Kim, K.H.; Lim, H.J.; Boichard, A.; Nikanjam, M.; Weihe, E.; Kuo, D.J.; Eskander, R.N.; Goodman, A.; Galanina, N.; et al. Real-world data from a molecular tumor board demonstrates improved outcomes with a precision N-of-One strategy. Nat. Commun. 2020, 11, 4965. [Google Scholar] [CrossRef] [PubMed]
- Sicklick, J.K.; Kato, S.; Okamura, R.; Patel, H.; Nikanjam, M.; Fanta, P.T.; Hahn, M.E.; De, P.; Williams, C.; Guido, J.; et al. Molecular profiling of advanced malignancies guides first-line N-of-1 treatments in the I-PREDICT treatment-naive study. Genome Med. 2021, 13, 155. [Google Scholar] [CrossRef]
- Sicklick, J.K.; Kato, S.; Okamura, R.; Schwaederle, M.; Hahn, M.E.; Williams, C.B.; De, P.; Krie, A.; Piccioni, D.E.; Miller, V.A.; et al. Molecular profiling of cancer patients enables personalized combination therapy: The I-PREDICT study. Nat. Med. 2019, 25, 744–750. [Google Scholar] [CrossRef]
- Rodon, J.; Soria, J.C.; Berger, R.; Miller, W.H.; Rubin, E.; Kugel, A.; Tsimberidou, A.; Saintigny, P.; Ackerstein, A.; Brana, I.; et al. Genomic and transcriptomic profiling expands precision cancer medicine: The WINTHER trial. Nat. Med. 2019, 25, 751–758. [Google Scholar] [CrossRef]
- Pleasance, E.; Bohm, A.; Williamson, L.M.; Nelson, J.M.T.; Shen, Y.; Bonakdar, M.; Titmuss, E.; Csizmok, V.; Wee, K.; Hosseinzadeh, S.; et al. Whole-genome and transcriptome analysis enhances precision cancer treatment options. Ann. Oncol. 2022, 33, 939–949. [Google Scholar] [CrossRef]
- Bertucci, F.; Goncalves, A.; Guille, A.; Adelaide, J.; Garnier, S.; Carbuccia, N.; Billon, E.; Finetti, P.; Sfumato, P.; Monneur, A.; et al. Prospective high-throughput genome profiling of advanced cancers: Results of the PERMED-01 clinical trial. Genome Med. 2021, 13, 87. [Google Scholar] [CrossRef]
- Berger, R.; Dinstag, G.; Tirosh, O.; Schiff, E.; Kleiner, D.; Aldape, K.D.; Ruppin, E.; Beker, T.; Kurzrock, R. Fibrolamellar carcinoma transcriptomic-based treatment prediction: Complete response after nivolumab and ipilimumab. J. Immunother. Cancer 2022, 10, 12. [Google Scholar] [CrossRef]
- Brown, A.L.; Li, M.; Goncearenco, A.; Panchenko, A.R. Finding driver mutations in cancer: Elucidating the role of background mutational processes. PLoS Comput. Biol. 2019, 15, e1006981. [Google Scholar] [CrossRef]
- Yeh, Y.; Chen, C.; Ko, Y. Effectiveness and cost-effectiveness of trastuzumab emtansine in women with HER2-positive locally advanced or metastatic breast cancer: A systematic review and meta-analysis. J. Cancer Res. Ther. 2022, 18, 1061–1072. [Google Scholar]
- Wang, J.; Yi, Y.; Wan, X.; Zeng, X.; Peng, Y.; Tan, C. Cost-Effectiveness Analysis of Trastuzumab Deruxtecan versus Trastuzumab Emtansine in Human Epidermal Growth Factor Receptor 2-Positive Metastatic Breast Cancer in the USA. Adv. Ther. 2022, 39, 4583–4593. [Google Scholar] [CrossRef] [PubMed]
- Conti, R.M.; Frank, R.G.; Gruber, J. Regulating Drug Prices while Increasing Innovation. N. Engl. J. Med. 2021, 385, 1921–1923. [Google Scholar] [CrossRef] [PubMed]
- Engelberg, A.B.; Avorn, J.; Kesselheim, A.S. A New Way to Contain Unaffordable Medication Costs—Exercising the Government’s Existing Rights. N. Engl. J. Med. 2022, 386, 1104–1106. [Google Scholar] [CrossRef]
- Yang, W.; Soares, J.; Greninger, P.; Edelman, E.J.; Lightfoot, H.; Forbes, S.; Bindal, N.; Beare, D.; Smith, J.A.; Thompson, I.R.; et al. Genomics of Drug Sensitivity in Cancer (GDSC): A resource for therapeutic biomarker discovery in cancer cells. Nucleic Acids Res. 2013, 41, D955–D961. [Google Scholar] [CrossRef]
- Liebmann, J.E.; Cook, J.A.; Lipschultz, C.; Teague, D.; Fisher, J.; Mitchell, J.B. Cytotoxic studies of paclitaxel (Taxol) in human tumour cell lines. Br. J. Cancer 1993, 68, 1104–1109. [Google Scholar] [CrossRef]
- de Vries, J.F.; Zwaan, C.M.; De Bie, M.; Voerman, J.S.; den Boer, M.L.; van Dongen, J.J.; van der Velden, V.H. The novel calicheamicin-conjugated CD22 antibody inotuzumab ozogamicin (CMC-544) effectively kills primary pediatric acute lymphoblastic leukemia cells. Leukemia 2012, 26, 255–264. [Google Scholar] [CrossRef]
- Burns, K.E.; Robinson, M.K.; Thevenin, D. Inhibition of cancer cell proliferation and breast tumor targeting of pHLIP-monomethyl auristatin E conjugates. Mol. Pharm. 2015, 12, 1250–1258. [Google Scholar] [CrossRef] [PubMed]
- Doronina, S.O.; Toki, B.E.; Torgov, M.Y.; Mendelsohn, B.A.; Cerveny, C.G.; Chace, D.F.; DeBlanc, R.L.; Gearing, R.P.; Bovee, T.D.; Siegall, C.B.; et al. Development of potent monoclonal antibody auristatin conjugates for cancer therapy. Nat. Biotechnol. 2003, 21, 778–784. [Google Scholar] [CrossRef] [PubMed]
- Elgersma, R.C.; Coumans, R.G.; Huijbregts, T.; Menge, W.M.; Joosten, J.A.; Spijker, H.J.; de Groot, F.M.; van der Lee, M.M.; Ubink, R.; van den Dobbelsteen, D.J.; et al. Design, Synthesis, and Evaluation of Linker-Duocarmycin Payloads: Toward Selection of HER2-Targeting Antibody-Drug Conjugate SYD985. Mol. Pharm. 2015, 12, 1813–1835. [Google Scholar] [CrossRef]
- Ando, T.; Ishiguro, H.; Kuwabara, Y.; Kimura, M.; Mitsui, A.; Sugito, N.; Mori, R.; Ogawa, R.; Katada, T.; Fujii, Y. Relationship between expression of 5-fluorouracil metabolic enzymes and 5-fluorouracil sensitivity in esophageal carcinoma cell lines. Dis. Esophagus 2008, 21, 15–20. [Google Scholar] [CrossRef]
- Cui, Z.J.; Gao, M.; Quan, Y.; Lv, B.M.; Tong, X.Y.; Dai, T.F.; Zhou, X.H.; Zhang, H.Y. Systems Pharmacology-Based Precision Therapy and Drug Combination Discovery for Breast Cancer. Cancers 2021, 13, 3586. [Google Scholar] [CrossRef] [PubMed]
- Chatterjee, M.; Turner, D.C.; Felip, E.; Lena, H.; Cappuzzo, F.; Horn, L.; Garon, E.B.; Hui, R.; Arkenau, H.T.; Gubens, M.A.; et al. Systematic evaluation of pembrolizumab dosing in patients with advanced non-small-cell lung cancer. Ann. Oncol. 2016, 27, 1291–1298. [Google Scholar] [CrossRef] [PubMed]
- Ho, W.J.; Mehra, R. Pembrolizumab for the treatment of head and neck squamous cell cancer. Expert Opin. Biol. Ther. 2019, 19, 879–885. [Google Scholar] [CrossRef] [PubMed]

{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Drug | Target | Payload | Linker | DAR | Indication of Approval | Date of FDA Approval | Outcomes | Ref. |
|---|---|---|---|---|---|---|---|---|
| Ado-trastuzumab emtansine (Kadcyla) or T-DM | HER2 | Emtansine (DM1) * | Non-cleavable | 3.5 | HER2-positive breast cancer, late stage (EMILIA (phase III) | February 2013 | ORR 43.6% vs. lapatinib + capecitabine 30.8%, p < 0.001, CR 1%, PR 42.6%, PFS 12.6 months (95% CI 8.4–20.8) vs. 6.5 months (95% CI 5.5–7.2) | [21] |
| HER2-positive breast cancer, early stage, adjuvant treatment (KATHERINE Trial) | May 2019 | 3-year IDFS (T1DM vs. trastuzumab), 87.7% (85.2–90.2) vs. 76.9% (73.7–80.1), HR 0.51 (0.40–0.66), 3-year disease-free survival—87.4% (84.9–89.9) vs. 76.9 (73.6–80.1), overall survival 5.7% vs. 7.5% (p = 0.08) | [22] | |||||
| Enfortumab vedotin, EV (Padcev) | Nectin-4 | MMAE * | Enzyme-cleavable | 3.8 | Advanced urothelial cancer (EV-301 Trial) | December 2020 | EV vs. chemotherapy, ORR 40.6% (34.9–46.54) vs. 17.9% (13.7–22.76), p < 0.001; CR 4.9% vs. 2.7%, PR 35.8% vs. 15.2%, SD 31.3% vs. 35.5%, PD 15.3% vs. 28% | [23] |
| Trastuzumab deruxtecan/T-DXd (Enhertu) | HER2 | Deruxtecan ** | Enzyme-cleavable | 8 | HER2-positive unresectable or metastatic breast cancer following two or more prior anti-HER2-based regimens (DESTINY-Breast01 trial) | December 2019 | Single arm, ORR 60.9% (53.4–68), PFS 16.4 months (12.7-not reached), detailed response rates (6.4 mg/kg–7.4 mg/kg): CR 4.2–4.8%, PR 64.6–81%, SD 29.2–14.3% | [24] |
| HER-2-positive advanced gastric or gastrojejunal junction adenocarcinoma (DESTINY-Gastric01 trial) | December 2019 | T-Dxd vs. chemotherapy, confirmed ORR 43% (34–52) vs. 12 (5–24), CR 8% vs. 0, PR 34% vs. 12%, SD 43% vs. 50%, PR 12% vs. 30% | [6] | |||||
| HER2-low unresectable or metastatic breast cancer after 2 or more HER-2 regimens, or rapid (<6 months) recurrence (DESTINY-Breast04) | 5 August 2022 | T-Dxd vs. chemotherapy (all patients), ORR 52.3% (47.1–57.4) vs. 16.3 (11.3–22.5), CR 3.5% vs. 0.5%, PR 48.8% vs. 15.8% | [7] | |||||
| HER2+ unresectable advanced non-small-cell lung cancer (NSCLC) (DESTINY-Lung02 trial) | 11 August 2022 | T-Dxd, ORR 55% (44–65%), CR 1%, PR 54%, SD 37%, PD 3% | [5] | |||||
| Sacituzumab Govitecan (Trodelvy) | Trop2 | SN-38 ** (active metabolite of irinotecan) | Acid-cleavable | 7.6 | Previously treated metastatic triple negative breast cancer (ASCENT Trial) | April 2020 | SG vs. TPC, PFS 4.8 months (4.1–5.8) vs. 1.7 (1.5–2.5), ORR—31% vs. 4%, CR 4% vs. 1%, PR 27% vs. 3%, SD at 6 months 9% vs. 4%, PD 24% vs. 38% | [25] |
| HR+/HER2− metastatic breast cancer patients who had received prior endocrine-based therapy and at least two chemotherapies (TROPiCS-02 trial, Phase II) | 3 February 2023 | SG (n = 272) vs. TPC (n = 271), PFS 5.5 months (4.2–7.0) vs. 4 months (3.1–4.4), OS 14.4 months (13–15.7), 11.2 months (10.1–12.7), | [26] | |||||
| Tisotumab vedotin (Tivdak) | Tissue factor (CD 142) | MMAE * | Enzyme-cleavable | 4 | Recurrent or metastatic cervical cancer (innovaTV 204 trial) | September 2021 | Single arm, ORR 24% (16–33%), CR 7%, PR 17%, SD 49%, PD 24% | [27] |
| Mirvetuximab soravtansine | folate receptor alpha (mirvetuximab) | DM4 * | Cleavable | 3–4 | folate receptor alpha (FRα)-positive, platinum-resistant epithelial ovarian, fallopian tube, or primary peritoneal cancer, who have received one to three prior systemic treatment regimens (Study 0417) | 14 November 2022 | Single arm (n = 96 by BICR), ORR 30.2% (21.3–40.4%), CR (6.3%), PR (24%), SD 56.3%, PD 9.4% | [28] |
| NCT Number | Title | Sponsor/Collaborators | Target | Payload | Linker |
|---|---|---|---|---|---|
| NCT04714190 | A Study of RC48-ADC in Local Advanced or Metastatic Gastric Cancer With the HER2-Overexpression | RemeGen Co., Ltd., Yantai, Shandong, China | HER2 (Hertuzumab) | MMAE | vc-cleavable |
| NCT04400695 | A Study of RC48-ADC for the Treatment of Locally Advanced or Metastatic Breast Cancer With Low Expression of HER2 | ||||
| NCT03500380 | A Study of RC48-ADC Administered Intravenously to Patients With HER2-Positive Metastatic Breast Cancer With or Without Liver Metastases | ||||
| NCT05302284 | A Study of RC48-ADC Combined With Toripalimab For First-line Treatment of Urothelial Carcinoma | ||||
| NCT05329545 | Upifitamab Rilsodotin Maintenance in Platinum-Sensitive Recurrent Ovarian Cancer (UP-NEXT) | Mersana Therapeutics Cambridge, MA USA|GOG Foundation| (ENGOT) | NaPi2b | AF-HPA (DolaLock®) | Protease-cleavable |
| NCT04595565 | Sacituzumab Govitecan in Primary HER2-negative Breast Cancer | German Breast Group| (GEICAM)|ETOP IBCSG Partners Foundation|Cancer Trials Ireland|UNICANCER | Trop-2 | SN38 (irinotecan) | Protease cleavable |
| NCT05609968 | Study of Pembrolizumab (MK-3475) Monotherapy Versus Sacituzumab Govitecan in Combination With Pembrolizumab for Participants With Metastatic Non-small Cell Lung Cancer (NSCLC) With Programmed Cell Death Ligand 1 (PD-L1) Tumor Proportion Score (TPS), (MK-3475-D46) | Merck Sharp & Dohme LLC Rahway, NJ, USA|Gilead Sciences Foster City, CA, USA | |||
| NCT05622890 | A Single-arm Clinical Trial of IMGN853 in Chinese Adult Patients With Platinum-resistant, Epithelial Ovarian Cancer | Hangzhou Zhongmei Huadong Pharmaceutical Co., Ltd. Hangzhou, China | FRα | DM4 | Cleavable |
| NCT05445778 | Mirvetuximab Soravtansine With Bevacizumab Versus Bevacizumab as Maintenance in Platinum-sensitive Ovarian, Fallopian Tube, or Peritoneal Cancer (GLORIOSA) | ImmunoGen, Inc. Waltham, MA, USA|GOG Foundation | |||
| NCT04924699 | A Study of MRG002 in the Treatment of Patients With HER2-positive Unresectable Locally Advanced or Metastatic Breast Cancer | Shanghai Miracogen Inc. Shanghai, China | HER2 (fucosylated trastuzumab) | MMAE | Vc-cleavable |
| NCT05629585 | A Study of Dato-DXd With or Without Durvalumab Versus Investigator’s Choice of Therapy in Patients With Stage I-III Triple-negative Breast Cancer Without Pathological Complete Response Following Neoadjuvant Therapy (TROPION-Breast03) | AstraZeneca, Wilmington, DE, USA|Daiichi Sankyo, Inc. Tokyo, Japan |SWOG Clinical Trials Partnerships | Trop2 (Datopotamab) | Deruxtecan (Dxd) | Tetrapeptide, cleavable |
| NCT05374512 | A Study of Dato-DXd Versus Investigator’s Choice Chemotherapy in Patients With Locally Recurrent Inoperable or Metastatic Triple-negative Breast Cancer, Who Are Not Candidates for PD-1/PD-L1 Inhibitor Therapy (TROPION-Breast02) | AstraZeneca Wilmington, DE, USA |Daiichi Sankyo, Inc. Tokyo, Japan | |||
| NCT05687266 | Study of Datopotamab Deruxtecan (Dato-DXd) in Combination With Durvalumab and Carboplatin for First-Line Treatment of Patients With Advanced NSCLC Without Actionable Genomic Alterations | AstraZeneca Wilmington, DE, USA | |||
| NCT04494425 | Study of Trastuzumab Deruxtecan (T-DXd) vs. Investigator’s Choice Chemotherapy in HER2-low, Hormone Receptor Positive, Metastatic Breast Cancer | AstraZeneca Wilmington, DE, USA |Daiichi Sankyo Company, Limited 3-5-1 Nihonbashihoncho, Chuo-ku, Tokyo, Japan | HER2 (Trastuzumab) | Deruxtecan (Dxd) | Vc-cleavable |
| NCT05426486 | A Study of ARX788 Combined With Pyrotinib Maleate Versus TCBHP (Trastuzumab Plus Pertuzumab With Docetaxel and Carboplatin) as Neoadjuvant Treatment in HER2-positive Breast Cancer Patients | Caigang Liu|NovoCodex Biopharmaceuticals Co., Ltd. Yuecheng, Zhejiang, China |Jiangsu HengRui Medicine Co., Ltd. Lianyungang, Jiangsu Province, China |Shengjing Hospital | HER2 | MMAF (AS269) | para-acetylphenylalamine (pAcF); non-cleavable |
| NCT03262935 * | SYD985 vs. Physician’s Choice in Participants With HER2-positive Locally Advanced or Metastatic Breast Cancer | Byondis B.V. Nijmegen, Netherlands | HER2 (Trastuzumab) | Duocarmazine | Vc-cleavable |
| Agent | Trial (n-Treatment Arm) | Most Common Side Effects (Any Grade) | Grade ≥ 3 Adverse Events | Agent Interruption/Discontinuation | Grade 5 (Deaths) | Ref. |
|---|---|---|---|---|---|---|
| T-DM1 | KATHERINE trial (n = 740) | Any adverse event 98.8%, fatigue 49.5%, nausea 41.6%, thrombocytopenia 28.5%, increased AST 28.4%, headache 28.4%, arthralgia 25.9%, radiation-related skin injury 25.4%, increased ALT 23.1%, epistaxis 21.5%, peripheral sensory neuropathy 18.6%, constipation 17%, myalgia 15.4%, hot flashes 12.8% | Any event 25.7%; thrombocytopenia 5.7%, hypertension 2.0%, radiation-related skin injury 1.4%, peripheral sensory neuropathy 1.4%, neutropenia is 1.2%, hypokalemia 1.2%, fatigue 1.1%, anemia 1.1% | Any event 18%; thrombocytopenia 4.2%, hyperbilirubinemia 2.6%, elevated AST 1.6%, elevated ALT 1.5%, peripheral neuropathy 1.5%, decreased ejection fraction 1.2% | 0.1% | [22] |
| TH3RESA (n = 403) | Nausea 35%, fatigue 29%, headache 24%, vomiting 18%, asthenia 18%, pyrexia 20%, epistaxis 16%, arthralgia 15%, thrombocytopenia 15%, constipation 22%, cough 19%, lack of appetite 16%, myalgia 11%, increased AST 10%, dyspnea 9%, anemia 8%, abdominal pain 6%, rash 6%, neutropenia 5%, and leukopenia 2%. | Any event 40%; thrombocytopenia 5%, increased AST 2%, anemia 1%, neutropenia 2%, fatigue 2%, dyspnea 2%, increased ALT 2%. | 15% Discontinued, 13% dose reduction | 0.6% | [86] | |
| EMILIA (n = 397) | Any event 94.9%, event-specific rates: nausea 39.2%, fatigue 35.1%, diarrhea 23.3%, thrombocytopenia 28%, elevated AST 22.4%, elevated ALT 16.9%, vomiting 19%, hypokalemia 8.6%, neutropenia 5.9%, mucosal inflammation 6.7%, palmar plantar erythrodysesthesia 1.2% | Thrombocytopenia 12.9%, elevated ALT 4.3%, elevated ALT 2.9%, anemia 2.7%, fatigue 2.4%, hypokalemia 2.2%, neutropenia 2%, diarrhea 1.6%, vomiting 0.8%, nausea 0.8% mucosal inflammation 0.2% | T-Dm was discontinued in 5.9% of patients, mainly due to thrombocytopenia | 0. 2% | [56] | |
| T-Dxd | DESTINY-Breast01 (n = 184) | Any adverse event 99.5%, nausea 77.7%, fatigue 49.5%, alopecia 48.4%, vomiting 45.0%, constipation 35.9%, neutropenia 34.8%, decreased appetite 31%, anemia 29.9%, diarrhea 29.3% leukopenia 21.2%, thrombocytopenia 21.2% headache 19.6%, cuff 90%, abdominal pain 16.8%, lymphopenia 14.1%, interstitial lung disease 13.6%, QT prolongation 4.9%, infusion related reaction 2.2%, decreased EF 1.6% | Any adverse event 52.2%, neutropenia 20.7%, anemia 8.7% nausea 7.6%, fatigue 6.0%, vomiting 4.3%, leukopenia 6.0%, thrombocytopenia 3.8%, lymphopenia 6.0%, decreased appetite 1.6%, interstitial lung disease 2.7%, QT prolongation 1.1%, decreased LVEF 0.5%, alopecia 0.5% | Any event 15.2%, dose reduction 23.4%, pneumonitis 5.9%, interstitial lung disease 2.7% | 0.21% | [24] |
| DESTINY-Breast03 (n = 261) | Any event 99.5%, nausea 73%, fatigue 47.7%, alopecia 37.7%, vomiting 34%, neutropenia 33.2%, anemia 33.2%, increased LFTs 23.5%, thrombocytopenia 23.7%, leukopenia 23.2%, diarrhea 22.4%, constipation 21.3%, decreased appetite 20.6%, pneumonitis 12.1% | Any event 52.6%; neutropenia 13.7%, pneumonitis anemia 8.1%, thrombocytopenia 5.1%, fatigue 7.5%, leukopenia 6.5%, decreased appetite 2.4%, increased LFTs 3.2%, nausea 4.6%, vomiting 1.3%, pneumonitis 2.1%, diarrhea 1.1% | Not reported | 0.8% | [7] | |
| DESTINY-Lung01 (n = 91) | Any adverse event 97%, nausea 73%, fatigue 53%, alopecia 46%, vomiting 40%, neutropenia 35%, anemia 33%, diarrhea 33%, decreased appetite 30%, interstitial lung disease 26%, leukopenia 23%, constipation 20%. | Any adverse event 46%, neutropenia 18%, any adverse event 46%, anemia 10%, nausea 9%, fatigue 7%, leukopenia 4%, vomiting 3%, diarrhea 3% | Dose reduction 34%, dose interruption 32%, %, treatment discontinuation 25%, pneumonitis 13%, interstitial lung disease 5% | 2.91% | [5] | |
| Enfortumab vedotin (Padcev) or EV | EV-301 (n = 296) | Any adverse event 93.9%, skin reactions 47%, peripheral neuropathy 46.3%, alopecia 45.3%, peripheral sensory neuropathy 33.8%, pruritus 32.1%, fatigue 31.1%, decreased appetite 30.7%, diarrhea 24.3% dysgeusia 24.3%, nausea 22.6%, anemia 11.5% decrease neutrophil count 10.1%, dry eye 15.9%, infusion related reactions 8.8%neutropenia 6.8%, hyperglycemia 6.4%, decreased leukocyte count 5.4%, febrile neutropenia 0.7% | Any adverse event 51.4%, maculopapular rash 7.4%, fatigue 6.4%, decreased neutrophil count 6.1%, neutropenia 4.7%, diarrhea 3.4%, peripheral sensory neuropathy 3.0%, pruritus 1.4%, decreased white cell count 1.4%, anemia 2.7%, decreased appetite 3%, nausea 1%, febrile neutropenia 0.7% | Dose interruption 51%, dose reduction 32.4%, peripheral sensory neuropathy 15.5%, fatigue 5.4%, decreased neutrophil count 5.1%, rash 3.4%, peripheral neuropathy 3%, anemia 2.7%, drug eruption 2.4% neutropenia 2%, diarrhea 2%, asthenia 2% increased ALT 2% | 0.3% | [23] |
| Sacistuzuzmab Govitecan (SG) | ASCENT trial (n = 235) | Any adverse event 98%, neutropenia 63%, diarrhea 59%, nausea 57%, fatigue 45%, alopecia 46%, anemia 34%, vomiting 29%, nervous system disorders 25%, decreased appetite 20%, constipation 17%, leukopenia 16%, abdominal pain 11%, asthenia 12%, thrombocytopenia 5%, febrile neutropenia 6% | Any adverse event 64%, neutropenia 51%, leukopenia 10%, thrombocytopenia 2%, febrile neutropenia 6%, diarrhea 10%, nausea 3%, vomiting 3%, abdominal pain 1%, fatigue 3%, asthenia 1% | Dose reductions 22%, discontinuation 5%, | 1.27% | [25] |
| Tisotumab vedotin (Tivdak) or TV | innovaTV 204 (n = 101) | Any adverse event 92%, ocular treatment-related events 53% (conjunctivitis 26%, dry eye 23%, keratitis 11%), bleeding 39% (epistaxis 20%, vaginal hemorrhage 7%, hematuria 3%), peripheral neuropathy 33%, alopecia 38%, nausea 27%, fatigue 26%, myalgia 15%, anemia 13%, asthenia 12%, arthralgia 2%, decreased appetite 11%, pruritus 10%, constipation 9% | Any adverse event 28%, neutropenia 3%, fatigue 2%, ulcerative keratitis 2%, peripheral neuropathy 2%, bleeding 2% | Dose interruption 24%, dose reduction 22%, treatment discontinuation 12%, serious adverse events 31%, peripheral neuropathy 2%, pyrexia 2% | 0.9% | [27] |
| Mirvetuximab soravtansine | FDA approval notice and phase I safety study (n = 64) | Diarrhea 43.5%, blurry vision 41.3%, nausea 37%, fatigue 30%, neuropathy 28.3%, keratopathy 26%, AST increased 23.9%, ALT increased 15.2%, vomiting 21.7%, dry 30%, anemia 30%, headache 10.9%, hypokalemia 10.9%, hypomagnesemia 10.9% | Any adverse event 26%, fatigue 4%, hypotension 4%, febrile neutropenia and septic shock 1/64, | Serious adverse events 22% | 0 | [66] |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Kondrashov, A.; Sapkota, S.; Sharma, A.; Riano, I.; Kurzrock, R.; Adashek, J.J. Antibody-Drug Conjugates in Solid Tumor Oncology: An Effectiveness Payday with a Targeted Payload. Pharmaceutics 2023, 15, 2160. https://doi.org/10.3390/pharmaceutics15082160
Kondrashov A, Sapkota S, Sharma A, Riano I, Kurzrock R, Adashek JJ. Antibody-Drug Conjugates in Solid Tumor Oncology: An Effectiveness Payday with a Targeted Payload. Pharmaceutics. 2023; 15(8):2160. https://doi.org/10.3390/pharmaceutics15082160
Chicago/Turabian StyleKondrashov, Aleksei, Surendra Sapkota, Aditya Sharma, Ivy Riano, Razelle Kurzrock, and Jacob J. Adashek. 2023. "Antibody-Drug Conjugates in Solid Tumor Oncology: An Effectiveness Payday with a Targeted Payload" Pharmaceutics 15, no. 8: 2160. https://doi.org/10.3390/pharmaceutics15082160
APA StyleKondrashov, A., Sapkota, S., Sharma, A., Riano, I., Kurzrock, R., & Adashek, J. J. (2023). Antibody-Drug Conjugates in Solid Tumor Oncology: An Effectiveness Payday with a Targeted Payload. Pharmaceutics, 15(8), 2160. https://doi.org/10.3390/pharmaceutics15082160